Practical Neurology: Polyneuropathy for the Non …/media/files/providence or pdf... · Practical...
57
Practical Neurology: Polyneuropathy for the Non-Neurologist Steven A. Day, MD Providence Neurological Specialties
Transcript of Practical Neurology: Polyneuropathy for the Non …/media/files/providence or pdf... · Practical...

Practical Neurology:Polyneuropathy for the
Non-Neurologist
Steven A. Day, MD
Providence Neurological Specialties

Definitions
Foundational Principle:
With neurological problems think of
LOCALIZATION
before
SYNDROME

Definitions
• Neuronopathy
– Motor neuronopathy
– Sensory neuronopathy
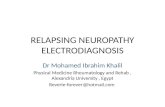
• Radiculopathy
• Plexopathy
• Neuropathy
– Mononeuropathy
– Polyneuropathy

The Netter Collection of Medical Illustrations, Volume 1, Nervous System, 2002
C4
C5
C6
C7
T1
CCF 2002
TRUNKS
Ulnar n.
Radial n.
CORDS
TERMINALNERVES
TRUNKS
“ROOTS”
DIVISIONS
Suprascapular n.
Dorsal scapular n.
Long thoracic n.
Median n.
Axillary n.
Musculocut-
aneous n.
CCF©2002

Definitions
‘Neuropathy’ is a diagnosis which specifies the location of pathology, not a symptom

Definitions
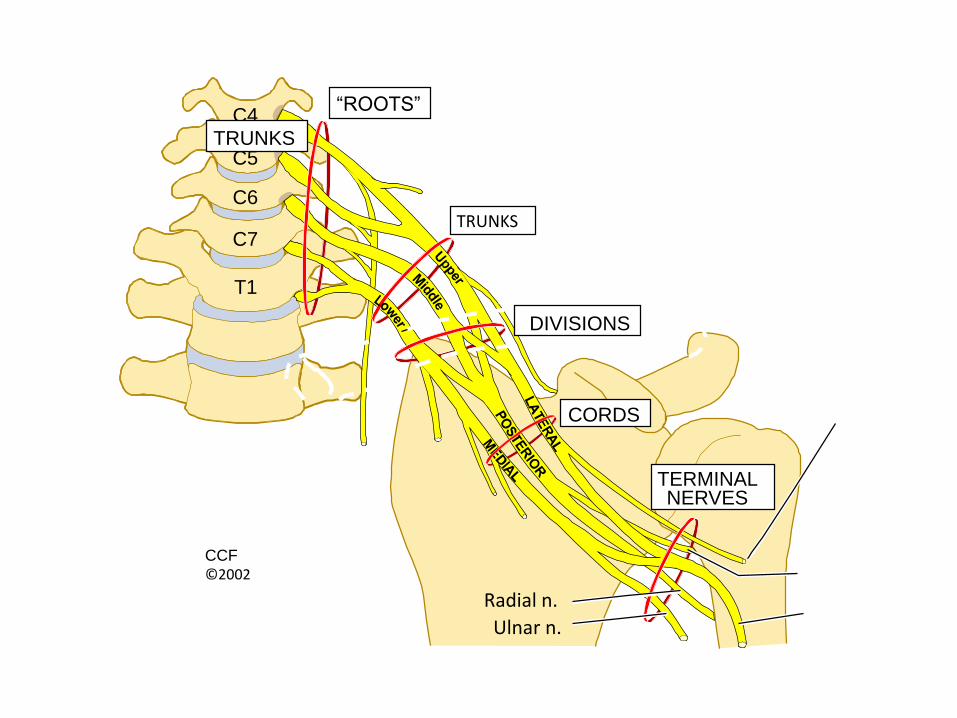
• Axonal = axon loss pathology
• Demyelinating = myelin loss pathology
Topical Diagnosis in Neurology, 3rd ed. 1998
Topical Diagnosis in Neurology, 3rd ed. 1998

Duss’ Topical Diagnosis in Neurology, 4th ed. 2005

Polyneuropathy

Polyneuropathy: Typical Presentation
• Insidious onset
• Distal (toes, pads of feet)
• Gradual progression
• Complaints are primarily sensory

Polyneuropathy: Key Exam Features
• Sensory
– Distal gradient of sensory loss
• Pin prick or cold
• Monofilament
• Cotton wisp
• Vibration at toes and ankles
• Proprioception: toe movements
Polyneuropathy: Key Exam Features
• Motor
– Is there intrinsic foot or hand muscle atrophy?
– Weakness pattern
• Distal
• Proximal and distal
• Asymmetric
– Able to stand/elevate on toes and heels?

Polyneuropathy: Key Exam Features
• Reflexes
– Distal gradient of loss of reflexes
• Ankle jerks
– Brachioradialis

Polyneuropathy: Key Exam Features
• Gait/Station
– Narrow vs wide or variable/stumbling base
– Steppage gait
– Watching ground
– Tandem gait steady?
– Romberg: swaying when standing with eyes closed with a narrow base

Polyneuropathy: causes
• Endocrinopathies
• Other systemic disease
• Nutritional deficiencies
• Infections
• Toxins
• Autoimmune
• Idiopathic: 1/3rd to 1/2 of all cases
• Senescent
• Hereditary
PN and Endocrinopathy
• Diabetes
• Hypothyroidism
• Hyperinsulinemia (e.g. insulinoma)
Neuropathy and Diabetes
• Most common cause of PN in developed countries
• DM1 and DM2
– 15-20% with symptomatic PN
– 66% with objective evidence of PN
• Treatment-induced
• Glucose intolerance
• Metabolic syndrome

Neuropathy and Diabetes
• Associated neuropathies– Distal symmetric sensory or sensorimotor PN
– Mononeuropathy (e.g. CTS)
– Autonomic• Orthostasis, arrhythmias
• Gastroparesis
– Cranial neuropathies
– Polyradiculoneuropathies
– Small fiber

Neuropathy and Diabetes:Distal Symmetric Sensorimotor PN
• Most common form of diabetic neuropathy
• Slowly progressive
• Length dependent (distal to proximal)
• Symptoms– Numbness
– Paresthesias
– Dysesthesias
– Allodynia
– Autonomic dysfunction

Neuropathy and Diabetes:Distal Symmetric Sensorimotor PN
• Can be the presenting symptom of DM
• Can be a presenting symptom of glucose intolerance/prediabetes/metabolic syndrome
Neuropathy and Diabetes:Distal Symmetric Sensorimotor PN
Pathology– Axon loss
– Segmental demyelination
– loss of intraepidermal nerve fibers
– arteriole/capillary endothelial hyperplasia
• Pathophysiology:– Metabolic derangement
– Microangiopathic ischemia
– Inflammation
Neuropathy and Diabetes:Distal Symmetric Sensorimotor PN
Treatment
• Exquisite glucose control
• Symptomatic pain control

Neuropathy and Hypothyroidism
• Median mononeuropathy at the wrist (Carpal Tunnel Syndrome)
– Etiology: edema in tunnel
• Generalized sensorimotor polyneuropathy
– Etiology: unknown
Neuropathy and other Systemic Disease
• Renal Failure
• Chronic Liver Failure
• Cancer (paraneoplastic)
• Sjögren syndrome
• Rheumatoid arthritis
• Systemic lupus erythematosus
• Sarcoidosis
• Scleroderma (Systemic Sclerosis)
• Vasculitis

Neuropathy and Nutritional Deficiencies
• Overall uncommon in developed countries
• Treatable

Neuropathy and B12 Deficiency
• Most common nutritional cause of neuropathy in developed countries
• Can occur in the absence of macrocytic anemia• At risk
– Chronic metformin– Chronic antacids– Chronic alcoholics– Post-bariatric surgery– Vegans– Pernicious anemia– Inflammatory bowel disease at ileum

Neuropathy and B12 Deficiency
Dietary B12 Absorption
– binds to R proteins in saliva, gastric secretions
– Release requires acidic pH
– intrinsic factor produced by gastric parietal cells
– bound by intrinsic factor at duodenum
– B12-intrinsic factor complex absorbed at ileum

Neuropathy and B12 Deficiency
Impaired Absorption– Gastrectomy
– Gastric bypass
– Celiac sprue
– Crohn’s disease
– Ileal resection
– Chronic use/high dose H2 and proton pump inhibitors
– Pancreatic insufficiency
– Bacterial overgrowth (blind loop syndrome)
– Fish tapeworm
Neuropathy and B12 Deficiency
1. Sensory predominant polyneuropathy
2. Subacute Combined Degeneration:
– Polyneuropathy
• Decr light touch
• Decr proprioception
• Sensory ataxia
– Myelopathy
• Increased DTRs (except ankles)
• spasticity

Subacute Combined Degeneration
Duss’ Topical Diagnosis in Neurology, 4th ed. 2005

Neuropathy and B12 Deficiency
• Diagnosis
– B12 levels
• specific but not sensitive
– MMA
• > 0.40 umol/L
• More sensitive than B12
– Homocysteine
• >21 umol/L
• More easily confounded by other conditions

Nitrous Oxide Abuse
• A very rare cause of Subacute Combined Degeneration
• B12 levels may be normal
– N2O inactivates (via oxidation) but does not lower B12 level
• May not present until become B12 deficient
• Dx dependent on high level of suspicion (specifically obtaining hx of NO abuse)

Other Nutritional Neuropathies
• Folate deficiency: as in B12
• Copper deficiency: resembles SCD– Bariatric surgery/small bowel resection
– Zinc toxicity: e.g. zinc supplement, (denture creams)
• Thiamine deficiency (esp. alcoholics)
• Vitamin E deficiency (malabsorption)
• Vitamin B6 deficiency– Chronic alcoholism
– Isoniazid, hydralazine
• Vitamin B6 toxicity: max 50 mg/day
Infectious Neuropathies
• HIV• CMV• Hepatitis C• Lyme• HTLV-1• Diphtheria: Corynebacterium diphtheriae• Leprosy
– Mycobacterium leprae– most common cause of all neuropathies in SE Asia,
Africa, S America

Toxic Neuropathies
• Alcohol• Phenytoin (Dilantin)• Chemotherapy (platinum-based, taxanes, vinca alkaloids, etc)
• Nucleosides for HIV• Metronidazole• Chloroquine and Hydroxychlorquine• Amiodarone• Cholchicine• Lithium• Vitamin B6 (pyridoxine)• Heavy metals (Lead, mercury, thallium, inorganic arsenic, gold,
etc)
Autoimmune Neuropathies
• Acute Inflammatory DemyelinatingPolyradiculoneuropathy (AIDP/GBS)
• Chronic Inflammatory DemyelinatingPolyradiculoneuropathy (CIDP)
• Monoclonal gammopathies
• Paraneoplastic
• Vasculitis
Practical Matters: what your patients need from you
• Attempt to identify a directly treatable cause
• Symptom mitigation

Practical Matters: Laboratory evaluation
• High Yield minimum
– Diabetic screen
– B12
– MMA
– Serum Immunofixation

Practical Matters: Laboratory evaluation
• Routine/1st tier labs– CBC
– CMP
– B12, folate, MMA
– ANA
– ESR/CRP
– TSH
– A1c or Fasting glucose [-> 2 hour glucose tolerance test]
– Serum immunofixation

Practical Matters: EMG
• Purpose– Confirm clinical dx
– Assess severity
– Prognosis (compressive mononeuropathies)
– Differentiate axon loss from demyelination• Implications for possible etiology
• What?– Nerve conduction testing
– Needle electrode exam

The Netter Collection of Medical Illustrations, Volume 1, Nervous System, 2002

Practical Matters: EMG
• Not every patient with neuropathy needs an EMG– e.g. typical DM or ETOH PN
• When to perform– Idiopathic
– Clarify clinical situation• Central vs. peripheral localization
• Symptoms out of proportion to findings
– Rapidly progressive (days to months)
– Motor predominant
– Documentation needed for medical or medicolegal
Practical Matters: EMG
EMG limitations• Intolerant/non-cooperative patients
• Obese
• Elderly
• Multiple peripheral lesions
– e.g. radiculopathy + neuropathy
• Anticoagulation
• Does not assess small fibers (isolated small fiber PN)
• Operator dependent
Practical Matters: Pain Control
Set appropriate expectations
• What medications treat– Burning
– Pins/needles prickling
– Aching
– sensitivity
• No benefit for lack of sensation numbness
• Treatments do not heal nerves/promote growth
• Degree of benefit
Practical Matters: Pain Control
• Extrapolated from trials on diabetic PN
• Clinical experience
• Most medications are used off-label
• “start low, go slow”
• Consider topical approach:
– Elderly/sensitive to medications
– Very localized, e.g. toes
– Intermittent dosing

Practical Matters: Pain Control
• Topical Agents
– Lidocaine
• 5% ointment: BID to TID
• Lidoderm 5% patch: up to 3 patches for 12 hrs /day
– OTC Menthol/Camphor ointment
• Cooling relief for burning dysesthesias
– Doxepin 5% BID
– Compounded topicals
– (Capsaicin 0.75% TID to QID)

Practical Matters: Pain Control
• 1st Line– Alpha lipoic acid
• 600 mg daily (diabetic PN)
– Gabapentin• Start 300 mg TID (100 mg TID in elderly)
• Titrate to 1200 mg TID (as tolerated)
• Newer Qday, BID agents better tolerated
– Tricyclic (e.g. nortriptyline > amitriptyline)• Start 10 mg QHS
• Titrate to 100 mg QHS (as tolerated)

Practical Matters: Pain Control
• 1st Line (cont)– Pregabalin
• Start 50 mg TID (25 mg TID in elderly)
• Titrate to 100 mg TID (as tolerated)
– Duloxetine• Start 60 mg QHS (30 mg QHS in elderly)
• Titrate up to 60 mg BID or 120 mg QHS (as tolerated)
– Venlafaxine XR• 37.5-75 mg Qday
• Titrate by 75 mg/day to 225 mg/day

Practical Matters: Pain Control
• 2nd Line– Oxcarbazepine
• Start 150-300 mg BID
• Titrate by 300 mg/day up to 1200 mg BID
• Follow levels, safety labs (CBC, CMP)
– Carbamazepine• Start 200 mg BID
• Titrate by 200 mg/day to 400 mg QID
• Not as well tolerated as oxcarbazepine
• Follow levels, safety labs (CBC, CMP)

Practical Matters: Pain Control
– Topiramate
• Start 25 mg QHS
• Titrate qweek by 25 mg to max 200 mg BID
– Divalproex sodium
• Start 250 mg BID
• Titrate by 250 mg up to 500 mg TID

Practical Matters: Pain Control
• Marijuana
– Largely an unknown due to lack of research
– 2014 American Academy of Neurology (AAN) systemic review of data:
• No studies to review on peripheral neuropathic pain

Practical Matters: Pain Control
• Other– TENS: may be beneficial (1 study in DM)
– Magnetic therapy: no benefit based on current data• Pulsed electromagnetic
• Magnetic shoe insoles
– Light/LASER therapy: no benefit based on current data
– Reiki therapy: no benefit based on current data
– Acupuncture: no benefit based on current data

Practical Matters: Other
• Physical therapy
– Strengthening
– Gait safety, fall prevention
– Assistive device training
• Ankle Foot Orthotics (AFO)
– Treat foot drop
– Reduce tripping/falls

Neuropathy Red Flags
• Acute onset
• Rapid progression, esp of weakness – Days to weeks
• Asymmetry
• Proximal weakness
• Cranial and peripheral nerve involvement
• Early ataxia
• Associated with rash or petechiae