
PRaVDA mag copy
5
Positive Imaging Enhancing proton therapy in the treatment of cancer Seeing with protons, the positively-charged particles that give each atom its identity, is tough but if we are going to make full use of proton therapy in the treatment of cancer then we have to do it. PRaVDA is a Wellcome Trust funded consortium of medical and high-energy physicists, and engineers that has taken on this challenge. The result is perhaps the most complex medical imaging instrument ever constructed. Steps in the production of a single slice of a head phantom CT using simulated proton imaging. The final image is a combination of 180 projections as the head is rotated in a proton beam One in two people will develop cancer during their lifetime, and cancer is the cause of nearly one third of all deaths in the UK. Radiotherapy treatments account for over 40% of curative treatments, through over 130,000 treatments carried out annually – the majority using some 300 x-ray linacs. The UK has recently invested £250m in two NHS Proton Therapy centres that will treat at least 1,500 patients per year, and another 5 private centres will open in the UK within three years. Proton Therapy is rapidly growing across the world with the 60 operating sites to be augmented by a further 40 under construction. With reducing costs, it is likely that a significant proportion of future radiotherapy will utilise high-energy beams of protons – most likely about 10% of cases. Its primary application will be treating childhood cancers – though these are rare, cancer is the largest single cause of death between the ages of 2 and 14. Protons lose their energy in a very different way to x-rays (photons) as they pass through the body. Most of a of 1 5
Transcript of PRaVDA mag copy
Positive ImagingEnhancing proton therapy in the treatment of cancer
Seeing with protons, the positively-charged particles that give each atom its identity, is tough but if we are going to make full use of proton therapy in the treatment of cancer then we have to do it. PRaVDA is a Wellcome Trust funded consortium of medical and high-energy physicists, and engineers that has taken on this challenge. The result is perhaps the most complex medical imaging instrument ever constructed.
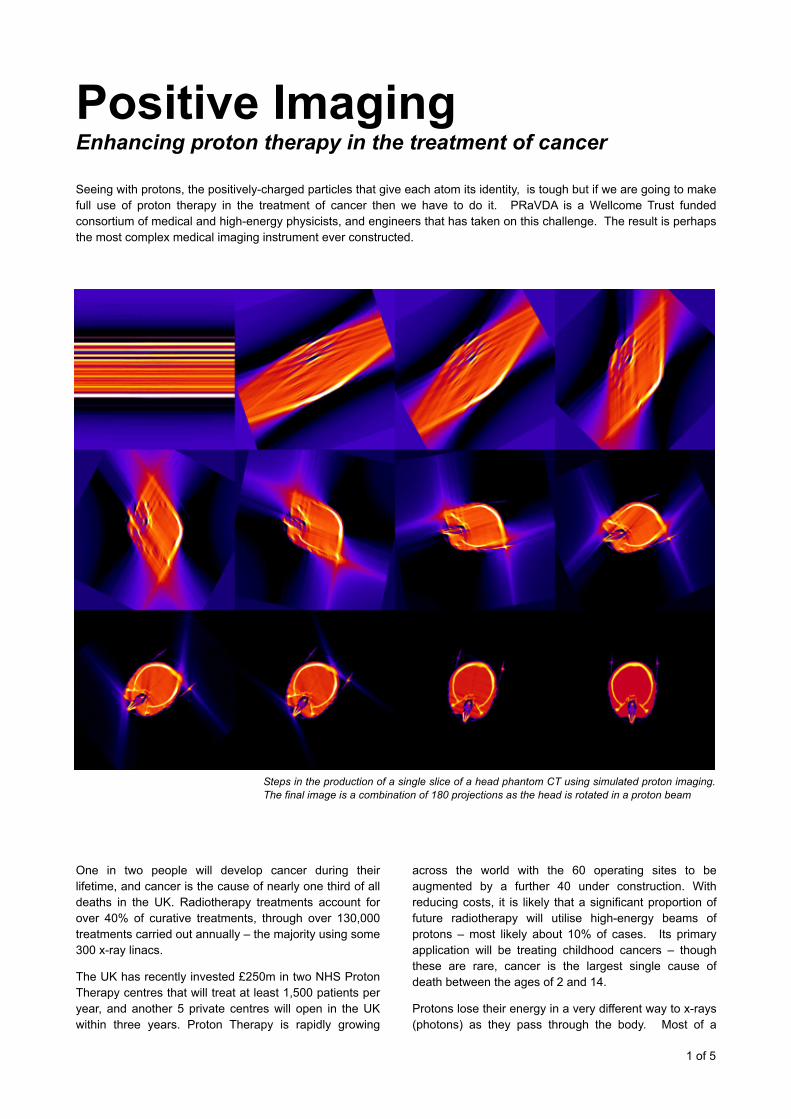
Steps in the production of a single slice of a head phantom CT using simulated proton imaging. The final image is a combination of 180 projections as the head is rotated in a proton beam
One in two people will develop cancer during their lifetime, and cancer is the cause of nearly one third of all deaths in the UK. Radiotherapy treatments account for over 40% of curative treatments, through over 130,000 treatments carried out annually – the majority using some 300 x-ray linacs.
The UK has recently invested £250m in two NHS Proton Therapy centres that will treat at least 1,500 patients per year, and another 5 private centres will open in the UK within three years. Proton Therapy is rapidly growing
across the world with the 60 operating sites to be augmented by a further 40 under construction. With reducing costs, it is likely that a significant proportion of future radiotherapy will utilise high-energy beams of protons – most likely about 10% of cases. Its primary application will be treating childhood cancers – though these are rare, cancer is the largest single cause of death between the ages of 2 and 14.
Protons lose their energy in a very different way to x-rays (photons) as they pass through the body. Most of a
! of !1 5

proton’s energy is deposited near its end of travel – the Bragg Peak – so this allows greater accuracy of dose deposition than x-ray therapy and more importantly less radiation to healthy tissues. We can vary the position (or depth) of the Bragg Peak by changing the proton’s energy.
! The first stage in all radiotherapy is to acquire an x-ray CT image of the patent’s internal anatomy. The treatment plan is formulated from this – calculating the energy of the beam, the directions of the different beams, total dose and number of treatments (fractions)
The need to image with protons CT images are normally produced using high-energy x-ray beams but treatment uses very high-energy beams of protons. X-rays (photons) interact very differently with the material they pass through compared to protons. There is no accurate way to relate the scale of the x-ray CT to the depth and distribution of the treatment protons. The error between x-ray distances and proton distances is typically ±4% (even greater in the head and neck region). For a difficult deep-seated tumour, after 20 cm of healthy tissue penetration, the Bragg Peak could be off target by 1.6 cm. So we either under-dose the tumour or heavily irradiate healthy tissue.
In essence, the advantage of protons is that they stop; the challenge is we are not quite certain where. Ideally, we should to image using the same radiation that we use for treatment – protons: then we are using the same ruler.
Protons experience repeated scattering from the atoms in the materials they pass through – termed Multiple Coulomb Scattering - .so they follow very non-linear paths. Unlike forming images with photons (visible light or x-rays), we have to track the path of individual protons if we want a sharp image.
The sensors The heart of any imaging system is, of course, the sensors themselves. A system that has to operate for many years in a very hostile environment of high radiation levels means that all elements, but especially the sensors, have to be radiation-hard. As we are counting individual protons, we have to count fast otherwise the patient is going to have to stay motionless on the couch for a long time.
Silicon strips (see box) were developed by the high-energy physics community and are critical to experiments at the Large Hadron Collider and other large accelerators. Part of the PRaVDA team provided the
sensors for the ATLAS experiments at CERN, so they designed custom strips for our proton trackers. We also designed a new readout chip that could cope with not only the very low flux during imaging but also the much higher flux during treatment.
Each tracker unit consists of three equi-rotated 10 cm square thin silicon strips which operate at over 100 MHz readout frequency.
Measuring the residual energy Stopping a 50 MeV proton requires a reasonable amount of material, so the Residual Energy Resolving Detector, or Range Telescope, consists of 24 closely packed
! of !2 5
During treatment, the protons complete their travel within the patient – at the site of the tumour. Increasing the proton energy and reducing the intensity of the beam by a factor of 10 thousand allows most protons to emerge from the patient with greatly reduced energies. A pair of position-sensitive proton trackers in front of the patient records the trajectory of each incident proton and an identical pair of trackers records its corresponding exit trajectory immediately after the patient. Hence, the entry and exit positions for each proton on the patient’s surface can be estimated (marked by ‘o’). The Residual Energy Resolving Detector (RERD) logs the residual energy of each proton. This detector is the most complex element of the entire instrument, as it requires a significant volume of material to stop a proton with energies up to 50 MeV.
So knowing the initial energy of the proton beam, we have the following information for each proton: entry position, exit position and
energy absorbed. To produce a clinical-quality CT, we require about 10 million such triplets.
Proton imaging: the basics

! Silicon strips are monolithic sensors that comprise of many diode channels. When a proton passes through a strip it generates a charge pulse, which is processed by a custom readout chip. Strips can only provide one co-ordinate so normally a second strip is mounted a right angles to give a full x-y position. If there more than a very few proton events in a read cycle, then the fundamental structure of strip sensors causes the creation of many false events. To overcome this we use three strips at 120° to each other
layers of silicon strips. Between the strips, thin sheets of polymethyl methacrylate, PMMA (more commonly known as Perspex), can be inserted to change the energy resolution and range of the telescope. We can track the
passage of individual protons through the layers and record where they finally stop (the Bragg Peak), and knowing the stopping power of all the materials along this path, we can then relate range to energy.
In total, there is nearly half a square metre of processed silicon and the output data rate of the whole instrument is equivalent to about 300 HDTV channels.
! Proton tracker unit under construction
All our designs and confirmation of experimental findings are supported by extensive Monte Carlo simulations, which runs on the GridPP – a powerful computing grid developed between the UK high-energy physics community and CERN. We won the Institution of Engineering and Technology Innovation Award (Model-based engineering) for this aspect of PRaVDA.
CT reconstruction The most common method for creating the three-d imensional in ter ior image is us ing F i l tered Backprojection (see box). This will work to some extent for protons but unlike photons, including x-rays, protons do not travel in straight lines. So new methods for CT reconstruction had to be developed.
Of primary clinical use is the relative stopping-power proton CT, as directly represents how the treatment beam will interact inside the patient. However, there is a family of proton CTs. In addition to stopping-power, there
! of !3 5
Principles of computerised tomography A: Imagine a cube filled with a semi-transparent liquid and two darker cylinders and a hollow cylinder
B: Project light through the cube and record the projected image
C: Repeat at different directions
D: Combine these projected images. Begin to discern the internal structures, but lots of blurred artifacts. In practice, the individual projection images are filtered before combined – hence, the name Filtered Backprojection.

is attenuation-power, straggling-power and scattering-power. Some of these do not require the measurement of the residual energies, so the instrument can be much simpler.
The potential of image with protons, and in the future other charged particles, is just being realised. How we can fuse information from different proton CT modes together, as well as with PET and x-ray imagery, is a new exciting field in medical imaging.
Future prospects It is generally agreed that better use of images to plan and guide proton therapy is needed. Several options are proposed from cone-beam x-ray CT to MRI. Though only imaging with protons – the same ruler argument – will eliminate the errors to the underlying level imposed by the basic physics of how protons interact with tissue.
Though it will be a few years before proton CT is a regular feature in therapy centres, it has the potential revolutionise proton therapy treatment – not only in producing accurate planning images but also imaging during and between treatments. A patient’s internal anatomy changes during treatment: as tumours shrink and other organs move. Today we plan for robust treatments but in the future we can provide adaptive optimum treatments.
! First relative scattering power proton CT (a); compared to x-ray CT (b), for a test phantom.
!
PRaVDA is a consortium of 6 universities (Lincoln, Liverpool, Birmingham, Surrey, Warwick, Cape Town), 4 NHS Trusts/Foundation Trusts, Karolinska University Hospital, Sweden, and iThemba LABS, South Africa. It is supported by a translational grant from The Wellcome Trust. PRaVDA is represented in the IET’s “One Hundred Objects that Changed the World” exhibition at Savoy Place and has been exhibited at The Royal Society Summer Science Exhibition.
Nigel Allinson holds the position of Distinguished Chair of Image Engineering, University of Lincoln. He was awarded the MBE for Services to Engineering in 2012, and holds a DSc from the University of Cambridge. He has co-founded five spin-off companies based on work in his research group.
! of !4 5
Reconstructed images of a Pacman-shaped 29 MeV proton beam passing through the four tracker units

! of !5 5
(a) (b)
tissue sparing regions
Comparative planning maps for a nasopharyngeal* cancer. (a) Intensity modulated proton therapy (IMPT) and (b) Tomotherapy. In IMPT the treatment modulates the intensity of the proton beam and shapes it to match the contours of the tumour. Tomotherapy is a current state-of-the-art form of x-ray radiotherapy in which is delivered slice-by-slice together with intensity modulated radiotherapy (IMRT). Notice how various critical regions, regions where any exposure to radiation may lead to further cancers, are saved from significant exposure with protons compared to x-rays. * – upper part of the throat
The PRaVDA instrument installed in the Proton Vault at iThemba LABS, Somerset West, South Africa.
Cou
rtesy
: Que
en E
lizab
eth
Hos
pita
l, B
irmin
gham
, UK


















