

Power point pulmonary pathophysiology - v.1
408
Pulmonary Pathophysiology
-
Upload
stephen-collins -
Category
Healthcare
-
view
1.471 -
download
0
Transcript of Power point pulmonary pathophysiology - v.1

Pulmonary Pathophysiology

Suggested HW: Complete the end of
chapter questions for:
• CH 11-30• ANSWERS TO THESE QUESTIONS FOUND ON
EVOLVE WEBSITE
• EXAM WILL PARTLY COME FROM THESE CHAPTER
QUESTIONS

Educational Objectives
• List the etiology and risk factors, clinical manifestations,
pathological changes, and diagnostic results for:
– Bronchitis
– Pulmonary emphysema
– Asthma
– Bronchiectasis
– Pulmonary infections
– Acute respiratory distress syndrome (ARDS)
– Interstitial lung disease (ILD)
– Lung cancer
– Pulmonary Vascular Disorders
– Neuromuscular Disorders
– Pleural Diseases (including pneumothorax)
Educational Objectives
• Differentiate and define obstructive pulmonary
disease and restrictive pulmonary disease
Classification of Pulmonary Disorders
• Obstructive disease
– Causes a decrease in the rate of airflow in the
conducting airways
• Restrictive disease
– Causes a decrease in the volume of lung, especially
the inspiratory capacity and vital capacity
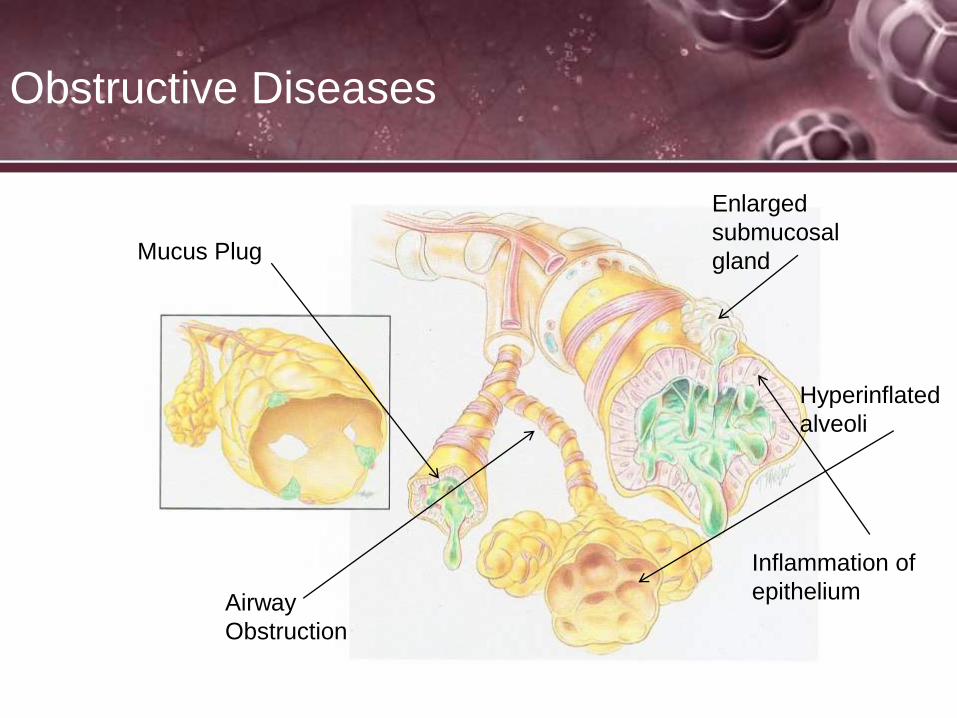
Obstructive Diseases
Airway
Obstruction
Enlarged
submucosal
gland
Hyperinflated
alveoli
Mucus Plug
Inflammation of
epithelium

Chronic Obstructive Pulmonary Disease
• A group of disorders characterized by progressive
limitations in predominantly expiratory airflow that
are partially reversible by bronchodilator or anti-
inflammatory therapy
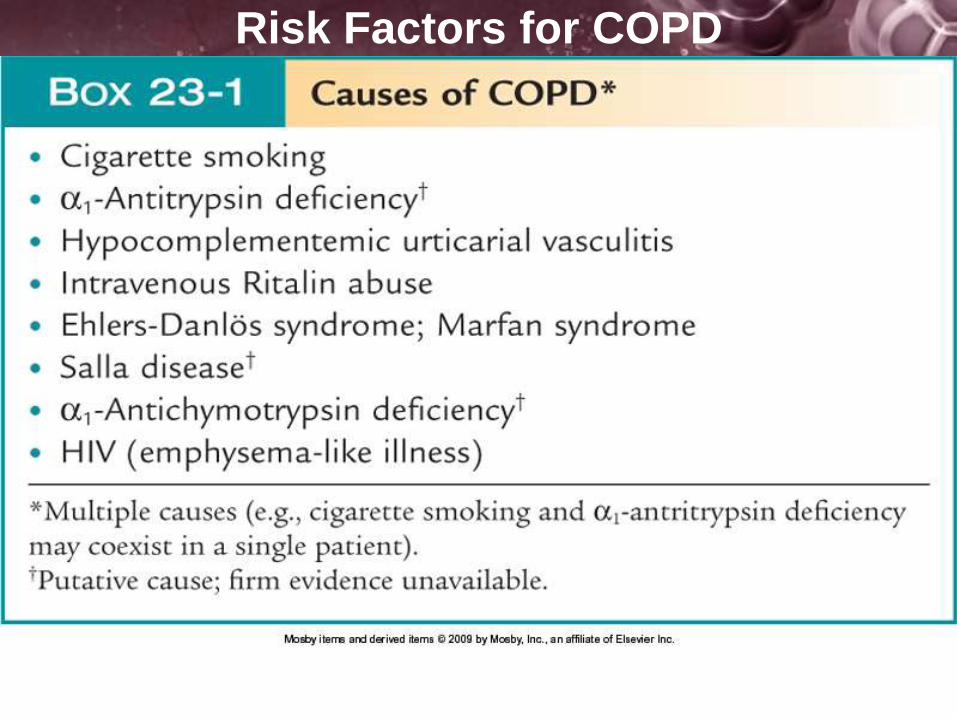
Risk Factors for COPD

Definitions
• FVC Forced vital capacity: the determination of the vital
capacity from a maximally forced expiratory effort
• FEV1 Volume that has been exhaled at the end of the
first second of forced expiration
• PEF The highest forced expiratory flow measured with a
peak flow meter
• MVV Maximal voluntary ventilation: volume of air
expired in a specified period during repetitive maximal
effort
• MIP: Maximum inspiration (IC), used to assess
diaphragm strength

Forced Vital Capacity
• Vital capacity is the maximum amount of air a person can expel from
the lungs after a maximum inspiration. It is equal to the inspiratory
reserve volume plus VT plus the expiratory reserve volume.
• A person's vital capacity can be measured by a spirometer
• In combination with other physiological measurements, the vital
capacity can help make a diagnosis of underlying lung disease. The
unit that is used to determine this vital capacity is the millilitre (mL).
• A normal adult has a vital capacity between 3 and 5 litres.
Predicted normal values for VC depend on age, sex, height,
weight and ethnicity

Overall Classification of Pulmonary
Disorders
• Obstructive Disease (COPD)
– Causes a decrease in the rate of airflow in the conducting
airways, causes an increase in residual volume due to air
trapping
FEV1 , FVC , FEV1/FVC < 70% of predicted, TLC > 120% of predicted,
RV > 120% of predicted, MMV , DLCO < 80% of predicted, PEF

Overall Classification of Pulmonary
Disorders
• In obstructive lung disease, the FEV1 is reduced due to
obstruction to air escape. Thus, the FEV1/FVC ratio will
be reduced.
• More specifically, the diagnosis of COPD is made when
the FEV1/FVC ratio is less than 70%.
• The Global Initiative for Obstructive Lung Disease
(GOLD) criteria also require that values are after
bronchodilator medication has been given to make the
diagnosis
• Dx: Pre-post bronchodilator testing with Spriomtery
testing. In Emphysema/Bronchitis small change less
than 5%; Asthma typically changes >12% or 200 mL

Overall Classification of Pulmonary
Disorders
• Restrictive Disease (everything besides COPD)
– Causes a decrease in the volume of lung, especially the
inspiratory capacity and vital capacity
FEV1 , FVC , FEV1/FVC or normal, TLC < 80% of predicted,
RV < 80% of predicted, MVV , DLCO > 120-140% of predicted,
PEF normal or increased

Overall Classification of Pulmonary
Disorders
• In restrictive lung disease, the FEV1 and FVC are
equally reduced due to fibrosis or other lung pathology
(not obstructive pathology).
• Thus, the FEV1/FVC ratio should be approximately
normal, or even increased due to an increased FEV1
value (because of the decreased compliance associated
with the presence of fibrosis in some pathological
conditions).

Spirogram

Spirogram Capacities and Volumes
• TLC Total lung capacity: the volume in the lungs at
maximal inflation
• RV Residual volume: the volume of air remaining in the
lungs after a maximal exhalation
• ERV Expiratory reserve volume: the maximal volume of
air that can be exhaled from the end-expiratory position
• IRV Inspiratory reserve volume: the maximal volume
that can be inhaled from the end-inspiratory level

Spirogram Capacities and Volumes
• IC Inspiratory capacity: the sum of IRV and TV
• IVC Inspiratory vital capacity: the maximum volume of
air inhaled from the point of maximum expiration
• VC Vital capacity: the volume equal to TLC − RV
• VT Tidal volume: that volume of air moved into or out of
the lungs during quiet breathing
• FRC Functional residual capacity: the volume in the
lungs at the end-expiratory position RV/TLC% Residual
volume expressed as percent of TLC
FEV1/FVC ratio
• The FEV1/FVC ratio, also called Tiffeneau index, is a calculated ratio
used in the diagnosis of obstructive and restrictive lung disease
• It represents the proportion of the forced vital capacity exhaled in the
first second
• Normal values are approximately 80% of predicted
• Predicted normal values are calculated based on age, sex, height,
weight and ethnicity, sometimes smoking
• A derived value of FEV1% is FEV1% predicted, which is defined as
FEV1% of the patient divided by the average FEV1% in the population
for any person of similar age, sex and body composition.

DLCO
• DLCO test is performed by having the test subject blow out all of the
air that they can to reach residual volume.
• The person then takes a full vital capacity inhalation of a test gas
mixture that contains a small amount of carbon monoxide (usually
0.3%) and some helium or other non-absorbed tracer gas.
• The test gas is held in the lung for about 10 seconds and then is
exhaled from the lung. The first part of the expired gas is discarded
and the next portion which represents gas from the alveoli is collected.
• By analyzing the concentrations of carbon monoxide and helium in the
inspired gas and in the exhaled gas, it is possible to calculate how
much carbon monoxide was taken up during the breath hold, and what
the partial pressure of carbon monoxide was during the breath hold.
This method is known as the single-breath diffusing capacity
test.

DLCO
• Values between 75% and 125% of average diffusion
capacity in the healthy population are considered
normal.
• The diffusing capacity (DLCO) is a test of the integrity of
the alveolar-capillary surface area for gas transfer. It
may be reduced in disorders that damage the alveolar
walls (septa) such as emphysema, which leads to a loss
of effective surface area. The DLCO is also reduced in
disorders that thicken or damage the alveolar walls such
as pulmonary fibrosis.
• Lung Volumes and DLCo

Chronic Obstructive Pulmonary
Disease
• May be preventable and treatable. Disease state
characterized by airflow limitation that is not fully responsive
to bronchodilator therapy. The airflow limitation is
progressive and associated with an abnormal inflammatory
response of the airway.
• Primary cause is cigarette smoking
• A significant response to the bronchodilator is considered by
an increase in the FEV1 by 12% AND an increase in VC by
200 mL.

Therapy at Each Stage of COPD

Epidemiology
• Some 16 Million Americans are affected
• COPD is the 3rd leading cause of death in the U.S.
• COPD caused 726,000 hospitalizations in 2000
• Total health expenditure of $32.1 Billion in 2000
• Most common form of COPD is Chronic Bronchitis

Risk Factors for COPD
1. Cigarette smoking/passive smoking
2. Pollution
3. Occupational exposure to dust and
fumes
4. Recurrent lung infections
5. Hereditary factors
6. Allergies
7. Socioeconomic factors
8. Alcohol ingestion
9. Age
Chronic Obstructive Pulmonary
Disease
• Smoking
– #1 cause of COPD
– Increased mucous production
– Inhibition of mucociliary clearance
– Toxicity of inhaled gases and particulates
– Bronchospasm
– Decrease in macrophage activity
– Disruption of the alveolar wall and capillary endothelium

General Manifestations of COPD
1. Small airways ( < 2mm) are most susceptible to airway obstruction in COPD
2. Diagnosed by PFT, clinical signs and symptoms
3. Early to middle manifestations of COPD include:
I. Changes in pulmonary function testing
II. Shortness of breath with exertion
III. Changes in CXR
IV. Increases in sputum production
V. Cough
VI. Recurrent pulmonary infections
VII.Wheezing
4. Late manifestations of COPD include:
I. Accessory muscle usage
II. Edema from Cor Pulmonale
III. Mental status changes from chronic hypoxia/hypercapnea
IV. Clubbing of fingers
V. Barrel Chest or Increased A-P Diameter

Chronic Obstructive Pulmonary
Disease
• ystic Fibrosis
• ronchitis – Chronic
• sthma
• ronchiectasis
• mphysema
• ronchiolitis

Emphysema

What is Emphysema?
Loss of elastic recoil
This loss of recoil leads to an
increased compliance and
inability to expel gas out of the
alveoli
Leading to trapped air in the
lung
Alveoli cluster together forming
“blebs”
Understanding COPD
Emphysema

What is Emphysema Cont…
Damage occurs to the tiny airways in the lungs called bronchioles. Bronchioles are joined to alveoli, tiny grape-like clusters of sacs in the lungs where oxygen from the air is exchanged for carbon dioxide from the body. The elastic properties of the lung reside in the tissue around the alveoli
Because the lungs lose elasticity they become less able to contract.
This prevents the alveoli from deflating completely, and the person has difficulty exhaling.
Emphysema Cont…
• Hence, the next breath is started with more air in the
lungs.
• The trapped "old" air takes up space, so the alveoli are
unable to fill with enough fresh air to supply the body
with needed oxygen.

Pulmonary Emphysema
• Centrilobular emphysema
– Abnormal weakening and
enlargement of the respiratory
bronchioles in the proximal
portion of the acinus
– Primary changes occur in
upper lobes
– High correlation with smoking
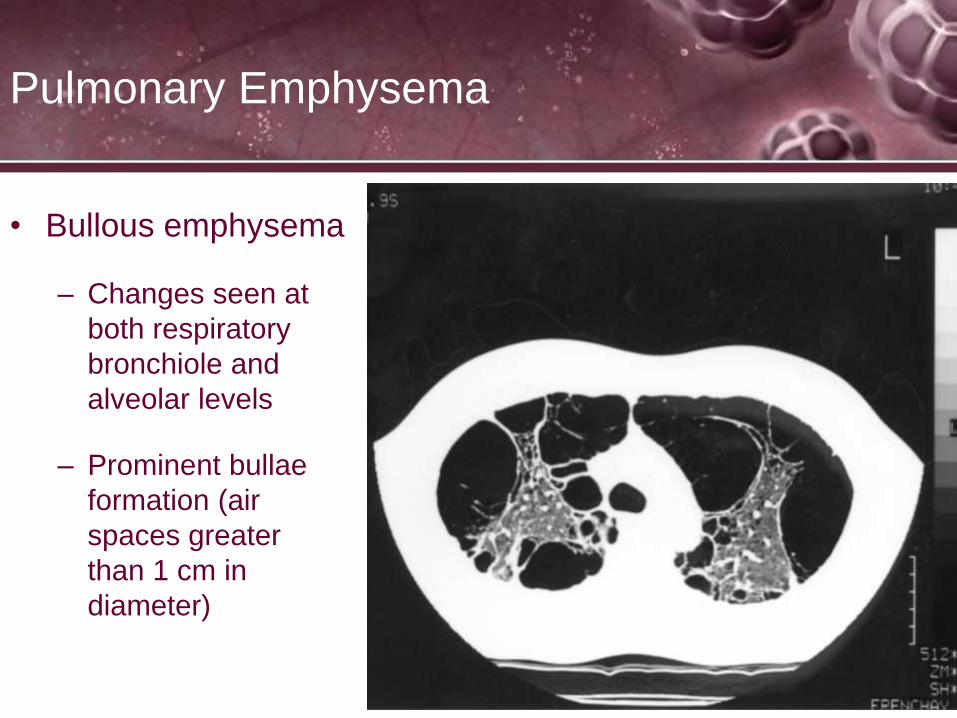
Pulmonary Emphysema
• Bullous emphysema
– Changes seen at
both respiratory
bronchiole and
alveolar levels
– Prominent bullae
formation (air
spaces greater
than 1 cm in
diameter)

Emphysema Cont…
A person with emphysema may feel short of breath
during exertion and, as the disease progresses, even
while at rest.
Emphysema is one of several irreversible lung diseases
that diminish the ability to exhale. This group of diseases
is called chronic obstructive pulmonary disease
(COPD). The two major diseases in this category are
emphysema and chronic bronchitis, which often
develop together.

Accessory muscle use

Emphysema
Typically, symptoms of emphysema appear only after 30
to 50 percent of lung tissue is lost.
Emphysema rates are highest for men age 65 and older.
More people in the Midwest have emphysema than in
any other region in the country.
Emphysema is an irreversible disease that can be
slowed but not reversed or stopped.

Causes
• Generally, lungs become damaged because of reactions to irritants entering the airways and alveoli. Researchers continue to investigate the factors that may make some people more susceptible to emphysema than others. But there are some clear causes for emphysema:
• Cigarette smoking
• Alpha-1 antitrypsin deficiency

Other Cause
Alpha-1 Antitrypsin Deficiency
• People who a deficiency of a protein called alpha-1 antitrypsin (AAT) are at a higher risk of developing severe emphysema. Alpha-1 antitrypsin deficiency (AAT deficiency) is an inherited condition and occurs in varying degrees

AAT
• AAT is thought to protect against some of the damage caused by macrophages. In AAT deficiency-related emphysema, the walls of the bronchial tubes and the alveoli are both damaged, often leading to severe disease.
• About 2 out of every 1,000 people have an alpha-1 antitrypsin deficiency. People who smoke and have AAT deficiency are almost certain to develop emphysema.

Causes
Cigarette smoking is the major cause of emphysema. When exposed to cigarette smoke, the air sacs of the lungs produce defensive cells, called macrophages, which "eat" the inhaled particles. But macrophages are stimulated to release materials which can destroy the proteins that let the lungs expand and contract, called elastin and collagen.
Cigarette smoke also damages the cilia, tiny hair-like projections in the bronchi that "sweep" foreign bodies and bacteria out of the lungs

Symptoms
The first sign of emphysema is shortness of breath during exertion.
Eventually, this shortness of breath occurs while at rest. As the
disease progresses, the following symptoms which are related to one
of the other major lung diseases also caused by smoking - bronchitis
- may occur:
• Difficulty breathing (dyspnea)
• Coughing (with or without sputum)
• Wheezing (this can also be caused by emphysema itself)
• Excess mucus production
• A bluish tint to the skin (cyanosis)
• Hypoxemia
• Tachycardia
• Polycythemia
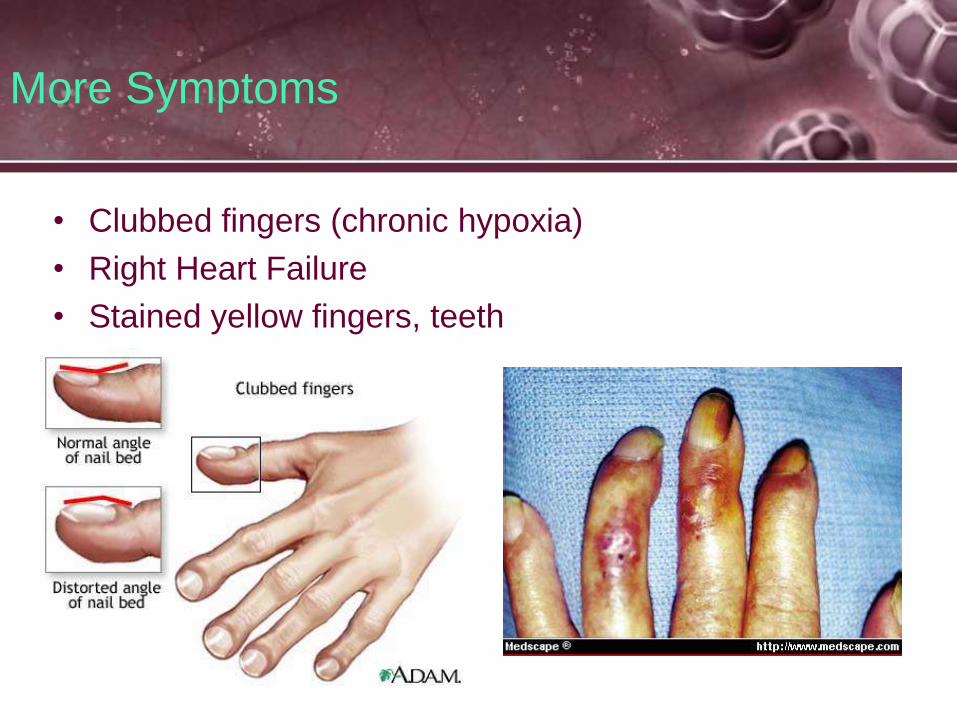
More Symptoms
• Clubbed fingers (chronic hypoxia)
• Right Heart Failure
• Stained yellow fingers, teeth

Diagnosis
History And Physical Examination
Smoking history (calculate pack years, # packs smoked times # years smoked)
Working environment- breathing in any harmful chemicals?
A physical examination will include an examination of your chest and breathing patterns; prolonged expiratory times
Nasal flaring, accessory muscle usage (due to loss of diaphragm recoil from air trapping)

Diagnosis Continued
X-Ray and/or CT of the Chest
Chest x-rays are a very useful tool to evaluate anatomy of the lung. In emphysema, there is evidence of increased air in the chest and destruction of some of the lung tissue. Bronchitis can be suspected on a chest x-ray by presence of thickening of the tissue around the large airways (bronchi). Chest x-rays are also useful as screening for lung cancer and heart disease.
Computerized axial tomography or CAT scans indicate lung anatomy in greater detail. In some cases, this information is needed to fully evaluate lung disease.

• Routine lung function tests can help define the kind and amount of damage to the lungs. The following tests can identify various stages of emphysema:
• Spirometry measures breathing capacity. A common measure of breathing capacity is the forced expiratory volume in one second (FEV1), or the amount of air that can be forced out of the lungs in one second. This is a common way to determine the amount of airway obstruction.
Lung Function Tests

Lung Function Tests
• Frequently, your physician will ask that spirometry and body plethysmography be repeated after administration of an inhaled bronchodilator
• This test will help your physician determine if there is an asthmatic component present
• Lung Volumes measures the amount of air in the lungs. This increases markedly in emphysema.

Lung Function Tests
• Diffusing Capacity measures the ability of the lung to transfer the gases from the air to the blood and vice versa. Decrease in diffusing capacity allow fairly accurate estimation of amount of emphysema.
• Body Plethysmography is a rapid way of evaluating both degree and type of obstruction and lung volumes. It is a useful adjunct to understanding the mechanism of airway obstruction - e.g., asthma vs emphysema.
• Arterial blood gases (ABG) analyzes blood from an artery for amounts of carbon dioxide and oxygen. This test is often used in more advanced stages of emphysema to help determine if a person needs supplemental oxygen.

Lung Function Tests
Arterial Blood Gas
• Patient’s with emphysema have chronic CO2 retention
due to the inability to expel gas. Their blood reflects
higher levels of CO2 than normal people; CO2 is acidic
in nature.
• Over time their body compensates for this higher CO2
by creating more buffer in the blood in the form of
HCO3- from the kidneys.
Emphysema Diagnosis Cont…
Tests For Alpha-1 Antitrypsin Deficiency
The symptoms of alpha-1 antitrypsin deficiency-related
emphysema tend to appear between the ages of 30 and
40. The symptoms and diagnostic tests are basically the
same in any kind of emphysema except that, in this
disease, emphysematous changes are greatest in the
lower lung. However, if AAT deficiency is suspected, a
special blood test can confirm the diagnosis.

Treatment for Emphysema
• There is no cure for emphysema. The goal of treatment is to slow the development of disabling symptoms. The most important step to take is to stop smoking.
• Treatments for emphysema caused by smoking include medication, breathing retraining, and surgery.
• People with inherited emphysema due to alpha-1 antitrypsin deficiency can receive alpha 1-proteinase inhibitor (A1PI), which slows lung tissue destruction.

Breathing TechniquesDiaphragmatic Breathing
• The diaphragm is a major muscle used in breathing and is located beneath the lowest two ribs. At rest, the diaphragm muscle is bell shaped. During inspiration, it lowers and flattens out.
• Optimizing the use of the diaphragm is beneficial because it pulls air into the lower lobes of the lungs where more gas exchange takes place. Not only is the diaphragm the most efficient of all respiratory muscles, but using it tends to be very relaxing and calming.
• Along with our diaphragm, we use intercostal and abdominal muscles in the work of breathing. The intercostals (muscles between the ribs) pull to lift the rib cage up and out. This causes the lungs to open in all directions and air can be pulled down the airways. To exhale, the muscles that have been pulling relax and air is forced out.
• The diaphragm tenses, pulling air in; and relaxes, letting the spring of the ribs push the air out again.

Breathing Techniques
Diaphragmatic Breathing
Pursed Lip Breathing
How:
• Breathe in through your nose.
• Purse lips slightly as if to whistle.
• Breathe out slowly through pursed lips.
• Do not force the air out.
• Pursed Lip Exercise

Medications Used
Medications To Treat Emphysema
Emphysema cannot be cured and, except for oxygen, does not reverse with any medication. However, emphysema is frequently associated with bronchitis and asthma and the symptoms associated with these processes often can be alleviated with medication (hence, you can see the value of pulmonary function and other tests designed to discover if there is asthmatic component present:
Bronchodilator medication
Corticosteroids
Supplemental oxygen

Bronchodilator Medication
• Bronchodilator medication may be prescribed for airway tightness. Bronchodilators react similar to norepinephrinethrough the sympathetic nervous system
• The most commonly prescribed bronchodilators are beta2 agonists, the anti-cholinergic drug ipatropiumbromide, and theophylline.
• Anti-cholinergics block musacaric receptors which normally respond to acetylcholine and cause bronchoconstriction
Medications Used

Medications Used
Corticosteroids
• The potent anti-inflammatory medications known as corticosteroids - commonly called steroids - may be used to help lessen the inflammation that often accompanies emphysema. These may be taken by mouth or inhaled.

Oxygen
• Due to the chronic state of increased CO2 in the blood (hypercapnia), the patient has adapted a breathing regulation in the brain that responds to changes in O2
and not CO2 like most people
• If you give a patient with COPD more than 30% oxygen they will slow their breathing
• Give low flow oxygen at 2 LPM by NC
• Or high flow oxygen with a venturi mask at 22-30%
• What Would Happen If The World Lost Oxygen For 5 Seconds?
• Home Oxygen Therapy, What To Expect
Surgical Interventions
• Surgical treatments for emphysema remain experimental and are not covered by insurance. Most people with emphysema are not candidates for surgery.
• Two types of surgery for people with emphysema are:
• Lung Reduction
• Lung Transplantation
• History of lung volume reduction surgery
Lung Reduction
A surgical procedure called lung reduction may improve symptoms for people with certain types of emphysema. During the procedure, part of the lung is cut out, giving healthy lung tissue more room to expand.
Lung reduction may eliminate the need for supplemental oxygen and make it much easier for the person to breathe. Early studies show that it reduces the volume of the over-inflated lungs. This improves the ability of the lung and chest wall to spring back during exhalation. This more-elastic lung appears to be the biggest reason that emphysema sufferers experience relief.

Conclusion
Emphysema is a chronic disease that takes years to progress; usually as a result of heavy cigarette smoking but also can be caused by inherited Alpha-1 antitrypsin deficiency
It destroys the stability of the alveoli and bronchioles leaving them over compliant
This leads to air trapping and an accumulation of CO2 and decrease in O2
The air trapping leads to dyspnea
Diagnose with symptoms, ABG, CXR, PFT and history
Treatment consists of stop smoking, medications and lung reduction surgery or transplant

Cystic Fibrosis(Mucoviscidosis)

Cystic Fibrosis
• Hereditary Disease
• Most common lethal genetic disease among Caucasian
Americans
• Affects 30,000 persons in the U.S.
• Mean life expectancy – +/-(5 years) 38 yrs.
• Caused by a genetic mutation of the gene coding for a
large protein that controls the movement of chloride ions
through the cell membrane.
• Movement of chloride is vital to the proper production
and regulation of secretions in the lungs, pancreas,
sweat glands and others.

Introduction
• CF is an inherited disease of your mucus and sweat glands
• It affects mostly the lungs, pancreas, liver, intestines, sinuses and sex organs
• An abnormal gene causes mucus to become extra thick and sticky
• This gene makes a protein that controls the movement of salt and water not work properly (retaining salt=thick secretions)
• This leads to mucus plugs

Introduction Continued
• Mucus plugs lead to collapsed lungs (atlectasis)
• Increased mucus in the lungs also allows for more bacterial growth which leads to frequent pneumonia
• Constant infections lead to inflammation in the lung
Introduction Continued
Cystic fibrosis is the most common cause of chronic
genetic lung disease in children and young adults,
and the most common fatal hereditary disorder
affecting Caucasians in the US.
CF is a multi-system disorder of exocrine glands causing
the formation of a thick mucus substance that affects
the lungs, intestines, pancreas, and liver. The
standard test for diagnosis is a sweat test which
evaluates the level of chloride excreted by the body.

Cystic Fibrosis
• Chloride levels in sweat is elevated due to lack of
normal removal, as a result CF patients are vulnerable
to dehydration. A sweat chloride test is used for the
diagnosis of the disease (> 60mEq/L in infants and > 80
in adults)
• Pancreatic insufficiency reduces the number of
digestive enzymes. These patients experience
malnutrition, diarrhea, vitamin deficiency and
undigested fat in the stool.

Diagnosis
The sweat chloride test is performed to determine the amount of
chloride that is excreted in sweat from the body during a certain
period of time. The test may be performed on infants to determine if
cystic fibrosis is present. Children with cystic fibrosis have
increased sodium and chloride concentrations in their sweat.
Normal Sweat
18 mEq/L
Positive Test
60 mEq/L

• Often the first sign of CF
begins after birth, the
mother kisses the baby
and they taste salty.
• Poor feeding occurs from
blocked bile ducts (bile
released from pancreas
helps digest food)
Diagnosis

Diagnosis

Diagnosis
• Cystic Fibrosis: Early Intervention
• Genetic Carrier Testing — More than 10 million Americans are
symptomless carriers of the defective CF gene. This blood test can
help detect carriers, who could pass CF onto their children. To have
cystic fibrosis, a child must inherit one copy of the defective CF gene
from each parent.
• Each time two carriers of the CF gene have a child, the chances are:
• 25% (1 in 4) the child will have CF;
• 50% (1 in 2) the child will carry the CF gene but not have CF; and
• 25% (1 in 4) the child will not carry the gene and not have CF

Diagnosis

Diagnosis Continued
Diagnosis Continued
• Detailed medical history is obtained (CF is Hereditary)
• Chest X-RAY to show scarring from frequent
inflammation
• Sinus X-RAY
• Pulmonary Function Test (CF is a COPD); used only
with individuals old enough to comply > 8years old
usually
• Sputum Cultures to determine certain bacteria growth
• Blood tests to find abnormal CF gene

Symptoms

Symptoms
• Increased WOB from plugged airways and air trapping
• Tenacious Secretions
• Frequent productive cough
• Frequent bouts of bronchitis and pneumonia
• Dehydration and malnutrition despite huge appetite;
failure to thrive
• Infertility (mostly in men)
• Ongoing diarrhea and stomach pain

Cystic Fibrosis
Finger Clubbing

Cystic Fibrosis
Radiologic Findings:
1. Translucent (dark) lung
fields
2. Depressed or flattened
diaphragms
3. Right ventricular
enlargement
4. Areas of atelectasis
and fibrosis
Occasionally:
1. Abscess formation
2. Pneumothorax

CF leads to…
• Sinusitis: the sinuses have mucus build up leading to headaches, ear and equilibrium problems.
• Bronchiectasis: damaged lungs become overly stretched and retain secretions and gas.
• Pancreatitis: Leads to inability to digest food, leading to bowel obstruction and sepsis.
• Liver Disease, Diabetes, Gallstones and low bone density from lack of Vitamin D.

CF leads to Respiratory failure
• The mucus plugs the airways causing collapse of
the alveoli and increased WOB
• Increased PaCO2, decreased PaO2 and eventual
death if not treated.
• Infections lead to inflamed and damaged lung lining
• Blocked pancreas leads to vitamin deficiencies
• There is no cure for CF only treatments; average life
span is 38 years

Treatments for CF
• Chest physiotherapy (CPT) is the traditional means of airway clearance in CF. It uses postural drainage in various positions, percussion, vibration, deep breathing, and coughing to loosen and move secretions out of the lungs. The treatment time including an aerosol before is about 45 minutes. Done so by using manual percussion with hand, pneumatic precursor with device or by Vest.

Treatment for CF
Chest Physical Therapy:
Using the “Vest” or manual
precursor. Helps loosen
secretions with percusion

Treatment Continued
• PEP is a technique that uses a hand held device
which can be used with a nebulizer attached. It
has a restricted orifice. When exhaled into, this
creates pressure in the lungs. This pressure
allows air to enter behind areas of mucus
obstruction and keeps the airways open during
exhalation. As you exhale, mucus moves
towards the larger airways, so it can be more
easily coughed up with the huff technique. PEP
can be taught to children as young as 5 years,
and can be passively given to infants via a
mask. The treatment time is about 20 minutes.

PEP Device
Treatment Continued
• Vibratory Positive Expiratory Pressure (Flutter®,
Acapella®)
Vibratory positive expiratory pressure is a hand held
device. Exhaling into this device results in oscillations
of pressure and airflow which vibrate the airway walls
(loosening mucus), helps hold the airway open (which
allows air to get behind secretions and keeps the
airways open during exhalation). It speeds up airflow
helping mucus move up to the larger airways where it
can be more easily coughed up. Vibratory PEP can
be taught to children as young as 2 years old by
mask, and to ages 5 and up via mouthpiece.
Treatment time is about 20 minutes.
Treatment Continued…
Intrapulmonary Percussive Ventilation.
The IPV is a pneumatic (air driven) device that
delivers both continuous airway pressure and mini
bursts of air. At the same time the IPV delivers a
dense aerosol.
The combination allows air to
enter behind mucus blockage,
and vibration to dislodge mucus
from the airway walls so it can
be more easily coughed up.
IPV
Treatment Continued
• Active Cycle of BreathingActive cycle of breathing is a series of breathing techniques, consisting of thoracic expansion exercises (deep breathing), breathing control (using the diaphragm), and the forced expiration technique (huff). These breathing cycles are performed in various positions of drainage similar to CPT positions but without the percussion. This can be taught at about the age of 8 years. Treatment time, including an aerosol before, is about 45 minutes.
Treatments
• Autogenic Drainage is a breathing technique which involves 3 phases of breathing levels:
• Phase One is the unsticking phase which is inhalation and exhalation of small amounts of air.
• Phase Two is the collection phase where medium sized breaths are inhaled and exhaled.
• Phase Three is the evacuation phase where large amounts of air are inhaled and exhaled.
Treatments
• Hand Held Nebulizers are used in
conjunction with PEP, IPV, CPT and
breathing techniques
• The nebulizer will nebulize medications
that bronchodilate and help break up
mucus
• Antibiotics can also be used in a
nebulizer
Medications Used
• Antibiotics: Tobramycin and Azithromycin to fight
bacterial infection. Given by aerosol in nebulizer
or by IV
• Anti-Inflammatory Drugs: Steroids given inhaled
or by IV; also Ibuprofen is given
• Bronchodilators: Albuterol/Xopenex given to
relax smooth muscle
• Mucolytics: Given with bronchodilators to break
up thick secretions. Main one is Dornase Alfa
(Pulmozyne) made specifically for CF patients

More Treatments
• Oxygen Therapy at low concentrations.
• Lung Transplantation; depends on severity of illness and health of participate
• Nutritional therapy; oral pancreatic enzymes to digest fats and proteins and absorb vitamins.
• Vitamin supplements of A, D, E and K
• Feeding tube at night (G-Tube)
• Enemas and stomach meds to control acid

Conclusion
• CF is a deadly hereditary disease that is treatable but not curable
• CF causes abnormally thick mucus which blocks bile ducts and plugs up the lung and sinus
• May lead to respiratory failure, malnutrition and frequent occurrences of pneumonia
• Treatment includes methods to remove and thin mucus and medications to treat digestive problems, and infections

Chronic Bronchitis
Chronic Bronchitis
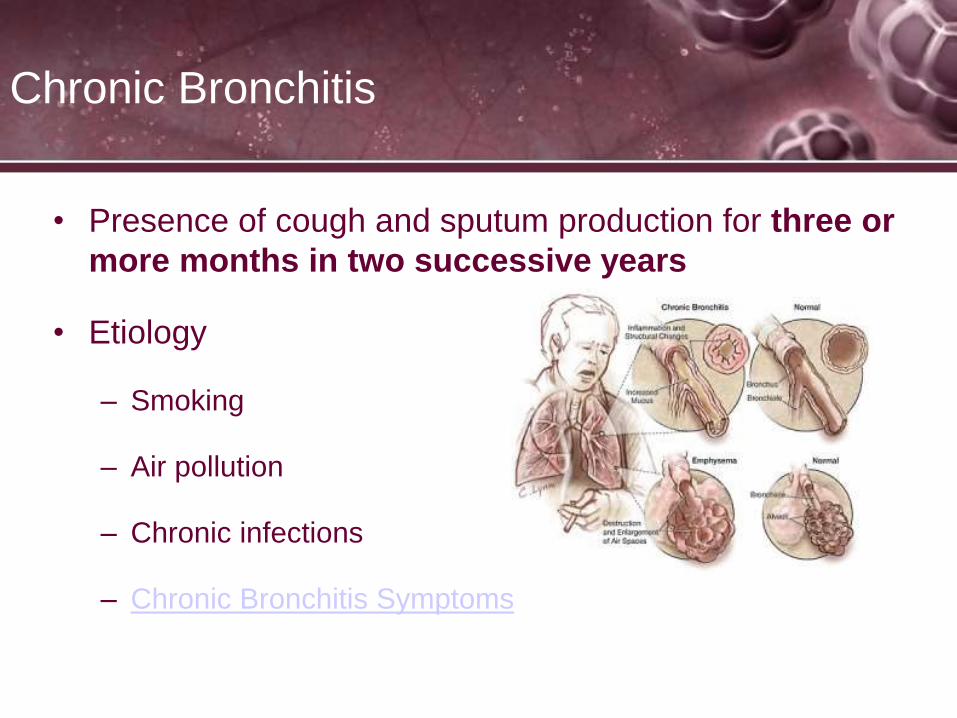
• Presence of cough and sputum production for three or
more months in two successive years
• Etiology
– Smoking
– Air pollution
– Chronic infections
– Chronic Bronchitis Symptoms
Chronic Bronchitis
• 14 million Americans are affected
• Most common causes are smoking/pollution
• Repeated lung infections, especially in childhood increase
risk
• Common pathogens include Haemophilus influenzae and
Streptococcus pneumoniae
• Gastroesophageal reflux disease (GERD) can lead to
pneumonias from aspiration of stomach contents

Chronic Bronchitis – Pathophysiology
• Most changes in the lungs occur in the conducting
airways
• Airway changes occur from:
– Chronic inflammation and swelling
– Excessive mucus production and accumulation
– Partial or total mucus plugging
– Hyperinflation of alveoli
– Smooth muscle constriction of airways

Chronic Bronchitis – Pathophysiology
• Changes in mucus glands
– Increase in number of mucus secreting glands; goblet
cells increase, causing decrease in ciliated columnar
cells; submucosal glands hypertrophy
• Smooth muscle hypertrophy in bronchial airways
• Diminished airway radius
Chronic Bronchitis – Pathophysiology
• Increase in sputum production
• Accumulation of secretions
• Loss of ciliated cells
• Impairment of mucociliary escalator
• Decreased flow rates, VC, FVC, FEV1, MVV
• Increased RV, FRC, TLC

Chronic Bronchitis
Radiologic Findings
1.Hyperinflation of the Lungs
2.Flattened Hemidiaphram
3.Peripheral Pulmonary
Vasculature may be Prominent
4.Pulmonary Vascular
Engorgement
5.Long and narrow heart (pulled
down by the diaphragms)
6.Enlarged heart

Chronic Bronchitis

Chronic Bronchitis – Clinical Findings
• Typical appearance is of the “Blue Bloater”
– Stocky build
– Cyanotic
– Increased A-P diameter
– Jugular vein distension
– Edema

Chronic Bronchitis – Clinical Findings
• Cough
– Smoker’s cough
– Morning cough
– Continual cough
• Sputum production
– Volume increases slowly leading to abnormal production but
typically less than a cup/day
– Thick, gray, mucoid in nature
– Mucopurulent infections leading to yellow or green sputum
Chronic Bronchitis – Clinical Findings
• Increase in respiratory rate
– Stimulation of peripheral chemoreceptors secondary to hypoxemia
and chronic CO2 retention
– Decrease in lung compliance
– Anxiety
• Increase in heart rate
• Dyspnea, especially on exertion
• Use of accessory muscles
• BS: rhonchi, crackles, wheezing and decreased BS
• Breath Sounds

Chronic Bronchitis – Clinical Findings
• Pursed lip breathing
• Increase in A-P diameter of the chest (barrel chest)
secondary to hyperinflation
• Clubbing
• Increased sputum production
• ABG results
– Fully compensated pH unless in an acute exacerbation
– Increase in PaCO2
– Decrease in PaO2
CXR Interpretation for COPD
• Chest x-ray interpretation --COPD and Emphysema

Pink Puffer Vs. Blue Bloater
• A "pink puffer" is a person where emphysema is the
primary underlying pathology. As you recall,
emphysema results from destruction of the airways
distal to the terminal bronchiole--which also includes the
gradual destruction of the pulmonary capillary bed and
thus decreased inability to oxygenate the blood. So, not
only is there less surface area for gas exchange, there
is also less vascular bed for gas exchange--but less
ventilation-perfusion mismatch than blue bloaters. The
body then has to compensate by hyperventilation (the
"puffer" part).
Pink Puffer Vs. Blue Bloater
• Pink Puffers: Their arterial blood gases (ABGs) actually
are relatively normal because of this compensatory
hyperventilation. Eventually, because of the low cardiac
output, people afflicted with this disease develop muscle
wasting and weight loss. They actually have less
hypoxemia (compared to blue bloaters) and appear to
have a "pink" complexion and hence "pink
puffer". Some of the pink appearance may also be due
to the work (use of neck and chest muscles) these folks
put into just drawing a breath.
Pink Puffer Vs. Blue Bloater
• A "blue bloater" is a person where the primary
underlying lung pathology is chronic bronchitis. Just a
reminder, chronic bronchitis is caused by excessive
mucus production with airway obstruction resulting from
hyperplasia of mucus-producing glands, goblet cell
metaplasia, and chronic inflammation around
bronchi. Unlike emphysema, the pulmonary capillary
bed is undamaged. Instead, the body responds to the
increased obstruction by decreasing ventilation and
increasing cardiac output.
Pink Puffer Vs. Blue Bloater
• There is a dreadful ventilation to perfusion mismatch
leading to hypoxemia and polycythemia. In addition,
they also have increased carbon dioxide retention
(hypercapnia). Because of increasing obstruction, their
residual lung volume gradually increases (the "bloating"
part). They are hypoxemic/cyanotic because they
actually have worse hypoxemia than pink puffers and
this manifests as bluish lips and faces--the "blue" part.

Pink Puffer Vs. Blue Bloater

Asthma
• A disease of the airway “characterized by an
increased responsiveness of the trachea and
bronchi to various stimuli and is manifested by
widespread narrowing of the airways that change
in severity either spontaneously or as a result of
treatment” (ATS)
Asthma
• Airway constriction may be partially or completely
reversible either spontaneously or with treatment
• Affects more than 15 million Americans
• Recognized more than 2000 years ago
• More than 5,000 die per year - Teen dies of asthma
• The most common chronic illness of childhood
• May develop in adulthood with increased mortality
• May disappear at puberty

Asthma
• Allergic or Extrinsic Asthma
– Results from an antigen-antibody reaction on mast cells
causing a release of histamine, bradykinins, and other
chemicals
• Idiopathic or Intrinsic Asthma
– Cannot be linked to a specific antigen
– Results from an imbalance of the autonomic nervous system
• Non-specific Asthma
– Results from an unknown cause, possibly viral, emotional, or
exercise

Asthma
• From your text page 189:
• Occupational Sensitizers (box 12-1)
• Seen predominantly in adults, more than 300
substances contribute to it.
• Sensitive work environments include:
– Farming
– Agricultural
– Painting
– Cleaning work
– Plastic manufacturing

Immunologic Mechanism (from your
text, page 188)
• When exposed to specific antigens, lymphoid tissue
forms specific IgE antibodies
• The IgE antibodies attach themselves to surface of
mast cells in the bronchial wall
• Re-exposure to the same antigen creates antigen-
antibody reaction on the surface of the mast cell,
causes mast cell to degranulate and release chemical
mediators:
– Histamine
– Eosinophil/neutrophil chemotactic factors
– Leukotrienes
– Prostglandins and platelet activating factor
– Allergies

Mast Cell Degranulation
Exposed to antigen, form
antibodies, attach to mast cells
Re-exposure to antigen causes
the degranulation of mast cell
and release of inflammatory
cells

Mast Cell Degranulation
Following an Asthma attack; the patient will have congestion and increased sputum production for several days

Inflammatory cell release (page 189)
• Release of chemical mediators from mast cell stimulates
parasympathetic nerve endings in the bronchial airways
leading to reflex bronchoconstriction and mucous hyper-
secretion
• The mediators also increase permeability of capillaries
causing dilation of blood vessels and tissue edema
Early vs. late response (after steroids and bronchodilators
have worn off)
Mast Cell inhibitors for asthma
treatment
• Cromolyn sodium (Intal) and nedocromil (Tilade) are used to prevent
allergic symptoms like runny nose, itchy eyes, and asthma. The response is
not as potent as that of corticosteroid inhalers.
How mast cell inhibitors work
• These drugs prevent the release of histamine and other chemicals from mast
cells that cause asthma symptoms when you come into contact with an
allergen (for example, pollen). The drug is not effective until four to seven
days after you begin taking it.
Who should Use it
• Patients with extrinsic asthma, with known allergies
• Frequent dosing is necessary, since the effects last only six to eight hours.
Mast cell inhibitors are available as a liquid to be used with a nebulizer, a
capsule that is placed in a device that releases the capsule powder to inhale,
and handheld inhalers

Intal and Tilade
Both drugs are used only for prophylaxis of asthma, not for
treatment of the acute exacerbation or for the symptomatic
patient

Anti- Leukotriens
• Do not prevent mast cell degranulation, as do Intal and
Tilade
• They stop the inflammatory mediators once the mast
cells is degranulated
• Leukotrienes are proinflammatory mediators with
special significance in asthma. Released by numerous
cell types, particularly after exposure to allergens,
leukotrienes cause a potent contraction of bronchial
smooth muscle, resulting in reduced airway caliber.
Further, they cause plasma to leak from the vessels,
resulting in edema, and enhance the secretion of mucus

Anti-leukotriene drugs
• ORAL ONLY. First drug of this type (Nov 1996) is the
leukotriene-receptor antagonist Zafirlukast [Accolate],
20 mg bid. The 2nd approved anti-leukotriene (Jan 1997)
is the leukotriene-synthesis inhibitor Zileuton [Zyflo],
with a 600 mg QID dosage schedule. Both are approved
only for asthma, and for patients 12 years or older. The
3rd approved anti-leukotriene, Montelukast (Singulair),
10 mg qd, is also approved for ages 6-14 in a 5 mg QD
dose. All anti-leukotrienes have some bronchodilator as
well as anti-inflammatory activity.
Asthma
• Etiology
– Heredity – one or more parents with disease
– Allergies, especially if onset between ages five and fifteen
– Inhaled irritants
• Pollen
• Dust mites
• Grasses
• Pollution
• Animal dander
• Chemicals

The Role of Heredity in
Asthma
• Heredity. To some extent, asthma seems to run in families. People whose brothers, sisters or parents have asthma are more likely to develop the illness themselves.
• Atopy. A person is said to have atopy (or to be atopic) when he or she is prone to have allergies. For reasons that are not fully known, some people seem to inherit a tendency to develop allergies. This is not to say that a parent can pass on a specific type of allergy to a child. In other words, it doesn't mean that if your mother is allergic to bananas, you will be too. But you may develop allergies to something else, like pollen or mold.
• In addition, several factors must be present for asthma symptoms to develop:
• Specific genes must be acquired from parents.
• Exposure to allergens or triggers to which you have a genetically programmed response.
• Environmental factors such as quality of air, exposure to irritants, behavioral factors such as smoking, etc.

Asthma Risk Factors (page 190)
• Obesity: Certain mediators such as leptins may have an
effect on airway function that can lead to development of
asthma
• Gender: Males up to 14, have a higher prevalence, due to
possible lung size of boys vs. girls, after 14, girls have a
higher prevalence
• Infections: upper viral infections and bacterial infections
contribute to asthma. Commonly seen in children after
RSV, parainfluenza, rhinovirus.
• Exercise induced: heat loss, water loss, increased
osmolority increase inflammatory release
Asthma Risk Factors (page 190)
• Outdoor/indoor air pollution: increases in asthma
incidences occur in heavily polluted areas. Smoke, gas
fumes, biomass fuels for heating, molds and cockroach
droppings contribute to asthma
• Drugs/foods/preservatives: Aspirin sensitivity, and other
non-steroidals (NSAIDS), beta-blocking agents to treat
hypertension and tachycardia, tartazine (food coloring),
and preservatives for restaurant food
• GERD: regurgitation and aspiration, may lead to asthma
or exacerbate it

Asthma Risk Factors (page 190)
• Emotional Distress: psychological factors can induce
tachypnea and stress the lung contributing to asthma
exacerbation
• Perimenstrual asthma: symptoms worsen 2-3 days
before menstruation
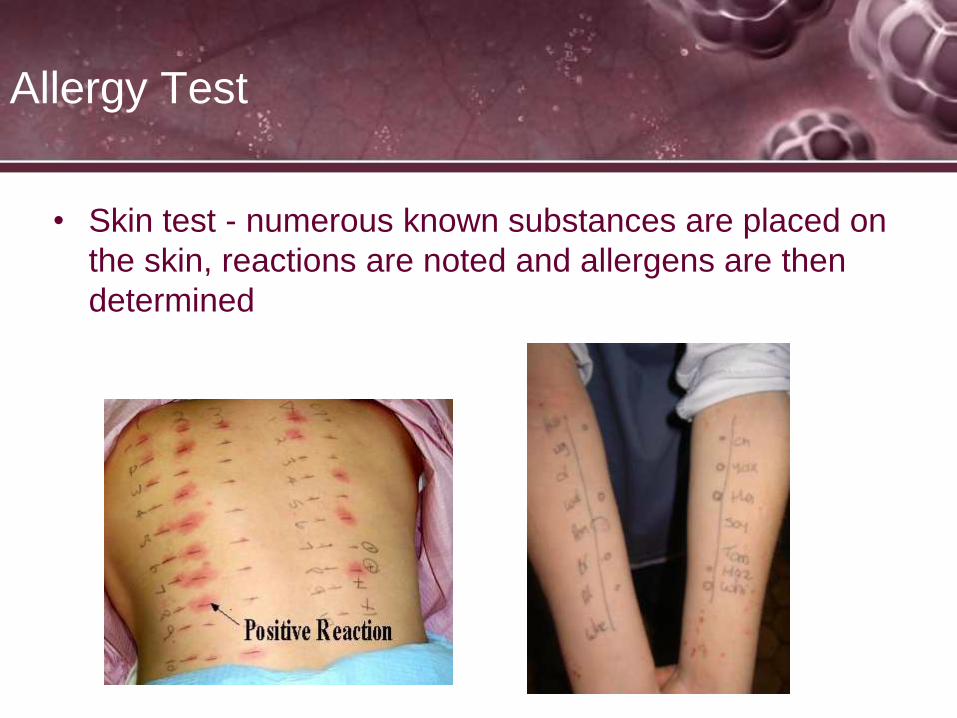
Allergy Test
• Skin test - numerous known substances are placed on
the skin, reactions are noted and allergens are then
determined
Allergy Test
• Besides the skin allergy test they also do blood tests.
The RAST test measures the levels of the allergy
antibody IgE that is produced when your blood is mixed
with a series of allergens
• in a laboratory.

Causes
• Substances that cause allergies (allergens) such as dust
mites, pollens, molds, pet dander, and even cockroach droppings. In
many people with asthma, the same substances that cause allergy
symptoms can also trigger an asthma episode. These allergens may
be things that you inhale, such as pollen or dust, or things that you
eat, such as shellfish. It is best to avoid or limit your exposure to
known allergens in order to prevent asthma symptoms.
• Irritants in the air, including smoke from cigarettes, wood fires, or
charcoal grills. Also, strong fumes or odors like household sprays,
paint, gasoline, perfumes, and scented soaps. Although people are
not actually allergic to these particles, they can aggravate inflamed,
sensitive airways. Today most people are aware that smoking can
lead to cancer and heart disease. Smoking is also a risk factor for
asthma in children, and a common trigger of asthma symptoms for all
ages

Causes
• Respiratory infections such as colds, flu, sore throats, and sinus infections. These are the number one asthma trigger in children
• GERD: Gastric esophageal reflux disease, stomach acid can be aspirated and inflame the airway
• Exercise and other activities that make you breathe harder. Exercise—especially in cold air—is a frequent asthma trigger. A form of asthma called exercise-induced asthma is triggered by physical activity. Symptoms of this kind of asthma may not appear until after several minutes of sustained exercise. (When symptoms appear sooner than this, it usually means that the person needs to adjust his or her treatment.) The kind of physical activities that can bring on asthma symptoms include not only exercise, but also laughing, crying, holding one's breath, and hyperventilating (rapid, shallow breathing). The symptoms of exercise-induced asthma usually go away within a few hours
Exercise Induced Asthma Attack

More Causes…
• Weather such as dry wind, cold air, or sudden changes in weather can sometimes bring on an asthma episode.
• Expressing strong emotions like anger, fear or excitement. When you experience strong emotions, your breathing changes -- even if you don’t have asthma. When a person with asthma laughs, yells, or cries hard, natural airway changes may cause wheezing or other asthma symptoms.
• Some medications like aspirin can also be related to episodes in adults who are sensitive to aspirin. Irritants in the environment can also bring on an asthma episode. These irritants may include paint fumes, smog, aerosol sprays and even perfume.

Why Does My Asthma Act Up at
Night?
• For reasons we don't fully understand, uncontrolled asthma -- with its underlying inflammation -- often acts up at night. It probably has to do with natural body rhythms and changes in your body’s hormones, as well as the fact that some symptoms appear hours after you come in contact with a trigger.
• Also during sleep you release less norepinephrine (adrenaline) which acts as your bodies natural bronchodilator
• A Tragic Asthma Attack Story

Asthma – Pathophysiology
• Airway Inflammation
– Acute Phase Response – triggered by activation of mast
cells and the release of intracellular mediators
• Bronchospasm
• Increase in secretions
• Mucosal edema
• Significant reduction in airflow

Asthma – Pathophysiology
• Airway Inflammation
– Subacute phase
• Continuous inflammatory pattern
• Significant airflow limitation
• Can continue for days to weeks

Asthma – Pathophysiology
• Airway Inflammation
– Chronic inflammation
• Present between episodes of exacerbation
• Controlled by corticosteroids, mast cell modifiers, or
leukotriene modifiers

Asthma – Pathophysiology
• Airway Hyperresponsiveness
– Usually most evident in acute phase
– Increased sensitivity to both specific and non-specific
causes
– Release of immunoglobulin E (IgE) mediators into the
cellular tissue causing bronchoconstriciton of the smooth
muscle of the airway, degranulation of mast cells releasing
histamines, leukotrienes, certain interleukins, prostaglandins
and others
– Treated with beta2 agonists
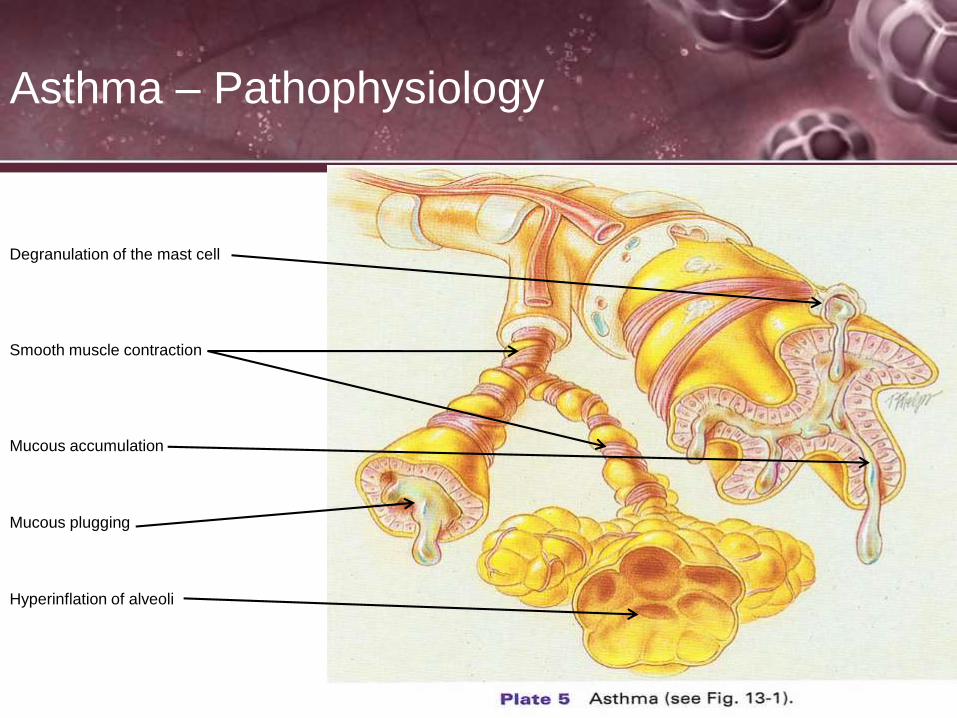
Asthma – Pathophysiology
Degranulation of the mast cell
Smooth muscle contraction
Mucous accumulation
Mucous plugging
Hyperinflation of alveoli
Asthma – Classification
• Classifications of Asthma
– Mild intermittent asthma
• Symptoms < 2/week or < 2 times/month at night
• Little effect on day to day activities
• Expiratory flow ≥ 80% of predicted

Asthma – Classification
• Classifications of Asthma
– Mild Persistent Asthma
• Symptoms > 2/week but less than 1/day; < 2
times/month at night
• Exacerbations may affect activity
• Expiratory flow ≥ 80% of predicted
Asthma – Classification
• Classifications of Asthma
– Moderate persistent asthma
• Symptoms daily; > 1/week at night
• Limitations ≥ 2/week; may last days
• Expiratory flow > 60% but < 80% of predicted

Asthma – Classification
• Classifications of Asthma
– Severe persistent asthma
• Symptoms continually with frequent symptoms at night
• Frequent exacerbations which limit activity
• Expiratory flow < 60% of predicted

Asthma – Pulmonary Function
Results
• May have normal results when asymptomatic
• Airway obstruction
– Decrease in FEV1
– Decrease in FEV1/FVC ratio
– Demonstrate reversibility of obstruction following
bronchodilator administration (↑ in FEV1 of at least 12% and
an increase in VC of 200mL or more)
– Decrease in expiratory flow rates: peak flows are used to
monitor asthmatic events in the home.

Asthma – Pulmonary Function
Results
• Bronchoprovocation Testing
– Administration of Methacholine
– Causes decrease in FEV1 by 20% or more in
hyperresponsive airways
• Diagnostic test used in the evaluation of suspected asthma. The methacholine
challenge is also used for research purposes to study airway hyperreactivity.
Under special circumstances it plays a role in the clinical arena. Cold-air
exercise tests are another example of a bronchoprovocation test.
• A bronchoprovocation test might be ordered in the evaluation of suspected
asthma. It is not considered a “routine” test. Usually, the patient describes
subtle symptoms suggestive of asthma. Spirometry and other pulmonary
function testing are entirely normal.

Methacholine
• Methacholine (Provocholine) is a synthetic choline
ester that acts as a non-selective muscarinic receptor
agonist in the parasympathetic nervous system
Using a Peak Flow
• A Peak Flow device is a assessment tool used to
measure the effectiveness of fast acting
bronchodilators.
• Given during the attack, before and after treatments
• It is a handheld device that the patient exhales forcibly
on; as the airway opens and improves, the value
increases

Asthma Action Plan

Asthma – Clinical Findings

Asthma – Clinical Findings
• Auscultation – episodic wheezing
– Absence of wheezing does not preclude asthma
– Not all wheezing is asthma
– Breath sounds may get worse but patient could be improving
• Shortness of breath
• Tachypnea
• Tachycardia
• Use of accessory muscles
• Pursed-lip breathing
• Anxiety
• Hypoxia
• Altered LOC
• Full Arrest
• BS – wheezes, crackles, rhonchi, decreased BS

Asthma – Clinical Findings
• Blood Gas Results
– In mild to moderate episode:
pH PCO2 HCO3 slightly PaO2
– In moderate to severe episode:
• pH PCO2 HCO3 slightly PaO2

Status Asthmaticus
• A severe asthma attack not responsive to bronchodilators
• Typically requires intubation and mechanical ventilation due to
respiratory failure
• Typically, patients present a few days after the onset of a viral
respiratory illness, following exposure to a potent allergen or irritant, or
after exercise in a cold environment. Frequently, patients have
underused or have been under prescribed anti-inflammatory therapy.
Illicit drug use may play a role in poor adherence to anti-inflammatory
therapy. Patients report chest tightness, rapidly progressive shortness
of breath, dry cough, and wheezing and may have increased their
beta-agonist intake (either inhaled or nebulized) to as often as every
few minutes.
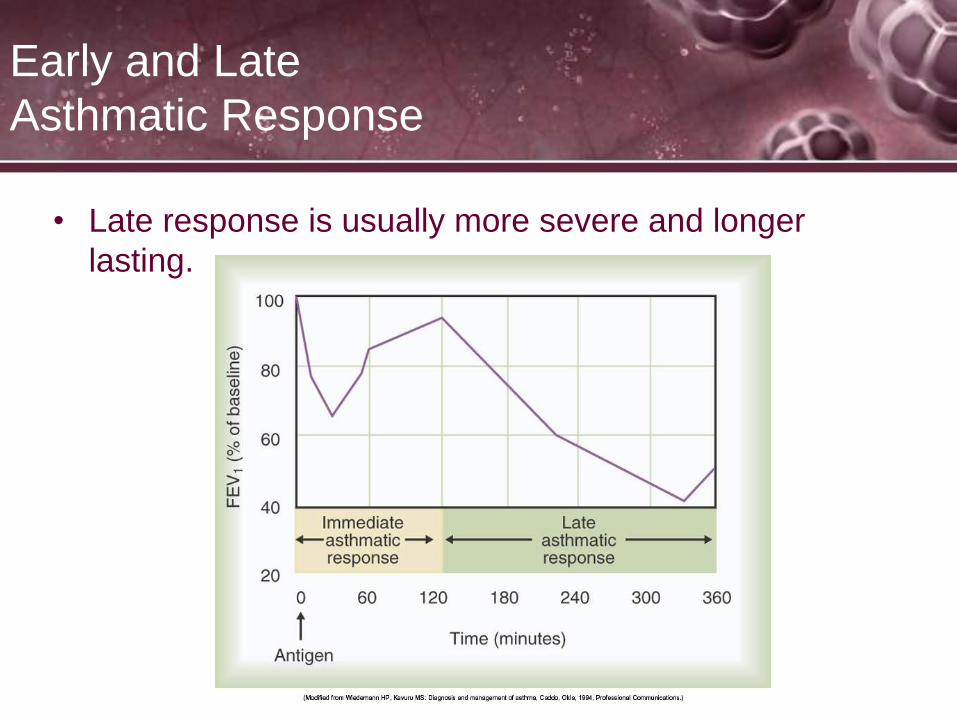
Early and Late
Asthmatic Response
• Late response is usually more severe and longer
lasting.
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
158
Pharmacotherapy
Corticosteroids
– Most effective mediation in treatment of asthma
• Reduces symptoms and mortality
– Use of inhaled steroids for long-term treatment preferred
• Use spacer and rinse mouth to eliminate or minimize
side effects
– Long-term use of oral steroids should be restricted to
patients with asthma refractory to other treatment.
– Short-term oral steroid use during exacerbation reduces
severity, duration, and mortality.

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
159
Pharmacotherapy
Inhaled Corticosteroids (page 194)
• Beclomethasone (QVAR); 40 or 80 ug/puff BID
• Flunisolide (Aerobid); 250 ug/puff; BID
• Fluticosone (Flovent); 44, 110, or 220 ug/puff, BID
• Budesonide (Pulmicort); SVN 0.25 or 0.5 mg, BID
• Momestone furoate (Asmanex twisthaler) DPI 220 ug QD
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
160
Pharmacotherapy
Systemic Steroids Corticosteroids (page 194)
• Prednisone (short term use following an acute attack)
usually 3-5 days, BID
• Methylpredinsone (Solu-Medrol); Typically an IV potent
systemic steroid, given during and after acute attacks

HHN Delivery
• Delivery of the a small volume nebulizer takes practice
and in fact the way the medication is delivered to a
patient can dictate the hazards. Below is a link of the
proper way to give a nebulizer treatment, granted it is
from another RT program, I think it shows the proper
components of neb delivery
You Tube- Neb Delivery
MDI Delivery
• Delivering an MDI to a patient takes some practice.
Below are three videos, one for an MDI using a closed
mouth technique, one showing an open mouth
technique and one showing an MDI with a holding
chamber (Aerochamber). You should encourage MDI
use with a holding chamber
1. You Tube- closed mouth
2. You Tube- open mouth
3. You Tube- holding chamber

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
163
Pharmacotherapy (cont.)
Cromolyn (NSAID) non-steroidal anti-inflammatory drug
– Protective against allergens, cold air, exercise
– Administered prophylactically, CANNOT be used during an
acute asthma attack
– Of limited use in adults
– Drug of choice for atopic children with asthma
Nedocromil (NSAID)
– Similar to Cromolyn, it is 4–10 times more potent in
preventing acute allergic bronchospasm.

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
164
Pharmacotherapy (cont.)
DOSAGES AND FREQUENCIES:
Cromolyn (NSAID)
• SVN 20 mg QID
• MDI 2 puffs 800 ug QID
Nedocromil (NSAID)
– Similar to Cromolyn, it is 4–10 times more potent in
preventing acute allergic bronchospasm.
– MDI only, 2 puffs 1.75 mg/puff QID
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
165
Pharmacotherapy (cont.)
Leukotriene inhibitors
– Leukotrienes mediate inflammation and bronchospasms.
– Modestly effective to control mild to moderate asthma
– Accolate, Singular, Zyflo
Inhaled steroids remain the anti-inflammatory drug of
choice for the treatment of asthma.
Methyxanthines (use is controversial)– Oral or IV use if admitted for acute asthma attack
– Theophylline

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
166
Pharmacotherapy (cont.)
2-Adrenergic agonists Short Acting
– Most rapid and effective bronchodilator
– Drug of choice for exercise-induced asthma and emergency
relief of bronchospasms
• Should be used PRN
– Improves symptoms not underlying inflammation
• Regular use may worsen asthma control and increase
risk of death.
• Albuterol (Proventil, Ventolin); SVN UD 0.5% Soln, or 2.5
mg (0.5 ml) give TID, QID, Q4, Q6 or PRN
• Levalbuterol (Xopenex), SVN 0.31, 0.63, or 1.25 mg
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
167
Pharmacotherapy (cont.)
2-Adrenergic agonists Short Acting
Albuterol MDI = Pro Air/ Ventolin 90 ug: 2 puffs TID/QID
Xopenex MDI = Xopenex HFA 45 ug/puff x 2 puffs Q4-6
Combivent: MDI of Albuterol and Atrovent
DuoNeb: SVN of Albuterol and Atrovent

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
168
Pharmacotherapy (cont.)
2-Adrenergic agonists Ultra Short Acting
• Epinephrine (Epinephrine Mist, Primatene mist): SVN
1% soln (1:100), 0.25-0.5 ml QID; MDI 0.22 mg/puff
• Racemic Epinephrine; (Micronephrine, Nephrone); SVN
2.25% soln, 0.25-0.5 ml QID
Last about 90 minutes, Racemic has a strong Beta and
Alpha response, used for upper airway swelling

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
169
Pharmacotherapy (cont.)
2-Adrenergic agonists Long Acting and Combination
drugs
Salmeterol (Serevent); DPI 50 ug/inhalation; 50 ug BID
Formoterol (Foradil) DPI, 12 ug, BID
Arformoterol (Brovona) SVN 15 ug/2ml, BID (some fast
acting response)

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
170
Pharmacotherapy (cont.)
2-Adrenergic agonists Long Acting and Combination
drugs
Advair (fluticosone and Serevent); DPI; 3 doses; 500/50,
250/50 and 100/50; the fluctuating dose is the steroid
Also comes in a MDI
Symbicort (Pulmicort and Foradil); MDI 80 and 160 ug
• DULERA mometasone furoate and a long acting
beta2-agonist medicine (LABA) called formoterol
fumarate
Arcapta (indacaterol maleate inhalation powder)

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
171
Pharmacotherapy (cont.)
Anticholinergics– Can be used as adjunct to first-line bronchodilators if there is an
inadequate response
– Has an additive affect to 2-agonists
– Blocks musacarenic receptors (Acetycholine)
– Ipatropium Bromide (Atrovent); SVN 0.5 mg, 0.02% solution
– MDI 18 ug/puff; dose TID, Q6
– Tiotropium (Spiriva), used through a handi-haler, QD
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
172
Asthma and Environmental Control
• Recognized relationship between asthma and allergy
– 75–85% asthma patients react to inhaled allergens
• Environmental control is aimed at reducing exposure to allergens.
– Avoid outdoor allergens by remaining inside, windows closed, AC on
– Indoor allergens are combated by
• Air purifiers and no pets
• Dust mites: airtight covers on bed and pillow, no carpets in bedroom, chemical agents to kill mites

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
173
Special Considerations in Asthma
Management (cont.)
• Nocturnal asthma
– Present in two-thirds of poorly controlled asthmatics
– May be due to diurnal decrease in airway tone or gastric reflux
– Treatment should include:
• Steroid treatment targeted to relieve night symptoms
• Sustained release theophylline
• New long-acting 2-agonists
• Antacids for reflux
Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
174
Special Considerations in Asthma
Management (cont.)
• Aspirin sensitivity
– 5% of adult asthmatics will have severe, life-threatening asthma
attacks after taking NSAIDs.
– All asthmatics should avoid; suggest Tylenol use.
• Asthma during pregnancy
– A third of asthmatics have worse control at this time.
– Much higher fetal risk associated with uncontrolled asthma than
that of asthma medications
– Theophyllines, 2-agonists, and steroids can be used without
significant risk of fetal abnormalities.

Mosby items and derived items ©
2009 by Mosby, Inc., an affiliate of
Elsevier Inc.
175
Special Considerations in Asthma
Management (cont.)
• Sinusitis may cause asthma exacerbation.– CT of sinuses will diagnosis problem.
– Treat: 2–3 weeks antibiotics, nasal decongestants, and nasal
inhaled steroids
• Surgery– Asthmatics at higher risk for respiratory complications
• Arrest during induction
• Hypoxemia with/without hypercarbia
• Impaired cough, atelectasis, pneumonia
– Optimize lung function preoperatively.
– Use steroids during procedure.
Review
• Emphysema:
– Low expiratory flows (FVC, FEV1 less than 80%), FEV1/FVC less
than 70%
– Decreased DLCO
– Increased Lung Volumes
– Main cause smoking, also caused by genetic alpha anti-trypson
disorder, environmental
– Chronic hypercapnia, hypoxemia, barrel chest, clubbing of fingers,
hyperinflated lungs on CXR (hyperlucent with flattened
diaphragms), accessory muscle use, SOB at rest...
– Damage occurs primarily in upper lobes
– Persistent irritants overwhelm lungs natural macrophage and
neutrophil removal, causing loss of elastin creating bullae
Review
• Emphysema:
– Treatments include breathing exercises, diaphragmatic
breathing, pursed lip breathing; low supplemental oxygen
less than 30% to avoid knocking out hypoxic drive;
bronchodilators, and steroids. Bronchial hygiene, Possible
lung transplant, smoking cessation
– Increased pressure in alveoli causes: decreased VA,
increased VD/VT, decreased in PaO2, PAO2, CaO2, SaO2,
increase in A-a gradient, CO2, Hb
– Get frequent pneumonia, bronchitis…

Review
• Cystic Fibrosis
– Heredity based
– Disease of tenacious mucus, blocks bile ducts, lungs and
sinuses.

Bronchiectasis
Bronchiectasis
An Amazing Story

Bronchiectasis
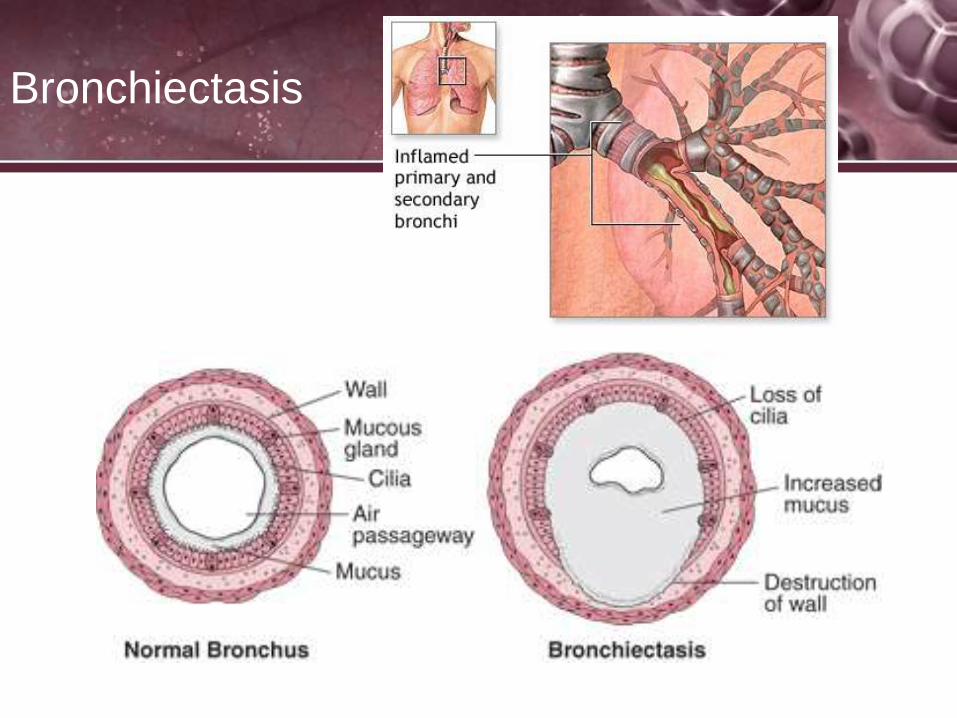
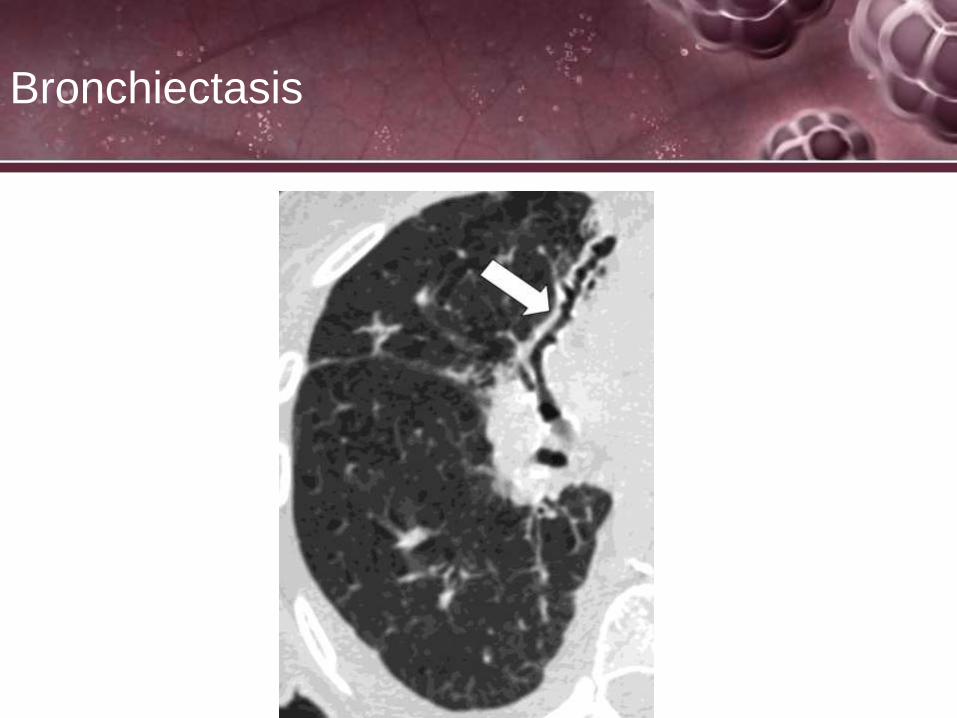
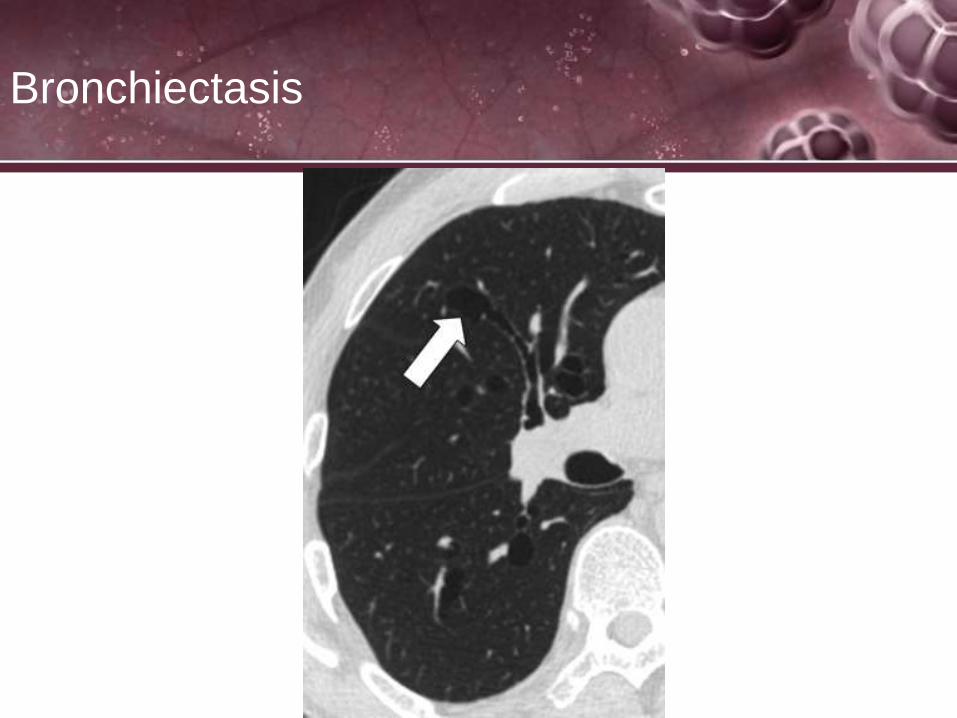
• Bronchiectasis is characterized by chronic dilation and
distortion of one or more bronchi as a result of extensive
inflammation and destruction of the bronchial wall
cartilage, blood vessels, elastic tissue, and smooth
muscle components
• Can affect one or both lungs
• Commonly limited to a lobe or segment
• Most frequently found in the lower lobes
• The smaller bronchi, with less supporting cartilage are
predominantly affected
Bronchiectasis

Bronchiectasis
• Three forms or anatomic varieties of bronchiectasis
have been described:
– Varicose or fusiform
– Cylindrical or tubular
– Saccular or cystic

Bronchiectasis
• Etiology
– Not as common today because of increased use of antibiotics
for lower respiratory infections
– May be acquired or congenital but not thoroughly understood
– Acquired bronchiectasis is thought to occur by repeated and
prolonged respiratory infections, bronchial obstruction from a
foreign body, tumor or enlarged hilar lymph nodes
– People with cystic fibrosis have a much higher incidence of
bronchiectasis due to the chronic airway obstruction

Bronchiectasis
• Etiology
– Congenital Bronchiectasis
• Kartagener’s Syndrome responsible for 20% of all
bronchiectasis. Consists of a triad of Bronchiectasis,
dextracardia (heart on right side of chest), and
pansinusitus
• Hypogammaglobulinemia: An inherited immune deficiency
disorder that leaves the lung vulnerable to infection

Bronchiectasis
• Fusiform or Varicose
– Bronchial walls are dilated and constricted in an irregular
fashion similar to varicose veins ultimately ending in a
distorted bulbous shape ending in nonfunctional respiratory
units
– Evidence of bronchitis or bronchiolitis often present
Bronchiectasis
Bronchiectasis
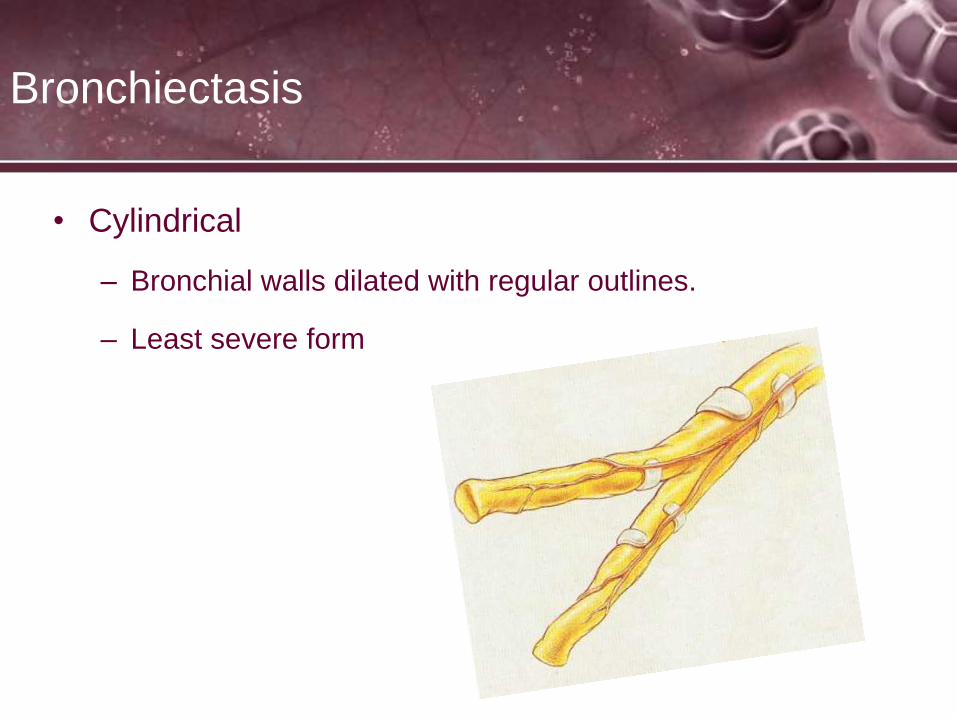
• Cylindrical
– Bronchial walls dilated with regular outlines.
– Least severe form

Bronchiectasis

Bronchiectasis
• Saccular
– Complete destruction of bronchial walls
– Normal tissue replaced by fibrous tissue
– Most severe form with poorest prognosis
Bronchiectasis

Bronchiectasis
• Pathophysiology
– Loss of ciliated epithelium and respiratory units
– Chronic inflammation
– Sloughing of mucosa with ulceration and possible abscess formation
– Reduced volume of distal lung and adjacent lung secondary to scarring
and bronchial obstruction
– Excessive production of sputum (greater than 1 cup/day)
– Sputum is foul-smelling and hemoptysis is common
– Hyperinflation of alveoli
– Atelectasis, consolidation and parenchymal fibrosis
Bronchiectasis
• Radiologic Findings
– Bronchograms have been largely replaced by thin slice CT
imagery
– May show multiple cysts
– May show cor pulmonale
Bronchiectasis

Bronchiectasis
• PFT Findings
– FVC , FEV1 , FLOWS , VC , FRC , TLC
Bronchiectasis is obstructive in nature when in a non acute
phase
When in an acute phase, can be restrictive due to
bronchial filling and subsequent alveolar atelectasis and
collapse
Bronchiectasis – Clinical Findings
• Chronic loose cough exacerbated by change of position
• Recurrent infections
• Increased sputum production: tri-layer sputum
– Top layer – thin, frothy
– Middle layer – mucopurulent
– Bottom layer – opaque, mucopurulent or purulent with
mucus plugs, foul-smelling
Bronchiectasis – Clinical Findings
• Halitosis (bad
breath)
• Hemoptysis
• Severe V/Q
abnormalities
• Clubbing
• BS- rhonchi,
crackles,
diminished

Bronchiolitis
• Also called pneumonitis
• Caused primarily by the respiratory syncytial virus
(RSV)
• RSV is the most common viral respiratory pathogen
seen in infancy and early childhood but can be acquired
at any age
• Outbreaks are usually seasonal in fall and winter
• Most children under 6 months of age require
hospitalization.
• Spread by aerosol/droplets from coughs and sneezes
• Bronchiolitis Boy
• Baby with Bronchiolitis and seconday complications

Old Treatment for RSV- Ribavirin
• Ribavirin (Virazole) is an anti-viral drug indicated for
severe RSV infection. Ribavirin is active against a
number of DNA and RNA viruses. It is a member of the
nucleoside antimetabolite drugs that interfere with
duplication of viral genetic material. Ribavirin is active
against influenzas, flaviviruses and agents of many viral
hemorrhagic fevers.
• Side effects:
– Teratogenic effects
– Anemia
RSV - what is it?
RSV preventions

Bronchiolitis
• Pathophysiology –
– Inflammation and swelling of the peripheral airways
– Excessive airway and nasal secretions
– Sloughing of necrotic airway epithelium
– Partial airway obstruction and alveolar hyperinflation
– Complete airway obstruction and atelectasis
– Consolidation

Bronchiolitis
• Diagnosis made by:
– Obtaining a nasal swab or
nasopharyngeal aspirate
– Immunofluorescense staining
– Results available within 2-6
hours
– X-ray results show streaky
peribronchial opacities
associated with air trapping,
hyperinflation, and lobar
pneumonic consolidation
Bronchiolitis
• Clinical Manifestations
– Excessive nasal, oral and bronchial secretions
– BS: wheezes, crackles, rhonchi, expiratory grunting
– Increased RR, HR, BP, CO
– Apnea
– Intercostal/Substernal retractions
– Cyanosis
– Nasal flaring
Pulmonary Infections
Pulmonary Infections
• Infections occur more frequently in the respiratory tract
than in any other organ, yet this might be anticipated
when one considers the heavy and constant
environmental exposure to which the lung is subjected
by breathing.
• Although most of these infections are in the upper
airways, various types of microbial agents also injure
the lung. In the upper airways, viral infections
predominate.

Pulmonary Infections
• Pneumonia is the commonest type of lung infection and
accounts for 8.5-10% of hospitalizations in the US, as well
as for 3% of deaths in the population .
• PNA is the 4th leading cause of death in the population over
75 yrs. of age, and is a common autopsy finding, often
representing the "immediate cause of death." 80% of AIDS
patients die of respiratory failure and over 60% of these
have a pulmonary infection . Pneumonia has a morphologic
spectrum which traditionally includes bronchopneumonia,
lobar pneumonia, and interstitial pneumonia. In addition,
there is a category of infectious granulomas, due primarily
to tuberculosis and a variety of fungi.
• A Patient's Story
Pulmonary Infections
Bacterial infections typically cause lobar or
bronchopneumonia both of which are characterized
histologically by neutrophilic intra-alveolar exudates. Viral
pneumonias generally manifest as interstitial inflammatory
processes, while fungal and mycrobacterial infections are
granulomatous. Other infectious lesions are an abscess
and empyema (infection of the pleura).
• Atypical pneumonia is a clinical term applied to patients
with an acute febrile respiratory presentation and patchy
interstitial infiltrates without alveolar exudates. The most
common agents are mycoplasma and legionella.
• Mycoplasma Pneumonia Rap

Pulmonary Infections
The lung is normally a sterile environment. Infection
results when there is alteration in normal host defense
mechanisms or diminution in the general immune status
of an individual, or when an immunocompetent
individual is exposed to a virulent organism which
overwhelms the host defenses

Entry of Microorganisms
Inhalation
• Most microbes can be inhaled but in most cases this exposure is without
untoward effects on the host. Infection by inhalation depends in some
instances on the virulence of the organism i.e. tuberculosis, and in other
situations on the dosage of exposure i.e. Histoplasma from bat droppings in
caves or the Hantavirus from rodent droppings. Bacteria & viruses are small
enough to reside on aerosolized droplets that can be inhaled. Mechanisms
which trap particles in the airways are more effective against dry materials
than against liquid droplets.
• The Hantavirus Diseases
• Hoarder's Hanta Virus
• Yosemite Hanta Virus Outbreak
• A Patient's Story

Entry of Microorganisms
• Aspiration
• Aspiration, particularly at night, is a common event and
may include small amounts of the bacterial and fungal
flora which resides normally in our mouths. Nocturnal or
similar aspiration is not usually a problem as our normal
defense mechanisms can eliminate these small
dosages. Sometimes, however, these microbes lodge in
the upper airways and form larger colonies which when
aspirated result in infection.

Pulmonary Infections
• Pneumonia – Inflammatory process of the lung parenchyma, usually
infectious in origin
• 6th leading cause of death in the United States and the most common
cause of infection-related mortality
• Classifications of Pneumonia
– Community Acquired: Acute
• Typical: Streptococcus Pneumoniae, Hemophilus Influenzae,
Staphylococcus Aureus
• Atypical: Legionella Pneumophila, Chlamydophila
Pneumoniae, Mycoplasma Pneumoniae, Viruses

Streptococcus Pneumoniae
• Gram-positive, A significant human pathogenic
bacterium, S. pneumoniae was recognized as a major
cause of pneumonia in the late 19th century.
• The organism causes many types of pneumococcal
infections other than pneumonia. These invasive
pneumococcal diseases include acute sinusitis, otitis
media, meningitis, bacteremia, sepsis, osteomyelitis,
septic arthritis, endocarditis, peritonitis, pericarditis,
cellulitis, and brain abscess
• S. pneumoniae is one of the most common causes of
bacterial meningitis

Streptococcus Pneumoniae
• A vaccine against Streptococcus pneumoniae exists,
recommended for the elderly or those with chronic lung
disease.
• S. pneumoniae is part of the normal upper respiratory
tract flora, but, as with many natural flora, it can become
pathogenic under the right conditions (e.g., if the
immune system of the host is suppressed). Invasins,
such as pneumolysin, an antiphagocytic capsule,
various adhesins and immunogenic cell wall
components are all major virulence factors.

Hemophilus Influenzae
• Gram-negative, rod-shaped bacterium first described in
1892 during an influenza pandemic.
• it is generally aerobic, but can grow as a facultative
anaerobe
• H. influenzae was mistakenly considered to be the
cause of influenza until 1933, when the viral etiology of
the flu became apparent. Still, H. influenzae is
responsible for a wide range of clinical diseases;
• A Patient's Story

Hemophilus Influenzae
• Most strains of H. influenzae are opportunistic
pathogens; that is, they usually live in their host without
causing disease, but cause problems only when other
factors (such as a viral infection, reduced immune
function or chronically inflamed tissues, e.g. from
allergies) create an opportunity.
• In infants and young children, H. influenzae type b (Hib)
causes bacteremia, pneumonia, and acute bacterial
meningitis AND Epiglotttis
• Due to routine use of the Hib conjugate vaccine the
incidence of invasive Hib disease has declined

Staphylococcus Aureus
• Gram-positive coccal bacterium. It is frequently found as part of the
normal skin flora on the skin and nasal passages.
• It is estimated that 20% of the human population are long-term
carriers of S. aureus. S. aureus is the most common species of
staphylococci to cause Staph infections. The reasons S. aureus is a
successful pathogen are a combination of bacterial immuno-evasive
strategies. One of these strategies is the production of carotenoid
pigment staphyloxanthin which is responsible for the characteristic
golden color of S. aureus colonies.
• This pigment acts as a virulence factor, primarily being a bacterial
antioxidant which helps the microbe evade the hosts immune system
in the form of reactive oxygen species which the host uses to kill
pathogens
Staphylococcus Aureus
• S. aureus can cause a range of illnesses from minor skin infections, such
as pimples, impetigo, boils (furuncles), cellulitis folliculitis, carbuncles,
scalded skin syndrome, and abscesses; to life-threatening diseases such
as pneumonia, meningitis, osteomyelitis, endocarditis, toxic shock
syndrome (TSS), bacteremia, and sepsis.
• It is still one of the five most common causes of nosocomial infections,
often causing postsurgical wound infections. Each year, some 500,000
patients in American hospitals contract a staphylococcal infection.
• Methicillin-resistant S. aureus, abbreviated MRSA and often pronounced
"mer-sa" is one of a number of greatly-feared strains of S. aureus which
have become resistant to most antibiotics.
• Map
• Pimple/Boil
• Meningitis - Meningoccal

Staphylococcus Aureus
• MRSA strains are most often found associated with
institutions such as hospitals, but are becoming
increasingly prevalent in community-acquired infections.
• The treatment of choice for S. aureus infection is
Penicillin; in most countries, though, Penicillin
resistance is extremely common, and first-line therapy is
most commonly a penicillinase-resistant β-lactam
antibiotic (for example, Oxacillin or Fucloxacillin).
Combination therapy with Gentamicin may be used to
treat serious infections, such as endocarditis, but its use
is controversial because of the high risk of damage to
the kidneys. The duration of treatment depends on the
site of infection and on severity.

Legionella Pneumophila
• Aerobic, non-spore forming, Gram-negative bacterium
• the primary human pathogenic bacterium in this group
and is the causative agent of Legionellosis or
Legionnaires' disease.
• In humans, L. pneumophila invades and replicates in
macrophages. The internalization of the bacteria can be
enhanced by the presence of antibody and complement,
but is not absolutely required. A pseudopod coils around
the bacterium in this unique form of phagocytosis
• Primary source of infection = water supply
• Azithromycin or Moxifloxacin are the standard treatment
Chlamydophila Pneumoniae
• C. pneumoniae is a common cause of pneumonia
around the world. C. pneumoniae is typically acquired
by otherwise healthy people and is a form of
community-acquired pneumonia. Because treatment
and diagnosis are different from historically recognized
causes such as Streptococcus pneumoniae, pneumonia
caused by C. pneumoniae is categorized as an "atypical
pneumonia.“
• This atypical bacterium commonly causes pharyngitis,
bronchitis and atypical pneumonia

Mycoplasma Pneumoniae
• the causative agent of human primary atypical
pneumonia (PAP) or "walking pneumonia.“
• Mycoplasma pneumoniae is a very small bacterium
• Antibiotics with activity against these organisms include
certain macrolides (Erythromycin, Azithromycin,
Clarithromycin), fluoroquinolones and their derivatives
(e.g., Ciprofloxacin, Levofloxacin), and Tetracyclines
(e.g., Doxycycline)

Viral Pneumonia
• Viral pneumonia is a pneumonia caused by a virus
• Viruses are one of the two major causes of pneumonia,
the other being bacteria; less common causes are fungi
and parasites. Viruses are the most common cause of
pneumonia in children, while in adults bacteria are a
more common cause.
• Symptoms of viral pneumonia include fever, non-
productive cough, runny nose, and systemic symptoms
(e.g. myalgia, headache). Different viruses cause
different symptoms.

Viral Pneumonia
• Common causes of viral pneumonia are:
• Influenza virus A and B
• Respiratory syncytial virus (RSV)
• Human parainfluenza viruses (in children)
• Rarer viruses that commonly result in pneumonia include:
• Adenoviruses (in military recruits)
• Metapneumovirus
• Severe acute respiratory syndrome virus (SARS, coronavirus)
• Viruses that primarily cause other diseases, but sometimes cause
pneumonia include:
• Herpes simplex virus (HSV), mainly in newborns
• Varicella-zoster virus (VZV) – chickenpox, shingles
• Measles virus
• Rubella virus
• Cytomegalovirus (CMV), mainly in people with immune system problems
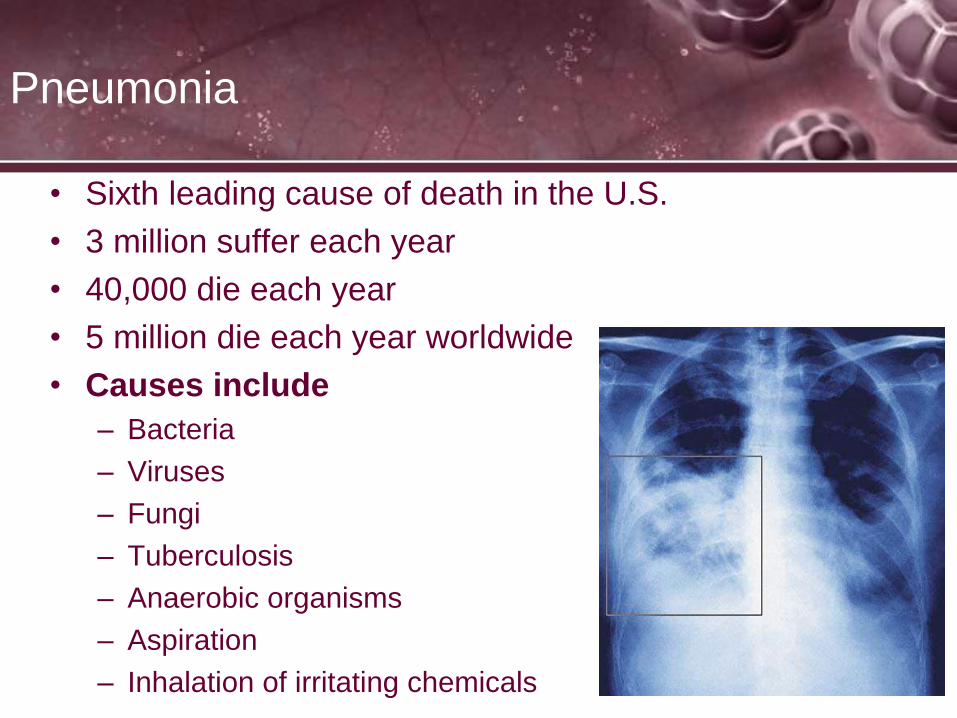
Pneumonia
• Sixth leading cause of death in the U.S.
• 3 million suffer each year
• 40,000 die each year
• 5 million die each year worldwide
• Causes include
– Bacteria
– Viruses
– Fungi
– Tuberculosis
– Anaerobic organisms
– Aspiration
– Inhalation of irritating chemicals
Pneumonia
• Pneumonia or pneumonitis with consolidation is the
result of an inflammatory process that primarily affects
the gas exchange area of the lung.
• In response to the inflammation, blood serum and some
RBC’s from the adjacent capillaries pour into the alveoli
• Leukocytes move into the infected area to engulf and kill
the invading bacteria
• Increased numbers of macrophages appear to remove
cellular and bacterial debris
• If all this material fills the alveoli, they are said to be
“consolidated”

Pneumonia
• Pathologic and structural changes associated with
pneumonia are:
– Inflammation of the alveoli
– Alveolar consolidation
– Atelectasis
– Primarily obstructive in nature
Pneumonia– Etiology
• Inhalation of aerosolized infectious particles – aerosol
particles generated by coughing
• Aspiration of organisms colonizing the oropharynx
– Occurs in all individuals, especially during sleep
– Impairment of the gag reflex allows large volume aspiration
• Direct inoculation of organisms into the lower airway –
suction catheters, ET tubes

Pneumonia – Etiology
• Spread of infection to the lungs from adjacent structures
– Infrequent source of infection
– Liver abscesses
• Spread of infection to the lungs through the blood
– Hematogenous dissemination (septic spread)
– Right-sided bacterial endocarditis

Pneumonia – Etiology
• Reactivation of latent infection, usually resulting from
immunosuppression but may occur spontaneously
• There are four stages of progression in pneumonia:
– Inflammatory Stage
– Red hepatization stage
– Grey hepatization stage
– Resolution stage

Pneumonia
• Inflammatory Stage
– Inflammatory pulmonary edema
– Engorgement of the pulmonary capillaries
– Exudation of serous fluid
– This stage is localized to the areas of infection

Pneumonia
• Red Hepatization Stage
– Onset 24 to 48 Hours Post Infection
– Alveolar spaces filled with coagulated exudate
• Fibrin
• Red blood cells
• Polymorphonuclear leukocytes
• Bacteria
– Red liver-like appearance of lung tissue

Pneumonia
• Gray Hepatization Stage
– Occurs 4 to 5 days post infection
– Alveolar spaces filled with many polymorphonuclear
leukocytes and few red blood cells
– Yellow-gray appearance of lung tissue

Pneumonia
• Resolution Stage
– Healing stage
– Exudate liquefied by enzymes of leukocytes
– Phagocytes reabsorb the liquid
– Areas of atelectasis begin to re-inflate

Pneumonia
• Types of pneumonia
– Lobar pneumonia: affects a large and continuous area of the
lobe of a lung
– Bronchial pneumonia: the acute inflammation of the walls of
the bronchioles. It is a type of pneumonia characterized by
multiple foci of isolated, acute consolidation, affecting one or
more pulmonary lobules.

Pneumonia
• Classification of Pneumonia
– Community acquired: acute and chronic
• Acute: rapid onset of symptoms
• Chronic: slower onset with gradually escalating symptoms
– Health care associated pneumonia (HCAP) [previously known
as nosocomial infections]
• Defined as pneumonia occurring in any pt. hospitalized for
2 or more days in the past 90 days in an acute care setting
or who, in the past 30 days resided in a LTC or SNF
Pulmonary Infections
• Classifications of Pneumonia
– Ventilator associated pneumonia (VAP)
• A lower respiratory tract infection that develops more
than 48 – 72 hrs after endotracheal intubation.
• VAP Busters


Pneumonia
• Causative agents
– Gram positive organisms
– Gram negative organisms
– Atypical organisms
– Anaerobic bacterial infections
– Viral causes
– Other causes

Pneumonia
• Gram Positive Bacteria
– Streptococcus pneumoniae
• Accounts for 80% of all bacterial pneumonias
• Found singly, in pairs, and in short chains
• Transmitted by aerosol via cough or sneeze
• Generally an acute community acquired organism
• Sputum is usually yellow in color

Pneumonia
• Gram Positive Bacteria (cont)
– Clostridium difficile (C-diff)
• Anaerobic spore-forming organisms of drumstick or
spindle shape
• Hospital acquired in patients on antibiotic therapy
• Replaces normal flora causing severe gastric instability
and diarrhea mimicking flu and colitis
• Fast becoming antibiotic resistant
• Hands MUST be washed with soap and water before and
after entering patient room
Pneumonia
• Gram Positive Bacteria (cont)
– Staphylococcus aureus
• Responsible for “Staph infections” in humans
• Found singly, in pairs and in irregular clusters
• Transmitted by aerosol from a cough or sneeze and via
fomites
• Common cause of hospital acquired pneumonia and is
becoming extremely resistant to antibiotics thus the
abbreviation: MDRSA – multiple drug-resistant S. Aureus
• Sputum is usually yellow in color and foul smelling

Pneumonia
• Gram Negative Bacteria
– Rod shaped Bacilli
– Haemophilus influenzae
• Common pharyngeal organism
• Infections most often seen in children between 1 month to 6 yrs
of age
• Almost always the cause of acute epiglotitis
• Usually community acquired
• Transmitted via aerosol, contact, fomites
• Sensitive to cold and does not survive long
• Picmonic – Epiglotitis
• Clinical Symptoms - Stridor,Wheezing and Croup Cough
• Epiglotitis Explained and Illustrated

Pneumonia
• Gram Negative Bacteria (cont)
– Klebsiella pneumoniae
• Associated with lobar pneumonia
• Found singly, pairs and chains
• A normal inhabitant of the GI tract
• Transmitted by aerosol or fomites – especially the hands
of healthcare workers
• Usually a hospital acquired infection
• Mortality is high because septicemia is a frequent
complication
Pneumonia
• Gram Negative Bacteria (cont)
– Pseudomonas aeruginosa
• Water loving organism
• Leading cause of hospital acquired pneumonia
• Normally colonizes in the GI tract
• Frequently found in burns, the respiratory tract of
intubated or trached respiratory patients, catheters,
respiratory therapy equipment
• Transmitted via aerosol or contact with fomites
• Sputum infected is usually sweet smelling and green
Pneumonia
• Gram Negative Bacteria (cont)
– Escherichia coli or E.coli
• Normal GI inhabitant
• Usually hospital acquired pneumonia
– Moraxella catarrhalis
• Naturally inhabits the pharynx
• Third most common cause of acute exacerbation of
chronic bronchitis
• Usually hospital acquired

Pneumonia
• Gram Negative Bacteria (cont)
– Serratia Species
• Very water loving species
• Usually hospital acquired
• Lives well on fomites, under sinks, rampant spread in
respiratory equipment
• Multi Drug Resistant Infections

Pneumonia
• Atypical Organisms
– Mycoplasma pneumoniae
• Common cause of mild pneumonia (walking pneumonia)
• Smaller than bacteria but larger than viruses
• Described as Primary Atypical Pneumonia because the
organism escapes ID by standard bacteriologic tests
• Most frequently seen in people younger than 40
• Spreads easily where people congregate
• Usually community acquired

Pneumonia
• Atypical Organisms (cont)
– Legionella pneumophila
• Discovered in 1976 during an outbreak of severe
pneumonia-like disease at an American Legion
convention
• Gram negative bacillus
• Transmitted via aerosol
• Thought to have colonized in the AC units of the
convention hall
• Community acquired

Pneumonia
• Viral Causes
– Influenza Virus
• Several subtypes in which A and B are the most common
causes of viral respiratory tract infections
• Commonly occur in epidemics
• Children, young adults and the elderly are most at risk
• Transmitted via aerosol
• Survives well in conditions of low moisture and humidity
• Found also in swine, horses and birds

Pneumonia
• Viral Causes (cont)
– Respiratory Syncytial Virus (RSV)
• Member of the paramyxovirus group along with
parainfluenza, mumps and rubella viruses
• Most often seen in children under the age of 6
• Transmitted via aerosol and direct contact
– Parainfluenza Virus
• Member of the paramyxovirus group
• Type 1 is considered a “croup” type virus seen in the young
• Type 2 and 3 present as a severe type of infection
• Transmitted via aerosol and direct contact
Pneumonia
• Viral Causes (cont)
– Adenoviruses
• More than 30 subgroups
• Transmitted by aerosol
• Generally seasonal outbreaks
• Community acquired

Pneumonia
• Viral Causes (cont)
– Severe Acute Respiratory Syndrome (SARS)
• First reported in China in 2002
• Newly recognized Coronavirus
• Transmitted via droplet and aerosol and possibly
contaminated objects
• Incubation is 2-7 days
• 10-20% require mechanical ventilation
• Community acquired

Pneumonia
• Other Causes
– Aspiration Pneumonitis
• Caused by aspiration of stomach contents
• Major cause of anaerobic lung infections
• May progress into ARDS
– Varicella (chickenpox)
– Rubella (Measles)
– Rickettsiae
• Intracellular parasites
• Most well known: Rocky Mountain Spotted Fever

Pneumonia
• Other Causes
– Yeast pneumonias occur, some of the pathogens include:
• Candida albicans,
• Cryptococcus neoformans
• Aspergillus
– Fungal Infections
• Most fungi are aerobes thus making lungs prime targets
• Fungal pathogens include:
– Histoplasma capsulatum
– Coccidioides immitis
– Blastomyces dermatitidis

Tuberculosis
Tuberculosis Today CDC - TB statistics
Tuberculosis
• TB is a chronic bacterial infection that primarily affects the lungs but can involve
almost any part of the body
• It is one of the oldest diseases known to man and remains one of the most
widespread diseases in the world. Chapter 1 - TB
• Called “consumption, Captain of the men of death and the White plague
• 10 – 15 million infected in the U.S.
• 17,000 new infections per year
• WHO estimates that between the years 2000 and 2020 35 million people
worldwide will die from TB
• Chapter 2 - TB
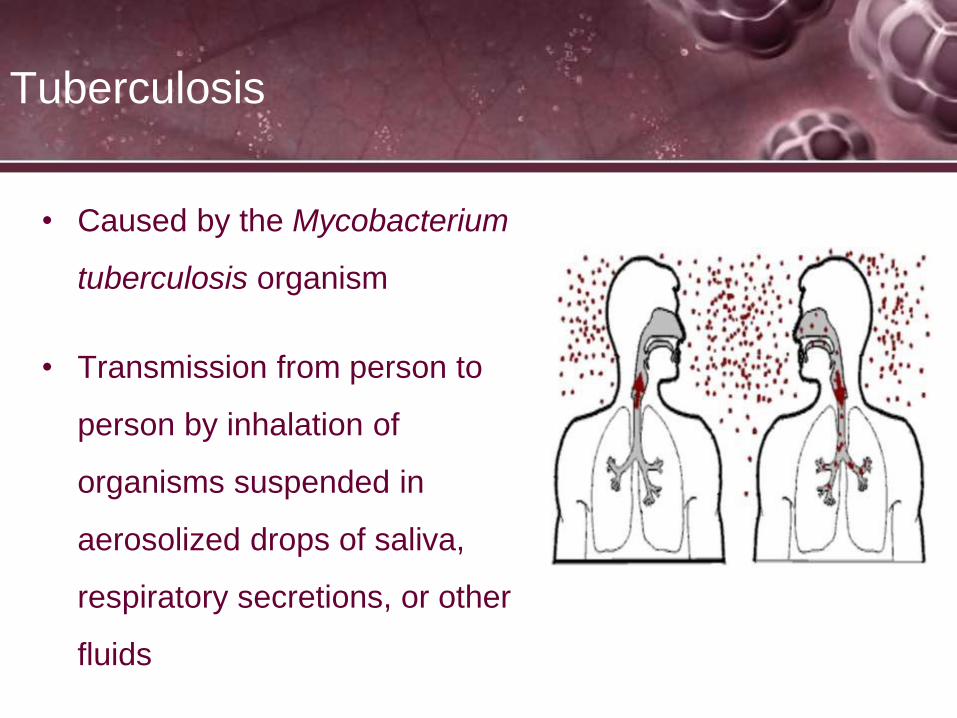
Tuberculosis
• Caused by the Mycobacterium
tuberculosis organism
• Transmission from person to
person by inhalation of
organisms suspended in
aerosolized drops of saliva,
respiratory secretions, or other
fluids

Tuberculosis
• Pathophysiology
– Highly aerobic organism
– Multiplies more rapidly in the presence of higher partial
pressures of oxygen, especially in lung apices
– Primary TB follows the patients first exposure to the organism
– Upon inhalation, the bacterium is implanted into the alveoli
and begin to multiply
– The initial inflammation causes an influx of macrophages and
leukocytes which engulf but do not kill the organism

Tuberculosis
• Pathophysiology
– This causes the pulmonary capillary bed to dilate, the
interstitium to fill with fluid, and the alveolar epithelium to
swell from the edema
– The alveoli become consolidated and at this point the TB
skin test becomes positive
– In approx. 2-10 weeks, the lung tissue surrounding the
infection slowly produces a protective cell wall around the
infection called a tubercle or granuloma

Tuberculosis
• Pathophysiology
– After the formation of the tubercle, the center of the mass
breaks down and fills with necrotic tissue. At this point the
tubercle is called a caseous lesion or caseous granuloma
– As the infection becomes controlled by the immune system
or medication, fibrosis and calcification of the lung
parenchyma replaces the tubercle.
– As a result of the fibrosis and calcification, the lung retracts,
becomes scarred, and can cause dilation of the bronchi and
bronchiectasis
– Chapter 3 - TB

Tuberculosis
• Post primary tuberculosis
– Also called secondary or reinfection TB
• A term used to describe the reactivation of TB months or
even years after the initial infection has been controlled
• Tubercle bacilli can remain dormant for decades
• At any time, TB can reactivate; especially in patients with
weakened immunity
Tuberculosis
• If the infection is uncontrolled, cavitation of the tubercle
develops
• In severe cases a deep tuberculous cavity may rupture and
allow air and infected material to flow into the pleural space
or the tracheobronchial tree
• Pneumothoracies and pleural disease are common
complications of TB

Tuberculosis
Granuloma
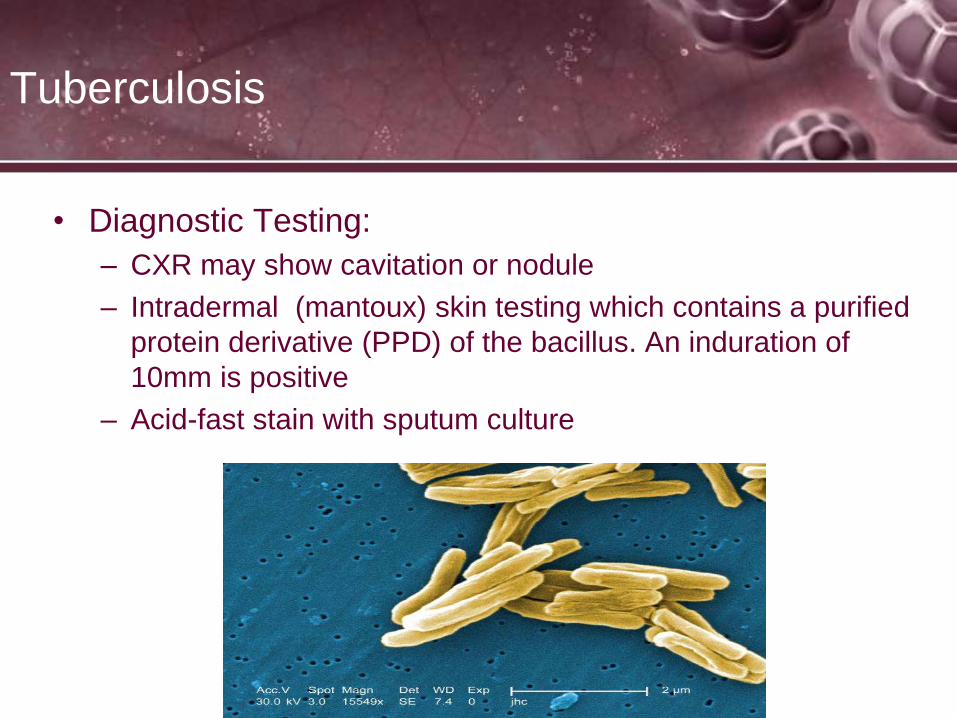
Tuberculosis
• Diagnostic Testing:
– CXR may show cavitation or nodule
– Intradermal (mantoux) skin testing which contains a purified
protein derivative (PPD) of the bacillus. An induration of
10mm is positive
– Acid-fast stain with sputum culture

Tuberculosis
• Radiologic findings
• Increased opacity
• Cavity formation
• Calcification & fibrosis
• Pleural effusions

Tuberculosis
• Clinical Findings
– Fatigue
– Fever
– Night sweats
– Weight loss
– Chronic cough
– Sputum production/hemoptiysis
Tuberculosis
• Clinical Findings
– Auscultation
• Crackles
• Wheezes
• Bronchial breath sounds
Tuberculosis/Treatment
• Keep isolated in a AIRBORN ISOLATION room,
(negative pressure room)• The goal of treatment is to cure the infection with drugs that fight the TB
bacteria. Treatment of active pulmonary TB will always involve a combination
of many drugs (usually four drugs). All of the drugs are continued until lab
tests show which medicines work best.• The most commonly used drugs include:
• Isoniazid
• Rifampin
• Pyrazinamide
• Ethambutol
• Other drugs that may be used to treat TB include:
• Amikacin
• Ethionamide
• Moxifloxacin
• Para-aminosalicylic acid
• Streptomycin
• Chapter 4 - TB


Restrictive Diseases
Ascites
No explanation needed

Restrictive Diseases
• Restrictive diseases generally:
– Causes a decrease in lung compliance
– Decrease in lung volumes
– Can be caused by any alveolar filling lung defect
– Can be intrinsic or extrinsic

Pneumothorax
• Presence of air or gas in the pleural
space of the thorax creating positive
pressure within the pleura
• This gas gains entrance into the
pleural space in 3 ways:
– Rupture of bronchus or alveoli
• Closed Pneumothorax
– Penetration of chest wall
• Open Pneumothorax
– Esophageal fistula/perforated
abdominal viscus
• Closed pneumothorax
Spontaneous
Pneumothorax

Spontaneous Pneumothorax
• Escape of air into the pleural space without an obvious
cause
• Spontaneous pneumothorax (closed)
– Can occur without apparent underlying disease
– Blebs from emphysema - HRCT shows presence of small
blebs in more than 80% of patients
– Brochopulmonary fistula, esophageal fistula, perforated
abdominal viscus

Spontaneous Pneumothorax
• Occurs commonly in tall males at the apices
• Usually patients in late teens to early twenties
• Cigarette smoking a factor in 90% of patients
• Occurs in patients with underlying COPD
• Mortality rate of patients with secondary spontaneous
pneumothorax was 43% in studies, most from their
underlying disease
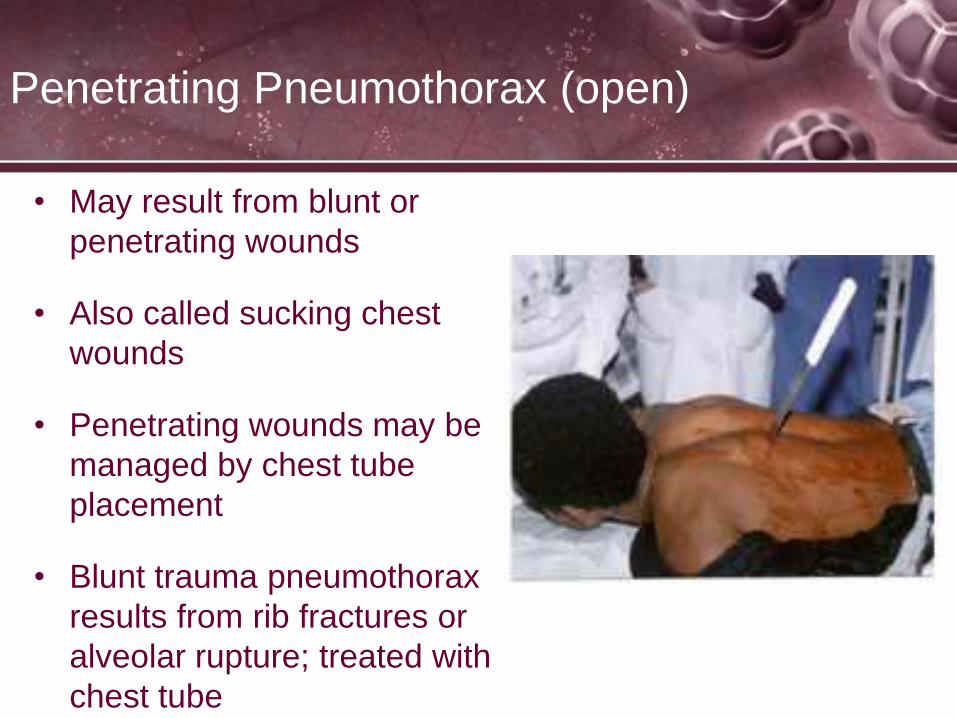
Penetrating Pneumothorax (open)
• May result from blunt or
penetrating wounds
• Also called sucking chest
wounds
• Penetrating wounds may be
managed by chest tube
placement
• Blunt trauma pneumothorax
results from rib fractures or
alveolar rupture; treated with
chest tube

Pneumothorax
• Esophageal rupture and tracheal
fracture: requires bronchoscopy and
surgical correction
• Iatrogenic pneumothorax: caused
by needle aspiration, thoracentesis,
or central line placement; usually
resolve without need for chest tube

Tension Pneumothorax
• Occurs when air in the pleural space exceeds
atmospheric pressure
• Creates mediastinal shift to the unaffected side
– Creates torsion on the inferior vena cava
– Decreases venous return to the right side of the heart
– Decrease in cardiac output resulting in hypotension and
tachycardia
– Tension Pneumothorax Explained

Tension Pneumothorax
• Depresses the diaphragm
• May cause collapse of the lung on the affected side
– Leads to tachypnea and increased work of breathing
– Hypoxemia.
• Treated with emergency decompression by insertion of
needle between the second and third ribs in the
midclavicular line; above the rib
• All positive pressure ventilation is Contraindicated!
until decompression is accomplished

Pneumothorax – Radiologic Findings
• Chest X-ray is Definitive
– Free air in pleural space
– Visible edge of lung
– Lack of vascular
markings
• Air must occupy at least
20% of pleural space to
be visible on x-ray

Tension
Pneumothorax
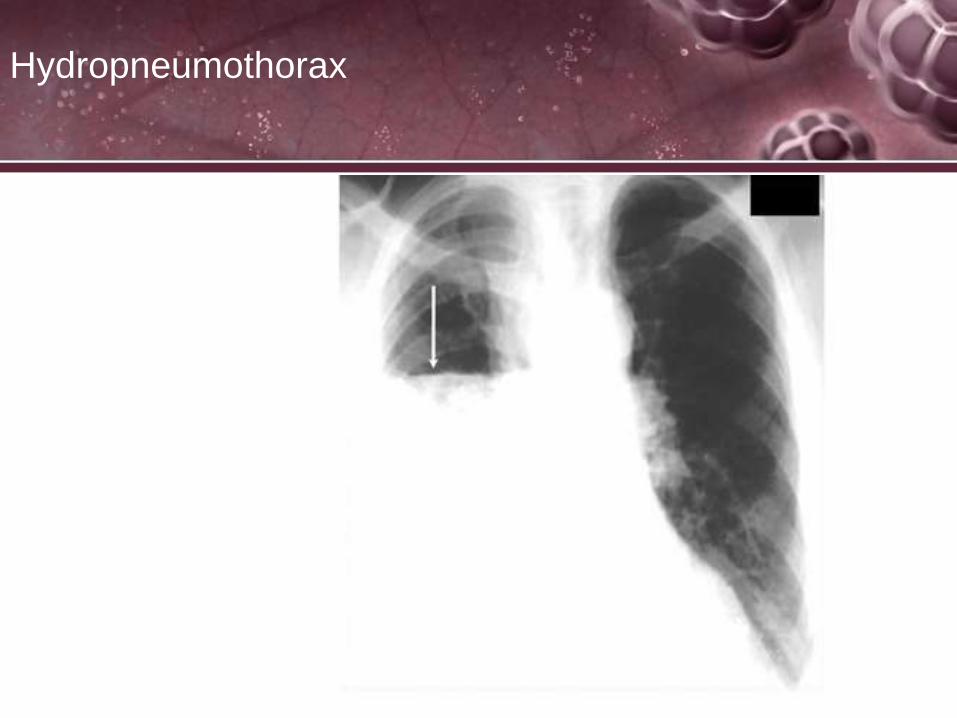
Hydropneumothorax

Pneumothorax – Clinical Findings
• Respiratory distress
• Dyspnea
• Chest pain
• Cyanosis/decrease in SPO2
• Tachycardia/Tachypnea
• Hypotension
• Reduced or absent breath sounds on the affected side
• Possible subcutaneous emphysema
• Mediastinal shift
• Unilateral chest rise and fall
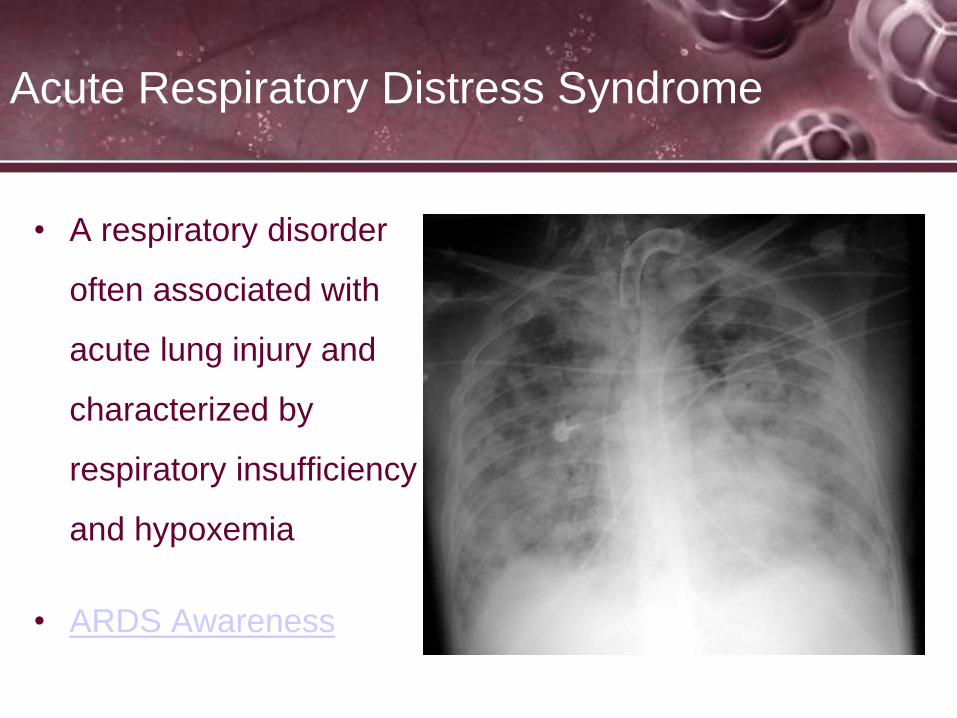
Acute Respiratory Distress Syndrome
• A respiratory disorder
often associated with
acute lung injury and
characterized by
respiratory insufficiency
and hypoxemia
• ARDS Awareness
Respiratory Distress Syndrome –
Etiology
• Primary Risk Factors – Direct Lung Injury
– Pneumonia
– Aspiration of gastric contents
– Inhalation of toxic substances, including high concentrations
of oxygen
– Near drowning
– Lung contusion
Respiratory Distress Syndrome –
Etiology
– Sepsis
– Burn injury
(chemical or heat)
– Prolonged systemic
hypotension
– Multiple traumas
(non-thoracic)
• Secondary Risk Factors – Indirect Lung Injury
– Hypovolemic shock
– Pancreatitis
– Effects of drugs
– Multiple drug infusions
– Sickle cell anemia crisis

Respiratory Distress Syndrome –
Pathophysiology
• Three Phases of ARDS
• Exudative phase – generally last three to five days
• Fibroproliferative phase – can last for a few days to
weeks
• Resolution phase

Respiratory Distress Syndrome –
Pathophysiology
• Exudative phase
• Consolidative process with injury to the alveoli
• Inflammatory process secondary to the presence of
activated macrophages
• Destruction of type I pneumocytes
• Migration of interstitial fluid, protein, fibrin,
neutrophils, and red blood cells through the damaged
alveolar wall

Respiratory Distress Syndrome –
Pathophysiology
• Fibroproliferative phase
• Lung repair begins
• Macrophage and lymphatic cleanup of cellular debris
• Hyperplasia of alveolar type II pneumocytes,
proliferation of fibroblasts within alveolar basement
membrane and intraalveolar spaces.
• Variable lung fibrosis can occur depending on the
extent of fibroblast involvement

Respiratory Distress Syndrome –
Pathophysiology
• Resolution phase
• Increases in lung compliance
• Decreases in oxygen requirements
• Clearing of CXR
• Weaning of ventilatory support

Respiratory Distress Syndrome
• Radiologic Findings
• Increased opacity
due to the increased
lung density
• Ground glass
appearance
• Infiltrates of one or
both lungs

Respiratory Distress Syndrome
• Clinical Findings
• Tachypnea disproportionate to blood gas changes
• Progressive hypoxemia
• Increase in A-a gradient
• Decrease in vital capacity
• Pulmonary capillary wedge pressure of < 18 mmHg
• A downward trending of static and dynamic compliance

Pulmonary Interstitial Disease (ILD)
• Refers to a broad category (over 100 separate
disorders) of lung diseases and all are associated with
inflammatory changes
• Anatomic alterations may involve the bronchi, alveolar
walls, and adjacent alveolar spaces
• Severe cases, inflammation leads to fibrosis,
granulomas, honeycombing, and cavitation

Pulmonary Interstitial Disease –
Pathophysiology
• Interstitial space is the
area between the Type I
and Type II alveolar cells
and the vascular
endothelial cells. It
contains macrophages,
interstitial fibroblasts, and
matrix substance.
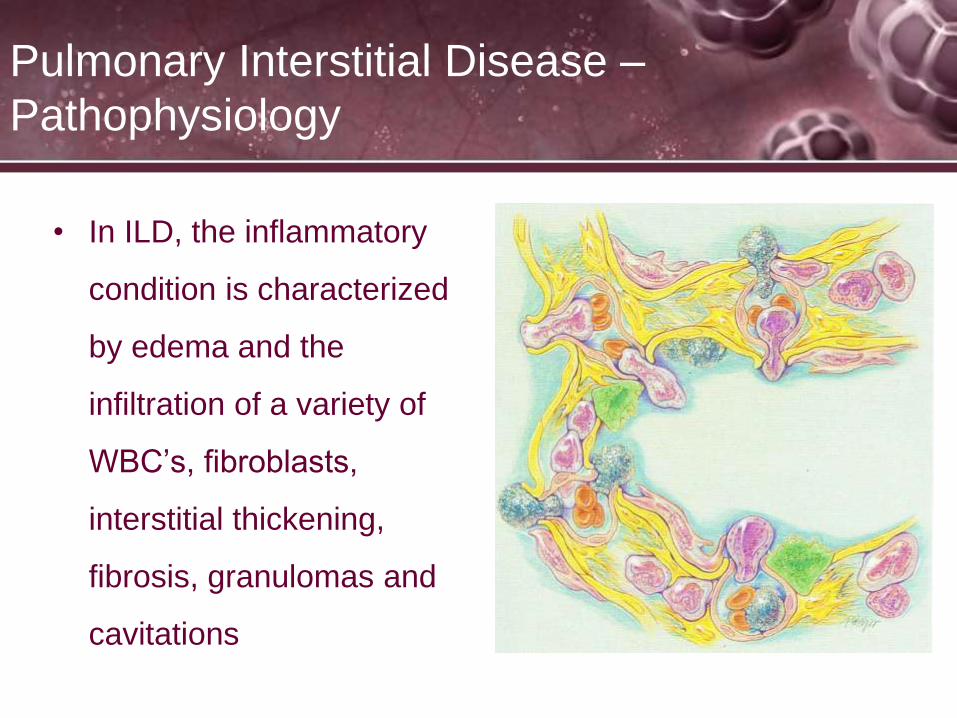
Pulmonary Interstitial Disease –
Pathophysiology
• In ILD, the inflammatory
condition is characterized
by edema and the
infiltration of a variety of
WBC’s, fibroblasts,
interstitial thickening,
fibrosis, granulomas and
cavitations

Pulmonary Interstitial Disease – Etiology
• May have known causes or associations
– Exposure to occupational and environmental factors, e.g.
asbestosis
– Exposure to radiation
– Smoking
– Associated with collagen diseases or diseases of the
connective tissue, e.g. sarcoidosis
– May have genetic associations

Pulmonary Interstitial Disease – Etiology
• May have unknown
causes
– Idiopathic pulmonary
fibrosis
– Non-specific interstitial
pneumonitis
Idiopathic Pulmonary Fibrosis

ILD Causes
• ILD may be classified according to the cause.
• Inhaled substances
– Inorganic
• Silicosis
• Asbestosis - Mesothelioma Story
– Organic
• Hypersensitivity pneumonitis - A Patient's Story
• Drug induced
– Antibiotics
– Chemotherapeutic drugs
– Antiarrhythmic agents
– Statins

ILD Causes
• Connective tissue disease
• Polymyositis
• Dermatomyositis
• Systemic lupus erythematosus - Personal Stories
• Rheumatoid arthritis - Statistics
• Infection Atypical pneumonia
• Pneumocystis pneumonia (PCP) - PCP Statistics
• Tuberculosis
• Chlamydia trachomatis
• Respiratory Syncytial Virus
• Idiopathic Sarcoidosis - Part I - Part II - Part III
• Hamman-Rich syndrome
• Antisynthetase Syndrome
• Malignancy Lymphangitic carcinomatosis

ILD treatment
• ILD is not a single disease, but encompasses many
different pathological processes. Hence treatment is
different for each disease.
• If a specific occupational exposure cause is found, the
person should avoid that environment. If a drug cause is
suspected, that drug should be discontinued.
• Many idiopathic and connective tissue-based causes of
ILD are treated with corticosteroids, such as
prednisolone. Some patients respond to
immunosuppressant treatment. Patients with hypoxemia
may be given supplemental oxygen

Pulmonary Fibrosis (from ILD)
• Pulmonary fibrosis occurs when lung tissue becomes
damaged and scarred. This thickened, stiff tissue
makes it more difficult for your lungs to work properly.
As pulmonary fibrosis worsens, you become
progressively more short of breath.
• The scarring associated with pulmonary fibrosis can be
caused by a multitude of factors. But in most cases,
doctors can't pinpoint what's causing the problem.
When a cause can't be found, the condition is termed
idiopathic pulmonary fibrosis.

Diagnosis of ILD/pulmonary fibrosis
• The diagnosis can be confirmed by lung biopsy
• The removed tissue is examined histopathologically by
microscopy to confirm the presence and pattern of fibrosis as
well as presence of other features that may indicate a specific
cause e.g. specific types of mineral dust or possible response
to therapy e.g. a pattern of so called non-specific interstitial
fibrosis
• On spirometry, as a restrictive lung disease, both the FEV1
(Forced Expiratory Volume in 1 Second) and FVC (Forced Vital
Capacity) are reduced so the FEV1/FVC ratio is normal or even
increased in contrast to obstructive lung disease where this
ratio is reduced. The values for residual volume and total lung
capacity are generally decreased in restrictive lung disease.

Diseases of the Spine
Kyphoscoliosis is
a combination of
Kyphosis and
Scoliosis and
causes the most
restriction of
the lungs
A Patient's Story
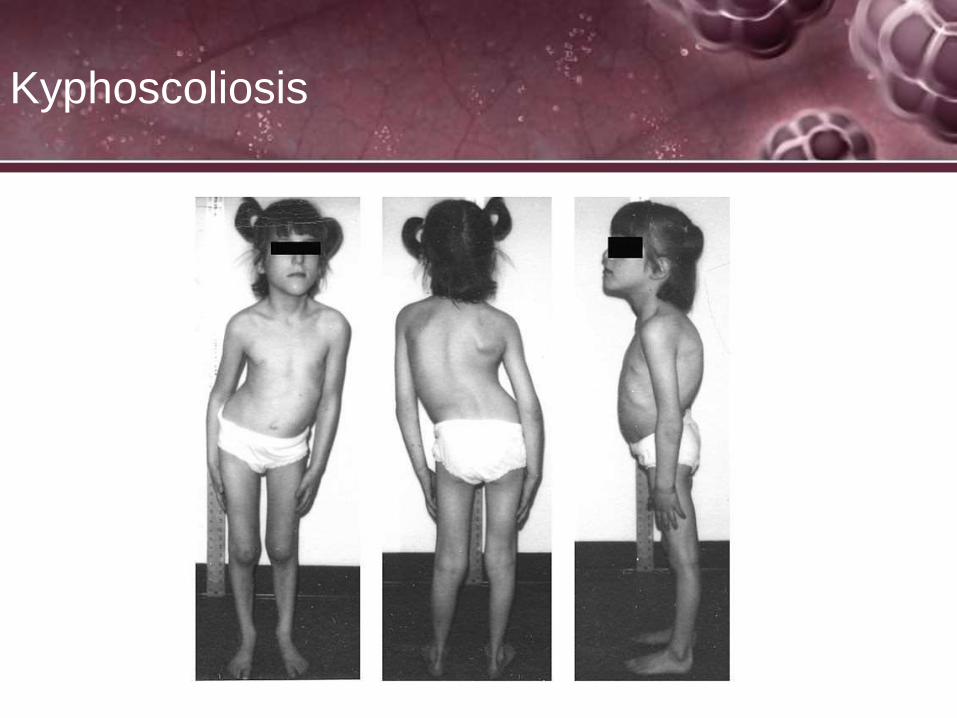
Kyphoscoliosis

Kyphoscoliosis treatments
• In kyphoscoliotic patients ventilatory mechanics are
impaired and may cause considerable hypoventilation,
especially during sleep
• Taking this into consideration nocturnal ventilation
seems to be the treatment of choice.
• intermittent positive pressure ventilation (nNIPPV) is
good in these patients
• the majority of these patients are still treated with long-
term oxygen therapy
• Tracheotomy and bronchial hygiene

Pectus carinatum
• also called pigeon chest, is a deformity of the chest
characterized by a protrusion of the sternum and ribs. It
is the opposite of pectus excavatum

Pectus carinatum
• People with pectus carinatum usually develop normal
hearts and lungs, but the deformity may prevent these
from functioning optimally. In moderate to severe cases
of pectus carinatum, the chest wall is rigidly held in an
outward position. Thus, respirations are inefficient and
the individual needs to use the diaphragm and
accessory muscles for respiration, rather than normal
chest muscles, during strenuous exercise. This
negatively affects gas exchange and causes a decrease
in stamina. Children with pectus deformities often tire
sooner than their peers, due to shortness of breath and
fatigue. Commonly concurrent is mild to moderate
asthma.
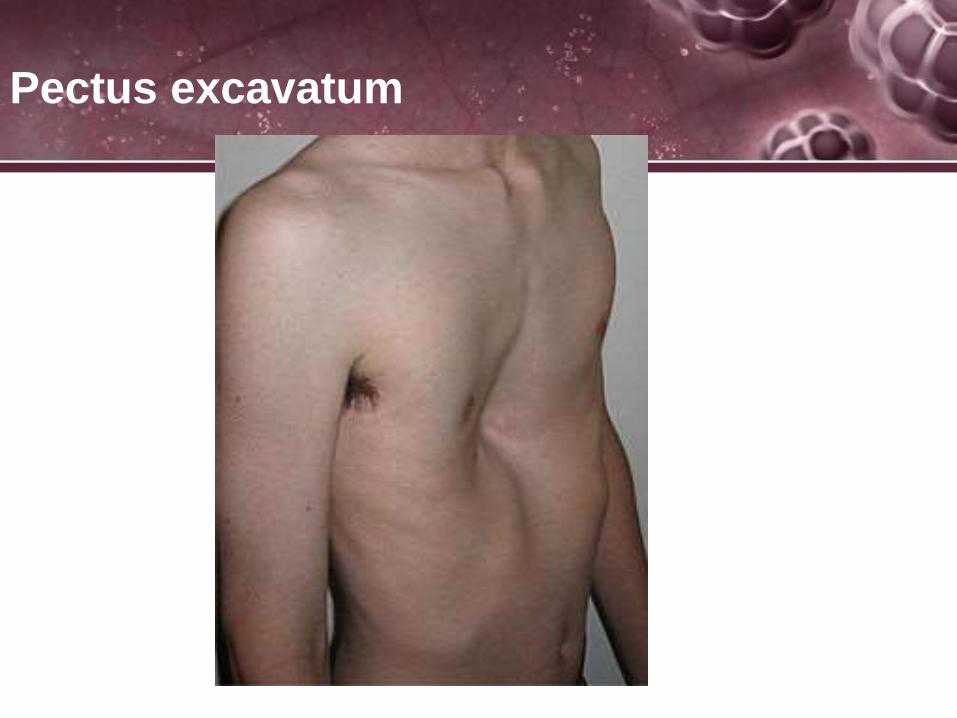
Pectus excavatum

Pectus excavatum
• Pectus excavatum is the most common congenital
deformity of the anterior wall of the chest, in which
several ribs and the sternum grow abnormally. This
produces a caved-in or sunken appearance of the chest
It can either be present at birth or not develop until
puberty.
• Pectus excavatum is sometimes considered to be
cosmetic; however, depending on the severity, it can
impair cardiac and respiratory function and cause pain
in the chest and back.[People with the condition may
experience negative psychosocial effects, and avoid
activities that expose the chest.

Flail Chest
• A flail chest is a life-threatening medical condition that
occurs when a segment of the rib cage breaks under
extreme stress and becomes detached from the rest of
the chest wall. It occurs when multiple adjacent ribs are
broken in multiple places, separating a segment, so a
part of the chest wall moves independently. The number
of ribs that must be broken varies by differing
definitions: some sources say at least two adjacent ribs
are broken in at least two places,[1] some require three
or more ribs in two or more places

Flail Chest
Flail Chest Treatment
• Good analgesia including intercostal blocks, avoiding
narcotic analgesics as much as possible. This allows
much better ventilation, with improved tidal volume, and
increased blood oxygenation.
• Positive pressure ventilation, meticulously adjusting the
ventilator settings to avoid pulmonary barotrauma.
• Chest tubes as required.
• Adjustment of position to make the patient most
comfortable and provide relief of pain.
• Aggressive pulmonary toilet
Pleural Diseases

Pleural Diseases
• Transudative effusion
• Caused by:
Greater hydrostatic pressure
within the alveoli or pulmonary
capillaries forces fluid into the
pleural space
– ARDS
– CHF/Left sided heart failure
– MI
– Pulmonary embolus
• Exudative effusion
• Caused by:
• Diseases of the pleural
surface creating a fluid high
in protein, cellular debris,
pus, infective material
– Malignancies of the pleura
– Lymphomas
– Pneumonias
– TB
– Fungal diseases

Other Lung Diseases
Lung Cancer
Lung Cancer
• Lung cancer is the leading cause of cancer
deaths in the U.S.
• Women have higher mortality with lung CA than
any other cancer
• Cigarette smoking is the most common cause
• Genetic factors
• Environmental and occupational risk factors
• A Patient's Story
Lung Cancer – Risk Factors
Occupational/Environmental Exposure
– Asbestos
– Arsenic
– Chromium
– Radon
– Vinyl chloride
– Polycyclic aromatic
hydrocarbons
– Air pollution

Lung Cancer
Lung Cancer
• Types of lung cancer
Small-cell or oat-cell carcinoma
Non-small cell carcinoma
Squamous cell carcinoma
Adenocarcinoma
Large-cell carcinoma

Lung Cancer – Classification
• Small Cell Carcinoma
– Approximately 20% of lung cancers
– Has highest association with cigarette smoking
– Arises from K-type cells in the bronchial epithelium
– Commonly found near the hilar region

Lung Cancer – Classification
• Small Cell Carcinoma
(oat cell)
– Originates in lung tissue
next to central airways
and major blood vessels
– Grows very rapidly;
characterized by early
metastasis
– Generally already
metastasized when
detected

Lung Cancer – Classification – Non-
Small Cell Carcinoma
– Most common form of lung
cancer, found in approximately
40% of lung cancers
– Occurs in smokers, but is most
common cancer in non-
smokers
– Arises in mucous glands of the
tracheobronchial tree and
metastasizes to other organs
through the circulatory and
lymphatic systems.
(bronchoalveolar type arises
out of the terminal bronchioles
and alveoli)
• Adenocarcinoma (including bronchoalveolar cell carcinoma)

Lung Cancer – Classification – Non-
Small Cell Carcinoma
– Strongly associated with
smoking
– Most common type of lung
CA in men
– Arises from basal cells of
the bronchial epithelium
affecting large bronchi and
spreads by direct invasion of
surrounding tissue or lymph
node metastasis
– Causes significant airway
obstruction
– Generally slow growing
• Squamous Cell Carcinoma

Lung Cancer – Classification – Non-
Small Cell Carcinoma
– Undifferentiated cell type
of cancer; lack of
squamous cell features
– Has two subsets: clear
cell and giant cell
– Large cell CA grows and
metastasizes rapidly via
the circulatory and
lymphatic systems
• Large Cell Carcinoma


Lung Cancer

Lung Cancer
Lung Cancer – Staging of Lung
Cancer
• Staging of lung cancer
• “T” – Extent of Primary Tumor
– T1 – Small tumor, not locally advanced or invasive, < 3 cm
and not extending into the main bronchus
– T2 – Larger than T1, but minimally invasive, > 3 cm and may
invade the visceral pleura or extend into the main bronchus,
but > 2 cm from main carina; may cause segmental or lobar
atelectasis
Lung Cancer – Staging of Lung
Cancer
• “T” – Extent of Primary Tumor
– T3 – Locally advanced or invasive up to but not including
major intrathoracic structures; can be any size and may
involve the chest wall, diaphragm, mediastinal pleura,
parietal pericardium, or main bronchus within 2 cm of main
carina (but not involving carina); may cause atelectasis of
the entire lung
– T4 – Invades one of major intrathoracic structures such as
mediastinum, heart, esophagus, or carina; may cause
malignant pericardial or pleural effusion.

Lung Cancer – Staging of Lung
Cancer
• “N” – Involvement of Lymph Nodes
– N0 – No involved lymph nodes
– N1 – Presence of metastatic disease to nodes on the same
side as the tumor
– N2 – Presence of metastatic disease to nodes beyond the
same side but not to other side of the tumor
– N3 – Spread to nodes on opposite side of tumor

Lung Cancer – Staging of Lung
Cancer
• “M” – Presence of Metastasis
– M0 – Absence of metastasis
– M1 – Metastasis outside the chest

Lung Cancer – Clinical
Manifestations
• Local Growth
– Cough
– Dyspnea
– Hemoptysis
– Pain

Lung Cancer – Clinical
Manifestations
• Regional Growth
– Dysphagia
– Dyspnea
– Hoarseness
– Hypoxia
Lung Cancer – Clinical
Manifestations
• Regional Growth
– Pancoast’s Syndrome
• Apical tumors
• Shoulder pain radiating to ulnar area
• Involvement of superior vena cava leading to swelling of
face, neck, and upper chest

Lung Cancer – Clinical
Manifestations
• Regional Growth
– Horner’s Syndrome (Occurs on same side as tumor)
• Ptosis (Drooping of eyelid)
• Anhidrosis (Absence of sweating)
• Miosis (Constricted pupil)
Lung Cancer – Clinical
Manifestations
• Pericardial/Pleural Effusions
• Metastatic Disease
– Headache
– Hepatomegaly
– Change in mental status
– Pain

Lung Cancer – Clinical
Manifestations
• Metastatic Disease
– Papilledema (edema of the optic disk)
– Seizures
– Skin or soft tissue mass
– Syncope
– Weakness

Cancer treatment
• Cancer Treatments
• Surgery:
• If investigations confirm lung cancer, CT scan and often
positron emission tomography (PET) are used to
determine whether the disease is localized and
amenable to surgery or whether it has spread to the
point where it cannot be cured surgically.
• Blood tests and spirometry (lung function testing) are
also necessary to assess whether the patient is well
enough to be operated on. If spirometry reveals poor
respiratory reserve (often due to chronic obstructive
pulmonary disease), surgery may be contraindicated.

Cancer treatment
• Radiotherapy is often given together with
chemotherapy, and may be used with curative intent in
patients with non-small-cell lung carcinoma who are not
eligible for surgery.
• For small-cell lung carcinoma cases that are potentially
curable, chest radiation is often recommended in
addition to chemotherapy
• The use of adjuvant thoracic radiotherapy following
curative intent surgery for non-small-cell lung carcinoma
is not well established and is controversial. Benefits, if
any, may only be limited to those in whom the tumor
has spread to the mediastinal lymph nodes

Cancer treatment
• Small-cell lung carcinoma
• Even if relatively early stage, small-cell lung carcinoma
is treated primarily with chemotherapy and radiation
• Non-small-cell lung carcinoma
• Primary chemotherapy is also given in advanced and
metastatic non-small-cell lung carcinoma.
Chemotherapy
• The most common chemotherapy agents act by killing
cells that divide rapidly, one of the main properties of
most cancer cells. This means that chemotherapy also
harms cells that divide rapidly under normal
circumstances: cells in the bone marrow, digestive tract,
and hair follicles. This results in the most common side-
effects of chemotherapy: myelosuppression (decreased
production of blood cells, hence also
immunosuppression), mucositis (inflammation of the
lining of the digestive tract), and alopecia (hair loss).
Radiation
• Ionizing radiation, used to control or kill malignant cells.
• Radiation therapy may be curative in a number of types of cancer if
they are localized to one area of the body. It may also be used as part
of curative therapy, to prevent tumor recurrence after surgery to
remove a primary malignant tumor (for example, early stages of breast
cancer). Radiation therapy is synergistic with chemotheraphy, and has
been used before, during, and after chemotherapy in susceptible
cancers.
• Radiation therapy is commonly applied to the cancerous tumor
because of its ability to control cell growth. Ionizing radiation works by
damaging the DNA of exposed tissue leading to cellular death. To
spare normal tissues (such as skin or organs which radiation must
pass through in order to treat the tumor),

Pulmonary Vascular Disease

Pulmonary Vascular Disease –
Pulmonary Embolism
• Presence of occluding
emboli within the
pulmonary vasculature
which leads to
obstruction of blood flow
to all or part of the lung
• Pulmonary Embolism
Pulmonary Vascular Disease –
Pulmonary Embolism
• Predisposing conditions
– Presence of deep vein thrombosis (DVT)
– Advanced age
– Previous history of venous thrombosis or pulmonary
embolism
– Trauma
– Cerebral vascular accident (CVA)
– Thrombocytosis
Pulmonary Vascular Disease –
Pulmonary Embolism
• Predisposing conditions
– Prolonged bed rest
– Long periods of travel
– Pregnancy
– Use of oral contraceptives
– Carcinoma
– Obesity

Pulmonary Vascular Disease –
Pulmonary Embolism
• Pathophysiology
– Sudden obstruction of a pulmonary arterial branch
– Decrease or total cessation in blood flow to the distal area of
the lung
– Increase in alveolar dead space
– Compensatory increase in total ventilation
– Sensation of dyspnea

Pulmonary Vascular Disease –
Pulmonary Embolism
• Pathophysiology
– Bronchoconstriction secondary to decrease in carbon
dioxide, regional hypoxia, and production of serotonin and
histamines
– Mismatch of ventilation and perfusion
– Decrease in production of surfactant in the affected area
– Atelectasis and intrapulmonary shunt
– May lead to cardiogenic shock and death

Pulmonary Vascular Disease –
Pulmonary Embolism
• Pathophysiology
– Extent of hemodynamic changes determined by degree of
pulmonary vasculature involved
• Small involvement of pulmonary vasculature has no
significant consequences.
• 50% involvement of vascular bed leads to pulmonary
hypertension
Pulmonary Vascular Disease –
Pulmonary Embolism
• Radiologic Findings (difficult to see on CXR)
– Enlargement of right descending pulmonary artery
– Elevation of diaphragm
– Enlargement of heart shadow
– Pleural effusion
– Pulmonary angiogram is diagnostic

Pulmonary Embolism
Diagnosis
• Diagnosis based on history, sudden dyspnea
• Example: post surgical patient with prolonged bedrest
who suddenly develops SOB/hypoxemia without other
obvious reasons.
• CT scan, VQ scans
• Coagulation studies (PTT – Partial Thromboplastin Time
– blood tests to determine how quickly your blood clots)

VQ scan
• A ventilation/perfusion lung scan, also called a V/Q
lung scan, is a type of medical imaging using
scintigraphy and medical isotopes to evaluate the
circulation of air and blood within a patient's lungs; in
order to determine the ventilation/perfusion ratio. The
ventilation part of the test looks at the ability of air to
reach all parts of the lungs, while the perfusion part
evaluates how well blood circulates within the lungs
– Scintigrahy – a diagnostic technique in which a two-dimensional
picture of internal body tissue is produced through the detection of
radiation emitted by a radioactive substance administered in the
body.


partial thromboplastin time
• partial thromboplastin time (PTT) or activated partial
thromboplastin time (aPTT or APTT) is a performance
indicator for detecting abnormalities in blood clotting, it
is also used to monitor the treatment effects with
heparin, a major anticoagulant. It is used in conjunction
with the prothrombin time (PT)

Pulmonary Vascular Disease –
Pulmonary Embolism
• Clinical Findings
– Sudden onset of dyspnea (ABG will show normal CO2, but
low PaO2)
– Pleuritic chest pain
– Cough
– Sensation of apprehension
– Swelling of extremities

Pulmonary Vascular Disease –
Pulmonary Embolism
• Clinical Findings
– Hemoptysis in small percentage of patients
– Tachypnea
– Inspiratory fine crackles on auscultation
– Tachycardia

Pulmonary Vascular Disease –
Pulmonary Embolism
• Clinical Findings
• ETCO2 values will show sudden decrease in
measurement from V/Q mismatch
• Treatment:
– anticoagulants (Heparin, Lovenox), oxygen, CPAP,
thrombolectomy

Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
– Idiopathic Pulmonary Hypertension
• More common among women than men (3:1 Ratio)
• More common from ages 20 to 50
• Often misdiagnosed
Pulmonary Hypertension
• increase in blood pressure in the pulmonary artery,
pulmonary vein, or pulmonary capillaries, together
known as the lung vasculature, leading to shortness of
breath, dizziness, fainting, and other symptoms, all of
which are exacerbated by exertion. Pulmonary
hypertension can be a severe disease with a markedly
decreased exercise tolerance and heart failure
• Pulmonary Hypertension
• A Patient's Story

Pulmonary Hypertension

Pulmonary Vascular Disease –
Idiopathic Pulmonary Arterial
Hypertension (IPAH)
• Mean pulmonary artery
pressure greater than 25
mmHg at rest of 30
mmHg during exercise
with increased pulmonary
vascular resistance and
normal left heart
ventricular function
Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
• Etiology
– Chronic obstructive pulmonary disease
– Congenital heart disease
– Collagen vascular disease
– Cirrhosis of the liver
– Viral infections (HIV)
– Drugs
Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
• Pathophysiology
– COPD
• Loss of vascular surface caused by destruction of lung parenchyma
• Compression of the pulmonary vascular bed secondary to hyperinflation
• Increased viscosity of the blood secondary to polycythemia
• Left ventricular dysfunction

Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
• Pathophysiology
– Idiopathic pulmonary arterial hypertension
• Initial insult to pulmonary endothelium in probable
presence of genetic predisposition
• Alteration in balance between vasoconstrictive mediators
and vasodilators
• Possible reduction in potassium channels results in
depolarization of the cellular membrane and elevation of
calcium level, causing pulmonary vasoconstriction
Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
• Radiologic Findings
– Enlargement of the main and hilar pulmonary arteries
– Narrowing (pruning) of peripheral arteries
– Right ventricular enlargement

Pulmonary Hypertension

MPA= remarkably
prominent main pulmonary
artery segment (MPA),
which appears to be
aneurysmally dilated.
Right pulmonary artery
(RPA) is also enlarged.
This X-ray also shows a
prominent right atrial
contour, indicating right
atrial dilatation as a
consequence of
pulmonary hypertension
and right ventricular
hypertrophy

EKG
• In pulmonary hypertension, the electrocardiogram
(ECG) may demonstrate signs of right ventricular
hypertrophy, such as tall right precordial R waves, right
axis deviation and right ventricular strain
• The higher the pulmonary artery pressure, the more
sensitive is the ECG.

Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension
• Clinical Findings
– Dyspnea
– Angina secondary to underperfusion of right ventricle or
stretching of large pulmonary arteries (approximately 50% of
the time)
– Cough
– Hemoptysis
– Raynaud’s Phenomenon: blanching of the fingers on
exposure to cold
– Palpable right ventricular heave
– Cyanosis

Pulmonary Vascular Disease –
Pulmonary Arterial Hypertension

Treatments
Correct underlying cause:
Surgical treatment of mitral stenosis, left to
right shunt or accessible chronic
thromboemboli
Afterload reduction, digoxin (Lanoxin) and
diuretics for left ventricular dysfunction
Prevention and treatment of respiratory
infection
Decrease pulmonary vascular resistance:
Vasodilators
Oxygen
Nitric Oxide Calcium channel blockers such as diltiazem
(Cardizem) or nifedipine (Procardia)
Prostacyclin (epoprostenol [Flolan]) or
prostacyclin analogs

Treatments
Anticoagulants for primary pulmonary hypertension and chronic thromboembolism
Increase cardiac output:
Short-term parenteral inotropes
Digoxin
Reduce volume overload:
Low-salt diet
Diuretics
Perform lung transplantation or atrial septosotomy (investigational)

Neuromuscular Disorders

Amyotrophic Lateral Sclerosis
• Amyotrophic Lateral Sclerosis (ALS) or Lou Gehrig
Disease
– Neuromuscular disorder characterized by progressive
degeneration of upper and lower motor neurons leading to
loss of skeletal muscle strength, including the respiratory
muscles
– Lou Gehrig's Disease
– The True Horrors of Lou Gehrig's Disease

Amyotrophic Lateral Sclerosis
• Etiology
– Heredity – 8 to 10% of cases are familial
– More common in males than females (2:1)
– Most common in ages 40 – 60
– 1 - 2 persons/100,000 in the U.S.
– Prognosis is poor

Amyotrophic Lateral Sclerosis
• Etiology
– Exact etiology unknown
• Genetic mutation present in 10 – 15% of patients
increases the susceptibility of neurons to oxidative stress
• Possible links to pesticides and other neurotoxic
chemicals
Neurotoxins alter the function of the nervous system by damaging brain
cells or nerves that carry signals to the body.

Amyotrophic Lateral Sclerosis
• Etiology
• Susceptibility to glutamate-induced neurotoxicity –
glutamate is the principal excitatory brain
neurotransmitter; decrease in uptake of glutamate may
lead to overstimulation of glutamate receptors leading to
increased intracellular calcium, triggering production of a
proteolytic enzymes causing cell membrane injury
Amyotrophic Lateral Sclerosis
• Pathophysiology
– Progressive death of both upper and lower motor neurons in
the motor cortex of the brain, the brain stem, and the spinal
cord
– Begins usually with weakness of large muscle groups or the
bulbar muscles (those supplied by nerves in the upper spinal
cord, such as those controlling swallowing and speaking)
Amyotrophic Lateral Sclerosis
• Pulmonary Function Findings
– Progressive decrease in FVC
– Decreased MVV
– Increase in RV
– Decrease in NIF

Amyotrophic Lateral Sclerosis
• Pulmonary Function Findings
– Will require ventilatory assistance when criteria are met
• PaCO2 > 45 mmHg
• VC < 20 ml/kg
• NIF < -20mmHg
• VT < 5 ml/kg

Amyotrophic Lateral Sclerosis
• Clinical Findings
– Progressive weakness of distal extremities
– If early involvement of phrenic nerve, then nocturnal
hypoventilation followed by acute respiratory failure
– Progressive deterioration of pulmonary function results
– Difficulty in swallowing
– Difficulty in speech
– Prognosis is poor with 80% mortality within five years of
diagnosis

ALS diagnosis
• No test can provide a definite diagnosis of ALS, although the presence of
upper and lower motor neuron signs in a single limb is strongly suggestive.
Instead, the diagnosis of ALS is primarily based on the symptoms and signs
the physician observes in the patient and a series of tests to rule out other
diseases. Physicians obtain the patient's full medical history and usually
conduct a neurologic examination at regular intervals to assess whether
symptoms such as muscle weakness, atrophy of muscles, hyperreflexia, and
spasticity are getting progressively worse.
• MRI demonstrates increased T2 signal within the posterior part of the internal
capsule, consistent with the clinical diagnosis of ALS.
• Because symptoms of ALS can be similar to those of a wide variety of other,
more treatable diseases or disorders, appropriate tests must be conducted to
exclude the possibility of other conditions. One of these tests is
electromyography (EMG), a special recording technique that detects electrical
activity in muscles
ALS treatment
• Slowing progression of disease, no cure exist
• RT treatment: bronchial hygiene, trachestomy,
continuous mechanical ventilation

Neuromuscular Disorders - Guillain-
Barre Syndrome
• is an acute polyneuropathy, a disorder affecting the
peripheral nervous system. Ascending paralysis,
weakness beginning in the feet and hands and
migrating towards the trunk, is the most typical
symptom, and some subtypes cause change in
sensation or pain as well as dysfunction of the
autonomic nervous system. It can cause life-threatening
complications, in particular if the breathing muscles are
affected or if there is autonomic nervous system
involvement. The disease is usually triggered by an
infection.
• Holly's Journey
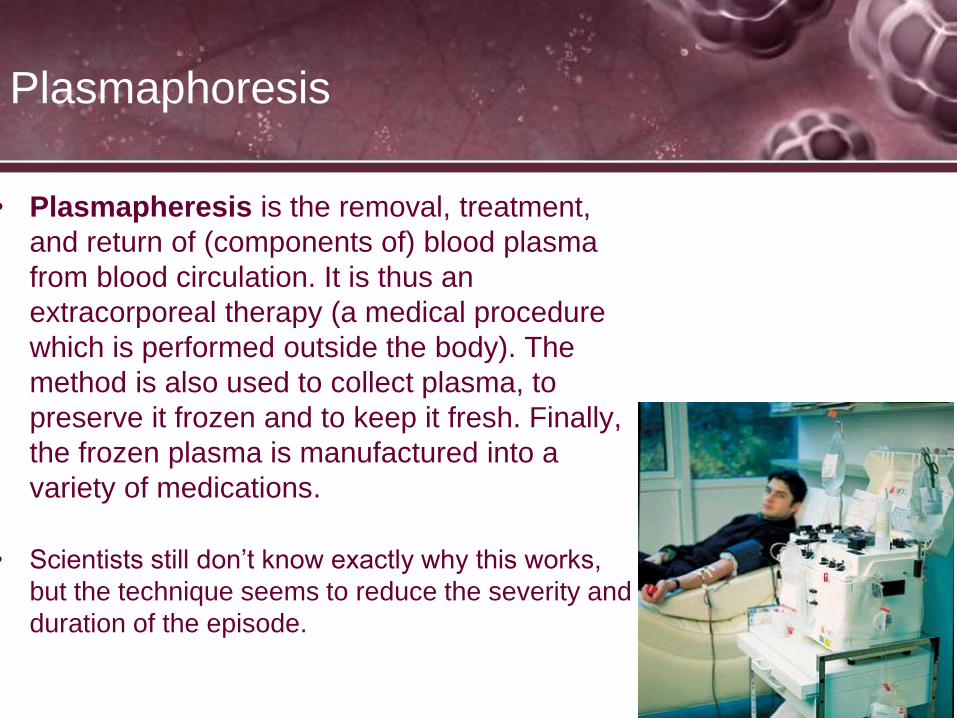
Plasmaphoresis
• Plasmapheresis is the removal, treatment,
and return of (components of) blood plasma
from blood circulation. It is thus an
extracorporeal therapy (a medical procedure
which is performed outside the body). The
method is also used to collect plasma, to
preserve it frozen and to keep it fresh. Finally,
the frozen plasma is manufactured into a
variety of medications.
• Scientists still don’t know exactly why this works,
but the technique seems to reduce the severity and
duration of the episode.

GB
• Polyneuropathy is a neurological disorder that occurs
when many nerves throughout the body malfunction
simultaneously.
• The diagnosis is usually made by nerve conduction
studies and with studies of the cerebrospinal fluid. With
prompt treatment by intravenous immunoglobulins or
plasmapheresis, together with supportive care, the
majority will recover completely. Guillain–Barré
syndrome is rare, at 1–2 cases per 100,000 people
annually, but is the most common cause of acute non-
trauma-related paralysis in the world.
Neuromuscular Disorders - Guillain-
Barre Syndrome
• Most common peripheral neuropathy causing
respiratory deficiency; characterized by paralysis and
hyporeflexia with or without sensory symptoms
• Affects 1 – 2/100,000
• All ages and genders affected

Neuromuscular Disorders - Guillain-
Barre Syndrome
Guillain-Barre Syndrome
• Etiology
– Believed to be caused by an autoimmune defect that
destroys the myelin sheath of the neuron
– Patient may have had a history of upper respiratory infection
or flu-like illness preceding onset of symptoms
– The Epstein-Barr virus may be implicated
EBV is a common human virus that causes infectious mononucleosis and
plays a role in emergence of two rare forms of cancer – Burkit’ts lymphoma
and nasopharyngeal carcinoma.

Guillain-Barre Syndrome
• Pathophysiology
– Progressive loss of myelin sheath
– Paralysis usually begins in lower extremities with or without
dysesthesia (abnormal sensations from damaged nerves)
– Progresses upward over hours or days to arms and facial
muscles
– Lower cranial nerves may be affected, leading to drooling,
difficulty swallowing, and/or maintaining an open airway

Guillain-Barre Syndrome
• Pathophysiology
– 30% of patients require ventilatory support
– Generally, spontaneously resolves, though sometimes with
sequelae – the condition that is the consequence of a previous disease
or injury.
– Mortality range of 3 to 6%.

Guillain-Barre Syndrome
• Clinical Findings
– Ascending symmetrical muscle weakness or paralysis
– Drooling
– Difficulty in speech
– Decreased vital capacity
– Respiratory failure
GB
• RT treatment trach and bronchial hygiene
• Mechanical ventilation
• Plasmapheresis
• Protein therapy
Myasthenia gravis
• Myasthenia gravis is a chronic autoimmune neuromuscular disease
characterized by varying degrees of weakness of the skeletal
(voluntary) muscles of the body. The name myasthenia gravis, which
is Latin and Greek in origin, literally means "grave muscle weakness."
With current therapies, however, most cases of myasthenia gravis are
not as "grave" as the name implies. In fact, most individuals with
myasthenia gravis have a normal life expectancy.
• The hallmark of myasthenia gravis is muscle weakness that increases
during periods of activity and improves after periods of rest. Certain
muscles such as those that control eye and eyelid movement, facial
expression, chewing, talking, and swallowing are often, but not
always, involved in the disorder. The muscles that control breathing
and neck and limb movements may also be affected.
• MG Information

Neuromuscular Disorders -
Myasthenia Gravis
• A chronic autoimmune disorder of the neuromuscular
junction characterized by fatigue and weakness, with
improvement following rest
• Sensory function is not lost
• Loss of strength may be confined to an isolated group of
muscles or as a generalized weakness
• Affects 20,000 – 70,000 people in the U.S. annually
• Peak age of onset: females 15-35 yrs, males 40-70yrs


Neuromuscular Disorders -
Myasthenia Gravis

Neuromuscular Disorders -
Myasthenia Gravis
• Etiology
– Thymic tumors are present in 10% of patients
– Antibodies to acetylcholine receptors is seen in 80% of
patients

Causes
• Myasthenia gravis is caused by a defect in the transmission of nerve
impulses to muscles. It occurs when normal communication between
the nerve and muscle is interrupted at the neuromuscular junction—
the place where nerve cells connect with the muscles they control.
Normally when impulses travel down the nerve, the nerve endings
release a neurotransmitter substance called acetylcholine.
Acetylcholine travels from the neuromuscular junction and binds to
acetylcholine receptors which are activated and generate a muscle
contraction.
• In myasthenia gravis, antibodies block, alter, or destroy the receptors
for acetylcholine at the neuromuscular junction, which prevents the
muscle contraction from occurring. These antibodies are produced by
the body's own immune system. Myasthenia gravis is an autoimmune
disease because the immune system—which normally protects the
body from foreign organisms—mistakenly attacks itself.

Neuromuscular Disorders -
Myasthenia Gravis
• Pathophysiology
– Normally acetylcholine is stored in pre-synaptic vesicles. it
is released into the synaptic space and binds to the receptor
on the post-synaptic membrane, depolarizing the nerve and
leading to contraction of the muscle
– Binding of cholinesterase to the acetylcholine receptors
blocks the impulse of the nerve, preventing muscle
contraction

Neuromuscular Disorders -
Myasthenia Gravis
• Clinical Findings
– Intermittent weakness of voluntary muscles
– Respiratory symptoms dependent upon severity of disease
• Upper airway obstruction due to muscle weakness
• Dyspnea on exertion
• Ventilatory failure in severe cases
• Decrease in VC, TLC, IRC, and ERV
• Most deaths occur secondary to pulmonary infections

Symptoms
• Although myasthenia gravis may affect any voluntary muscle, muscles that
control eye and eyelid movement, facial expression, and swallowing are most
frequently affected. The onset of the disorder may be sudden and symptoms
often are not immediately recognized as myasthenia gravis.
• In most cases, the first noticeable symptom is weakness of the eye muscles.
In others, difficulty in swallowing and slurred speech may be the first signs.
The degree of muscle weakness involved in myasthenia gravis varies greatly
among individuals, ranging from a localized form limited to eye muscles
(ocular myasthenia), to a severe or generalized form in which many
muscles—sometimes including those that control breathing—are affected.
Symptoms, which vary in type and severity, may include a drooping of one or
both eyelids (ptosis), blurred or double vision (diplopia) due to weakness of
the muscles that control eye movements, unstable or waddling gait, a change
in facial expression, difficulty in swallowing, shortness of breath, impaired
speech (dysarthria), and weakness is the arms, hands, fingers, legs, and
neck.

Diagnosis
• Because weakness is a common symptom of many other disorders, the
diagnosis of myasthenia gravis is often missed or delayed (sometimes up to
two years) in people who experience mild weakness or in those individuals
whose weakness is restricted to only a few muscles.
• The first steps of diagnosing myasthenia gravis include a review of the
individual's medical history, and physical and neurological examinations. The
physician looks for impairment of eye movements or muscle weakness
without any changes in the individual's ability to feel things. If the doctor
suspects myasthenia gravis, several tests are available to confirm the
diagnosis.
• A special blood test can detect the presence of immune molecules or
acetylcholine receptor antibodies. Most patients with myasthenia gravis have
abnormally elevated levels of these antibodies. Recently, a second antibody—
called the anti-MuSK antibody—has been found in about 30 to 40 percent of
individuals with myasthenia gravis who do not have acetylcholine receptor
antibodies. This antibody can also be tested for in the blood. However, neither
of these antibodies is present in some individuals with myasthenia gravis,
most often in those with ocular myasthenia gravis.
Diagnosis
• The edrophonium test uses intravenous administration of edrophonium
chloride to very briefly relieve weakness in people with myasthenia gravis.
The drug blocks the degradation (breakdown) of acetylcholine and temporarily
increases the levels of acetylcholine at the neuromuscular junction. Other
methods to confirm the diagnosis include a version of nerve conduction study
which tests for specific muscle "fatigue" by repetitive nerve stimulation. This
test records weakening muscle responses when the nerves are repetitively
stimulated by small pulses of electricity. Repetitive stimulation of a nerve
during a nerve conduction study may demonstrate gradual decreases of the
muscle action potential due to impaired nerve-to-muscle transmission.
• Single fiber electromyography (EMG) can also detect impaired nerve-to-
muscle transmission. EMG measures the electrical potential of muscle cells
when single muscle fibers are stimulated by electrical impulses. Muscle fibers
in myasthenia gravis, as well as other neuromuscular disorders, do not
respond as well to repeated electrical stimulation compared to muscles from
normal individuals.

Tests and Treatments for Myasthenia
Gravis
• Tensilon Test – Endophonium (Tensilon) may result in a
sudden, although temporary improvement in muscle
strength. This tests helps to diagnose the muscle
disorder MG.
• Treatments
Medicines:
Anticholinesterase (improves strength and energy)
Immunosuppressives – Steroids
Plasmastheresis
Thyrectomy - Thyamus removal
Pulmonary Pathophysiology