Pregnancy & Heart Disease - Iowa ACC
66
HEART DISEASE IN PREGNANCY Mahi L Ashwath MD, MBA, FACC, FASE, FSCMR President, Iowa ACC Associate Professor University of Iowa Hospitals and Clinics
Transcript of Pregnancy & Heart Disease - Iowa ACC

HEART DISEASE IN PREGNANCY
Mahi L Ashwath MD, MBA, FACC, FASE, FSCMR
President, Iowa ACC
Associate Professor
University of Iowa Hospitals and Clinics

DISCLOSURES:
None

OUTLINE…
Review the cardiovascular changes of normal pregnancy
High risk cardiac conditions
Hypertension
Cardiomyopathy (Peripartum)
SVT and arrhythmias
Coronary artery disease
Valvular disease Stenosis
Regurgitation
Prosthetic Valves
Anticoagulation in Pregnancy
Aortic disorders and pregnancy
CARDIOVASCULAR CHANGES OF
NORMAL PREGNANCY

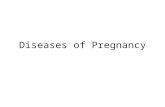
PREGNANCY PHYSIOLOGIC CHANGES

PREGNANCY PHYSIOLOGIC CHANGES
Elkayam et al. JACC 68,2016:396-410

CV EXAM DURING PREGNANCY
95% of pregnant patients have a systolic murmur
Loud S3 is normal
Increased volume status:
Brisk and full carotid upstroke
Displaced and enlarged apex
Varicose veins and edema

HIGH RISK CARDIAC CONDITIONS

PREPREGNANCY RISK ASSESSMENT
CARPREG
ZAHARA
WHO classification

CARPREG STUDY

ZAHARA

WHO CLASSIFICATION
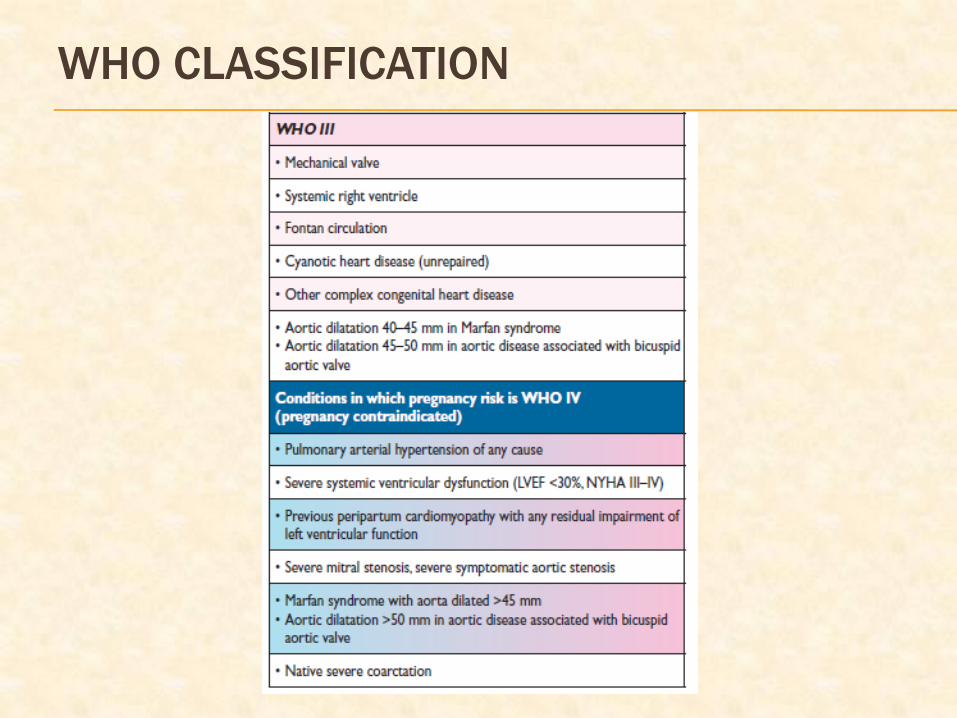
WHO CLASSIFICATION

IN BRIEF…

HIGH RISK CARDIAC CONDITIONS

Severe pulmonary arterial hypertension of any cause– 30-50% maternal mortality
Maternal left heart obstruction – Severe AS, Severe MS
Ventricular dysfunction – Our best medical therapy is not safe during pregnancy Class III or Class IV CHF, EF <30-40%
Prior peripartum cardiomyopathy with residual cardiomyopathy
Dilated or unstable aorta Marfan with aorta > 40-45 mm (advise against if >45 mm)
Severe cyanosis
Be careful with Mechanical valves
Moderate to severe regurgitation

HYPERTENSION IN PREGNANCY

HYPERTENSION IN PREGNANCY
Type Criteria
Pre – existing
Hypertension
> 140/90 mmHg, either
precedes pregnancy or <20 of
gestation
Gestational
Hypertension
>140/90 mmHg >20 weeks of
gestation
Pre Eclampsia Gestational hypertension +
proteinuria
Eclampsia Pre Eclampsia + Seizures

HYPERTENSION IN PREGNANCY
SBP> 170 mmHg or DBP > 110 mmHg – emergency
hospitalize
Preexisting HTN – continue same treatment, unless
the drugs are contraindicated in pregnancy
Severe - IV labetalol, Oral Methyldopa or nifedipine
IV Hydralazine is not recommended – unless other
treatments have failed
If pulmonary edema – IV Nitroglycerin
ESC Guidelines 2018. Eur Heart J 2018; 39:3165-3241

PREECLAMPSIA AND RISK OF CV DISEASE
Future risk of CV morbidity/mortality related to
severity/number of preeclampsia episodes
Early onset/severe preeclampsia
Highest risk of preterm delivery
8-9 fold risk of cardiovascular death
Mild late preeclampsia
no associated future cardiovascular disease

CARDIOMYOPATHY AND THE HEART

PERIPARTUM CARDIOMYOPATHY
NEJM 312;1432, 1985

PERIPARTUM CARDIOMYOPATHY
New diagnosis of Heart Failure due to LV dysfunction –
last trimester to first 6 months post partum
Increase in frequency
Age > 30 year
Multifetal pregnancy
Multiparity
Tocolytic
Black
HTN, DM, smoking

MANAGEMENT
Standard Heart Failure Treatment No ACEI or ARB or Aldosterone antagonists or ARNI or Atenolol
Can use Digoxin, Hydralazine, Beta blockers
Diuretics if needed
Bromocriptine – blocks prolactin release Increase in EF with improved outcome versus standard Rx
2.5 mg bid for 2 weeks, 2.5 mg daily for 6 weeks with HF therapy
Not much used in US
Anticoagulation for EF <35%, or bromocriptine
Continue Rx for 1 year and reassess
Life long follow up

PROGNOSIS
Multicenter Investigations of Pregnancy Associated Cardiomyopathy (IPAC) study 13% had major events or persistent severe decrease in
LVEF
Poor prognosis LVEF <30%
EDD >60mm
Subsequent Pregnancy: CHF in 21% normal EF and 44% reduced EF
Death – 10% normal EF and 19% reduced EF pts
Advise against pregnancy
EF <25% at presentation
Persistent decrease in EF
McNamara D et al: JACC 2015

PROGNOSIS
McNamara D et al: JACC 2015

ESC Guidelines 2018. Eur Heart J 2018; 39:3165-3241

ARRHYTHMIAS - SVT

SVT MANAGEMENT
Acute
Awake, alert patient - IV Adenosine
Hemodynamically unstable – DC Cardioversion
Recurrent SVT
Beta-blocker
Calcium channel blocker
Sotalol
Flecainide
Amiodarone-contraindicated by manufacturer
Monitor neonatal EKG and thyroid
Excreted in breast milk
Ablation

CORONARY ARTERY DISEASE

CORONARY ARTERY DISEASE
Mortality 7%
Treatment-
Initial-heparin, aspirin, beta-blocker, nitrate
Nitrates excreted in breast milk-possible fetal methemoglobinemia
Statins not recommended
Clopidogrel, GP IIb IIIa inhibitors, DOACs - Safety not established
PCI with bare metal stent
Thrombolytics if cath/PCI not available
Exclude spontaneous coronary artery dissection and aortic dissection

SPONTANEOUS CORONARY ARTERY DISSECTION
Most common cause of pregnancy associated MI
(43%)
Most frequent during late pregnancy / early
postpartum
Pregnant SCAD patients
More acute presentations and high-risk features
Mostly left sided vessels or multivessel disease

VALVULAR HEART DISEASE

MITRAL STENOSIS AND PREGNANCY
Poorly tolerated Tachycardia,
Increased plasma volume
Maternal Risks- Heart failure - Pulmonary edema in II & III trimester,
Atrial fibrillation
Fetal risks- Prematurity 20-30%;
IUGR 5-20%
Moderate & severe MS counseled against pregnancy
without prior intervention

• Pharmacological Management – Restrict activity
– Beta blockers
– Diuretics as needed
• NYHA III/ IV or PASP >50 mmHg – Balloon Mitral Valvotomy
• Anticoagulation – Atrial fibrillation, LA thrombus, LA smoke, Dilated LA
• Delivery – Vaginal – Mild MS, Class I/II, no PAH
– CS – Mod to Sev MS, Anticoagulation, Class III/ IV, PAH
MITRAL STENOSIS AND PREGNANCY

AORTIC STENOSIS
• Unable to augment Cardiac Output – Preload and Hypotension Sensitive
• Maternal – Heart failure
• Fetal – Decreased placental perfusion
– IUGR
– Preterm Labor

• Pharmacological Management
– Restrict activity
– Beta blockers
– Diuretics as needed
• Severe symptomatic Aortic stenosis,
– Consider Balloon Aortic Valvotomy/ Emergency AVR.
• Delivery
– Vaginal – Mild MS, Class I/II, no PAH
– CS – Mod to Sev MS, Anticoagulation, Class III/ IV, PAH
AORTIC STENOSIS

REGURGITANT LESIONS
Better tolerated
Maternal risk- HF,
Arrhythmias,
Progressive worsening of regurgitations
Moderate to severe regurgitant lesions – exercise testing to decide pre pregnancy intervention
Severe lesions + symptoms/ impaired LV function/
Ventricular dilatation treated surgically, if possible repair

PROSTHETIC VALVES

TISSUE PROSTHESIS
Increased degeneration
in young
Reoperation risk
Possible accelerated
degeneration in
pregnancy

MECHANICAL PROSTHESIS
Prepregnancy
counseling,
centralization of care
critical
Anticoagulation
management during
pregnancy and delivery
ANTICOAGULATION IN PREGNANCY

ANTICOAGULATION IN PREGNANCY
Hematologic changes
Increased clotting factor concentration
Increased platelet adhesiveness
Decreased fibrinolysis and protein S activity
Increased risk of thrombosis and embolization

WARFARIN IN PREGNANCY
Low molecular weight-crosses placenta
Increased risk of fetal loss, prematurity,
stillbirth, fetal intracranial hemorrhage,
retroplacental hemorrhage
Embryopathy risk-exposure 6-12 weeks
Safe to use greater than 5 mg per day after
12 weeks

UNFRACTIONATED HEPARIN
Increased molecular weight-does not cross
placenta
Treatment of choice-late pregnancy, delivery
Long-term-osteoporosis-30%, steroidal
abscesses, decreased platelets, alopecia
Vitale N et al: JACC 1999

LMWH IN PREGNANCY
Does not cross the placenta
No teratogenic effects
Potential advantages
Increased bioavailability, administration ease
Decreased osteoporosis and thrombocytopenia

ANTICOAGULATION IN PREGNANCY

ANTICOAGULATION IN PREGNANCY
ACC/ AHA VHD Guidelines 2014

ANTICOAGULATION IN PREGNANCY
Halpern et al. JACC 2019
ANTICOAGULATION IN PREGNANCY
Low-dose aspirin
Safe-antithrombotic effect not proven
Used in shunts, cyanosis, bioprosthesis
Possible decreased incidence of preeclampsia
Thrombolytic therapy
Emergency use only
Thrombin inhibitor/DOAC
No safety data

IE PROPHYLAXIS IN PREGNANCY
Not required during uncomplicated delivery
Reasonable to administer in high-risk patients

AORTIC DISORDERS AND PREGNANCY
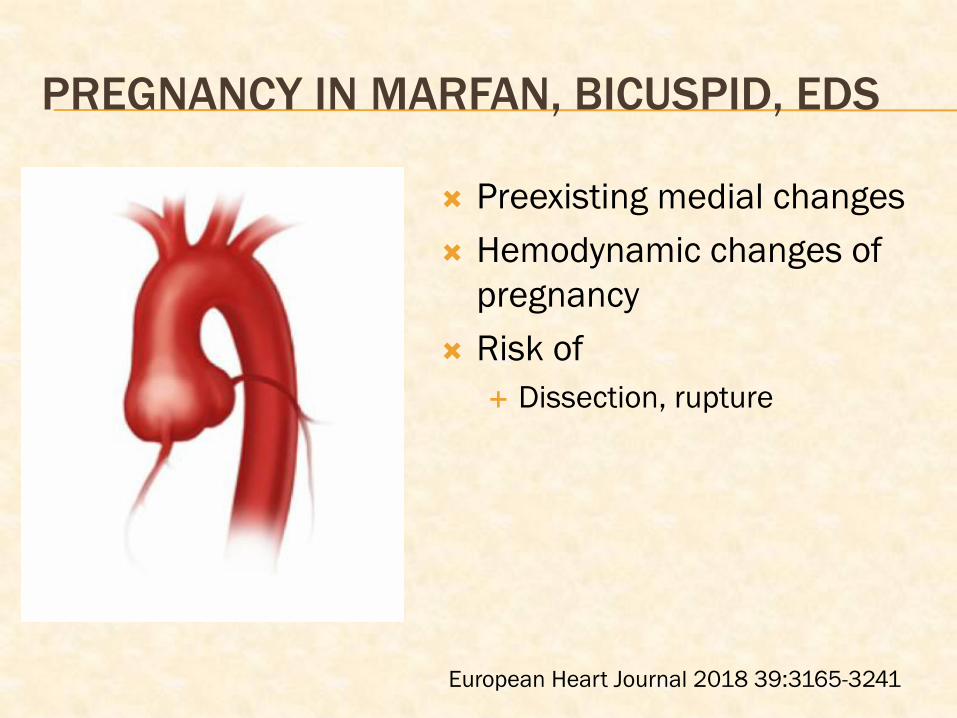
PREGNANCY IN MARFAN, BICUSPID, EDS
Preexisting medial changes
Hemodynamic changes of
pregnancy
Risk of
Dissection, rupture
European Heart Journal 2018 39:3165-3241

AORTIC DISORDERS AND PREGNANCY
Aorta imaging
Aorta > 45 mm – no pregnancy
Aorta < 40 mm – reasonable if low risk
Aorta 40-45 mm – individualize – family hx, rate of
aortic dilation
Genetics, prenatal diagnosis – Fetal
inheritance
European Heart Journal 2018 39:3165-3241

ESC GUIDELINES 2018
European Heart Journal 2018 39:3165-3241

RECOMMENDATIONS
During pregnancy
Beta blocker (even if aorta is normal size) regular aorta imaging (every 4-6 weeks)
Fetal echo
Peripartum
Facilitated vaginal delivery
C – section for Ao >40 mm or increase in size
IE prophylaxis
Postpartum
Dissection risk persists (highest risk upto 4-6 weeks after pregnancy)

ACUTE PERICARDITIS IN PREGNANCY
Not much data
High risk features – hospitalize
Anticoagulation, immunosuppressed, fever,
trauma, tamponade, large effusion,
myopericarditis
Management
<20 weeks – NSAIDs
>20 weeks – corticosteroid
Colchicine is contraindicated in Pregnancy

CARDIAC DRUGS IN PREGNANCY


MEDICAL THERAPIES AND PREGNANCY
Halpern et al. JACC 2019

RADIATION AND PREGNANCY

MRI DURING PREGNANCY
MRI is safe
Gadolinium crosses placenta – small molecule
– repeated swallowing by the fetus – unclear
risk

SUMMARY
Review the cardiovascular changes of normal pregnancy
High risk cardiac conditions
Hypertension
Cardiomyopathy (Peripartum)
SVT and arrhythmias
Coronary artery disease
Valvular disease
Stenosis
Regurgitation
Prosthetic Valves
Anticoagulation and Drugs in Pregnancy
Aortic disorders and pregnancy
Severe pulmonary arterial hypertension
Maternal left heart obstruction
Ventricular dysfunction
Dilated or unstable aorta
Severe cyanosis
CONTRAINDICATIONS TO PREGNANCY

Elkayam, U. et al. J Am Coll Cardiol. 2016;68(4):396–410.

Thank You!!!