PowerPoint Presentation - rnstudyguides.com · 2016-03-17 3 CELLULAR INJURY –PATHOGENESIS – 1)...
26
2016-03-17 1 PATHOPHYSIOLOGY: A REVIEW OF KEY CONCEPTS FOR EXAM PREPARATION Marnie Kramer - Kile RN, PhD PATHOPHYSIOLOGICAL REVIEW ALLOWS YOU TO: • Predict outcomes related to pathology • Focus in on specific assessment findings • Understand diagnostic testing for pathology • Predict interventional strategies • Understand potential outcomes for the client KEY AREAS FOR REVIEW IN THIS LECTURE • Cellular Injury • Inflammation • Hypersensitivity Reactions • Mechanisms of Hypoxemia
Transcript of PowerPoint Presentation - rnstudyguides.com · 2016-03-17 3 CELLULAR INJURY –PATHOGENESIS – 1)...
2016-03-17
1
PATHOPHYSIOLOGY: A REVIEW OF KEY
CONCEPTS FOR EXAM PREPARATION
Marnie Kramer-Kile RN, PhD
PATHOPHYSIOLOGICAL REVIEW ALLOWS YOU
TO:
• Predict outcomes related to pathology
• Focus in on specific assessment findings
• Understand diagnostic testing for pathology
• Predict interventional strategies
• Understand potential outcomes for the client
KEY AREAS FOR REVIEW IN THIS LECTURE
• Cellular Injury
• Inflammation
• Hypersensitivity Reactions
• Mechanisms of Hypoxemia

2016-03-17
2
PART ONE: CELLULAR INJURY
CELLULAR RESPONSE TO INJURY
Reversible: mild or short lived injury
Adaptation: persistent but sub lethal injury that cause the cells to adapt (i.e. hypertrophy)
Cell death: due to prolonged and serve injury that is irreversible.
Results in: Necrosis or Apoptosis
CELLULAR INJURY - PATHOGENESIS
• Direct cellular injury
• Indirect cellular injury
Three mechanisms
1) Free radical formation
2) Hypoxia & ATP depletion
3) Disruption of intracellular calcium homeostasis

2016-03-17
3
CELLULAR INJURY – PATHOGENESIS –
1) FREE RADICAL FORMATION
• Unstable molecule –
unpaired electrons
• Free radicals bond with other
molecules to form stable
molecules
• Many metabolic processes
result in free radical
formation
• Oxygen radicals
http://www.healthchecksystems.com/antioxid.htm
CELLULAR INJURY – PATHOGENESIS –
FREE RADICAL FORMATION
• Oxygen radicals cause injury by:
• Lipid peroxidation
• Cell membrane permeability altered
• Oxidative modification of proteins
• Enzyme functions altered
• Fragmenting DNA
• Direction of cellular activities interrupted
• Mitochondrial damage
• Altered ATP production
WHY IS THIS IMPORTANT?http://edcenter.med.cornell.edu/CUMC_PathNotes/Cell.Injury/Cell_Injury.html
http://edcenter.med.cornell.edu/CUMC_PathNotes/Cell.Injury/Cell_Injury.html
2016-03-17
4
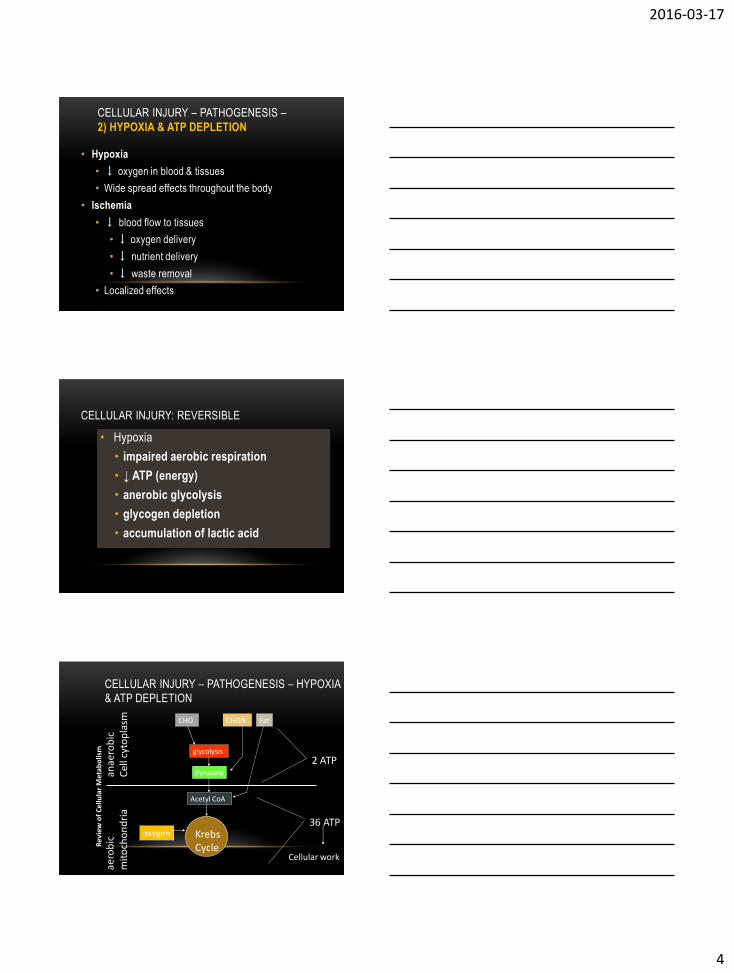
CELLULAR INJURY – PATHOGENESIS –
2) HYPOXIA & ATP DEPLETION
• Hypoxia
• ↓ oxygen in blood & tissues
• Wide spread effects throughout the body
• Ischemia
• ↓ blood flow to tissues
• ↓ oxygen delivery
• ↓ nutrient delivery
• ↓ waste removal
• Localized effects
CELLULAR INJURY: REVERSIBLE
• Hypoxia
• impaired aerobic respiration
• ↓ ATP (energy)
• anerobic glycolysis
• glycogen depletion
• accumulation of lactic acid
CELLULAR INJURY – PATHOGENESIS – HYPOXIA
& ATP DEPLETION
CHO CHON Fat
Pyruvate
Acetyl CoA
2 ATP
anae
rob
icC
ell c
yto
pla
smae
rob
icm
ito
cho
nd
ria
KrebsCycle
oxygen36 ATP
Cellular work
glycolysis
Rev
iew
of
Cel
lula
r M
etab
olis
m
2016-03-17
5
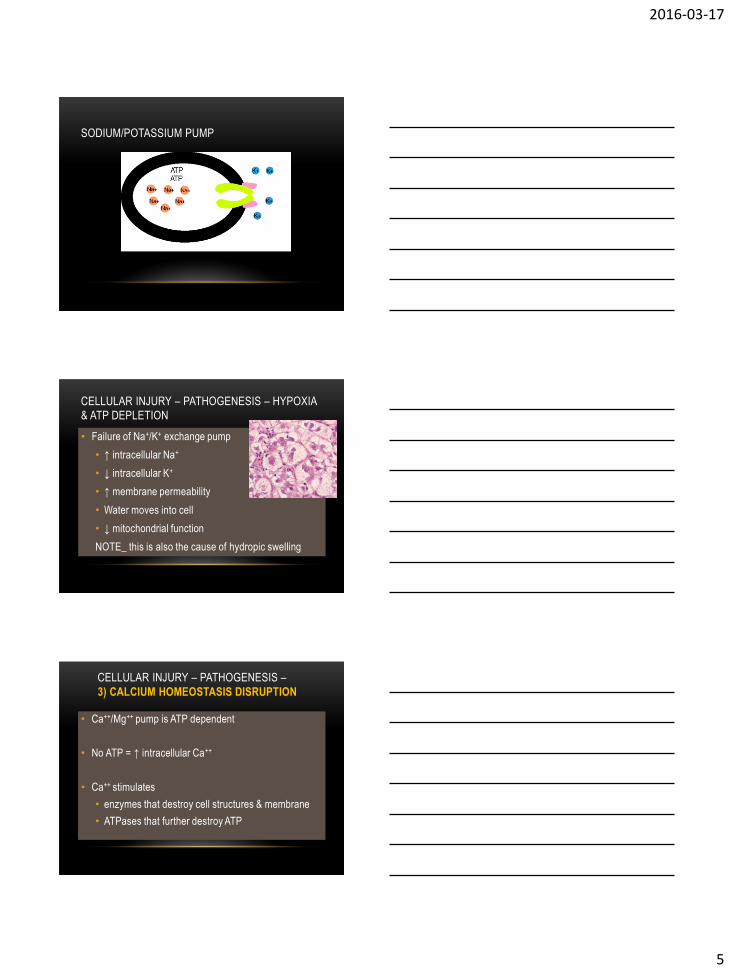
SODIUM/POTASSIUM PUMP
CELLULAR INJURY – PATHOGENESIS – HYPOXIA
& ATP DEPLETION
• Failure of Na+/K+ exchange pump
• ↑ intracellular Na+
• ↓ intracellular K+
• ↑ membrane permeability
• Water moves into cell
• ↓ mitochondrial function
NOTE_ this is also the cause of hydropic swelling
CELLULAR INJURY – PATHOGENESIS –
3) CALCIUM HOMEOSTASIS DISRUPTION
• Ca++/Mg++ pump is ATP dependent
• No ATP = ↑ intracellular Ca++
• Ca++ stimulates
• enzymes that destroy cell structures & membrane
• ATPases that further destroy ATP
2016-03-17
6
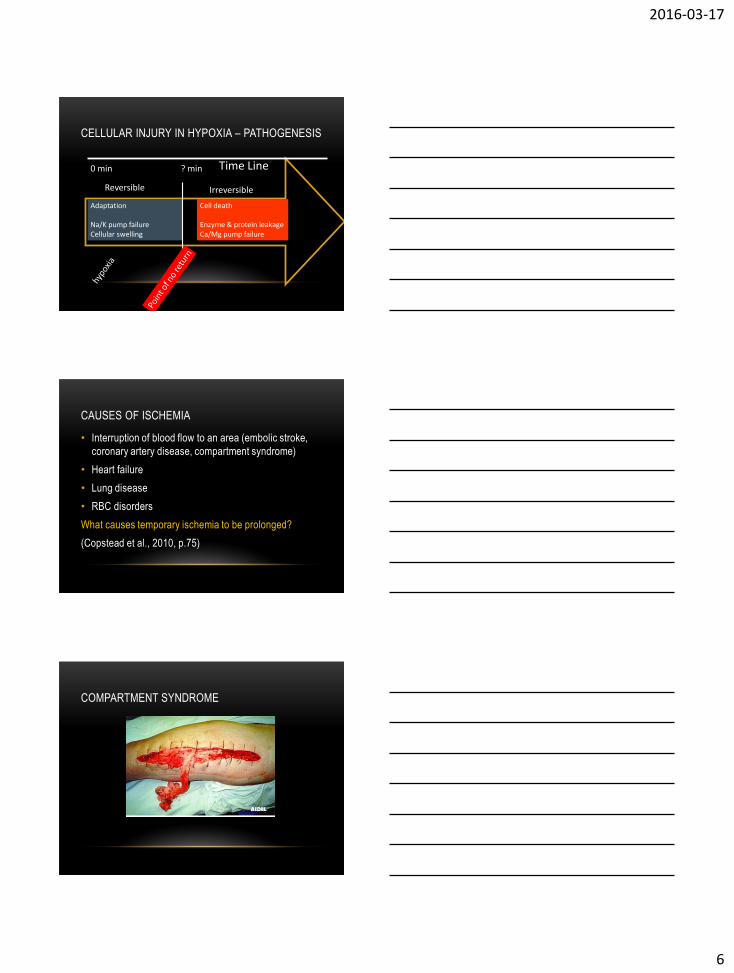
CELLULAR INJURY IN HYPOXIA – PATHOGENESIS
Adaptation
Na/K pump failureCellular swelling
Reversible Irreversible
Cell death
Enzyme & protein leakageCa/Mg pump failure
Time Line0 min ? min
CAUSES OF ISCHEMIA
• Interruption of blood flow to an area (embolic stroke,
coronary artery disease, compartment syndrome)
• Heart failure
• Lung disease
• RBC disorders
What causes temporary ischemia to be prolonged?
(Copstead et al., 2010, p.75)
COMPARTMENT SYNDROME
2016-03-17
7
MYOCARDIAL ISCHEMIA
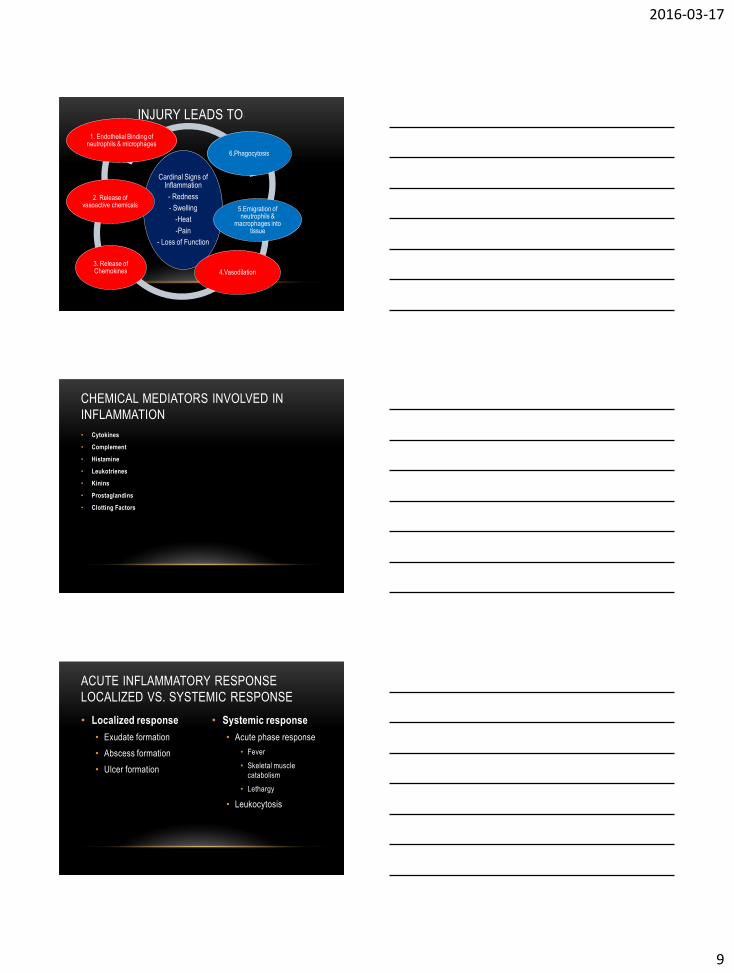
CEREBRAL ISCHEMIA
USD316.K12.KS.US/.../VALERIE/HOMEFRAME.HTML
TEMPORARY VS PERMANENT ISCHEMIA
(EXAMPLE ISCHEMIC PENUMBRA)

2016-03-17
8
CLINICAL PRESENTATIONS OF HYPOXIA
(LEADING TO ISCHEMIA)
• Hypotension (sys less 90 mmHg)- will be seen if shock state
from hypoxia occurring
• Tachycardia (increased HR to increase blood supply)
• Tachypnea (to increase intake O2)
• Cold clammy or mottled skin (result of hypoxia start of shock
state)
• Decreased urine output (start of shock state)
• Confusion (low O2)
• PaO2 low (can also detect low SaO2)
PART TWO: INFLAMMATION
THE INFLAMMATORY RESPONSE HAS THREE
PURPOSES
1. Neutralize and destroy invading and harmful agents
2. To limit the spread of harmful agents to other tissue
3. To prepare any damaged tissue for repair
(Adams et al., 2010, p.197)
2016-03-17
9
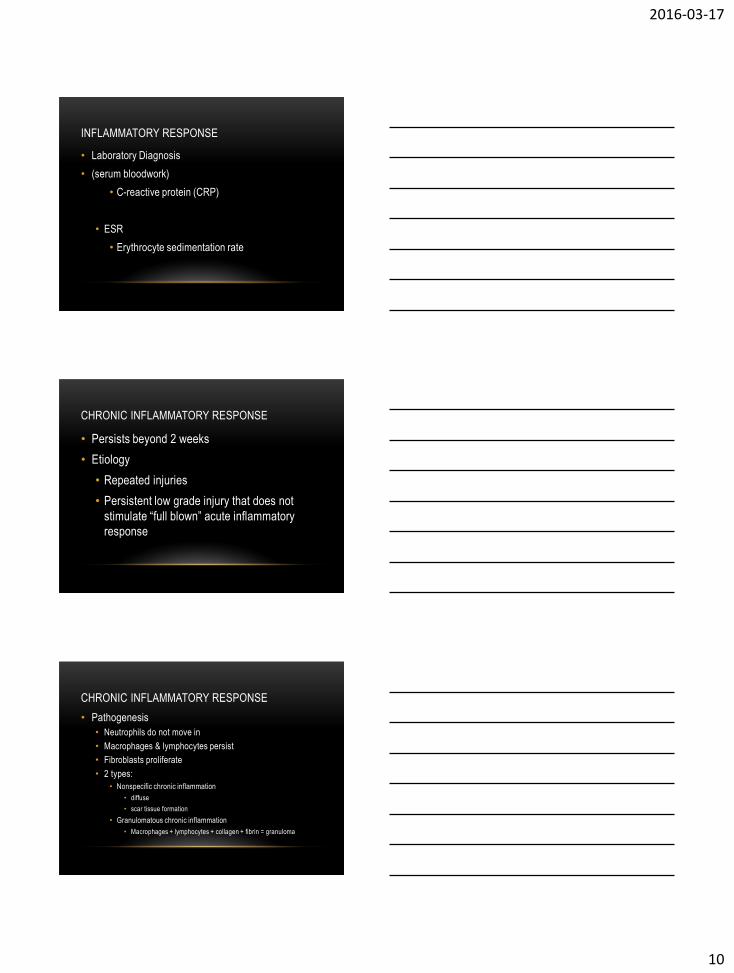
INJURY LEADS TO :
Cardinal Signs of Inflammation
- Redness
- Swelling
-Heat
-Pain
- Loss of Function
6.Phagocytosis
5.Emigration of neutrophils &
macrophages into tissue
4.Vasodilation
3. Release of Chemokines
2. Release of vasoactive chemicals
1. Endothelial Binding of neutrophils & microphages
CHEMICAL MEDIATORS INVOLVED IN
INFLAMMATION
• Cytokines
• Complement
• Histamine
• Leukotrienes
• Kinins
• Prostaglandins
• Clotting Factors
• Localized response
• Exudate formation
• Abscess formation
• Ulcer formation
• Systemic response
• Acute phase response
• Fever
• Skeletal muscle
catabolism
• Lethargy
• Leukocytosis
ACUTE INFLAMMATORY RESPONSE
LOCALIZED VS. SYSTEMIC RESPONSE
2016-03-17
10
INFLAMMATORY RESPONSE
• Laboratory Diagnosis
• (serum bloodwork)
• C-reactive protein (CRP)
• ESR
• Erythrocyte sedimentation rate
CHRONIC INFLAMMATORY RESPONSE
• Persists beyond 2 weeks
• Etiology
• Repeated injuries
• Persistent low grade injury that does not
stimulate “full blown” acute inflammatory
response
CHRONIC INFLAMMATORY RESPONSE
• Pathogenesis
• Neutrophils do not move in
• Macrophages & lymphocytes persist
• Fibroblasts proliferate
• 2 types:
• Nonspecific chronic inflammation
• diffuse
• scar tissue formation
• Granulomatous chronic inflammation
• Macrophages + lymphocytes + collagen + fibrin = granuloma

2016-03-17
11
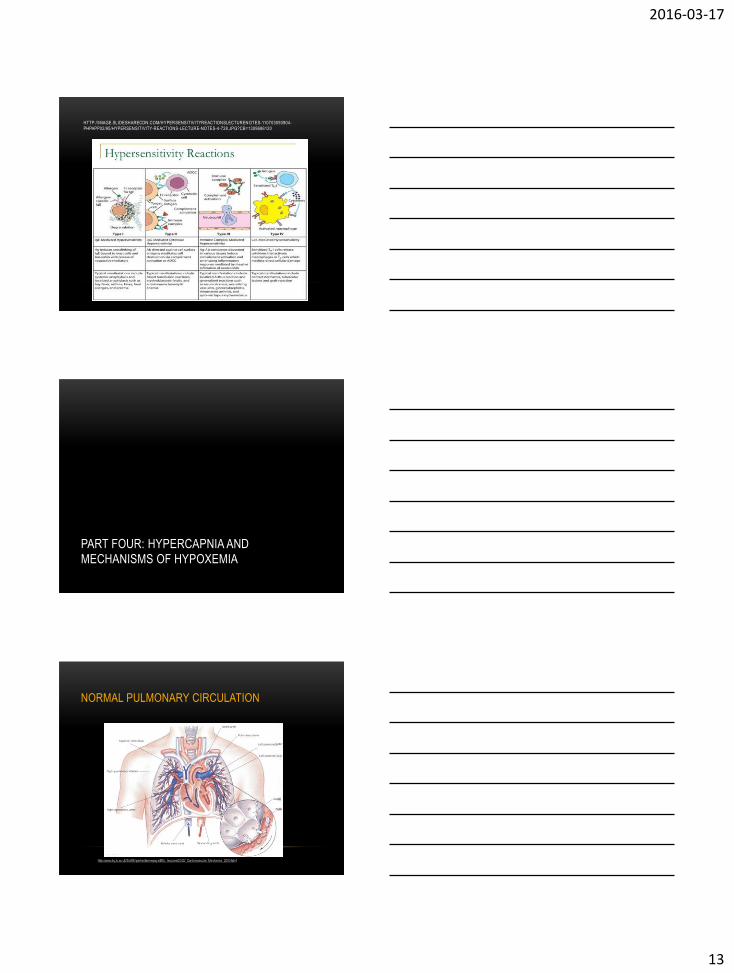
PART 3: HYPERSENSITIVITY REACTIONS
Type IgG IgA IgM IgD IgE
% of Total
Immunoglo-
bulins
75% 15% 10% 0.2% 0.004%
Part of the
body where
it is found
Action
Serum, tissues
Role in
bloodborne,
tissue infections,
enhances
phagocytosis
activates
complement
system
Body fluids
Protects
against GI,
Resp, GU
infections
Prevents
absorption
antigens from
food
Intra-vascular
serum
First immuno-
globulin
produced in
response to
bacterial and
viral infections
Activates
compliment
Serum
Role
unclear
May influ.
B cell
different-
itation
Serum
Allergic and
some hyper-
sensitivity
reactions
Combats
parasitic
infections

2016-03-17
12
Too big immune response!!!
exaggerated, inappropriate
HYPERSENSITIVITY DISORDERS
HYPERSENSITIVITY DISORDERS
(TABLE 10-2, COPSTEAD, 226)
• Antigen
• Protein particle capable of triggering immune response
• 4 types
• Type I hypersensitivity
• Type II hypersensitivity
• Type III hypersensitivity
• Type IV hypersensitivity
SUMMARY
Type I Type II Type III Type IV
Mediated by IgE IgM or IgG IgG T lymphocytes
Complement
Activation
No Yes Yes No
Peak Action 15-30 min 15-30 min 6 hrs 24-48 hrs
Causes of
reaction
T-cell
deficiency
Abnormal
mediator
feedback
Exposure Ag or
foreign tissue,
cells, or graft
Persistent
infection-microbe
Ag
Extrinsic Envir
Autoimmunity
Intradermal Ag
Epidermal Ag
Dermal Ag
Manifestations Asthma,
rhinitis, atopic
eczema, bee-
sting reaction
ABO transfusions,
hemolytic disease
newborn,
myasthenia gravis
Glomerulonephritis,
SLE
Vasculitis
TB test
Contact
dermatitis
MS
Guillain- Barre
disease
2016-03-17
13
HTTP://IMAGE.SLIDESHARECDN.COM/HYPERSENSITIVITYREACTIONSLECTURENOTES-110703093904-
PHPAPP02/95/HYPERSENSITIVITY-REACTIONS-LECTURE-NOTES-4-728.JPG?CB=1309686120
PART FOUR: HYPERCAPNIA AND
MECHANISMS OF HYPOXEMIA
NORMAL PULMONARY CIRCULATION
http://www.bg.ic.ac.uk/Staff/khparker/homepage/BSc_lectures/2002/_Cardiovascular_Mechanics_2003.html

2016-03-17
14
REVIEW
• Lungs
• Hgb releases CO2
• Hgb invites O2
• Body tissue
• Hgb releases O2
• Hgb invites CO2
• Overall
• CO2 and O2 move from an area of high concentration to an area of low concentration.
http://webschoolsolutions.com/patts/systems/lungs.htm
• Altered breath sounds
• Dyspnea
• Abnormal breathing
• Hypoventilation
• Hyperventilation
• Sputum
• Cough
• Hemoptysis
• Cyanosis
• Pain
• Clubbing
WHAT ARE CLINICAL MANIFESTATIONS OF
PULMONARY ALTERATIONS?
ARTERIAL BLOOD GAS INTERPRETATION
Ph (7.35- 7.45) Throughout Body
PaCO2 (35-45 Meq/L) Lungs
HCO3 (22-26 Meq/L) Kidneys
2016-03-17
15
ARTERIAL BLOOD GAS INTERPRETATION
Ph acidosis (7.35- 7.45) alkalosis
PaCO2 alkalosis (35-45 mmHg) acidosis
HCO3 acidosis(22-26 mEq/L) alkalosis
RESPIRATORY DYSFUNCTION
• Failure to maintain adequate oxygenation.
• Manifested with:
→ Hypercapnia leading to respiratory acidosis.
→ Hypoxemia (4 mechanisms)
1. Hypoventilation
2. Diffusion disturbances
3. Shunts
4. V/Q mismatch
• carbon dioxide in the blood.
• Measured by arterial blood gas (PaCO2).
• Causes:• Nervous system,
• Thoracic alterations,
• Airway obstruction:
• WOB.
• physiological dead space.
• Effects of hypercapnia:
• Respiratory acidosis
• Altered electrolytes
• Arrhythmias
• intracranial pressures
• Somnolence
• Coma
• Headache• Hypoxemia
HYPERCAPNIA
2016-03-17
16
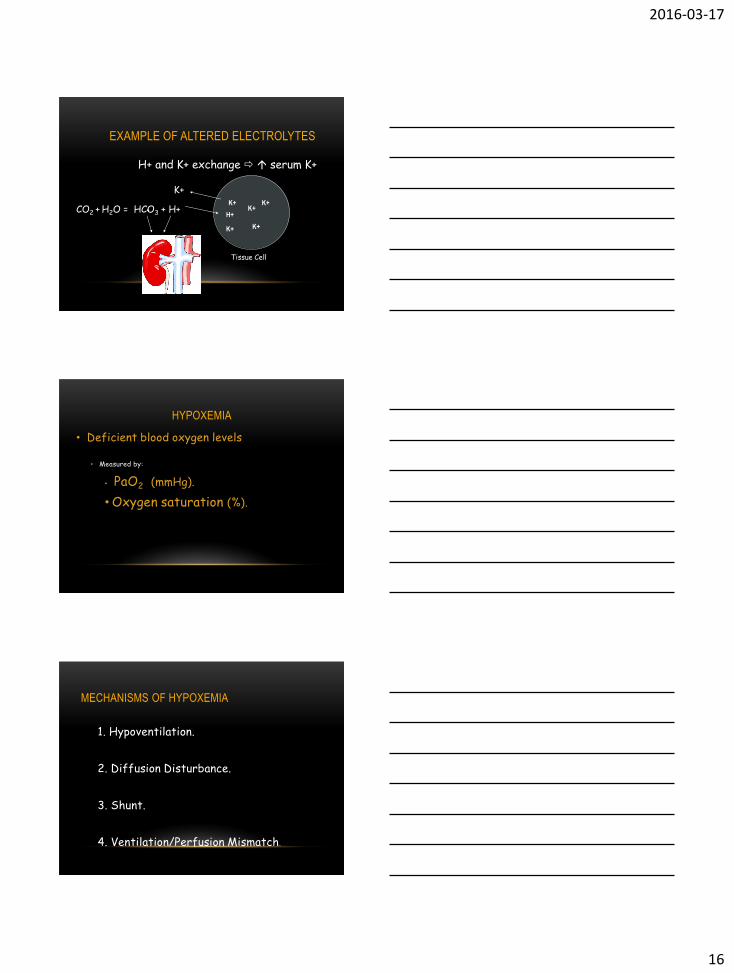
K+K+
K+ K+
K+CO2 + H2O = HCO3 + H+
H+
K+
H+ and K+ exchange serum K+
Tissue Cell
EXAMPLE OF ALTERED ELECTROLYTES
HYPOXEMIA
• Deficient blood oxygen levels
• Measured by:
• PaO2 (mmHg).
• Oxygen saturation (%).
MECHANISMS OF HYPOXEMIA
1. Hypoventilation.
2. Diffusion Disturbance.
3. Shunt.
4. Ventilation/Perfusion Mismatch.
2016-03-17
17
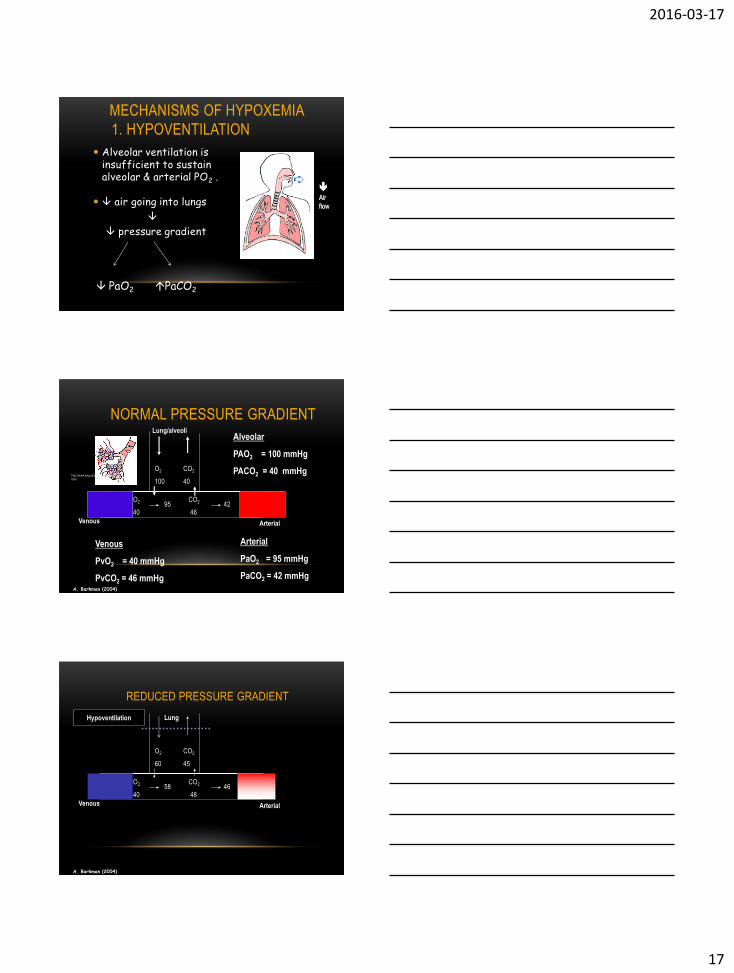
MECHANISMS OF HYPOXEMIA
1. HYPOVENTILATION
Alveolar ventilation is insufficient to sustain alveolar & arterial PO2 .
air going into lungs
pressure gradient
Air
flow
PaO2 PaCO2
Venous Arterial
O2 CO2
100 40
O2 CO2
40 46
NORMAL PRESSURE GRADIENT
95 42
Lung/alveoliAlveolar
PAO2 = 100 mmHg
PACO2 = 40 mmHg
Venous
PvO2 = 40 mmHg
PvCO2 = 46 mmHg
Arterial
PaO2 = 95 mmHg
PaCO2 = 42 mmHg
http://www.lung.ca/copd/anatomy/normal.
html
A. Barkman (2004)
Venous Arterial
O2 CO2
60 45
O2 CO2
40 48
REDUCED PRESSURE GRADIENT
58 46
Hypoventilation Lung
A. Barkman (2004)
2016-03-17
18
HYPOVENTILATION
• Example of Causes
• Medications
• Pleurisy
• Thorax muscular weakness
• Management
• Narcotic antagonists
• ↑ inspired oxygen
• Mechanical ventilation
Pleurisy: Inflammation
of the pleura.
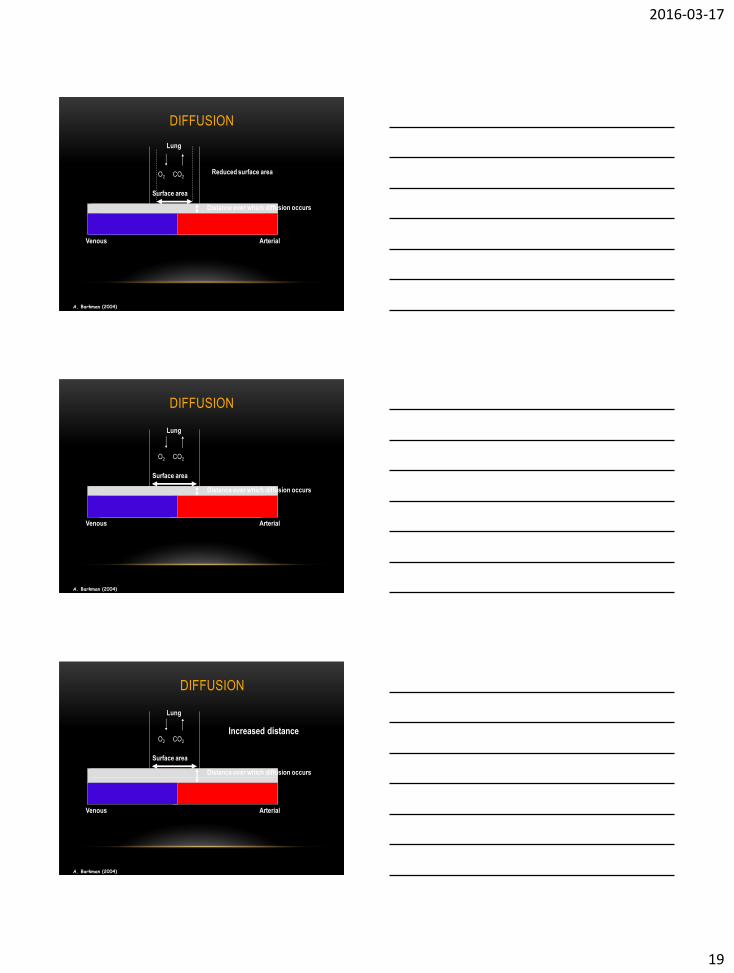
MECHANISMS OF HYPOXEMIA 2.DIFFUSION DISTURBANCE
Diffusion of gas across respiratory membrane normally depends on:
◦ Pressure gradient.
◦ Surface area through which diffusion occurs.
◦ Solubility of gas.
◦ Distance over which diffusion occurs.
Venous Arterial
DIFFUSION
Surface area
O2 CO2
Distance over which diffusion occurs
Lung
A. Barkman (2004)
2016-03-17
19
Venous Arterial
DIFFUSION
Surface area
O2 CO2
Distance over which diffusion occurs
Reduced surface area
Lung
A. Barkman (2004)
Venous Arterial
DIFFUSION
Surface area
O2 CO2
Distance over which diffusion occurs
Lung
A. Barkman (2004)
Venous Arterial
DIFFUSION
Surface area
O2 CO2
Distance over which diffusion occurs
Lung
Increased distance
A. Barkman (2004)

2016-03-17
20
DIFFUSION DISTURBANCE
• Example of Causes
• Alveolar cell carcinoma
• Interstitial Fibrous
• Pulmonary edema
Edema in the Lungs
DIFFUSION DISTURBANCE: INTERSTITIAL
LUNG FIBROSIS
http://www.umwa.org/blacklung/intro.shtml
Sarcoidosis
http://edcenter.med.cornell.e
du/CUMC_PathNotes/Respir
atory/RESPLIST.html
PULMONARY EDEMA
http://www.biovisuals.com/alveolus.html
2016-03-17
21
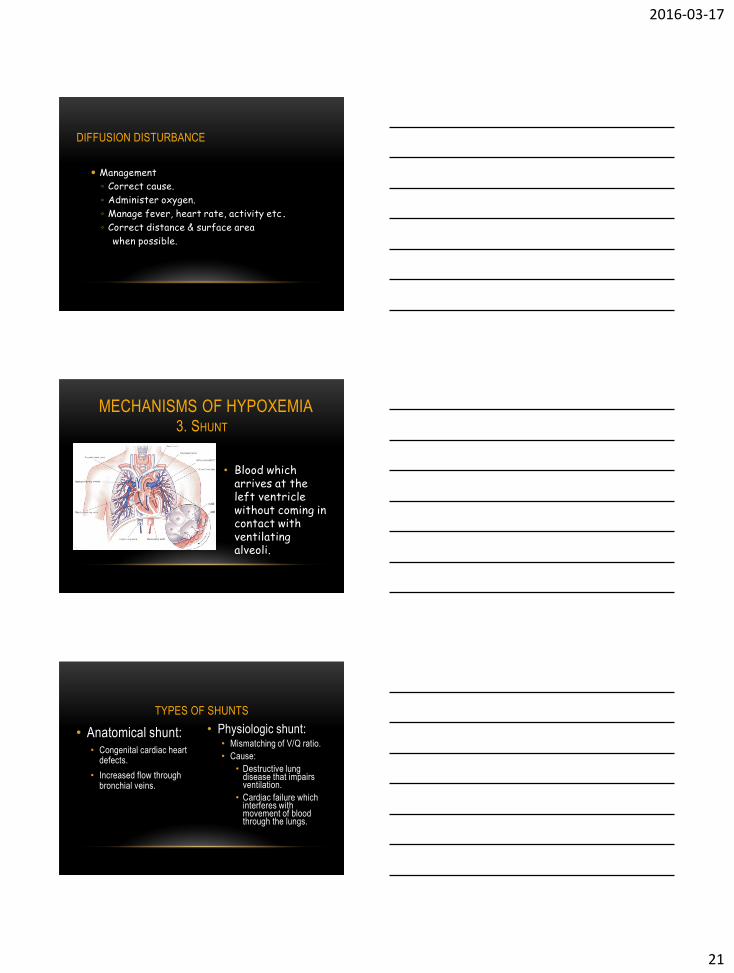
DIFFUSION DISTURBANCE
Management
◦ Correct cause.
◦ Administer oxygen.
◦ Manage fever, heart rate, activity etc.
◦ Correct distance & surface area
when possible.
MECHANISMS OF HYPOXEMIA3. SHUNT
• Blood which arrives at the left ventricle without coming in contact with ventilating alveoli.
TYPES OF SHUNTS
• Anatomical shunt: • Congenital cardiac heart
defects.
• Increased flow through bronchial veins.
• Physiologic shunt:• Mismatching of V/Q ratio.
• Cause:
• Destructive lung disease that impairs ventilation.
• Cardiac failure which interferes with movement of blood through the lungs.
2016-03-17
22
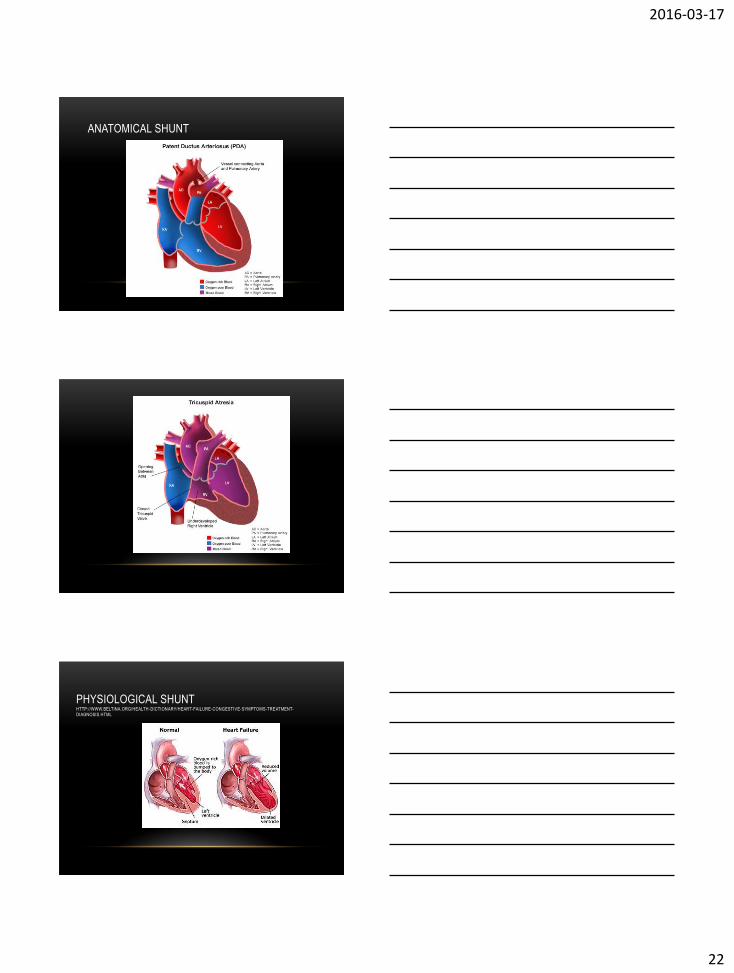
ANATOMICAL SHUNT
PHYSIOLOGICAL SHUNTHTTP://WWW.BELTINA.ORG/HEALTH-DICTIONARY/HEART-FAILURE-CONGESTIVE-SYMPTOMS-TREATMENT-DIAGNOSIS.HTML
2016-03-17
23
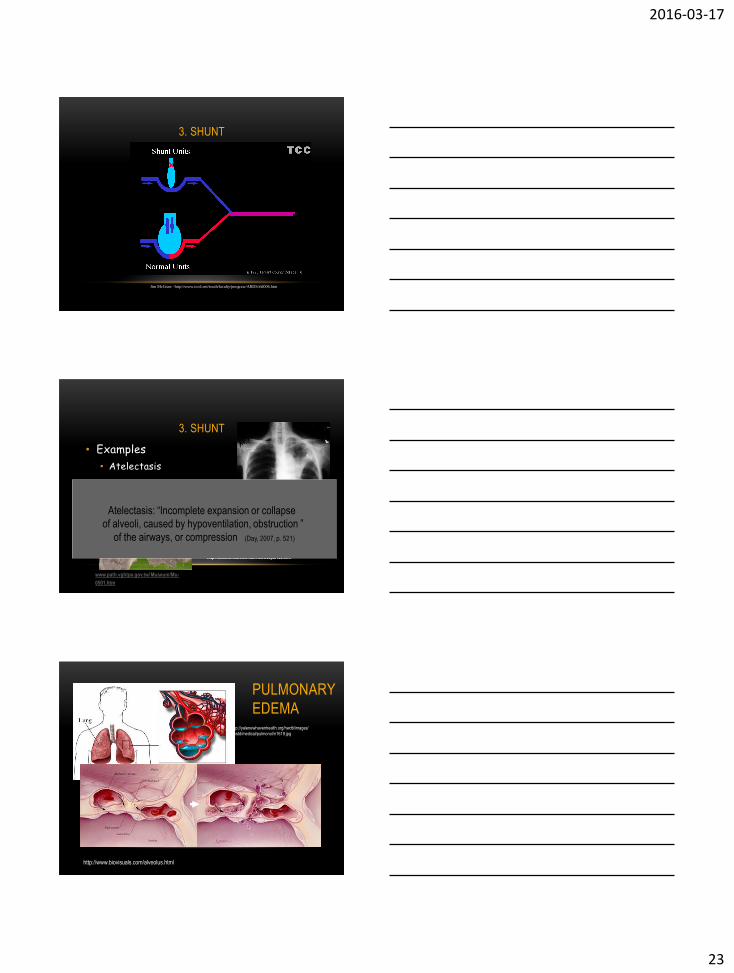
3. SHUNT
Jim McGraw -http://www.tccd.net/south/faculty/jmcgraw/ARDS/sld006.htm
3. SHUNT
• Examples
• Atelectasis
http://www.emedicine.com/med/topic180.htm
Atelectasis
www.path.vghtpe.gov.tw/ Museum/Mu-
0501.htm
Atelectasis: “Incomplete expansion or collapse
of alveoli, caused by hypoventilation, obstruction ”
of the airways, or compression (Day, 2007, p. 521)
PULMONARY
EDEMA
http://www.biovisuals.com/alveolus.html
http://yalenewhavenhealth.org/hwdb/images/
hwstd/medical/pulmonol/n1619.jpg
2016-03-17
24
Jim McGraw - http://www.tccd.net/south/faculty/jmcgraw/ARDS/sld012.htm
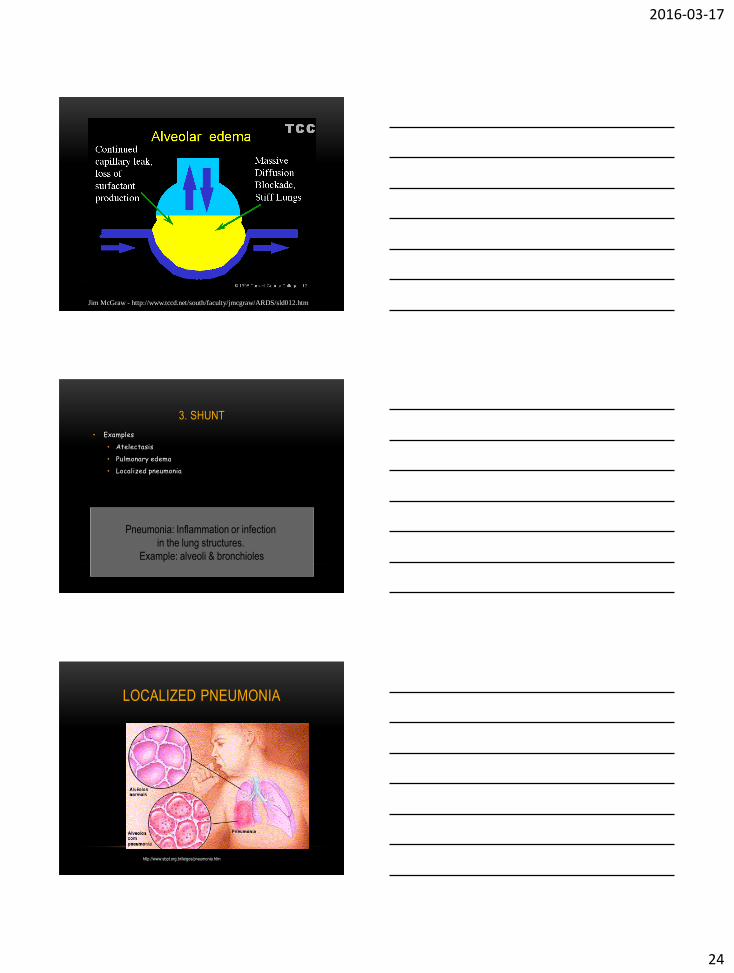
3. SHUNT
• Examples
• Atelectasis
• Pulmonary edema
• Localized pneumonia
Pneumonia: Inflammation or infection
in the lung structures.
Example: alveoli & bronchioles
LOCALIZED PNEUMONIA
http://www.sbpt.org.br/leigos/pneumonia.htm
2016-03-17
25
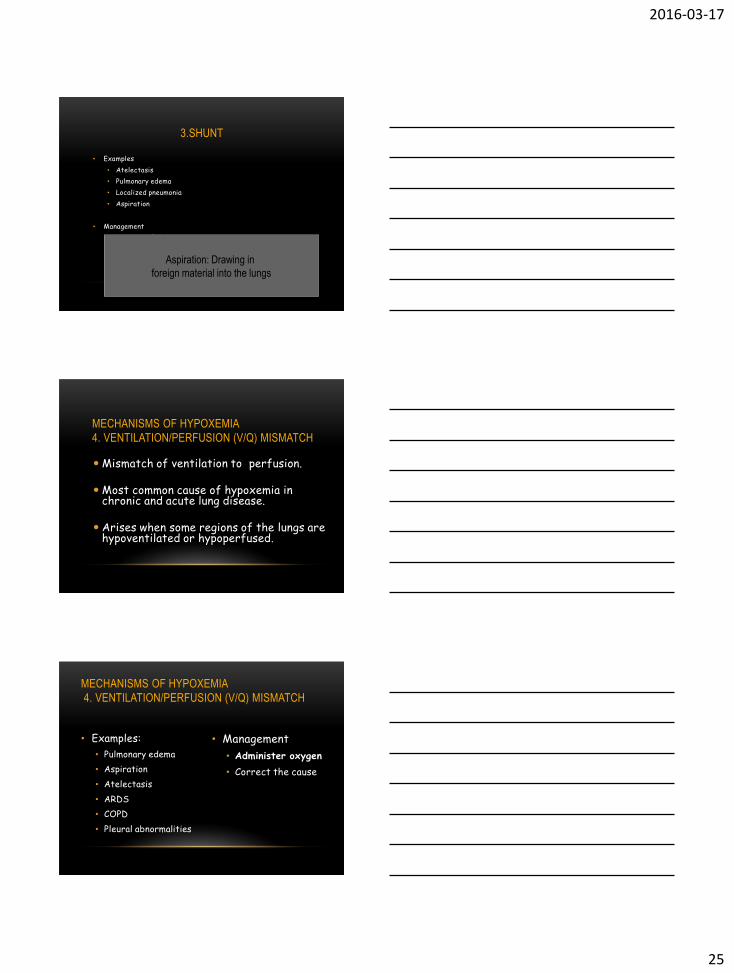
3.SHUNT
• Examples
• Atelectasis
• Pulmonary edema
• Localized pneumonia
• Aspiration
• Management
• ↓ amount of shunt
• Open up non-ventilating alveoli
• Treat causeAspiration: Drawing in
foreign material into the lungs
MECHANISMS OF HYPOXEMIA
4. VENTILATION/PERFUSION (V/Q) MISMATCH
Mismatch of ventilation to perfusion.
Most common cause of hypoxemia in chronic and acute lung disease.
Arises when some regions of the lungs are hypoventilated or hypoperfused.
• Management
• Administer oxygen
• Correct the cause
• Examples:
• Pulmonary edema
• Aspiration
• Atelectasis
• ARDS
• COPD
• Pleural abnormalities
MECHANISMS OF HYPOXEMIA
4. VENTILATION/PERFUSION (V/Q) MISMATCH

2016-03-17
26
SUMMARY OF KEY CONCEPTS
• Cellular injury
• Inflammation
• Hypersensitivity reactions
• Hypercapnia
• Mechanisms of Hypoxemia
QUESTIONS?
REFERENCES
Adams, M.P., Holland, L.N., Bostwick, P.M. & King (2010). Pharmacology for nurses: A pathophysiologic approach (Canadian ed). Toronto, ON: Pearson.
Copstead, L.C. & Banasik, J. L. (2010). Pathophysiology (4th ed.). St. Louis: Elsevier Canada.
Day, R., Paul, P., Williams, B., Smeltzer, S., & Bare, B. (2007, 2010). Brunner & Suddarth’s textbook of medical-surgical Nursing. Philadelphia: Lippincott Williams & Wilkins.






![Free Radicals in Andrology...supraphysiological levels, have a potential toxic effect on sperm quality and function [ 3 ]. Like other free radicals, ROS contain unpaired electrons](https://static.fdocuments.us/doc/165x107/60179a9b93287929057d97f5/free-radicals-in-supraphysiological-levels-have-a-potential-toxic-effect-on.jpg)










