Pre- and Perinatal Risk for Attention-Deficit ...€¦ · Pre- and Perinatal Risk for...
13
Pre- and Perinatal Risk for Attention-Deficit Hyperactivity Disorder: Does Neuropsychological Weakness Explain the Link? Kelsey Wiggs 1 & Alexis L. Elmore 1 & Joel T. Nigg 2 & Molly A. Nikolas 1 # Springer Science+Business Media New York 2016 Abstract Etiological investigations of attention-deficit hy- peractivity disorder (ADHD) and disruptive behavior prob- lems support multiple causal pathways, including involve- ment of pre- and perinatal risk factors. Because these risks occur early in life, well before observable ADHD and exter- nalizing symptoms emerge, the relation between risk and symptoms may be mediated by neurodevelopmental effects that manifest later in neuropsychological functioning. However, potential dissociable effects of pre/perinatal risk el- ements on ADHD and familial confounds must also be con- sidered to test alternative hypotheses. 498 youth aged 6– 17 years (55.0 % male) completed a multi-stage, multi- informant assessment including parent and teacher symptom reports of symptoms and parent ratings of pre/perinatal health risk indicators. Youth completed a neuropsychological testing battery. Multiple mediation models examined direct effects of pre- and perinatal health risk on ADHD and other disruptive behavior disorder symptoms and indirect effects via neuropsy- chological functioning. Parental ADHD symptoms and exter- nalizing status was covaried to control for potential familial effects. Effects of prenatal substance exposure on inattention were mediated by memory span and temporal processing def- icits. Further, effects of perinatal health risk on inattention, hyperactivity-impulsivity, and ODD were mediated by defi- cits in response variability and temporal processing. Further, maternal health risks during pregnancy appeared to exert direct rather than indirect effects on outcomes. Results suggest that after controlling for familial relatedness of ADHD be- tween parent and child, early developmental health risks may influence ADHD via effects on neuropsychological pro- cesses underpinning the disorder. Keywords Attention deficit hyperactivity disorder . Neuropsychological dysfunction . Prenatal risk Attention-deficit hyperactivity disorder (ADHD) is character- ized by developmentally inappropriate and impairing difficul- ties with inattention, hyperactivity, and impulsivity (American Psychiatric Association 2013). Etiological investigations of ADHD have implicated moderate to large genetic contribu- tions (Knopik et al. 2005; Nikolas and Burt 2010). Substantial evidence also supports multiple causal pathways involving interplay among genetic and environmental factors (Nigg et al. 2010). Due to their potential impact on brain development and subsequent neural function, pre- and perinatal health factors have been evaluated in relation to ADHD (Ernst et al. 2001; Gurevitz et al. 2014; Hofhuis et al. 2003). For example, low birth weight (LBW) robustly predicts ADHD symptoms (Langley et al. 2007; Nigg and Breslau 2007). Other relevant pre- and perinatal health risks include maternal stress during pregnancy (Bielas et al. 2014; Van den Bergh and Marcoen 2004), prenatal substance use (Ernst et al. 2001; Nigg and Breslau 2007), and perinatal complications (D’Onofrio et al. 2013). However, these risks are often correlated and, impor- tantly, it is unclear whether critical effects on ADHD risk occur prenatally or perinatally (or both). Despite the high co-occurrence of ADHD and other externalizing disorders, past research has hypothesized a potential dissociation of prenatal health risks and ADHD * Molly A. Nikolas [email protected] 1 Department of Psychological and Brain Sciences, University of Iowa, 11 Seashore Hall E., Iowa City, IA 52242, USA 2 Department of Psychiatry, Oregon Health and Science University, 3181 SW Sam Jackson Park Rd, Portland, OR 97239-3098, USA J Abnorm Child Psychol DOI 10.1007/s10802-016-0142-z
Transcript of Pre- and Perinatal Risk for Attention-Deficit ...€¦ · Pre- and Perinatal Risk for...

Pre- and Perinatal Risk for Attention-DeficitHyperactivity Disorder: Does Neuropsychological WeaknessExplain the Link?
Kelsey Wiggs1 & Alexis L. Elmore1 & Joel T. Nigg2 & Molly A. Nikolas1
# Springer Science+Business Media New York 2016
Abstract Etiological investigations of attention-deficit hy-peractivity disorder (ADHD) and disruptive behavior prob-lems support multiple causal pathways, including involve-ment of pre- and perinatal risk factors. Because these risksoccur early in life, well before observable ADHD and exter-nalizing symptoms emerge, the relation between risk andsymptoms may be mediated by neurodevelopmental effectsthat manifest later in neuropsychological functioning.However, potential dissociable effects of pre/perinatal risk el-ements on ADHD and familial confounds must also be con-sidered to test alternative hypotheses. 498 youth aged 6–17 years (55.0 % male) completed a multi-stage, multi-informant assessment including parent and teacher symptomreports of symptoms and parent ratings of pre/perinatal healthrisk indicators. Youth completed a neuropsychological testingbattery. Multiple mediation models examined direct effects ofpre- and perinatal health risk on ADHD and other disruptivebehavior disorder symptoms and indirect effects via neuropsy-chological functioning. Parental ADHD symptoms and exter-nalizing status was covaried to control for potential familialeffects. Effects of prenatal substance exposure on inattentionwere mediated by memory span and temporal processing def-icits. Further, effects of perinatal health risk on inattention,hyperactivity-impulsivity, and ODD were mediated by defi-cits in response variability and temporal processing. Further,maternal health risks during pregnancy appeared to exert
direct rather than indirect effects on outcomes. Results suggestthat after controlling for familial relatedness of ADHD be-tween parent and child, early developmental health risksmay influence ADHD via effects on neuropsychological pro-cesses underpinning the disorder.
Keywords Attention deficit hyperactivity disorder .
Neuropsychological dysfunction . Prenatal risk
Attention-deficit hyperactivity disorder (ADHD) is character-ized by developmentally inappropriate and impairing difficul-ties with inattention, hyperactivity, and impulsivity (AmericanPsychiatric Association 2013). Etiological investigations ofADHD have implicated moderate to large genetic contribu-tions (Knopik et al. 2005; Nikolas and Burt 2010). Substantialevidence also supports multiple causal pathways involvinginterplay among genetic and environmental factors (Nigg etal. 2010).
Due to their potential impact on brain development andsubsequent neural function, pre- and perinatal health factorshave been evaluated in relation to ADHD (Ernst et al. 2001;Gurevitz et al. 2014; Hofhuis et al. 2003). For example, lowbirth weight (LBW) robustly predicts ADHD symptoms(Langley et al. 2007; Nigg and Breslau 2007). Other relevantpre- and perinatal health risks include maternal stress duringpregnancy (Bielas et al. 2014; Van den Bergh and Marcoen2004), prenatal substance use (Ernst et al. 2001; Nigg andBreslau 2007), and perinatal complications (D’Onofrio et al.2013). However, these risks are often correlated and, impor-tantly, it is unclear whether critical effects on ADHD riskoccur prenatally or perinatally (or both).
Despite the high co-occurrence of ADHD and otherexternalizing disorders, past research has hypothesized apotential dissociation of prenatal health risks and ADHD
* Molly A. [email protected]
1 Department of Psychological and Brain Sciences, University ofIowa, 11 Seashore Hall E., Iowa City, IA 52242, USA
2 Department of Psychiatry, Oregon Health and Science University,3181 SW Sam Jackson Park Rd, Portland, OR 97239-3098, USA
J Abnorm Child PsycholDOI 10.1007/s10802-016-0142-z

versus other externalizing disorders. Nigg and Breslau (2007)found that LBW specifically predicted ADHD symptoms(with prenatal tobacco exposure covaried), whereas prenataltobacco exposure (with birth weight covaried) specificallypredicted oppositional defiant disorder (ODD) and conductdisorder (CD) symptoms. Similarly, Langley et al. (2007) re-ported that prenatal tobacco exposure significantly predictedCD, apart from effects on hyperactivity-impulsivity, suggest-ing that prenatal tobacco exposure may relate to ADHD solelyvia its impact on externalizing behaviors. However, this workdid not find a connection between LBW and ADHD, thusproviding only limited support for potential dissociation ofeffects. Overall, the high degree of correlation among riskfactors and mixed results regarding specificity of associationsbetween individual risk factors and externalizing syndromeswarrants further investigation.
Importantly, prior work examining pre- and perinatal healthrisk for ADHD has often failed to consider the impact offamilial confounds, including the role of parental ADHD.Associations between pre- and perinatal risk and ADHDmay partially reflect shared genes between parents and chil-dren (gene-environment correlation, rGE; Rice et al. 2010).For example, mothers with ADHD may be more likely tosmoke during pregnancy (Zhu et al. 2014), leading to a spu-rious environmental association between prenatal tobacco ex-posure and ADHD that may in fact be due to rGE (Altink et al.2009; Thapar et al. 2009) or another genetically-mediatedprocess. Thus, it remains critical for future work to considerthe potential confounding role of familial factors.
Pre- and perinatal risk may exert effects via disruption ofneurodevelopment, which then manifests in subsequent neu-ropsychological dysfunction in children with ADHD (Piperand Corbett 2012). Deficits in both executive functions andnon-executive processes have been well-documented amongyouth with ADHD (Nikolas and Nigg 2013; Willcutt et al.2005). Further, prenatal substance exposure and LBW influ-ence neural functioning in brain regions purported to underlieADHD symptoms (Ernst et al. 2001; Faraone and Biederman1998). For example, impulsive symptoms may stem from de-ficient reward processing underpinned by connections amongorbitofrontal and striatal regions (Wilbertz et al. 2012), whichappear to be affected by pre- and perinatal risk (Diwadkar etal. 2013; Derauf et al. 2012). Thus, pre- and perinatal healthmay indirectly influence risk for ADHD and other disruptivebehavior disorders, such that early insults influence the devel-opment of cortico-striatal circuitry, resulting in neuropsycho-logical dysfunction and subsequently increasing liability forADHD and/or other disruptive behavior problems. Hatch et al.(2014) recently demonstrated that primary neuropsychologi-cal functioning (defined as visuo-spatial perception and motorcoordination) mediated associations between birth weight andADHD symptoms. However, while innovative, this work didnot consider potential differential effects of pre- and perinatal
health risk on ADHD versus disruptive behavior disorders(Nigg and Breslau 2007), other potentially relevant indicatorsof risk (e.g., teratogen exposure, complications during preg-nancy and/or delivery, perinatal health), or familial confounds(i.e., potential impact of shared genetic and environmentalfactors).
The primary aim of the current study was to further developrecent work by Hatch et al. (2014) by examining direct andindirect effects of multiple pre- and perinatal risk factors onADHD and other disruptive behavior disorder symptoms vianeuropsychological dysfunction within a multiple mediationframework. We predicted that pre and perinatal health riskswould exert indirect effects on ADHD and other externalizingbehaviors via their influence on neuropsychological function-ing. Secondary aims to extend prior work included (1) statis-tical control for familial confounds, (2) incorporating compre-hensive measures of pre- and perinatal health risks dissociat-ing birth weight and teratogen exposure, (3) examining mul-tiple measures of neuropsychological processes, and (4) dif-ferentiating effects on ADHD versus co-occurring disruptivebehavior disorder outcomes.
Method
Participants
Participants were 498 children and adolescents ages 6 to17 years (M=10.8, SD=2.3, 55.0 % male). The sample, orig-inally recruited to examine genetic and endophenotype effectsfor ADHD, included 205 sibling pairs and 88 singletons.Participants were recruited using mass mailings to parents inlocal school districts, public advertisements, and communityoutreach to local clinics to recruit a broad sample whileavoiding potential biases inherent to purely clinic-referredsamples. A multi-stage, multi-informant assessment proce-dure was used to identify cases and non-cases. 902 individualchildren from 762 families completed the stage 1 initial tele-phone screen, which evaluated potential rule-outs, includingphysical handicap, non-native English speaking, history ofintellectual disability, autistic disorder, and prescription oflong-active psychoactive medications (e.g., atomoextine,buproprion). 724 individual children from 588 families werethen invited to complete stage 2 diagnostic assessment, whichincluded parent and teacher ratings on the DSM-IV ADHDRating Scale (DuPaul et al. 1998), and the Conners’ RatingScale –Revised Short Form (Conners 1997). Parents complet-ed the Kiddie Schedule for Affective Disorders andSchizophrenia-E (Puig-Antich and Ryan 1986) for each childwith a trained master’s level clinical interviewer. A three-subtest version of the Wechsler Intelligence Scale forChildren, 4th edition (WISC-IV; Wechsler 2003) was admin-istered to youth at this stage to estimate full scale IQ.
J Abnorm Child Psychol

Clinical data were reviewed and a best estimate diagnosticprocedure was implemented by a board-certified child psychi-atrist and a licensed child clinical psychologist. Both profes-sionals used a symptom count or algorithm from parent andteacher reports (i.e., symptom counted as present if endorsedby parent or teacher) as well as T-scores for both parent andteacher ratings on the Conners’ Cognitive Problems orHyperactivity Problems subscales (t-scores > 60 consideredclinically significant). Clinical decisions concerning ADHD,ADHD subtype, and comorbid diagnoses were made indepen-dently, using full DSM-IV-TR criteria. Agreement rates wereacceptable for all ADHD subtype diagnoses (κ>0.88) and allanxiety, mood, and disruptive behavior disorders occurring ata 5 % or more base rate in the sample (all κ>0.70).
Following the diagnostic assessment, youth were then in-vited to complete the stage 3 neuropsychological assessment,provided they were not identified for exclusion based on thefollowing criteria. Youth were excluded if the diagnostic teamidentified intellectual disability (defined as full-scale IQ<75,n=3 excluded), head injury with a loss of consciousness (n=8excluded), history of seizures as ascertained by parent report(n=5 excluded), or if youth met criteria on the KSADS-E forautism spectrum disorders (n=18 excluded), current majordepressive episode (n = 57 excluded), lifetime psychosis(n=5 excluded), or current substance abuse or dependence(n=5 excluded).
Of the 724 youth completing the diagnostic screen, 623qualified for the follow-up neuropsychological testing visit.Of these, 498 youth from 295 families completed the stage 3neuropsychological testing battery, on a separate day follow-ing the diagnostic visit (see below). There were no significantdifferences between those who participated in the stage 3 as-sessment (n = 498) and those who elected not to return(n=125) in regard to sex, age, ADHD severity and income(ps >0.26). The final sample included 251 youth with ADHDand 213 non-ADHD youth. 34 youth had subthreshold orsituational ADHD symptoms – these youth were excludedfor group comparisons but included in all dimensional medi-ation analyses. 37.4 % of participants who met criteria forADHD were prescribed stimulant medication (consistentwith expectations for community samples; Jensen et al.2001). Youth currently taking stimulant medication completeda minimum washout period of 24 h for short-acting prepara-tions and 48 h for long-acting preparations (range 24–152 h,mean=58 h) before completing neuropsychological testing,which occurred approximately 4 weeks after the diagnosticassessment (mean time between visits = 4.2 weeks,SD=3.2). Eligible participants using longer-acting psychoac-tive prescription medications (including atomextine andguanfacine) were excluded (2 %). Parents provided informedconsent for themselves and their child; youth provided writtenassent. All procedures were approved by the Michigan StateUniversity Institutional Review Board.
Measures
Neuropsychological Functioning
The battery of tests employed was organized to capture mul-tiple neuropsychological functions implicated in ADHD. Alist of measures and their associated constructs are presentedin Table 1. Tests measuredworking memory (Martinussen andTannock 2006), memory span, response inhibition (Barkley1997), processing speed, response variability (Karalunas et al.2014), temporal processing (Noreika et al. 2013; Toplak andTannock 2005), and arousal (or activation; operationalized assignal detection sensitivity; Sergeant 2005). All youth com-pleted the same battery of tests, which were administered in afixed order. Internal consistencies for each of the measureswere adequate (αs ranging from 0.85 to 0.97, calculated basedon non-ADHD participants only). Past research hasestablished evidence of construct, convergent, and discrimi-nant validity for several of the measures (Assesmany et al.2001; Delis et al. 2001; Logan 1994; Martinussen andTannock 2006; Toplak and Tannock 2005). Validity checksconducted for each measure indicated that invalid data wererare overall (less than 5 % on any one task) and presence ofinvalid data was unrelated to ADHD diagnostic status, age,and sex (all ps > 0.15; see Nikolas and Nigg 2013 for adetailed explanation of chosen measures and associatedvalidity criteria).
ADHD and Comorbid Disruptive Behavior Problems
Parent and teacher ratings on the ADHD Rating Scale(DuPaul et al. 1998) constituted the main outcome measure.Parents and teachers rated the frequency of all 18 DSMADHD symptoms on a 4-point Likert Scale (never, some-times, often, very often). Notably, parents and teachers wereinstructed to rate their child’s behavior off of medication, ifthey had observed such instances. Internal consistencies wereadequate for ratings of inattention (parent α=0.93; teacherα = 0.91) and hyperactivity-impulsivity (parent α = 0.90;teacher α= 0.88). Additionally, parent-reported ODD andCD symptoms were assessed with the KSADS-E (α=0.87ODD; α=0.85 CD), whereas teachers rated these behaviorsusing a measure similar to the ADHD Rating Scale. Itemsrated by teachers as occurring Boften^ or Bvery often^ werecounted as symptoms (α=0.86 ODD; α=0.81 CD). To re-duce the number of statistical tests required to achieve ouraims while maximizing data collected from multiple infor-mants, scores were averaged across informant for each symp-tom dimension (e.g., inattention, hyperactivity-impulsivity,ODD, and CD), based on recent work indicating that averagecomposite scores best predicted ADHD diagnosis when com-pared to other methods of combining across informants(Martel et al. 2015). Standard scores were averaged across
J Abnorm Child Psychol

informant for inattention and hyperactivity-impulsivity.Because assessment ODD and CD symptoms relied on differ-ent measures for parents versus teachers, we first created z-scores within informant and then took the average of parentand teacher z-scores. Cross-informant correlations for thesesymptom dimensions ranged from r=0.41 to r=0.58. Theseaverage composites were retained as the four primary out-comes in subsequent mediation models.
Parental Psychopathology
Primary parents provided ratings regarding current ADHDsymptoms for themselves and their child’s other biologicalparent on the Barkley and Murphy (2006) Adult ADHDRating Scale. Individuals rated the presence of each of the18 DSM-items on a 4-point Likert scale (never, sometimes,often, very often). Internal consistencies were adequate forboth self-report (inattention α = 0.90, hyperactivity-impulsivity α=0.86) and other reports (inattention α=0.87,hyperactivity-impulsivity α=0.81). A sum score was createdfor each parent, standardized, and then averaged to create anindex of parental ADHD symptoms. Primary parents also in-dicated positive family history of other externalizing disordersas part of the developmental history questionnaire (see be-low). This included if the child’s biological mother and/orfather have had a confirmed or suspected diagnosis of alco-holism or other form of substance abuse/dependence, or ahistory of delinquency, conduct, or legal problems. Items werescored to determine parental externalizing disorder (yes/no)status. These variables were included as covariates in all
analyses to account for associations between pre/perinatalhealth risk and child psychopathology potentially attributableto relatedness among families.
Pre- and Perinatal Risk Factors
A comprehensive developmental history questionnaire wascompleted for each youth by their primary caregiver (n=454mothers, n=44 fathers) to assess three aspects of early childhealth– prenatal substance exposure, maternal health duringpregnancy, and child perinatal health risk. This included sev-eral questions regarding the health and behavior of themothers during pregnancy and delivery as well as questionsregarding the health of the children during delivery and afterbirth. Prenatal substance exposure was assessed by havingparents indicate whether mothers used tobacco, alcohol, and/or recreational drugs during pregnancy. Maternal health dur-ing pregnancy comprised questions assessing the presence ofseveral illnesses during pregnancy, including toxemia, gesta-tional diabetes, preeclampsia, placenta previa, high bloodpressure, chronic infections, influenza, marked swelling ofhands and feet, convulsions, frequent headaches, and/or ab-dominal pain. Parents also indicated any additional maternalhealth issues during pregnancy not covered on the question-naire (most frequent responses including hyperemesis, spot-ting/bleeding, injuries/accidents) and reported the presenceand frequency of additional exposures during pregnancy, in-cluding x-rays, prescription medications (most common pre-scription medications used were for asthma, allergies, andanxiety/depression), and presence of significant emotional
Table 1 Neuropsychologicaltasks and measures, constructs,and factors
Task & Measure Construct First order factor
Spatial Span Forward Total Correct Encoding, span Memory spana
Spatial Span Backward Total Correct Working memory Working memorya
Digit Span Forward Total Correct Encoding, span Memory spana
Digit Span Backward Total Correct Working memory Working memorya
DKEFS Color-Word Color/Word Reading Time Speeded naming Processing speed
DKEFS Color-Word Inhibition Time Interference control Inhibitiona
DKEFS Inhibition/Switching time Switching speed Inhibitiona
DKEFS Trailmaking Number Sequencing Time Sequencing speed Processing speed
DKFES Trailmaking Number-Letter Sequencing Time Switching speed Working memorya
Stop Task Stop Signal Reaction Time Response inhibition Inhibitiona
Stop Task Reaction Time Variability Response time variability Response variability
Continuous Performance Task d-prime Arousal/activation Arousal
Tapping Task Visual 400-ms detrended SD Time reproduction Temporal processing
Tapping Task Auditory400-ms detrended SD Time reproduction Temporal processing
Tapping Task Visual 1000-ms detrended SD Time reproduction Temporal processing
Tapping Task Auditory 1000-ms detrended SD Time reproduction Temporal processing
DKEFS Delis-Kaplan Executive Function System, SD standard deviationa Factor significantly loaded on 2nd order cognitive control factor (Nikolas and Nigg 2013, 2015)
J Abnorm Child Psychol

stressors (e.g., frequent conflict with partner, divorce, loss ofemployment).
Labor and delivery characteristics were also assessed togauge perinatal health risks. These included the gestationalage at the time of delivery (number of weeks), the type ofdelivery (uncomplicated vaginal versus Caesarian or forceps),the length of labor (in hours), and the child’s birth weight (inounces). Further, the presence or absence of additional childhealth problems during delivery and immediately followingbirth were also assessed, including use of an incubator, heartand respiratory problems, jaundice, low Apgar score, meconi-um aspiration, and umbilical cord prolapse. Parents also indi-cated occurrence of any additional complication or health dif-ficulty not included on the questionnaire (most common re-sponses included infant temperature instability followingbirth, infections, and hernias). Parents also provided informa-tion regarding their age at each child’s birth, given the robustassociation between parental age and pre and perinatal healthrisks (Cleary-Goldman et al. 2005; Najati and Gojazadeh2010) as well as between parental age and ADHD (Chudalet al. 2015). Differences among ADHD and non-ADHDyouth across all of the pre- and perinatal health indicators aswell as in parental age at birth are presented in Table 2.
Data Reduction
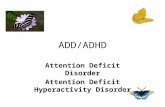
Data reduction for all pre- and perinatal health indicatorswas accomplished via confirmatory factor analyses (CFA).Given that the health and family background questionsconcerning pre- and perinatal health were developed to as-sess three broad domains (i.e., prenatal substance exposure,maternal health during pregnancy, and perinatal health in-dicators), a three-factor model determined a priori wasfitted to the data. Because several indicators were categor-ical or count variables and missingness was minimal(<1 %), weighted least-squares with mean and varianceadjustment estimation procedures (WLSMV) and theta pa-rameterization were utilized (note – gestational age andbirth weight were reversed scored so that all items hadthe same valence). Fit statistics indicated acceptable modelfit of the three-factor model (χ2=50.38, df=25, CFI=0.96,RMSEA=0.046, [0.027, 0.064]). Factor scores were thenderived for each individual for each of the three factorsusing a regression-based approach. These scores wereretained as predictors in all of the subsequent mediationanalyses. Factor loadings and correlations between factorsare depicted in Fig. 1.
Table 2 Descriptive anddemographic statistics Control ADHD p-value
N 213 251
% Male 42.3 66.9
Age (SD) 11.0 (2.4) 10.5 (2.3) 0.021
% Caucasian 76.5 72.1 0.64
Incomea (SD) 79.0 (47.4) 64.5 (38.7) 0.002
Inattention Symptoms (SD) 0.74 (1.4) 7.2 (1.9) <0.001
Hyperactivity-Impulsivity Symptoms (SD) 0.62 (1.2) 4.3 (2.9) <0.001
% ODD (lifetime) 14.1 41.6 <0.001
% CD (lifetime) 0.5 8.4 <0.001
% Parent with ADHD 17.4 31.1 <0.001
% Parent with Externalizing Disorder 8.5 13.5 0.083
% Tobacco Use During Pregnancy 14.9 22.7 0.036
% Alcohol Use During Pregnancy 10.9 12.6 0.59
% Drug Use During Pregnancy 3.6 5.0 0.49
% Mothers with Illness During Pregnancy 33.7 46.2 0.007
% Mothers with Severe Emotional Stress 18.8 31.5 <0.001
% Mothers Exposed to X-Ray 3.8 3.2 0.68
% Mothers Taking Prescription Medication 28.6 37.1 0.098
% Born 36 Weeks Gestation or Less 12.9 18.6 0.098
Length of labor (hours) 13.0 (12.3) 12.7 (26.4) 0.90
Birth Weight (oz) 125.2 (23.3) 118.9 (23.5) 0.006
% Children with Perinatal Difficulty 26.7 32.0 0.23
Values denote means and standard deviations of key variables
CD conduct disorder, ODD oppositional defiant disordera Income reported in thousands
J Abnorm Child Psychol

Neuropsychological factor scores from prior factor analyticwork were also utilized (see Nikolas and Nigg 2013, 2015).To create these factor scores, a series of confirmatory factoranalyses were conducted, which included evaluation ofmodels comprised of one through eight factors as well asseveral second-order factor models. The final second-ordermodel provided a good fit to the data (χ2 = 94.88, df = 60,CFI=0.98, TLI=0.98, RMSEA=0.034). This model includ-ed seven lower-order factors labeled as response inhibition,working memory, memory span, speed, response variability,arousal, and temporal processing as well as one second-orderfactor termed cognitive control. This second-order factor wascomprised of the inhibition, working memory, and memoryspan factors (see Table 1 for breakdown of how each measureloaded on each respective factor).
Data Analysis
Associations between outcome variables and predictor andmediating variables were examined via bivariatecorrelations. Tests of direct and indirect effects were basedon methodology by Preacher and Hayes (2008) using fullinformation maximum likelihood techniques to address miss-ing data. A series of mediation models were examined thatincluded (1) prenatal exposures, (2) maternal health risk fac-tors, and (3) perinatal health risk factors as separate predictorvariables. Composite scores for inattention, hyperactivity,ODD, and CD served as outcomes. The neuropsychologicalfactor scores (Nikolas and Nigg 2013) were examined simul-taneously as statistical mediators of the association betweenpre- and perinatal health risk and each outcome. Both the totalindirect effects and the point estimates for each pathway areestimated using this procedure. Sex, age, ethnicity, income,parental ADHD symptoms and externalizing disorder status,and maternal and paternal age at birth were included as
covariates in all models. Missing data was generally low(<3.2 %, with the exception of income, which was missingfor 9.4 % of the sample). Lastly, given the clustered nature ofthe sibling data, the CLUSTER option in MPlus was used toaccount for non-independence issues (Muthén and Muthén1998–2015). Further, delta method standard errors were com-puted, as bootstrapped confidence intervals could not be com-puted with clustered data.
Results
Demographic and Descriptive Statistics
Results indicated that diagnostic procedures effectively dis-criminated the ADHD from the control group (see Table 2).Significant differences emerged in regard to child sex, age,income, and parental psychopathology; all were included ascovariates in the models in addition to ethnicity, which wasincluded due to indications of variation in ODD symptoms,CD symptoms, and birth weight by ethnicity. A higher pro-portion of youth in the ADHD group was exposed to tobaccoprenatally and mothers of ADHD youth were more likely tohave health problems or experience significant emotionalstress during pregnancy relative to control mothers. Birthweight was also significantly lower among ADHD youthcompared to their non-ADHD counterparts (p = 0.002,Cohen’s d=0.28). Additionally, statistically reliable groupdifferences emerged across each of the pre- and perinatalhealth factor scores, such that youth with ADHD had higherscores on the prenatal substance exposure (p=0.02; d=0.28),maternal health risk (p<0.001, d=0.38), and perinatal healthrisk (p=0.001, d=0.30) factors. Maternal and paternal age atbirth did not differ across groups (ps>0.48), but maternal ageat birth was significantly correlated with all three pre- and
Fig. 1 Three factor model of pre-and perinatal health indicators.All loadings significant atp< 0.01. ** Indicates correlationsignificant at p < 0.01. Error termsare not included here to preservefigure clarity
J Abnorm Child Psychol

perinatal health factor scores, such that younger maternal agewas associated with increased scores on prenatal substanceexposure (r=−0.22, p=0.02) and older age was associatedwith increased scores on maternal health risk (r = 0.16,p=0.03) and perinatal health risk (r=0.19, p=0.01).
Examination of bivariate correlations revealed small butsignificant associations between the pre- and perinatal healthfactor scores and symptom outcomes (see Table 3). As shownin prior work, neuropsychological functioning is also relatedto ADHD symptom scores as well as ratings of ODD and CDsymptoms. Neuropsychological factors were moderately cor-related with each other (rs ranging from 0.37-0.61, allp<0.01).
Primary Tests of Direct and Indirect Effects
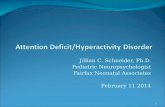
Prenatal Substance Exposures No direct effects of prenatalsubstance exposure were observed when predicting inatten-tion (β = 0.02, [−0.03, 0.07], p = 0.56, total R2 = 0.40),hyperactivity-impulsivity (β=0.01, [−0.05, 0.17], p=0.49,total R2=0.32), ODD (β=0.03, [−0.06, 0.12], p=0.62, totalR2= 0.19), or CD (β= 0.05, [−0.01, 0.11], p= 0.14, totalR2=0.11) after controlling for age, sex, ethnicity, income,parental psychopathology, and parental age at birth.However, a significant indirect effect emerged in predictinginattention, such that higher scores on prenatal substance ex-posure predicted increased inattention via its influence on neu-ropsychological performance (β = 0.13, [0.04, 0.22],p=0.003). Examination of the specific indirect pathways in-dicated that this effect was carried by the influence of prenatalexposures on both memory span deficits (β=0.07, [0.02,0.12], p=0.022) and temporal processing deficits (β=0.04,[0.01, 0.07], p=0.040, see Fig. 2).
Maternal Health During Pregnancy In contrast to substanceexposure, significant direct effects of maternal health risks
during pregnancy emerged for inattention (β=0.16, [0.05,0.27], p=0.014, total R2=0.38), hyperactivity-impulsivity(β=0.12, [0.04, 0.20], p=0.011, total R2=0.33), and ODD(β=0.15, [0.06, 0.24], p=0.005, total R2=0.20). In all cases,higher scores on the maternal health risks during pregnancyfactor was associated with increased symptom scores, evenafter controlling for multiple confounds. The direct effect ofmaternal health risks during pregnancy on CD symptomscores was not significant (β=0.10, [−0.005, 0.20], p=0.12,total R2=0.10). No significant indirect pathways emerged inthese models (see Fig. 3).
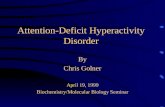
Perinatal Health Risk Direct effects of perinatal health riskwere not significant in predicting inattention (β = 0.03,[−0.02, 0.08], p=0.59, total R2=0.40), marginally significantin predicting both hyperactivity-impulsivity (β=0.08, [0.006,0.15], p=0.08, total R2=0.33) and ODD symptom scores(β=0.10, [0.01, 0.19], p=0.06, total R2=0.19), and signifi-cant in predicting CD symptom scores (β=0.15, [0.04, 0.26],p=0.03, total R2=0.11). For these three outcomes, increasedperinatal health risk was associated with an increase in symp-tom scores, even when including multiple covariates.Additionally, significant indirect effects of perinatal healthrisk emerged in predicting both inattention (β=0.09, [0.02,0.16], p= 0.021) and hyperactivity-impulsivity (β= 0.12,[0.04, 0.20], p<0.001). Examination of the specific indirectpathways indicated that in both models, perinatal health riskinfluenced ADHD outcomes via its influence on both re-sponse variability (inattention: β = 0.06, [0.03, 0.09],p=0.018; hyperactivity-impulsivity: β=0.07, [0.02, 0.12],p< 0.001) and temporal processing (inattention: β= 0.04,[0.002, 0.08], p=0.035; hyperactivity-impulsivity: β=0.04,[0.01, 0.07], p=0.007). In both cases, increased perinatalhealth risk predicted deficits in both response variability andtemporal processing, which, in turn, predicted increasedADHD symptom scores. Indirect effects of perinatal health
Table 3 Correlations among preand perinatal health risk,neuropsychological factors, andADHD and externalizingbehavior outcomes
Inattention Hyperactivity ODD CD
Prenatal Exposures 0.13** 0.07+ 0.09* 0.06
Maternal Health During Pregnancy 0.16** 0.13** 0.17** 0.10**
Perinatal Health Risks 0.18** 0.17** 0.11** 0.15**
Inhibition 0.40** 0.41** 0.28** 0.18**
Working Memory 0.40** 0.38** 0.28** 0.25**
Memory Span 0.34** 0.32** 0.23** 0.16**
Speed 0.36** 0.38** 0.24** 0.20**
Response Variability 0.25** 0.28** 0.17** 0.12**
Arousal 0.25** 0.25** 0.12** 0.15**
Temporal Processing 0.30** 0.32** 0.17** 0.13**
All variables scored such that higher scores reflects increased pre and perinatal problems, greater deficits inneuropsychological functioning, and increased symptomatology
+p < 0.10, *p< 0.05, **p< 0.01
J Abnorm Child Psychol

risks on ODD symptoms (β=0.06, [−0.009, 0.12], p=0.14)and CD symptoms (inattention: β= 0.05, [−0.004, 0.09],p=0.13) were not significant (see Fig. 4).
Follow-Up Analyses
While our use of factor scores allowed us to aggregate acrossmany highly correlated variables related to pre- and perinatalhealth, this methodmay alsomake it more difficult to comparefindings from the current study to prior work focusing onindicators that have been specifically examined in relation toexternalizing spectrum psychopathology, namely tobacco ex-posure during pregnancy and birth weight. Thus, we elected tore-run models examining these specific indicators as predic-tors rather than factor scores to facilitate comparisons withprior research.
Similar to findings using the exposures factor score, prena-tal tobacco exposure did not exert a significant direct effect oninattention (β=0.05, [−0.01, 0.11], p=0.19, total R2=0.40),hyperactivity-impulsivity (β=0.03, [−0.05, 0.11], p=0.56,total R2= 0.32), ODD symptom scores (β= 0.04, [−0.06,0.14], p = 0.19, total R2 = 0.20), or CD symptom scores(β=0.02, [−0.08, 0.12], p=0.76, total R2=0.11). Prenatal to-bacco exposure did, however, exert a significant indirect effecton inattention via neuropsychological functioning (β=0.08,[0.02, 0.14], p=0.020). Examination of specific indirect ef-fects revealed that tobacco exposure specifically influencedmemory span deficits, which increased inattention scores(specific indirect effect: β=0.03, [0.005, 0.06], p=0.039).Marginally significant indirect effects were also observed forODD (β=0.04, [0.002, 0.07], p=0.08) and CD symptomscores (β=0.04, [0.005, 0.07], p=0.060).
A
C
Inattentio
ODD
on B HHyperactivity
D CD
y-impulsivityy
Fig. 2 Direct and indirect effects of prenatal substance exposure oninattention, hyperactivity-impulsivity, ODD, and CD symptom scores.a. Inattention. b. Hyperactivity-impulsivity. c. ODD. d. CD. *p< 0.05,
**p< 0.01. Standardized parameter estimates reported for all pathways.Direct effect is presented to the left of the slash, whereas the sum of theindirect effect is presented to the right of the slash
J Abnorm Child Psychol

Birth weight did not significantly predict either inattention(β = 0.02, [−0.06, 0.10], p = 0.67, total R2 = 0.39) orhyperactivity-impulsivity (β=0.02, [−0.04, 0.08], p=0.72,total R2=0.33), but was a marginally significant predictor ofODD symptom scores (β=0.10, [0.01, 0.19], p=0.06, totalR2=0.20). Note, birth weight was inversed to facilitate com-parison of interpretations. Birth weight did exert a significantdirect effect on CD symptom scores (β=0.12, [0.03, 0.21],p=0.014, total R2=0.12), such that lower birth weight wasassociated with increased CD symptoms. Significant indirecteffects of birth weight via neuropsychological functioningwere again observed for inattention (β=0.09, [0.02, 0.16],p=0.018), hyperactivity-impulsivity, (β=0.10, [0.03, 0.17],p=0.006), and ODD symptom scores (β=0.09, [0.02, 0.16],p=0.018). In all cases, birth weight was associated with in-creased deficits in response variability, which predicted
increased externalizing symptoms, as indexed by the signifi-cant specific indirect effects (inattention: β= 0.05, [0.01,0.09], p=0.031; hyperactivity-impulsivity: β=0.07, [0.03,0.11], p=0.026; ODD: (β=0.03, [0.007, 0.06], p=0.044).Birth weight did not exert significant indirect effects on CDsymptom scores (β=0.04, [−0.04, 0.12], p=0.21).
Discussion
The current study evaluated direct and indirect effects of pre-and perinatal health risk factors on ADHD and other disrup-tive behavior disorder symptoms. Current analyses alsoaccounted for potential familial confounds by covarying pa-rental ADHD symptoms and externalizing disorder status.Results indicated that prenatal substance exposure did not
A
C
Inattention
ODD
B Hyperactivity-impulsivity
D CD
Fig. 3 Direct and indirect effects of maternal health risk duringpregnancy on inattention, hyperactivity-impulsivity, ODD, and CDsymptom scores. a. Inattention. b. Hyperactivity-impulsivity. c. ODD.d. CD. +p < 0.10, *p < 0.05, **p < 0.01. Standardized parameter
estimates reported for all pathways. Direct effect is presented to the leftof the slash, whereas the sum of the indirect effect is presented to the rightof the slash
J Abnorm Child Psychol

appear to be directly associated with ADHD, ODD, or CDsymptoms when these covariates were included. However,maternal health risks during pregnancy did exert significant(and marginally significant) direct effects on ADHD and otherexternalizing psychopathology (as did perinatal health riskson CD symptoms specifically). Our findings are consistentwith recent work suggesting that associations between prena-tal exposure and ADHDmay be dependent upon shared genesbetween parents and children (Knopik et al. 2005; Skoglund etal. 2014; Thapar et al. 2009), but that other pre- and perinatalrisk factors, such as birth weight, may play a causal role inADHD (Pettersson et al. 2015).
Furthermore, several indirect effects also emerged. Prenatalsubstance exposure indirectly predicted increased inattentionvia neuropsychological functioning (memory span and
temporal processing specifically), whereas perinatal healthrisk indirectly predicted increased inattention andhyperactivity-impulsivity via effects on response variabilityand temporal processing deficits. This is consistent with recentwork suggesting that primary neuropsychological functionsmay account for the association between LBW and ADHDsymptoms (Hatch et al. 2014) as well as one prior study dem-onstrating that motor coordination and motor speed mediatedthe association between birth weight and ADHD (Martel et al.2007). Similarly, the current study also demonstrated somespecificity in associations between early developmental riskand more basic cognitive processes, such as memory capacity,visuomotor coordination, and temporal processing. This mayindicate that disruptions in early neural development maybroadly impact several neural networks, which then give rise
A
C
Inattention
ODD
B Hyperactivity-impulsivity
D CD
Fig. 4 Direct and indirect effects of child perinatal health problems oninattention, hyperactivity-impulsivity, ODD, and CD symptom scores. a.Inattention. b. Hyperactivity-impulsivity. c. ODD. d. CD. +p < 0.10,
*p< 0.05, **p < 0.01. Standardized parameter estimates reported for allpathways. Direct effect is presented to the left of the slash, whereas thesum of the indirect effect is presented to the right of the slash
J Abnorm Child Psychol

to higher-order cognitive processes (Aylward 2014).Importantly, youth with ADHD have shown deficits in bothlower and higher-order cognitive domains (Halperin andSchulz 2006; Nikolas and Nigg 2013). Thus, it may be thatearly developmental risk factors play an etiological role inADHD and other externalizing psychopathology via effectson these more basic cognitive processes. However, more workin this area is needed, particularly within genetically-informeddesigns, to confirm this possibility.
An important implication of the present findings is thatprenatal substance exposure and perinatal risk may indepen-dently predict ADHD and comorbid externalizing behaviorsthrough somewhat similar (i.e., temporal processing) as wellas via somewhat distinct mechanisms (i.e., one route involv-ing memory span deficits and one involving response variabil-ity deficits). That is, while related, these early developmentalrisk factors may have partially separable effects onneurocognitive processes that underlie the development ofADHD and co-occurring externalizing disorders, rather thanthe double dissociation proposed in past work (Nigg andBreslau 2007). Future work may benefit by linking these in-direct effects to neural functioning, particularly in brain re-gions involved in primary neuropsychological processes(Russell et al. 2006). Further, current findings suggest thatidentifying and measuring multiple aspects of prenatal andearly development is likely important for discerning their ef-fects. Clinically, if such factors do indeed play a causal role inADHD and co-occurring externalizing behaviors (directly orindirectly), improvement of maternal health during pregnancyand implementing safeguards that promote perinatal health inthe infant may be important strategies in future efforts to pre-vent the development of psychopathology.
Results also highlight the importance of considering famil-ial confounds in these associations. Controlling for parentalADHD symptoms and externalizing disorder status reducedthe direct associations between prenatal substance exposureand ADHD and disruptive behavior disorder symptoms.That is, in addition to indirect effects on psychopathologyvia other intervening processes, such as neuropsychologicalfunctioning, future work would likely benefit by examiningthe interplay between these early neurodevelopmental insultsand familial risk for psychopathology, including potential epi-genetic effects (Nigg 2012).
There are several limitations to the current work. First, cur-rent data were cross-sectional, precluding definitive conclu-sions regarding temporal ordering of variables. Future workshould seek to collect data prospectively to verify the timecourse and order of these variables as well as evaluate thepotential impacts of age and development on these associations(Nikolas and Nigg 2015). However, the temporal primacy ofindices of pre- and perinatal risk increases our confidence in theproposed pathways and findings. Second, the current studyutilized categorical indicators of prenatal substance exposure.
Although this was done because a large proportion ofmothers reported not using any substances during pregnan-cy, future work should examine the frequency and intensityof substance exposure, and, if possible, examine such as-sociations in a prospective manner. Third, only a selectionof possibly relevant neuropsychological functions was in-cluded in current analyses; other domains such as delayaversion, temporal discounting, and decision-making mayalso be relevant (Barkley et al. 2001; Luman et al. 2008).Fourth, the current study used parental ADHD and exter-nalizing psychopathology as a proxy control for geneticrelatedness. We acknowledge that this is potentially a lim-ited method for controlling for genetic relatedness. Further,other parental factors (e.g., internalizing psychopathology)may also confound these associations. Examination ofsuch associations using twin/adoption designs and withmolecular genetic methodologies may enhance the abilityof future work to understand the contributions of these riskfactors and their interplay with genetic risk. Although thecurrent sample contained sibling pairs, examination of theimpact of genetic relatedness via a sibling design was pre-cluded due to lack of necessary statistical power. Lastly,although not within the scope of the current work, futureresearch could benefit by examining how these early de-velopmental risk factors impact the shared variance amongADHD and disruptive behavior disorder symptoms as wellas the developmental progression of ADHD and external-izing symptoms.
In spite of these limitations, the current work demonstratedthat pre- and perinatal health risk may influence ADHD andother disruptive behavior disorders via effects on neuropsycho-logical functioning. Findings also point toward specific process-es (i.e., memory span, response variability, temporal processing)as potential mechanisms for understanding how early risk fac-tors influence the later development of child behavior problems.
Acknowledgments This work was supported by R01-MH070004-01A2 from the National Institute of Mental Health. The content is solelythe responsibility of the authors and does not necessarily represent theofficial views of the National Institute of Mental Health or the NationalInstitutes of Health. The authors also thank all participating children andtheir families for making this work possible.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
Ethical Approval All procedures performed in studies involving hu-man participants were in accordance with the ethical standards of theinstitutional and/or national research committee and with the 1964Helsinki declaration and its later amendments or comparable ethicalstandards.
Informed Consent Informed consent was obtained from all individualparticipants included in the study.
J Abnorm Child Psychol

References
Altink, M. E., Slaats-Willemse, D. I., Rommelse, N. N., Buschgens, C. J.,Fliers, E. A., Arias-Vásquez, A., & Faraone, S. V. (2009). Effects ofmaternal and paternal smoking on attentional control in childrenwith and without ADHD. European Child & AdolescentPsychiatry, 18, 465–475.
American Psychiatric Association. (2013). Diagnostic and statisticalmanual of mental disorders (5th ed.). Arlington: AmericanPsychiatric Association.
Assesmany, A., McIntosh, D. E., Phelps, L., & Rizza, M. G. (2001).Discriminant validity of the WISC-III with children classified withADHD. Journal of Psychoeducational Assessment, 19, 137–147.
Aylward, G. P. (2014). Neurodevelopmental outcomes of infants bornprematurely. Journal of Developmental and Behavioral Pediatrics,35, 394–407.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, andexecutive functions: constructing a unifying theory of ADHD.Psychological Bulletin, 121, 65.
Barkley, R. A., & Murphy, K. R. (2006). Attention-deficit hyperactivitydisorder: A clinical workbook (3rd ed.). New York: The GuilfordPress.
Barkley, R. A., Edwards, G., Laneri, M., Fletcher, K., & Metevia, L.(2001). Executive functioning, temporal discounting, and sense oftime in adolescents with attention deficit hyperactivity disorder(ADHD) and oppositional defiant disorder (ODD). Journal ofAbnormal Child Psychology, 29, 541–556.
Bielas, H., Arck, P., Bruenahl, C., Walitza, S., & Grünblatt, E. (2014).Prenatal stress increases the striatal and hippocampal expression ofcorrelating c-FOS and serotonin transporters in murine offspring.International Journal of Developmental Neuroscience, 38, 30–35.
Chudal, R., Joelsson, P., Gyllenberg, D., Lehti, V., Leivonen, S., Hinkka-Yli-Salomäki, S., & Sourander, A. (2015). Parental age and the riskof attention-deficit/hyperactivity disorder: a nationwide, population-based cohort study. Journal of the American Academy of Child andAdolescent Psychiatry, 54, 487–494.e1.
Cleary-Goldman, J., Malone, F. D., Vidaver, J., Ball, R. H., Nyberg, D.A., Comstock, C. H., & FASTER Consortium. (2005). Impact ofmaternal age on obstetric outcome.Obstetrics and Gynecology, 105,983–990.
Conners, C. K. (1997). Conners rating scale-revised. Toronto: Multi-Health Systems.
D’Onofrio, B. M., Class, Q. A., Rickert, M. E., Larsson, H., Långström,N., & Lichtenstein, P. (2013). Preterm birth and mortality and mor-bidity: a population-based quasi-experimental study. JAMAPsychiatry, 70, 1231–1240.
Delis, D. C., Kaplan, E., & Kramer, J. H. (2001). Delis-Kaplan executivefunction system (DK-EFS) Psychological Corporation.
Derauf, C., Lester, B. M., Neyzi, N., Kekatpure, M., Gracia, L., Davis, J.,& Kosofsky, B. (2012). Subcortical and cortical structural centralnervous system changes and attention processing deficits inpreschool-aged children with prenatal methamphetamine and tobac-co exposure. Developmental Neuroscience, 34, 327–341.
Diwadkar, V. A., Meintjes, E. M., Goradia, D., Dodge, N. C., Warton, C.,Molteno, C. D., & Jacobson, J. L. (2013). Differences in cortico‐striatal‐cerebellar activation during working memory in syndromaland nonsyndromal children with prenatal alcohol exposure. HumanBrain Mapping, 34, 1931–1945.
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., & Reid, R. (1998).ADHD rating Scale—IV: Checklists, norms, and clinicalinterpretation. New York: The Guilford Press.
Ernst, M., Moolchan, E. T., & Robinson, M. L. (2001). Behavioral andneural consequences of prenatal exposure to nicotine. Journal of theAmerican Academy of Child & Adolescent Psychiatry, 40, 630–641.
Faraone, S. V., & Biederman, J. (1998). Neurobiology of attention-deficithyperactivity disorder. Biological Psychiatry, 44, 951–958.
Gurevitz, M., Geva, R., Varon, M., & Leitner, Y. (2014). Early markers ininfants and toddlers for development of ADHD. Journal of AttentionDisorders, 18, 14–22.
Halperin, J. M., & Schulz, K. P. (2006). Revisiting the role of the pre-frontal cortex in the pathophysiology of attention-deficit/hyperactiv-ity disorder. Psychological Bulletin, 132, 560–581.
Hatch, B., Healey, D.M., &Halperin, J. M. (2014). Associations betweenbirth weight and attention‐deficit/hyperactivity disorder symptomseverity: indirect effects via primary neuropsychological functions.Journal of Child Psychology and Psychiatry, 55, 384–392.
Hofhuis, W., de Jongste, J. C., & Merkus, P. J. (2003). Adverse healtheffects of prenatal and postnatal tobacco smoke exposure on chil-dren. Archives of Disease in Childhood, 88, 1086–1090.
Jensen, P. S., Hinshaw, S. P., Swanson, J. M., Greenhill, L. L., Conners,C. K., Arnold, L. E., & Hoza, B. (2001). Findings from the NIMHmultimodal treatment study of ADHD (MTA): implications andapplications for primary care providers. Journal of Developmental& Behavioral Pediatrics, 22, 60–73.
Karalunas, S. L., Geurts, H. M., Konrad, K., Bender, S., & Nigg, J. T.(2014). Annual research review: reaction time variability in ADHDand autism spectrum disorders: Measurement and mechanisms of aproposed trans-diagnostic phenotype. Journal of Child Psychologyand Psychiatry, 55, 685–710.
Knopik, V. S., Sparrow, E. P., Madden, P. A., Bucholz, K. K., Hudziak, J.J., Reich, W., & Todorov, A. (2005). Contributions of parental alco-holism, prenatal substance exposure, and genetic transmission tochild ADHD risk: a female twin study. Psychological Medicine,35, 625–635.
Langley, K., Holmans, P. A., van den Bree, M. B., & Thapar, A. (2007).Effects of low birth weight, maternal smoking in pregnancy andsocial class on the phenotypic manifestation of attention deficit hy-peractivity disorder and associated antisocial behaviour: investiga-tion in a clinical sample. BMC Psychiatry, 7, 26.
Logan, G. D. (1994). A user’s guide to the stop signal paradigm. In D.Dagenbach & T. H. Carr (Eds.), Inhibitory processes in attention,memory, and language (pp. 189–239). San Diego: Academic.
Luman, M., Oosterlaan, J., Knol, D. L., & Sergeant, J. A. (2008).Decision‐making in ADHD: sensitive to frequency but blind to themagnitude of penalty? Journal of Child Psychology and Psychiatry,49, 712–722.
Martel, M. M., Lucia, V. C., Nigg, J. T., & Breslau, N. (2007). Sexdifferences in the pathway from low birth weight to inattention/hy-peractivity. Journal of Abnormal Child Psychology, 35, 87–96.
Martel, M. M., Schimmack, U., Nikolas, M., & Nigg, J. T. (2015).Integration of symptom ratings from multiple informants inADHD diagnosis: a psychometric model with clinical utility.Psychological Assessment, 27, 1060–1071.
Martinussen, R., & Tannock, R. (2006).Workingmemory impairments inchildren with attention-deficit hyperactivity disorder with and with-out comorbid language learning disorders. Journal of Clinical andExperimental Neuropsychology, 28, 1073–1094.
Muthén, L. K., & Muthén, B. O. (1998–2015). Mplus user’s guide,Seventh Edition. Los Angeles: Muthén & Muthén.
Najati, N., &Gojazadeh,M. (2010).Maternal and neonatal complicationsin mothers aged under 18 years. Patient Preference and Adherence,4, 219–222.
Nigg, J. T. (2012). Future directions in ADHD etiology research. Journalof Clinical Child & Adolescent Psychology, 41, 524–533.
Nigg, J. T., & Breslau, N. (2007). Prenatal smoking exposure, low birthweight, and disruptive behavior disorders. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 46, 362–369.
Nigg, J. T., Nikolas, M., & Burt, S. A. (2010). Measured gene-by-environment interaction in relation to attention-deficit/hyperactivity
J Abnorm Child Psychol

disorder. Journal of the American Academy of Child & AdolescentPsychiatry, 49, 863–873.
Nikolas, M. A., & Burt, S. A. (2010). Genetic and environmental influ-ences on ADHD symptom dimensions of inattention and hyperac-tivity: a meta-analysis. Journal of Abnormal Psychology, 119, 1–17.
Nikolas, M. A., & Nigg, J. T. (2013). Neuropsychological performanceand attention-deficit hyperactivity disorder subtypes and symptomdimensions. Neuropsychology, 27, 107.
Nikolas, M. A., & Nigg, J. T. (2015). Moderators of neuropsychologicalmechanism in attention-deficit hyperactivity disorder. Journal ofAbnormal Child Psychology, 43, 271–281.
Noreika, V., Falter, C. M., & Rubia, K. (2013). Timing deficits in atten-tion-deficit/hyperactivity disorder (ADHD): evidence fromneurocognitive and neuroimaging studies. Neuropsychologia, 51,235–266.
Pettersson, E., Sjölander, A., Almqvist, C., Anckarsäter, H., D’Onofrio,B. M., Lichtenstein, P., & Larsson, H. (2015). Birth weight as anindependent predictor of ADHD symptoms: a within-twin pair anal-ysis. Journal of Child Psychology and Psychiatry, 56, 453–459.
Piper, B. J., & Corbett, S. M. (2012). Executive function profile in theoffspring of women that smoked during pregnancy. Nicotine &Tobacco Research, 14, 191–199.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strat-egies for assessing and comparing indirect effects in multiple medi-ator models. Behavior Research Methods, 40, 879–891.
Puig-Antich, J., & Ryan, N. (1986). Kiddie schedule for affective disor-ders and schizophrenia. Pittsburgh: Western Psychiatric Institute.
Rice, F., Harold, G. T., Boivin, J., Van den Bree,M., Hay, D. F., & Thapar,A. (2010). The links between prenatal stress and offspring develop-ment and psychopathology: disentangling environmental andinherited influences. Psychological Medicine, 40, 335–345.
Russell, V. A., Oades, R. D., Tannock, R., Killeen, P. R., Auerbach, J. G.,Johansen, E. B., & Sagvolden, T. (2006). Response variability in
attention-deficit/hyperactivity disorder: a neuronal and glial energet-ics hypothesis. Behavioral and Brain Functions, 2, 9081–9082.
Sergeant, J. A. (2005). Modeling attention-deficit/hyperactivity disorder:a critical appraisal of the cognitive-energetic model. BiologicalPsychiatry, 57, 1248–1255.
Skoglund, C., Chen, Q., D’Onofrio, B. M., Lichtenstein, P., & Larsson,H. (2014). Familial confounding of the association between mater-nal smoking during pregnancy and ADHD in offspring. Journal ofChild Psychology and Psychiatry, 55, 61–68.
Thapar, A., Rice, F., Hay, D., Boivin, J., Langley, K., van den Bree, M., &Harold, G. (2009). Prenatal smoking might not cause attention-def-icit/hyperactivity disorder: evidence from a novel design. BiologicalPsychiatry, 66, 722–727.
Toplak, M. E., & Tannock, R. (2005). Tapping and anticipation perfor-mance in attention-deficit Hyperactivity disorder. Perceptual andMotor Skills, 100, 659–675.
Van den Bergh, B. R., & Marcoen, A. (2004). High antenatal maternalanxiety is related to ADHD symptoms, externalizing problems, andanxiety in 8-and 9-year-olds. Child Development, 1085–1097.
Wechsler, D. (2003). Wechsler intelligence scale for children technicaland interpretive manual (4th ed.). San Antonio: The PsychologicalCorporation.
Wilbertz, G., Tebartz van Elst, L., Delgado, M. R., Maier, S., Feige, B.,Philipsen, A., & Blechert, J. (2012). Orbitofrontal reward sensitivityand impulsivity in adult attention deficit hyperactivity disorder.NeuroImage, 60, 353–361.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B.F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. BiologicalPsychiatry, 57, 1336–1346.
Zhu, J. L., Olsen, J., Liew, Z., Li, J., Niclasen, J., & Obel, C. (2014).Parental smoking during pregnancy and ADHD in children: theDanish national birth cohort. Pediatrics, 134, e382–e388.
J Abnorm Child Psychol