Practical upates in Diabetes & CV risk management: Brief ... · Slides presented during CDMC in...
31
Practical upates in Diabetes & CV risk management: Brief Updates Understanding new guideline of AACE, analyzing clinical advantages of AGI Yu Hu, MD Zhong Shan Hospital Fudan University China Slides presented during CDMC in Almaty, Kazakhstan on Sunday April 13 , 2014 and prepared by:
Transcript of Practical upates in Diabetes & CV risk management: Brief ... · Slides presented during CDMC in...

Practical upates in Diabetes & CV risk management: Brief Updates Understanding new guideline of AACE,analyzing clinical advantages of AGI
Yu Hu, MD Zhong Shan Hospital Fudan University China
Slides presented during CDMC in Almaty, Kazakhstan on Sunday April 13 , 2014 and prepared by:

Main contents
1
AGI is listed as alternative first-line agent 2
Interpretation for new idea and highlight of
AACE, 2013

AACE in 2013: a guideline to emphasize
comprehensive management
1.AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 1.
1. Management of obesity
2. Management of prediabetes
3. Lifestyle intervention, medication and management of insulin
for hyperglycemia
4. Management of hypertension
5. Management of hyperlipidemia
6. Management of other risk factors

AACE 2013 elevated management for overweight/obesity
and prediabetes to height of prevention and treatment for
macrovascular complications
1. AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 1.
AACE 2013
recommended
Studies of DCCT (1993), Kumamoto (1995) and UKPDS (1998) demonstrated
that controlling glucose strictly can reduce incidence of diabetic microvascular
complications.
Subsequently, in 2008, large-scale ACCORD study, VADT study and
ADVANCE study didn’t demonstrate that intensively reducing level of blood
glucose can reduce incidence of diabetic macrovascular complications.
Reducing level of blood
glucose can reduce
incidence of diabetic
microvascular complications
How to prevent and
treat macrovascular
complications?
Nip it in the bud……
Management for obesity and
prediabetes is associated
with outcome of
macrovascular complications

Lifestyle treatment is essential and
involved through all stages for all
patients with diabetes
1.AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 1.
AACE 2013 pointed out: Lifestyle is a basis of comprehensive treatment for
diabetes
Lifestyle intervention can be simultaneously
initiated with medications Gradual treatment program is once again verified
to be unreasonable
Lifestyle optimization is essential for all patients with diabetes. Lifestyle
optimization is multifaceted, ongoing, and should engage the entire
diabetes team. However, such efforts should not delay needed
pharmacotherapy, which can be initiated simultaneously and adjusted
based on patient response to lifestyle efforts. The need for medical therapy
should not be interpreted as a failure .

6
Colesevelam
α-GI
Insulin ±
other drugs
= Fewer adverse events or
obtaining benefits possibly
Single medication*
Entry A1c level < 7.5% Entry A1c level ≥ 7.5% Entry A1c level > 9.0%
Without symptoms With symptoms
Progression of diseases
* Sequence of drugs listed above indicates recommended rank order of medication
* * Data based on phase 3 clinical trials
Cutline
metformin
Combined treatment with 2 drugs*
If target isn’t still
achieved after 3
months, intensive
insulin treatment will
be carried out
Combined treatment with 3 drugs*
Lifestyle intervention including that reduction of bodyweight is
conducted via medical intervention
DPP4-inhibitors
TZD
** SGLT-2
Basal insulin
metformin
or other
first-line
drugs SU/GLN
Quick release type
bromocriptine
If target isn’t still
achieved after 3 months,
combined treatment with
3 drugs will be carried
out
metformin
or other
first-line
drugs
Colesevelam
α-GI
GLP-1 RA
TZD
** SGLT-2
Basal insulin
Quick release type
bromocriptine
DPP4-inhibitors
SU/GLN
Combined
treatment with 2
drugs
Combined
treatment with 3
drugs
Or
Adding drugs or intensive insulin
treatment
= Using cautiously
Management of blood glucose is conducted according to
stratification of baseline A1c levels of patients
GLP-1 RA
DPP4- inhibitors
α-GI
SGLT-2 **
TZD
SU/GLN
If A1c level is over 6.5%
after treatment is
conducted for 3 months,
second drug is added (2
drugs are combined)
GLP-1 RA

Primary principle of treatment stated by AACE 2013
1. AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 1.
Minimizing risk of
hypoglycemia and
weight gain
PRINCIPLES OF THE AACE ALGORITHM
FOR THE TREATMENT OF TYPE 2
DIABETES MELLITUS Minimizing risk of hypoglycemia is a priority.
It is a matter of safety, adherence, and cost.
Minimizing risk of weight gain is also a
priority. It too is a matter of safety,
adherence, and cost

Highlight evaluation of cardiovascular risk
factors of patients with T2DM
1. AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 1.

highlights of AACE guideline, 2013
Lifestyle intervention is essential for every diabetics and
medication can be simultaneously initiated with lifestyle
modification.
Management of cardiovascular risk factors to reduce the
CV events of T2DM patients. Such kind of management
needs to start early and maintain for the disease whole
process.
Achieve the glucose target safely with minimized risk of
hypoglycemia and weight gain

Main contents
Interpretation for new idea and highlight of
AACE, 2013 1
AGI is listed as alternative first-line agent 2

11
Colesevelam
α-GI
Insulin ±
other
drugs
= fewer adverse events or
obtaining benefits possibly
Single medication*
Entry A1c level < 7.5% Entry A1c level≥7.5% Entry A1c level > 9.0%
Without symptoms With symptoms
Progression of diseases
*Sequence of drugs listed above indicates
recommended rank order of medication
**Data based on phase 3 clinical trials
Cutline
metformin
Combined treatment with 2 drugs*
If target isn’t still
achieved after 3
months, intensive
insulin treatment will
be carried out
Combined treatment with 3 drugs*
Lifestyle intervention including that reduction of bodyweight is
conducted via medical intervention
DPP4 inhibitor
TZD
** SGLT-2
Basal insulin
metformin
or other
first-line
drugs SU/GLN
Quick release type bromocriptine
If target isn’t still
achieved after 3 months,
combined treatment with
3 drugs will be carried
out
metformin
or other
first-line
drugs
DPP4 inhibitor
α-GI
GLP-1 RA
TZD
** SGLT-2
Basal insulin
Quick release type bromocriptine
SU/GLN
Combined
treatment with 2
drugs
Combined
treatment with 3
drugs
or
Adding drugs or intensive insulin
treatment
= Using cautiously
AGI can be at first-line used singly or combined with other drugs
for patients with various level of A1c
GLP-1 RAs
DPP4 inhibitors
α-GI
SGLT-2
TZD
SU/GLN
If A1c level is over 6.5% after
treatment is conducted for 3
months, second drug is added
(2 drugs are combined)
GLP-1 RA
Colesevelam

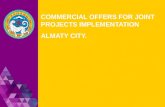
Mechanism of α-glycosidase inhibitors –
Reduction of postprandial blood glucose
*Compared with single α-amylase, starch can produce more oligosaccharides and maltose under the coaction
of α-amylase and α-glycosidase
#Small parts of starch can directly produce glucose under coaction of α-glycosidase
1.http://en.wikipedia.org/wiki/Acid_%CE%B1-glucosidase 2.http://en.wikipedia.org/wiki/Alpha-Amylase.
3.Dhital S, Lin AH, Hamaker BR, et al. PLoS One. 2013 Apr 25;8(4):e62546.
α-glycosidase#
Indicates glucose
Starch
α- amylase
Cooperate with α-glycosidase*
Maltose
Oligosaccharide
α-glycosidase
multiply
decomposed by
α-glycosidase

AGIs delay absorption of glucose

Voglibose can significantly decrease the PPG excursion
Satoh N ,et al. Metabolism.2006,55,786-93.
Obese T2DM,basen 0.9mg/d
**p<0.01 **
** **
Before TX
After TX
BG
(mg/d
l)
Before B After B Before L After L
mean±SE
100
150
200
250
50
0

(mg/dL)
血糖水平
300
250
200
150
100
50
Before B 2hr Before L Before d 2hr 2hr bedtime
*p<0.05 2W vs 3W
2W
3W
4W
acarbose
voglibose
〔before〕
(n=13)
* *
AGIs flatten BG fluctuation
阿部隆三(太田西ノ内医院・糖尿病中心):第41届日本糖尿病学会、 ‘98.5和歌山

AGI can reduce HbA1c significantly
1. Lu Juming. Chinese Journal of Endocrinology and Metabolism 2009; 25(2):2a-6-8
-0.5
-1.0
-1.5 Falli
ng a
mplit
ude o
f H
bA
1c (
%)
Westerner Chinese
-0.5~-0.8%
-1.3~-1.7%
Treatment with α-glycosidase inhibitors

Postprandial glucose and cardiovascular death
DECODE
19991
Pacific and
Indian Ocean
19992
Funagata
Diabetes Study 19993
Whitehall, Paris and
Helsinki Study
19984
Diabetes
Intervention Study
19965
The
Rancho-Bernardo Study
19986
pPG
Honolulu
Heart Programme
19877
CVD Death
1 DECODE Study Group. Lancet 1999;354:617. 2 Shaw JE et al. Diabetologia 1999;42:1050. 3 Tominaga M et al. Diabetes Care 1999;22:920. 4 Balkau B et al. Diabetes Care 1998;21:360. 5 Hanefeld M et al. Diabetologia 1996;39:1577. 6 Barrett-Connor E et al. Diabetes Care 1998;21:1236. 7Donahue, et al., Diabetes, 1987; 36:689

Toshihiko Y, et al. Intern Med. 2007, 46: 543-546
The relationship of 2 hours blood glucose
level and coronary heart diseases
2 hours blood suger level was significantly high in CHD group.
Blood sugar levels from OGTT in CHD and control groups

PPG but not FPG is associated with Myocardial infarction and death - the Diabetes
Intervention Study, 11-year follow-up (DIS)
Hanefeld M, et al. Diabetologia 1996, 39:1577-83
0
150
300
4.4 <7.8 >7.8
心肌梗死
死亡率
0
150
300
4.4 <7.8 >7.8
心肌梗死
死亡率
发生率
/1000人
发生率/100
0人
FPG PPG
P=NS P<0.05
MI
death
MI
death

40-114 mg/dL
115-133 mg/dL
134-156 mg/dL
157-189 mg/dL
190-532 mg/dL
1hr PBG
0
10
20
30
40
50
60
Fatal CHD fatal CHD +
nonfatal MI
发生
率/ 1000人
p<0.01
p<0.001
Postprandial glucose and fatal CHD and nonfatal
MI - Honolulu heart study
Donahue, et al., Diabetes, 1987; 36:689.
8000 japanese males, follow up for 11 years

Glucose Metabolism and Coronary
Heart Disease in Patients
With Normal Glucose Tolerance
80
81
82
83
84
85
86
87
88
89
90
91
0 1 2 3
100
110
120
130
0 1 2 3
Factor R P
Postload glucose 0.667 <0.001
HbA1c 0.561 <0.001
HOMA-IR 0.278 <0.001
Postload insulin 0.221 <0.001
Fasting insulin 0.297 <0.001
Triglycerides 0.531 <0.001
Total cholesterol 0.432 <0.001
HDL-C -0.156 0.009
Fasting glucose -0.003 0.83
LDL-C 0.501 <0.01
DBP 0.067 <0.01
SBP 0.004 0.76
Age 0.020 0.14
smoking 0.087 <0.001
Numbers of Coronary artery narrowing
FP
G
PP
G
Ferdinando CS et al. JAMA, 2004,291:1857 N=234
Numbers of Coronary artery narrowing

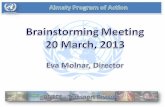
Acarbose treatment and the risk of cardiovascular
disease and hypertension in patients with impaired
glucose tolerance: the STOP-NIDDM trial
Hazard ratio (%)
p acarbose
(n=682)
placebo
(n=686)
No. experiencing event
Favors
0 0.5 1.0 1.5 2.0
Coronary heart disease
Myocardial infaction 1 12 91
Angina 5 12 55
Revascularization 11 20 39
CV death 1 2 5
Congestive heart failure 0 2 –
Cerebrovascular E./ stroke 2 4 44
Peripheral vascular Disease 1 1 –
Any CV events 15 32 49
0.02
0.13
0.18
0.63
–
0.51
0.93
0.03
acarbose placebo
Chiasson JL, et al. JAMA 2003;290:486–94.

Hanefeld M, et al. Eur Heart J 2004;25:10
Acarbose reduces the risk for MI and any CV-events in type 2
diabetic patients: meta-analysis of seven long-term studies

α-glycosidase inhibitors can reduce level of
postprandial blood glucose to help to protect
heart and blood vessels Home P. Diabetes Technol Ther. 2012 Jun;14 Suppl 1:S33-42.
1.Home P. Diabetes Technol Ther. 2012 Jun;14 Suppl 1:S33-42.
α-glycosidase inhibitors can play certain protective role for
heart and blood vessels through reducing postprandial
blood glucose. Although there are relatively fewer large
scale of hard endpoint studies for α-glycosidase inhibitors,
their delayed action for CIMT of alternative endpoint can
also evidence the benefit.

Overview for adverse reactions of
antidiabetes drugs
1.AACE Consensus Statement.ENDOCRINE PRACTICE Vol 19 (Suppl 2) May/June 2013 .
Brief introduction of antidiabetes drugs
Dimethylbig
uanide DPP-4 inhibitors GLP-1RA TZD
α-
glycosi
dase
inhibit
ors
COLSVL BCR-
QR
SU or
glinides Insulin SGLT-2 PRAML
hypoglycem
ia Neutral Neutral Neutral Neutral Neutral Neutral
Neutr
al
Moderate/se
rious, mild
Moderate-
serious Neutral Neutral
Body weight
Decreased
body weight
a bit
Neutral Decreased Increased Neutral Neutral Neutr
al Increased Increased Decreased
Decrea
sed
Renal
function
Forbidden
to use in 3B,
4 and 5
stages
Can need to
adjust dosage as
necessary (apart
from Linagliptin)
Exenatide is
forbidden
when CrCl<30
Can
aggravate
fluid
retention
Neutral Neutral Neutr
al
More risk
for
hypoglycem
ia
More risk
for
hypoglycem
ia and fluid
retention
Infection Neutral
Gastrointest
inal adverse
reaction
Moderate Neutral Moderate Neutral Modera
te Mild
Mode
rate Neutral Neutral Neutral
Modera
te
Congestive
heart failure Neutral Neutral Neutral Moderate Neutral Neutral
Neutr
al Neutral Neutral Neutral Neutral
CVD Obtain
benifits Neutral Neutral Neutral Neutral Neutral Safe ? Neutral Neutral Neutral
Sclerotin Neutral Neutral Neutral
Moderate
osteoporo
sis
Neutral Neutral Neutr
al Neutral Neutral
?
骨质疏松
Neutral
Fewer adverse
reactions or benifits Use cautiously
Possible adverse
reactions
Only a short board

AGI has lower risk for hypoglycemia even can
reduce the hypo when combined with INS
123 T2DM were randomly received Gansulin 30R+voglibose 0.2mg tid(treatment group,n=60) or Gansulin 30R (control group,n=63) for 6 weeks. Measure the change of FPG、
2hPG、insulin doses and rate of hypo.
1. Basen presicriber information. 2. 朱易.医学理论与实践.2012;25(16):1992-93.
20
10
control treatment
8.36 %
30
13.16%
* p<0.05 vs. control
control
treatment
Rate
of
hyp
og
lyce
mic
a(
%)
Extremely lower
hypoglycemia risk(<0.1%)
when monotherapy1
May reducing the risk of
hypo when combination
especially with insulin2

Mechanism α-glycosidase inhibitors –
why GI side effects
*Compared with single α-amylase, starch can produce more oligosaccharides and maltose under the coaction
of α-amylase and α-glycosidase
#Small parts of starch can directly produce glucose under coaction of α-glycosidase
1.http://en.wikipedia.org/wiki/Acid_%CE%B1-glucosidase 2.http://en.wikipedia.org/wiki/Alpha-Amylase.
3.Dhital S, Lin AH, Hamaker BR, et al. PLoS One. 2013 Apr 25;8(4):e62546.
α-glycosidase#
Indicates glucose
Starch
α- amylase
Cooperate with α-glycosidase*
Maltose
Oligosaccharide
α-glycosidase
multiply
decomposed by
α-glycosidase

Gastrointestinal adverse reactions of AGI
results from its inhibition to amylase
H2O & CO2
Undecomposed
polysaccharide
Colon
Decomposed by
intestinal flora
High glucose Hyperosmosis

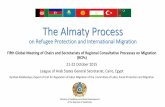
Voglibose has more stronger inhibition
and higher selection to α-glycosidase
小高 裕之(武田薬品).日本栄養・食糧学会誌(1992)45, 27
Half
in
hib
ito
ry c
on
ce
ntr
ati
on
*
(IC
50
) (m
mo
/L)
10-9
10-8
10-7
10-6
10-5
10-4
10-2
6.4×10-9
7.3×10-7
10-1
10-3
1.2×10-5
1.7×10-6
3.9×10-9
>4.5×10-2 Voglibose Acarbose
Maltase# Sucrase# α-amylase
*The smaller value of IC50 is, the more easily drugs are combined with enzymes,
the stronger inhibitory action is # Maltase and sucrase all are α-glycosidase
Maltase# Sucrase# α-amylase

Voglibose has much less GI side effects as compard to acarbose
1.来自倍欣®在日本申请上市时的研究报告 2.来自拜唐苹®在日本申请上市时的研究报告
voglibose acarbose
No. studied 965 603
Incidence of GI SE 15.96% 56.38%

Summary
• AACE Guideline for Comprehensive
management for Diabetes 2013: safely lower
glucose, comprehensive management
• AGI listed as alternative first-line medication by
AACE 2013, which can effectively lower BG
without hypoglycemia and weight gain.
Voglibose shows better tolerance.