PQCNC Grand Rounds 6/14/2012
63
Transforming Perinatal Care Through Quality Improvement Martin J McCaffrey, MD, CAPT USN (Ret) Clinical Professor of Pediatrics Director of the PQCNC For the PQCNC No disclosures to report.
description
PQCNC Grand Rounds: Wake Forest School of Medicine, Department of Pediatrics 6/14/2012
Transcript of PQCNC Grand Rounds 6/14/2012

Transforming Perinatal Care Through Quality Improvement
Martin J McCaffrey, MD, CAPT USN (Ret) Clinical Professor of Pediatrics
Director of the PQCNC For the PQCNC
No disclosures to report.

Aims
• Quality Improvement (QI) Collaborative Laboratories…and Why We Need Them
• The North Carolina Experience: PQCNC – CABSI, EHM Nursery/NICU
• The National Experience: NCABSI
• Lessons from collaboration
• Transforming the delivery of health care
• Revolutionizing the delivery of healthcare

Collaborative Laboratories
• Vermont Oxford Network 1988
• CPQCC 1997 – Focus on NICUs
– Benchmarking key clinical outcomes
– “You wouldn’t care for a critically ill infant without monitors. How can you care for 30 infants without monitoring outcomes?”
– Leadership includes doctors, nurses, and payers

Collaborative Laboratories
• Healthcare systems explore role of formal QI collaborative activities (2000s) – Intermountain Health – Ascension Healthcare – Others
• National organizations lead formal QI efforts – AHA: CLABSI, CAUTI, SSI
• CMS: “Hospital Compare” 2005 • State neonatal collaboratives conduct QI activities

State Neonatal/Perinatal Collaboratives

Why We Need State QI Collaboratives
Lee HC et al. Antenatal steroid administration for premature neonates in California From 2005-2007. Obstet Gynecol. 2011 Mar;117(3):603-9.

Why We Need State QI Collaboratives
Lee HC et al. Antenatal steroid administration for premature neonates in California From 2005-2007. Obstet Gynecol. 2011 Mar;117(3):603-9.

The North Carolina Experience: PQCNC
• The Perinatal Quality Collaborative of North Carolina (PQCNC)
• Stakeholders in perinatal care across the state – Doctors and Nurses (maternal and neonatal),
families and patients, administrators, DPH, payers (BCBS and DMA), legislators
• Conduct focused QI projects which target inpatient perinatal care

The North Carolina Experience: PQCNC
• Mission: Make North Carolina the best place to be born
• Return maximal value on perinatal care in North Carolina – Spread best practice – Partner with families and patients – Optimize resources
• Nine statewide initiatives – 55 hospitals, 210 teams, impacting 60% North
Carolina births

PQCNC CABSI
• 13 NC NICUs with 600 annual median admissions – 72% of NC VLBW infants
• Approved for ABP MOC Part IV Credit
• Expert team developed action plan – Led by Dr. David Fisher
– Review of existing literature
– Web based sessions including 45 participants • Doctors, Nurses, IC, Families, Senior Leaders
– Focus on insertion and maintenance activities

PQCNC CABSI • Agreed on goal of 75% CABSI reduction
• NHSN CABSI data at baseline & throughout
• NICU teams execute the Action Plan
– Neo, Nurse, Family member and Senior Leader
• Three learning sessions, monthly webinars and weekly email updates

PQCNC CABSI Data
• Observations for all line insertions
• Line maintenance all lines 7 shifts/week
• Infections based on NHSN criteria.
• Data entered in a secure web based PQCNC CABSI data system.
• Line insertions: 1308
• Maintenance reports: 17,801 shifts

Insertion Bundle
• Hand hygiene standards
• Maximum sterile barrier precautions
• Sterile gown for operator & assistant
• Skin disinfected and dried
• All supplies at the bedside
• Time out pre-procedure
• Insertion checklist utilized
• Staff empowered to stop procedure

Maintenance Bundle • Daily assessment of catheter need • “If no catheter today would one be
placed?” • DC catheters at >120 ml/kg/day • Review dressing integrity daily • Scrub connector friction for 15 sec • Gloves when accessing line • Allow surface to dry prior to entry

PQCNC CABSI
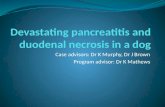
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct '09 Nov '09 Dec '09 Jan '10 Feb '10 Mar '10 Apr '10 May '10 Jun '10
% L
ines
Inse
rted
Com
plia
nt w
ith In
sert
ion
Bun
dle
Months
PQCNC CABSI Insertion Compliance

PQCNC CABSI Maintenance Compliance
Compliance excluding 120 cc/k/d and “If line not in today would one be placed?”

PQCNC CABSI Individual Elements

PQCNC CABSI Individual Elements

PQCNC CABSI Infection Rate

PQCNC CABSI Results
• 75% reduction in CABSIs
• Avoided 94 infections
• Saved 9 lives
• Hospital savings of $2.9M
• Assumptions: 10% mortality, 10 days extended hospital stay & $30K/infection
• Associated morbidities: CLD, IVH, NEC, ROP
http://www.hopkinsmedicine.org/quality_safety_research_group/our_projects/stop_bsi /toolkits_resources/clabsi_estimator.html



NCABSI
• Partnership with AHA/HRET • Mission
– Reduce CABSI rates 75% across the collaborative – Support state perinatal collaboratives
• Proposed May 2011 • Action plan and data support system developed
June-August 2011 • State teams recruited July-October 2011 • Start Nov 2011

NCABSI
• Nine States: MA, HI, WI, SC, NC, FL, NJ, MI, CO
• 95 NICUs entering data
• Partners include AHA/HRET, Pediatrix and State Hospital Associations
• Approved by ABP for MOC Part IV Credit

NCABSI Action Plan and Methods
• Action plan based on PQCNC CABSI
• Physician state leaders partnered with State HA
• State leaders received $70K in funding
• CUSP training led by Missouri HA (coaching and content) embedded in the project
• Insertion data on all central lines
• Daily maintenance observations on every central line

NCABSI Action Plan and Methods
• Insertion data reported by observer • Maintenance observations on every central
line daily by bedside nuirse • Web based reporting with real time updates
for hospital, state and national data metrics – Includes g-chart for days between infection for
hospitals, state, and nation
• Infections based on NHSN criteria • Centers report baseline & ongoing NHSN
data

NCABSI to Date
• Line Insertions – 9051 central lines (umbilical, PICC, Broviac and
other)
• Line Days – 69,057 closed line days
• Maintenance Observations – 50,588 daily observations of central line
maintenance care – 72% completion rate

NCABSI to Date Insertion Compliance

NCABSI to Date
Maintenance Compliance

NCABSI to Date
Line in place after 120 cc/k/d

NCABSI to Date Infections per 1000 Line Days

NCABSI Projections
• Reduction of CABSI rate from 3/1000 to 0.75/1000 line days
• 140,000 total line days in 95 NICUs
• Prevent 320 CABSIs
• Save 32 lives
• Avoid 3150 hospital days
• Save $9.5M in NICU costs



EHM Nursery

Phase I Skin to Skin

Phase II Skin to Skin

Phase I Breastfeeding Support

Phase II Breastfeeding Support

Phase I Separation

Phase II Separation

Phase I Hand Expression

Phase II Hand Expression

Phase I Exclusive Breastfeeding

Phase II Exclusive Breastfeeding

Key Drivers EHM Nursery
• Golden Hour – Skin to Skin after delivery
– Possible feed attempt with support
• Separation
• Breastfeeding Support
• Hand Expression
• Post Partum Skin to Skin

EHM NICU Phase I

Phase I Skin to Skin

Phase I Pumping Conversation

Discussion With Mom Re Milk Pumped

500 cc/day Week 2

Shift Knowledge of Hand Electric Pump Use

Only Human Milk First 3 DOL

Only Human Milk First 28 Days

Key Drivers
• Golden Hour (Golden Six Hours?) – Early Pumping
• Provider Conversation with Moms
• Nursing Oversight of Pumping Progress – Skin to Skin
– Volume
– Pump availability
– Use of pump

Transforming Perinatal Healthcare

Transforming Perinatal Healthcare
• Partnership with DMA (Medicaid)
• Partnership with BCBSNC
• Partnership with Office of Rural Health and Community Care
• Partnership with NC Legislature and DPH

Revolutionizing Perinatal Healthcare

Revolutionizing Perinatal Healthcare
• Leadership from the field
• Clear aim, measureable goal
• Data supports the work • Lean, flexible and necessary
• Sustainable change changes culture • CUSP
• Leadership
• Partnership with patients and families

Why We Do This? Gabby

Leadership and Teamwork
If you tell people where to go, but not how to get there, you’ll be amazed at the results. Gen George S Patton

Martin J McCaffrey, MD, CAPT USN (Ret) Director of the PQCNC
Clinical Professor of Pediatrics UNC Chapel Hill School of Medicine
Division of Neonatal Perinatal Medicine Department of Pediatrics
www.pqcnc.org

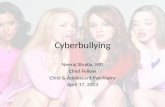
PQCNC VON Infection Rates
0
5
10
15
20
25
30
2005 2006 2007 2008 2009 2010
% V
LBW
With
Infe
ctio
n (F
unga
l and
/or
Nos
ocom
ial)
VON Years
PQCNC Combined Nosocomial and Fungal Infections
27% Reduction in Combined Infections