
Practical Controversies in MS - nationalmssociety.org · Siponimod is a selective S1P1 and S1P5...
50
Practical Controversies in MS Lucas McCarthy, MD, MSc Neurologist, MS Specialist
Transcript of Practical Controversies in MS - nationalmssociety.org · Siponimod is a selective S1P1 and S1P5...
Practical Controversies in MS
Lucas McCarthy, MD, MSc
Neurologist, MS Specialist

© 2016 Virginia Mason Medical Center
Practical Controversies
How to approach common questions in the gray-zone of evidence-based practice?

© 2016 Virginia Mason Medical Center
Practical Controversies
• Treatment of CIS or Benign MS
• Treatment of inactive primary progressive MS
• Treatment of secondary progressive MS
• DMT Discontinuation
• Use of Oral Steroids for MS relapses
© 2016 Virginia Mason Medical Center
Poll Everywhere – Audience Participation
Open cell phone or laptop to following link to participate in live questions
https://pollev.com/MSsummit

Treatment of Clinically Isolated Syndrome

© 2016 Virginia Mason Medical Center
Treatment of CIS
Clinically Isolated Syndrome (CIS)
- Single inflammatory demyelinating clinical event
Limited as of 2017 McDonald MS Diagnostic Criteria
– DIT = enhancing (except optic nerve) and non-enhancing typical MS lesion (>3mm in size)
- DIT = +OCB in CSF
- DIS = 2 or more lesions in 2 or more territories (periventricular, juxtacortical / cortical, infratentorial, spinal cord)
DIT = Dissemination in Time DIS = Dissemination in Space

© 2016 Virginia Mason Medical Center
McDonald 2017 MRI Criteria
MS Lesion >3 mm in size
4 Locations
- Periventricular (has to touch ventricles) – NOT subcortical
- Juxtacortical / Cortical
- Infratentorial
- Spinal Cord
Subcortical Lesions+Periventricular Subcortical Lesions
© 2016 Virginia Mason Medical Center
CIS Examples
Optic Neuritis isolated, no brain lesions
Optic Neuritis, 1+ non-enhancing lesions
Transverse Myelitis, isolated, no brain lesions
Transverse Myelitis, 2+ subcortical (non-periventricular) lesions
Transverse Myelitis, 2+ cord lesions
Transverse Myelitis, 1+ simultaneously enhancing brain lesion
Brain demyelinating lesion, isolated, no other lesions
Brain demyelinating lesion, 1+ subcortical lesions
Brain demyelinating lesion, simultaneous enhancing lesions (e.g. ADEM)

© 2016 Virginia Mason Medical Center
Treatment of CIS
Prior CIS (now different based on updated criteria)
- 60-80% Risk of MS conversion if other brain lesions
- 20% Risk for MS conversion in 10 years if no brain lesions
Multiple Trials for treatment of CIS - Interferons (BENEFIT, ETOMS, CHAMPS), Glatiramer (PreCISe), Teriflunomide (TOPIC)
CIS DMT Treatment reduced MS conversion by ~30% in 2 years

© 2016 Virginia Mason Medical Center
Treatment of CIS
AAN DMT Guideline
Clinicians should prescribe DMT to people with a single clinical demyelinating event and two or more brain lesions characteristic of MS who decide they want this therapy (Level B)
Clinicians may recommend serial imaging at least annually for the first 5 years and close follow-up rather than initiating DMT in people with CIS or relapsing forms of MS who are not on DMT, have not had relapses in the preceding 2 years, and do not have active new MRI lesion activity on recent imaging (Level C).

© 2016 Virginia Mason Medical Center
Treatment of CIS
Does Isolated CIS require treatment without risk factors?
- Isolated Unilateral Optic Neuritis?
- Isolated Transverse Myelitis?
Risk Factors:
- CSF Oligoclonal bands (satisfies DIT but not DIS)
- Other brain / cord lesions that do not make diagnostic criteria
- Associated factors (age, peri-infectious onset, gender, family history)
- Presence of auto-antibodies (AQP-4, MOG)

© 2016 Virginia Mason Medical Center
Treatment of CIS
Risk factors for Optic Neuritis conversion to MS in 15 years1
Lesions on MRI
Brain
Probability of MS, % Probability of MS
None 25 Reference
1 60 2.8x higher
2 68 2.7x higher
≥3 78 4.5x higher
The Optic Neuritis Study Group. “Multiple Sclerosis Risk After Optic Neuritis:
Final Optic Neuritis Treatment Trial Follow-up”. Arch Neurol. 2008.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2440583/

© 2016 Virginia Mason Medical Center
Treatment of CIS
Risk factors for Optic Neuritis conversion to MS in 15 years1
The Optic Neuritis Study Group. “Multiple Sclerosis Risk After Optic Neuritis:
Final Optic Neuritis Treatment Trial Follow-up”. Arch Neurol. 2008.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2440583/
Risk Factor Probability of MS
Female Gender 3.6x higher
White Race 0.6x higher
Preceding “Viral Symptoms” 2.4x higher
No Optic Disc Swelling on Exam 2.4x higher
CSF with antibodies (Oligoclonal
Bands)
Higher risk
Older Age Higher risk

© 2016 Virginia Mason Medical Center
Treatment of CIS
Would you recommend serial monitoring or early treatment for low/moderate risk patients?
Example:
- Young female with isolated classic unilateral moderately severe Optic Neuritis, no OCB, but 1 suspect >3mm periventricular brain lesion

Treatment of (inactive) Primary Progressive MS

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Miller DH, Leary SM. Primary-progressive multiple sclerosis. Lancet
Neurol 2007; 6: 903-12.
10-15% of all MS
Older age of onset
Higher proportion male
Axonal loss more predominant than active inflammation

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Dis
ab
ility
Relapsing-Remitting
Time
Dis
ab
ility
Secondary Progressive
Time
Dis
ab
ility
Time
Primary Progressive
Dis
ab
ility
Time
Progressive Relapsing
Lublin FD et al. Neurology. 1996;46:907-911.

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Primary Progressive MS
- ORATORIO Trial – Ocrelizumab
• 732 PPMS, randomized, placebo controlled
• 18 – 55yrs old, EDSS 3.0 – 6.5, < 10-15yrs of MS, +OCB
• 26% with Gad+ Lesions on baseline MRI
• 88% not on DMT prior

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Primary Progressive MS
- ORATORIO Trial – Ocrelizumab
• 732 PPMS, randomized, placebo controlled
• 18 – 55yrs old, EDSS 3.0 – 6.5, < 10-15yrs of MS, +OCB
• 26% with Gad+ Lesions on baseline MRI
• 88% not on DMT prior
• 2x higher Gad+ lesions on baseline MRI than Fingolimod PPMS trial (INFORMIS, Lublin et al. Lancet, 2016)

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Primary Progressive MS - ORATORIO Trial – Ocrelizumab- 24% Disability Progression Relative Reduction- Significantly reduced T2 lesion volume compared with increase in placebo

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
ORATORIO Subgroup Analysis – Disability Progression
Younger patients (< 45yrs) and those with +Gad enhancing lesions have greater benefit.
Subgroup HR 95% CI
< 45 years 0.64 0.45 – 0.92
> 45 years 0.88 0.62 – 1.26
WITH Gad+ Lesions 0.65 0.40 – 1.06
WITHOUT Gad+ Lesions 0.84 0.62 – 1.13
BOTH < 45 and WITH Gad+ Lesions 0.52 0.27 – 1.00

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Primary Progressive MS
FDA Indication for Ocrevus – 3/2017:
“OCREVUS is indicated for the treatment of adult patients with relapsing or primary progressive forms of multiple sclerosis.”
EMA Indication for Ocrevus – 10/2017:
“Ocrevus is indicated for the treatment of adult patients with early primary progressive multiple sclerosis (PPMS) in terms of disease duration and level of disability, AND with imaging features characteristic of inflammatory activity”

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
AAN MS DMT Guideline 2018
The [AAN] committee recommends that ambulatory patients [with primary progressive
MS] should be prescribed ocrelizumab barring any contraindication or situation
whereby risk outweighs benefit. (Level B)

© 2016 Virginia Mason Medical Center
Treatment of Primary Progressive MS
Should patients with INACTIVE primary progressive MS be placed on DMTs?
Are there benefits of Ocrelizumab for inactive progressive MS?
Are there benefits of other DMTs for inactive progressive MS?
Do risks / burdens outweigh benefits for patients with longstanding inactive primary progressive disease?

Treatment of (inactive) Secondary Progressive MS

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
Secondary Progressive MS
Progression of clinical disability from MS unrelated to clinical relapses after an initially relapsing course
Differentiate progressive MS in two groups:
ACTIVE MS – with relapses and new lesions
vs.
INACTIVE MS – without relapses or new lesions
Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course
of multiple sclerosis: the 2013 revisions. Neurology 2014; 83: 278–86.

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
Should we consider starting or changing a DMT in patients with INACTIVE secondary progression of clinical disability?
Inflammation
Regeneration
TimeRelapsing Remitting MS
Compston A, et al. Lancet. Kuhlmann T, et al. Brain. 2002;125:2202-2212; Paolilo A, et al J Neurol. 2004;251:432-439.
Secondary Progressive MS

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
Dis
ab
ility
Relapsing-Remitting
Time
Dis
ab
ility
Secondary Progressive
Time
Dis
ab
ility
Time
Primary Progressive
Dis
ab
ility
Time
Progressive Relapsing
Lublin FD et al. Neurology. 1996;46:907-911.
© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
Should we consider starting or changing a DMT in patients with INACTIVE secondary progression of clinical disability?
Some SPMS Trials- ASCEND – Natalizumab in SPMS – Lancet 2018
- Betaseron in SPMS – Lancet 1998, Neurology 2004
- Mitoxantrone in SPMS – Lancet 2002
- Avonex in SPMS – Neurology 2001
© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
EXPAND Trial 2017
Siponimod is a selective S1P1 and S1P5 receptor modulator
Similar to Gilenya (Fingolimod), a non-specific sphingosine 1-phosphate receptor modulator
Inclusion:
• 18-60yrs old with SPMS (progression in >=2yrs in-between relapses or without relapses, no relapse within 3 months)
• Moderately disabled (EDSS 3.0 – 6.5, ambulate with walker >20m)
• 1651 patients - randomized 2:1 Siponimod to placebo
Kappos et al. Lancet 2018

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
Siponimod for Secondary Progressive MS
Very active patients included, many untreated
• 21% of patients with Gad+ enhancing lesions at baseline
• 36% of patients with clinical relapses in last 2 years
• 22% did not ever have DMT use
• 33% in Placebo vs. 11% in Siponimod group had new gad+ lesions
on follow-up

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
EXPAND - Siponimod Trial – Clinical Disability Progression
Subgroup HR (95% CI)
No Relapses in prior 2 yrs 0.87 (0.68 - 1.11)
Relapses in prior 2yrs 0.67 (0.49 - 0.91)
No Gad+ lesions at baseline 0.87 (0.68 - 1.11)
Gad+ lesions at baseline 0.64 (0.42 - 0.95)
MS Duration since first symptoms
< 10 yrs 0.77 (0.61 - 0.97)
10-20yrs 0.82 (0.66 - 1.02)
20-30yrs 0.88 (0.59 - 1.31)
This benefit seems most prevalent in those with ACTIVE MS, early in disease course

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
AAN DMT Guideline
Clinicians should assess the likelihood of future relapse in individuals with SPMS by assessing patient age, disease duration, relapse history, and MRI-detected activity (e.g., frequency, severity, time since most recent relapse or gad+ lesion) (Level B).
Clinicians may advise discontinuation of DMT in people with SPMS who do not have ongoing relapses (or gad+ lesions on MRI activity) and have not been ambulatory (EDSS 7 or greater) for at least 2 years (Level C).

© 2016 Virginia Mason Medical Center
Treatment of Secondary Progressive MS
For a patient with inactive secondary progressive MS, do you initiate DMT?
Do you change DMT based on inactive secondary progression?
Do you stop DMT if secondary progression occurs with longstanding inactivity (no relapses or new lesions in 5-10+ years)?

DMT Discontinuation
© 2016 Virginia Mason Medical Center
DMT Discontinuation
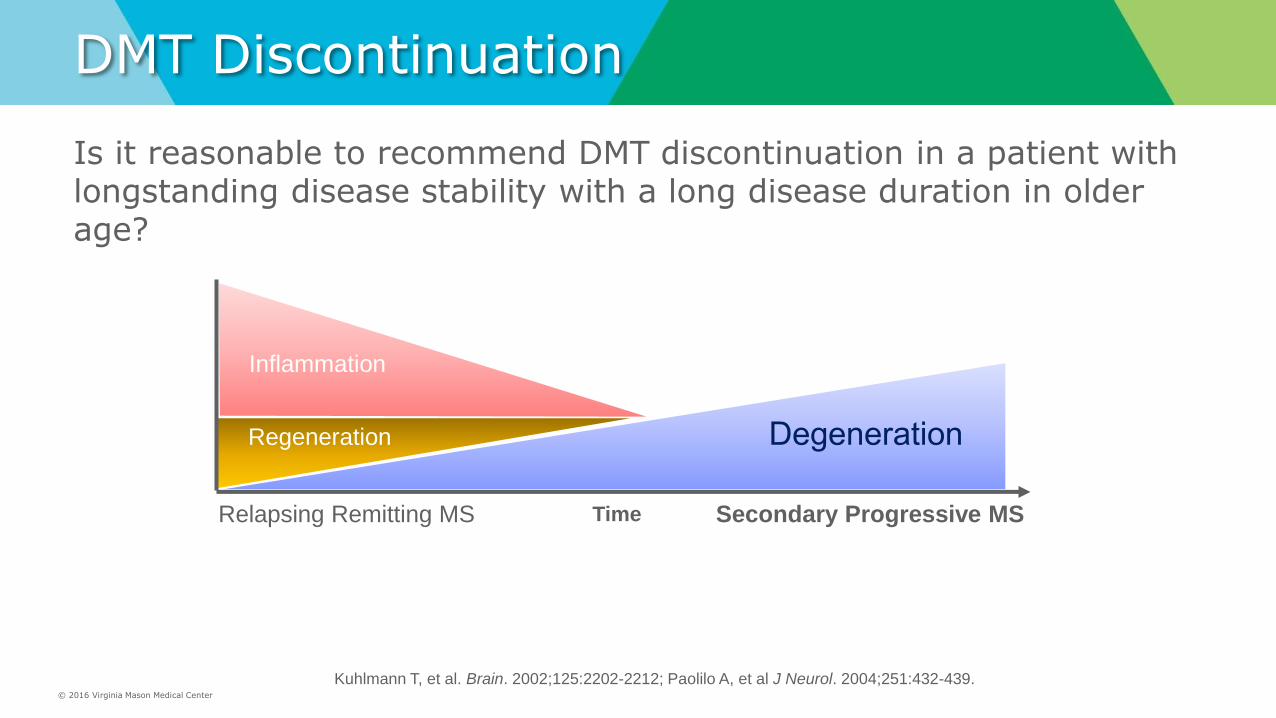
Is it reasonable to recommend DMT discontinuation in a patient with longstanding disease stability with a long disease duration in older age?
Inflammation
Regeneration
TimeRelapsing Remitting MS
Compston A, et al. Lancet. Kuhlmann T, et al. Brain. 2002;125:2202-2212; Paolilo A, et al J Neurol. 2004;251:432-439.
Secondary Progressive MS

© 2016 Virginia Mason Medical Center
DMT Discontinuation
Hua et al. Mult Scler 2018
Clevaland Clinic Group
Large observational trial on DMT discontinuation
600 patients, >60yrs old, DMT > 2 years
178 (30%) discontinued DMT, mostly by provider recommendation
10.7% re-initiated DMT
1 clinical relapse in discontinuers (1 in 178 pts)

© 2016 Virginia Mason Medical Center
DMT Discontinuation – Upcoming Trial
Discontinuation of Disease Modifying Therapies (DMTs) in Multiple Sclerosis (MS) (DISCOMS)
NCT 03073603 – University of Colorado, PI – John Carboy, MD
Randomized Controlled Trial of DMT discontinuation
Funded by the Patient-Centered Outcomes Research Institute and the National Multiple Sclerosis Society
DMT discontinuation in those >= 55 years with no evidence of relapse or MRI activity for >= 5 years
Goal – 300 patients
Start – 4/2017
Trial Duration – 2 years
Estimated End – 2/2021
Measures – EDSS, MSIS, MRI, Relapses – every 6 months

© 2016 Virginia Mason Medical Center
DMT Discontinuation
AAN DMT Guideline
In people with RRMS who are stable on DMT and want to
discontinue therapy, clinicians should counsel people regarding
the need for ongoing follow-up and periodic reevaluation
of the decision to discontinue DMT (Level B).
Clinicians should advocate that people with MS who are
stable (that is, no relapses, no disability progression, stable
imaging) on DMT should continue their current DMT unless
the patient and physician decide a trial off therapy is warranted
(Level B).

© 2016 Virginia Mason Medical Center
DMT Discontinuation
Is it reasonable (risks / burdens / costs vs. benefits) to discontinue a DMT in patients with longstanding stable and inactive MS?
What about DMTs with possible rebound effects - Natalizumab and possibly Fingolimod?
What age, disease duration, activity free duration should be used?
- ongoing trial for age >55, >5 years stable

Oral Steroids for MS Relapse

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Is it reasonable to routinely use high dose oral steroids for MS relapse in place of IV steroids?

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Is is equally effective? Is it well tolerated?
Is is cost effective? Is it more convenient?
1,250mg PO Prednisone = 1,000mg IV Methylprednisolone1
USA Doses - Prednisone 50mg pill size max = 25 pills per day
UK Doses – Methylprednisolone 100mg pills (USA 32mg max)
Drug Costs:
- Methylprednisolone = $150 (3gm IV) + infusion costs
- Prednisone = $25 (3.75gm PO)1 Morrow et al. Neurology 2004
© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Largest PO vs. IV Steroid trial in any MS Relapse
COPOUSEP Trial – Le Page et al. Lancet 2015
• 199 pts, RRMS, 18-55yrs age, relapse within 15 days (avg 7 days)
• 1000mg IV vs 1000mg PO Methylprednisolone
• Endpoint – improvement of 1 point EDSS FSS after 28 days
81% in PO and 80% in IV group had clinical improvements
Similar adverse events
- except slight increase in Insomnia (77% in PO vs. 64% in IV)

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Systematic Reviews comparing IV vs. Oral Steroids:
• Burton et al. Cochrane Database, 2012
• Lattanzi et al. Journal of Neurology 2017; Lui et al. PLoS One 2017
No differences in 6 trials -
- similar rates of improvement of EDSS at 1 and 4 weeks
- similar adverse effects
- no differences in relapse rates on 6 month follow-up
“Based on the evidence, oral steroid therapy may be a practical and effective alternative to intravenous steroid therapy in the treatment of MS relapses.”

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
What about Optic Neuritis?
Optic Neuritis Treatment Trial (ONTT)
- 457 patients, ON, <= 8 days since onset
- IV Steroids 250mg Solumedrol q6 hours x 3 days with oral taper vs. Prednisone 1mg/kg (~70mg x 14 days) vs. Placebo
LOW DOSE PO steroid group
– increased risk for short term recurrent optic neuritis
- no difference in outcomes compared to placebo
HIGH DOSE IV steroid group
- slight improvement in visual outcomes at 6 months
- shorter time to recovery
Beck et al. NEJM, 1992

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Optic Neuritis Treatment Trial
Beck et al. NEJM, 1992

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
High dose oral steroids for Optic Neuritis
Morrow et al JAMA Neurol. 2018
- 55 patients, ON with visual acuity < 20/40
- 1000mg IV Methylprednisolone vs. 1250mg PO Prednisone
Results:
- no difference in VEP at 6 months
- no difference in relapses
High dose oral steroids may be just as good for Optic Neuritis as high dose IV Steroids

© 2016 Virginia Mason Medical Center
Oral Steroids for MS Relapse?
Are oral steroids as effective for MS relapses than IV?
Do they have equal tolerability and risks?
Would you prefer to give a patient with a severe MS relapse IV or Oral Steroids?

Thank you


















