PRECISION AND PREDICTABILITY: Streamliningthe Implant and ... · successful section of the Seattle...
9
Knowledge for Clinical Practice WWW.DENTALLEARNING.NET A PEER-REVIEWED PUBLICATION D ENTAL L EARNING CE Course: Implant Planning and Treatment: The Digital Workflow P. 2 CASE PRESENTATION: A ‘Triple Scan Plan’ for the Digital Implant Workflow P. 10 Digital Dentistry's Bottom Line P. 13 CASE PRESENTATION: Digital Ortho Treatment Planning for Clinical Success P. 14 Streamlining the Implant Workflow P. 17 Using Digital Technology in Orthodontics P. 18 PRECISION AND PREDICTABILITY: Streamlining the Implant and Ortho Workfl ow Inside Earn 2 CE Credits Written for dentists, hygienists and assistants
Transcript of PRECISION AND PREDICTABILITY: Streamliningthe Implant and ... · successful section of the Seattle...

Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATIONA PEER-REVIEWED PUBLICATION
DENTAL LEARNING
CE Course: ImplantPlanning and Treatment:The Digital Workfl ow P. 2
CASE PRESENTATION:A ‘Triple Scan Plan’ for theDigital Implant Workfl ow P. 10
Digital Dentistry's Bottom Line P. 13
CASE PRESENTATION:Digital Ortho TreatmentPlanning for Clinical Success P. 14
Streamlining the ImplantWorkfl ow P. 17
Using Digital Technology inOrthodontics P. 18
PRECISION AND PREDICTABILITY:
Streamlining the Implant and Ortho Workfl ow
Inside Earn
2 CE CreditsWritten for dentists, hygienists and assistants

2 | DENTAL PRODUCT SHOP- PER www.dentalproductshop- per.com
LEARNING OBJECTIVES
The overall goal of this course is to provide information on the digital workfl ow for implant therapy. After completing this course, participants will be able to:
1. Describe key factors in implant treatment planning;
2. Review the digital workfl ow and the use of digital setups in implant treatment planning;
3. Outline implant components that can be viewed virtually; and,
4. Describe CAD/CAM digital technology as part of the digital workfl ow and its use for printed and milled components used during implant therapy.
Implant treatment is a reliable treatment that is increasingly in demand for the replacement of missing teeth. During implant treatment planning, anatomical structures must be accurately identifi ed and treatment must be planned from the perspective of the desired restorative result. This is of particular importance in the anterior region, where esthetics is a primary consideration. The digital workfl ow has improved the predictability and execution of implant therapy. It has also made it possible to increase accuracy, effi ciency, and patient comfort during treatment and to reliably achieve an esthetic result.
ABSTRACT
Introduction
Implant treatment is a reliable and predictable treatment for the
replacement of missing teeth,1,2,3 and demand for implant therapy
continues to increase. With precise planning and consideration of
all treatment aspects, implant-retained restorations have a good
prognosis, result in patient satisfaction, and do not involve adjacent
teeth.4,5 Subjective oral health improvement following single
implant treatment has also been found to improve, especially for
patients whose implants were placed in the anterior esthetic zone.6
Clinician and patient expectations dictate that treatment
planning consider anatomical, functional, and esthetic aspects of
implant therapy for the desired long-term outcomes. The maxillary
and mandibular anatomy at and adjacent to the proposed implant
site must be known. These will dictate the possible length of
implants, and whether ridge augmentation/bone grafting/sinus lift
is required to provide adequate bone height and volume. Buccal
ABOUT THE AUTHOR
Sonia S. Leziy, DDSSonia S. Leziy, DDS, received her dental degree from McGill University and post-graduate degree in periodontics from the University of British Columbia, Canada, where she is currently a clinical professor and sessional lecturer. Dr. Leziy is a Fellow of the Royal College of Dentists of Canada, a Fellow of the International
Congress of Oral Implantologists, and a member of the Canadian Academy of Periodontists and the American Academy of Periodontists. In addition, she co-mentors a highly successful section of the Seattle Study Club. A national and international lecturer, Dr. Leziy has published extensively on the subjects of implant esthetics and related surgical and restorative techniques. She maintains a private practice in North Vancouver.
Implant Planning and Treatment:The Digital Workfl ow
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. COMMERCIAL SUPPORTER: This course has been made possible through an unrestricted educational grant from HENRY SCHEIN. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Dental Learning, LLC designates this activity for 2 CE credits. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2016 - 1/31/2020. Provider ID: # 346890. Dental Learning, LLC is a Dental Board of California CE provider. The California Provider number is RP5062. This course meets the Dental Board of California’s requirements for 2 units of continuing education. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $29.00 for 2 CE credits. PUBLICATION DATE: July 2017. EXPIRATION DATE: June 2020. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 2 CE credits for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidence-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the � eld related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learning does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Joe Riley, does not have a leadership or commercial interest in any products or services discussed in this educational activity. He can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satis� ed with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. Go Green, Go Online to www.dentallearning.net to take this course. © 2017
Integrated Media Solutions Inc./DentalLearning.net is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the pro-vider or to ADA CERP at www.ada.org/cerp. Integrated Media Solutions Inc./DentalLearning.net designates this activity for 2 continuing education credits.
Approved PACE Program Provider FAGD/MAGD Credit Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement.2/1/2016 - 1/31/2020 Provider ID: # 346890AGD Subject Codes: 691,692,734
Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information contained on this certi� cate is truthful and accurate. Completion of this course does not constitute authorization for the attendee to perform any services that he or she is not legally authorized to perform based on his or her license or permit type. This course meets the Dental Board of California’s requirements for 2 units of continuing education. CA course code is 02-5062-17019.

DENTALLEARNING.NET DENTAL LEARNING | 3
DENTAL LEARNING
and palatal/lingual resorption of the alveolar ridge and undercuts
can also result in the need for ridge augmentation, where defects
would otherwise result in perforation of the bony plate or poor
positioning of an implant.
Implants placed at an angle to compensate for inadequate bone
volume can also compromise clinical outcomes by causing abnormal
loading of the restored implant. This can increase bone loss beyond
that which is physiological, and can also result in mechanical failure
of the implant or restorative components. In addition, the implant
must be placed in a three-dimensional position that will allow for an
esthetic emergence profi le, peri-implant soft tissue development,
and a natural-looking defi nitive restoration. Factors infl uencing
patient satisfaction with esthetics include the color and shape of
the crown, and the amount of papillary fi ll.8 Treatment planning
must address implant position relative to the crestal bone and
buccal-lingual and mesio-distal dimensions, tissue type and volume,
development of the peri-implant tissue and achievement of papillary
fi ll, and the type of abutment and emergence profi le of the fi nal
restoration for an esthetic result. Digital treatment planning and the
digital workfl ow have improved the predictability and execution of
implant therapy, especially in the esthetic zone.
Digital Treatment Planning and the Digital Workfl owTraditionally, an initial patient assessment for implant therapy
included radiographs. However, radiographs do not provide a three-
dimensional (3D) view. Cone beam computed tomography (CBCT)
and computerized axial tomography (CAT), in addition to STL digital
scans/impressions, are now available and used to obtain 3D digital
images, with signifi cant improvements in planning and diagnostic
capabilities. Based on the risk of lingual plate perforation in the
posterior mandible, for instance, it was concluded that CBCT scanning
is essential for planning immediate implant placement.7 The implant
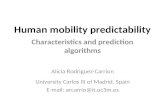
planning software creates virtual models to visualize a virtual implant
in the arch using 3D images and cross-sectional views captured using
the digital scans. The result is an overview of the ideal implant position
(Figure 1). 3D images and implant planning software show bone
defects where resorption has occurred, and show the clinician during
the treatment planning where insuffi cient bone volume is present and
where anatomical structures are in close proximity. In the example
shown, the patient had presented with generalized recession in the
region 5-12 and failing teeth #7 and 9, while periapical radiographs
revealed an apical bone defect in the area of tooth #7 and prior
apical surgery in teeth #7 and 9. The preoperative axial view sections
identifi ed a narrow/slender ridge and large nasopalatine duct. Teeth
#7 and 9 also appeared to have little/no overlying facial bone. The
unfavorable ridge anatomy and bone defects coupled with clinical
tissue challenges necessitated multistaged gingival tissue and bone
grafting procedures prior to implant placement (Figures 2, 3).
Due to the complexity of the case, bone grafting was fi rst
performed and the implant would be placed later. The digital
STLdigitalscan/
impression
Implantplanningsoftware
‘Placement’ofvirtualimplant
components
Createsvirtualmodels
Overviewofidealimplantposition.Overviewof
emergenceprofileandrestorative
result
CBCTScans
Figure 1—The Digital Workfl ow
Figure 2—Preoperative axial view section and identifi cation of minimal facial bone at #7 and 9
Figure 3—Minimal facial bone

4 DENTAL LEARNING
workfl ow continued with treatment planning of implants in sites #7
and 9, as shown by the Implant Studio screen capture of the axial
section. The implant at site #7 was shown planned approximately
1.5 mm from the adjacent root, but staying distal to the nasopalatine
canal (Figure 4). The planning of the precise implant position also
allowed for use of an angled screw channel for a defi nitive screw-
retained restoration. A new CBCT scan and optical scan were taken
5 months after bone grafting, and a screen capture of the virtual
tooth setup and position of implants respecting the adjacent roots
obtained (Figure 5). A palatal view screen capture showed the
planned implant and screw access positions. The digital workfl ow
enabled highly precise treatment planning for implant placement,
avoiding closely adjacent anatomical structures. In addition, virtual
implants, abutments, and restorations can be ‘placed’ to view
resulting emergence profi les and the restorative result.
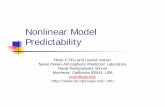
The digital workfl ow also includes the creation of milled or
printed models, and printed surgical guides allow for precise creation
of osteotomies for implant placement, since the surgical guide’s
osteotomy window is printed based on the results from the implant
planning software. In addition to precision and the opportunity
to create custom healing abutments, the digital workfl ow offers
increased effi ciency and a better patient experience. For example,
scan fl ags and optical scanning can be used instead of using
traditional copings, impressions, and poured models with analogs. In
the case shown here, scan fl ags constructed of a titanium base and
PEEK (BioHorizons) were positioned over the implant and verifi ed
with radiographs to ensure they were properly seated (Figure 6).
Optical intraoral scans were then taken. These are interpreted by
CAD software, which creates a 3D digital model. The fi les can then be
transferred digitally to the laboratory for restoration fabrication, which
can be performed using the 3D digital model and CAD software, or a
milled/printed model for traditional restoration fabrication. Scan fl ags
enable high-precision intraoral optical scanning whereby the digital
images accurately record the implant fi xture, peri-implant mucosa,
and adjacent structures. As a result, effi ciency and accuracy are
greater, and the patient avoids a traditional impression.
Milled custom healing abutments and custom abutments are also
created using the digital workfl ow and CAD/CAM software, as well
as milled models for provisional fabrication and CAD/CAM or milled
models for fabrication of the defi nitive restoration (Figure 7).
The digital workfl ow has made implant treatment more precise and predictable, in addition to stream-lining treatment and improving overall effi ciency.
The case below demonstrates the digital workfl ow for single
implant therapy in the anterior esthetic zone.
Case 1. Single implant restoration replacing the upper left lateral incisor
The patient presented with a fractured upper left lateral
incisor that was deemed hopeless (Figures 8, 9). Together with
Implant Planning and Treatment: The Digital Workfl ow
Figure 4—Screen capture with virtual setup.Facial opacities are the titanium-reinforced PTFE membrane and tacks.
Figure 6—Scan fl ags positioned
Figure 5—Screen capture with virtual setup

DENTALLEARNING.NET DENTAL LEARNING | 5
DENTAL LEARNING
the patient, it was decided that the best option was extraction,
immediate implant placement, and temporization. Ideal planning
mandated the use of a CBCT scan. The digital workfl ow continued
with the use of implant planning software (3Shape) for assessment
of bone volume and quality, adjacent structures, and position of
a virtual implant. The initial planning was for immediate implant
placement of a 4.6 × 15 TLXP implant (BioHorizons) in order to
allow for apical bone engagement for primary implant stability.
However, using the implant planning software, the probability
of leaving less than 2 mm of facial bone was identifi ed (Figure
10). This would be undesirable and could result in future
postrestoration instability of the facial and gingival tissue, with
compromised esthetics. As a result, treatment was replanned for a
3.8 × 18 TLX implant (increased length, reduced diameter) (Figure
11). This would allow for primary implant stability, improved facial
bone volume for long-term tissue contour stability, and improved
positioning relative to the virtual tooth contour bucco-lingually.
After the ideal implant position was determined, the digital
workfl ow allowed for alignment and printing of a surgical
guide with inspection windows to verify full seating and color-
coding for the planned implant and incorporating sleeves
to aid precision during the osteotomy (Figure 12). Printed
surgical guides have been shown to have a high degree of
accuracy.9 Printed models were also created that would be
used to fabricate components for temporization. A broad
range of transitional restorative options can be preplanned
to adapt to the unique features of the clinical environment.
These include prefabricated, customized, healing abutments
that can be coupled with a bonded nano-ceramic or PMMA
bridge, and a transitional implant crown/engaging titanium
base and seating jig where stability and occlusion permit. While
engaging abutments are generally used in single restorations,
non-engaging bases can be used to allow for prefabricated
one-piece provisional restorations to overcome the problem of
vertical implant positioning (timing) in a guided protocol.
Customized healing abutments allow for ideal soft tissue
guidance and protection of underlying bone or bone graft
materials in immediate implant placement. Adjacent natural
teeth are predictive of papillary development and maintenance,
and the distance from the bone level to the contact point with
Figure 8—Fractured upper left lateral incisor Figure 9—Periapical radiograph
CAD/CAMsoftware
Printed/milledsurgicalguides
Printedmodelsfor
fabricationofprovisionals
Milledcustomhealing
abutments
Scanflagsforscanningofimplantfixture
Milledabutments
anddefinitiverestorations
Figure 7—Digital workfl ow and CAD/CAM fabrication

6 DENTAL LEARNING
the adjacent tooth must be preplanned to foster papillary fill.10,11
Greater facial-lingual mucosal width at the base of the complete
papillae also results in more complete papillae. These factors
again highlight the desirability of precision planning, as offered
by the digital workflow.
In this case, a customized PMMA healing abutment on an
engaging titanium base was used that had been prefabricated
with 3D information from the STL and DICOM files taken at the
planning stage. The implant and healing abutment were verified
radiographically postsurgery, and a bonded bridge was used
for immediate temporization (Figures 13-15). Once peri-implant
soft tissue is subject to remodeling as with a custom healing
abutment/provisional restoration, it has been shown that papillae
will regenerate when both one-stage and two-stage surgical
protocols are maintained.12 Conservative surgical treatment was
possible (extraction, implant placement, and bone grafting of the
facial residual horizontal bone defect, custom healing abutment),
resulting in uneventful soft tissue healing.
After soft tissue remodeling, the tissue contour was ideal,
and a custom zirconia abutment was digitally designed and
milled. Custom zirconia abutments result in superior esthetics
and avoid the gray shine-through of metal abutments that may
Implant Planning and Treatment: The Digital Workflow
Figure 14—Illustration of a custom healing abutment scaffolding/supporting the marginal tissues
Figure 12—The printed surgical guide
Figure 15—7 days after surgery
Figure 13—Custom healing abutment. The black occlusal dot identifies facial orientation of the abutment.
Figure 10—Potentially inadequate bone
Figure 11—Mesial-distal view showing redirected implant position

DENTALLEARNING.NET DENTAL LEARNING | 7
DENTAL LEARNING
be observed at gingival margins. The margin was also designed
to be 0.5 mm subgingival to mirror the marginal gingival tissue
defined by the healing abutment. A screw-retained lithium
disilicate crown was milled from a digital model, and placed
(Figures 16, 17). The result was an esthetic restoration that
mimicked nature, and a satisfied patient.
ConclusionsImplant therapy is now mainstream and frequently the
treatment of choice. In the anterior esthetic zone, the emergence
profile must allow for excellent esthetics, and the final restoration
must mimic (or improve on) nature in addition to being functional.
The advent of CBCT scans, digital impressions and the digital
workflow has made treatment more precise and predictable.
Virtual implant planning supports a restorative-driven approach
with improved esthetics and function.13, 14 The digital workflow
also streamlines treatment with fewer appointments, and is more
efficient overall, resulting in time and cost savings.15 It also allows
the clinician and laboratory technician to share the same 3D
images and treatment planning tools, improving communication,
planning, and actual treatment.
For the patient, the office is seen as high-tech, treatment
is easier (e.g., scan flags and scanning remove the need for
unpleasant traditional impressions and are quicker), and
customized CAD/CAM components result in excellent esthetics.
In summary, the digital workflow provides predictability,
precision, efficiency, and a great patient experience.
References1 Mangano C, Mangano F, Piattelli A, et al. Prospective clinical evaluation of 307
single-tooth morse taper-connection implants: a multicenter study. Int J Oral Maxillofacial Implants. 2010;25(2):394-400.
2 Buser D, Merickse-Stern R, Bernard JP, et al. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res. 1997;8(3):161-72.
3 Kourtis SG, Sotiriadou S, Voliotis S, Challas A. Private practice results of dental implants. Part I: survival and evaluation of risk factors. Part II: surgical and prosthetic complications. Implant Dent. 2004;13(4):373-85.
4 Andersson B, Bergenblock S, Fürst B, Jemt T. Long-Term Function of Single-Implant Restorations: A 17- to 19-year follow-up study on implant infraposition related to the shape of the face and patients’ satisfaction. Clin Implant Dent Relat Res. 2013;15(4):471-80.
5 Suphanantachat S, Thovanich K, Nisapakultorn K. The influence of peri-implant mucosal level on the satisfaction with anterior maxillary implants. Clin Oral Implants Res. 2012;23(9):1075-81.
6 Ponsi J, Lahti S, Rissanen H, Oikarinen K. Change in subjective oral health after single dental implant treatment. Int J Oral Maxillofac Implants. 2011;26(3):571-7.
7 Huang RY, Cochran DL, Cheng W-C, et al. Risk of lingual plate perforation for virtual immediate implant placement in the posterior mandible. A computer simulation study. J Am Dent Assoc. 2015;146(10):735-42.
8 Suphanantachat S, Thovanich K, Nisapakultorn K. The influence of peri-implant mucosal level on the satisfaction with anterior maxillary implants. Clin Oral Implants Res. 2012;23(9):1075-81.
9 Neumeister A, Schulz L, Glodecki C. Investigations on the accuracy of 3D-printed drill guides for dental implantology. Int J Comput Dent. 2017;20(1):35-51.
10 Chang M, Wennström JL. Soft tissue topography and dimensions lateral to single implant-supported restorations. A cross-sectional study. Clin Oral Impl Res. 2013;24:556-62.
11 Cosyn J, Raes M, Packet M, et al. Disparity in embrasure fill and papilla height between tooth- and implant-borne fixed restorations in the anterior maxilla: a cross-sectional study. J Clin Periodontol. 2013;40(7):728-33.
12 De Rouck T, Collys K, Wyn I, Cosyn J. Instant provisionalization of immediate single-tooth implants is essential to optimize aesthetic treatment outcome. Clin Oral Implants Res. 2009;20(6):566-70.
13 D’haese J, Ackhurst J, Wismeijer D, et al. Current state of the art of computer-guided implant surgery. Periodontol 2000. 2017;73(1):121-33.
14 Barros V de M, Costa NR, Martins PHF, et al. Definitive presurgical CAD/CAM-guided implant-supported crown in an esthetic area. Braz Dent J. 2015;26(6):695-700.
15 Joda T, Brägger U. Time-efficiency analysis of the treatment with monolithic implant crowns in a digital workflow: a randomized controlled trial. Clin Oral Implants Res. 2016;27(11):1401-6.
Figure 16—Milled custom zirconia abutment
Figure 17 —Ceramic crown at 1 year
Digitally designed and milled custom zirconia abutments result in superior esthetics.

8 DENTAL LEARNING
1. Clinician and patient expectations dictate that treatment planning consider the ____________ aspect ofimplant therapy.a. quantificationb. anatomical, functional, and estheticc. volumetric and anatomic d. perspective
2. To avoid causing abnormal loading of an implant, these can be placed ____________ to compensate for inadequate bone volume.a. at an angleb. counter-rotationally c. subgingivallyd. none of the above
3. Factors influencing patient satisfaction with esthetics include the ____________.a. use of masking techniquesb. amount of papillary fillc. number of teeth remainingd. color of the gingivae
4. Cone beam computed tomography (CBCT) used to obtain 3D digital images has resulted in significant improvements in planning and diagnostic capabilities.a. Trueb. False
5. Implant planning software creates virtual models to visualize a virtual implant in the arch using 3D images and _____________ views.a. diagonal b. trans-sectionalc. cross-sectional d. mirrored
6. Implant planning software permits an overview of the emergence profile and restorative result.a. True b. False
7. The osteotomy window in a printed surgical guide is printed based on the results from _____________. a. a visual assessmentb. the clinician’s assessment of the
CBCT scanc. implant planning softwared. a and b
8. _____________ avoid the use of traditional copings, impressions, and poured models with analogs. a. Scan flags and CBCT scansb. Abutment flags and optical scanningc. Visual scanning and scanned flagsd. Scan flags and optical scanning
9. Optical scans are interpreted by _____________, which creates a 3D digital model. a. implant planning software b. CAD softwarec. CBCT softwared. CAM software
10. _____________ record the implant fixture, peri-implant mucosa, and adjacent structures. a. Analogs b. Healing abutments c. CBCT scans d. Scan flags
11. Milled custom healing and definitive abutments are created using the digital workflow and CAD/CAM software.a. True b. False
12. Leaving less than 2 mm of facial bone could result in postrestoration instability of the _____________.a. facial and gingival tissueb. restorationc. facial and palatal boned. all of the above
13. Inspection windows are included in surgical guides to verify _____________.a. the position of the osteotomyb. full seating of the guidec. the width of the osteotomyd. the implant position
14. Where _____________ permit, a transitional implant crown/engaging titanium base and seating jig can be used for provisional restorative care.a. stability and emergence profile b. occlusion and esthetics c. stability and occlusiond. esthetics and peri-implant
mucosal tissue
15. Non-engaging abutments are generally used for single restorations. a. Trued. False
16. The distance from the bone level to the contact point with the adjacent tooth must be preplanned to foster _____________. a. emergence profileb. the health of peri-implant mucosac. papillary filld. a naturally shaped crown
17. 3D information from the _____________ files are taken at the planning stage. a. STL b. jpeg c. DICOMd. a and c
18. Custom zirconia abutments ____________. a. are stronger than traditional
abutmentsb. avoid gray shine-through c. are recommended to improve soft
tissue developmentd. all of the above
19. One reason a digital workflow makes treatment easier for patients is because _____________. a. treatment is slower b. traditional impressions are not
requiredc. x-ray exposure is not required at any point in treatment planningd. fewer locals are required
20. The digital workflow _____________. a. streamlines treatment with fewer
appointmentsb. is efficientc. results in time and cost savings d. all of the above
CEQuizTo complete this quiz online and immediately download your CE verification document, visit www.dentallearning.net/SIO-ce, then log in to your account (or register to create an account). Upon completion and passing of the exam, you can immediately download your CE verification document. We accept Visa, MasterCard, Discover, and American Express.
Implant Planning and Treatment: The Digital Workflow

DENTALLEARNING.NET DENTAL LEARNING | 9
Implant Planning and Treatment: The Digital WorkflowCE ANSWER FORM (E-mail address required for processing)
*Name: Title: Specialty
*Address: NPI No.
*City: *State: *Zip: AGD Identification No.
*E-mail:
*Telephone: License Renewal Date:
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the evaluation included with the course. INSTRUCTIONS: All questions have only one answer. Participants will receive confirmation of passing by receipt of a verification certificate. Verification certificates will be processed within two weeks after submitting a completed examination. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and research-based evidence. Any opinions of efficacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of Dental Learning. Completing a single continuing education course does not provide enough information to make the participant an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a CE verification certificate. Dental Learning, LLC is an ADA CERP recognized provider. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Please contact Dental Learning, LLC for current terms of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California Provider number is RP5062. The cost for courses ranges from $19.00 to $90.00. RECORD KEEPING: Dental Learning, LLC maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of request. Dental Learning, LLC maintains verification records for a minimum of seven years. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC in writing or by calling 1-888-724-5230. Go Green, Go Online to www.dentallearning.net to take this course. © 2017
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
21. A B C D
22. A B C D
23. A B C D
24. A B C D
25. A B C D
26. A B C D
27. A B C D
28. A B C D
29. A B C D
30. A B C D
QUIZ ANSWERSFill in the circle of the appropriate answer that corresponds to the question on previous pages.
EDUCATIONAL OBJECTIVES1. Describe key factors in implant treatment planning;
2. Review the digital workflow and the use of digital setups in implant treatment planning;
3. Outline implant components that can be viewed virtually; and,
4. Describe CAD/CAM digital technology as part of the digital workflow and its use for printed and milled components used during implant therapy.
If you have any questions, please email Dental Learning at [email protected] or call 888-724-5230.
COURSE SUBMISSION: 1. Read the entire course.2. Complete this entire answer sheet in
either pen or pencil.3. Mark only one answer for each question.4. Mail or fax answer form. For immediate results:1. Read the entire course.2. Go to www.dentallearning.net/SIO-ce.3. Log in to your account or register to create an
account.4. Complete course and submit for grading to
receive your CE verification certificate.
A score of 70% will earn your credits.
Dental Learning, LLC500 Craig Road, First FloorManalapan, NJ 07726
*If paying by credit card, please note:MasterCard | Visa | AmEx | Discover
*Account Number
______________________________________________
*Expiration Date
______________________________________________
The charge will appear as Dental Learning, LLC.
If paying by check, make check payable to Dental Learning, LLC.
ALL FIELDS MARKED WITH AN ASTERISK (*) ARE REQUIRED
AGD Codes: 691, 692, 734
Price: $29 CE Credits: 2Save time and the environment by taking this course online.
COURSE EVALUATIONPlease evaluate this course using a scale of 3 to 1, where 3 is excellent and 1 is poor.
1. Clarity of objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
2. Usefulness of content . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
3. Benefit to your clinical practice . . . . . . . . . . . . . . . . . . . . 3 2 1
4. Usefulness of the references . . . . . . . . . . . . . . . . . . . . . . 3 2 1
5. Quality of written presentation . . . . . . . . . . . . . . . . . . . . 3 2 1
6. Quality of illustrations . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
7. Clarity of quiz questions . . . . . . . . . . . . . . . . . . . . . . . . . 3 2 1
8. Relevance of quiz questions . . . . . . . . . . . . . . . . . . . . . . 3 2 1
9. Rate your overall satisfaction with this course . . . . . . . . 3 2 1
10. Did this lesson achieve its educational objectives? Yes No
11. Are there any other topics you would like to see presented in the future? __________________________________________________________________________
_______________________________________________________________________________________
SPECIAL CODE __________________________