Pre-operative MRI of Endometrial Cancer: Clinically ... · + Hormonal Rx Tumor on T2-wt images ......
28
Pre-operative MRI of Endometrial Cancer: Clinically relevant findings and pitfalls to avoid. Krupa Patel-Lippmann, MD 1 Kristie Guite, MD 1 Jessica Robbins, MD 1 Ahmed Al-Niaimi, MD 2 Elizabeth Sadowski, MD 1 University of Wisconsin SCHOOL OF MEDICINE AND PUBLIC HEALTH Department of Radiology 1 Department of Obstetrics and Gynecology-UW 2
Transcript of Pre-operative MRI of Endometrial Cancer: Clinically ... · + Hormonal Rx Tumor on T2-wt images ......

Pre-operative MRI of Endometrial Cancer:
Clinically relevant findings and pitfalls to avoid.
Krupa Patel-Lippmann, MD1
Kristie Guite, MD1
Jessica Robbins, MD1
Ahmed Al-Niaimi, MD2
Elizabeth Sadowski, MD1
University of Wisconsin SCHOOL OF MEDICINE AND PUBLIC HEALTH
Department of Radiology1
Department of Obstetrics and Gynecology-UW2

No disclosures to report.
Disclosures

Overview of normal MRI uterine anatomy
Describe MR imaging features and staging of endometrial cancer
Learn to differentiate the appearance of endometrial cancer
from endometrial hyperplasia, adenomyosis, fibroids, and polyps
Highlight common pitfalls encountered in the MRI assessment of endometrial cancer
Objectives

Introduction
Endometrial cancer
4th most common cancer in women
Most common gynecologic malignancy
Peak incidence: 55 and 65 years
Risk factors
Obesity
Nulliparity
Late menopause
Unopposed estrogen exposure
Tamoxifen

Introduction
Over 80% of patients present with early stage disease due to symptoms of abnormal uterine bleeding, with an overall excellent prognosis.
Endometrial cancer is traditionally surgically staged and the treatment varies by stage, grade, regional guidelines, and expertise.
MRI is a valuable adjunct to pre-operative planning as it can accurately depict endometrial cancer . The goal of MRI is to identify patients pre-operatively who would benefit from abdominopelvic lymph node dissection and adjuvant therapy while avoiding overtreating early stage patients with unnecessary lymphadenectomies.
MRI Protocol
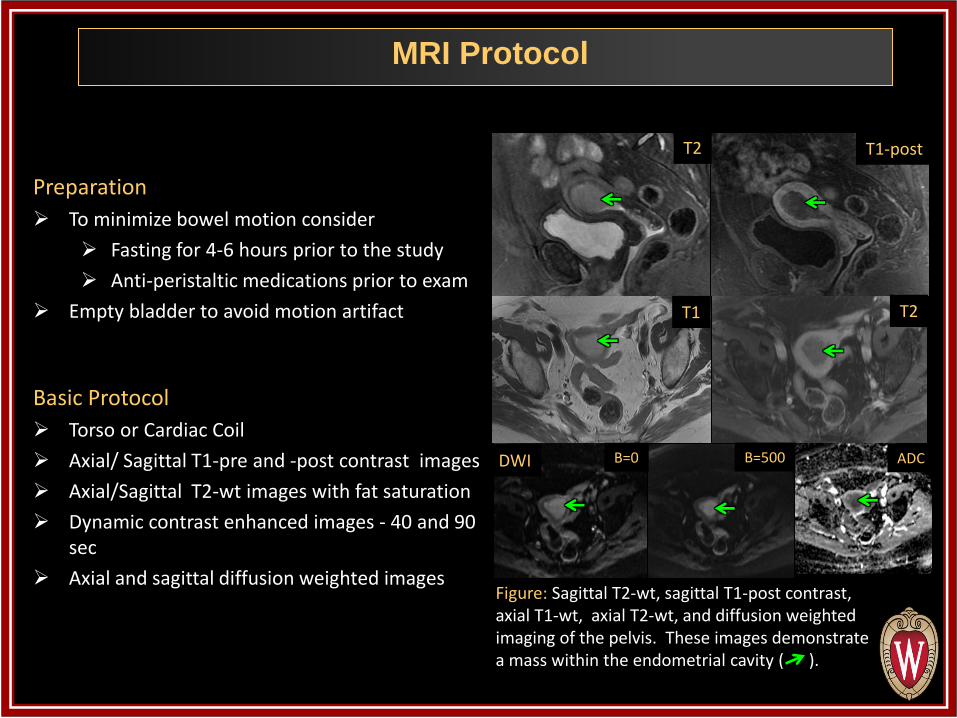
Preparation
To minimize bowel motion consider
Fasting for 4-6 hours prior to the study
Anti-peristaltic medications prior to exam
Empty bladder to avoid motion artifact
Basic Protocol
Torso or Cardiac Coil
Axial/ Sagittal T1-pre and -post contrast images
Axial/Sagittal T2-wt images with fat saturation
Dynamic contrast enhanced images - 40 and 90 sec
Axial and sagittal diffusion weighted images
Figure: Sagittal T2-wt, sagittal T1-post contrast, axial T1-wt, axial T2-wt, and diffusion weighted imaging of the pelvis. These images demonstrate a mass within the endometrial cavity ( ).
T2 T1-post
DWI
T2 T1
B=0 B=500 ADC
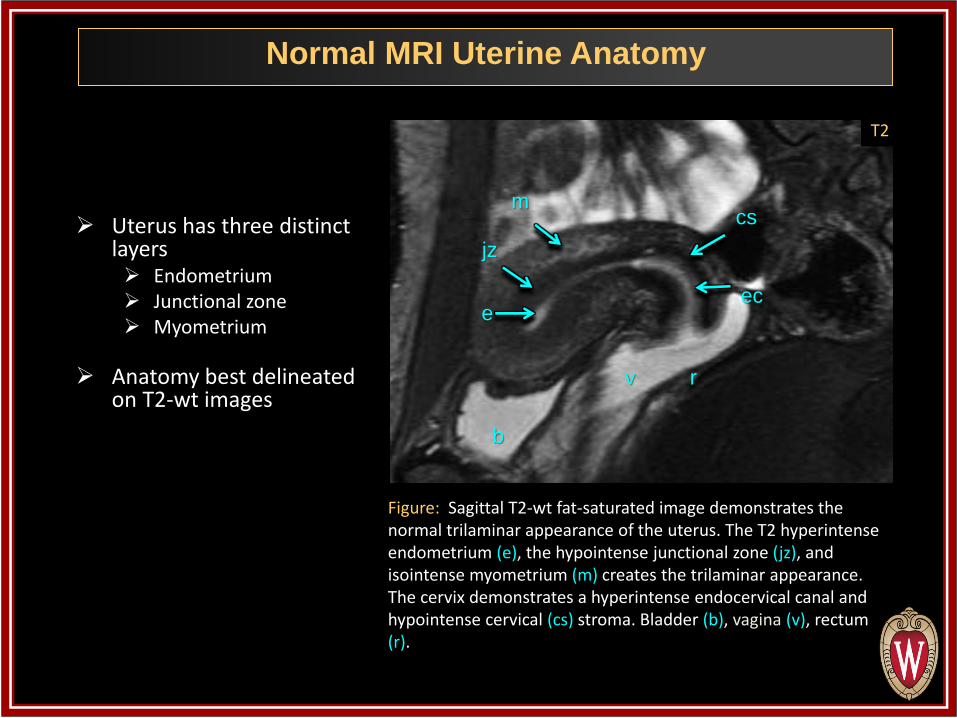
Uterus has three distinct layers Endometrium Junctional zone Myometrium
Anatomy best delineated on T2-wt images
Normal MRI Uterine Anatomy
GUCXM3
Figure: Sagittal T2-wt fat-saturated image demonstrates the normal trilaminar appearance of the uterus. The T2 hyperintense endometrium (e), the hypointense junctional zone (jz), and isointense myometrium (m) creates the trilaminar appearance. The cervix demonstrates a hyperintense endocervical canal and hypointense cervical (cs) stroma. Bladder (b), vagina (v), rectum (r).
b
v r
jz
m
ec e
cs
T2

Endometrial Cancer Staging and Grading
Tumor Histology : pre-operative from endometrial biopsy
Tumor grade: I-III (well -poorly differentiated)
Tumor cell type: 90% adenocarcinoma with endometroid subtype. Clear cell and papillary serous carcinoma have a worse prognosis.
Tumor Stage : surgically staged in the OR
Based on 2009 International Federation of Gynecologic and Obstetrics (FIGO) Surgical Staging System
Full staging consists of total abdominal hysterectomy, bilateral salpingo-oophorectomy, peritoneal washings, and retroperitoneal lymph node dissection
Key prognostic factors are depth of myometrial invasion( MI), cervical stromal invasion, and lymphovascular invasion (LVSI)
Stage Description
IA Tumor confined to uterus, <50% MI
IB Tumor confined to uterus, ≥50% MI
II Cervical stromal invasion
IIIA Tumor invasion into serosa or adnexa
IIIB Vaginal or parametrial involvement
IIIC1 Pelvic node involvement
IIIC2 Para-aortic node involvement
IVA Tumor invasion into bladder/bowel mucosa
IVB Distant metastases
Risk stratification and treatment planning is based on tumor histology and tumor stage.
FIGO 2009 Surgical Staging System
Figure modified from: Beddy et al. FIGO Staging System for Endometrial Cancer. RadioGraphics 2012
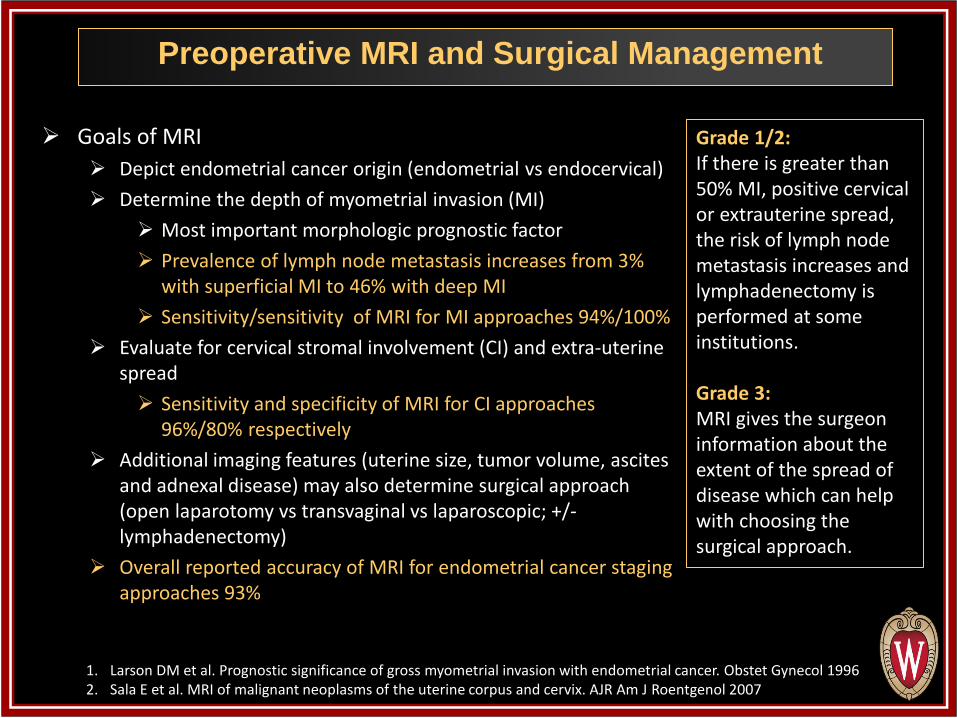
Goals of MRI
Depict endometrial cancer origin (endometrial vs endocervical)
Determine the depth of myometrial invasion (MI)
Most important morphologic prognostic factor
Prevalence of lymph node metastasis increases from 3% with superficial MI to 46% with deep MI
Sensitivity/sensitivity of MRI for MI approaches 94%/100%
Evaluate for cervical stromal involvement (CI) and extra-uterine spread
Sensitivity and specificity of MRI for CI approaches 96%/80% respectively
Additional imaging features (uterine size, tumor volume, ascites and adnexal disease) may also determine surgical approach (open laparotomy vs transvaginal vs laparoscopic; +/- lymphadenectomy)
Overall reported accuracy of MRI for endometrial cancer staging approaches 93%
Preoperative MRI and Surgical Management
Grade 1/2: If there is greater than 50% MI, positive cervical or extrauterine spread, the risk of lymph node metastasis increases and lymphadenectomy is performed at some institutions. Grade 3: MRI gives the surgeon information about the extent of the spread of disease which can help with choosing the surgical approach.
1. Larson DM et al. Prognostic significance of gross myometrial invasion with endometrial cancer. Obstet Gynecol 1996 2. Sala E et al. MRI of malignant neoplasms of the uterine corpus and cervix. AJR Am J Roentgenol 2007

Stage Description
IA Tumor confined to uterus, <50% myometrial invasion
IB Tumor confined to uterus, ≥50% myometrial invasion
II Cervical stromal invasion
IIIA Tumor invasion into serosa or adnexa
IIIB Vaginal or parametrial involvement
IIIC1 Pelvic node involvement
IIIC2 Para-aortic node involvement
IVA Tumor invasion into bladder or bowel mucosa
IVB Distant metastases
FIGO 2009: Management based on Stage
Surgery
Surgery +/- vaginal brachytherapy
Modified from: Beddy et al. FIGO Staging System for Endometrial Cancer. RadioGraphics 2012
Surgery + vaginal brachytherapy +/- pelvic radiotherapy
Surgery + pelvic radiotherapy +/- chemotherapy
+ Hormonal Rx
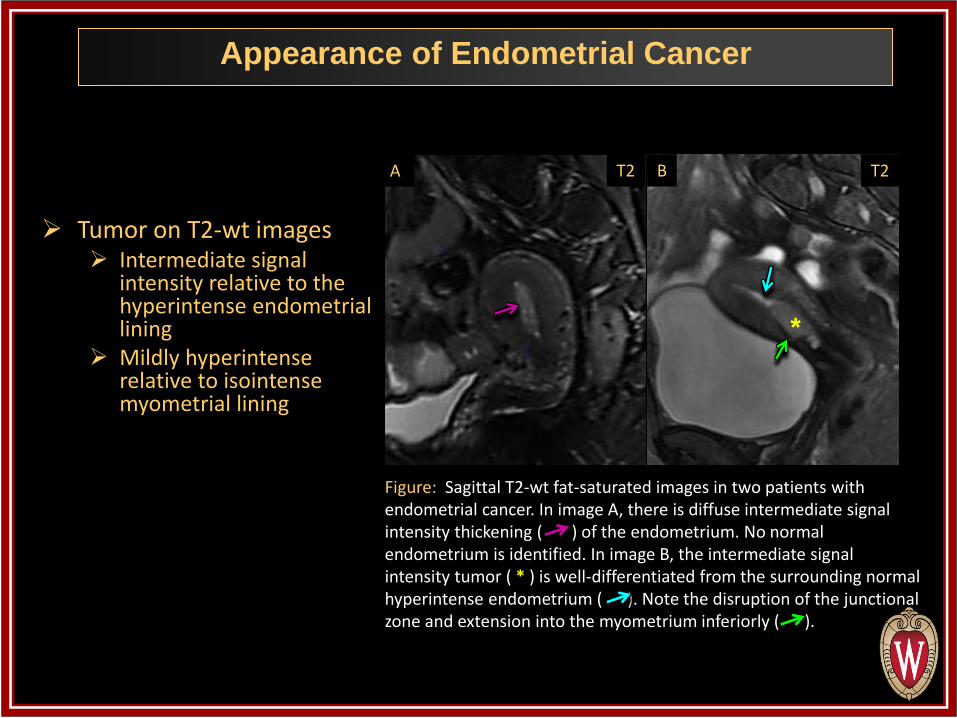
Tumor on T2-wt images Intermediate signal
intensity relative to the hyperintense endometrial lining
Mildly hyperintense relative to isointense myometrial lining
Appearance of Endometrial Cancer
GUCXM3
Figure: Sagittal T2-wt fat-saturated images in two patients with endometrial cancer. In image A, there is diffuse intermediate signal intensity thickening ( ) of the endometrium. No normal endometrium is identified. In image B, the intermediate signal intensity tumor ( * ) is well-differentiated from the surrounding normal hyperintense endometrium ( ). Note the disruption of the junctional zone and extension into the myometrium inferiorly ( ).
A B
*
T2 T2

T1-pre contrast imaging Tumor isointense relative to
hypointense normal endometrium on unenhanced images
Often difficult to discern on pre- contrast imaging, especially in small tumors
T1-post contrast images Dynamic contrast enhanced
images are obtained Tumor enhances
homogenously and more slowly with less avidity than adjacent myometrium
Endometrial tumors enhance earlier than normal endometrium
Appearance of Tumor
Figure: Sagittal T2-wt and T1-post contrast images in a 55 year old female with endometrial cancer. The tumor demonstrates intermediate T2 signal intensity ( ) as well as hypoenhancement (*) relative to the avidly enhancing myometrium ( ). Note the irregular myometrial contour ( ) consistent with myometrial invasion.
*
T2 T1-post

Endometrial cancer demonstrates diffusion restriction compared to surrounding tissue
Diffusion weighted imaging (DWI) B=0, B=500 and ADC maps The tumor will become progressively brighter from B=0 to B=500 On the ADC map, the tumor is dark relative to the endometrium and myometrium,
but can blend in with the junctional zone
Appearance of Tumor
GUCXM3
Figure: Sagittal T2-wt, T1-post-contrast and diffusion weighted images. The tumor appears round, minimally hyperintense on T2-wt images ( ), hypointense compared to avidly enhancing myometrium on post contrast images ( ), and on DWI ( ) was gray on B=0, bright on B=500 and dark on ADC map. In this case there is greater than 50% myometrial invasion.
T2 T1-post B=0 B=500 ADC

Depth of myometrial invasion is optimally seen on T2-wt images and DWI images
Appearance of Endometrial Cancer
GUCXM3
T2 A
Figure: (A) Sagittal T2-weighted image of the deepest extent of myometrial invasion. Measure the depth of myometrial invasion by drawing a line along the expected inner edge of the myometrium. Then draw lines measuring the thickness of the entire myometrium and the extent of tumor invasion in to the myometrium. The ratio of the black line over the white line is the percentage of MI. (B) B=0, B=500, and ADC map depicting the tumor. Use the DWI image to aid in your measurement and help find the deepest extent of MI ( ).
B

Stage IA
Figure: Sagittal T2-wt, T1-post contrast and diffusion weighted images in a 68 y/o female with Stage IA endometrial cancer. The abnormal signal intensity on the T2-wt image is confined to the endometrium ( ). There is preservation of the junctional zone ( ) and no evidence of myometrial invasion. The mass restricts diffusion ( ) on the ADC map.
Figure: Sagittal T2-wt and T1-post contrast images in a 64 y/o female with Stage IA endometrial cancer. There is focal abnormal T2 signal intensity involving the endometrium (*). There is disruption of the junctional zone anteriorly and posteriorly in the region of the body with less than 50% myometrial invasion ( ). No cervical invasion.
Stage 1 tumors account for over 80% of cases Abnormal signal intensity on T2-wt images confined to the endometrium as
well as tumor that invades less than 50% of the myometrium
T2 T2 T1-post T1-post
B=0 B=500 ADC
*

Stage IB
Figure: T2-wt and T1-post contrast images in a 59 year old female with Stage IB endometrial cancer. The abnormal signal intensity on the T2-wt images involves greater than 50% of the myometrium ( ). T1-post contrast images provide tumor to myometrium contrast and demonstrates the hypoenhancement of the tumor ( ) relative to the adjacent myometrium.
T2 T1-post

Direct invasion of the cervical stroma
Tumor demonstrates intermediate to high signal intensity on T2-wt images that disrupts the normal low signal intensity cervical stroma
Radical hysterectomy is required for these patients as opposed to total abdominal hysterectomy in earlier stage patients
Lymphadenectomy is also performed at many institutions in these patients
Stage II
GUCXM3
Figure: T2-wt and T1-post contrast images in a 51 year old female with Stage II endometrial cancer. There is a lobulated T2 hyperintense non-enhancing mass along the posterior uterine wall in the lower uterine segment ( ). The mass splays open the endocervical canal ( ) and extends into the hypointense cervical stroma ( ).
T2 T1-post

IIIA Invasion of uterine serosa or adnexa
IIIB Invasion into upper vagina or parametrium
IIIC-Enlarged regional lymph nodes IIIIC1-pelvic lymph node involvement IIIIC2-paraortic lymph node involvement
IVA Bladder or rectal wall invasion
IVB Distant metastasis Lymphadenopathy above the renal vein,
malignant ascites or peritoneal carcinomatosis
Imaging features of lymph node metastasis Size criteria > 1 cm in short axis diameter Rounded or irregular contour Multiplicity Central necrosis Diffusion restriction Hypermetabolic activity on PET However, metastasis can be present in normal
sized lymph nodes!
Stage III and IV
Figure: Axial T2-wt and T1-post contrast images in a 56 year old female with stage IIIC1 endometrial cancer. There is an enlarged 1.5 cm rounded left external iliac lymph node present ( ). Notice there is an area of intermediate signal in the endometrial canal on the T2-wt image ( ), which is seen to subtly enhance on the T1-post image ( ) .
T2
T1-post

Fibroid
Adenomyosis Polyp
Endometrial hyperplasia
Benign mimics of Endometrial Cancer
GUCXM3

Fibroid
GUCXM3
Figure: Sagittal T2-wt, T1-post contrast and diffusion weighted images demonstrating two large fibroids ( , ) , one of which is degenerating ( ). Fibroids typically demonstrate low T1 and T2 signal and heterogeneous enhancement; however, degenerating fibroids demonstrate increased T2 signal intensity. Typical fibroids will be dark on B=0, B=500 and the ADC map. Degenerating fibroids will be bright on the B=0 and B=500, having a variable appearance on the ADC map .
T2 T1-post B=0 B=500 ADC

Adenomyosis
Figure: Sagittal T2-wt and diffusion weighted images in a 45 year old female with adenomyosis ( ) and concurrent endometrial cancer ( ). Adenomyosis is defined as the presence of heterotopic endometrial glands and stroma in the myometrium with adjacent smooth muscle hyperplasia. MRI imaging features include diffuse widening of the junctional zone with bright T2 foci within the junctional zone (corresponds to heterotopic endometrial tissue); both of these findings are seen in this case. PITFALL: In patients with coexistent endometrial cancer and adenomyosis, myometrial invasion is often overestimated leading to staging errors. In this case, less than 50% myometrial invasion was called on MRI and pathology demonstrated no myometrial invasion.
B=0 B=500 ADC T2

Polyp
GUCXM3
Figure: Sagittal T2-wt, T1-post contrast and diffusion weighted imaging in a 55 year old female demonstrating a polyp in the endometrial canal ( ). Polyps can demonstrate low T2 signal intensity secondary to the central fibrous core. However polyps can also contain glandular secretions and cystic areas and therefore can also demonstrate high T2 signal. Polyps enhance briskly and sometimes have a “lace-like” appearance on the post-contrast images. When polyps are dark on the T2-wt images, they are dark or isointense on B=0, B=500 and ADC map compared with endometrium. When polyps display high signal on T2-weighted images, they will follow the endometrium on B=0, B=500 and ADC map. PEARL: Diffusion weighted imaging is key, polyps won’t restrict diffusion while endometrial cancer will.
T2 T1-post B=0 B=500 ADC

Endometrial hyperplasia
GUCXM3
Figure: Same case! There is concurrent endometrial hyperplasia ( ) in the canal. PEARL: The appearance of the tissue surrounding the polyp ( ) is T2 bright and is bright on B=0, B=500 and ADC map, typical of endometrial hyperplasia. Endometrial hyperplasia does not restrict diffusion.
T2 T1-post B=0 B=500 ADC

Same patient…keep looking
GUCXM3
Figure: Sagittal T2-wt, T1-post and diffusion weighted images again in the same patient, now to the right of midline. The patient also has concurrent endometrial cancer ( ). The round area within the fundus demonstrates T2 hyperintensity, minimal enhancement, slight hypointensity compared to endometrium on B=0, becomes bright on B=500, and is dark on the ADC map. This is consistent with endometrial cancer. Adjacent hyperplastic endometrium is bright on B=0, B=500 and ADC ( ). This was proven on surgical pathology.
T2 T1-post
B=0 B=500 ADC

Concurrent endometrial cancer, hyperplasia and polyp
GUCXM3
Figure: Axial T2-wt, T1-post-contrast and diffusion weighted images depict all three entities in one plane. Endometrial hyperplasia ( ) is hyperintense to myometrium on T2-wt images and is bright on all DWI images and the ADC map. Endometrial cancer ( ) and the polyp ( ) are isointense to myometrium on the T2-wt images and enhance on post contrast images. The endometrial cancer becomes brighter on the B=500 image and darker on the ADC map. The endometrial polyp remains dark on all DWI images and ADC map. These findings were confirmed on surgical pathology.
T2 T1-post
B=0 B=500 ADC

MRI is excellent at depicting uterine anatomy and assessing endometrial cancer. Tumor size and extension Myometrial invasion Parametrial/cervical invasion Lymphadenopathy
Although currently endometrial cancer is staged surgically,
MRI does play a critical role in pre-operative planning.
Differentiating endometrial cancer from co-existing endometrial hyperplasia, adenomyosis, fibroids, and polyps is important in the accurate assessment of endometrial cancer.
Summary

• ASTEC study group, Kitchener H, SwartAM, Qian Q, Amos C, Parmar MK. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomized study. Lancet 2009;373(9658):125–136.
• Beddy P, Ailbhe D, O’Neill MB, Yamamoto A, Addley H, Reinhold C. Sala E. FIGO Staging System for Endometrial Cancer: Added Benefits of MR Imaging. Radiographics 2012; 32:241-254
• Beddy P, Moyle P, Kataoka M, et al. Evaluationof depth of myometrial invasion and overall staging in endometrial cancer: comparison of diffusion-weighted and dynamic contrast-enhanced MR imaging. Radiology2012;262(2):530–537.
• Berman ML, Ballon SC, Lagasse LD, Watring WG. Prognosis and treatment of endometrial cancer. Am J Obstet Gynecol 1980;136(5):679–688.
• Duncan KA, Drinkwater KJ, Frost C, Remedios D, Barter S. Staging cancer of the uterus: a national audit of MRI accuracy. Clin Radiol 2012;67(6):523–530.
• Larson DM, Connor GP, Broste SK, Krawisz BR, Johnson KK. Prognostic significance of gross myometrial invasion with endometrial cancer. Obstet Gynecol 1996;88(3):394–398.
• Manfredi R, Mirk P, Maresca G, et al. Local-regional staging of endometrial carcinoma: role of MR imaging in surgical planning. Radiology 2004;231(2):372–378.
• Murase E, Siegelman E, Outwater E, Perez-Jaffe L, Tureck R. Uterine Leiomyomas: Histopathologic Features, MR Imaging Findings, Differential Diagnosis and Treatment. September 1999. Radiographics, 19, 1179-1197
• Nalaboff K, Perllerito J, Ben-Levi E. Imaging the Endometrium: Disease and Normal Variants. Radiographics. November 2001; 21; 1409-1424
• National Comprehensive Cancer Network: Uterine neoplasms. NCCN clinical practice guidelines in oncology. Version 3. Fort Washington, Pa: National Comprehensive Cancer Network, 2012.
• Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet 2009;105(2):103–104.
• Reinhold C, Tafazoli F, Mehio A, Wang L, Atri M, Siegelman E, Rohoman L. Uterine Adenomyosis: Endovaginal US and MR Imaging Features with Histopathologic Correlation. October 1999 Radiographics, 19, S147-S160
• Sala E. Rockall A,G Freeman SJ, Mitchell D, Reinhold C. The Added Role of MR Imaging in Treatment Stratification of Patients with Gynecologic Malignancies: What the radiologist needs to know. Radiology March 2013 266(3) 717-740
• Sala E, Wakely S, Senior E, Lomas D. MRI of malignant neoplasms of the uterine corpus and cervix. AJR Am J Roentgenol 2007;188(6):1577–1587.
• Siegelman E. Body MRI. Saunders 2005
• Todo Y, Kato H, Kaneuchi M, Watari H,Takeda M, Sakuragi N. Survival effect of para-aortic lymphadenectomy in endometrial cancer (SEPAL study): a retrospective cohort analysis. Lancet 2010;375(9721):1165–1172.
Sources

Questions or Comments? Please feel free to contact us at [email protected] or [email protected].
Contact Information
THANK YOU FOR YOUR ATTENTION!