Predictors of Health Outcomes Among Patients With Type II Diabetes Mellitus
138
PREDICTORS OF HEALTH OUTCOMES AMONG PATIENTS WITH TYPE II DIABETES MELLITUS A Thesis Presented to the Faculty of the Graduate School of the University of the Visayas Cebu City, Philippines In Partial Fulfillment of the Requirements for the Degree of MASTER OF ARTS IN NURSING Major in Medical-Surgical Nursing
-
Upload
norman-batalla-juruena -
Category
Documents
-
view
16 -
download
4
description
Master of Arts in Nursing major in Medical-Surgical Nursing
Transcript of Predictors of Health Outcomes Among Patients With Type II Diabetes Mellitus

PREDICTORS OF HEALTH OUTCOMES AMONG PATIENTS WITH TYPE II DIABETES MELLITUS
A Thesis Presented tothe Faculty of the Graduate School
of the University of the VisayasCebu City, Philippines
In Partial Fulfillment of the Requirements for the Degree ofMASTER OF ARTS IN NURSINGMajor in Medical-Surgical Nursing
NORMAN B. JURUENA
August 2015

APPROVAL SHEET
This thesis titled “PREDICTORS OF HEALTH OUTCOMES AMONG PATIENTS WITH TYPE II DIABETES MELLITUS” submitted by NORMAN B. JURUENA in partial fulfillment of the requirements for the degree of MASTER OF ARTS IN NURSING MAJOR IN MEDICAL-SURGICAL NURSING has been examined and is recommended for acceptance and approval for ORAL EXAMINATION.
BRENDA P. MANGUILIMOTAN, Ph.D.Professor, Graduate SchoolUniversity of the Visayas
Adviser
THE THESIS COMMITTEE
EDSEL P. INOCIAN, Ph.D.Professor
Velez CollegeChairman
GERONIMA EMMA A. AMORES, D.M. ISABELITA T. ABELLANOSA, D.M.Program Coordinator, Graduate School Professor, Graduate School
University of the Visayas University of the VisayasMember Member
Accepted and approved for oral examination
ZOSIMA A. PANARES, Ph.D.Dean, Graduate School
PANEL OF ORAL EXAMINERS
Approved by the Committee on Oral Examination with a grade of PASSED.
EDSEL P. INOCIAN, Ph.D.Professor
Velez CollegeChairman
GERONIMA EMMA A. AMORES, D.M. ISABELITA T. ABELLANOSA, D.M.Program Coordinator, Graduate School Professor, Graduate School
University of the Visayas University of the VisayasMember Member
Accepted and approved in partial fulfilment of the requirements for the degree of MASTER OF ARTS IN NURSING Major in Medical-Surgical Nursing.
Comprehensive Examination: PASSEDOral Examination: August 08, 2015Book Submission:
ZOSIMA A. PANARES, Ph.D.Dean, Graduate School
ACKNOWLEDGEMENT
The researcher would like to express his deepest gratitude and indebtedness to the
several individuals who have contributed in making this study possible:
Dr. Brenda P. Manguilimotan, Adviser, for her patience, support, untiring
guidance, valuable advises and provisions that benefited the researcher for establishing
and completion of this study;
Dr. Zosima A. Panares, Dean of Graduate School, for allowing the researcher to
conduct this study;
The Committee, Chairman Dr. Edsel P. Inocian, Dr. Geronima Emma A.
Amores and Dr. Isabelita T. Abellanosa, for their assistance, valuable comments and
recommendations that benefited the researcher for the improvement of this study;
The family and friends, for their undying support, words of encouragement in
order to sustain the researcher in his field of endeavor and inspirations that helped the
researcher to achieve this study; and
Most of all, to Almighty God, who is the researcher’s ultimate source of strength,
knowledge, wisdom, inspiration, and guiding consciousness during the course of this
study and as well as the overall success of this study.
The Researcher
ABSTRACT
Diabetes Mellitus is a common chronic condition almost worldwide. The management of this disease is a lifelong care with complex course of therapy which requires thorough understanding of the disease and adherence to treatment regimen. However, Diabetes Mellitus remains to be a major public health challenge worldwide. The study examined the factors that predict the health outcomes among patients with Type II Diabetes Mellitus for the month of July 2015 utilizing a descriptive-analytical design. The study was composed of 128 patients who were 18 years old and above, diagnosed at least a year with Type II Diabetes Mellitus, no previous surgeries or hospitalization from May 2015 up to dated study conducted, independent and with little assistance in self-care activities, able to read, understand and sign informed consent, lives in a home setting, and currently on an outpatient status. An adapted-and-modified Health Interview Questionnaire from the National Health and Nutrition Examination Survey (NHANES) and Diabetes Attitudes, Wishes and Needs (DAWN™) Study were used to determine the factors that predict the health outcomes among patients with Type II Diabetes Mellitus.
Most of the respondents were 60 years and above and were females with vocational education, married, retired, with more than 16 years of diagnosis, with perceived good health status, mostly weighing below 50 kilograms, and were within the 1.54 to 1.69 meters (5’1 to 5’6 feet) height range. In terms of treatments as perceived barriers to action, 60 respondents agreed that there were too many treatments to manage. Most respondents considered situational influences a moderate problem. The adherence level to health-promoting behaviors of the respondents was rated good. The health outcomes of the respondents in terms of body mass index, lipid profile, fasting blood sugar, and glycosylated hemoglobin A1c had normal results. Sex and weight were predictors of health outcomes for body mass index. Weight was a predictor of health outcomes for lipid profile. Dietary behavior, civil status and weight predicted the health outcomes for glycosylated hemoglobin A1c. The researcher proposed to develop a health promotion program to improve and prolong the lives of the patients with Type II Diabetes Mellitus.
Keywords: Healthcare Management, Health-Promoting Behaviors, Predictors of Health Outcomes, Type II Diabetes Mellitus Patients, Asia, Philippines

TABLE OF CONTENTS
TITLE PAGE i
APPROVAL SHEET ii
ACKNOWLEDGMENT iv
ABSTRACT v
TABLE OF CONTENTS vi
LIST OF FIGURES ix
LIST OF TABLES x
Chapter Page
I THE PROBLEM
Introduction 1
Theoretical Framework 3
Statement of Purpose 12
Null Hypothesis 13
Significance of the Study 13
DEFINITON OF TERMS 15
II REVIEW OF RELATED LITERATURE AND STUDIES
Personal Factors 18
Perceived Barriers to Action 22
Situational Influences 24
Health-Promoting Behaviors 27

Health Outcomes 34
Overall Summary of the Review 37
III METHODOLOGY AND PROCEDURES
Design 38
Environment 38
Respondents 39
Instruments 39
Data Gathering Procedure 41
Data Analysis 42
Ethical Considerations 43
IV PRESENTATION, ANALYSIS AND INTERPRETATION OF DATA
Profiles of the patients with Type II Diabetes Mellitus 46
Adherence Level to Health-Promoting Behaviors 52
Health Outcomes of the patients with Type II Diabetes Mellitus60
Predictors of Health Outcomes for Body Mass Index 61
Predictors of Health Outcomes for Lipid Profile 63
Predictors of Health Outcomes for Fasting Blood Sugar 65
Predictors of Health Outcomes for Hemoglobin A1c 66
V SUMMARY OF FINDINGS, CONCLUSIONS AND RECOMMENDATIONS
Summary of Findings 69
Conclusions 71
Recommendations 71
REFERENCES 74

APPENDICES
Appendix A: Transmittal Letter to the Dean of Graduate School 82
Appendix B: Transmittal Letter to the Medical Center Chief 83
Appendix C: Informed Consent English Version 84
Appendix D: Informed Consent Cebuano Version 85
Appendix E: Instrument English Version 86
Appendix F: Instrument Cebuano Version 91
Appendix G: Proposed Health Promotion Program 96
Appendix H: Certificate of Integrated Research Board Approval 101
Appendix I: Certificate of Anti-plagiarism Check 104
Appendix J: Certificate of Critic Reader 109
CURRICULUM VITAE 110
LIST OF FIGURE
Figure Page
1 Schematic Diagram of Theoretical Framework of the Study 11
LIST OF TABLES
Table Page
1 Personal Factors of the patients with Type II Diabetes Mellitus 47
2 Treatments as Perceived Barriers to Action of the patients with
Type II Diabetes Mellitus 49
3 Situational Influences of the patients with Type II Diabetes Mellitus 50
4 Adherence Level to Health-Promoting Behaviors of the patients with
Type II Diabetes Mellitus 53
5 Summary of Adherence Level to Health-Promoting Behaviors of the
patients with Type II Diabetes Mellitus 58
6 Health Outcomes of the patients with Type II Diabetes Mellitus 60
7 Predictor of Health Outcomes for Body Mass Index 61
8 Predictor of Health Outcomes for Lipid Profile 64
9 Predictor of Health Outcomes for Fasting Blood Sugar 65
10 Predictor of Health Outcomes for Glycosylated Hemoglobin A1c 66

Chapter I
THE PROBLEM
Introduction
Diabetes Mellitus is a common chronic condition almost worldwide. The
management of this disease is a lifelong care with complex course of therapy which
requires thorough understanding of the disease and adherence to treatment regimen.
Every diabetic individual is expected to assume his duties to manage himself, requiring
involvement in the treatment regimen. Adherence to health-promoting behaviors may
improve the over-all diabetic individual’s health outcome.
However, Diabetes Mellitus remains to be a major public health challenge
worldwide. Apparently, the global prevalence of the Diabetes Mellitus is significantly
growing. This may due to lack of health education regarding on the disease and lack of
health promotions, thus, poor understanding of the disease and poor adherence to health-
promoting behaviors which may lead to poor health outcome among diabetic individuals.
According to the International Diabetes Federation (2011), approximately 366 million of
populace worldwide has a Diabetes Mellitus. In 2012, nearly 1.5 million deaths were
directly caused by the Diabetes Mellitus and over 80% of Diabetes Mellitus deaths were
come from in low- and middle-income countries (World Health Organization, 2012).
Moreover, this public health challenge has reached pandemic proportions and a
prevalence of 552 million people with Diabetes Mellitus in the year 2030 has been
predicted (International Diabetes Federation, 2011).

In the Philippines, there is a drastic increase in number of incidence of the
diabetes mellitus affecting the Filipinos. In fact, a survey conducted by the Philippine
Cardiovascular Outcome Study on Diabetes Mellitus last 2008 that one out of every five
Filipinos aged 30 years and above were found to have a Diabetes Mellitus which means
20.6% of the population have Diabetes Mellitus from only 3.9% in 1998 (Philippine
Diabetes Statistics, 2012). Furthermore, according to the International Diabetes
Federation (2010), Philippines ranks in the top 15 worldwide and now become one of the
world’s emerging Diabetes Mellitus hotspots.
According to the Department of Health (2010), in Davao Region, there are 1,122
reported cases of deaths in Diabetes Mellitus, a significant increase of mortality rate from
784 in 2001. In Davao City, there are 329 mortality rates of Diabetes Mellitus in 2011
from 227 reported cases of deaths in 2010 according to Davao City Health Office.
Provision to every Filipino of the highest possible quality of health care that is
accessible, efficient, equitably distributed, adequately funded, fairly financed, and
appropriately used by an informed and empowered public is the greatest aim of the
Universal Health Care of the Department of Health in order to address the equity of the
health care delivery system in the Philippines (Department of Health, 2010). Health and
Wellness advocacy towards health-promoting behaviors is strongly encouraged.
Therefore, health care providers need effective ways to develop, implement and support
health promotions among diabetic individuals. The purpose of this study is to examine
the factors that predict the health outcomes among patients with Type II Diabetes
Mellitus.

Theoretical Framework
This study anchored the Health Promotion Model (HPM) by Nola J. Pender
(1996). The theory discussed about the factors that predict the health promotion
behaviors which can influence the individual to engage on health-promoting behaviors
and these may affect the individual’s over-all health outcomes.
Nola J. Pender’s background in nursing, human development, experimental
psychology, and education led her to use a holistic nursing perspective, social
psychology, and learning theory as the foundations for the Health Promotion Model.
Health Promotion Modeld expands to encompass behaviors for enhancing health and
potentially applies across the lifespan (Tomey & Alligood, 2002).
Health Promotion Model is an attempt to describe the multifaceted nature of
persons interacting with the environment as they pursue health. It is driven by the desire
to increase well-being and actualize the human potential. Nola J. Pender asserts that there
are complex biophysical processes that motivate individuals to engage in behaviors
directed toward the enhancement of health (Tomey & Alligood, 2002).
The major concepts utilized in the Health Promotion Model are divided into three
following categories: (1) individual characteristics and experiences; (2) behavior-specific
cognitions and affect; and (3) behavioral outcome.
The major concepts in the Individual Characteristics and Experiences category are
as followed: (1) prior related behavior; and (2) personal factors such as biological,
psychological, and socio-cultural.
Prior related behaviors are defined as frequency of the same or similar behavior in
the past. Personal factors are defined as those distinguishing characteristics, which might
affect behaviors. It categorized into three factors as: (1) biological factors including age,
gender, body mass index, pubertal or menopausal status, aerobic capacity, strength,
agility, or balance; (2) psychological factors including self-esteem, self-motivation,
personal competence, perceived heath status, and definition of health; and (3) socio-
cultural factors including race, ethnicity, acculturation, education, and socio-economic
status (Tomey & Alligood, 2002).
The major concepts in the Behavior-specific Cognition and Affect category are as
followed: (1) perceived benefits of action; (2) perceived barriers to action; (3) perceived
self-efficacy; (4) activity-related affect; (5) interpersonal influences; and (6) situational
influences.
Perceived benefits of action are defined as anticipated positive outcomes that will
occur from health behavior. Perceived barriers to action are defined as anticipated,
imagined or real blocks and personal costs of undertaking a given health behavior.
Perceived self-efficacy is defined as the judgment of personal capacity to organize and
execute a health-promoting behavior. Perceived self-efficacy influences perceived
barriers to action so higher efficacy results in lowered perceptions of barriers to the
performance of the behavior. Activity-related affect is defined as the subjective positive
or negative feelings that occur prior to, during, and following behavior based on the
stimulus properties of the behavior itself. It also influences perceived self-efficacy, which
means the more positive the subjective feeling, the greater the feeling of efficacy. In turn,
increase feelings of efficacy can generate further positive affect. Interpersonal influences

are defined as the cognitions concerning the behaviors, beliefs, or attitudes of others. It
includes the norms (expectations of significant others), social support (instrumental and
emotional encouragement), and modeling (various learning through observing others
engaged in a specific behavior). Primary sources of interpersonal influences are families,
peers, and healthcare providers. Situational influences are defined as those personal
perceptions and cognitions of any given situation or context that can facilitate or impede
behavior. It includes perceptions of options available, demand characteristics, and
aesthetic features of the environment in which a given health-promoting behavior is
proposed to take place. It may have direct or indirect influences on health behavior
(Tomey & Alligood, 2002).
The major concepts in the Behavioral Outcome category are as followed: (1)
commitment to a plan of action; (2) immediate competing demands and preferences; and
(3) health-promoting behavior.
Commitment to a plan of action is defined as the concept of intention and
identification of a planned strategy leads to implementation of health behavior.
Immediate competing demand is defined as an alternative behavior over which
individuals have low control because there are environmental contingencies such as work
or family care responsibilities. Immediate competing preference is defined as an
alternative behavior over which individuals exert relatively high control, such as choice
of ice cream or an apple for a snack. Health-promoting behavior is defined as endpoint or
action outcome directed toward positive outcomes such as optimal well-being, personal
fulfillment, and productive living (Tomey & Alligood, 2002).

The independent and dependent variables used in this study had been categorized
according to the Health Promotion Model by Nola J. Pender (1996). The independent
variables were divided into two properties: (1) profile of the patients with Type II
Diabetes Mellitus in terms of personal factors, treatments as perceived barriers to action
and situational influences; and (2) adherence level to health-promoting behaviors in terms
of health-responsibility, medication adherence, dietary and exercise behaviors. On the
other hand, the dependent variable was the health outcomes of the patients with Type II
Diabetes Mellitus in terms of body mass index, lipid profile, fasting blood sugar and
glycosylated hemoglobin A1c.
The following independent variables were categorized under the construct of
personal factors including the demographic profiles such as age, sex, educational
attainment, civil status, occupation and financial status, the length of disease diagnosis,
perceived health status, and body measurements such as weight and height.
Demographic Profile. The respondents were asked to self-report their age in
years; sex whether male or female; elementary indicated as the lowest educational
attainment and post-graduate indicated as the highest educational attainment; civil status
whether single, married, widow/er or annulled/separated; occupation whether none, self-
employed, employed or retired; financial status whether below average, average or above
average income earner/pensioner.
Length of Disease Diagnosis. The respondents were asked to self-report the year
at the time when they were diagnosed with Type II Diabetes Mellitus by their physician.
The researcher calculated the length of disease diagnosis by subtracting the respondents’
reported year from the present year of this study conducted. The researcher categorized

the length of disease diagnosis using the 4-point likert scale indicating value 1 as 1 to 5
years, value 2 as 6 to 10 years, value 3 as 11 to 15 years and value 4 as more than 16
years.
Perceived Health Status. The respondents were asked to rate their general health
condition using the 4-point likert scale indicating “very good”, “good”, “fair”, and
“poor”. These values were reverse scored by the researcher and used to represent the
variable perceived heath status in the study where a value of 1 indicated poor and a value
of 5 indicated excellent. The researcher calculated the variable “perceived health status”
by taking the frequency and percentage of the respondents’ responses from this item.
Body Measurements. The body measurements including the weight and height
were obtained thru actual assessment at the time of scheduled interview using calibrated
equipment such as weighing scale and stadiometer respectively. The weight
measurements were reported in kilograms and the height measurements were reported in
meters. The researcher categorized the weight using the 6-point likert scale indicating
value 1 as less than 50 kg, value 2 as 51 to 55 kg, value 3 as 56 to 60 kg, value 4 as 61 to
65 kg, value 5 as 66 to 70 kg and value 6 as more than 71 kg. Also, the researcher
categorized the height using 4-point likert scale indicating value 1 as less than 1.53
meters, value 2 as 1.54 to 1.69 meters, value 3 as 1.70 to 1.84 meters and value 4 as more
than 1.85 meters. These body measurements were used for the calculations of the body
mass index. The researcher also obtained the baseline data of both weight and height thru
chart review within the period from January to April 2015.
The following independent variables were categorized under the construct of
Perceived Barriers to Action and Situational Influences.

Treatments as Perceived Barriers to Action. The respondents were asked to
rate the treatments as perceived barriers to action using the 4-point likert scale from 1 to 4
indicating “strongly disagree”, “disagree”, “agree” and “strongly agree” that addressed
the difficulties on treatment adherence where a value of 1 indicated strongly disagree and
a value of 4 indicated strongly agree. The researcher calculated the variable “treatments
as perceived barriers” by taking the frequency and percentage of the respondents’
responses from this item.
Situational Influences. The respondents were asked to answer 20 items in the
problem areas in diabetes survey that addressed the diabetes-related emotional distress
which also correlates with measures of related concepts such as depression, social
support, health beliefs, and coping style, as well as predicts future blood glucose control
of the patient. The respondents were asked to rate each item using the 5-point likert scale
from 0 to 4 indicating “not a problem”, “minor problem”, “moderate problem”,
“somewhat serious problem” and “serious problem” where a value of 0 indicated not a
problem and a value of 4 indicated serious problem. The researcher calculated the
variable “diabetes-related emotional distress” by taking the weighted mean of the
respondents’ responses from each item and grand weighted mean from these 20 items. A
serious problem is an indicative of emotional burnout and warrant special attention. The
result may drop up to moderate problem in response to educational and medical
interventions. An extremely low score combined with poor glycemic control may be
indicative for denial.

The following independent variables were categorized under the construct of
Health-Promoting Behaviors including health responsibility, medication adherence,
dietary and exercise behaviors.
Health-Promoting Behaviors. The respondents were asked to answer 14 items in
the health-promoting behavior survey that addressed the adherence level to the following
variables of health-promoting behaviors including three-item health responsibility
behaviors, four-item medication adherence behaviors, five-item dietary behaviors and
two-item exercise behaviors. The respondents were asked to rate each item using the 5-
point likert scale from 1 to 5 indicating “never/poor”, “rarely/fair”, “sometimes/good”,
“oftentimes/very good” and “always/excellent” where a value of 1 indicated never/poor
and a value of 5 indicated always/excellent. The researcher calculated each variable of
“health-promoting behaviors” by taking the weighted mean of the respondents’ responses
from each variable. The lower the result is an indicative of low adherence level and the
higher the result is an indicative of high adherence level.
The following dependent variables were categorized under the construct of Health
Outcomes including the body mass index and the diabetic control measures such as lipid
profile, fasting blood sugar and glycosylated hemoglobin A1c.
Body Mass Index. The respondents received body measurements including
weight and height were obtained thru actual assessment at the time of scheduled
interview. The weight and height measurements were reported in kilograms and meters
respectively and these values were used in the direct calculation of body mass index by
the researcher. Body Mass Index (BMI) values were calculated using the formula of
weight in kilograms divided by the squared value of the height in meters. The researcher
also obtained the baseline data of body mass index thru chart review within the period
from January to April 2015. The results were scored using the 3-point likert scale from 1
to 3 indicating “below normal”, “normal” and “above normal”. A value of 1 indicated
below normal and a value of 3 indicated above normal.
Diabetic Control Measures. The diabetic control measures including the lipid
profile, fasting blood sugar and glycosylated hemoglobin A1c were obtained thru actual
assessment of the latest results within the period from May to July 2015 and were
extracted from the respondents’ records from Mindanao Diabetes Center Clinic thru chart
review. The researcher also obtained the baseline data of these diabetic control measures
thru chart review within the period from January to April 2015. The results were scored
using the 3-point likert scale from 1 to 3 indicating “below normal”, “normal” and
“above normal”. A value of 1 indicated below normal and a value of 3 indicated above
normal.
Based on the findings of this study, the researcher developed a propose health
promotion program to the patients with Type II Diabetes Mellitus.

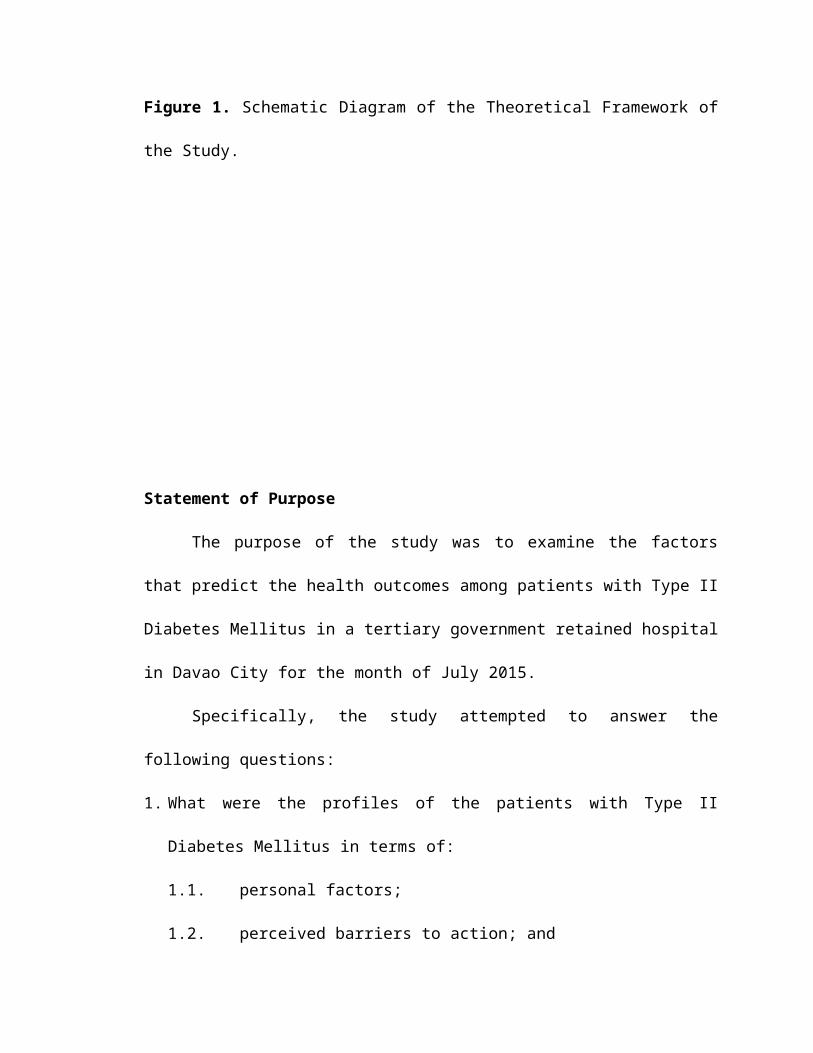
Health outcomes in terms of:Body Mass IndexLipid ProfileFasting Blood SugarGlycosylated Hemoglobin A1c
Profile in terms of:Personal FactorsTreatments as Perceived Barriers to ActionSituational Influences
Adherence level to health-promoting behaviors in terms of:Health-Responsibility BehaviorsMedication Adherence BehaviorsDietary BehaviorsExercise Behaviors
Health Promotion Model(Pender, 1996)
Type II Diabetes Mellitus PatientsSouthern Philippines Medical Center
J.P. Laurel Avenue, Bajada, Davao City
Proposed Health Promotion Program Figure 1. Schematic Diagram of the Theoretical Framework of the Study.
Statement of Purpose
The purpose of the study was to examine the factors that predict the health
outcomes among patients with Type II Diabetes Mellitus in a tertiary government
retained hospital in Davao City for the month of July 2015.
Specifically, the study attempted to answer the following questions:
1. What were the profiles of the patients with Type II Diabetes Mellitus in terms of:
1.1. personal factors;
1.2. perceived barriers to action; and
1.3. situational influences?
2. What was the adherence level of the patients with Type II Diabetes Mellitus to health-
promoting behaviors in terms of:
2.1. health responsibility behaviors;
2.2. medication adherence behaviors;
2.3. dietary behaviors; and
2.4. exercise behaviors?
3. What were the health outcomes of the patients with Type II Diabetes Mellitus in
terms of:
3.1. body mass index;
3.2. lipid profile;

3.3. fasting blood sugar; and
3.4. glycosylated hemoglobin A1c?
4. Which factor predicted the health outcomes of the patient with Type II Diabetes
Mellitus?
5. Based on the findings, what health promotion program can be developed?
Null Hypothesis
Ho: There is no factor that predicts the health outcomes of patients with Type II
Diabetes Mellitus.
Significance of the Study
The result of this study will benefit the following:
Patients with Type II Diabetes Mellitus. They may benefit from the result of
this study because the information will make them more cognizant about their illness and
will give them a better understanding on the importance of their treatment regimen.
Health Care Providers. This study may aid the health institutions, medical and
allied practitioners, and nurses to plan more attainable goals for the patients with
Diabetes Mellitus. Also, this can facilitate the improvement of the patient’s health
outcomes.
Health Policy Makers. This study may help them to further develop a standard of
care to support the needs of the diabetic patients.
Non-government Organizations. This study may aid the local and international
non-government organizations to establish a community support group of among the
diabetic patients and to help conduct concrete researches on adjuvant or alternative
treatments on diabetes mellitus.
Department of Health. This study may help the officials, the rank and files of the
Department of Health to further develop health promotion programs in order to
strengthen the preventive campaign against diabetes mellitus and may aid them to
educate the public who are already affected with diabetes mellitus on the other well-
studied treatment modalities on such disorder.
The Researcher. The researcher as being part of the health care providers, this
study may aid him to develop effective ways to promulgate health promotions.
Future Researchers. This study may enhance the knowledge and skills for future
purposes for the improvement of the nursing practice for the regimen of care of diabetes
mellitus in the hospital and even in the community.

DEFINITION OF TERMS
To have better understanding of this study, the following were operationally
defined by the researcher:
Adherence level to health-promoting behaviors refers to the degree of
collaborative involvement of the patient with the healthcare provider in the treatment of
care to produce therapeutic results.
Health-responsibility behaviors refer to the patient’s key role in self-care
management in adherence to treatment regimen.
Medication adherence behaviors refer to the medicines prescribed by the health
care provider which may help to control the patient’s blood glucose and lipid levels.
Dietary behaviors refer to the nutritional intake of the patients advised by the
health care provider which may help to improve or maintain the optimal health condition.
Exercise behaviors refer to the physical activity which may help to enhance or
maintain the physical fitness and overall health and wellness of the patients.
Health outcomes among patients with Type II Diabetes Mellitus refer to the
change of health status of the patients in adherence to health-promoting behaviors.
Body mass index refers to the body measurement to determine the patient’s
thickness or thinness using the weight and height.

Lipid profile refers to the diabetic control measure to identify the average amount
of blood lipids while the patients are refrained from eating, and drinking any liquids for
the minimum of eight hours.
Fasting blood sugar refers to the diabetic control measure to identify the average
amount of blood glucose while the patients are refrained from eating, and drinking any
liquids for the minimum of eight hours.
Glycosylated hemoglobin A1c refers to the diabetic control measure to identify
the average amount of blood glucose over prolonged periods of time.
Predictors of health outcomes refer to the determinant factors that can affect the
patient’s health outcomes.
Profiles of the patients with Type II Diabetes Mellitus refer to the brief
biography of the patient diagnosed with chronic metabolic disorder in terms of personal
factors, treatments as perceived barriers to action and situational influences.
Patient with Type II Diabetes Mellitus refers to the patient diagnosed with
chronic metabolic disorder characterized with high blood sugar due to relative lack of
insulin or insulin resistance and receives a medical care treatment of such disorder.
Personal factors refer to the patient’s characteristics such as age, sex and etc. that
define the nature of patient’s behaviors.
Treatments as perceived barriers to action refer to the patient’s treatment of
care as the anticipated possible impediments on the achievement of positive health
outcomes.
Situational influences refer to the internal or external stimuli which can directly
affect the patient’s cognition towards achieving positive health outcomes.

Chapter II
REVIEW OF RELATED LITERATURE AND STUDIES
This chapter presents related literature and studies relevant to the study on the
predictors of health outcomes among patients with Type II Diabetes Mellitus. Related
literatures are provided information taken from the reliable resources such as journals,
books, and government and non-government organizations website. Related studies are
the previous studies conducted by the several researchers to explore and examine the
variables being studied. Some of the variables used in the previous studies are the same
variables being used in this present study. However, this present study will further
examine the predictors of health outcomes among diabetic patients. Hence, this will help
the present study to determine of what is not yet known and unknown.
Though diabetes mellitus cannot be cured, this chronic disease usually requires a
combination of therapies including adherence to health-promoting behaviors such as
prescribed maintenance blood glucose-regulating drugs, prescribed diet, regular exercise
and regular blood glucose self-monitoring in order to prevent the progression of diabetes-
related complications. Therefore, health care providers need effective ways to develop,
implement and support health promotions among diabetic individuals.
However, the most important thing than the medical management prescribed by
the health care providers is the patients’ key role in the self-care management. On a daily
basis, patients have to take responsibility for a large number of behavioral choices and
activities to manage their condition, predominantly outside the healthcare setting (Jarvis

et al., 2009). The choices that patients make during daily life have a greater impact on
health outcomes than those made by the health care providers. Once patients are outside
the healthcare setting, they themselves are in control. They decide whether or not to
implement recommendations in their daily life (Funnell et al., 2004).
Personal Factors
According to Nola Pender’s Health Promotion Model, personal factors are
defined as those distinguishing characteristics, which might affect behavior. It
categorized as biological, psychological, or socio-cultural factors (Tomey & Alligood,
2002). The following personal factors used in this study were age, sex, education, civil
status, occupation, financial status, length of disease diagnosis, perceived health status
and body measurements.
Age. Age can affect the diabetes treatment care regimen, especially in older
individuals. Older diabetic individuals are often have poor financial status, experience
higher frequency of social isolation and depression, and are often more susceptible to
hypoglycemic episodes (Sinclair, 2006). Age is also associated with worsening of
diabetic-related complications such as diabetic retinopathy, nephropathy and neuropathy.
This can cause to be more challenging for the older diabetic individuals on their self-
management.
Recent epidemiological studies have shown a clear relationship between age and
prevalence of Type II Diabetes Mellitus in the United States. Approximately 11% of
individuals aged 65 years and older and 6% of those aged 45 to 64 years have Diabetes
Mellitus, while only 1.5% among those aged 18 to 44 years is affected by this chronic

disease. At the same time, younger age groups are being diagnosed with Type II Diabetes
Mellitus (Harris, 1998).
Sex. Health behaviors are dynamically different between men and women. While
most studies have found that men are more physically active than women. Women’
exercise patterns are more health-promoting and sustainable relative to those of men
(Dean, 1989). Women and men also differ in health care utilization, with men generally
utilizing fewer health services (Courtenay, 2000). Although women are more likely to
seek preventive care, extensive research has documented sex disparities in the care that
men and women receive (Bird et al., 2007).
Educational Attainment. The associations between educational attainment and
health behaviors are particularly important in Diabetes Mellitus, given the critical role of
health behaviors, including diabetes self-care management and health-related lifestyle
(Mirowsky, 1998).
According to American Medical Association (1999), functional health literacy is
the ability to read and understand the prescription bottles, appointment slips, and other
health-related materials of which will be required to successfully function as a person.
Functional health literacy may mediate the relationship between low financial and health
status (American Medical Association, 1999). Lower educational attainment is strongly
associated with worse health literacy (Baker et al., 1998) and inadequate health literacy
has been linked to poorer health status (Street et al., 1993). Diabetic individuals who have
inadequate or marginal literacy are less likely to know the hypoglycemic symptoms
(Williams, 1998) and they have higher results of glycosylated hemoglobin A1c
(Schillinger, 2002).
Financial Status. In 2012, nearly 1.5 million deaths were directly caused by
Diabetes Mellitus and over 80% of Diabetes Mellitus deaths were come from in low- and
middle-income countries (World Health Organization, 2012). The influence of wealth on
healthcare access and utilization of healthcare services affects the individual’s adherence
to health promoting behaviors. Even within publicly and universally accessible systems,
there is evidence that individuals from lower financial groups have impaired access to
care reflected in longer wait times and fewer referrals to specialist care (Dunlop et al.;
2002). This might contribute to the observation of worse health outcomes, such as the
increased rate of diabetic-related complications (Booth et al., 2003).
According to the study of Rabi and colleagues (2006), they explored the
association between financial status with prevalence and utilization of diabetes care
services. Their findings showed that low income earners have higher prevalence of
Diabetes Mellitus than those high income earners. In another study conducted, only 30%
were treatment regimens compliant and the non-compliant were greater among groups
belonging to the lower socio-economic status (Shrivastava et al., 2013).
Length of Disease Diagnosis. According to the study conducted by Rhee and
colleagues (2005) and Lee and colleagues (2009), they explored the relationship between
personal factors and glycemic control, which was defined as glycosylated hemoglobin
A1c levels.
Rhee and colleagues (2005) explored the relationship between age, length of
diabetes diagnosis, and glycosylated hemoglobin A1c levels and the study obtained
significant results. The length of diabetes diagnosis was found to be positively related to
glycosylated hemoglobin A1c level. The longer the diagnosis the higher the glycosylated

hemoglobin A1c level. Age was negatively related to glycosylated hemoglobin A1c level,
indicating that the older the individual the lower the glycosylated hemoglobin A1c level.
Conversely, Lee and colleagues (2009) explored the relationship between the
same variables (age, length of diabetes diagnosis, and glycosylated hemoglobin A1c
levels) but no significant relationship was found. The Rhee and colleagues study had a
sample size of 1,560 whereas the Lee and colleagues study only had a sample size of 55.
Perceived Health Status. Perceived health is a subjective assessment that people
make about their own health state and it is an indicator of over-all health status (European
Community Health Indicators and Monitoring, 2010). It is included as one of the World
Health Organization (WHO) health targets. Perceived health status is not a substitute for
more objective health outcomes but rather complements them (The European
Commission, 2011). Perceived health status accords well with objective health status
(Unden et al., 2001).
According to Mitchell and colleagues (2004) study, they explored the relationship
between perceived health status, blood glucose self-monitor, and glycosylated
hemoglobin A1c levels but no significant relationship was found between these variables.
Another study conducted by Vince and colleagues (2004), they explored the relationship
between personal factors and adherence to blood glucose self-monitor. The personal
factors of age, length of diabetes diagnosis, and perceived health status were included. No
significant relationship was found between these personal factors and adherence to blood
glucose self-monitor.
Perceived Barriers to Action
According to Nola Pender’s Health Promotion Model, perceived barriers to action
are defined as anticipated, imagined, or real blocks and personal costs of undertaking a
given behavior (Tomey & Alligood, 2002). The perceived barriers to action used in this
study were too many treatments to manage.
There are a number of potential barriers to self-management. People may not be
able to access the information, resources or services that will enable them to develop their
self-management skills, or the actual services and information may not be available.
Physical barriers include the nature of their condition or conditions where people have
different needs. Financial or logistical barriers include physical limitations of access to
services, time and locations, financial cost, local availability of services and ongoing
support once people have had self-management training or guidance. System barriers
include conflicting advice or a lack of collaborative working between healthcare social
care professionals in providing joined-up information, services and ongoing support for
self-management (Diabetes UK, 2009).
Perceived barriers to action have an important role in the self-care process among
diabetic individuals. Important barriers are non-awareness of health nutritional program,
lack of social support and self-care management perception (Nagelkerk et al., 2006).
According to Rothman and colleagues (2008) study, they showed inappropriate diet and
sport habit among diabetic patients were related with perceived barriers. In the study of
Glasgow and colleagues (2001), there is a significant but reverse relationship between
perceived barriers to action and self-care behaviors.
Perceived barriers to action have been associated with lower rates of adherence to
a variety of self-care regimens including diet, exercise, blood glucose self-monitor, and

medication adherence behaviors (Aljasem et al., 2001). The increased impact of these
barriers, in turn, may have longer reaching implications, including influencing metabolic
control and overall functioning. In one study, greater reported frequency of barriers to
general diabetes self-care among Type I and II diabetic patients was associated with
higher glycosylated hemoglobin A1c levels, demonstrating poorer metabolic control and
increased likelihood complications (Mollem et al., 1996).
According to Wen and colleagues (2004) study, they showed as perceived barriers
to action among their research groups increase, prescribed physical activity and following
nutritional diet increase. Koch (2002) study indicated a negative significant relationship
between perceived barriers to action and self-care behaviors. Corina (2004) study showed
as perceived barriers to action increase, a significant decrease happens in diabetic self-
acre action. These were the same results seen in both Karter and colleagues (2000) and
Adams and colleagues (2003) studies.
According to the study of Nagelkerk and colleagues (2006), they provided
examples of common barriers to diabetes self-care management. Frequently reported
barriers were time constraints, limited social support, limited coping skills, lack of
knowledge related to diet management, helplessness and frustration from lack of
glycemic control, and continued disease progression despite of treatment adherence.
Although some of these barriers may appear static and not likely to change and many of
these perceived barriers to action can vary in intensity from day to day.
In spite of different studies, which demonstrated reverse and significant
relationship between self-care behaviors and perceived barriers to action, one study did
not receive this negative correlation (Gillibrnad et al., 2006). In fact, according to Janz &

Becker (1984) study, in a review of the general medical literature, concluded that the
increased presence of perceived barriers to treatment was consistently reported as the
strongest predictor of health action.
Situational Influences
According to Nola Pender’s Health Promotion Model, situational influences are
defined as those personal perceptions and cognitions of any given or context that can
facilitate or impede behavior. It includes perceptions of options available, demand
characteristics, and aesthetics features of the environment in which a given health-
promoting behavior is proposed to take place. It may have direct or indirect inlfuences on
health behavior (Tomey & Alligood, 2002). Situational influences used in this study were
the diabetes-related emotional distress.
Diabetes-related emotional distress can be defined as a range of emotional
responses and reactions to life with diabetes, especially those related to the treatment
regimen and self-care demands. It is part of a person’s experience of managing diabetes
and its treatment in the social context of family and health-care personnel (Fisher et al.,
2012; and Polonsky et al., 2005). The under recognition of emotional problems, such as
depression, anxiety, and diabetes-specific emotional distress, has been reported (Pouwer
et al., 2006), and when such concerns are recognized, problems might be identified as
depression, even in patients whose problems are directly related to diabetes and its
treatment related to diabetes and its treatment (Gonzales et al., 2011).
The ability to self-manage also includes how people are supported by peers,
family and care givers. The provision of emotional and psychological support should be
an integral part of a diabetes service. Emotional and psychological needs of a person with
diabetes have to be properly assessed in partnership with the person as part of the care
planning process. It is important that people are made aware of the support available, so
that they are able to choose if and when they need to access it (Diabetes UK, 2009).
Family relationships play a significant role in diabetes care management. Studies
have demonstrated that low levels of conflict, high levels of cohesion and organization,
and good communication patterns are linked with better treatment adherence (Delameter
et al., 2001). Higher levels of social support, specifically the diabetes-related support
from partners and their significant others are linked with better treatment adherence
(Glasgow et al., 1998). Social support serves as to buffer the adverse reactions of stress
on diabetes care management (Griffith et al., 1990).
Poor stress management and coping mechanism have been linked with more
adherence problems (Peyrot et al., 1999). Diabetes-related emotional distress such as
anxiety, depression, and eating disorders has also been associated with worse diabetes
care management in both young and adult diabetic population groups (Delametrer et al.,
2001). According to the recent Diabetes Attitudes, Wishes and Needs Study (2001)
initiated by Novo Nordisk, the study showed that a significant number of diabetic patients
have poor psychological well-being and those health care providers handling them
reported that there psychological problems adversely affected the treatment adherence
(Peyrot et al., 2005).
Depression may exert its effect through poor self-care behaviors such as over-
eating, not exercising, or failing to keep medical appointments (Trief, 2007). The over-all
depression rate in people with chronic illnesses is 20% to 70% paralleled to the estimated
5% seen in the general population group. The incidence of depression in diabetic

individuals has been approximately estimated to 25% (Madden, 2010). Identifying and
treating depression in Diabetes Mellitus is strongly recommended (Trief, 2007). One of
the issues linked with Diabetes Mellitus is that many individuals are not clinically
depressed but still experience feelings that are associated to depression in the course of
living with their chronic disease. This state is sometimes referred to as diabetes-related
emotional distress, and is associated to depression but not suffice to qualify a diagnosis of
depression (Solowiejczyk, 2010).
Depression may affect the communication with healthcare providers, self-care
management behaviors, utilization of healthcare services, and metabolic control. In a
study conducted by Ciechanowski and colleagues (2000), among diabetic individuals
with more depressive symptoms were found to have higher rates of non-adherence to oral
anti-diabetes medications than those with fewest symptoms, with the results of 15% and
7% respectively. A meta-analysis study revealed a positive correlation between
depression and glycosylated hemoglobin A1c levels (Lustman et al., 2000). Though, it is
not known whether the treatment of depression is linked with better Diabetes Mellitus
management.
According to the study of Fisher and colleagues (2012), they found non-linear
relationships of diabetes-specific emotional distress with glycosylated hemoglobin A1c,
diet, self-efficacy, and physical activity in two samples of persons with Type II Diabetes
Mellitus, with stronger relationships for lower levels of diabetes-specific emotional
distress.
Health-Promoting Behaviors

According to Nola Pender’s Health Promotion Model, health-promoting behavior
is defined as endpoint or action outcome directed toward attaining positive health
outcomes such as optimal well-being, personal fulfillment, and productive living (Tomey
& Alligood, 2002). The following health-promoting behaviors used in this study were
health responsibility, medication adherence, dietary and exercise behaviors.
In spite of the remarkable success in improving the lives of those living with
diabetes mellitus with technological innovation in biomedical sciences, the management
of Type II Diabetes Mellitus lies largely with those with diabetic individuals. It includes
the practices that must be carried out by the patients themselves. Such practices include
eating a healthy diet, performing physical activity, taking prescribed medications, self-
monitoring of blood glucose level, regular clinic appointments, and stress management,
among other practices (American Diabetes Association, 2002).
There are seven essential self-care behaviors in diabetic individuals which predict
the good health outcomes. These are healthy eating, being physically active, self-
monitoring of blood glucose level, compliant with prescribed medications, good problem-
solving skills, healthy coping skills, and risk reduction behaviors. All these seven
behaviors have been demonstrated to be positively associated with good glycemic
control, reduction of diabetic-related complications, and quality of life improvement
(Shrivastava et al., 2013).
Adherence to the prescribed maintenance blood glucose-regulating drugs, blood
glucose self-monitoring, prescribed diet, and regular exercise are often identified as
health-promoting behaviors. Diabetic individuals are expected to follow a multifaceted
set of behaviors to manage their chronic disease on a daily basis. These actions include

positive lifestyle behaviors engagement such as following a meal plan, do an appropriate
physical activity, taking prescribed medications, self-monitoring blood glucose levels,
responding to and self-treating diabetes-related symptoms, following foot-care
guidelines, and seeking individually appropriate medical care for Diabetes Mellitus or
other health-related problems (Shrivastava et al., 2013).
Health-responsibility behaviors. Successful self-care management requires
knowledge about the condition, how it needs to be treated and what needs to be done. The
key of self-care management activities specific to diabetes care and living with Diabetes
Mellitus are: (1) managing the relationships between food, activity and medications; (2)
self-monitoring of blood glucose, blood pressure and having retinal screening carried out;
(3) targeting goals tailored to individual need, for example around foot care, weight loss,
injection technique and self-monitoring activities; (4) applying sick day rules when ill, or
what to do if going into hospital; (5) understanding diabetes, what care to expect and how
to access services; (6) managing acute complications such as hypoglycemia and
hyperglycemia; and (7) understanding legislative issues such as those related to
employment and driving (Diabetes UK, 2009).
Successful control of diabetes mellitus requires lifelong adherence to multiple
self-management activities in close collaboration with the health care professionals. Lack
of adherence to such activities has been revealed to be linked with negative health
outcomes. For instance, prescription refill adherence to Diabetes Mellitus medications
correlates with improved glycosylated hemoglobin A1c results (Schectman et al., 2002).
Blood glucose self-monitoring is a cornerstone of Diabetes Mellitus management that can
warrant patient participation in specific glycemic controls achievement and maintenance.

It has been utilized for over 25 years with current technological innovations making the
procedure very easy to practice. Research has exhibited that higher blood glucose self-
monitoring practice is linked with glycemic control improvement. In spite of the
technology advancement, however, patients often do not adhere well to this diabetes care
regimen (Delamater, 2008).
Daily blood glucose self-monitoring is believed to be essential for the diabetic
patients under treatment to detect asymptomatic hypoglycemia and to guide the patients
and healthcare providers’ behaviors toward reaching the adequate blood glucose control
(Harris, 2001). Blood glucose self-monitoring provides detail about current glycemic
status and assessment of current therapy including modifications in medication, diet, and
exercise in order to attain the optimal glycemic control (Shrivastava et al., 2013)
Among diabetic patients treated with insulin and either oral medications or diet
and exercise, only 39% and 5% respectively were adhered to daily blood glucose self-
monitoring of at least one blood glucose check per day (Harris et al., 2001). According to
Delamater (2008) study, blood glucose self-monitoring adherence between diabetic
patients treated with insulin and either oral medications or diet and exercise was 70% and
64% respectively and appointment keeping adherence was 71% and 72% respectively.
Medication adherence behaviors. The goal of the medical treatment is primarily
to save life and alleviate symptoms. Secondary goals are to prevent long term diabetic-
related complications and, by eliminating various risk factors, to increase longevity.
Insulin replacement therapy is considered to be one of the cornerstones for the patients
with Type I Diabetes Mellitus while diet and lifestyle modifications are for the treatment

and management of Type II Diabetes Mellitus patients. Oral hypoglycemic agents are
also useful in the treatment of Type II Diabetes Mellitus (Bastaki, 2005).
Diabetes progression can be prevented by adequate glycemic control (Funnell, 2000).
However, unfortunately, diabetic individuals often do not follow their prescribed glucose-
regulating regimen. Considering that 95% of Diabetes Mellitus treatment is by self-care
management (Funnell, 2004), non-adherence to treatment results in significant increase of
the diabetes progression, higher costs to the healthcare system, and frustration in both
patients and healthcare providers.
The results from the study of Diabetes Attitudes, Wishes, and Needs (DAWN)
conducted by Novo Nordisk, the study showed patient-reported medication adherence
rates between Type I and Type II Diabetes Mellitus were 83% and 78% respectively
(Delamater, 2008). Another study using a large national sample of patients with Type II
Diabetes Mellitus showed that only 24% of insulin-treated patients, 65% of oral
medications-treated patients, and 80% of those treated by both diet and exercise alone
either never practiced blood glucose self-monitoring or did so less than once a month
(Harris et al., 2001). Two studies showed that adherence to oral medications in patients
with Type II Diabetes Mellitus were 53% and 67% respectively when measured by
electronic monitoring (Delamater, 2008).
Dietary behaviors. Dietary management is considered to be one of the
cornerstones in treatment of Diabetes Mellitus. It is based on the adherence of healthy
diet behaviors in the context of social, cultural, and psychological influences on food
choices (Ekore et al., 2008). Dietary practice refers to patients’ food intake selections
based on the diabetes nutrition education that provides importance on low fat and sodium

intake, and high fiber intake (Shamsi et al., 2013). Several studies have shown that
healthy diet behaviors could lead to significantly lower glycosylated hemoglobin A1c
levels among diabetic patients (American Diabetes Association, 2008).
Patients newly diagnosed with Type II Diabetes Mellitus have similar diet
behaviors compare to general population groups. Both external and emotional diet
behaviors are linked with high-energy intake and controlled diet behavior with low-
energy intake upon diagnosis. Women with high scores for emotional diet behavior were
seemed to be less able to make initial dietary changes after being diagnosed with
Diabetes Mellitus and having received dietary advice by healthcare providers (Laar et al.,
2006).
Moreover, both external and emotional diet behaviors were linked with increased
energy and fat intake. On the other hand, controlled diet behavior displayed an inverse
relationship between energy and fat intake. External diet behavior, but not emotional diet
behavior, revealed a significantly relationship with a decrease in energy intake in women
and found no statistically significant relationships between diet behavior which was
measured upon diagnosis and changes in energy and fat intake between diagnosis and
four years (Laar et al., 2006). Diet behaviors adherence rates between Type I and Type II
diabetic patients were 39% and 37% respectively (Delamater, 2008).
According to Plotnikoff and colleagues (2009) study, they explored the
relationship between dietary behaviors, body mass index, and exercise. A significantly
relationship was found for both body mass index and exercise for patients who reported
more fruit and vegetable intake. Dietary behavior practice was associated with lower
body mass index and an increase in frequency of physical activity. This study showed
that adherence to dietary behaviors can be related with another health-promoting
behaviors and health outcomes. Study demonstrated that the three types of diet behaviors
distribution including energy fat intake at diagnosis, changes in energy and fat intake
between diagnosis, and both eight weeks and four years were similar in patients with
Type II Diabetes Mellitus and the general population groups.
Exercise behaviors. Exercise has long been considered as essential component of
diabetes care management. Diabetes Mellitus Specialists have established exercise as one
of the four cornerstones of health-promoting behaviors, along with medication, diet and
blood glucose self-monitor. Exercise appears to support in the visceral fat loss. More
recent study suggested that exercise may exert favorable effects on emerging vascular
disease risk factors. Exercise may also play a protective role by increasing patient
resilience to the emotional stress and depression often experienced with Diabetes
Mellitus care management (Zecker, 2004). Irrespective of weight loss, regular physical
activity engagement has beed exhibited to be related with health outcomes improvement
among diabetic individuals. The National Institutes of Health and the American College
of Sports Medicine (NIHACSM) recommend that all adults including those with Diabetes
Mellitus should engage in regular physical activity (Shrivastava et al., 2013).
A weekly 150-minute moderate-intensity exercise can improve glycemic control.
These exercises include cardiopulmonary function-improving activities such as brisk
walking, biking, badminton, tai-chi, and aerobics mediated by repeated exercise
involving large muscle groups (Haskell et al., 2007).
Another study by Diedrich and colleagues (2010), they explored the exercise
program outcomes on weight, body fat, glycosylated hemoglobin A1c levels, and blood

pressure. The participants who completed the program showed a significantly decrease in
weight, body fat, glycosylated hemoglobin A1c levels, and in their diastolic blood
pressure. The participants also showed an increase in their daily steps as indicated by a
pedometer. This study showed that the exercise behaviors can be related with the health
outcomes including glycosylated hemoglobin A1c levels, and the loss of weight and body
fat could be interpreted as an improvement in the health outcome of body mass index.
The exercise behaviors adherence rates between Type I and Type II diabetic patients
were 37% and 35% respectively (Delamater, 2008).
Moreover, in a study conducted by Castillo and colleagues (2010), they explored
the effect of a diabetes empowerment education program on diet, exercise, blood glucose
self-monitoring, depression, and glycosylated hemoglobin A1c levels. A significant effect
was seen on all the variables from the diabetes empowerment program. A significantly
increased in dietary, exercise, and blood glucose self-monitor behaviors were noted while
a significantly decreased in reported depression and glycosylated hemoglobin A1c levels
were seen.
According to Vallis and colleagues (2005) study, they explored the effect of the
diabetes management education program on blood glucose self-monitor, diet, exercise,
and glycosylated hemoglobin A1c levels. A significant effect was seen on all the
variables from the diabetes management education program. A significantly increased in
blood glucose self-monitoring, dietary, and exercise behaviors were noted while
significant decreases in glycosylated hemoglobin A1c levels were seen.
Health Outcomes

Treatment for Diabetes Mellitus involves restoring blood glucose to or near
normal levels in all patients. The American Diabetes Association (ADA) recommends a
treatment target for diabetes that includes a glycosylated hemoglobin A1c (HbA1c) level
less than 7% and a fasting blood sugar (FBS) of less than 120 mg/dl (American Diabetes
Association, 2000). Treatment for Type II Diabetes Mellitus is designed to maximize the
effect of endogenous insulin by decreasing insulin resistance (American Diabetes
Association, 2000). However, significant patient’s key role in self-management is
necessary to achieve the positive overall health outcomes. The following health outcomes
used in this study were body mass index (BMI), lipid profile, fasting blood sugar (FBS)
and glycosylated hemoglobin A1c (HbA1c).
Body Mass Index. Body Mass Index (BMI) is an accurate indicator of fat in
adults. The most commonly used BMI is Quetelet’s Index, which is obtained by dividing
weight in kilograms by height in meters squared (Dillon, 2007). According to the
National Institutes of Health (NIH) interpret BMI values for adults with one fixed
number, regardless of age or sex, using the following guidelines: (1) underweight: below
18.5; (2) normal weight: 18.5 to 24.9; (3) overweight: 25.0 to 29.9; and (4) obese: more
than 30 (Dillon, 2007).
Nearly 90% of individuals with Type II Diabetes Mellitus are overweight or
obese. Both body mass index (BMI) and body fat distribution are considered as strong
predictors of obesity-related health risks, especially the Type II Diabetes Mellitus. The
American Diabetes Association has stated that modest weight loss and reduced energy
intake will help the insulin-resistant individuals to improve their glycemic control
(Boucher et al., 2007).
Achievement of the ideal body mass index has been recommended among
diabetic individuals. Adherence to both diet and exercise behaviors have been considered
to contribute weight loss, which reduces the body mass index (Franz, 2007). Even though
the patient is still considered as overweight, as little as 5% to 10% of weight loss from the
initial weight can help to prevent the weight-related complications such as hypertension,
dyslipidemia, and Type II Diabetes Mellitus. However, weightwatchers may not be
satisfied with such modest goals and sometimes conclude that a desirable weight loss is
unachievable (Kazaks & Stern, 2003). According to Franz (2007) study, he stated that
although a reduction of body mass index has been linked with an improvement in
Diabetes Mellitus is still unclear if the weight loss itself is linked with reduction in
glycosylated hemoglobin A1c levels or if it is from the dietary changes of a decrease in
total energy intake.
Weight loss of more than 3% from the initial weight was linked with glycemic
control improvement in patients who are newly treated for Type II Diabetes Mellitus.
Anti-diabetics medicines associated with weight loss or neutrality were associated with
greater weight loss and glycosylated hemoglobin A1c goal attainment and may facilitate
efforts to co-manage weight and blood sugar in the ambulatory-care setting (McAdam et
al., 2014).
Diabetic control measures. The ideal of diabetic control was mainly assessed
by measuring fasting blood sugar (FBS), glycosylated hemoglobin A1c (HbA1c), blood
pressure and low density lipoprotein-cholesterol (LDL-C) (American Diabetes
Association, 2008). Reduced incidences of diabetes-related complications have been
reported when blood glucose, blood pressure and blood lipid are well controlled
(American Association of Diabetes Educators, 2008).
Lipid abnormalities are common in people with Type II Diabetes Mellitus. Insulin
resistance and central obesity are two closely linked factors that are important in
determining the additional lipid abnormalities found in Type II Diabetes Mellitus
(Brunzell & Hokanson, 1999). The role of insulin resistance in the pathogenesis of Type
II Diabetes Mellitus was recognized by Himsworth (1936) over 60 years ago. According
to Vague (1956) study, central obesity was recognized as a risk factor for the
development of Type II Diabetes Mellitus over 40 years ago and many succeeding
studies have confirmed this relationship.
The measurement of the glycosylated hemoglobin A1c (HbA1c) is a target
indicator suggested by the American Diabetes Association which provides a stable and
longer term measurement of glycemic control status. A glycosylated hemoglobin A1c can
provide a reliable blood sugar history of the previous 120 days, and most accurately
reflects the previous two to three months of glycemic control status. The American
Diabetes Association recommends routine glycosylated hemoglobin A1c testing, two
times per year in diabetic patients maintaining adequate glycemic control, and more
frequently among diabetic patients who have not maintained glycemic control or who
have changed their therapeutic regimen. The American Diabetes Association
recommends the goal of therapy as a glycosylated hemoglobin A1c of less than 7%, and
recommends that treatment be re-evaluated when glycosylated hemoglobin A1c exceeds
8% (American Diabetes Association, 2008).
Overall Summary of the Review

The literature and studies mentioned above provide information on the
determinants of the two variables of this study. The reviews will help bridge the known
from the unknown and as well as give mutual benefits between the patients involved and
the healthcare providers of explaining the possible results of this study.

Chapter III
METHODOLOGY AND PROCEDURES
This chapter presents the methodology involved in the completion of this
undertaking. It describes the processes which will be used to answer the problems of the
present study.
Design
This study utilized a descriptive-analytical research design to examine the
predictors of health outcomes among patients with Type II Diabetes Mellitus. This study
described the characteristics of the population group being studied and further attempted
to describe, explain, and interpret the conditions that already existing in records and
documents.
Environment
This study was conducted in Southern Philippines Medical Center, a tertiary
government retained hospital under the Department of Health, located at the J.P. Laurel
Avenue, Bajada, Davao City. The hospital offers specialty care program in treating adult
patients with Type I and II Diabetes Mellitus and its complications. This is located at the
Mindanao Diabetes Center Clinic at the second floor of Out-Patient Preventive and Care
Center Building every Tuesday and Wednesday from eight in the morning up to twelve
noon.
The Mindanao Diabetes Center Clinic is one of the clinical services offered by the
Department of Internal Medicine. The clinic is also catering pediatric patients and is
manned by a Diabetes Nurse Educator. There are department guidelines and work
instructions followed by the Resident Physicians and Medical Specialists prior they refer
and/or enroll their patients to Mindanao Diabetes Center Clinic. The patient must be
diagnosed with Diabetes Mellitus in any type with supportive health history and diabetic
control measure results including lipid profile, fasting blood sugar and glycosylated
hemoglobin A1c. The patients are instructed when to visit the clinic without fail in as
much as once a month in order to monitor and evaluate their prognosis. Implemented
programs and activities to date are Diabetes Education and Insulin Therapy
Administration.
Respondents
The respondents were the adult patients. The eligibility criteria for the study
participation were as followed: (1) age 18 and above; (2) diagnosed of at least one year
with Type II Diabetes Mellitus; (3) no previous surgeries or hospitalizations from May
2015 up to date of scheduled interview; (4) independent and with little assistance in self-
care activities; (5) able to read, understand and sign informed consent; (6) lives in a home
setting; and (7) currently out-patient status. The non-probability convenience sampling
technique was used in this study. The researcher was allowed to select respondents based
on the above eligibility criteria. There were 128 patients with Type II Diabetes Mellitus
obtained who sought consultation within the period from July 14 to 22, 2015 and were
completely enumerated. A power analysis was performed to determine the acceptable
minimum sample size for this study.
Instruments
Health Interview Questionnaire was used to obtain secondary data from the
respondents. This was adapted-and-modified both from the National Health and Nutrition

Examination Survey (NHANES) and Diabetes Attitudes, Wishes and Needs (DAWN™)
Study.
NHANES is one of the major programs of the National Center for Health
Statistics (NCHS) by the Centers for Disease Control and Prevention (CDC). In early
1960s, the NHANES program was first initiated and had been conducted as a series of
surveys primary focusing on different population groups or health topics. The survey
became a continuous program from 1999 up to date of which it has a changing focus on
health and nutrition measurements variation to meet the emerging necessities of different
population groups (Centers for Disease Control and Prevention, 2015).
DAWN™ Study was first started in 2001 and was introduced by the Novo
Nordisk in partnership with the International Diabetes Federation (IDF) and an
international advisory panel comprising prominent diabetes mellitus specialists and
patient advocates. The first DAWN™ Study was considered to be the largest conducted
study of its kind to explore the psychosocial challenges faced by diabetic individuals and
the people helping them, and search new ways on the improvement of the Diabetes
Mellitus care. In spite of the availability of effective treatments, less than half of diabetic
populations were able to achieve adequate glycemic control; hence, the study was
initiated (Diabetes Attitudes, Wishes and Needs, 2015).
The survey instrument used in this study was divided into five parts: (1) personal
factors; (2) perceived barriers to action; (3) situational influences; (4) health-promoting
behaviors; and (5) health outcomes. The survey instrument was translated from English
version to local dialect version, Cebuano version, in order to understand by the
respondents the questions that were being asked in their own vernacular language. The
Cebuano version of the survey instrument was preliminary developed in this study. Ten
respondents who were not considered to be part of this study were involved for critiques
and pilot trials for content validity of the Cebuano version survey instrument. Reliability
test was also performed using cronbach’s alpha with a grand result of 0.892 interpreted as
very good.
The responses on the survey instrument were treated correspondingly and
interpreted based on the scale below:
Problem Areas in Diabetes Survey Parameter LimitsScale Interpretations Parameter Limits
4 Serious problem 3.21 – 4.03 Somewhat serious problem 2.41 – 3.22 Moderate problem 1.61 – 2.41 Minor problem 0.81 – 1.60 Not a problem 0 – 0.8
Adherence Level to Health-Promoting Behaviors Survey Parameter LimitsScale Interpretations Parameter Limits
5 Always/ Excellent 4.21 – 5.04 Oftentimes/ Very Good 3.41 – 4.23 Sometimes/ Good 2.61 – 3.42 Rarely/ Fair 1.81 – 2.61 Never/ Poor 1.0 – 1.8
Data Gathering Procedure
To be able to fully determine the important details and information, the researcher
devised a systematic approach to fully compensate the time involved therein.
Before the researcher carried out this study, a transmittal letter was addressed to
the Dean of Graduate School Department of University of the Visayas, the Medical
Center Chief of Southern Philippines Medical Center and as well as the informed consent
form for the respondents was considered, seeking approval to conduct this study. The
informed consent form was translated from English version to local dialect version,

Cebuano version, in order to understand by the respondents the purpose of this study in
their own vernacular language before they signed the form. Furthermore, the researcher
sought for permission to the respondents to conduct physical examination to obtain the
body measurements such as weight and height and to review the chart to obtain the
diabetic control measure results such as lipid profile, fasting blood sugar and
glycosylated hemoglobin A1c from the records of Mindanao Diabetic Center Clinic of
Southern Philippines Medical Center within the period from January to July 2015. The
researcher of this study utilized the health interview questionnaires to the respondents to
answer the following questions regarding on the profiles including personal factors, too
many treatments as perceived barriers to action and situational influences, the adherence
level to health-promoting behaviors, and the health outcomes.
Data Analysis
The gathered data were tabulated for the analysis and converted into Statistical
Package for the Social Sciences (SPSS) data files using Statistical Analysis System
(SAS) Version 21 software using the following statistical treatment: (1) frequency,
percentage and weighted mean were used for the profiles of the patients; (2) weighted
mean was used for the adherence level of the patients to health-promoting behaviors; (3)
frequency and percentage were used for the patients’ health outcomes; and (4) logistic
regression analyses were performed for the predictors of health outcomes among patients
with Type II Diabetes Mellitus.
Ethical Considerations
Approvals of the study were obtained from the Office of Dean of Graduate School
of the University of the Visayas and Integrated Research Board of Southern Philippines

Medical Center. The potential respondents were invited to listen to a short discussion of
the study objectives and all the queries were entertained right after the discussion. After
the study objectives discussed and explained very well, selected eligible respondents who
agreed to be part of the study were asked to sign two copies of informed consent form
(one for the researcher’s copy and the other one was the respondent’s copy). The
researcher obtained the informed consent at the Mindanao Diabetes Clinic Center in
Southern Philippines Medical Center. The information from this study was kept as
confidential as possible. The researcher did not reveal information about the respondents
to a third party without their consent or a clear legal reason. All transcripts and
summaries were given codes and stored separately from any names or other direct
identification of the respondents. Study information was kept in locked files at all times.
Only the researcher has the access to the files and essential need to see names had
accessed to that particular file.
The researcher did not force anybody to participate in this study researcher. If the
respondents did not decide to participate in this research, there was no further
consequence be made. If the respondents decided to participate, the respondents may stop
participating at any time and the respondents may decide not to answer any specific
question. The researcher respected the respondents’ decision if they decided to withdraw
or refuse to participate in the study, and they were not be penalized or given charges for
that matter. The data were encoded in the computer. There was no identifying
information encoded to the computer so that the information cannot be traced back to the
respondent concerned. Only the researcher had the access to the data and the interview
schedule. The interview schedules were kept at the data storage area at the Graduate

School Department of the University of the Visayas. The interview schedule kept for a
period of five years. After five years, the interview schedule disposed of by shredding.
There was no conflict of interest happen in this study. This study did not receive funds or
support from any source.

Chapter IV
PRESENTATION, ANALYSIS, AND INTERPRETATION OF DATA
This chapter presents the data collected from the different respondents of the
study. The presentation and interpretation of data are laid out following the order of the
specific problems, as follows:
Part I listed the profile of the patients with Type II Diabetes Mellitus in terms of
personal factors such as age, sex, civil status, occupation, financial status, length of
disease diagnosis, perceived health status, weight and height; treatments as perceived
barriers to action; and situational influences. The responses were based on the data
gathered from the survey.
Part II showed the adherence level of the patient with Type II Diabetes Mellitus to
health-promoting behaviors in terms of health responsibility, medication adherence,
dietary, and exercise behaviors. The responses were also based on the data gathered from
the survey.
Part III showed the health outcomes of the patient with Type II Diabetes Mellitus
in terms of body mass index, lipid profile, fasting blood sugar, and glycosylated
hemoglobin A1c. The responses were obtained through actual assessment.
Part IV showed the predictors of the health outcomes of the patients with Type II
Diabetes Mellitus. The predictors were computed using the logistic regression.
Lastly, Part V showed the health promotion program that can be developed based
on the findings of the study. The health promotion program is a matrix-based plan that
shows the pre-determined predictors with low indicators.

Profiles of the patients with Type II Diabetes Mellitus
Table 1 shows personal factors of the patients with Type II Diabetes Mellitus such
as age, sex, education, civil status, occupation, financial status, length of disease
diagnosis, perceived health status, and body measurements including weight and height.
In terms of age, more than half of the respondents were 60 years old and above,
comprising 66.4% and the majority of the respondents were females, comprising 68.8%.
Almost half of the respondents obtained at least vocational education, comprising 42.2%
and approximately half of the respondents were married, comprising 52.2%.
Approximately one-third of the respondents were retired, comprising the 29.7% and most
of the respondents live with below-average salaries, comprising 79.7%. The length of
disease diagnosis showed more than 16 years, comprising the 35.9%. Most of the
respondents perceived a good health status, comprising the 40.6%. For the weight, most
of the respondents were less than 50 kilograms, comprising 23.4%. Finally, the average
height of the respondents was within the 1.54 to 1.69 meters range (5’1 to 5’6 feet),
comprising 64.1%.
As noted, age can affect the diabetes treatment care regimen, especially in older
individuals. Older diabetic individuals are often have poor financial status, experience
higher frequency of social isolation and depression, and are often more susceptible to
hypoglycemic episodes (Sinclair, 2006). On the other hand, as noted, health behaviors are
dynamically different between men and women. Women and men also differ in health
care utilization, with men generally utilizing fewer health services (Courtenay, 2000).
Although women are more likely to seek preventive care, extensive research has
documented sex disparities in the care that men and women receive (Bird et al., 2007).
Table 1.
Personal Factors of the patients with Type II Diabetes MellitusProfile Indicators n %
Age 18 to 29 years 6 4.730 to 39 years 4 3.140 to 49 years 12 9.450 to 59 years 21 16.460 years and above 85 66.4
Sex Male 40 31.3Female 88 68.8
Educational attainment Elementary 12 9.4High School 51 39.8Vocational 54 42.2College 3 2.3Post-Graduate 8 6.3
Civil status Single 7 5.5Married 67 52.3Widow/Widower 42 32.8Annulled/Separated 12 9.4
Occupation Unemployed 33 28.5Self-Employed 31 24.2Employed 26 20.3Retired 38 29.7
Financial status Below Average 102 79.7Average 25 19.5Above Average 1 0.8
Length of disease diagnosis 1 to 5 years 9 7.06 to 10 years 29 22.711 to 15 years 44 34.4More than 16 years 46 35.9
Perceived health status Poor 12 9.4Fair 46 35.9Good 52 40.6Very Good 18 14.1
Weight Less than 50 kg 30 23.451 to 55 kg 28 21.956 to 60 kg 15 11.761 to 65 kg 28 21.966 to 70 kg 17 13.3More than 71 kg 10 7.8
Height Less than 1.53 m (5 ft.) 25 19.51.54 to 1.69 m (5’1 to 5’6 ft.)1.70 to 1.84 m (5’7 to 6 ft.)
8221
64.116.4
Note: n=128

The associations between educational attainment and health behaviors are
particularly important in Diabetes Mellitus, given the critical role of health behaviors,
including diabetes self-care management and health-related lifestyle (Mirowsky, 1998).
As noted, lower educational attainment is strongly associated with worse health literacy
(Baker et al., 1998) and inadequate health literacy has been linked to poorer health status
(Street et al., 1993). Diabetic individuals who have inadequate or marginal literacy are
less likely to know the hypoglycemic symptoms (Williams, 1998) and they have higher
results of glycosylated hemoglobin A1c (Schillinger, 2002).
As noted, the influence of wealth on healthcare access and utilization of
healthcare services affects the individual’s adherence to health promoting behaviors.
Even within publicly and universally accessible systems, there is evidence that
individuals from lower financial groups have impaired access to care reflected in longer
wait times and fewer referrals to specialist care (Dunlop et al.; 2002). According to the
study of Rabi and colleagues (2006), they explored the association between financial
status with prevalence and utilization of diabetes care services. Their findings showed
that low income earners have higher prevalence of Diabetes Mellitus than those high
income earners.
According to the study conducted by Rhee and colleagues (2005) explored the
relationship between length of diabetes diagnosis, and glycosylated hemoglobin A1c
levels and the study obtained significant results. The length of diabetes diagnosis was
found to be positively related to glycosylated hemoglobin A1c level. The longer the
diagnosis the higher the glycosylated hemoglobin A1c level.

Perceived health is a subjective assessment that people make about their own
health state and it is an indicator of over-all health status (European Community Health
Indicators and Monitoring, 2010). According to Mitchell and colleagues (2004) study,
they explored the relationship between perceived health status, blood glucose self-
monitor, and glycosylated hemoglobin A1c levels but no significant relationship was
found between these variables.
Table 2 shows treatments as perceived barriers to action of the patients with Type
II Diabetes Mellitus. The 60 respondents (46.88%) with Type II Diabetes Mellitus agreed
that there were too many treatments to manage. The least number of respondents (7.81%)
strongly disagreed on this indicator.
Table 2.
Treatments as Perceived Barriers to Action of the patients with Type II Diabetes MellitusIndicators n %
Strongly Agree 44 34.38Agree 60 46.88Disagree 14 10.94Strongly Disagree 10 7.81
Note: n=128
This may be due to financial or logistical barriers include physical limitations of access to
services, time and locations, financial cost, local availability of services and ongoing support
once people have had self-care management training or guidance. System barriers include
conflicting advice or a lack of collaborative working between healthcare social care professionals
in providing joined up information, services and ongoing support for self-care management
(Diabetes UK, 2009).
As noted, this is due to constraints of time, limited social support and coping skills, the
lack of knowledge related to diabetes management, helplessness and frustration from lack of
glycemic control, and continued disease progression despite adherence. Although some of these

Table 3.
Situational Influences of the patients with Type II Diabetes MellitusIndicators Mean Interpretation
1. Not having clear and concrete goals for your diabetes care.
1.34 Minor problem
2. Feeling discouraged with your diabetes treatment plan.
1.52 Minor problem
3. Feeling scared when you think about living with diabetes.
1.97 Moderate problem
4. Uncomfortable social situations related to your diabetes care (e.g., people telling you what to eat).
1.98 Moderate problem
5. Feelings of deprivation regarding food and meals.
1.99 Moderate problem
6. Feeling depressed when you think about living with diabetes.
1.73 Moderate problem
7. Not knowing if your mood or feelings are related to your diabetes.
1.87 Moderate problem
8. Feeling overwhelmed by your diabetes. 1.95 Moderate problem9. Worrying about low blood sugar reactions. 2.30 Moderate problem
10. Feeling angry when you think about living with diabetes.
2.16 Moderate problem
11. Feeling constantly concerned about food and eating.
2.13 Moderate problem
12. Worrying about the future and the possibility of serious complications.
2.56 Somewhat serious problem
13. Feelings of guilt or anxiety when you get off track with your diabetes management.
2.11 Moderate problem
14. Not accepting your diabetes. 1.88 Moderate problem15. Feeling unsatisfied with your diabetes
physician.1.73 Moderate problem
16. Feeling that diabetes is taking up too much of your mental and physical energy every day.
2.09 Moderate problem
17. Feeling alone with your diabetes. 2.14 Moderate problem18. Feeling that your friends and family are not
supportive of your diabetes management efforts.2.02 Moderate problem
19. Coping with complications of diabetes. 2.55 Somewhat serious problem
20. Feeling burned out by the constant effort needed to manage diabetes.
2.59 Somewhat serious problem
Grand Mean 2.03 Moderate problemNote: n=128. 3.21-4.0 Serious problem; 2.41-3.2 Somewhat serious problem; 1.61-2.4 Moderate problem; 0.81-1.6 Minor problem; 0-0.8 Not a problem
barriers may appear static and not likely to change and many of these perceived barriers can vary
in intensity from day to day.
Table 3 shows situational influences of the patients with Type II Diabetes
Mellitus. Worrying about the future and the possibility of serious complications
(Mean=2.56), coping with complications of diabetes (Mean=2.55), and feeling burned
out by the constant effort needed to manage diabetes (Mean=2.59) were all rated as
somewhat serious problem. The overall situational influences had a grand mean of 2.08,
which means that the respondents considered it a moderate problem.
It is part of a person’s experience of managing diabetes and its treatment in the
social context of family and health-care personnel (Fisher et al., 2012; and Polonsky et
al., 2005). The under recognition of emotional problems, such as depression, anxiety, and
diabetes-specific emotional distress, has been reported (Pouwer et al., 2006), and when
such concerns are recognized, problems might be identified as depression, even in
patients whose problems are directly related to diabetes and its treatment related to
diabetes and its treatment (Gonzales et al., 2011).
Thus, as observed, it became a problem when there is a little support from the
family or peers, particularly financial, emotional, and psychological support. People with
diabetes have to be assessed in partnership with the person as part of the care planning
process. Family relationships play an important role in diabetes management particularly
in communication, regimen, and low conflict levels.
The respondents worry about the future and the possibility of serious
complications (Mean=2.56), which was somewhat a serious problem. Later in life, poor
stress management and coping mechanism have been linked with more adherence
problems (Peyrot et al., 1999). Diabetes-related emotional distress such as anxiety,

depression, and eating disorders has also been associated with worse diabetes
management in both young and adult diabetic population groups (Delameter et al., 2001).
As noted, the respondents did not foresee themselves with a bright future ahead as
patients with Type II Diabetes Mellitus. Coping mechanisms were weak as it had always
been associated with problems. Most of the respondents were stressed and depressed,
thus having eating disorders. The respondents did not see themselves to be healthy in the
future and believed it was only going to get worse; thus, it posed a serious problem to
most respondents.
However, not having clear and concrete goals for diabetes care (Mean=1.34) was
a minor problem. Perceived barriers have an important role in the self-care process
among diabetic individuals. Important barriers are non-awareness of health nutritional
program, lack of social support and self-management perception (Nagelkerk et al., 2006).
Rothman and colleagues (2008) showed inappropriate diet and sport habit in these
patients was related with perceived barriers. In the study of Glasgow and colleagues
(2001), there is a significant but reverse relationship between perceived barriers to action
and self-care behaviors.
As noted, it was only a minor problem for not having clear and concrete goal for
diabetes care because respondents were already aware on how to perform self-care, diet
management and being able to know the importance of sport as part of the day-to-day
activities of the patient with Type II Diabetes Mellitus.
Adherence Level to Health-Promoting Behaviors of the patients with Type II Diabetes Mellitus
Table 4 shows the level of adherence of the patients with Type II Diabetes
Mellitus to health-promoting behaviors in terms of health-promoting behaviors had a
factor mean of 3.44 rated as very good, medication adherence behaviors had a factor
mean of 3.61 rated as very good, dietary behaviors had a factor mean of 3.59 rated as
very good, and exercise behaviors had a factor mean of 2.93 rated as good.
In spite of the remarkable success in improving the lives of those living with
Diabetes Mellitus with technological innovation in biomedical sciences, the management
of Type II Diabetes Mellitus lies largely with those with diabetic individuals. It includes
the practices that must be carried out by the patients themselves. Such practices include
eating a healthy diet, performing physical activity, taking prescribed medications, self-
monitoring of blood glucose level, regular clinic appointments, and stress management,
among other practices (American Diabetes Association, 2002).
Table 4.
Adherence Level to Health-Promoting Behaviors of the patients with Type II Diabetes Mellitus
Indicators Mean InterpretationHealth-Responsibility Behaviors
1. I visit my doctor periodically. 3.47 Very good2. I self-monitor my blood sugar daily. 3.45 Very good3. I have Lipid Profile, Fasting Blood Sugar (FBS)
and Glycosylated Hemoglobin A1c (HbA1c) examined periodically.
3.41 Very good
Factor Mean 3.44 Very goodMedication Adherence Behaviors
1. I take my prescribed medications on time daily. 3.73 Very good2. I never forget to take my prescribed
medications.3.70 Very good
3. Sometimes if I feel worse when taking the prescribed medications, I never stop taking it.
3.52 Very good
4. Even if I feel better, I still take my prescribed medications.
3.51 Very good
Factor Mean 3.61 Very goodDietary Behaviors
1. I control my diet while eating outside. 3.51 Very good2. I avoid high fat, oily and sweet foods intake. 3.55 Very good3. I am concerned with my blood sugar. 3.69 Very good4. I have a balanced diet. 3.55 Very good5. I include fruits and vegetables intake daily. 3.63 Very good
Factor Mean 3.59 Very good
Indicators Mean InterpretationExercise Behaviors
1. I do 150-minutes exercise every week. 3.01 Good2. On bad-weather days, I do exercise. 2.86 Good
Factor Mean 2.93 GoodGrand Mean 3.39 Good
Note: n= 128. 4.21-5.0 Excellent; 3.41-4.2 Very good; 2.61-3.4 Good; 1.81-2.6 Fair; 1.0-1.8 Poor
As noted, the health-promoting behavior was perceived only good because of the
practices of the patients itself. The respondents only sometimes performed exercises,
being responsible for their health, and even daily intake of medicines. Diabetic
individuals are expected to follow a multifaceted set of behaviors to manage their chronic
disease on a daily basis. The respondents must engage in a healthy lifestyle, which
includes meal planning and engaging in appropriate physical activities as well adherence
to medication. However, many respondents still did not follow steps to good health and
continually live an unhealthy lifestyle through binge eating and having a sedentary
lifestyle.
Health-responsibility behaviors had a factor mean of 3.44, which was rated very
good. Successful control of diabetes mellitus requires lifelong adherence to multiple self-
management activities in close collaboration with the healthcare professionals. Lack of
adherence to such activities had been revealed to be linked with negative health
outcomes. For instance, prescription refill adherence to diabetes mellitus medications
correlates with improved glycosylated hemoglobin A1c results (Schectman et al., 2002).
As noted, the patients with Type II Diabetes Mellitus periodically visited their physicians
for check-ups, and monitored their blood sugar on a regular basis. That is why there is
better control of the sugar in the blood to good level.
The respondents visited their doctors periodically (Mean=3.47), which was rated
very good. Successful control of diabetes mellitus requires lifelong adherence to multiple

self-management activities in close collaboration with the healthcare professionals
(Schectman et al., 2002). As noted, continuous collaboration with the healthcare
professionals can aid in the control of the sugar; thus, promoting long life to the patients
with Type II Diabetes Mellitus.
However, the respondents had lipid profile, fasting blood sugar (FBS) and
glycosylated hemoglobin A1c (HbA1c) examined periodically (Mean=3.41) was rated
very good, but the lowest among the indicators. As observed, these medical laboratory
tests were done oftentimes but the lowest in the indicator since these would require
substantial amount of money to take these tests particularly the lipid profile, which is
very expensive.
Medication adherence behaviors had a factor mean of 3.61, which was rated very
good. The goal of the medical treatment is primarily to save life and alleviate symptoms.
Secondary goals are to prevent long term diabetic-related complications and, by
eliminating various risk factors, to increase longevity. Insulin replacement therapy is
considered to be one of the cornerstones for the patients with Type I Diabetes Mellitus
while diet and lifestyle modifications are for the treatment and management of Type II
Diabetes Mellitus patients. Oral hypoglycemic agents are also useful in the treatment of
Type II Diabetes Mellitus (Bastaki, 2005). As noted, the respondents wanted to live a
longer, healthy life; thus, most of the respondents got medical treatment in the event of
secondary symptoms appears.
The respondents took the prescribed medication on time daily (Mean=3.73),
which was rated very good. The results from the study of Diabetes Attitudes, Wishes, and
Needs (DAWN) conducted by Novo Nordisk, the study showed patient-reported
medication adherence rates between Type I and Type II Diabetes Mellitus were 83% and
78% respectively (Delamater, 2008). Another study using a large national sample of
patients with Type II Diabetes Mellitus showed that only 24% of insulin-treated patients,
65% of oral medications-treated patients, and 80% of those treated by both diet and
exercise alone either never practiced blood glucose self-monitoring or did so less than
once a month (Harris et al., 2001). Thus, as observed, the respondents adhered to
prescribed medication on a daily basis by following the medication pattern prescribed by
the healthcare professionals.
However, even if the respondents feel better, they still take the prescribed
medications (Mean=3.51), rated very good. As noted that this was the lowest indicator
because respondents highly regarded the medication instruction given to them by the
medical professionals by attending into detail the prescribed medication to prolong their
lives and live a healthy lifestyle.
For the dietary behaviors, it had a factor mean of 3.59, which was rated very
good. Dietary management is considered to be one of the cornerstones in treatment of
Diabetes Mellitus. It is based on the adherence of healthy diet behaviors in the context of
social, cultural, and psychological influences on food choices (Ekore et al., 2008). As
noted, respondents had control in their diet while eating outside and most of them
avoided high fat, oily and sweet food intake as well as being concerned with their blood
sugar. Most respondents had balanced diet and included fruits and vegetables in their
daily intake.
The respondents were concerned with their blood sugar (Mean=3.69), which was
rated very good. Daily blood glucose self-monitoring is believed to be essential for the

diabetic patients under treatment to detect asymptomatic hypoglycemia and to guide the
patients and healthcare providers’ behaviors toward reaching the adequate blood glucose
control (Harris, 2001). Blood glucose self-monitoring provides detail about current
glycemic status and assessment of current therapy including modifications in medication,
diet, and exercise in order to attain optimal glycemic control (Shrivastava et al., 2013). As
observed that part of medication or self-care involved checking one’s blood sugar on a
regular basis.
However, the respondents controlled their diets while eating outside
(Mean=3.51), although rated very good, was the lowest among the indicators. As noted
that respondents followed the same diet pattern even when eating outside and did not
differ with the general population (Laar et al., 2006).
For the exercise behaviors, it had a factor mean of 2.93, which was rated good.
Exercise has been considered as an essential component of diabetes management.
Diabetes specialists have established exercise as one of the four cornerstones of health-
promoting behaviors, along with medication, diet and blood glucose self-monitoring.
Exercise appears to support in the visceral fat loss. More recent study suggested that
exercise may exert favorable effects on emerging vascular disease risk factors. Exercise
may also play a protective role by increasing patient resilience to the emotional stress and
depression often experienced with diabetes management (Zacker, 2004). However, as
noted, this was only rated good as most of the respondents lived a sedentary lifestyle. The
respondents did not involve much of their time into brisk exercise.
Most respondents did 150-minute exercise every week (Mean=3.01), which was
rated good. A weekly 150-minute moderate-intensity exercise can improve glycemic

control. These exercises include cardiopulmonary function-improving activities such as
brisk walking, biking, badminton, tai-chi, and aerobics mediated by repeated exercise
involving large muscle groups (Haskell et al., 2007). As observed, inactive lifestyles of
the respondents, this really did not involve themselves in exercise like brisk walking,
biking, badminton, and others. However, respondents exercised even on bad-weather days
(Mean=2.86), rated good, was the lowest indicator. As noted, whether on good or bad
weather days, respondents did not have enough exercise.
Table 5 shows the summary of level of adherence of the patients with Type II
Diabetes Mellitus to health-promoting behaviors in terms of health-responsibility,
medication adherence, dietary and exercise behaviors. It had a grand mean of 3.39, which
was rated good.
Table 5.
Summary of Adherence Level to Health-Promoting Behaviors of the patients with Type II Diabetes Mellitus
Indicators Factor Mean InterpretationHealth-Responsibility Behaviors 3.44 Very goodMedication Adherence Behaviors 3.61 Very goodDietary Behaviors 3.59 Very goodExercise Behaviors 2.93 Good
Grand Mean 3.39 GoodNote: n=128. 4.21-5.0 Excellent; 3.41-4.2 Very good; 2.61-3.4 Good; 1.81-2.6 Fair; 1.0-1.8 Poor
Health-responsibility behaviors had a factor mean of 3.44, which was rated very
good. Successful control of Diabetes Mellitus requires lifelong adherence to multiple
self-management activities in close collaboration with the healthcare professionals. Lack
of adherence to such activities has been revealed to be linked with negative health
outcomes. For instance, prescription refill adherence to diabetes mellitus medications
correlates with improved glycosylated hemoglobin A1c results (Schectman et al., 2002).
As noted, the patients with Type II Diabetes Mellitus periodically visited their physicians

for check-ups, and monitored their blood sugar on a regular basis. That is why there is
better control of the sugar in the blood to good level.
Medication adherence behaviors had a factor mean of 3.61, which was rated very
good. The goal of the medical treatment is primarily to save life and alleviate symptoms.
Secondary goals are to prevent long term diabetic-related complications and, by
eliminating various risk factors, to increase longevity. Insulin replacement therapy is
considered to be one of the cornerstones for the patients with Type I Diabetes Mellitus
while diet and lifestyle modifications are for the treatment and management of Type II
Diabetes Mellitus patients. Oral hypoglycemic agents are also useful in the treatment of
Type II Diabetes Mellitus (Bastaki, 2005). As noted, the respondents wanted to live a
longer, healthy life; thus, most of the respondents got medical treatment in the event of
secondary symptoms appears.
For the dietary behaviors, it had a factor mean of 3.59, which was rated very
good. Dietary management is considered to be one of the cornerstones in treatment of
Diabetes Mellitus. It is based on the adherence of healthy diet behaviors in the context of
social, cultural, and psychological influences on food choices (Ekore et al., 2008). As
noted, respondents had controlled in their diet while eating outside, and most of them
avoided high fat, oily and sweet food intake as well as being concerned with their blood
sugar. Most respondents had balanced diet and included fruits and vegetables in their
daily intake.
For the exercise behaviors, it had a factor mean of 2.93, which was rated good.
Exercise has been considered as an essential component of diabetes management.
Diabetes specialists have established exercise as one of the four cornerstones of health-
promoting behaviors, along with medication, diet and blood glucose self-monitoring.
Exercise appears to support in the visceral fat loss. More recent study suggested that
exercise may exert favorable effects on emerging vascular disease risk factors. Exercise
may also play a protective role by increasing patient resilience to the emotional stress and
depression often experienced with diabetes management (Zacker, 2004). However, as
noted, this was only rated good as most of the respondents lived a sedentary lifestyle. The
respondents did not involve much of their time into brisk exercise.
Health Outcomes of the patients with Type II Diabetes Mellitus
Table 6 shows the health outcomes of the patients in terms of the actual
assessment. Most of the respondents had body mass indices that were normal, comprising
73.4%; and, those who were above normal only comprised 26.6%. The lipid results of the
respondents were mostly normal, comprising 78.1%; and, those who were above normal
only comprised 21.9%. The fasting blood sugar of the respondents was mostly normal,
comprising 80.5%; and, above normal comprised 19.5%. Finally, the result in
glycosylated hemoglobin A1c showed more normal diagnoses at 53.1%; and, those above
normal resulted at 46.9% as the least.
Table 6.
Health Outcomes of the patients with Type II Diabetes MellitusIndicators N %
Body Mass Index Normal 94 73.4Above Normal 34 26.6
Lipid Profile Normal 100 78.1Above Normal 28 21.9
Fasting Blood Sugar Normal 103 80.5Above Normal 25 19.5
Glycosylated Hemoglobin A1c NormalAbove Normal
6860
53.146.9
Note: n=128

As noted, the overall health outcomes of the patients with Type II Diabetes
Mellitus were normal. Treatment for Diabetes Mellitus involves restoring blood glucose
to or near normal levels in all patients. The American Diabetes Association (ADA)
recommends a treatment target for diabetes that includes a glycosylated hemoglobin A1c
(HbA1c) level less than 7% and a fasting blood sugar (FBS) of less than 120 mg/dl
(American Diabetes Association, 2000). Treatment for Type II Diabetes Mellitus is
designed to maximize the effect of endogenous insulin by decreasing insulin resistance
(American Diabetes Association, 2000). However, significant patient’s key role in self-
management is necessary to achieve the positive overall health outcomes.
Predictor of Health Outcomes for Body Mass Index
Table 7 shows the predictors of health outcomes of the patients in terms of body
mass index. The perceived barriers to action, situational influences, health responsibility,
medication adherence, dietary, exercise, age, educational attainment, civil status,
occupation, financial status, length of disease diagnosis, and perceived health status had
p-values greater than 0.05. Thus, the aforementioned factors did not predict the health
outcomes for body mass index of the patient with Type II Diabetes Mellitus.
Table 7.
Predictor of Health Outcomes for Body Mass IndexPredictors B p Exp(B) Decision Interpretation
Personal FactorsAge 0.160 0.719 1.174 Accept Ho Not significantSex 2.740 0.022 15.482 Reject Ho SignificantEducational attainment -0.597 0.305 0.551 Accept Ho Not significantCivil status -1.001 0.142 0.368 Accept Ho Not significantOccupation 0.463 0.249 1.588 Accept Ho Not significantFinancial status 1.840 0.109 6.300 Accept Ho Not significantLength of disease diagnosis -0.924 0.147 0.397 Accept Ho Not significantPerceived health status -0.841 0.143 0.431 Accept Ho Not significantWeight 2.493 0.000 12.101 Reject Ho SignificantHeight -3.453 0.001 0.032 Reject Ho Significant

Treatments as Perceived Barriers to Action
0.420 0.388 1.522 Accept Ho Not significant
Situational Influences -0.152 0.775 0.859 Accept Ho Not significantHealth-Promoting BehaviorsHealth-responsibility behaviors 0.305 0.687 1.357 Accept Ho Not significantMedication adherence behaviors 1.561 0.073 4.762 Accept Ho Not significantDietary behaviors -1.877 0.094 0.153 Accept Ho Not significantExercise behaviors 0.080 0.918 1.083 Accept Ho Not significant
(Constant) -4.815 0.429 0.008 Accept Ho Not significantNote: Significant at p < 0.05
The BMI can be predicted using the following model: BMI = 2.740 (Sex) + 2.493
(Weight) – 3.453 (Height). Thus, if sex is female (sex=2), weight is less than 50
kilograms (weight=1), and height is between 1.54 to 1.69 meters (5’1 to 5’6 feet)
(height=2), then BMI = 2.74(2) + 2.493(1) – 3.453(2) then BMI = 1.067. Thus, BMI is
below normal (BMI=1) for a female who weighs less than 50 kilograms and whose height
is between 1.54 to 1.69 meters (5’1 to 5’6 feet).
If sex is a male (sex=1), weight is less than 50 kilograms (weight=1), and height
is less than 1.53 meters (5 feet) (height=1), then BMI = 2.74(1) + 2.493(1) – 3.453(1)
then BMI = 1.78 (approximately 2). Thus, BMI is above normal (BMI=2) for a male
patient whose weight is less than 50 kilograms and whose height is less than 1.53 meters
(5 feet).
However, sex had a p-value of 0.022, which rejected the null hypothesis. Sex was
a predictor for health outcomes for body mass index. The females were 15.48 times more
likely to become obese. Health behaviors are dynamically different between men and
women. While most studies have found that men are more physically active than women.
Women’ exercise patterns are more health-promoting and sustainable relative to those of
men (Dean, 1989). Women and men also differ in health care utilization, with men
generally utilizing fewer health services (Courtenay, 2000). Although women are more

likely to seek preventive care, extensive research has documented sex disparities in the
care that men and women receive (Bird et al., 2007). With this, as observed that since
men had more physically active lifestyle than women, and then it showed that women
tend to become more obese than men.
The weight and height had p-value of 0.000 and 0.001 respectively, which
rejected the null hypothesis. Thus, weight and height were predictors to health outcomes
for body mass index. Respondents with weights less than 50 kilograms are 12.1 times
more likely to have normal body mass index and respondents with heights between 1.54
to 1.69 meters were 0.032 times more likely to have normal body mass index. Body Mass
Index is an accurate indicator of fat in adults. Nearly 90% of individuals with Type II
Diabetes Mellitus are overweight or obese. Body Mass Index and body fat distribution,
which individuals’ weight must be proportionate to their height, are both considered as
strong predictors of obesity-related health risks, especially the Type II Diabetes Mellitus.
The American Diabetes Association has stated that modest weight loss and reduced
energy intake will help insulin-resistant individuals improve their glycemic control
(Boucher et al., 2007). As noted, periodic weight monitoring could help respondents to be
more cognizant about their weight and calculated BMI changes in concordance to health-
promoting behaviors.
Predictor of Health Outcomes for Lipid Profile
Table 8 shows the predictor of health outcomes in terms of the lipid profile. The
perceived barriers to action, situational influences, health-responsibility, medication
adherence, dietary, exercise, age, sex, educational attainment, civil status, occupation,
financial status, length of disease diagnosis, perceived health status, and height had p-

Table 8.
Predictor of Health Outcomes for Lipid ProfilePredictors B p Exp(B) Decision Interpretation
Personal FactorsAge -0.169 0.593 0.844 Accept Ho Not significantSex 0.272 0.719 1.312 Accept Ho Not significantEducational attainment -0.395 0.310 0.673 Accept Ho Not significantCivil status -0.173 0.709 0.842 Accept Ho Not significantOccupation 0.200 0.516 1.221 Accept Ho Not significantFinancial status 0.821 0.268 2.272 Accept Ho Not significantLength of disease diagnosis -0.424 0.279 0.654 Accept Ho Not significantPerceived health status -0.689 0.079 0.502 Accept Ho Not significantWeight 0.713 0.002 2.041 Reject Ho SignificantHeight -1.010 0.110 0.364 Accept Ho Not significantTreatments as Perceived Barriers to Action
0.664 0.064 1.942 Accept Ho Not significant
Situational Influences -0.578 0.147 0.561 Accept Ho Not significantHealth-Promoting BehaviorsHealth responsibility behaviors -0.146 0.781 0.864 Accept Ho Not significantMedication adherence behaviors 0.055 0.919 1.057 Accept Ho Not significantDietary behaviors -0.979 0.131 0.376 Accept Ho Not significantExercise behaviors -0.011 0.981 0.989 Accept Ho Not significant
(Constant) 4.114 0.305 61.172 Accept Ho Not significantNote: Significant at p < 0.05
values more than 0.05. Thus, the aforementioned indicators did not predict the lipid
profile of the patients with Type II Diabetes Mellitus.
The lipid profile can be predicted using the following model: Lipid Profile =
0.713 (Weight).
Weight had a p-value of 0.002, which rejected the null hypothesis. Weight was a
predictor of health outcomes for lipid profile. Those who weighed more were 2.041 times
more likely to have an increase lipid profile result. Lipid abnormalities are common in
people with Type II Diabetes Mellitus. Insulin resistance and central obesity are two
closely linked factors that are important in determining the additional lipid abnormalities
found in Type II Diabetes Mellitus (Brunzell & Hokanson, 1999). The role of insulin
resistance in the pathogenesis of Type II Diabetes Mellitus was recognized by Himsworth
(1936) over 60 years ago. According to Vague (1956) study, central obesity was
recognized as a risk factor for the development of Type II Diabetes Mellitus over 40
years ago and many succeeding studies have confirmed this relationship. As noted,
periodic weight monitoring could help the respondents to be more cognizant about their
weight changes thus help to control eating habits and decrease sedentary lifestyle.
Predictor of Health Outcomes for Fasting Blood Sugar
Table 9 shows the predictor of health outcomes in terms of the fasting blood
sugar. The perceived barriers to action, situational influences, health-responsibility
behaviors, medication adherence behaviors, dietary behaviors, exercise behaviors, age,
sex, educational attainment, civil status, occupation, financial status, length of disease
diagnosis, perceived health status, and height had p-values more than 0.05. Thus, the

aforementioned indicators did not predict the fasting blood sugar of the patients with
Type II Diabetes Mellitus.
Predictor of Health Outcomes for Glycosylated Hemoglobin A1c
Table 10 shows the predictor of health outcomes in terms of glycosylated
hemoglobin A1c. The perceived barriers to action, situational influences, health-
responsibility behaviors, medication adherence behaviors, exercise behaviors, age, sex,
education attainment, occupation, financial status, length of disease diagnosis, perceived
health status, and height had p-values more than 0.05. Thus, the aforementioned
indicators did not predict the glycosylated hemoglobin A1c of the patients with Type II
Diabetes Mellitus.
Table 10.
Predictor of Health Outcomes for Glycosylated Hemoglobin A1cPredictors B p Exp(B
)Decision Interpretation
Personal FactorsAge -0.204 0.632 0.815 Accept Ho Not significantSex -1.113 0.211 0.328 Accept Ho Not significantEducational attainment -0.399 0.350 0.671 Accept Ho Not significantCivil status -1.117 0.028 0.327 Reject Ho SignificantOccupation -0.282 0.398 0.754 Accept Ho Not significantFinancial status 1.886 0.088 6.594 Accept Ho Not significantLength of disease diagnosis -0.061 0.896 0.941 Accept Ho Not significantPerceived health status -0.086 0.837 0.918 Accept Ho Not significantWeight 0.907 0.000 2.477 Reject Ho SignificantHeight -1.106 0.103 0.331 Accept Ho Not significantTreatment as Perceived Barriers to Action
0.458 0.243 1.580 Accept Ho Not significant
Situational Influences 0.387 0.352 1.473 Accept Ho Not significantHealth-Promoting BehaviorsHealth responsibility behaviors 0.344 0.568 1.410 Accept Ho Not significantMedication adherence behaviors -0.425 0.477 0.654 Accept Ho Not significantDietary behaviors -1.606 0.022 0.201 Reject Ho SignificantExercise behaviors -0.101 0.847 0.904 Accept Ho Not significant
(Constant) 8.954 0.066 7737.401 Accept Ho Not significantNote: Significant at p < 0.05

The glycosylated hemoglobin A1c can be predicted using the following model:
HbA1c = 8.954 – 1.606 (Dietary Behavior) – 1.117 (Civil Status) + 0.907 (Weight).
Dietary behavior had a p-value of 0.022, which rejected the null hypothesis.
Dietary behavior was a predictor to health outcomes for glycosylated hemoglobin A1c.
Better dietary behavior was 0.201 times more likely to improve the results for
glycosylated hemoglobin A1c. Dietary management is considered to be one of the
cornerstones in treatment of diabetes mellitus. It is based on the adherence of healthy diet
behaviors in the context of social, cultural, and psychological influences on food choices
(Ekore et al., 2008). Dietary practice refers to patients’ food intake selections based on
the diabetes nutrition education that provides importance on low fat and sodium intake,
and high fiber intake (Shamsi et al., 2013). Several studies have showed that healthy diet
behaviors could lead to significantly lower glycosylated hemoglobin A1c levels among
diabetic patients (American Diabetes Association, 2008). As noted that proper eating
habits could improve or normalize the blood glucose and may reduce the risk of diabetes-
related complications.
Civil status had a p-value of 0.028, which rejected the null hypothesis. Civil status
was a predictor to health outcomes for glycosylated hemoglobin A1c. Married
respondents were 0.327 times more likely to have better results for glycosylated
hemoglobin A1c. As observed, most of the married respondents might had strong spouse
support thus adequate glycemic control in terms of glycosylated hemoglobin A1c levels.
The weight had a p-value of 0.000, which rejected the null hypothesis. Weight
was a predictor for health outcomes for glycosylated hemoglobin A1c. Those who
weighed below 50 kilograms were 2.48 times more likely to have better results for
glycosylated hemoglobin A1c. Nearly 90% of individuals with Type II Diabetes Mellitus
are overweight or obese. Weight loss of more than 3% was linked with glycemic control
improvement in patients who are newly treated for Type II Diabetes Mellitus. Anti-
diabetics medicines associated with weight loss or neutrality were associated with greater
weight loss and glycosylated hemoglobin A1c goal attainment and may facilitate efforts
to co-manage weight and blood sugar in the ambulatory-care setting (McAdam et al.,
2014). With this, as noted, proper weight management in adherence to anti-diabetic
medications may help to improve glucose control of the respondents and thus better
glycosylated hemoglobin A1c results.

Chapter V
SUMMARY OF FINDINGS, CONCLUSION, AND RECOMMENDATIONS
This chapter presents the summary of the findings of this study, the conclusion
that was drawn from the findings, and the recommendations in the areas of theoretical
advancement and practical significance.
Summary of Findings
Most of the respondents were 60 years and above and were females with
vocational education, married, retired, with more than 16 years of diagnosis, with
perceived good health status, mostly weighing less than 50 kilograms, and were within
the 1.54 to 1.69 meters (5’1 to 5’6 feet) height range. In terms of treatments as perceived
barriers to action, 60 respondents with Type II Diabetes Mellitus agreed that there were
too many treatments to manage. Most respondents considered situational influences a
moderate problem. The respondents worried about the future and the possibility of
serious complications, coping with complications of diabetes, and feeling burned out by
the constant effort needed to manage diabetes were viewed somewhat a serious problem.
However, not having concrete goals for diabetes care and feeling discouraged with your
diabetes treatment plan were considered minor problem.
The health-responsibility behavior of the respondents was rated very good.
Oftentimes, the respondents visited their physicians periodically. Although oftentimes,
the respondents had lipid profile, fasting blood sugar (FBS) and glycosylated hemoglobin
A1c (HbA1c) examined periodically. Medication adherence behavior was rated very
good. Oftentimes, the respondents took the prescribed medication on time daily. Although
oftentimes, even if the respondents feel better, they still take the prescribed medications,
was the lowest indicator. Dietary behavior was rated very good. The respondents were
concerned with their blood sugar oftentimes. The respondents also oftentimes controlled
their diets while eating outside, the lowest in the indicators. Exercise behavior was rated
good. Most respondents did 150-minute exercise every week, which was rated
sometimes. The lowest in the indicator showed that respondents exercise even on bad-
weather days, which was rated sometimes. The body mass index, lipid profiles, fasting
blood sugar, and glycosylated hemoglobin A1c among patients with Type II Diabetes
Mellitus had normal results.
Sex was a predictor of health outcomes for body mass index and females were
more likely to become obese. Weight was also a predictor of health outcomes for body
mass index and those respondents who weighed less than 50 kilograms were more likely
to have normal body mass index. Weight was a predictor of health outcomes for lipid
profile and those who weighed below 50 kilograms were more likely to have normal
results. Dietary behavior predicted the health outcomes for glycosylated hemoglobin A1c
and those with better dietary behaviors were more likely to have better glycosylated
hemoglobin A1c results. Civil status predicted the health outcomes for glycosylated
hemoglobin A1c and those who were married were more likely to have better
glycosylated hemoglobin A1c results. Weight predicted the health outcomes glycosylated
hemoglobin A1c and those who weighed below 50 kilograms were more likely to have
better glycosylated hemoglobin A1c results.
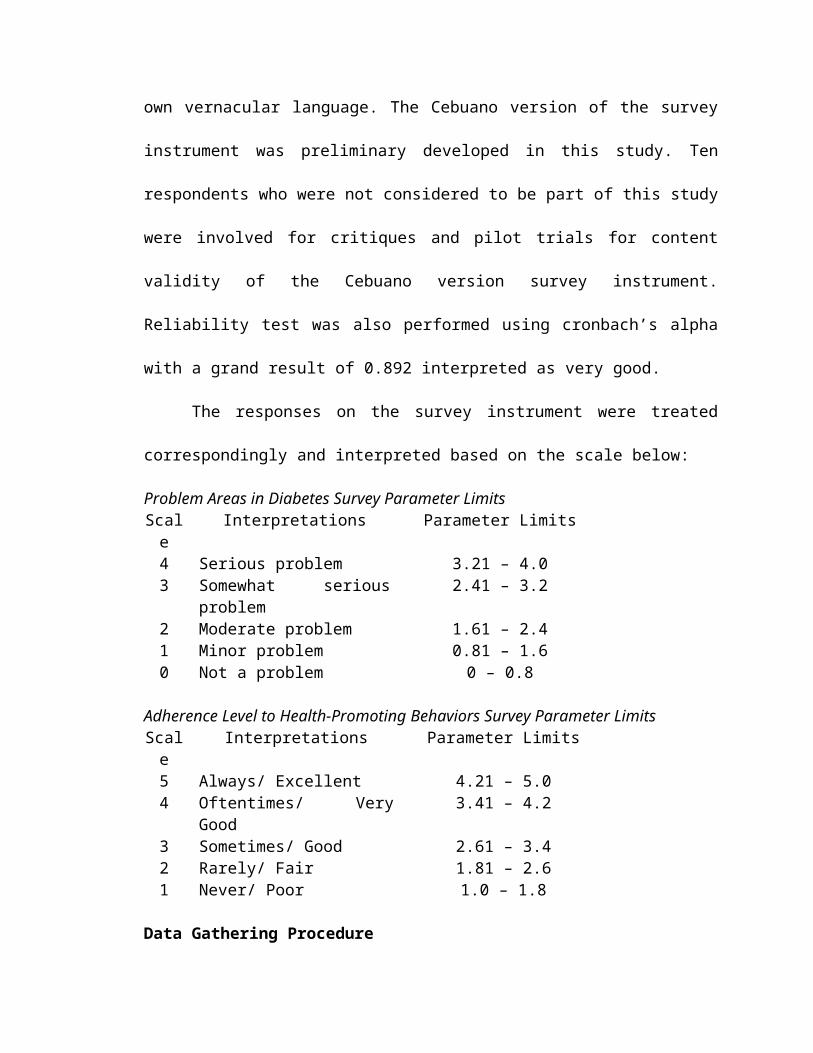
The findings of the study rejected the null hypothesis thus the factors that
predicted the health outcomes among patients with Type II Diabetes Mellitus were weight
for BMI, lipid profile and HbA1c, height for BMI, lipid profile and HbA1c, sex for BMI
and civil status and dietary behaviors for HbA1c.
Conclusions
Based on the findings of the study, it is concluded that sex, weight and height
were the predictors of health outcome for body mass index, weight was the predictor of
health outcome for lipid profile and civil status, weight and dietary behaviors were the
predictors of health outcome for glycosylated hemoglobin A1c among patients with Type
II Diabetes Mellitus.
These findings can be used to develop a health promotion program which
affirmed to the Health Promotion Model by Nola J. Pender (1996) for improving the self-
care management among patients with Type II Diabetes Mellitus in order to enhance their
over-all health outcomes.
Recommendations
Based on the findings and conclusion of the study, it is recommended that:
1. Use the health promotion program to improve and prolong the lives of the patients
with Type II Diabetes Mellitus. The patients must live a healthy lifestyle by following
proper diet management, updating his knowledge about the illness, constant contact
with a health professional, following religiously the medication prescribed by the
physician, exercising on a regular basis, and many others.

2. The health care providers must update the patients the necessary knowledge as well
help them not only for their physical needs but for emotional and psychological needs
as well.
3. The health policy makers must ensure that policies on health promotion and the
procedures for control are strictly followed and monitored.
4. The Department of Health must ensure that hospitals and clinics give the up-to-date
information on diabetes control and that they perform community-based immersion
programs in educating the locals about the disease.
5. The researcher must apply the relevant knowledge particularly to patients with
diabetes in order to control and help them attain better health.
6. The future researchers must find other means or factors not only to improve the lives
of the patients with diabetes mellitus but also to propose the following studies that
might be deemed useful in the future such as the following:
6.1. Classification and Diagnosis of Diabetes Mellitus of Glucose Intolerance;
6.2. Predictors of Care Improvement of Geriatric Patients with Diabetes Mellitus;
and
6.3. Influence of Body Fat Distribution on the Incidence of Diabetes Mellitus among
patients in Davao City.
REFERENCES

References
Adams, A.S., Mah, C. Soumerai S.B., Zhang, F., Barton M.B. & Ross-Degnan, D. (2003). Barriers to self-monitoring of blood sugar among adults with Diabetes Mellitus in an HMO: A cross-sectional study. BMC Health Service Research, 3:6.
Aljasem, L.I., Peyrot, M., Wissow, L., & Rubin, R.R. (2001). The impact of barriers and self-efficacy on self-care behaviors in Type II Diabetes Mellitus. The Diabetes Educator, 27:393-404.
American Association of Diabetes Educators (2008). Self-care behaviors. The Diabetes Educator, 34, 445-449.
American Diabetes Association (2008). Standards of medical care in Diabetes Mellitus. Diabetes Care, 32:S62-S63.
American Diabetes Association (2002). Standards of medical care for patients with Diabetes Mellitus. Diabetes Care, 25:S33-S49.
American Diabetes Association. (2000). Screening for Type II Diabetes Mellitus. Diabetes Care, 23:S20-S23.
American Diabetes Association. (2000). Tests of glycemia in Diabetes Mellitus. Diabetes Care, 23:S80-82.
American Medical Association (1999). Health literacy: Report of the Council on Scientific Affairs. Journal of American Medical Association, 281:552-7.
Baker, D.W., Parker, R.M., Williams, M.V., et al. (1998). Health literacy and the risk of hospital admission. Journal of General Internal Medicine, 13:791-8.
Bastaki, S. (2005). Review Diabetes Mellitus and its Treatment. International Journal of Diabetes and Metabolism, 13:111-114.
Bird, C.E., Fremont, A.M., Bierman, A.S., Wickstrom, S., Shah, M. et al. (2007). Does quality of care for cardiovascular disease and diabetes differ by gender for enrollees in managed care plans? Women’s Health Issues, 17:131–138.

Booth G.L., & Hux J.E (2003). Relationship between avoidable hospitalizations for Diabetes Mellitus and income level. Archives of Internal Medicine, 163(1):101-6.
Boucher, J. L., Benson, G. A., Kovarik, S., Solem, B., & Van Wormer, J. J. (2007). Current trends in weight management: What advice do we give to patients? Diabetes Spectrum, 20(3):153-158.
Brunzell, J.D. & Hokanson, J.E. (1999). Dyslipidemia of central obesity and insulin resistance. Diabetes Care, 22(3):C10-3.
Castillo, A., Giachello, A., Bates, R., Concha, J., Ramirez, V., Sanchez, C., Pinsker, E., & Arrom, J. (2010). Community-based diabetes education for Latinos. The Diabetes Educator, 36(4):586-594.
Centers for Disease Control and Prevention (2015). About National Health and Nutrition Examination Survey. Retrieved from http://www.cdc.gov/nchs/nhanes/about_nhanes.htm.
Ciechanowski, P.S., Katon, W.J. & Russo, J.E. (200). Depression and Diabetes: Impact of depressive symptoms on adherence, function and costs. Archive of Internal Medicine, 160:3278-85
Corina, G. Michael, P.R. & James, J.D. (2004). Diabetes education program use and patient-perceived barriers to attendance. Journal of Clinical Research Methods, 31:358-63.
Davao City Health Office (2010). Mortality rates of Diabetes Mellitus. Retrieved from http://davaohealth.brinkster.net/HealthStatus-2011.asp.
Dean, K. (1989) Self-care components of lifestyles: The importance of gender, attitudes and the social situation. Social Science Medicine, 29:137–152.
Delamater, A.M. (2008). Improving patient adherence. Clinical Diabetes, 24(2):71-76.
Delamater, A.M., Jacobson, A.M., Anderson, B.J., Cox, D., Fisher, L., Lustman, P., Rubin, R. & Wysocki, T. (2001). Psychosocial therapies in diabetes: report of the Psychosocial Therapies Working Group. Diabetes Care, 24:1286-1292.
Department of Health (2010). Universal Health Care of the Department of Health. Retrieved from http://www.doh.gov.ph/Overview.html.
Diabetes Attitudes, Wishes and Needs (2015). About Diabetes Attitudes, Wishes and Needs. Retrieved from http://www.dawnstudy.com/dawn-programmes/about-dawn.html.

Diabetes UK (2009). Improving supported self-management for people with diabetes. Retrieved from https://www.diabetes.org.uk/Documents/Reports/Supported_self-management.pdf.
Diedrich, A., Munroe, D.J., & Romano, M. (2010). Promoting physical activity for persons with Diabetes Mellitus. The Diabetes Educator, 36(1):132-140.
Dillon, P.M. (2007). Body Mass Index. Nursing Health Assessment: A Critical Thinking, Case Studies Approach 2nd edition, Chapter 8 Assessing Nutrition. F.A. Davis Company, Philadelphia.
Dunlop, S., Cayote, P. & McIsaac, W. (2000): Socio-economic status and the utilization of physician’s services: results from the Canadian National Population Health Survey. Social Science and Medicine, 51 (1):123-33.
Ekore, R.I, Aljay, I.O. & Ekore, J.O. (2008). Dietary Management of Diabetes: A practical approach for primary care physicians in Nigeria. Diabetes, 16:13-14.
European Community Health Indicators and Monitoring (2010). Public Health. Retrieved from http://www.healthindicators.eu/object_document/o5873n28314.html .
Franz, M.J. (2007). The dilemma of weight loss in Diabetes. Diabetes Spectrum, 20(3):133-136.
Fisher, L., Hessler, D.M., Polonsky, W.H. & Mullan, J. (2012). When is diabetes distress clinically meaningful? Establishing cut points for the diabetes distress scale. Diabetes Care, 35:259-64.
Funnell, M.M., & Anderson, A.M. (2004). Empowerment and Self-Management of Diabetes. Clinical Diabetes, 22:123-127.
Funnell, M.M. & Anderson, R.M. (2000). The problem with compliance in Diabetes Mellitus. Journal of American Medical Association 284:1709.
Glasgow, R.E., Toobert, D.J. & Gillette, C.D. (2001). Psychosocial barriers to diabetes self-management and quality of life. Diabetes Spectrum, 14:33-41.
Glasgow, R.E. & Toobert, D.J. (1988). Social environment and regimen adherence among Type II diabetic patients. Diabetes Care, 11:377-386.
Gonzales, J.S., Fisher, L. & Polonsky, W.H. (2011). Depression in diabetes: have we been missing something important? Diabetes Care, 34:236-9.
Griffith, L.S., Field, B.J. & Lustman, P.J. (1990). Life stress and social support in diabetes: Association with glycemic control. International Journal of Psychiatric Medicine, 20:365-372.
Harris, M.I. (2001). Frequency of blood glucose monitoring in relation to glycemic control in patients with Type II Diabetes Mellitus. Diabetes Care, 24(6):979-981.
Harris, M.I. (1998). Diabetes in America: Epidemiology and scope of problem. Diabetes Care, 21(3):C11-C14.
Haskell, W.L. & Lee, I.M. (2007). Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Curriculum, 116, 1081-1093.
Himsworth, H.P. (1936). Diabetes Mellitus: Its differentiation into insulin-sensitive and insulin-insensitive types. Lancet, 1:127-30.
International Diabetes Federation (2011). Global prevalence of Diabetes Mellitus. Retrieved from http://www.idf.org/diabetesatlas/diabetesand-impairedglucosetolerance.
Jarvis, J., Skinner, T.C., Carey, M.E., & Davies, M.J. (2009). How can structured self-management patient education improve outcomes in people with Type II Diabetes Mellitus? Diabetes, Obesity and Metabolism, 12:12-19.
Kalergis, M., Nadeau, J., Pacaud, D., Yared, Z., & Yale, J. (2006). Accuracy and reliability of reporting self-monitoring of blood glucose results in adults with Type I and Type II Diabetes Mellitus. Canadian Journal of Diabetes, 30(3):241-247.
Karter A.J., Ferrara, A., Darbinian, J.A., Ackerson, L.M. & Selby, J.V. (2000). Self-monitoring of blood glucose: Language and financial barriers in a managed care population with Diabetes Mellitus. Diabetes Care, 23:477-83
Kazaks, A., & Stern, J.S. (2003). Obesity treatments and controversies. Diabetes Spectrum, 16(4):231-235.
Koch, J. (2002). The roles of exercise in the African-American woman with Type II Diabetes Mellitus: Application of the health belief model. Journal of American Academy Nurse Practitioner, 14:126-9.
Laar, F.A., Lisdonk, E.H., Lucassen, P.L., Stafleu, A., Mulder, J., Hoogen, H.J., Rutten, G.E. & Weel, C. (2006). Eating behavior and adherence to diet in patients with Type II Diabetes Mellitus. Diabetes Medicine, 23(7):788-794.
Lustman, P;J;, Anderson, R.J. & Freedland, K.E. (2000). Depression and poor glycemic control: A meta-analytic review of the review of the literature. Diabetes Care, 23:932-42.

Madden, P.B. (2010). Diabetes and depression: Challenges and some opportunities. Diabetes Spectrum, 23(1):7-9.
McAdam-Marx, C., Mukherjee, J., Bellows, B.K., Unni, S., Ye, X., Iloeje, U., & Brixner, D.I. (2014). Evaluation of the relationship between weight change and glycemic control after initiation of anti-diabetic therapy in patients with Type II Diabetes Mellitus using electronic medical record data. Diabetes Research Clinical Practice, 103(3):402-11.
McKellar, J.D., Humphreys, K., & Piette, J.D. (2004). Depression increases diabetes symptoms by complicating patients’ self-care adherence. The Diabetes Educator, 30(3):485-492.
McNabb, W.L. (1997). Adherence in diabetes: Can we define it and can we measure it? Diabetes Care, 20(2):215-218.
Mitchell, C.G., Bowker, S.L., Majumdar, S.R., Toth, E. L., & Johnson, J.A. (2004). Lack of correlation between patient-reported outcomes and glycemic control in Type II Diabetes Mellitus not managed by insulin. Canadian Journal of Diabetes, 28(4):362-368.
Mirowsky, J. & Ross, C.E. (1998). Education, Personal Control, Lifestyle and Health. A Human Capital Hypothesis. Research on Aging, 20:415-449.
Mollem, E.D., Snoek, F.J., & Heine, R.J. (1996). Assessment of perceived barriers in self-care of insulin-requiring diabetic patients. Patient Education and Counseling, 29:277-281.
Nagelkerk, J. Reick, K. & Meengs, L. (2006). Perceived barriers and effective strategies to diabetes self-management. Journal of Advance Nursing, 54:151-8.
Peyrot, M., Rubin, R.R., Lauritzen, T., Snoek, F.J., Matthews, D.R. & Skovlund, S.E. (2005). Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabetes Medicine, 22:1379-1385.
Peyrot, M., McMurry, J.F. & Kruger, D.F. (1999). A bio-psychosocial model of glycemic control in diabetes: stress, coping, and regimen adherence. Journal of Health Social Behavior, 40:141-158.
Philippine Diabetes Statistics (2012). Incident rate of Diabetes Mellitus in the Philippines. Retrieved from http://www.allaboutdiabetes.net/philippine-diabetes-statistics/.
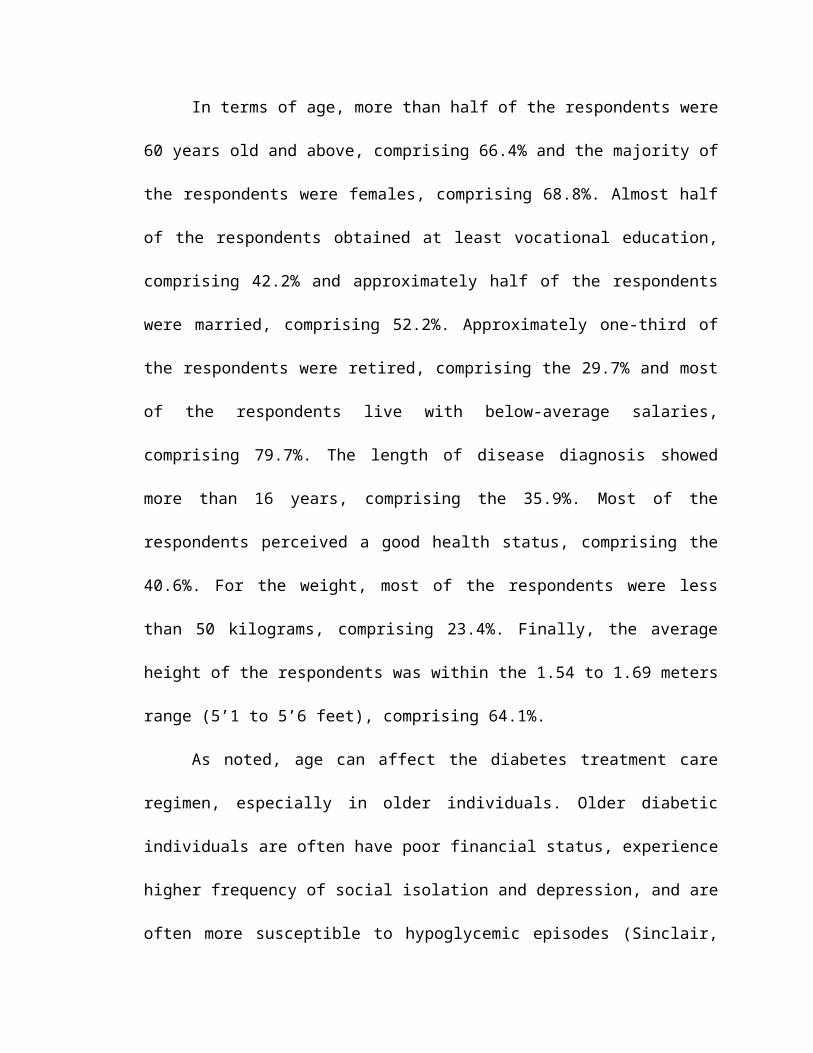
Polonsky, W.H., Fisher, L., Earles, J., Dudl, R.J., Lees, J., Mullan, J., et al. (2005). Assessing psychosocial distress in diabetes: Development of the diabetes distress scale. Diabetes Care, 28:626-31.
Polonsky, W.H., Anderson, B.J., Lohrer, P.A., Welch, G., Jacobsen, A.M., Aponte, J.E., et al. (1995). Assessment of diabetes-related distress. Diabetes Care, 18:754-60.
Plotnikoff, R.C., Karunamuni, N., Taylor, L., & Schmidt, C. (2009). An examination of the relationship between dietary behaviours and physical activity and obesity in adults with Type II Diabetes Mellitus. Canadian Journal of Diabetes, 33(1):27-34.
Pouwer, F., Beekman, A.T.F., Lubach, C. & Snoek, F.J. (2006). Nurses’ recognition and registration of depression, anxiety and diabetes-specific emotional problems in outpatients with Diabetes Mellitus. Patient Education Counsel, 60:235-40.
Rabi, D.M, Edwards, A.L., Southern, D.A., Svenson, L.W., Sargious, P.M., Norton, P., Larsen, E.T. & Ghali, W.A. (2006). Association of socio-economic status with diabetes prevalence and utilization of diabetes care services. Retrieved from http://www.biomedcentral.com/1472-6963/6/124.
Rhee, M.K., Slocum, W., Ziemer, D.C., Culler, S.D., Cook, C.B., El-Kebbi, I.M., Gallina, D.L., Barnes, C., & Phillips, L.S. (2005). Patient adherence improves glycemic control. The Diabetes Educator, 31(2):240-250.
Riffle, K.L. & Yoho, J., Sams, J. (1989). Health-promoting behaviors, perceived social support, and self-reported health of Appalachian elderly. Public Health Nursing, 6(4):204-211.
Rothman, R.L., Mulvaney, S., Elasy, T.A., VamderWoude, A., Gabretsadik, T., Shintani A., et al. (2008). Self-management behaviours, racial disparities, and glycemic control among adolescents with Type II Diabetes Mellitus. Pediatrics. 121:e912-9.
Schectman, J.M., Nadkarni, M.M. & Voss, J.D. (2002). Diabetes metabolic control and medication adherence in an indigent population. Diabetes Care, 25:1015–1021.
Schillinger D, Grumbach K, Piette J, et al. (2002). Association of health literacy with diabetes outcomes. Journal of American Medical Association, 288:475-82.
Shamsi, N., Shehab, Z., AlNahash, Z., AlMuhanadi, S. & Al-Nasir, F. (2013). Factors influencing dietary practice among Type II Diabetes Mellitus. Bahrain Medical Bulletin, 35(3).
Shrivastava, S.R., Shrivastava, P.S., & Ramasamy, J. (2013). Role of self-care in management of Diabetes Mellitus. Journal of Diabetes & Metabolic Disorders 2013:12-14.

Sinclair, A.J. (2006). Special considerations in older adults with diabetes: Meeting the challenge. Diabetes Spectrum, 19(4):229-233.
Solowiejczyk, J. (2010). Diabetes and depression: Some thoughts to think about. Diabetes Spectrum, 23(1):11-15.
Street, R.L. Jr., Piziak, V.K., Carpentier, W.S. et al (1993). Provider-patient communication and metabolic control. Diabetes Care, 16:714–21.
The European Commission (2011). Development of public health performance indicators for the pharmaceutical sector. Retrieved from http://ec.europa.eu/health/ph_information/dissemination/pharma/index_en.print.
Tomey A.M., & Alligood M.R. (2002). Nola J. Pender: Health Promotion Model. Nursing Theorists and their work 5th edition. Mosby, Singapore.
Trief, P.M. (2007). Depression in elderly Diabetes patients. Diabetes Spectrum, 20(2):71-75.
Unden, A.L. & Elofsson, S. (2001). Health from the patient’s point of view. How does it relate to the physician’s judgment? Family Practitioner, 18(2):174–80.
Vague, J. (1956). The degree of masculine differentiation of obesities: A factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. American Journal of Clinical Nutrition, 4:20-34.
Vallis, T.M., Higgins-Bowser, I., Edwards, L., Murray, A., & Scott, L. (2005). The role of diabetes education in maintaining lifestyle changes. Canadian Journal of Diabetes, 29(3):193-202.
Vincze, G., Barner, J.C., & Lopez, D. (2004). Factors associated with adherence to self-monitoring of blood glucose among persons with Diabetes Mellitus. The Diabetes Educator, 30(1):112-125.
Voorham J., Haaijer-Ruskamp, F.M., Wolffenbuttel, B.H.R., Stolk, R.P., & Denig, P. (2011). Medication adherence affects treatment modifications in patients with Type II Diabetes Mellitus. Clinical Therapeutics, 33(1):130-131
Wen, L.K., Shepherd, M.D. & Parchman, M.L. (2004). Family support, diet and exercise among older Mexican Americans with Type II Diabetes Mellitus. Diabetes Education, 30:980-93.
Williams, M.V., Baker, D.W., Parker, R.M., et al. (1998). Relationship of functional health literacy to patients’ knowledge of their chronic disease: A study of patients
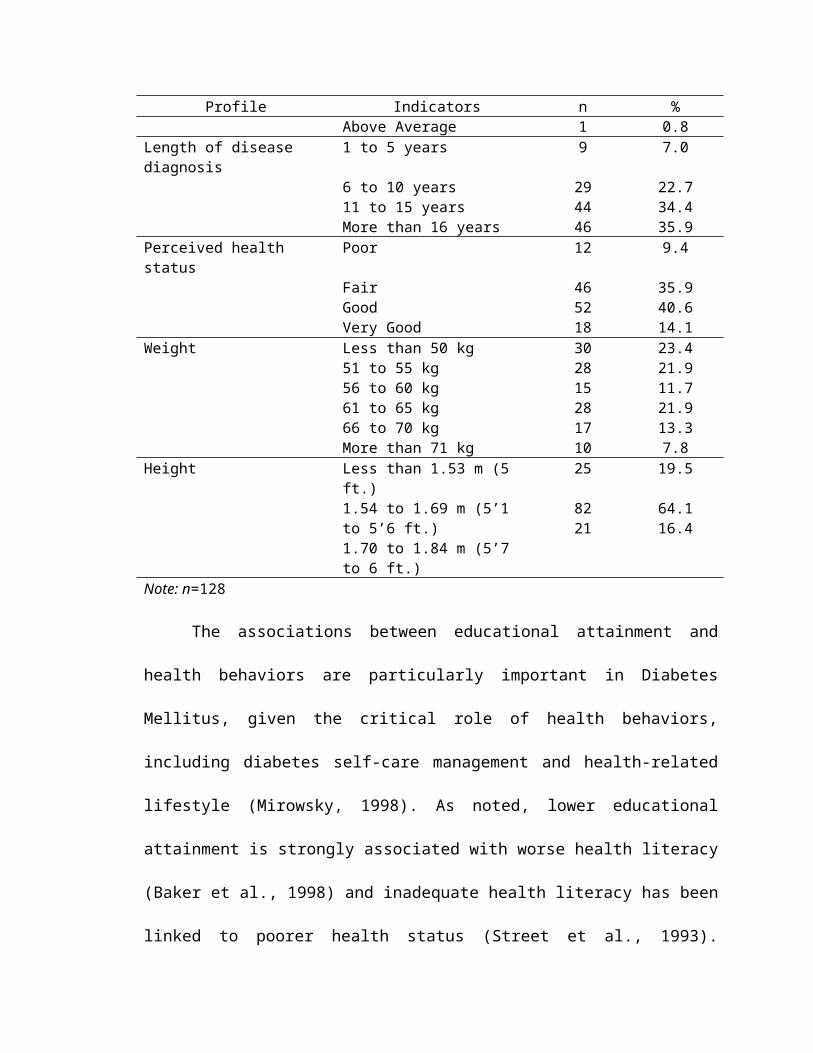
with hypertension and Diabetes Mellitus. Archive of Internal Medicine, 158:166-72.
World Health Organization (2012). Global mortality rates of Diabetes Mellitus. Retrieved from http://www.who.int/mediacentre/factsheets/fs312/en/
Zacker, R.J. (2004). Exercise: A key component of diabetes management. Diabetes Spectrum, 17(3):142-144