Preimplantation analysis of kidney biopsies from expanded criteria donors Amaia Sagasta, Ana...
16
Preimplantation analysis of kidney biopsies from expanded criteria donors Amaia Sagasta, Ana Sánchez-Escuredo, Frederic Oppenheimer, Manel Solé Department of Pathology and Kidney Transplant Unit, Hospital Clínic, Barcelona, Spain * DISCLOSURE OF INTEREST: The authors report no conflicts of interest.
-
Upload
pierce-patterson -
Category
Documents
-
view
215 -
download
0
Transcript of Preimplantation analysis of kidney biopsies from expanded criteria donors Amaia Sagasta, Ana...

Preimplantation analysis of kidney biopsies from
expanded criteria donorsAmaia Sagasta, Ana Sánchez-Escuredo,
Frederic Oppenheimer, Manel Solé
Department of Pathology and Kidney Transplant Unit, Hospital Clínic, Barcelona, Spain
* DISCLOSURE OF INTEREST: The authors report no conflicts of interest.

Introduction I• Patients with end-stage renal disease attain longer life
expectancy and better quality of life through kidney transplantation
• Critical shortage of kidneys for transplantation
ONT 2011
> 60 y
45-60 y
30-45 y
15-30 y
< 15 y
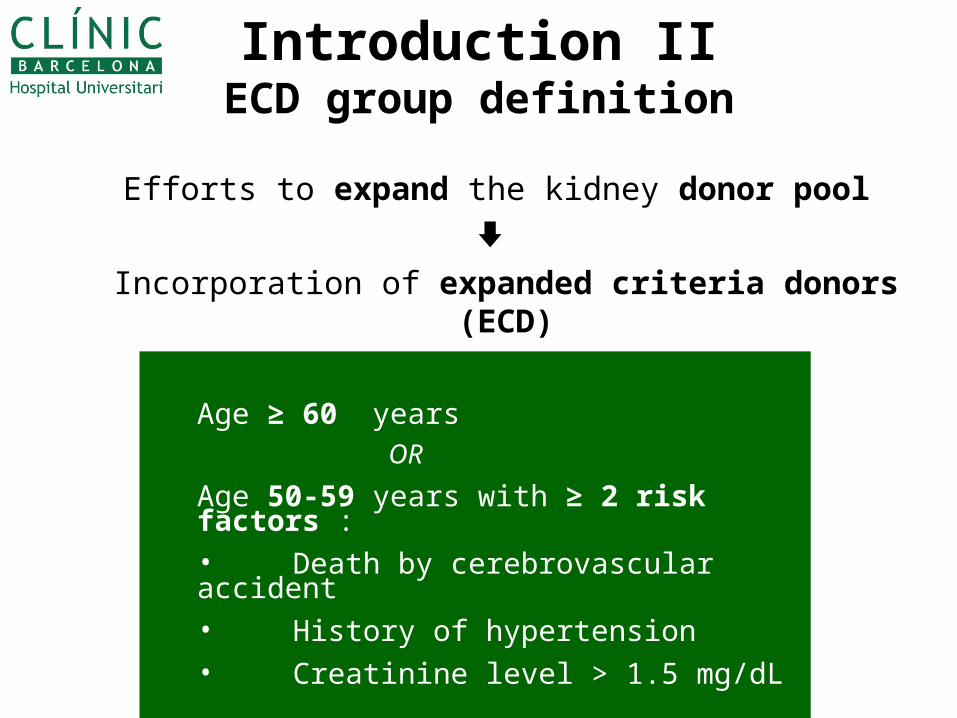
Introduction IIECD group definition
Efforts to expand the kidney donor pool
Incorporation of expanded criteria donors (ECD)
Age ≥ 60 years OR
Age 50-59 years with ≥ 2 risk factors :• Death by cerebrovascular accident• History of hypertension• Creatinine level > 1.5 mg/dL

Introduction IIIECD group associated problems
#ONT 2011
Implanted Discarded (total)
Discarded (due to bx)
USA (ECD) * 59% 41% 51%
Spain (>60y) # 67.5% 32.5% 41.5%
*Sung RS, et al. Transplantation. 2005 May 15;79(9):1257-61
Suboptimal post-transplant function
Shorter graft survival Careful selection of the
grafts before
trasplantation
Preimplantation kidney
biopsy in ECD
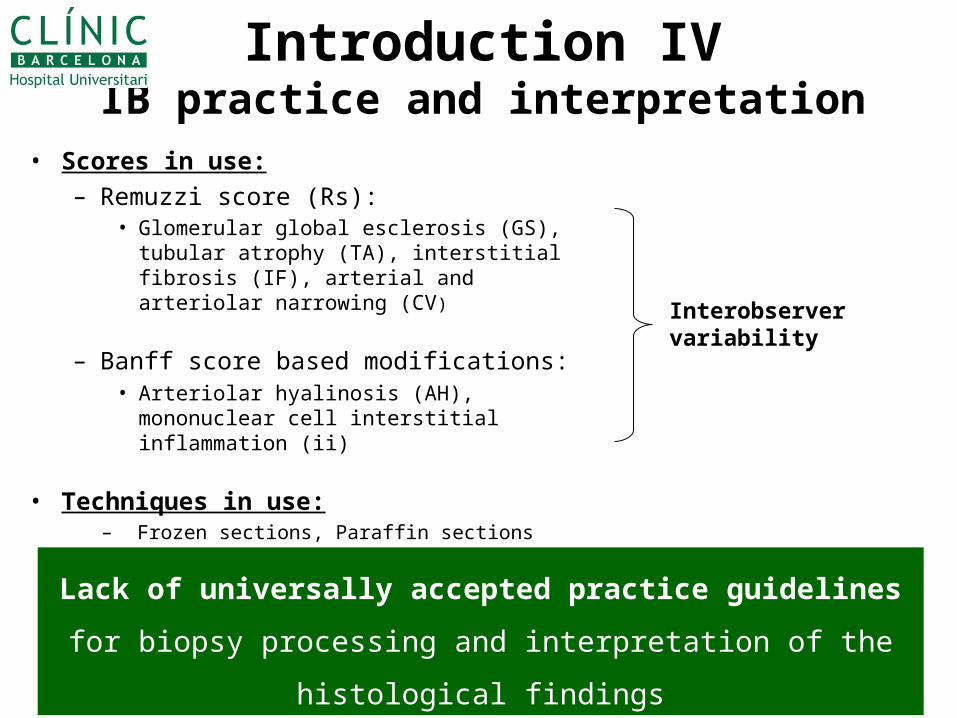
Introduction IVIB practice and interpretation
• Scores in use:– Remuzzi score (Rs):
• Glomerular global esclerosis (GS), tubular atrophy (TA), interstitial fibrosis (IF), arterial and arteriolar narrowing (CV)
– Banff score based modifications:• Arteriolar hyalinosis (AH), mononuclear
cell interstitial inflammation (ii)
• Techniques in use: – Frozen sections, Paraffin sections
Interobserver variability
Lack of universally accepted practice guidelines for biopsy
processing and interpretation of the histological findings
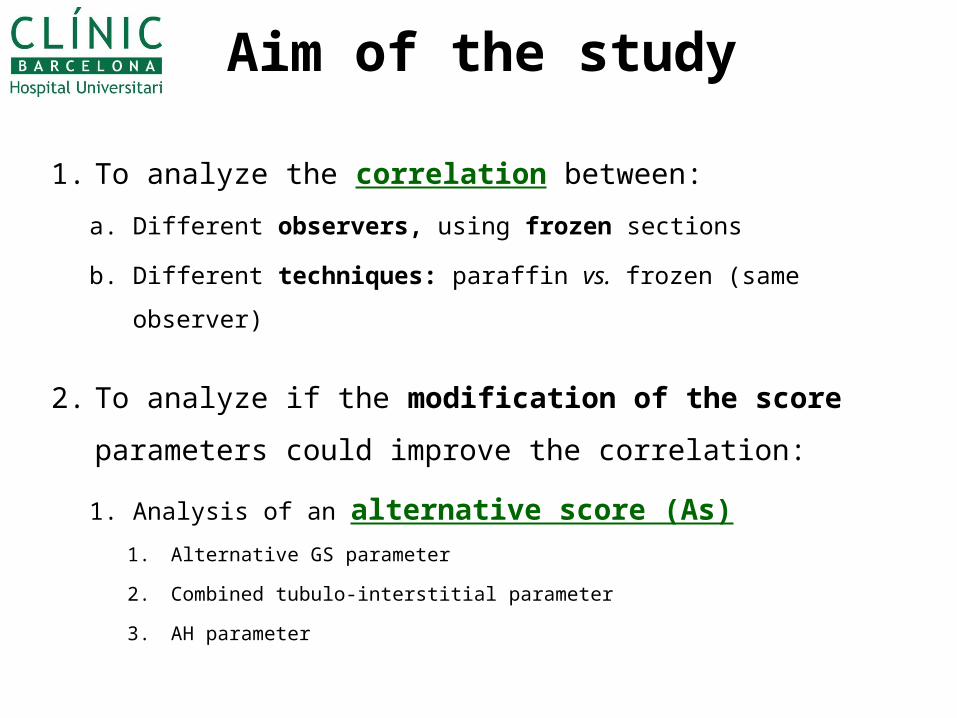
Aim of the study
1. To analyze the correlation between:
a. Different observers, using frozen sections
b. Different techniques: paraffin vs. frozen (same observer)
2. To analyze if the modification of the score
parameters could improve the correlation:
1. Analysis of an alternative score (As)
1. Alternative GS parameter
2. Combined tubulo-interstitial parameter
3. AH parameter
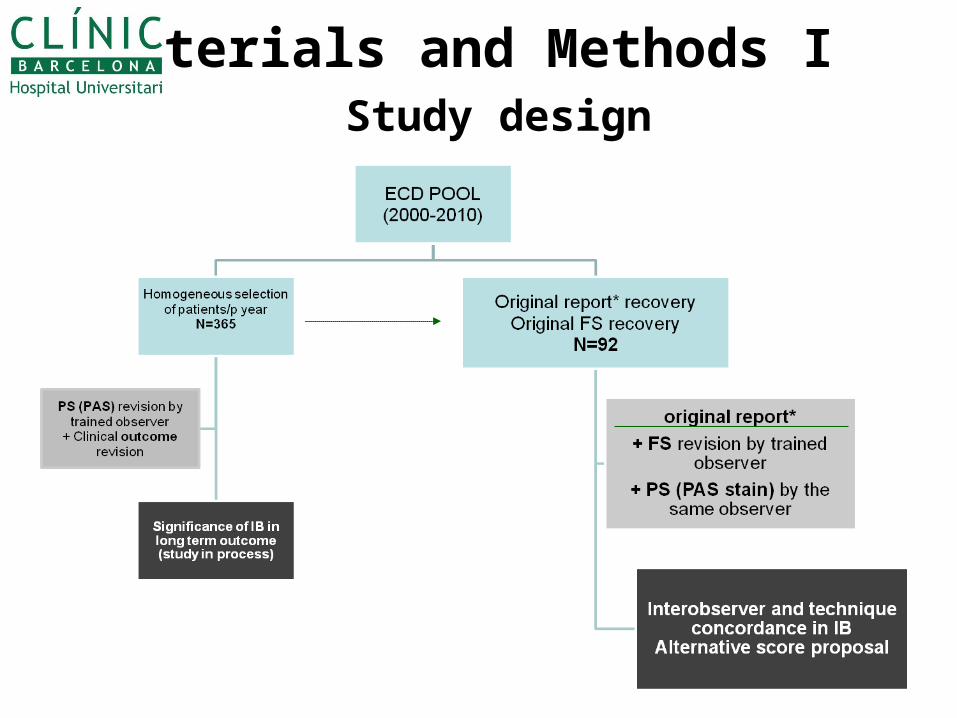
Materials and Methods I Study design

Original report
• Pathologist-on-call: Several
general pathologists
• Time of transplantation
• Frozen section
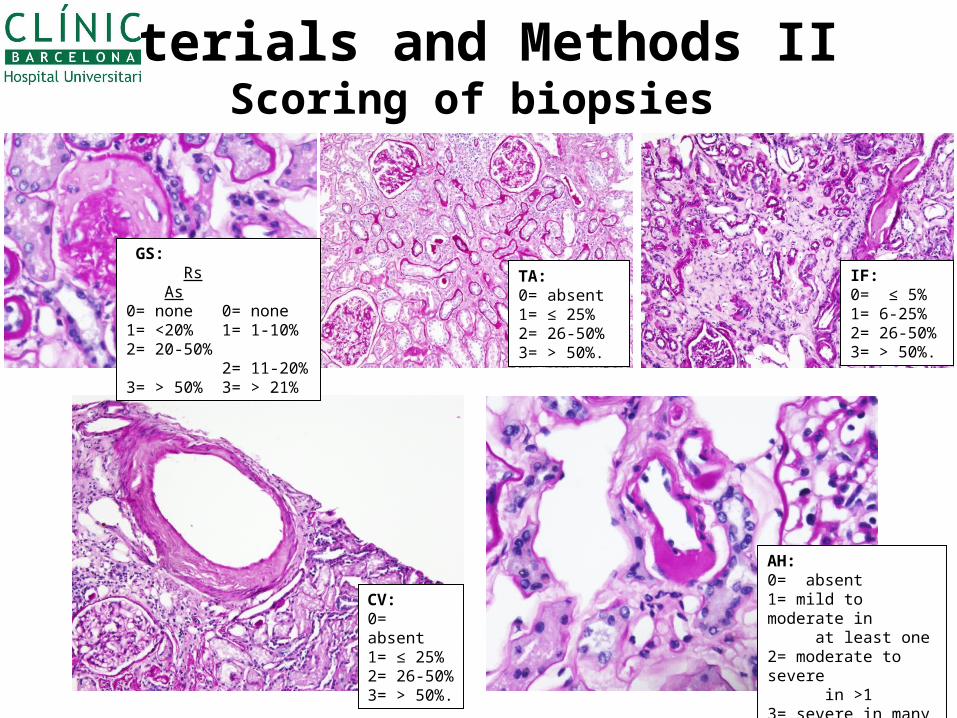
Materials and Methods II Scoring of biopsies
GS: Rs As 0= none 0= none1= <20% 1= 1-10%2= 20-50% 2= 11-20%3= > 50% 3= > 21%
TA:0= absent1= ≤ 25%2= 26-50%3= > 50%.
IF:0= ≤ 5%1= 6-25%2= 26-50%3= > 50%.
CV:0= absent1= ≤ 25%2= 26-50%3= > 50%.
AH: 0= absent1= mild to moderate in at least one2= moderate to severe in >13= severe in many

Materials and Methods IIIElegibility; statistics
• Elegibility for transplant or discard (biopsy): – ≤ 4 points Remuzzi score: acceptance / >4 : discard
• Statistics for concordance in organ elegibility analysis: – Kappa index (K): values between 0 (no agreement) and 1 (perfect
agreement)
• Statistics for correlation analysis (parameters, scores): – Kendall’s Tau b (KTb): values between -1 (perfect disagreement)
and 1 (perfect agreement), 0 (absence of association)

Results I - Parameters
Interobserver
correlation
(frozen sections)
correlation between techniques: PS/FS
(same observer)
Kendall’sTau b Lower C.I.,KTb Upper C.I.,KTb Kendall’s Taub Lower C.I.,KTb Upper C.I.,KTb
GS (Rs) 0.19 -0.06 0.45 0.36 0.13 0.59
GS (As) - - - 0.30 0.11 0.50
TA 0.10 -0.09 0.30 0.16 -0.13 0.45
IF 0.24 0.03 0.44 0.35 0.15 0.55
TA/IF (As) - - - 0.16 -0.13 0.45
CV 0.21 0.005 0.41 0.31 0.11 0.51
AH (As) - - - 0.32 0.18 0.46
PS: parraffin sections (PAS); FS: frozen sections (H/E)
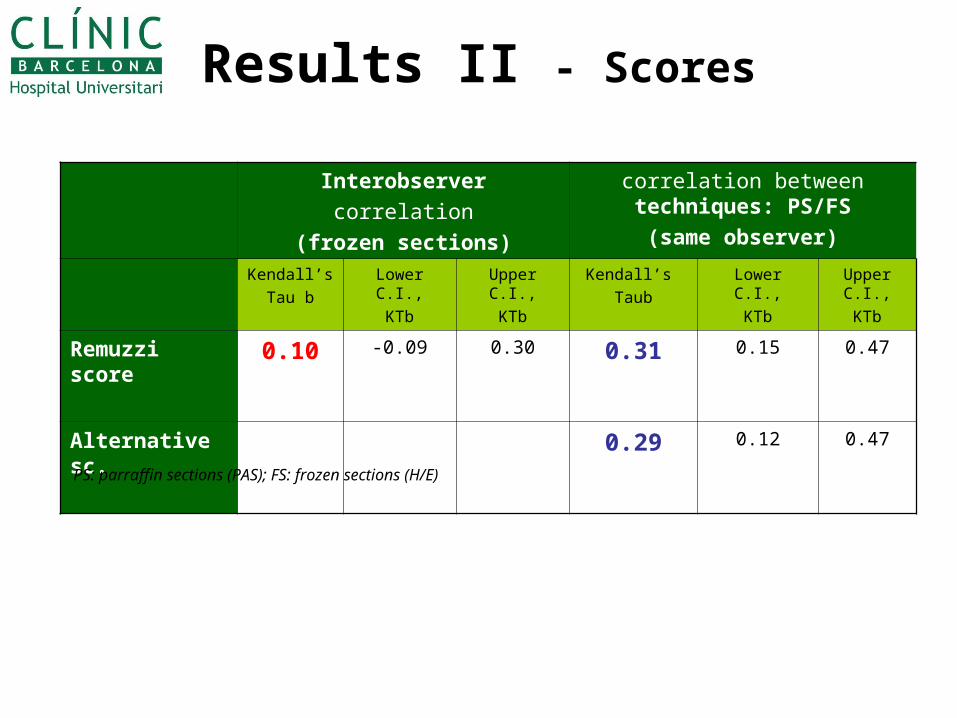
Results II - Scores
Interobserver
correlation
(frozen sections)
correlation between techniques: PS/FS
(same observer)
Kendall’s
Tau b
Lower C.I.,
KTb
Upper C.I.,
KTb
Kendall’s
Taub
Lower C.I.,
KTb
Upper C.I.,
KTb
Remuzzi score 0.10 -0.09 0.30 0.31 0.15 0.47
Alternative sc. 0.29 0.12 0.47
PS: parraffin sections (PAS); FS: frozen sections (H/E)
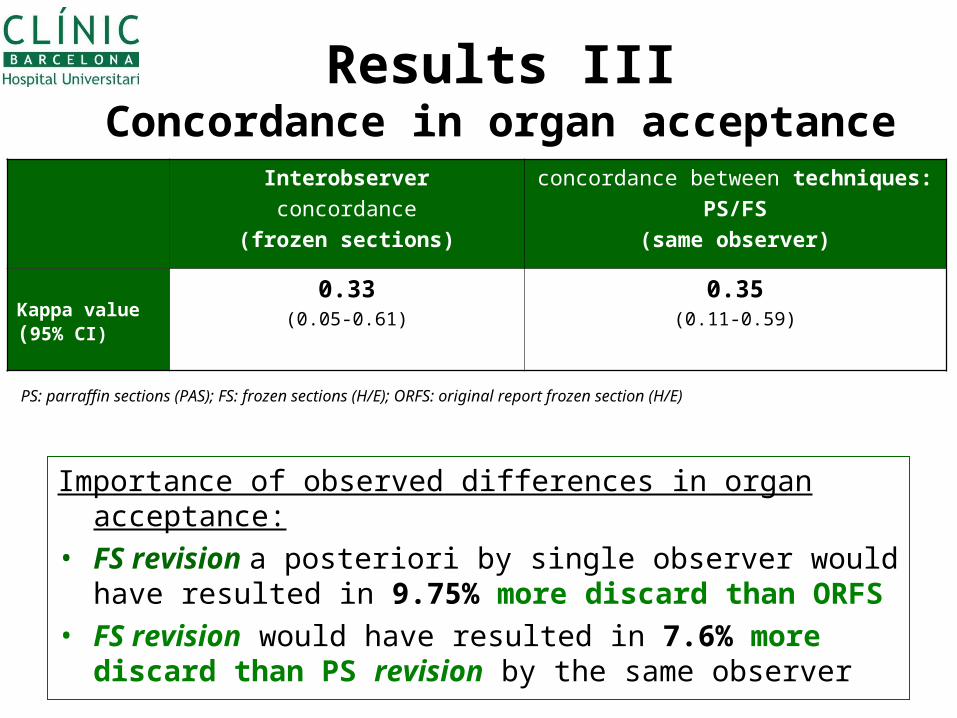
Results IIIConcordance in organ acceptance
Interobserver
concordance
(frozen sections)
concordance between techniques:
PS/FS
(same observer)
Kappa value(95% CI)
0.33(0.05-0.61)
0.35(0.11-0.59)
PS: parraffin sections (PAS); FS: frozen sections (H/E); ORFS: original report frozen section (H/E)
Importance of observed differences in organ acceptance:
• FS revision a posteriori by single observer would have resulted in 9.75% more discard than ORFS
• FS revision would have resulted in 7.6% more discard than PS revision by the same observer
Conclusions
• The evaluation of the score items by a single, trained observer improved the correlation in all values, despite the use of different techniques
• Remuzzi score was the parameter with the best improvement in correlation
• Given the relevance of the observed differences in organ acceptance, specific training is advisable irrespective of the technique used

References
• Remuzzi G, Grinyo J, Ruggenenti P et al. Early experience with dual kidney transplantation in adults using expanded donor criteria. Double Kidney Transplant Group (DKG). J. Am. Soc.Nephrol. 1999; 10; 2591–2598.
• Perico N, Ruggenenti P, Scalamogna M, Remuzzi G.Tackling the shortage of donor kidneys: how to use the best that we have. Am.J.Nephrol.2003;23:245-259.
• Munivenkatappa RB, Schweitzer EJ, Papadimitriou JC et al. The Maryland aggregate pathology index: a deceased donor kidney biopsy scoring system for predicting graft failure. Am. J.Transplant. 2008; 8; 2316–2324.
• El-Husseini A, Sabry A, Zahran A et al.Can Donor implantation renal biopsy predict long-term renal allograft outcome?Am.J.Nephrol.2007;27:144-151
• Snoeijs MG, Boonstra LA, Buurman WA et al.Histological assessment of pre-transplant kidney biopsies is reproducible and representative. Histopathology 2010;56;198-202.
• Sung RS, Christensen LL, Leichtman AB et al.Determinatns of discard of expanded criteria donor kidneys: impact of biopsy and machine perfusion. Am.J.Transplant.2008;8:738-792.
• Furness PN, Taub N, Assmann KJ et al. International variation in histologic grading is large, and persistent feedback does not improve reproducibility. Am. J. Surg. Pathol. 2003; 27; 805–810.
• Organización Nacional de Transplantes (ONT) Database