
Preeclampsia, Severe, Uncontrolled
28
BUKIDNON STATE UNIVERSITY COLLEGE OF NURSING City of Malaybalay In Partial Fulfillment of the Course Requirements in NCM 108 A Case Presentation on PREECLAMPSIA, SEVERE, UNCONTROLLED Presented by: Group 2 Cagulada, Lharra Mae Santillan, Cheerille Telin, Marvin Rachelle Villamor Loweelyn Tortola Junfelm Gomez Nielmark Casite Joy Homamoy Ma. Zusette Doydora Fe Auguis Joshua Robosa Marcher Palado
-
Upload
lharra-cagulada -
Category
Documents
-
view
23 -
download
2
description
Preeclampsia, Severe, Uncontrolled
Transcript of Preeclampsia, Severe, Uncontrolled

BUKIDNON STATE UNIVERSITYCOLLEGE OF NURSING
City of Malaybalay
In Partial Fulfillment of the Course Requirements inNCM 108
A Case Presentation onPREECLAMPSIA, SEVERE, UNCONTROLLED
Presented by:Group 2
Cagulada, Lharra MaeSantillan, Cheerille
Telin, MarvinRachelle VillamorLoweelyn TortolaJunfelm GomezNielmark CasiteJoy Homamoy
Ma. Zusette DoydoraFe Auguis
Joshua RobosaMarcher Palado
Clinical Instructor:
April Ahne C. Guibone, RN, MAN
December 12, 2014
TABLE OF CONTENTS
I. Introduction
a. Objectives of the CP
b. Patient’s Profile
c. Etiology of the Disease/ Anatomy and Physiology
II. Theoretical Framework
III. Nursing Care Plans
Assessment
Subjective
Objective
Signs and Symptoms
Laboratory Tests
Nursing Diagnosis
Planning
Implementation/ Nursing Interventions
Independent
Dependent
Evaluation
IV. Discharge Plans
Follow-up Visit
Home Medication
V. Bibliography
VI. Appendix

I- INTRODUCTION
Pregnancy- Induced Hypertension (PIH) is a condition in which vasospasm occurs
during pregnancies in both small and large arteries. Signs of hypertension, proteinuria, and
edema develop. It is a unique to pregnancy and occurs in 5% to 10% of pregnancies in the
United States. (Abramovici et al., 2000) Despite of years of research, the cause of the disorder is
still unknown. Originally it was called toxaemia because the researchers pictured a toxin of some
kind being produced by a woman in response to the foreign protein of the growing fetus, the
toxin leading to the typical symptoms. No such toxin has ever been identified.
PIH, a condition separate from chronic hypertension, tends to occur most frequently in
primiparas younger than 20 years of age and older than 40 years old, women from low
socioeconomic backgrounds (perhaps of poor nutrition), those who have had five or more
pregnancies, women of color, those who have hydramnios, or those who have an underlying
disease such as heart disease, diabetes with vessel or renal involvement, and essential
hypertension. (Addele Pilliteri, Maternal and Child Health Nursing 2003)
Ten percent of all pregnancies are complicated by hypertension. Eclampsia and
preeclampsia account for about half of these cases worldwide and have been recognized and
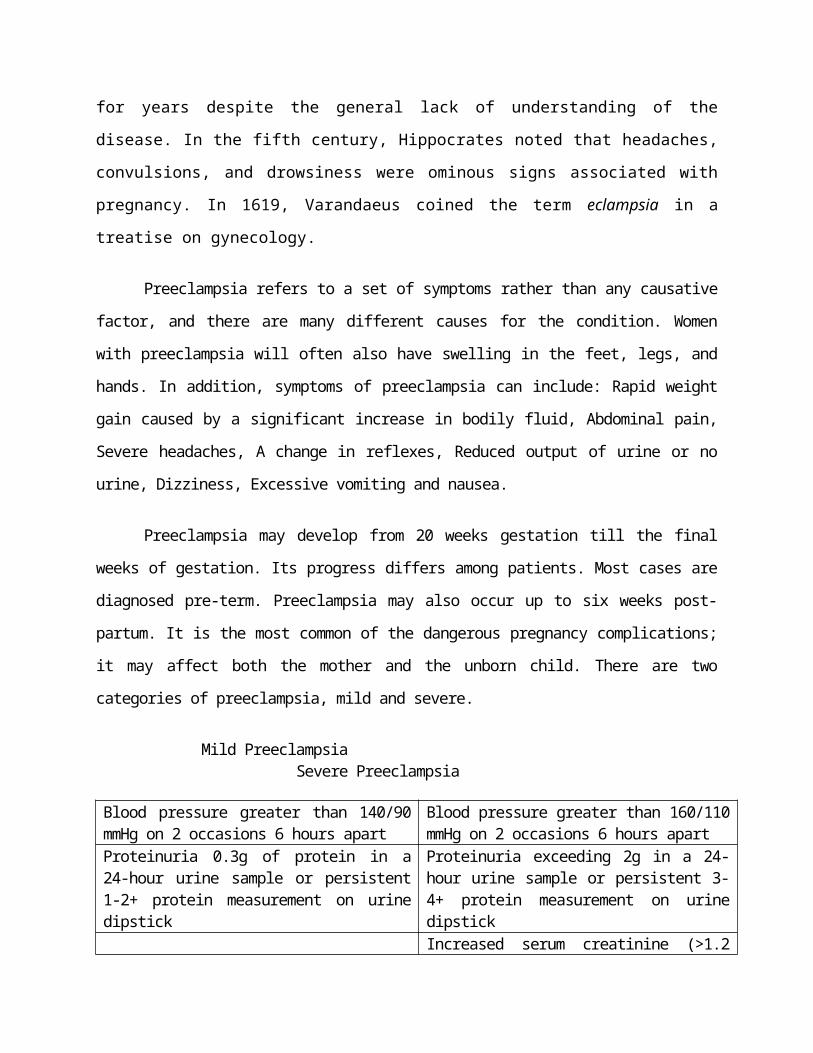
described for years despite the general lack of understanding of the disease. In the fifth century,
Hippocrates noted that headaches, convulsions, and drowsiness were ominous signs associated
with pregnancy. In 1619, Varandaeus coined the term eclampsia in a treatise on gynecology.
Preeclampsia refers to a set of symptoms rather than any causative factor, and there are many different
causes for the condition. Women with preeclampsia will often also have swelling in the feet, legs, and hands. In
addition, symptoms of preeclampsia can include: Rapid weight gain caused by a significant increase in bodily
fluid, Abdominal pain, Severe headaches, A change in reflexes, Reduced output of urine or no urine, Dizziness,
Excessive vomiting and nausea.
Preeclampsia may develop from 20 weeks gestation till the final weeks of gestation. Its progress differs
among patients. Most cases are diagnosed pre-term. Preeclampsia may also occur up to six weeks post-partum. It
is the most common of the dangerous pregnancy complications; it may affect both the mother and the unborn
child. There are two categories of preeclampsia, mild and severe.

Mild Preeclampsia Severe Preeclampsia
Blood pressure greater than 140/90 mmHg on 2 occasions 6 hours apart
Blood pressure greater than 160/110 mmHg on 2 occasions 6 hours apart
Proteinuria 0.3g of protein in a 24-hour urine sample or persistent 1-2+ protein measurement on urine dipstick
Proteinuria exceeding 2g in a 24-hour urine sample or persistent 3-4+ protein measurement on urine dipstickIncreased serum creatinine (>1.2 mg/dL unless known to be elevated previously)Oliguria < 500 mL/24hCerebral or visual disturbancesEpigastric painThrombocytopenia (platelet count < 100,000/mm)
A. Objectives
General Objectives
Our group aims to present a case study that will show a comprehensive discussion of Severe Preeclampsia, for us to share knowledge to our audience and to gain further details about the disease.
Specific Objectives
At the end of 2 hours, we will be able to:
1. Define Severe Preeclampsia.
2. Describe the causes, sign, and symptoms of the disease.
3. Present a thorough general health assessment of the client which includes physical assessment and family history.
4. Discuss an overview anatomy and physiology of the system involved.
5. Thoroughly discuss, explain, and elaborate the pathophysiology of the disease process of the patient’s conditions.
6. Determine the laboratory and diagnostic procedure done and its significance
7. Described the different medications administered for the disease, their indications, contraindications, side effects, and specific nursing responsibilities.
8. Identify and discuss nursing care plans for the different problems identified.
9. Discuss the discharge planning intended for the patient

B. Patient’s Profile
Demographic Data
A. Name : Mrs. Pre-Eclampsia
b. Age : 39 years old
c. Sex : Female
d. Date of Birth : July 07, 1975
e. Address : Kibalaan Ginuyuran Valencia city
f. Religion : Roman Catholic
g. Nationality : Filipino
h. Civil status : Married
i. Occupation : House Keeper
j. Informant : Mrs. Eclampsia
k. Relation :Patient
l. Date of Admission : December 3, 2014
m. Time of admission : 6:45 PM
n. Attending Physician : Dr. Victoria Galang
. Admitting Vital Signs : BP: 160/100 mmHg RR: 26 cpm PR: 86 bpm T: 37.7°C
p. Food Allergy : No known food allergy
q. Drug Allergy : No known drug allergy
r. Educational Attainment : Elementary
s. Chief Complain : Few days prior to admission patient had experience elevated BP.
t. Admitting Diagnosis : Pregnancy Uterine Full Term, Pre eclampsia, Severe

A. History of Past Illness
Mrs. Preeclampsia had her complete vaccination in her childhood and had already
experienced mumps and measles during her pre-school years. She had no history of
hospitalizations due to any medical problems not until her present illness occurred. Normally,
she just uses over-the-counter drugs (paracetamol, biogesic, mefenamic acid, amoxicillin, etc.)
when experiencing common diseases such as moderate toothaches, cough, flu, and fever. Before
her pregnancy, she consumes alcoholic drinks occasionally. She had no history of smoking and
drug abuse, and she had no pre-existing hypertension. When she got pregnant, she normally eats
rice with meat and vegetable soup, and one fruit; supplied with regular glass of Anmum milk.
But the one food she can’t stop her self eating is “bulad”, as said by the pt.
Mrs. Preeclampsia’s blood pressure reading were actually low during her first, second
and thrird prenatal check-ups last October, November, and December; with 90/50mmHg, 90/70
mmHg, and 100/60 mmHg respectively. Mrs. Preeclampsia’s mother had history of high blood
pressure and heart disease, which she wasn’t able to recognize. Her elder sister experienced
hypertension during her first pregnancy, and delivered her baby via Caesarian Operation too.
Mrs. Preeclampsia stated that she had a lot of support system coming from her family,
relatives and friends. She is a Roman Catholic and makes it a point to visit and attend a mass
every Sunday with her husband. Their beliefs about life, their source for guidance in acting their
beliefs, and the relationship they have in exercising their faith is truly God-centered manner.

B. History of Present Illness
On December 3, 2014 at 10 in the morning, patient experienced slight pain with a scale of
2-3 from 0-10 pain scale. Since she is a nullipara, it was her first time to experience that pain and
didn’t know whether if it’s normal abdominal pain of if it was that of the labor’s pain. Without
further ado, she went to Bluestar Lying Inn Clinic at Casisang, Malaybalay City with her sister,
and her IE measured 4cm. Calming back from the panic, she then went home at her sister’s
house. At about 2pm, patient had blood show with a tolerable pain at 4-5 out of 0-10 pain scale.
At 6PM, the patient experienced severe abdominal pain at a pain scale of 8-9 over 10. IE was
done by the barangay midwife with 4-5cm cervical dilatation. At about 10PM, they went back to
Bluestar Lying Inn Clinic, her BP measured high at 140/80mmHg; so she was referred to Dra.
Galang at Bukidnon Provincial Medical Center.
At 1:30AM on February 17, 2013, she was admitted and diagnosed with Pregnancy
Uterine Full Term In Labor, Gravida 1 Para 0, Pre eclampsia, Severe; with an initial Blood
Pressure reading at 160/100mmHg. Mrs. Preeclampsia was then admitted to OB Ward at 6:30PM
and was monitored by the nurse-on-duty. Her wital signs and her baby’s fetal heart rate were
continuously monitored (FHT range from 140-155bpm). The doctor decided to perform “E”
Cesarean Operation.
Systems InvolvedASSESSMENT – December 4, 2014 Thursday
A. DIGESTIVE SYSTEM
OBJECTIVE SUBJECTIVE General Appearance:
Slight weakness Ambulatory Dressing noted on abdomen
Skin: Dry Cold , Clammy Good turgor
Eyeball: Sunken Moist
Tongue: Dry
Venous Filling: 2 seconds
Capillary refill: 2 seconds
Nail bed: Pale
Vital Signs: Temperature- 37.2C Pulse Rate- 96 bpm Respiratory Rate-20 cpm Blood pressure- 130/90
Intake and Output: Intake-370cc Output-500cc
Body Type: Ectomorph
Abdomen: Firm Bowel sounds: 15
Note: D5LR @ 30gtts/min
Pain: P – “Sakit akong tiyan nga geoperahan” Q – “Sakit nga ngot-ngot” R – “tibook jud naku tiyan” S – 9/10 T – “kanang galihok ko”
Respiration: “normal raman sir akong pagginhawa.”
as verbalized by Patient Diet:
NPO
Elimination Pattern: Bowel Movement “Wala pako kalibang sukad tung
gioperahan ko,’ as verbalized by the patient.

B. CARDIOVASCULAR/ CIRCULATORY SYSTEM
OBJECTIVE SUBJECTIVE Vital Signs:
Temperature- 36.6C Pulse Rate- 96 bpm Respiratory Rate-20 cpm Blood pressure- 130/90
Capillary refill: 2 seconds
Nail bed: Pale
Edema: Non-pitting Lower extremities
Varicosities: Both legs
Intake and Output: Intake-370cc Output-500cc
Note: D5LR @ 30gtts/min
History of present illness: Mother side of the patient had a history
of Hypertension
Do you experience any of the following: “Talagsa ga labad akong ulo” as
verbalized by the patient. “Ug gapaminhod akong mga tiil” as
verbalized by the patient
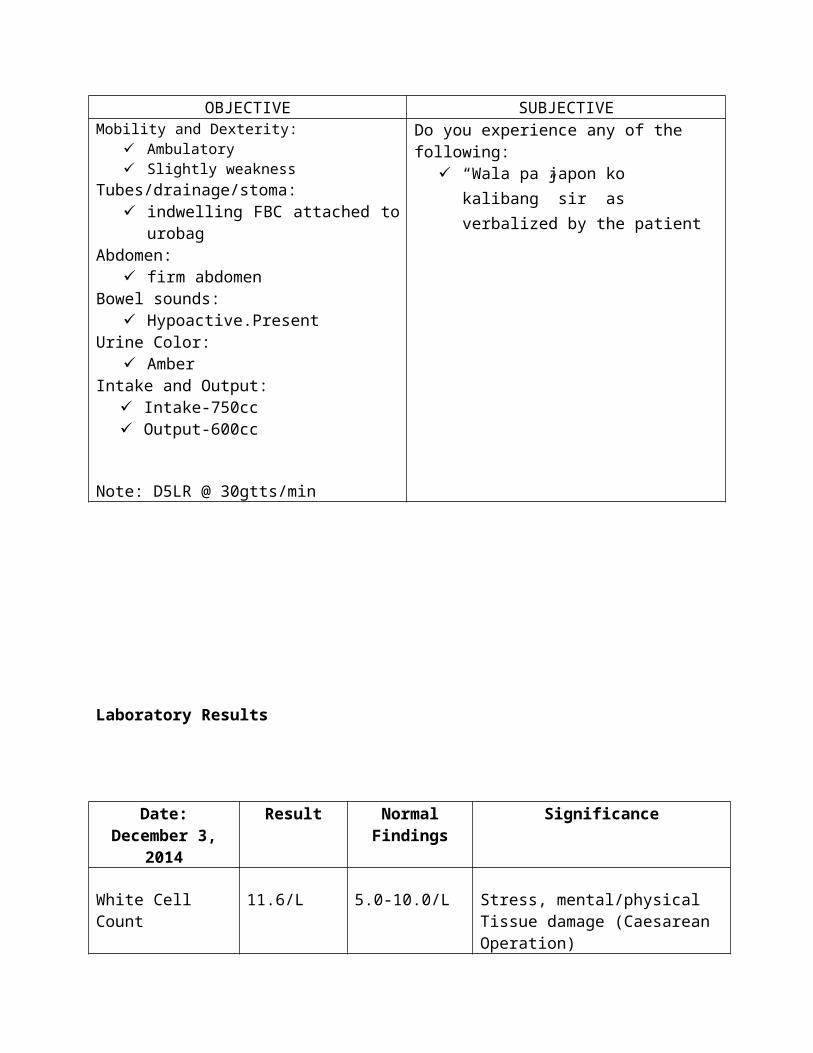
C. ELIMINATION
OBJECTIVE SUBJECTIVEMobility and Dexterity:
Ambulatory Slight weakness
Tubes/drainage/stoma: indwelling FBC attached to urobag
Abdomen: firm abdomen
Bowel sounds: Hypoactive.Present
Urine Color: Dark Amber
Note: D5LR @ 30gtts/min
Do you experience any of the following: “Wala pa ko kalibang gikan tong
naoperahan ko” sir as verbalized by the patient
ASSESSMENT – December 5, 2014 Friday
A. DIGESTIVE SYSTEM
OBJECTIVE SUBJECTIVE General Appearance:
Slight weakness Ambulatory Dressing noted at abdomen
Skin: Dry Good turgor
Eyeball: Sunken Moist
Tongue: Dry
Venous Filling: 2 seconds
Capillary refill: 2 seconds
Nail bed: Pink
Vital Signs: Temperature- 36.6C Pulse Rate- 82bpm Respiratory Rate-33cpm Blood pressure- 120/80
Intake and Output: Intake-750cc Output-600cc
Body Type: Ectomorph
Abdomen: Firm Bowel sounds: 10
Note: D5LR @ 30gtts/min
Pain: P – “Sakit akong tiyan nga geoperahan” Q – “Sakit nga ngot-ngot” R – “tibook jud naku tiyan” S – 8/10 T – “kanang galihok ko”
Respiration: “normal raman sir akong pagginhawa.”
as verbalized by Patient Diet:
Soft Diet
Elimination Pattern: Bowel Movement “wala pako kalibang sukad tung
gioperahan ko,’ as verbalized by the patient.
B. CARDIOVASCULAR/ CIRCULATORY SYSTEM
OBJECTIVE SUBJECTIVE

Vital Signs: Temperature- 36.6C Pulse Rate- 82bpm Respiratory Rate-33cpm Blood pressure- 120/80
Capillary refill: 2 seconds
Nail bed: Pink
Varicosities: Both legs
Intake and Output: Intake-750cc Output-600cc
Note: D5LR @ 30gtts/min
History of present illness: Mother side of the patient had a history
of Hypertension
Do you experience any of the following: “Talagsa ga labad akong ulo” as
verbalized by the patient. “mao ra japon sir gapaminhod akong
mga tiil pero panagsa nlng” as verbalized by the patient
C. ELIMINATION
OBJECTIVE SUBJECTIVEMobility and Dexterity:
Ambulatory Slightly weakness
Tubes/drainage/stoma: indwelling FBC attached to urobag
Abdomen: firm abdomen
Bowel sounds: Hypoactive.Present
Urine Color: Amber
Intake and Output: Intake-750cc Output-600cc
Note: D5LR @ 30gtts/min
Do you experience any of the following: “Wala pa japon ko kalibang” sir as
verbalized by the patient

Laboratory Results
Date: December 3, 2014
Result Normal Findings
Significance
White Cell Count 11.6/L 5.0-10.0/L Stress, mental/physical Tissue damage (Caesarean Operation)
Red Cell Count 4.75mil/mm3 3.69-5.13mil/mm3
Normal; ‹ anemia, bleeding, dehydration› smoking, congenital heart disease, hypoxia
Hemoglobin 14.7g/dL 11.7-14.5g/dL Due to low Oxygen levels in the bloodBody not having as much fluids and water as it should
Hematocrit 40.7vols% 34.1-44.3vols% Normal; ‹ anemia, bleeding, malnutrition › dehydration, erythrocytosis, hypoxia
Platelet Count 224,000/ml 174,000-390,000/ml
Normal; ‹ thrombocytopenia, autoiimune disorders, risk of bleeding is much higher› thrombocytosis, risk of forming blood clots
Mean Corpuscular Volume
85.7fL 81.5-96.7fL Normal (Normocytic anemia) ; ‹ microcytic. Small average RBC size› macrocytic, large average RBC size
Mean Corpuscular Hemoglobin
30.9pg 26.5-33.5pg Normal; ‹ small red cells would have a lower value› macrocytic RBCs are large so tend to have a higher MCH.
Mean Corpuscular Hemoglobin Concentration
36g/dL 31.9-36g/dL Normal; ‹ May be low when MCV is low; decreased MCHC values (hypochromia) are seen in conditions

such as iron deficiency anemia and thalassemia› Increased MCHC values (hyperchromia) are seen in conditions where the hemoglobin is more concentrated inside the red cells, such as autoimmune hemolytic anemia, in burn patients, and hereditary spherocytosis, a rare congenital disorder
Segmenters 65% 43.4-76.2% Normal; ‹ viral infection, autoimmune diseases, some medications and malignancy› Ongoing infection, an inflammation, malignancy
Lymphocyte 35% 17.4-46.2% Normal; ‹ usually not significant› acute infection especially viral infections, leukemia, smoking
Urine Analysis Result Normal Findings
Significance
Color Yellow Light Yellow- Amber
Normal; concentrated is darker, kidney stones may produce blood in
urineTransparency Clear Clear-Slightly
HazyNormal; transparent when freshly
voided but becomes turbid (cloudy) upon standing
Sugar (Glucose) Negative Negative Normal; > stress, diabetes mellitus, brain injury, myocardial infarction
Specific Gravity 1.015 1.005-1.025 Normal; (density) the higher the concentration of solutes, the higher
the specific gravityProtein Negative 0-Trace Normal; > nephritis, fever, severe
anemias, trauma and hyperthyroidismPus Cells 0-3pvf 0-4 pvf Normal; infectionRBC 2-5HPF 0-3HPF Infection/inflammation in the Urinary
Tract itself, trauma to the bladder or kidney disease, trauma
Epithelium few 0-few Normal; > urinary tract infections, inflammation, malignancies

C. Etiology of the Disease/ Anatomy and Physiology
Etiology: Unknown
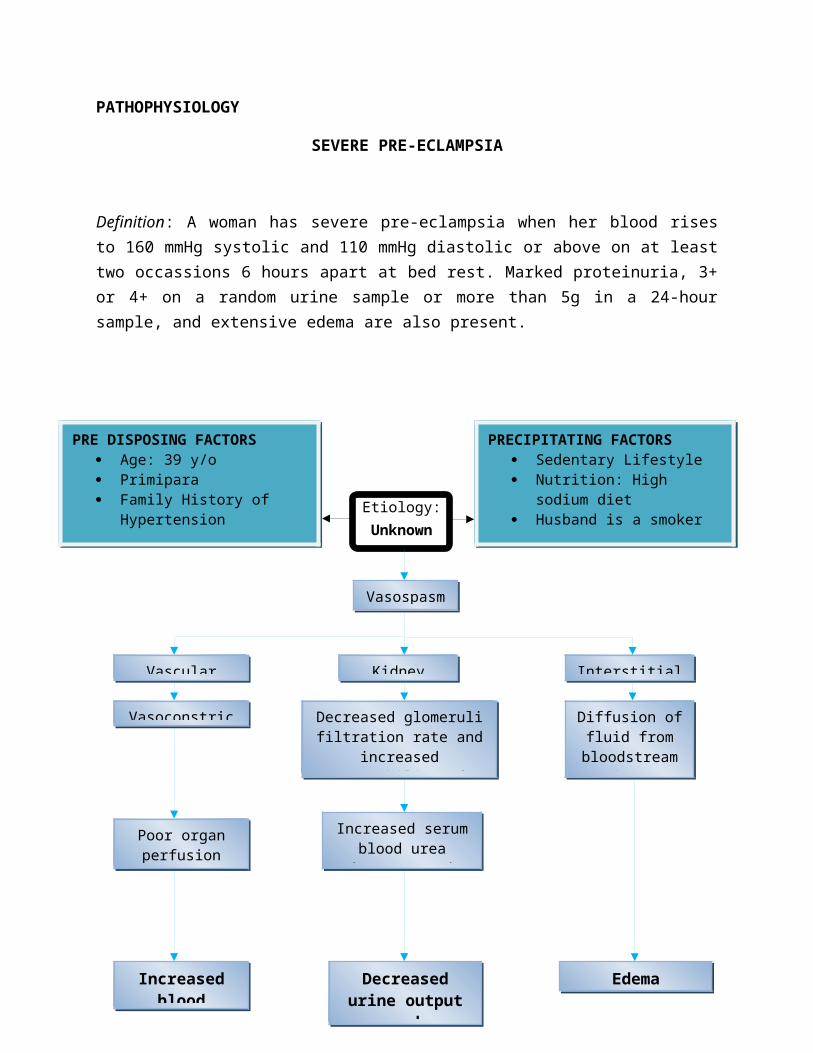
PATHOPHYSIOLOGY
SEVERE PRE-ECLAMPSIA
Definition: A woman has severe pre-eclampsia when her blood rises to 160 mmHg systolic and 110 mmHg diastolic or above on at least two occassions 6 hours apart at bed rest. Marked proteinuria, 3+ or 4+ on a random urine sample or more than 5g in a 24-hour sample, and extensive edema are also present.
PRE DISPOSING FACTORS Age: 39 y/o Primipara Family History of
Hypertension
PRECIPITATING FACTORS Sedentary Lifestyle Nutrition: High sodium diet Husband is a smoker
Vasospasm
Vascular Effects Kidney Effects Interstitial Effects
Vasoconstriction Decreased glomeruli filtration rate and increased permeability of glomeruli
membranes
Diffusion of fluid from bloodstream
into interstitial tisssue
Poor organ perfusion
Increased blood pressure
Increased serum blood urea nitrogen, uric acid, and creatinine
Decreased urine output and proteinuria
Edema

II- THEORETICAL FRAMEWORK
CARE, CURE, CORE (3 C’S)By: Lydia Eloisa Hall
Lydia Hall Care Core Cure enumerated three aspects of the person as patient: the person (core), the body (care), and the disease (cure). These aspects were envisioned as overlapping circles that influence each other.
Hall clearly stated that the focus of nursing is the provision of intimate bodily care. She reflected that the public has long recognized this as belonging exclusively to nursing. Being expert in the area of body involved more than simply knowing how to provide intimate bodily care. To be expert, the nurse must know how to modify care depending on the pathology and treatment while considering the unique needs and personality of the patient.
Based on her view of the person as patient, Hall conceptualized nursing as having three aspects, and delineated the area that is the specific domain of nursing, as well as those areas that are shared with other professions. Hall believed that this model reflected the nature as a professional interpersonal process. She visualized each of the three overlapping circles as an aspect of the nursing process related to the patient, to the supporting sciences, and to the underlying philosophical dynamics. The circles overlap and change in size as the patient progresses through a medical crisis to the rehabilitative phase of the illness. In the acute care phase, the cure is the largest. During the evaluation and follow-up phase, the care circle is predominant.
Care
This is the part of the model reserved for nurses, and focused on performing that noble task of nurturing the patients, meaning the component of this model is the “motherly” care provided by nurses, which may include, but is not limited to provision of comfort measures, provision of patient teaching activities and helping the patient meet their needs where help is needed. This aspect provided the opportunity for closeness and required seeing the process as an interpersonal relationship. Hands on care for patients produce an environment of comfort and trust and promotes open communication between nurses and patients.
Cure
The second aspect of the nursing process is shared with medicine and is labeled as the “cure”. Hall comments on the two ways that this medical aspect of nursing may be viewed; it may be viewed as the nurse assisting the doctor by assuming medical tasks or functions. The other view of this aspect of nursing is to see the nurse helping the patient through his or her medical, surgical, and rehabilitative care in the role of comforter and nurturer.
Core

The third are that nursing shares with all of the helping professions is that of using relationships for therapeutic effect – the core. This area emphasizes the social, emotional, spiritual, and intellectual needs of the patient in relation to family, institution, community and the world. Knowledge foundational to the core was based on the social sciences and therapeutic use of self. Through the closeness offered by the provision of intimate bodily care, the patient will feel comfortable enough to explore with the nurse “who he is, where he is, where he wants to go and will take or refuse help in getting there – the patient will make amazingly rapid progress toward recovery and rehabilitation”. Hall believed that through this process, the patient would emerge as a whole person.
SELF-CARE MODELBy: Dorothea Orem
1. Self-care comprises those activities performed independently by an individual to promote and maintain person well-being
2. Self-care agency is the individual’s ability to perform self-care activities3. Self- care deficit occurs when the person cannot carry out self-care4. The nurse then meets the self-care needs by acting or doing for; guiding, teaching,
supporting or providing the environment to promote patient’s ability5. Wholly compensatory nursing system-Patient dependent6. Partially compensatory- Patient can meet some needs but needs nursing assistance7. Supportive educative-Patient can meet self-care requisites, but needs assistance with
decision making or knowledge
HEALTH CARE SYSTEMS MODEL By: Betty Neuman
1. The person is a complete system, with interrelated parts2. Maintains balance and harmony between internal and external environment by adjusting
to stress and defending against tension-producing stimuli3. Focuses on stress and stress reduction4. Primarily concerned with effects of stress on health5. Stressors are any forces that alter the system’s stability6. Flexible lines of resistance - Surround basic core7. Internal factors that help defend against stressors8. Normal line of resistance - Normal adaptation state9. Flexible line of defense - Protective barrier, changing, affected by variables10. Wellness is equilibrium

IV. DISCHARGE PLANS
DISCHARGE GOALS:
1. Pain relieved/controlled.2. Complications prevented/minimized.3. Mobility/function regained or compensated for.4. Surgical procedure, prognosis, and therapeutic regimen understood.5. Plan in place to meet needs after discharge
M - Medications
Take home medication as prescribed by the Physician which includes the following: Cefuroxime 500mg BID x 7 daysMefenamic Acid 500mg TID x 7 days
Report any side effects & adverse reactions as indicated by the healthcare provider. Check with physician about administration of other medications.
E - Environment/Exercise
Instruct patient to stay in calm, quiet environment. Home environment must be free from slipping or accident hazards.
Don’t try to take care of anyone other than your baby and yourself. Remember, the more active you are, the more likely you are to have an increase in your
bleeding. Get lots of rest. Take naps in the afternoon. Increase your activities gradually. Plan your activities so that you don’t have to go up or down stairs more than necessary.
T - Treatment
Encourage to take Vitamin C and Iron Supplements. Proper wound care at surgical site.
H – Health Teachings
Encourage to increase fluid intake. Proper hygiene.
Watch incision for signs of infection, such as increasing redness or drainage. Hold a pillow against the incision when you laugh or cough and when you get up from a
lying or sitting position Do postsurgical deep breathing and coughing exercises. Ask your doctor for instructions. Don’t lift anything heavier than your baby until your doctor tells you it’s okay.
Don’t have sexual intercourse until after you’ve had a follow-up appointment with your doctor and you’ve decided on a birth control method.
O – Out Patient
Inform patient to have a follow-up check up after 1 week. Inform patient to return after 1 week for removal of sutures.
When to Call Your Doctor?
Call your doctor right away if you have any of the following:• Fever of 38.0°C or higher• Redness, pain, or drainage at your incision site• Repeated clots of blood (the size of a quarter or larger) passing from the vagina• Bleeding that requires a new sanitary pad every hour• Severe pain in the abdomen• Pain or urgency with urination• Trouble urinating or emptying your bladder• No bowel movement within 1 week after the birth of your baby
D- Diet
Encourage intake of foods rich in fiber such as green leafy vegetables. Encourage increase intake of foods rich in Iron such as dark green leafy vegetables. Low sodium and avoidance of fatty foods. Encourage intake of foods rich in Vitamin C such as citrus.
V. BIBLIOGRAPHY
Books
Brunner and Suddarth’s Textbook of Medical and Surgical Nursing by Suzanne c. Smelter & Brenda G. Bare 10th Edition Volume 1
Focus on Nursing Pharmacology 3rd Edition by Amy M. Karch
2010 Edition Delmar Nurse’s Drug Handbook by George R. Spratto and Adrienne L. Woods
Concise Pocket Medical Dictionary 2nd Edition by UN Panda
Nurse’s Pocket Guide 9th Edition by Merilynn E. Doenges
Pathophysiology Made Incredibly Easily 3rd Edition
Webster’s New World Dictionary of the American Language – Student’s Edition
Fundamentals of Nursing 7th Edition by Barbara Kozier
Principles of anatomy and Physiology 9th Edition by tortora and Grabowski


















