Medical disorders in Pregnancy & Complications in pregnancy Tutorial.
Upload
bcooper876Category
view
922download
0
Late Complications in Pregnancy
Grand Rounds Presentation
Whitney Lewis DO, MS
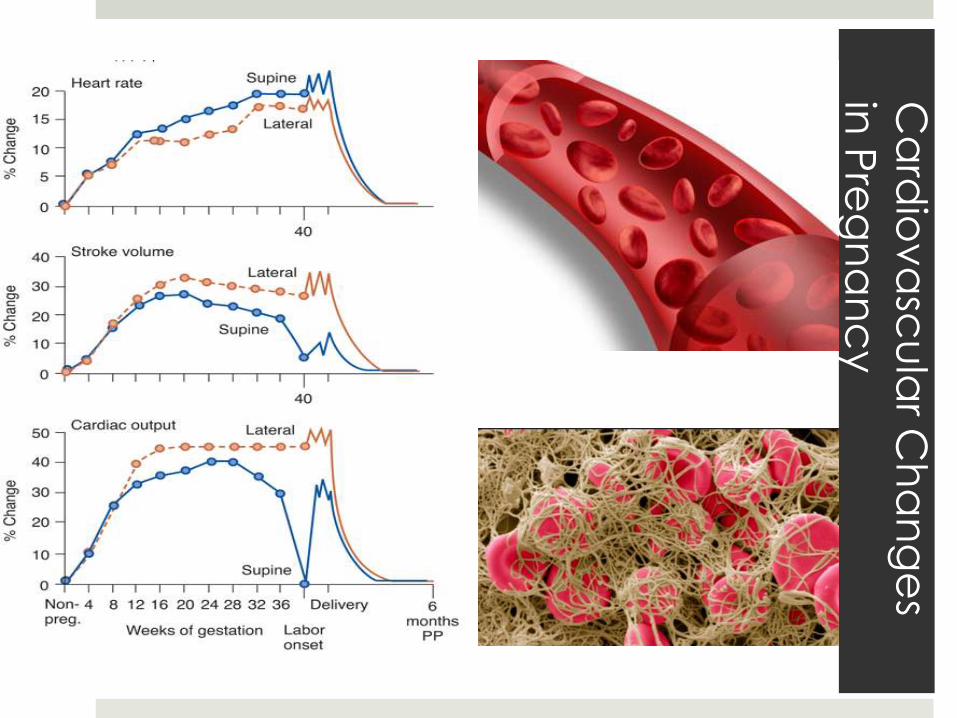
Ca
rdio
va
scu
lar C
ha
ng
es
in P
reg
na
nc
y
UCC transfer for CP
25yo G3P2 39 wks, no PMH with acute onset of sharp, non-
radiating R sided chest pain PTA, SOB and LLE edema.
EKG: ST
VS: HR 110, RR 26, BP 108/76, Temp 36.8, SpO2 94%
Pulmonary Embolism
Leading cause of morbidity/mortality
High pretest probability of DVT/PE = HIGH RISK
Aortic Dissection
PTX
Pneumonia/URTI
ACS/UA
Esophageal Perforation
Pericarditis/Myocarditis
Pleuritis
Cardiac Tamponade
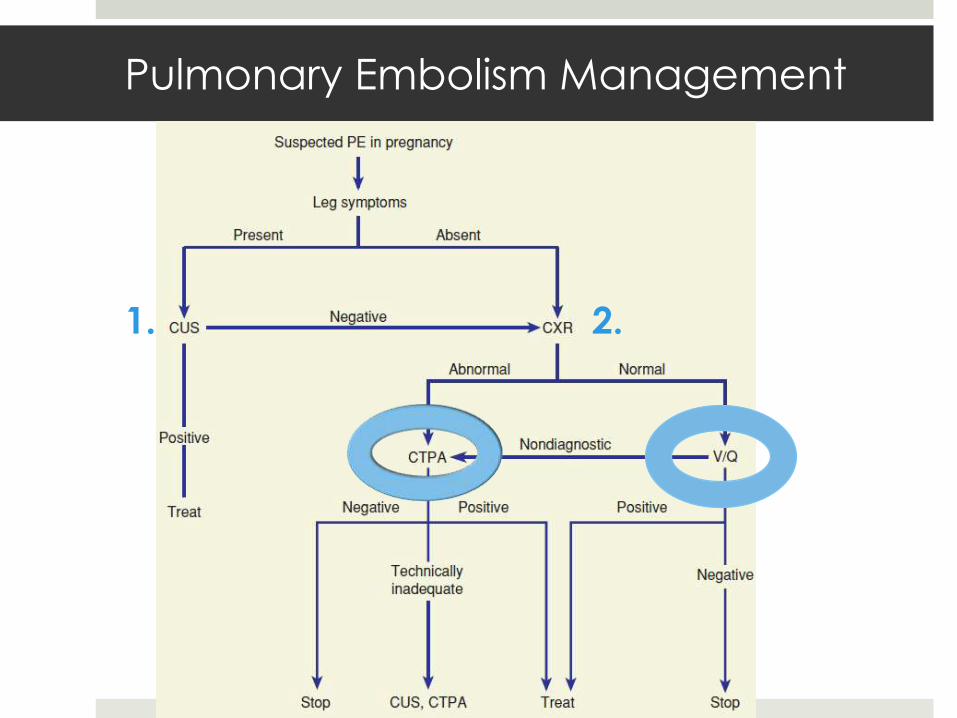
Pulmonary Embolism Management
1. 2.
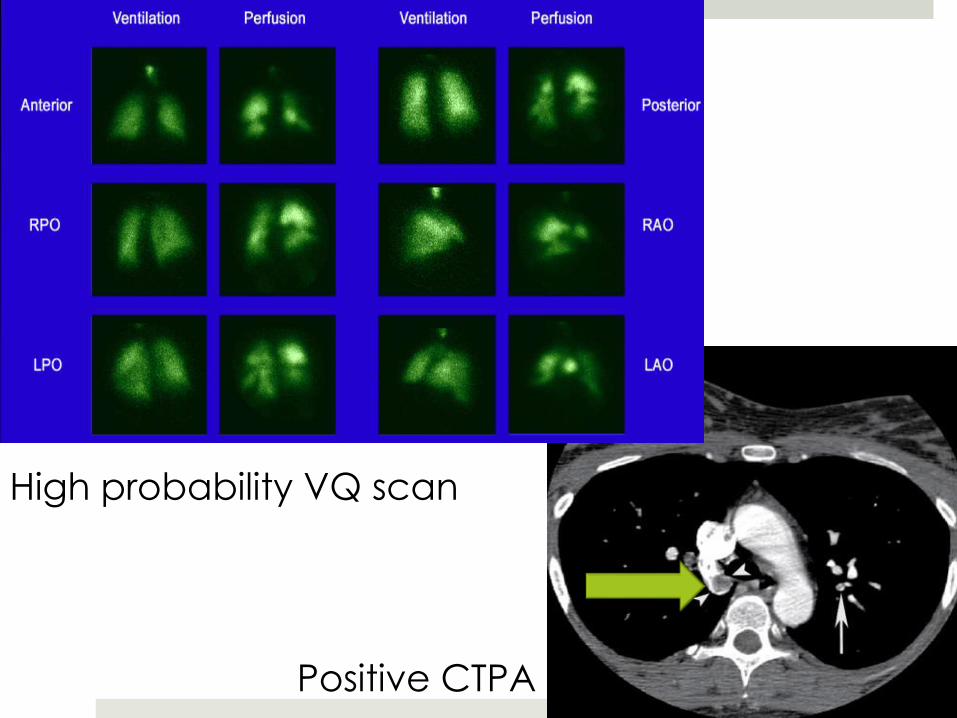
High probability VQ scan
Positive CTPA
PE Treatment in Pregnancy
Heparin wt based LD/gtt
LMWH 1mg/kg q12hrs SQ
POD 4 Booth 32
19yo G1P0 black female at 36 wks, no PMH presents to the
ED s/p 3 minute GTC seizure with headache, MEG abd pain
and blurry vision.
VS: HR 100, RR 16, BP 160/115, Temp 37.3, SpO2 100%
POC Glucose 85
Elevated Blood Pressure in Pregnancy
1. Eclampsia:
Pre-eclampsia plus seizures and/or coma
2. Pre-eclampsia:
New onset HTN >140/90 mmHg and proteinuria or
end organ dysfunction >20 wks
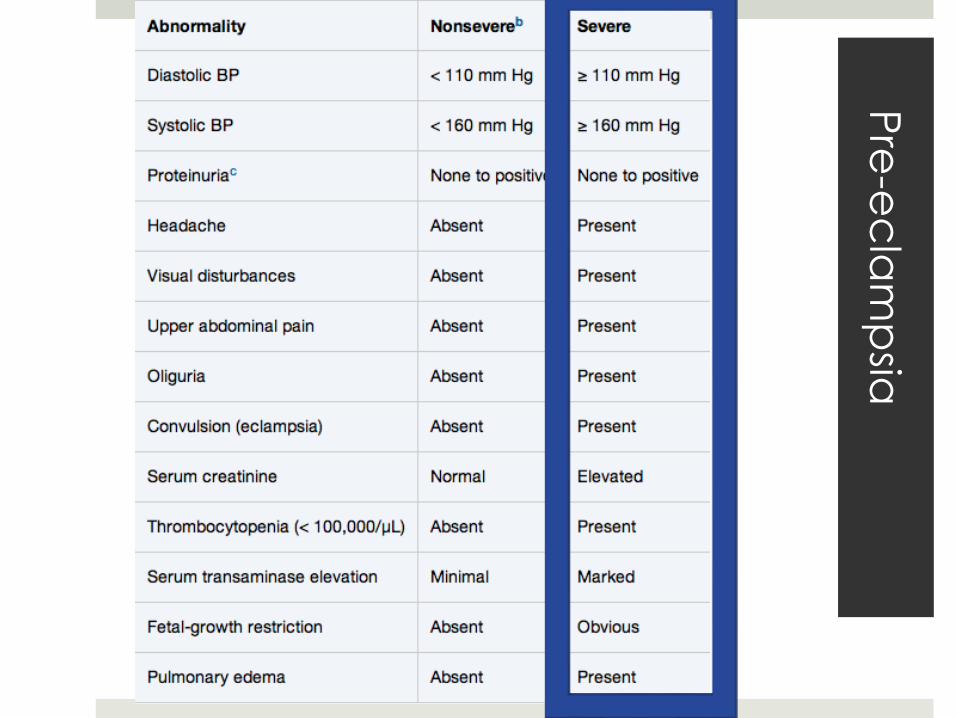
Pre
-ec
lam
psia
Management
ABCs, IV, O2, monitor
Labs: CBC, CMP, coags, LDH, T&S
Imaging: MR/CT abd and pelvis, US, CT head
OB consult:
1. Nonsevere Pre-eclampsia
Serial BPs, US, bed rest
Management
2. Severe Pre-eclampsia
SBP 140-155 mmHg and DBP 90-105 mmHg
Tx: Labetalol, Hydralazine, Nifedipine, Nicardipine gtt
DOC ppx or Eclampsia Magnesium sulfate
Toxicity: Calcium gluconate
Continued seizures = benzos
DELIVERY per OB >34 wks
POD 2
28yo F G2P1 at 37 wks, no PMH presents with painless bright
red vaginal bleeding.
VS: HR 90, RR 14, BP 110/70, Temp 37.1, SpO2 99%
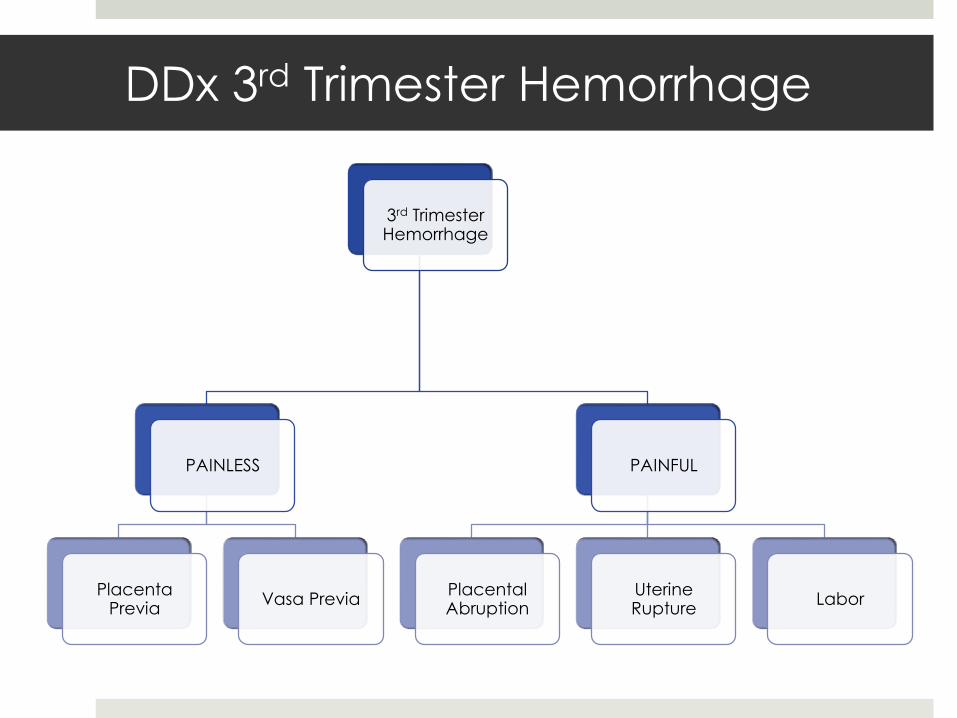
DDx 3rd Trimester Hemorrhage
3rd Trimester Hemorrhage
PAINLESS
Placenta Previa
Vasa Previa
PAINFUL
Placental Abruption
Uterine Rupture
Labor
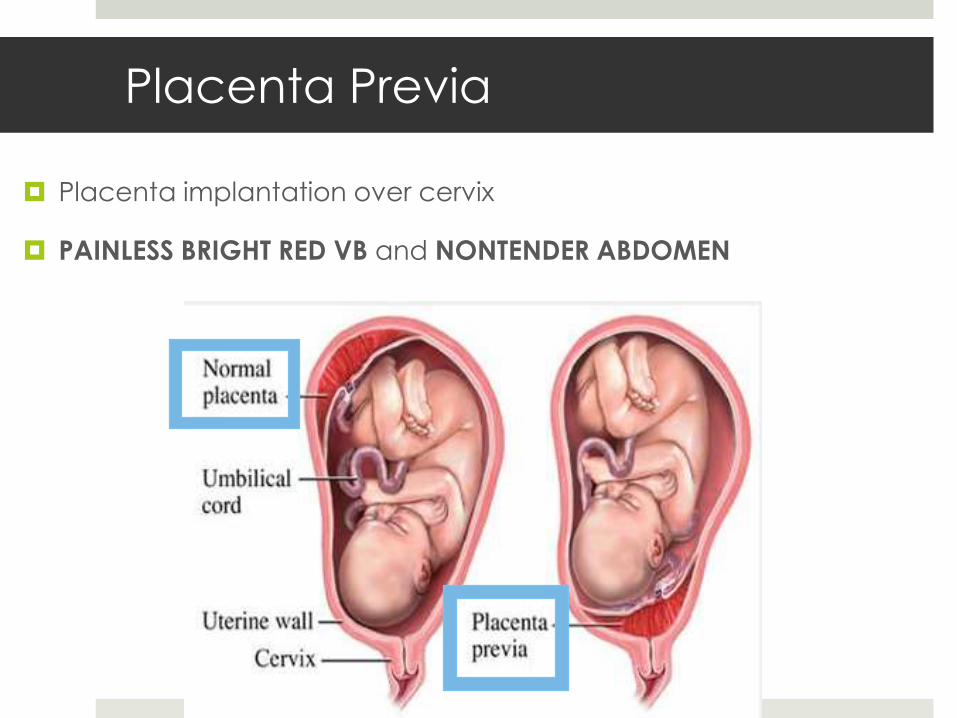
Placenta Previa
Placenta implantation over cervix
PAINLESS BRIGHT RED VB and NONTENDER ABDOMEN
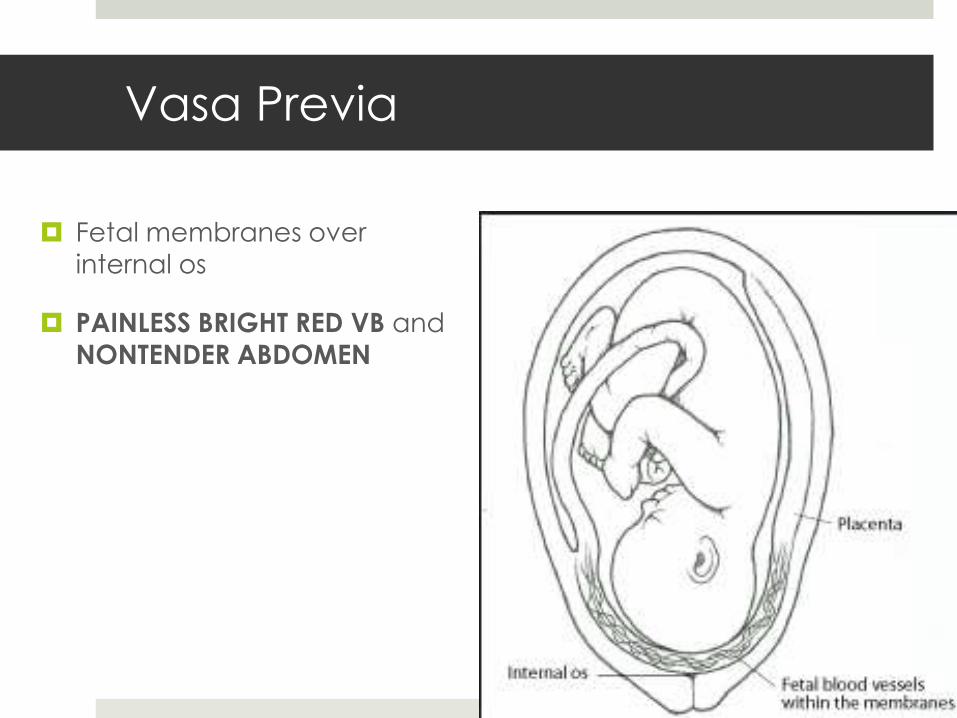
Vasa Previa
Fetal membranes over
internal os
PAINLESS BRIGHT RED VB and
NONTENDER ABDOMEN
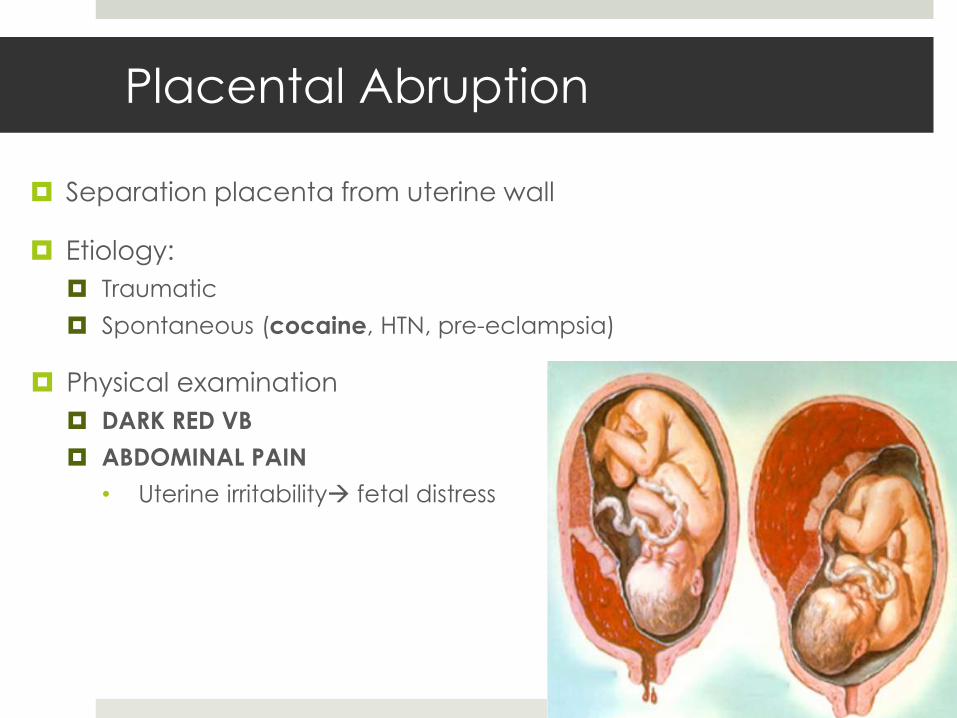
Placental Abruption
Separation placenta from uterine wall
Etiology:
Traumatic
Spontaneous (cocaine, HTN, pre-eclampsia)
Physical examination
DARK RED VB
ABDOMINAL PAIN
• Uterine irritability fetal distress
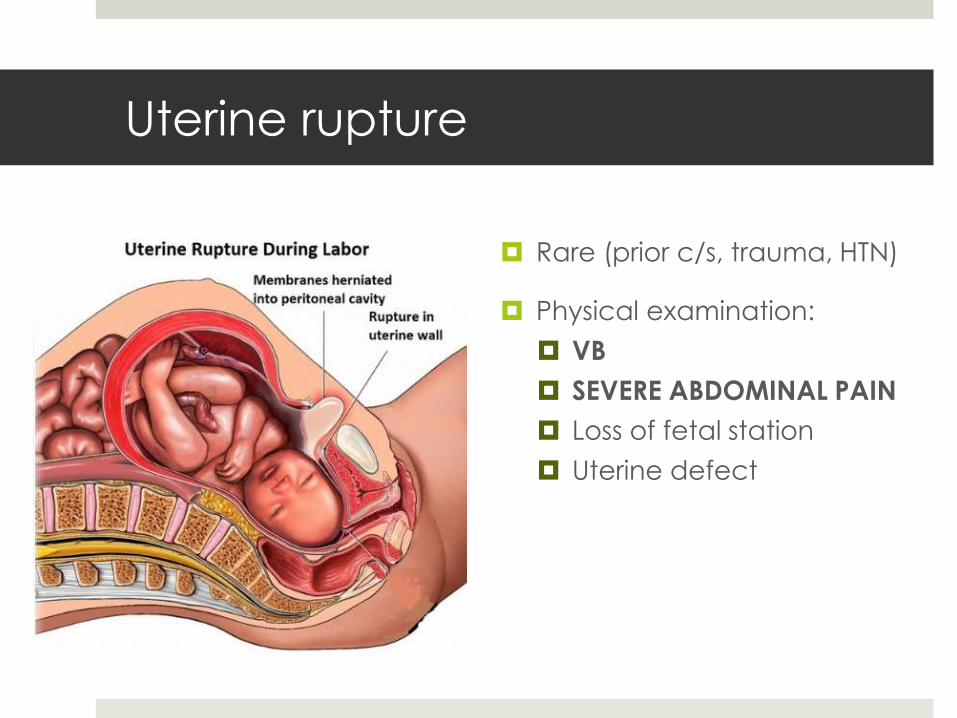
Uterine rupture
Rare (prior c/s, trauma, HTN)
Physical examination:
VB
SEVERE ABDOMINAL PAIN
Loss of fetal station
Uterine defect
Management
ABCs, IVx2, O2, Monitor
NO BIMANUAL EXAMINATION
Labs: CBC, CMP, coags, T&S, fibrinogen, FDP
Imaging: US r/o previa does NOT r/o abruption, FAST
IVF, PRBCs/MTP, Rhogam
OB consult:
C/S delivery (>37 wks or unstable mother)
Expectant management
POD 1: WBPW from triage
38yo F, holding her abdomen in a wheelchair
screaming "no puedo.”

ED Delivery
ABCs, IV, O2, monitor
HPI: G&P's, prenatal care, complications
Precipitous delivery kit and Peds cart
OB and NICU consults




38yo F G8P8, SVD, placenta delivered, baby APGARs 9 and 10,
vaginal bleeding continues...

Postpartum Hemorrhage (PPH)
SVD >500 mL
IVx2, O2, monitor
Labs: CBC, CMP, coags, T&S, FDP, fibrinogen
IVF 1-2L LR, PRBCs/MTP
PPH
4 T's:
1. Tone
2. Tissue
3. Trauma
4. Thrombin
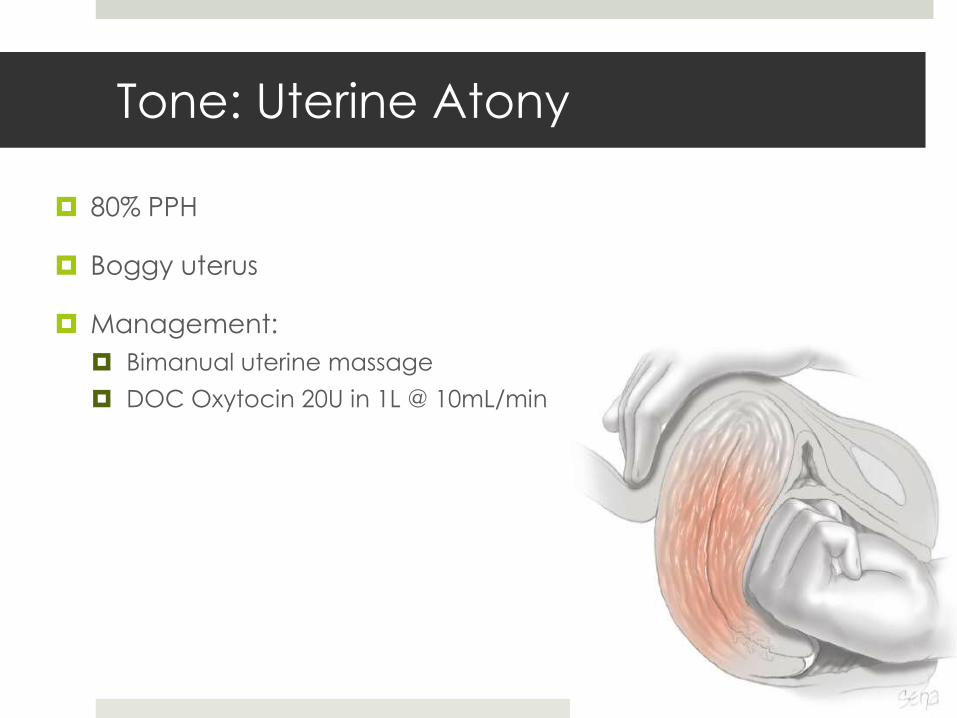
Tone: Uterine Atony
80% PPH
Boggy uterus
Management:
Bimanual uterine massage
DOC Oxytocin 20U in 1L @ 10mL/min
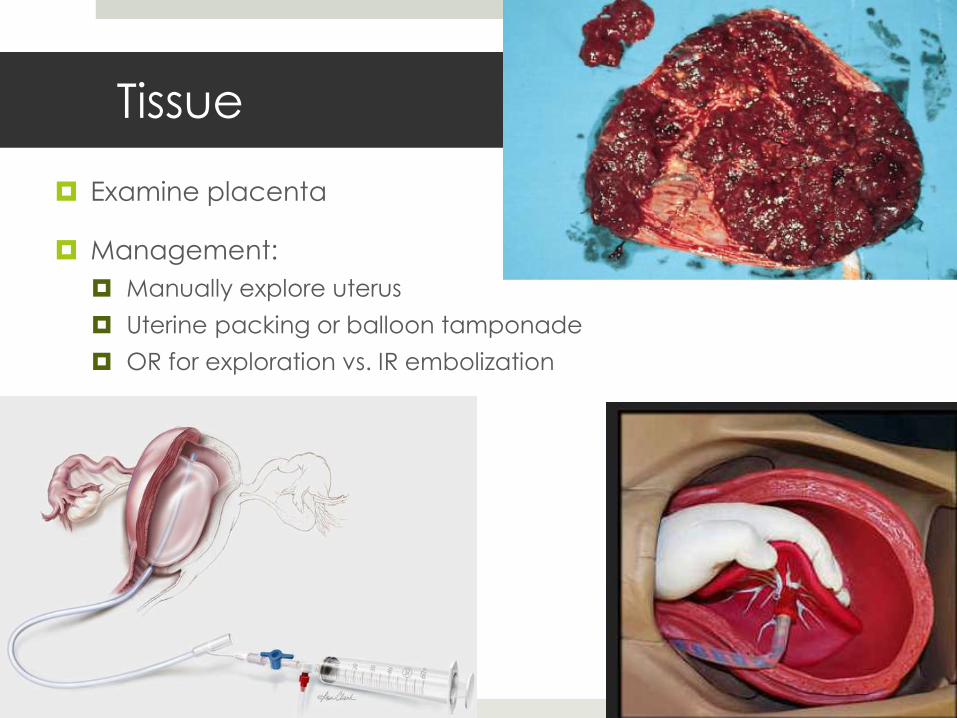
Tissue
Examine placenta
Management:
Manually explore uterus
Uterine packing or balloon tamponade
OR for exploration vs. IR embolization
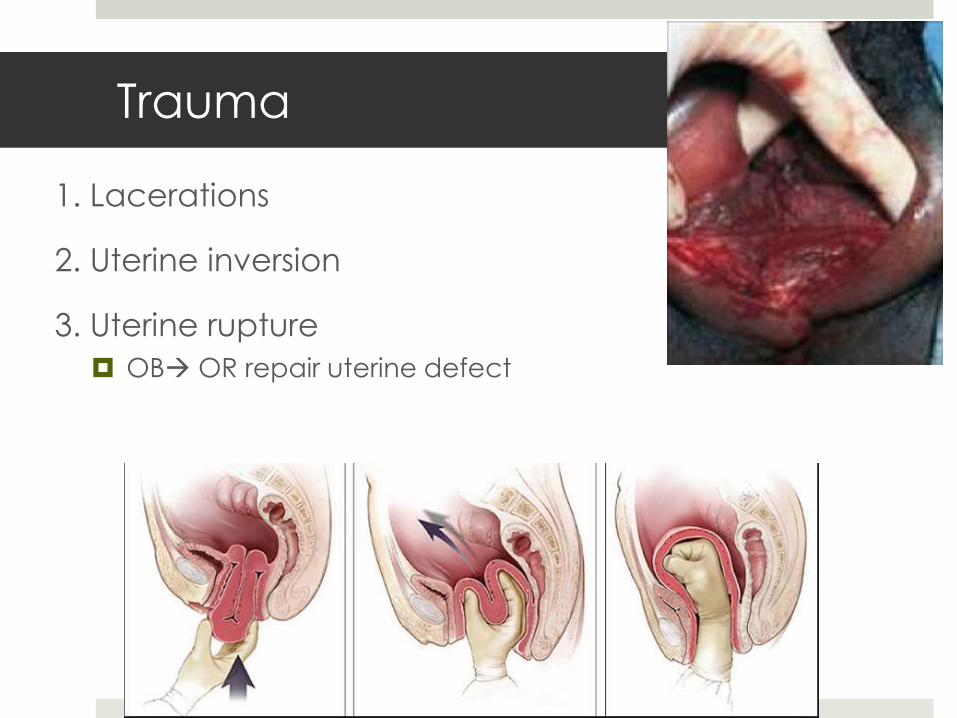
Trauma
1. Lacerations
2. Uterine inversion
3. Uterine rupture
OB OR repair uterine defect
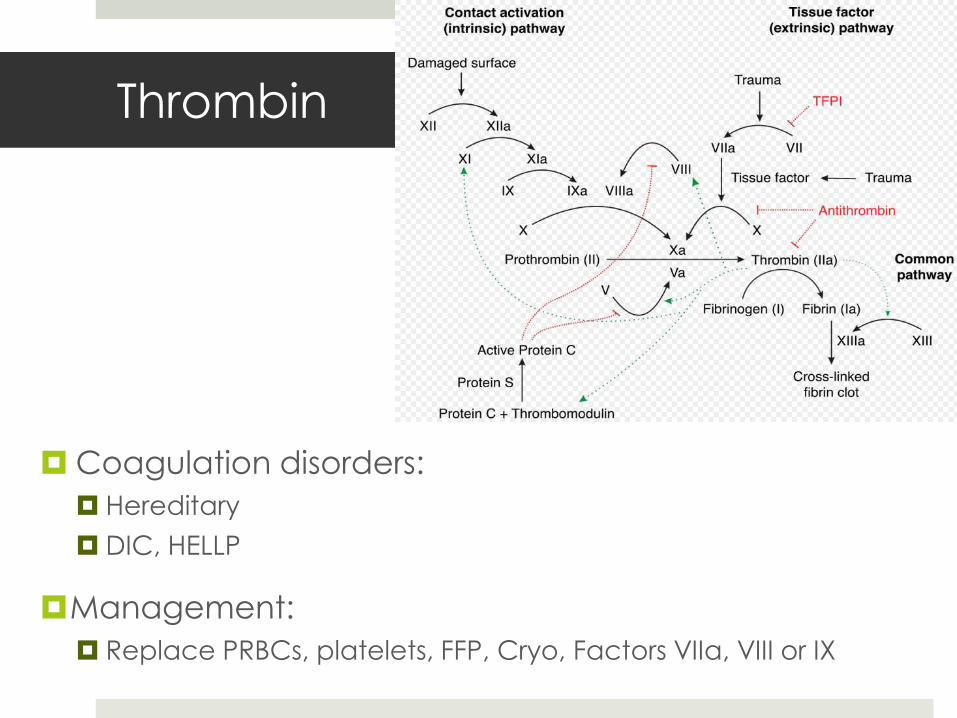
Thrombin
Coagulation disorders:
Hereditary
DIC, HELLP
Management:
Replace PRBCs, platelets, FFP, Cryo, Factors VIIa, VIII or IX
Postpartum Hemorrhage
Hemorrhagic Shock:
Signs of shock develop after 30% blood volume lost
CO maintained until Hgb <7 or HCT <20%
Management:
Give PRBCs if HCT < 25-30% with ongoing bleeding
Platelets <50,000 replace
Fibrinogen <100 mg/dL FFP, Cryo
PT/INR, PTT Cryo, recombinant factor VIIa, PCC
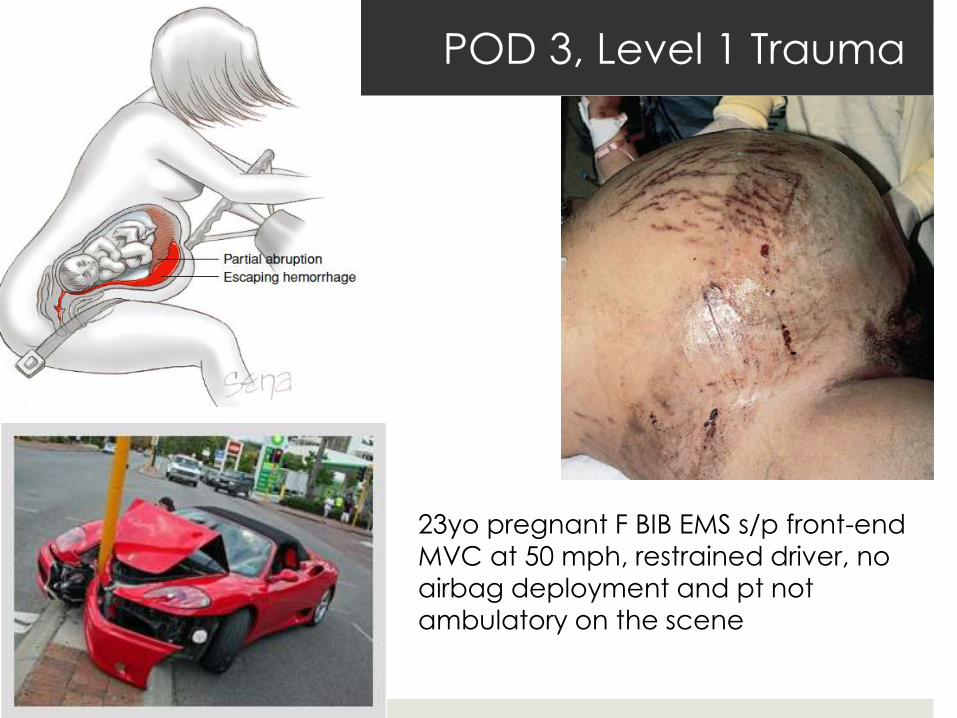
POD 3, Level 1 Trauma
23yo pregnant F BIB EMS s/p front-end
MVC at 50 mph, restrained driver, no
airbag deployment and pt not ambulatory on the scene
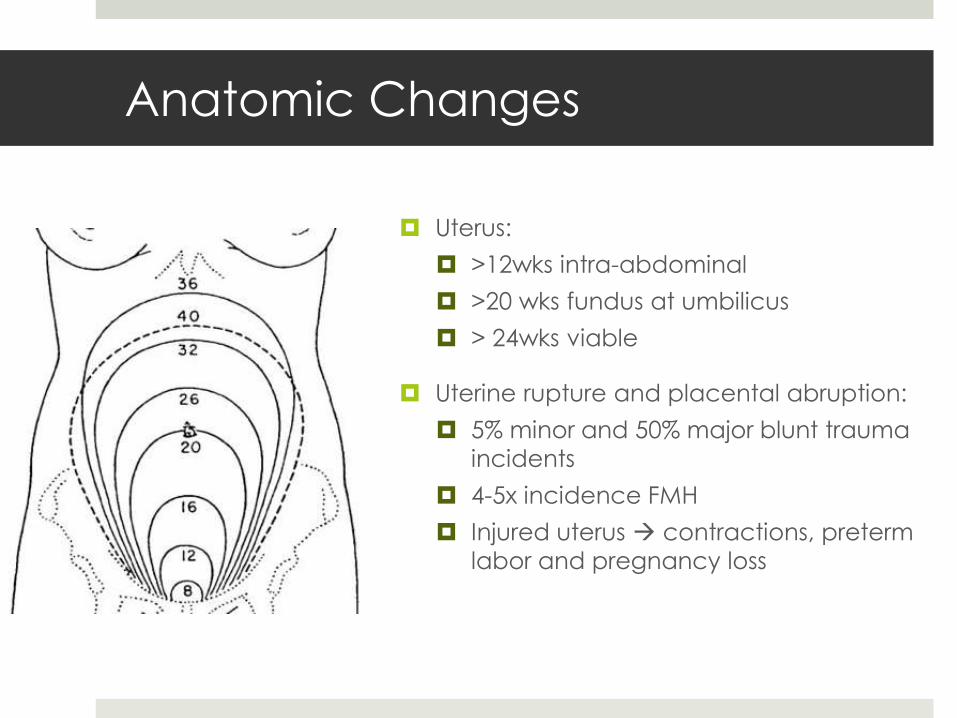
Anatomic Changes
Uterus:
>12wks intra-abdominal
>20 wks fundus at umbilicus
> 24wks viable
Uterine rupture and placental abruption:
5% minor and 50% major blunt trauma
incidents
4-5x incidence FMH
Injured uterus contractions, preterm
labor and pregnancy loss
Management of Abdominal Trauma
in Pregnancy
IVx2, O2, monitor, trauma labs, 1L LR, Tetanus and Rhogam prn
L tilt 15-30o
1o Survey:
Airway
Breathing
Circulation
Disability: GCS
Exposure
FAST
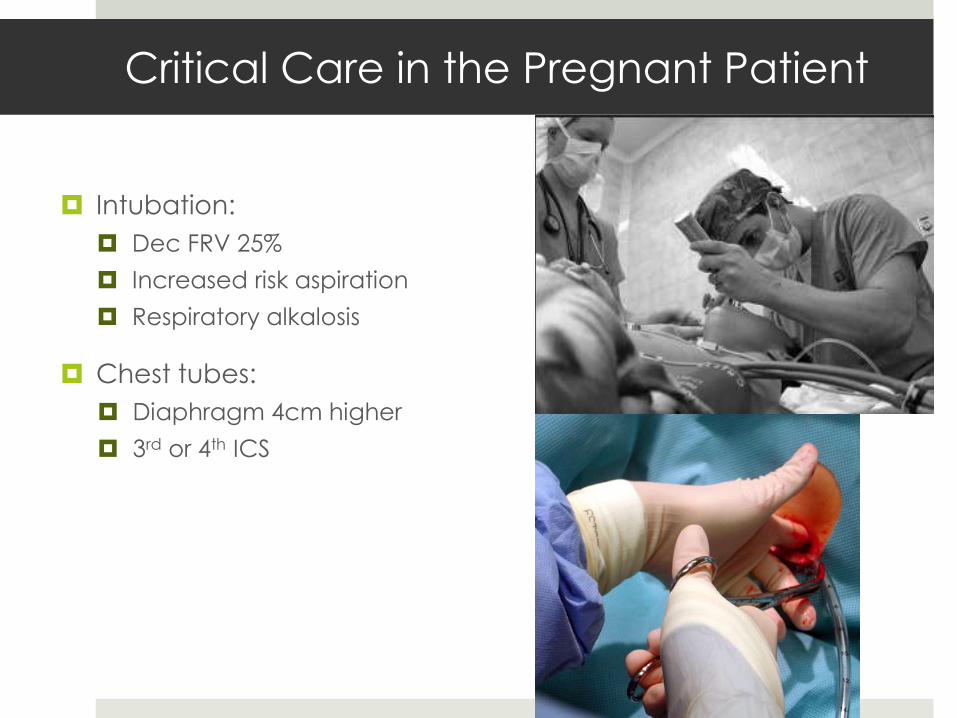
Critical Care in the Pregnant Patient
Intubation:
Dec FRV 25%
Increased risk aspiration
Respiratory alkalosis
Chest tubes:
Diaphragm 4cm higher
3rd or 4th ICS
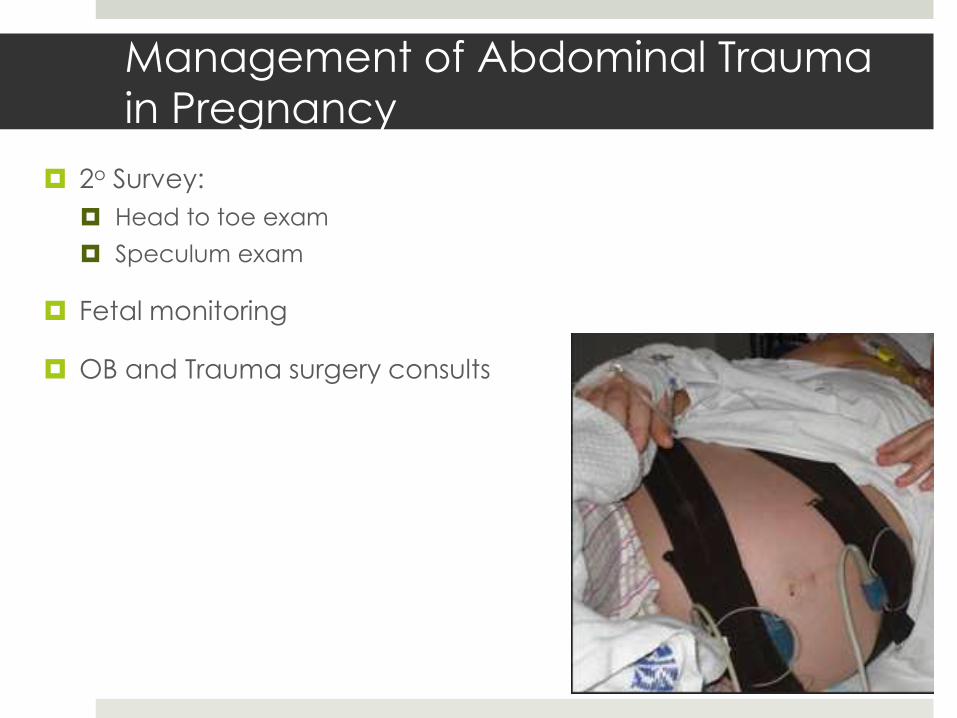
Management of Abdominal Trauma
in Pregnancy
2o Survey:
Head to toe exam
Speculum exam
Fetal monitoring
OB and Trauma surgery consults
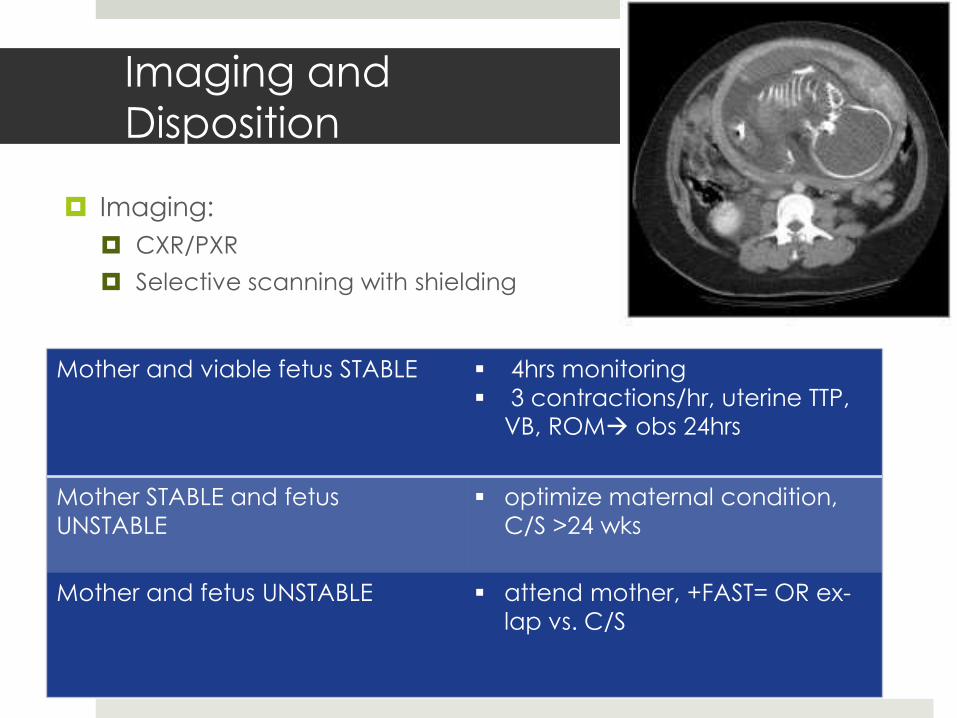
Imaging and
Disposition
Imaging:
CXR/PXR
Selective scanning with shielding
Mother and viable fetus STABLE 4hrs monitoring
3 contractions/hr, uterine TTP, VB, ROM obs 24hrs
Mother STABLE and fetus
UNSTABLE
optimize maternal condition,
C/S >24 wks
Mother and fetus UNSTABLE attend mother, +FAST= OR ex-
lap vs. C/S
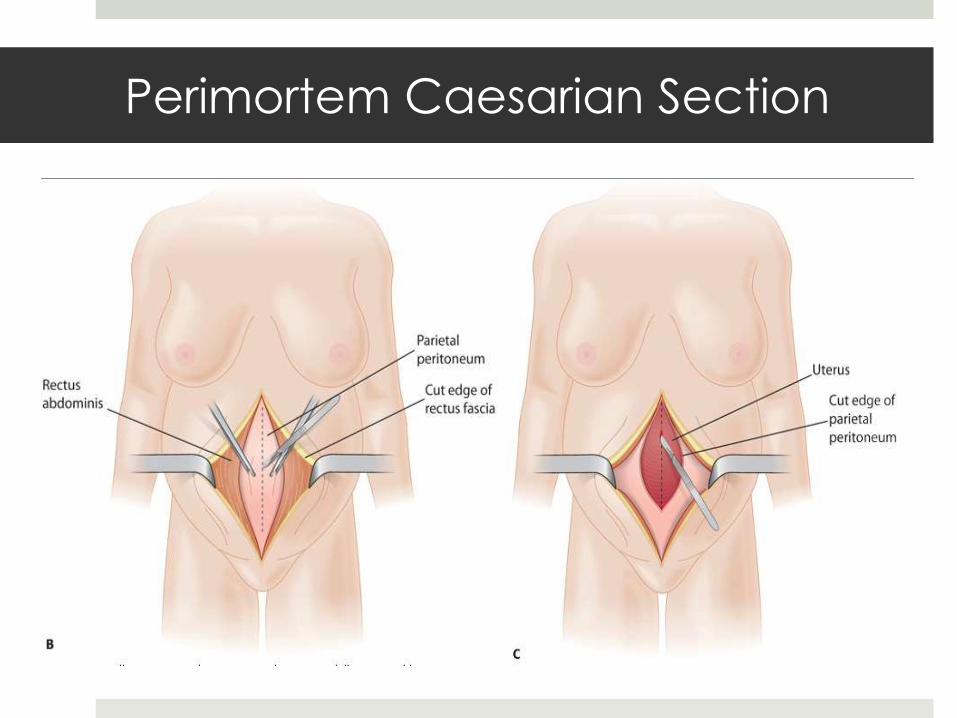
Perimortem Caesarian Section
Perimortem C/S maternal cardiac arrest and viable fetus
Continue ATLS/ACLS
<5 min = best prognosis, 98% neuro intact
0% survival >25 min
Equipment: scalpel, Mayo scissors, retractors, towels, chromic
#0 or 1 and needle holder

Pe
rimo
rtem
Ca
esa
rian
Se
ctio
n

Questions?
References: pictures
community. babycenter.com
community.freescale.com
http://http://en.wikipedia.org/wiki/Coagulation#mediaviewer/File:Coagulation_full.svg
www.brooksidepress.org/Products/Obstetric_and_Newborn_Care_1/lesson_5_Section_1.htm
http://radiology.med.miami.edu/documents/2009Lungs.pdf
http://accessmedicine.mhmedical.com.foyer.swmed.edu/ViewLarge.aspx?figid=39621558
http://accessmedicine.mhmedical.com.foyer.swmed.edu/content.aspx?bookid=351§ionid=39619709
http://thedefinitionofnerd.blogspot.com/2013/08/life-matters-true-blood-pros-and-cons.html
www.theamericanmama.com
www.webmd.boots.com
http://accessmedicine.mhmedical.com.foyer.swmed.edu/book.aspx?bookid=351
www.merkmanuals.com
http://mdcurrent.in/primary-care/practical-advice-on-preventing-maternal-death-due-to-postpartum-hemorrhage/
www.medpagetoday.com
http://www.trauma.org/archive/thoracic/CHESTdrain.html
www.wisegeek.com
References: sources
American College of Surgeons Committee on Trauma. ATLS, Student Course Manual. 8th Ed.2008. Pgs 260-265.
Anderson J.M., and Etches D. (2007). Prevention and management of postpartum hemorrhage. American Family Physician. 75(6), 875-882.
Brown, Carlos MD. Trauma in Pregnancy. EM:RAP. January 2013.
Cunningham, F., Leveno, K., Bloom, S., Spong, C., Dashe, J. Williams Obstetrics, 24th Ed. McGraw-Hill Education, 2014. Chapter 47.
Knoop, Kevin, Stack, S., Storrow, A. The Atlas of Emergency Medicine, 3rd Ed. McGraw-Hill Companies, Inc, 2010. Chapter 10.
Marx, John MD, Hockberger, R. MD, Walls, R. MD. Rosens Emergency Medicine-Concepts and Clinical Practice 8th
Ed. Elsevier, 2013. Chapters 34, 37, 178, 179.
Orman, Rob, Jasumback, M. VQ in Pregnancy? A Rant and Response. EM:RAP. March 2011.
Orman, Rob. Klien, J. Chest Pain in Pregnancy. EM:RAP. December 2011.
Rivers, Carol M.D. Preparing For the Written Board Exam. Urogenital Emergencies. 6th Ed., Vol. 1. Ohio ACEP. 2011. Pgs 556-575.
Tintinalli, Judith E., J. Stephan Stapczynski, O. John Ma, David M. Cline, Rita K. Cydulka, Garth D. Meckler, The American College of Emergency Physicians. Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7th Ed. The McGrw-Hill Companies, Inc. 2011. Chapters 103-104.