Prehospital management and recognition: SIRS, Sepsis...
33
Prehospital management and recognition: SIRS, Sepsis and Septic Shock Riverside County EMS Agency Protocol Update Course 2015 SIRS, Sepsis and Septic Shock
Transcript of Prehospital management and recognition: SIRS, Sepsis...
Prehospital management and
recognition: SIRS, Sepsis and Septic Shock Riverside County EMS Agency Protocol Update Course 2015 SIRS, Sepsis and Septic Shock
Objectives O Define systemic inflammatory response
syndrome (SIRS) O Identify SIRS criteria O Understand pathophysiology of SIRS O Understand relationships and interplay
between SIRS and sepsis O Identify and describe the spectrum of sepsis O Discuss Early Goal Directed Therapy O Identify EMS treatment for SIRS and sepsis
What is SIRS? O SIRS is Systemic Inflammatory Response
Syndrome O A clinical response to an insult to the body
that is either infectious or noninfectious O Can come from ischemia, trauma, infection,
inflammation or combined insults
Presenter
Presentation Notes
Systemic inflammatory response DOES NOT have to come from an infection, but it is an early herald for deranged physiology
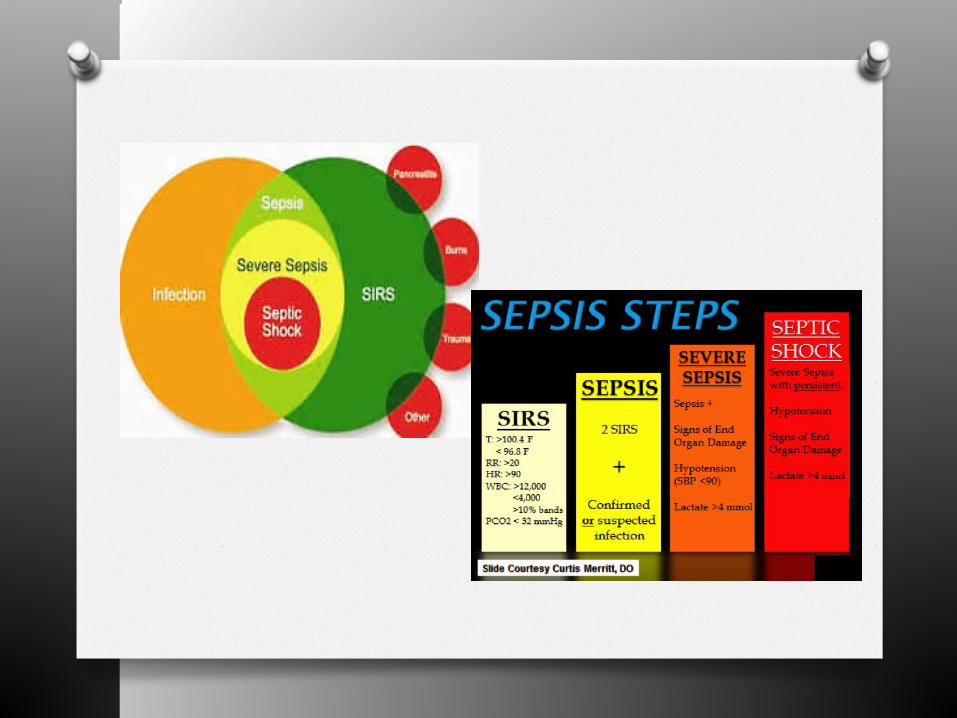
SIRS Criteria O SIRS has a set of objective identifiers:
O Heart rate > 90 bpm O Respiratory rate > 20 breaths/min or an
arterial CO2 of < 32 mmHg O Temperature > 100.4°F or < 96.8°F O Abnormal WBC count (> 12,000 µL or <
4,000 µL) O Serum lactate levels ≥ 4 mmol/L O *SBP < 90 mmHg has been added by some
facilities
Presenter
Presentation Notes
SIRS criteria in use at our paramedic receiving centers are very similar to this; some measures are adapted to be slightly higher/lower depending on the receiving facility (CONCEPTS are the same)
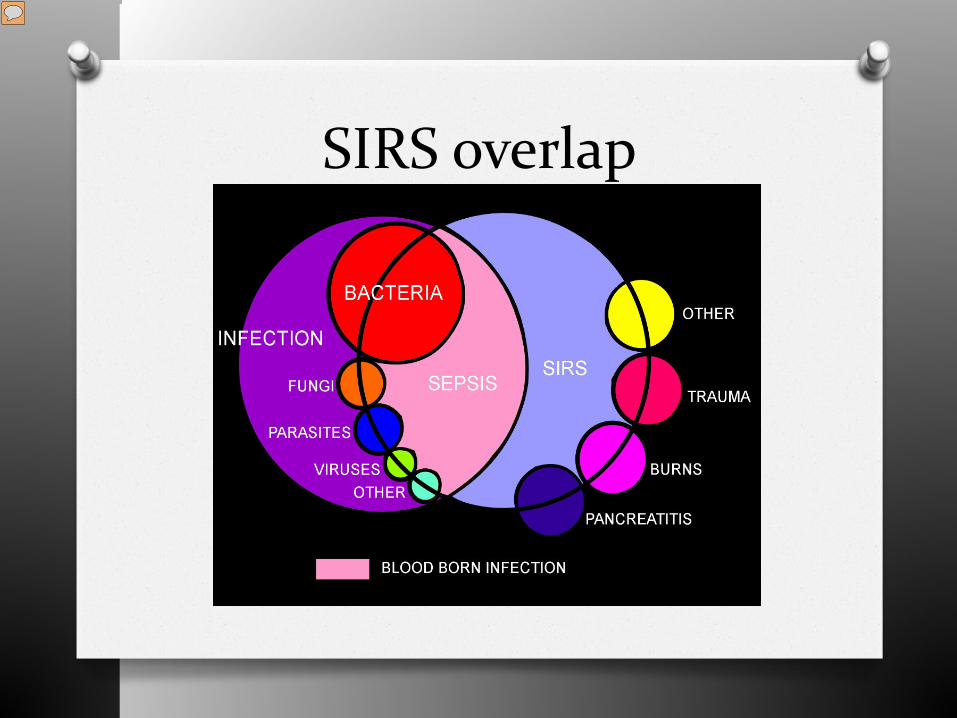
SIRS overlap
Presenter
Presentation Notes
Causes of SIRS can include: Other (yellow dot) Trauma (dark pink dot) Burns (bright pink dot) Pancreatitis (Blue dot) - SIRS and Sepsis often overlap – but in this case SIRS is present with a known/suspected source of infection
Pathophysiology of SIRS O Bone’s stage theory (paraphrased)
O Insult/injury local inflammatory response local redness/edema/warmth localized macrophages for defense growth factors and systems activated to restore function/repair system balanced by CARS (Counter inflammatory response syndrome)
O If unchecked blood vessel integrity is damaged
Presenter
Presentation Notes
Stage I Following an insult, cytokines are produced at the site. Local cytokin production incites an inflammatory response, thereby promoting wound repair and recruitment of the reticular endothelial system Stage II Small quantities of local cytokines are released into the circulation, improving the local response. This leads to growth factor stimulation and the recruitment of macrophages and platelets. This acute phase response is typically well controlled by a decrease in the proinflammatory mediators and by the release of endogenous antagonists; the goal is homeostasis. Stage III If homeostasis is not restored, a significant systemic reaction occurs. The cytokine release leads to destruction rather than protection. A consequence of this is the activation of numerous humoral cascades and the activation of the reticular endothelial system and subsequent loss of circulatory integrity. This leads to end-organ dysfunction.
SIRS and Coagulation (Pathophysiology continued…)
O SIRS can progress to cause repeated and increased production of thrombin O Promoting coagulation O Promoting further inflammation as well
O Unchecked this will lead to large amounts of
microvascular coagulation and eventual organ dysfunction.
Presenter
Presentation Notes
Interleukin-1 and Tumor Necrosis Factor- alpha directly affect the endothelial lining of all lumens (blood vessels, GI tract, heart chambers – anything with endothelial lining). These two chemicals (IL-1, TNF- alpha) lead to the expression of tissue factor. Tissue Factor is part of the clotting cascade, and activates the cascade to block leakage from the damaged lumens. However, inflammation is a positive feedback loop…. - unless inflammation is balanced or controlled, it will progress until thrombin forms micro clots systemically. These clots will block organs from functioning, leading to further inflammation, further repeats of the cycle.
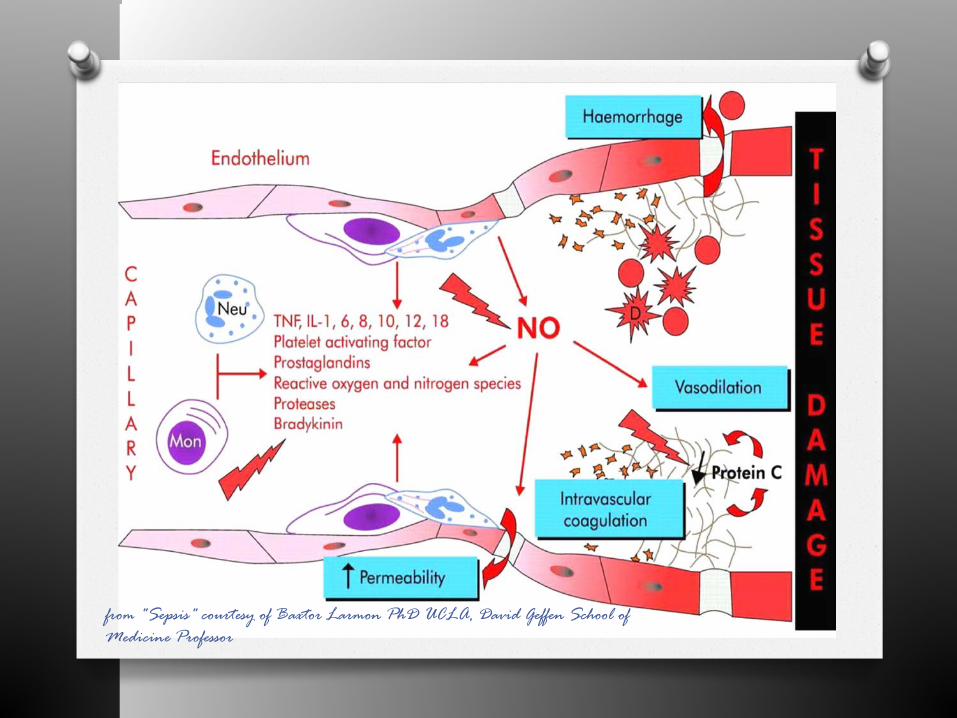
from "Sepsis" courtesy of Baxtor Larmon PhD UCLA, David Geffen School of Medicine Professor

Multiple Organ Dysfunction Syndrome (MODS)
O Occurs when there is organ dysfunction O Organ dysfunction occurs from:
O Hypoxia O Uncontrolled cell death O Direct cytotoxicity O Immunosuppression (imbalance in SIRS and
CARS)
Presenter
Presentation Notes
Organ dysfunction can be mild or severe Cells are programmed to die at certain intervals (apoptosis) – in MODS this apoptosis is unbalanced CARS – counter inflammatory response syndrome
SIRS and MODS O SIRS can lead to MODS if the origin of the
insult or injury isn’t identified and the patient appropriately resuscitated.
O MODS is often irreversible and has a high degree of mortality O Prehospital interventions can prevent MODS
from occurring.
Presenter
Presentation Notes
SIRS – systemic inflammatory response syndrome MODS – multiple organ dysfunction syndrome
Infection O Defined:
O A microbial presence inside a host’s normal tissues that may or may not cause an inflammatory response.
Presenter
Presentation Notes
There are infectious and non-infectious causes of SIRS: causes with infection can range from cholecystitis, to influenza to meningitis, cellulitis, pyelonephritis and other “-itis” infections non infectious causes of SIRS can be related to dehydration, drug reactions, autoimmune disorders, MI’s, seizures and transfusion reactions.
Sepsis (and SIRS) O Defined:
O The organism’s systemic response to infection O Perpetuated by response to endotoxin
O Characterized by the presence of: O 2 SIRS criteria O Presumed/known infection
Presenter
Presentation Notes
Discuss sources/common sites of infection – give concrete examples: - indwelling catheters (peripheral IV, urinary catheters, central lines, feeding tubes, shunts) - UTI, pyelonephritis, cholecystitis, diverticulitis, appendicitis - infectious diseases (Meningitis, pneumonia, TB, influenza, etc, etc) - cellulitis, osteomyelitis


Spectrum of Sepsis
OSepsis Severe Sepsis Septic Shock Irreversible Shock MODS Death
Presenter
Presentation Notes
If sepsis is unrecognized, unmanaged the patient will often progress inevitably towards irreversible state Amount of time in each stage is unpredictable and complicated by comorbidities such as age, immune health, medical history, etc.

SIRS Research O Prospective study of tertiary care center
admissions – 68% of hospital admissions met SIRS criteria. O Incidence of SIRS ↑ as patient acuity ↑
O Of those with SIRS over 25% developed sepsis, 18% developed severe sepsis, 4% developed septic shock within 28 days of admission
O Comstedt et al (2009 Scandinavia) cohort study that showed that 62% of patients presenting to the ER with SIRS had a confirmed infection.
Presenter
Presentation Notes
Emphasize that SIRS & Sepsis can be found independent of each other. A patient can have SIRS from a noninfectious source. When infection is suspected/present, in conjunction with 2 SIRS criteria (or more), then sepsis should be assessed for, and the patient treated accordingly.
SIRS and Sepsis Research O Angus et. al found the incidence of SIRS
associated with an infection to be 3 cases per 1,000 population, or 2.26 per 100 hospital discharges.
O Wang et. al EMS system (Boston, MA) comparison: EMS provides initial care for more than 1/3 of all ED sepsis patients O Opportunity!!
Presenter
Presentation Notes
Riverside Community Hospital 243 sepsis cases March 2014-August 2014 (ambulance arrival patients) Desert Regional MC: 222 total sepsis cases (Jan-Aug 2014) - Opportunity: EMS Providers can recognize SIRS and Sepsis and begin initial treatment and resuscitation, drastically decreasing mortality from sepsis.
Sepsis Research O More than 1.1 million cases annually as of
2008 O Sepsis is the 10th leading cause of death in
the US O Mortality rates estimated 25-50% O Snapshot reference (March – August 2014 at
RCH sepsis mortality was 37%) O That’s is higher that cardiac arrests, MI or
stroke (combined)
How does the hospital deal with sepsis?
* Unique to each facility O Implement and follow “Surviving Sepsis
Campaign Guidelines for Management of Severe Sepsis and Septic Shock” O Team approach with a structured process
O Checklist and “code team activations” O Often called “code sepsis”
O Early Goal Directed Therapy (EGDT)
Surviving Sepsis Guidelines were updated in 2012
Presenter
Presentation Notes
* Many Riverside County facilities have a “Code Sepsis” and a specialized care team, though not all of them do. MICN’s at some facilities have updated radio contact forms that now have screening questions to assist with the early notification process.
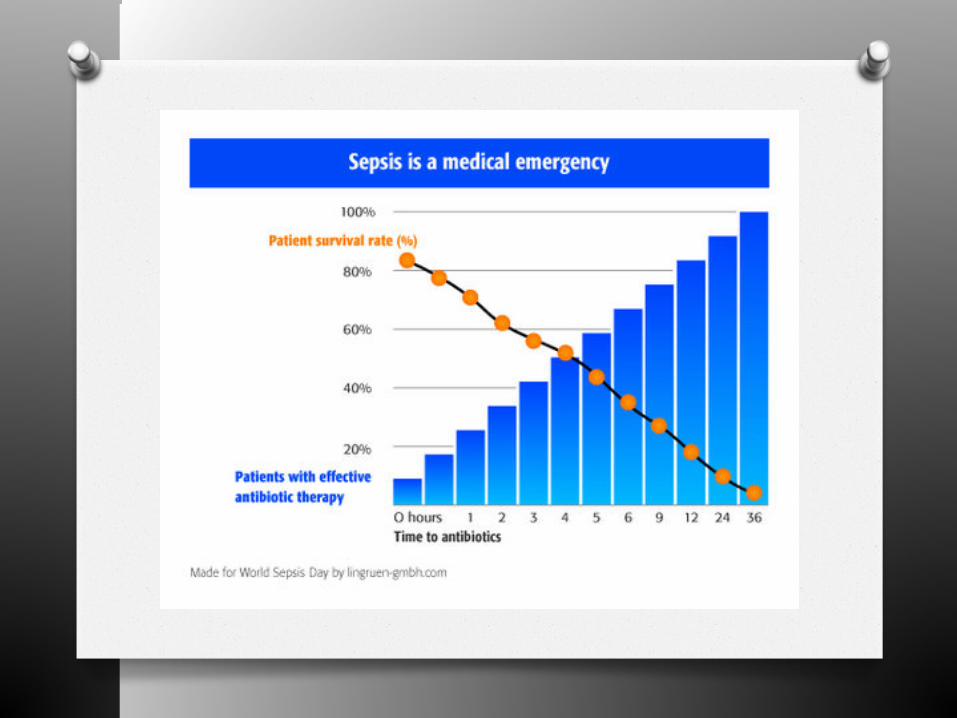
EGDT O Early Goal Directed Therapy
O Structured interventions that have fluids, vasopressors, steriods and antibiotics administered to the patient at critical time intervals.
O Largest overwhelming goal: O Broad spectrum antibiotics administered IV to
patient within 60 minutes of recognition of sepsis
O Blood cultures drawn before antibiotics
Presenter
Presentation Notes
EGDT goals no different than STEMI or STROKE time frames for door to balloon/door to drug Each hospital has their own approach, but they use similar criteria and checklists Some base stations integrating SIRS/Sepsis questions into their MICN Forms for early recognition
EGDT in EMS O EMS can play an active role in the
beginnings of sepsis treatment O #1 priority is recognition of this patient type O Sepsis patients can present in the covert
compensated state to the overt decompensated state O i.e. stable with sepsis, to the decompensating
unstable septic shock patient
Presenter
Presentation Notes
Studies show that EMS intervention and recognition of sepsis can decrease ED antibiotic administration time by nearly 20%. Early recognition in the ED + early antibiotic administration has been shown to decrease morbidity and mortality of sepsis.
EMS Treatment\Recognition
O Assess patient for SIRS criteria (it just takes two): O HR > 90 bpm O RR > 20 breaths/min O Capnography readings < 32 mmHg
O Particular attention should be given when this reading is < 25 mmHg as this is highly suggestive of an elevated lactate
O Temperature > 100.4°F O SBP < 90 mmHg
EMS Treatment\Recognition
O If patient meets SIRS criteria (only two are needed) then next: O Evaluate for infection (known/suspected)
O Look for common sources/sites for infection O Physical exam findings
O If an infection is known/suspected + SIRS criteria are met then notify the hospital early of your suspicions
O Treat life threats appropriately
Presenter
Presentation Notes
SIRS Criteria + known/suspected infection – HIGH likelihood that your patient has sepsis and EGDT could apply to them!
EMS Treatment\Recognition
O Mortality is most decreased by: O Establishing and maintaining the patient’s airway
O Supplemental O2 to advanced airway placement – as clinically indicated/required.
O Maintaining circulating blood volume
O Appropriate vascular access (IV or IO) O Fluid resuscitation – appropriate bolus repeated
as needed to maintain perfusion O Assess your patient’s response to therapy
O Intervene as often as patient condition demands
Presenter
Presentation Notes
How do you know when to stop giving fluids? It’s not always just 250 ml for the adult. It could be more. ASSESS!! - tachycardia resolves or bradycardia improves - SBP is sufficient to give a strong distal pulse - MAP improves, DBP increases. - mental status improves - skin turgor improves - skin signs improve - CHF develops (if this happens then stop fluid boluses, and treat the CHF)
Reminders: O Sepsis becomes septic shock if untreated or
under-managed O Septic shock is a distributive shock
O DBP ↓↓ as condition worsens O Pulses will often be bounding to compensate O Large amounts of fluid resuscitation are often
needed – repeat boluses! O Assess your patient’s response to therapy
O Not all patients are febrile! (aspirin anyone)
Presenter
Presentation Notes
Emphasize: fluid boluses can be repeated. Reassessment of vital signs (a full BP, LOC, skin signs) are of paramount importance. Document the patient’s response to therapy - Aspirin is one of the most commonly taken OTC meds in patients > 35. Aspirin is an anti-pyretic, and limits the presentation of fever.
Knowledge Check Case Review:
O 28 year old female patient, calls 911 for lower quadrant abdominal and flank pain. HR 110 bpm, RR 24 breaths/min, skins are hot to the touch. She describes dysuria, with blood present intermittently. O Does this patient meet SIRS criteria? O Is there evidence to support a
known/suspected infection?
Knowledge Check:
O SIRS? YES O Known/suspected infection? YES
Presenter
Presentation Notes
SIRS? YES HR is elevated RR is elevated Skins are hot Known or suspected infection? YES - Possible medical conditions: UTI, pyelonephritis, cystitis, kidney stones with obstruction, etc.
Case Review #2 O 74 year old male patient calls 911 for
dyspnea. The patient is found pale, cool, diaphoretic with an irregular heartbeat @ 114; RR of 36, labored; and BP is 80/30. Lung sounds reveal fine crackles, physical exam shows dependent edema. O Does this patient meet SIRS criteria? O Is there evidence to support a
known/suspected infection?
Knowledge Check:
O SIRS? YES O Known/suspected infection? NO
Presenter
Presentation Notes
SIRS? YES HR is elevated RR is elevated BP is low Known or suspected infection? NO - Possible medical conditions: CHF, cardiogenic shock, MI
Objectives O Define systemic inflammatory response
syndrome O Identify systemic inflammatory response
syndrome criteria O Understand pathophysiology of SIRS O Understand relationships and interplay between
SIRS and sepsis O Identify and describe the spectrum of sepsis O Discuss EGDT O Identify EMS treatment for SIRS and sepsis
QUESTIONS?
References O NCHS Data Brief No.. 62 June 2011 “Inpatient Care for Septicemia or
Sepsis: A Challenge for Patients and Hospitals” O www.cdc.gov/sepsis O www.survivingsepsis.org O Baxter Larmon Ph.D. “Sepsis” Instructional Presentation
(www.cpc.mednet.ucla.edu) O Wang et al. Resuscitation “Opportunities for Emergency Medical
Services care of Sepsis” November 2009. O Studnek et al American Journal of Emergency Medicine “The impact of
emergency medical services on the ED care of severe sepsis” Jan 2012.
O www.sccm.org “International Guidelines for Management of Severe Sepsis and Septic Shock 2012.
O Riverside County Prehospital Liaison Nurses, data collection for individual statistics reporting.
O Herlitz et al. Scandinavian Journal EM “Suspicion and treatment of severe sepsis. An overview of the prehospital chain of care” Jan 2012