PowerPoint Presentation john olver.pdfTitle PowerPoint Presentation Author Bianca Fedele Created...
17
29/11/2018 1 John OLVER AM MBBS MD FAFRM (RACP) Director Rehabilitation Epworth Healthcare Professor Rehabilitation Medicine Department of Medicine Monash University Long-Term Functional Outcome after Acquired Brain Injury (ABI) 0 10 20 30 40 50 60 70 80 Fatigue Balance Hearing Smell Vision Headaches Dizziness Epilepsy % 1 year post-injury 2 year post-injury 3 year post-injury 5 year post-injury 10 year post-injury Neurological Complaints by years post-injury
Transcript of PowerPoint Presentation john olver.pdfTitle PowerPoint Presentation Author Bianca Fedele Created...

29/11/2018
1
John OLVER AM MBBS MD FAFRM (RACP)
Director Rehabilitation Epworth HealthcareProfessor Rehabilitation MedicineDepartment of Medicine Monash University
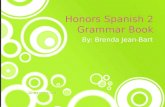
Long-Term Functional Outcome after Acquired Brain Injury (ABI)
0 10 20 30 40 50 60 70 80
Fatigue
Balance
Hearing
Smell
Vision
Headaches
Dizziness
Epilepsy
%
1 year post-injury
2 year post-injury
3 year post-injury
5 year post-injury
10 year post-injury
Neurological Complaints by years post-injury

29/11/2018
2
Areas responsible for olfactory functioning are vulnerable post TBI (due to the mechanics of the injury)
Injuries such as facial fractures (23.3% of patients) can damage sinonasal structures and limbic system which are central to sense of smell and taste
Olfactory impairment can affect 50-60% of patients yet is not routinely assessed in clinical settings. This results in significant rates of unawareness of the deficit
Olfactory Functioning – Sense of Smell
Drummond et al., 2015 ; Zandi & Hoseini, 2013
TEXT Loss of Sense of Smell Limitations
3. Food Preparation/Enjoyment
Unable to detect flavour (excessive use of salt/condiments)
Restrict engagement in social occasions based around food
1. Personal Safety (most serious)
Inability to detect gas, smoke or spoiled food. Can result in excessive checking (e.g. stoves)
4. Employment
Can affect employment (gas workers, chefs)
5. Personal Hygiene
Inability to monitor self body odours after exercise. Inability to determine whether clothes need washing
2. Relationships
Familiar smells of loved ones are lost, reduced intimacy
Drummond et al., 2013

29/11/2018
3
Identify the incidence of olfactory impairment in a consecutive sample of 134 adults post TBI admitted to Epworth HealthCare for rehabilitation
Compare the sensitivity and specificity of an olfactory function assessment scale which uses microencapsulation technique (scratch ‘n’ sniff)
UPSIT (Uni of Pennsylvania Smell Identification Test)
Investigate whether age, duration of post traumatic amnesia and facial fractures significantly predict the severity of olfactory impairment
Olfactory Impairment post TBI 3 Study Aims
Drummond et al., 2015
Olfactory Impairment post TBI Incidence using UPSIT
Drummond et al., 2015
66.4% of participants demonstrated olfactory impairment (12% more than the PST)
Of these patients, 25% had no sense of smell
In addition, 56% of patients were unaware that they had olfactory impairment

29/11/2018
4
Patient with olfactory impairment were:-
- Significantly older than those unimpaired and had worse injury severity (PTA) (non-sig)
Mean UPSIT score did not differ significantly for those with or without facial fractures
Only age and injury severity (PTA) significantly predicted UPSIT performance (10.3% total variance explained)
Participants were then followed up at 6 and 12 months post injury
Olfactory Impairment post TBI Predicting Olfactory Impairment
Drummond et al., 2015
This is simple dummy holder text.
Results
Although 68% (n=32) showed some improvement from baseline, only 1 in 4 scored within the normal range and these patients had mild olfactory impairment at baseline
Baseline assessment was the only significant predictor of 12month outcome (73.5% of the variance). Age, injury severity and facial factors were non-significant predictors
Study Aim
6-month follow up study investigated the natural progression and associated predictors of olfactory impairment from baseline
Participants / Method
Of the original sample who had OI (n=89), 47 adults participated. Mean age 43.1 years, mostly post severe TBI. Patients administered the UPSIT
Phase 3 – Olfactory Impairment at 6mths
Drummond et al., 2017

29/11/2018
5
This is simple dummy holder text.
Results
83.3% of patients presented with olfactory impairment(with 24% being completely anosmic)
44.4% did not show any improvement from baseline and 11.1% had a more severe level of olfactory impairment (only 1 in 6 reached normal limits)
Baseline assessment continued to be the only significant predictor of 12month outcome (61% of the variance)
Study Aim
To investigate the natural progression and predictive factors (age, injury severity, baseline UPSIT score) of olfactory impairment at 12 months post initial assessment
Participants / Method
37 adults (out of 76 eligible participants); mean age 42.3 years and predominately severe TBI. Patients re-administered the UPSIT and interview of experiences of having olfactory impairment
Phase 3 – Olfactory Impairment at 12mths
Drummond et al., 2017
Concussion

29/11/2018
6
‘A clinical syndrome characterized by immediate and
transient alteration in brain function from a mechanical force or trauma.’ It is a mild injury to the brain causing temporary disruption of normal brain function. Loss of consciousness (10-20% cases). Concussion should be seen as
an evolving injury in that symptoms might be delayed for several hours. 80-90% of
concussions will resolve within 7-10 days
What is Concussion?
American Association of Neurological Surgeons, (n.d.); Finch et al., 2013
Pathophysiology of Concussion – Acute?
Acute Pathophysiology:-
Ion imbalance, metabolic disruptions, blood flow abnormalities, autonomic nervous system dysfunction. K efflux, glutamate release, mitochondrial Ca overload and dec ATP production. Trying to restore ion balance turns on ATP pump and creates an energy crisis with the decreased ATP causing “spreading depression.” Resolves 1-4 weeks

29/11/2018
7
This is simple dummy holder text.
Psychological component
Post Concussion Syndrome:- 3 or more symptoms for 4 weeks)
Persisting ion imbalance Persisting autonomic dysfunction
Cervicogenic injury (causing neck pain and restriction, headache, numbness and tingling in arms or legs, dizziness, vomiting, tinnitus, visual problems
Pathophysiology of Concussion – PCS?
Acute Concussion
Subacute Concussion
Chronic Concussion
2 Weeks
4 Weeks
6 Weeks
8 Weeks
10 Weeks
12 Weeks
14 Weeks
Injury16
Weeks
80% Recover during this
stage
20% Take Longer: This is
who we see
The Three Groups

29/11/2018
8
Epworth Concussion Clinic Patient Demographics (n=165)
GenderMale 52.1%
Female 47.9%
Mean
Age35.38 years (14 – 77)
Medical
History
Anxiety 31.0%
Depression 24.2%
Traumatic Brain Injury
10.9%
Employment
Categories
Full-time 50.9%
Part-time 14.5%
Student (full-time)
12.1%Injury
Details
Loss Of
Consciousness 43.0%
First Concussion 45.5%
Number of prior
concussions1.84 (0 – 12)
Post-Concussion Symptom Checklist
Dischinger et al., 2009
4 symptoms can be diagnosed as post concussive syndrome
Physical symptoms are most common (cognitive/emotional symptoms are likely to persist longer than 3mth)
The best predictors of symptom persistence are noise sensitivity and anxiety

29/11/2018
9
PCS Checklist Preliminary Results (n = 60; time in clinic = 124 days
On admission to the clinic, physical and thinking symptoms were the most prominent (increased number/severity of symptoms)
By discharge, all symptom categories significantly decreased
There was also a significant increase in patients’ typical daily activity levels from admission (41.5%) to discharge (79.3%)
17.48
10.53
6.48 6.556.80
3.252.22 2.73
0
2
4
6
8
10
12
14
16
18
20
Physical Thinking Sleep Emotional
Admission to Clinic Discharge from Clinic
*significant difference p <.05
*
** *
Significant decrease in patient stress, anxiety and depression scores between admission to discharge (p <.05)
On admission, average anxiety levels were considered moderate and mild levels of depression
By discharge, patients achieved ‘normal levels’ on all three subscales
11.26
4.97
12.65
5.00
9.35
3.71
0
2
4
6
8
10
12
14
Admission Discharge
Depression Anxiety Stress
Depression Anxiety Stress Scale (preliminary, n=44)

29/11/2018
10
Brief Illness Perception Questionnaire (preliminary, n=43)
Key Item Scoring
Control How much control do you feel you have over your illness?
0 = absolutely no control; 10 = extreme amount of control
Symptoms How much do you experience symptoms from your illness?
0 = no symptoms at all; 10 = many severe symptoms
Concern How concerned are you about your illness 0 = not at all concerned; 10 = extremely concerned
Graph illustrates results from 3 questions on the BIPQ. There were significant, positive changes for all 8 questions
All other items on the BIPQ showed statistically significant changes from admission to discharge
Effect sizes were large for the three items displayed (e.g. Cohen’s d = 1.01 – 1.47)
Case Study Two – Female, 59 year old
This is simple dummy holder text.
Referral to Epworth Concussion Clinic
At the time, she was only managing 1-2 hours of work per day over 7 days. Subsequently referred to Epworth Concussion Clinic 1 month later (23rd August 17)
Concussion Details
Patient works from home and took a break going outside holding a washing basket
She went outside and lost balance, falling backwards hitting the back of her head on the windowsill. LOC for a few seconds, does not recall the fall (22nd June)
Acute and Ongoing Symptoms
Increased dizziness and nausea. Markedly increased anxiety when approached from behind
hospital ER: CT – no abnormalities and she was sent home. Saw a local doctor weekly – symptoms not improving
Past medical history: anxiety disorder, osteoarthritis

29/11/2018
11
Case Study Two Discharge Symptom Checklist
Symptoms none mild moderate severe P
hys
ica
l
Headache 0 1 2 3 4 5 6
Nausea 0 1 2 3 4 5 6
Vomiting 0 1 2 3 4 5 6
Balance Problem 0 1 2 3 4 5 6
Dizziness 0 1 2 3 4 5 6
Visual Problems 0 1 2 3 4 5 6
Fatigue 0 1 2 3 4 5 6
Sensitivity to Light 0 1 2 3 4 5 6
Sensitivity to Noise 0 1 2 3 4 5 6
Numbness/Tingling 0 1 2 3 4 5 6
Pain other than Headache 0 1 2 3 4 5 6
Th
inki
ng
Feeling Mentally Foggy 0 1 2 3 4 5 6
Feeling Slowed Down 0 1 2 3 4 5 6
Difficulty Concentrating 0 1 2 3 4 5 6
Difficulty Remembering 0 1 2 3 4 5 6
Sle
ep
Drowsiness 0 1 2 3 4 5 6
Sleeping Less than Usual 0 1 2 3 4 5 6
Sleeping More than Usual 0 1 2 3 4 5 6
Trouble Falling Asleep 0 1 2 3 4 5 6
Em
oti
on
al Irritability 0 1 2 3 4 5 6
Sadness 0 1 2 3 4 5 6
Nervousness 0 1 2 3 4 5 6
Feeling More Emotional 0 1 2 3 4 5 6
Patient was treated within the clinic for 61 days. On discharge, all symptoms completely resolved
On discharge, the patient was able to manage 90% of her usual daily activities (+60% change) and the patient resumed bike riding, swimming and paddle boarding
As a result of the experience, she changed her job and initiated a home business – developing an online programme of mindfulness, yoga and stress reduction techniques
https://www.safetyandquality.gov.au
Patient Reported Outcomes Measures – PROMs (ABI)
‘PROMs are questionnaires which patients complete. They ask for the patient’s assessment of how health services and interventions have, over time, affected their quality of life, daily functioning, symptom severity, and other dimensions of health which only patients can know. PROMs promise to fill a vital gap in our knowledge about outcomes and about whether healthcare interventions actually make a difference to people’s lives.’

29/11/2018
12
Global Stroke Community Advisory Panel (GSCAP)
GSCAP consists of 21 multidisciplinary stroke experts from 9 countries (Australia – 2, Austria, Canada, France, Germany, Singapore, Sweden, UK and USA)
Created by Allergan to improve education surrounding spasticity, stroke and post-stroke care. As part of the latter, GSCAP produced a checklist identifying ongoing, common problems post stroke
Participants / Method
37 adults; mean age 42.3 years and predominately severe TBI. Patients administered the UPSIT and interview of experiences of having olfactory impairment
Post Stroke Checklist Development
A list of the most common problems patients experience post stroke was initially generated by the GSCAP
Using Delphi methods, a consensus was reached on which of these problem areas were most important and relevant to include in the PSC
Swedberg 2017 ; Ekeland et al., 2017 ; Hagel 2005 ; Philp et al., 2012
- Designed as simple “easy to do” checklist- Provides a standardised approach for the identification of
long-term problems in stroke survivors- Covers wider aspects of quality of life- Should be carried out with patient (and care giver if needed)
- Ask patient each question, indicating the answer in the “response section”
- Generally, if answer is “No” observe patient’s progress- If answer is “Yes, follow-up with appropriate action
Following the trials of this checklist in Australia and other countries…. Could it be used as a PROM for TBI?
What?
How?
Most Common Issues Post Stroke Reported to General Practitioners Post Stroke Checklist (PSC) Version II
Philp et al., 2012

29/11/2018
13
Philp et al., 2012
The PSC was developed to help healthcare professionals identify the occurrence of 10 common persisting sequelae post-stroke that are amenable to treatment and suggests appropriate referral for treatment
Common long-term issues post stroke
Referral for treatment according to the patient’s response
Follow up questions to determine the impact of long-term problems
Philp et al., 2012

29/11/2018
14
Study Aim and Methodology
This international, collaborative study trialled the Post Stroke Checklist (PSC) in an Australian and Chinese population. The primary aim is to identify the frequency of long-term problems in patients at six months post stroke
PARTICIPANTS
210 participants were recruited from consecutive admissions to three stroke units (across Australia - 113 and China – 97)
Patients were administered the PSC at 6 months post injury and were also asked three questions relating to their satisfaction with the PSC and its relevance to their needs
Of the sample, 82.4% of patients have reported at least one deficit at 6 months. On average, patients were experiencing 3 problems at 6 months post stroke (SD=2.556, range = 0 – 10)
Post Stroke Checklist Study Results
The most prevalent symptom groups were:life difficulties, cognition,activities of daily living,mobility, mood and spasticity (all found to be the
most common issues as per Iosa et al. paper except for ADL)

29/11/2018
15
Patients have reported high levels of satisfaction with
the PSC (9.16 / 10)
Patients also considered the
checklist highly relevant and felt it identified their needs correctly
(9.22 / 10)
A third of patients requested their PSC responses be relayed
to a healthcare professional
Post Stroke Checklist – Patient Satisfaction
21.9%
26.6%
34.4%
50.0%
26.6%
28.1%
37.5%
42.2%
53.1%
43.7%
40.6%
29.3%
70.7%
75.6%
73.2%
43.9%
41.5%
39.0%
65.9%
56.1%
51.2%
63.4%
10.0%
16.7%
24.0%
21.3%
7.3%
11.3%
21.3%
14.7%
17.3%
12.0%
9.3%
24.7%
60.8%
47.4%
44.3%
25.8%
4.1%
19.6%
24.7%
54.6%
56.7%
9.3%
16.8%
38.9%
44.2%
28.3%
26.5%
21.2%
9.7%
34.5%
23.9%
27.4%
16.8%
0% 50% 100% 150% 200% 250%
Carer Relationship
Life after stroke
Cognition
Mood
Communication
Continence
Pain
Spasticity
Mobility
Activities of daily living
Absence of secondary prevention
Italy UK Singapore China Australia
Iosa et al., 2017 ; Ward et al., 2014
Italy (n=64), UK (42), Singapore (100), China (97),
Australia (113). Spectrum of long term issues post stroke across 5 countries

29/11/2018
16
11.5%
11.5%
23.0%
29.5%
23.8%
36.1%
36.9%
41.0%
51.6%
36.9%
16.4%
23.0%
23.0%
27.9%
29.5%
41.0%
50.8%
50.8%
55.7%
*59.0%
60% 40% 20% 0% 20% 40% 60%
INCONTINENCE
PAIN
RELATIONSHIP WITH FAMILY STRESSES
SPASTICITY
COMMUNICATION DIFFICULTIES
MOOD
MOBILITY LIMITATIONS
ACTVITIES OF DAILY LIVING DIFFICULTIES
LIFE LIMITATIONS (WORK, HOBBIES)
COGNITIVE DIFFICULTIES
Female
Male
Frequency of Persisting Problems by Gender Results
Overall 82.5% patients reported at least one deficit at 6 months; with a higher incidence amongst females (86.9%) compared to males (80.3%) (non-significant)
The top 5 symptoms were the same for males and females but the number affected were different (greater in females)
Persisting Problems by Gender Results
Females reported significantly more cognitive difficulties than males (59.0% to 36.9%, *p<0.01)
Females are over twice as likely to report persisting cognitive difficulties at six months post stroke (Odds Ratio: 2.46, 95% Confidence Interval (CI) = 1.31 - 4.62)
Females also reported increased mobility limitations (50.8% to 36.9%), pain (23.0% to 11.5% - trending towards significance; p=.070), difficulties performing activities of daily living (50.8% to 41.0%) and communication difficulties (29.5% to 23.8%)
Cognition was the only significant predictor of symptom presentation differentiating between females and males

29/11/2018
17
Conclusion
Without a lot of modification, this checklist can be
trialled as a PROM for TBI
Epworth Monash Rehabilitation Medicine Unit Research Team
Thank you
Email: [email protected]