PowerPoint Presentation · Overview: Leak points Charges Collections & Controls Patient Volume...
17
4/3/2015 © Capko & Morgan - Reuse with Permission Only 1 Capture Every Dime: Finding and Plugging Revenue Leaks Presented By Laurie Morgan Senior Consultant, Capko & Morgan Overview: Leak points Charges Collections & Controls Patient Volume Graphic: AnalyticsHero.com
Transcript of PowerPoint Presentation · Overview: Leak points Charges Collections & Controls Patient Volume...

4/3/2015
© Capko & Morgan - Reuse with Permission Only 1
Capture Every Dime: Finding and Plugging Revenue Leaks
Presented By
Laurie Morgan Senior Consultant, Capko & Morgan
Overview: Leak points
Charges
Collections & Controls
Patient Volume
Graphic: AnalyticsHero.com

4/3/2015
© Capko & Morgan - Reuse with Permission Only 2
Overview: Leak points
Charges
Collections & Controls
Patient Volume
Benchmarks: reality test volume
Gross Charges
Physician Work RVUs
Per FTE physician Mean $1,154,490 90th%ile $1,633,450 10th%ile $777,612
Mean 5,801 90th%ile 8,737 10th%ile 3,070
Per FTE provider Mean $997,208 90th%ile $1,423,445 10th%ile $660,331
Mean 4,693 90th%ile 7,521 10th%ile 1,774
Source: MGMA Cost Survey 2013, Pediatrics, all
Medscape: very useful, and it’s free
Source: MedScape 2014 OB/GYN Compensation Report

4/3/2015
© Capko & Morgan - Reuse with Permission Only 3
Medscape: hours seeing patients
Source: MedScape 2014 OB/GYN Compensation Report
Benchmark resources
MGMA
Medscape
NSCHBC
Specialty management groups
Specialty societies
Consultants
Magazines (e.g., Physicians Practice)
© Capko & Morgan
Scheduling
Access and awareness
Staffing
Patient volume drivers
1

4/3/2015
© Capko & Morgan - Reuse with Permission Only 4
Track no-shows accurately
Practice management system
Phone reminders
More than one-two a day per provider is a problem
One per day = $25,000 per year
Measure, don’t rely on gut
Scheduling efficiency: no shows
Reduce no-shows/cancels
Examine your reminder process Explain need for follow-up visits: “even if
you’re feeling better…” Let patient know if visit carries no cost
Remind three days out
Text+phone, text+email better than vmail
Use technology – seek help from vendors
Reduce no-shows/cancels
Cover lunch – don’t turn away late arrivals
Avoid balance build-ups
Review reports and audit schedules regularly

4/3/2015
© Capko & Morgan - Reuse with Permission Only 5
Audit a month periodically, check for gaps
All providers lightly booked or just some?
Cyclicality? Are other practices busy?
Is provider time being maximized?
Assess time spent on non-essential tasks
Audit scheduling efficiency
Instruct schedulers to avoid gaps
Offer soonest available
Keep a waiting list
Introduce scheduling rules, then check impact: is marketing needed?
If providers are booked but have down time, review slot lengths
© Capko & Morgan 14
Make changes to increase capacity
No/low availability can be costly, too
Review clinic hours, division of labor
Teach staff to “sell” team approach, NPPs
Review slots, add shorter ones
Open-access time can serve urgent needs
Group visits can add capacity
© Capko & Morgan 15

4/3/2015
© Capko & Morgan - Reuse with Permission Only 6
Don’t be passed over
Cover phones during times new patients will call in (e.g., lunch)
Don’t let emails, vmails go unanswered for more than a few hours
PCPs: recall for wellness on time
10 year visits
10-yr revenue
differential
Each patient @$100/visit
2000 patients /10 years
100% on time 10 - - -
Average six weeks late
9 10% $ (100.00) $ (200,000.00)
Average three months late
8 25% $ (200.00) $ (400,000.00)
Average six months late
6 40% $ (400.00) $ (800,000.00)
Average 18 months late
4 60% $ (600.00) $ (1,200,000.00)
© Capko & Morgan 17
Job One: verify/edit/enhance health plan directory listings
Locations, certs, availability, subspecialties
Claim, verify, customize your Google My Business listing
Claim, verify, update your medical directory listings: HealthGrades, Vitals, etc.
Make sure you’re found when patients search
© Capko & Morgan 18

4/3/2015
© Capko & Morgan - Reuse with Permission Only 7
© Capko & Morgan
Directories like HealthGrades, Vitals publish availability stats
“Secret patient” phone calls
ZocDoc can bring patients in immediately, raise profile
Analyze market coverage
© Capko & Morgan 20
© Capko & Morgan

4/3/2015
© Capko & Morgan - Reuse with Permission Only 8
© Capko & Morgan
Monitoring/analyzing referrals
How did you hear about us?
Were you referred by a physician?
Be sure you have a system in place for reporting back to referring physicians – and thanking them
© Capko & Morgan 24

4/3/2015
© Capko & Morgan - Reuse with Permission Only 9
Patient surveys/feedback
Simple survey is best tool for understanding if/why people are leaving your practice
Learn/correct problems before they appear on Yelp, etc.
Just being asked may improve people’s views
Third-party services simplify, meet HIPAA
© Capko & Morgan 25
Staffing influences productivity
FTE Staff
FTE Clinical Supp
Staff
FTE Providers
Per FTE physician Mean 3.8 90th%ile 5.2 10th%ile 2.5
Mean 1.8 90th%ile 2.5 10th%ile 1.1
Mean 1.38 90th%ile 1.74 10th%ile 1.06
Per FTE provider Mean 3.2 90th%ile 4.3 10th%ile 2.4
Mean 1.5 90th%ile 1.9 10th%ile 1.1
Source: MGMA 2013 Cost Survey – Pediatrics, all
© Capko & Morgan 26
Overview: Leak Points
Charges
Collections
Patient Volume

4/3/2015
© Capko & Morgan - Reuse with Permission Only 10
Know how your fee schedule compares with contracts – avoid under-billing
Spot-check payer contract fee schedules against EOBs
Review amendments immediately to avoid automatic implementations
Review your fee schedule(s) annually
© Capko & Morgan 28
Evergreen renewals may suppress your revenue
Review other contract terms to ensure compliance
Don’t assume you can’t negotiate Compare contracts
Identify key codes
Look for points of differentiation
Set a tickler to review contracts
© Capko & Morgan 29
Review coding performance
Defensive under-coding is costly Atypical distribution of E&M can still trigger an
audit 99212 versus 99213 or 99214 might sacrifice
$50/visit or more – thousands of dollars per year
Overly aggressive coding can also invite an audit – aim for accuracy, not conservatism
Consider a coding refresher seminar to get everyone on the same page
© Capko & Morgan 30

4/3/2015
© Capko & Morgan - Reuse with Permission Only 11
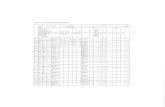
Check utilization versus CMS data
1%
21%
75%
1% 2% 0%
9%
67%
24%
0% 1%
90%
9%
0% 0% 0% 3%
55%
33%
9%
1% 4%
82%
12%
2% 2%
11%
35% 39%
13%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
code 99201 code 99202 code 99203 code 99204 code 99205
CMS avg
© Capko & Morgan
AAPC offers free comparison tool using CMS E/M distribution data
Evaluate your data against national data to gauge audit risk and under-coding
© Capko & Morgan 32
Consider dropping “high hassle” contracts
Costly annoyances: Consistently slower processing More denials/down-coding Atypical referral or authorization rules Frequent patient complaints Poor support
Cutting an unprofitable payer creates room to add another plan Important to evaluate total revenue payer
represents to practice
© Capko & Morgan 33

4/3/2015
© Capko & Morgan - Reuse with Permission Only 12
Graphs spotlight reimbursement differences . . .
© Capko & Morgan 34
. . . collection delays . . .
© Capko & Morgan 35
. . . and overall revenue contribution
© Capko & Morgan 36

4/3/2015
© Capko & Morgan - Reuse with Permission Only 13
Use a grid to compare
Reimbursement Volume Collections New
Patients
“Hassle Factor”
BestPay Network 1st 4th 3rd 5th Low
So-So Plan 2nd 1st 2nd 1st Medium
Okay Insurance 3rd 3rd 4th 4th Low
Medicare 4th 2nd 1st 2nd Low
Lowball Health 5th 5th 5th 3rd High
© Capko & Morgan 37
Confirm the problem’s not on your end
Training issue?
Ask for new contact at payer
If many patients are irritated, too, urge them to go to HR
Work with benefits department yourself
Attempt reform
© Capko & Morgan 38
Overview: Leak Points
Charges
Collections & Controls
Patient Volume

4/3/2015
© Capko & Morgan - Reuse with Permission Only 14
PAGE 40
© CAPKO & COMPANY | CONFIDENTIAL
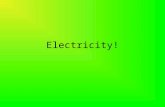
Time of service collections
Copay collection: minimum standard
Collect now or you automatically give up a percentage Plus, invoicing costs approach co-pay value
$20*25 appts=$500/day, $10,000/month, $120,000/year!
Waiving breaches contract
Audit weekly
Tablet tools like Phreesia may be helpful
Patient responsibility % of allowed amounts
Aetna Anthem Cigna UHC Medicare
20.40% 23.10% 25.90% 23.40% 24.60%
Source: 2013 AMA NHIRC
ACA Bronze ACA Silver ACA Gold ACA Platinum
40% 30% 20% 10%

4/3/2015
© Capko & Morgan - Reuse with Permission Only 15
Time of service collections
Know eligibility, patient responsibility before procedures/visits – payer portals, your PMS
External credit for some practices (e.g., elective cosmetic surgery, bariatric)
Card-on-file/auto-payments for balances and pre-payment for surgeries, maternity, etc.
Investigate technology solutions
Prevent internal leaks
90% of practices will experience employee theft
Cash is biggest temptation First ‘test of the waters’ Keep petty cash petty – and separate Separate co-pay collection from daily
reconciliation Receipt stock
Reconcile superbills, appointment schedule against payments daily Split tasks Deposit daily
Prevent internal leaks
Credit, bank statements to physician or external accountant
Use EFT and lockbox EMR, billing system settings
Permissions, password hygiene
Get training from vendor
Look to integrate
Monitor refunds, write-offs, A/R
Background checks
Patient billing complaints
© Capko & Morgan 45

4/3/2015
© Capko & Morgan - Reuse with Permission Only 16
Ensure charge and receipt data are clear
Integrate EHR and PMS if possible
Audit charges against schedule
Analyze denials and down-coding
Manage a 3rd party service as an employee
Revenue cycle starts with scheduling, front desk
Help your biller bill better
© Capko & Morgan 46
Ensure processes allow billing w/in 24 hours
Statement mailings – weekly runs are best
Email statements and payment portal!
Help your patients pay faster
© Capko & Morgan 47
Time is money
Charting: same day
Integrate EHR and PMS if possible
Posting charges: within 24 hours
Exception: hospital services for which approval or documentation from multiple surgeons is needed
Claims submission: within 48 hours
Hospital services 3-5 days
Payment: 30-45 days (insurance), 60-75 days (patient balances after insurance)
© Capko & Morgan 48

4/3/2015
© Capko & Morgan - Reuse with Permission Only 17
Maximizing Collections
Compress schedule: two statements, ‘urgent’ letter, then collections
Remember, each additional statement costs $30 or more to send on average
The staff resources deployed for collecting could be more profitably doing other things
© Capko & Morgan 49
Closing thoughts
Variable #1: Patients Schedule optimally Be sure you’re found (phone, online) when patients search Track patient perceptions
Variable #2: Charges Monitor coding – it drifts – recalibrate when needed Avoid passivity with payers
Variable #3: Collections and controls Collect routinely at time of service – use technology to help Bill and collect promptly Establish and monitor internal controls
© Capko & Morgan 50
Feel free to contact me or my colleagues Laurie Morgan, [email protected]
Visit our blog at www.capko.com/blog
Facebook: www.facebook.com/capkoandmorgan
Twitter: @capkoandcompany and @managementrx
Management Rx: www.managementrx.biz
More Questions?
E-book series – ask for a free review copy!