Treatment of radioactive iodine-refractory metastatic differentiated thyroid carcinoma

Postoperative Surveillance of
Differentiated Thyroid
Carcinoma
Mitchell E. Tublin, M.D.
Vice Chair & Professor of Radiology
Section Chief: Abdominal Imaging
University of Pittsburgh
School of Medicine

Postoperative Surveillance of
DTC….and some observations
from a recovering cynic
Mitchell E. Tublin, M.D.
Vice Chair & Professor of Radiology
Section Chief: Abdominal Imaging
University of Pittsburgh
School of Medicine

Thyroid carcinoma: “epidemic”
• 2014 ACS estimate:
– 63K new cases (2009: 37K)
– 1,890 deaths, 0.3% of all cancer deaths (CA Cancer J Clin, 2014, Cancer Statistics, 2014)
• Majority are differentiated thyroid carcinoma
– Papillary cancer 80%
– Follicular cancer 11%
• Most slow growing and respond to tx

Thyroid carcinoma: recurrence basics
• Typically indolent tumor
• 5 year survival rate: 97.3%
• Tumor may present decades after initial presentation
• ↑ risk of recurrence, mortality if > 45, advanced tumor at initial presentation

Differentiated thyroid cancer
• Surveillance approaches for DTC rapidly
evolving in context of recent thyroid
carcinoma “epidemic”, improvements in
imaging, and molecular diagnostics
• ATA guidelines: 2006, 2009, 2015

Sono surveillance of DTC: My
world view
• I’m a sono advocate, I like scanning but I’m a
natural cynic
• Use of sono as primary modality for detection of
regional recurrence highlighted in recent (non-
radiology) literature
• Central role in 2015 ATA guidelines
• Imaging has outpaced understanding of biology
• Intervention often patient (and RVU) driven

DTC Surveillance:
controversies
• Which modality and when (it’s
still not all ultrasound…..)
• What criteria
• How report
• Should we care?
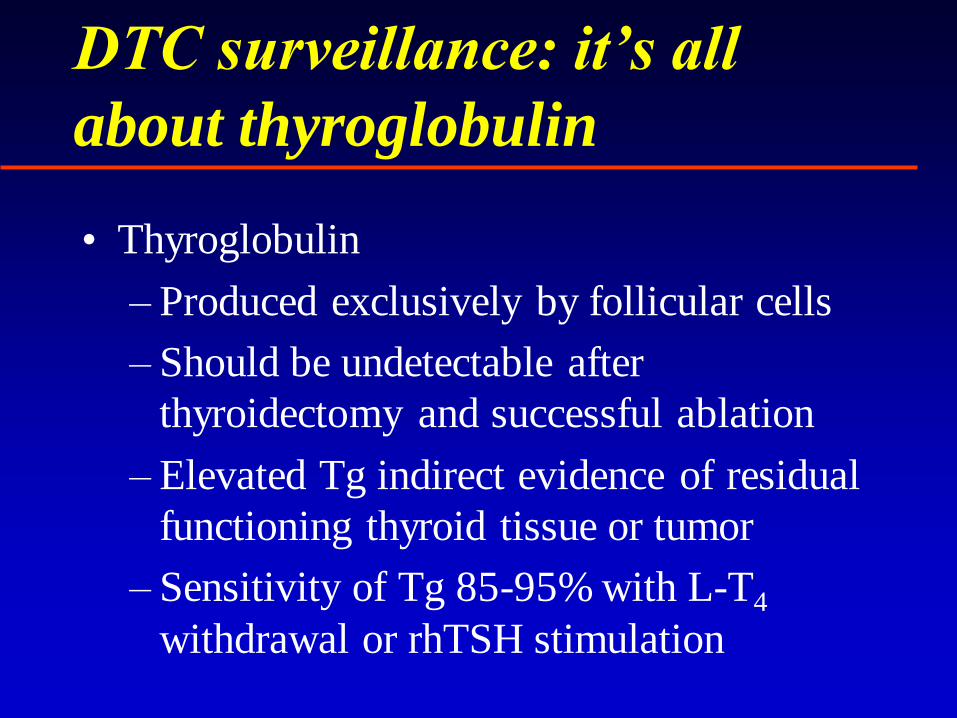
DTC surveillance: it’s all
about thyroglobulin
• Thyroglobulin
– Produced exclusively by follicular cells
– Should be undetectable after
thyroidectomy and successful ablation
– Elevated Tg indirect evidence of residual
functioning thyroid tissue or tumor
– Sensitivity of Tg 85-95% with L-T4
withdrawal or rhTSH stimulation

Thyroglobulin
• Very high negative predictive value
• False negatives may occur:
–Anti Tg Ab
–Absent or abnormal Tg production
by dedifferentiated metastases

131 (123)I Whole Body Scan
• Traditional strategy:
– Surveillance 131I whole body scan and
serum Tg post thyroidectomy and
ablation
• WBS utility discounted in 2009, 2015 ATA
guidelines
• Limited additional benefit if stimulated
thyroglobulin undetectable (and sono - )
Pacini, J Clin Endo & Metab, 2002

131 I Whole Body Scan
• 2009/2015 ATA guidelines
– Surveillance WBS not advocated for low
risk pts (no locoregional dz, favorable
histology) with neg Tg/sono
– Surveillance Dx WBS (1123 or low dose
I132) may be useful for intermediate or
high risk pts

131 I Whole Body Scan
• Still used if TG +, cervical US –
• With elevated Tg, 131I WBS localizes
recurrence in:
– 50 – 60% papillary carcinoma
– 64 – 67% follicular carcinoma
• Anatomic detail limited

131 I Whole Body Scan
• Potential causes for false negative WBS
– Insufficient TSH stimulation
– Iodine contamination
– Low volume tumor
– Dedifferentiated tumor
• Absence of 131I uptake in metastatic disease
may be a predictor of poor outcome

Fluorine-18-fluorodeoxyglucose
(FDG) PET
• Long accepted utility in Tg positive, WBS negthyroid cancer
– Sensitivity 60 - 94%
– Specificity 25 – 90%
• Recommended threshold Tg > 10 µg/L
• Increased FDG uptake and loss of 131I uptake may reflect dedifferentiation and more aggressive tumor (flip-flop phenomenon)
• Limited spatial resolution
• False positives (physiologic activity, inflammation)

Combined CT-PET
• Advantages
– Spatial localization
– Increased specificity (physiologic uptake)
• ATA 2015: FDG-PET / CT-PET synonymous
• Potential indications beyond Tg +, WBS – dz
– Initial staging & f/u of high risk pts with poorly differentiated dz
– Selection tool for pts unlikely to respond to 131I ablation

PET-CT Study Patients Sensitivity Specificity
Nahas et al. 33 66% 100%
Palmedo et al. 40 95% 91%
Iagaru et al. 76 88.6 89.3
Finkelstein et al. 65 98% 81%
Shammas et al. 61 68.4% 82.4%
Kim et al. 20 90%
Freudenberg et al. 36 96% 100%
UPitt (Ferris) 123 82.1% 89.7%
CT-PET: Literature

Thyroid cancerCT: 160 mAs; 130 KVp; pitch 1.6; 5 mm slices PET: 7 mCi FDG; 3 x 10 min; 3.4 mm slices
78 year-old male. Thyroid cancer
in 1993. Elevated thyroglobulin.
Negative 131I study. Four lesions identified on PET/CT
PET/CT scannerUniversity of Pittsburgh
131I scan

Thyroid cancer surveillance
• CT
– Useful for distant (lung) metastases
– Limited role for regional recurrence
• Size only useful criteria for nodal dz
• Anatomy may be obscured without IV contrast
• MRI
– Local dz, FSE T2, neck coil
– 1cm size threshold, high T2 signal (n = 26)
• Sensitivity 95% Specificity 51%
• PPV 84% NPV 78% Accuracy 83%
– Interobserver variability
Gross, Laryngoscope, 2001
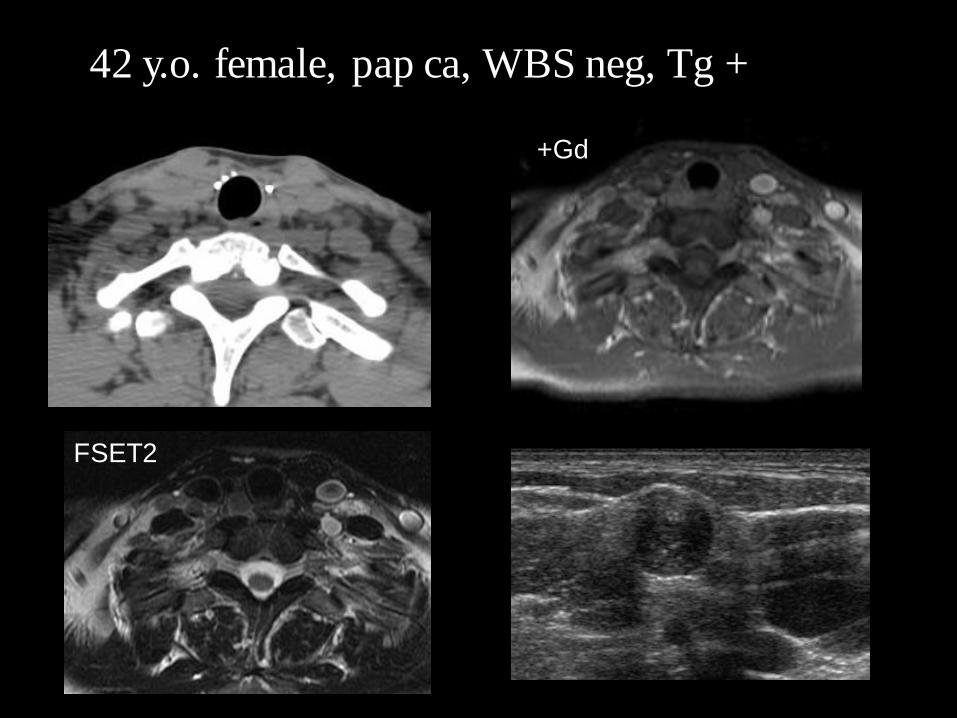
42 y.o. female, pap ca, WBS neg, Tg +
FSET2
+Gd

Ultrasound
• Premier modality for thyroid imaging,
nodule identification, characterization (?)
and bx
• Optimum technique critical for imaging of
local-regional recurrence
– High frequency probe (10-14 MHz)
– Compound imagining
• Operative hx, zone classification
• Physician scanning crucial

Som, Curtin, Mancuso. Arch Otolaryngol-
Head Neck Surg, 1999

Ultrasound
• Combination of rhTSH-stimulated Tg and sonography most sensitive for monitoring differentiated thyroid ca regional recurrence in recent large series (n = 340)
Sens Spec
Sono 70 97.5131I WBS 20 100
Stim Tg 78.2 100
Sono/Tg 96.2 100
Pacini, J Clin Endocrinol Metab, 2003


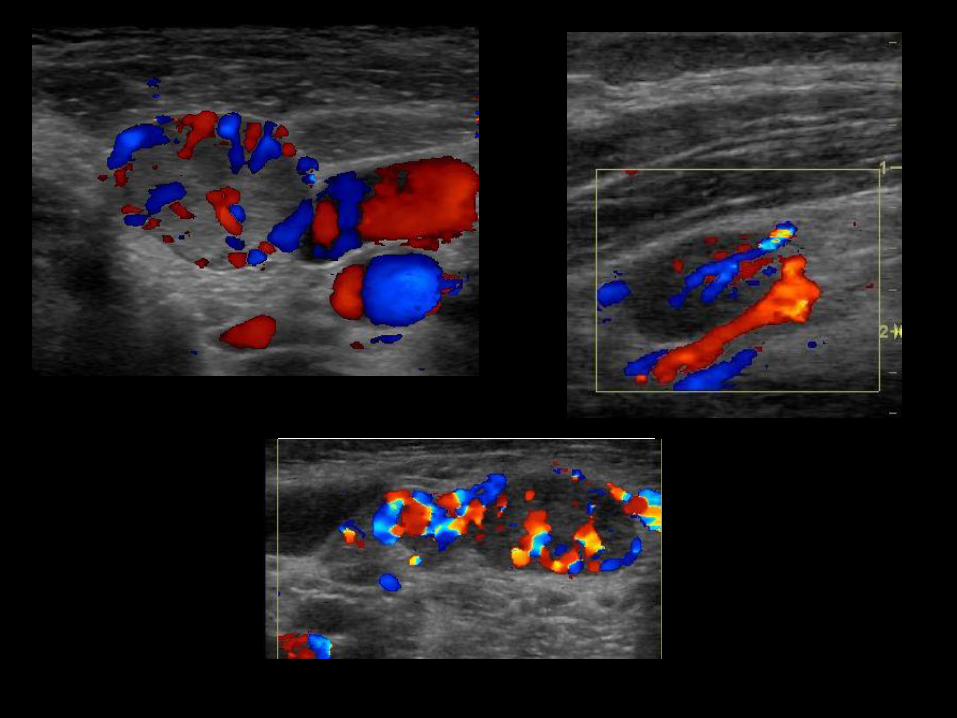
Ultrasound: Lymph node
diagnositc criteria
• Grey scale
– Size
– Shape
– Internal architecture
• Color (power) Doppler
– Vascularity
– Pattern

Grey scale: malignant cervical
lymph nodes
• Size
– “large” (threshold dependent upon station)
• Short axis measurement
– Increased specificity with ↑ threshold
– ROC thresholds: 5mm (submental) → 9mm (submand)
Ying, JIUM,1998
• Clustering
• Shape
– Round (short axis/long axis ratio > .5)

Grey scale: malignant cervical
lymph nodes
• Internal architecture
– Hypoechoic
– Effaced echogenic hilum
• Unique features of papillary carcinoma
– Cystic
– Microcalcifications

41 y.o. female: “branchial
cleft cyst” at OSH
Metastatic papillary
carcinoma

Doppler: malignant cervical
lymph nodes
• Vascular pattern
– Capsular vessels
– “Low” resistive index (<.8)
– Issues
• Operator, parameter, dependent
• Interobserver variability
• Overlap

Non
necrotizing
granulomas
Suture
granulomas
Mimics

Mimics
Thoracic Duct Gel Foam
IJ
SC

Ultrasound: Lymph node
diagnostic criteria
• Combination of criteria improves sensitivity/specificity
– Ability of sono to depict internal grey scale and Doppler architecture increases accuracy relative to CT
– Comparison of sono and CT for differentiation of malignant and benign cervical lymph nodes in H/N SCCA (n = 62)
Sensitivity Specificity
CT .68 .82
Sono/doppler .78 .96Sumi, AJR 2001
• Ultrasound guided FNAC still crucial

Ultrasound: ATA 2015 triage
(recommendation # 65)
• Cervical ultrasound q 6-12 mos, and then “periodically” depending on Tgand risk level
• FNA of suspicious nodes > 8-10 mm short axis
• Tg aspirate recommended to ↑ yield
• “Cervical metastases may occasionally be detected at neck US even with undetectable Tg” (ATA 2009)

CS 211666020
• 28 y.o. female, total thyroidectomy, selective
bilateral neck dissection for multifocal, node
positive pap ca
• Completion ablation, right neck dissection 4/02
for recurrence
• Tg 226, neg WBS 8/02, 131I tx
• 2/03 Tg 73.5 / 10/03 Tg 100.5
• WBS neg, CT/PET: small left supraclav node,
mild thymic FDG uptake
• Ultrasound performed prior to resection

L4
L6

SM 163526819
• 30 y.o female, s/p thyroidectomy for tall cell variant papillary carcinoma 3 yrs prior
• 131I ablation x 2
• rhTSH 151
• WBS neg
• CT/PET
– 2 subcm right paratracheal nodules
– Diffuse left paratracheal uptake ? brown fat. “Correlation with Tg level and prior CT recommended.”

T
T
Central recurrence

R Level 6
R Level 4
Compound & SR14 MHz

MP 050446785
• 45 y.o male, post thyroidectomy, Left RND
for papillary carcinoma
• 131I ablation
• Persistent elevated Tg despite selective
node dissection WBS: mild uptake within
thyroid bed
• MRI: small left level 6 node
• Level 6 dissection (metastatic pap ca)


T
L Level 6
L4R4

“Micrometastases”

More “micrometastases”: 3 patients

Differentiated thyroid cancer
• Subclinical nodal metastases probably present
in high percentage of patients with DTC
– No value of prophylactic lymph node
dissection in 57 patients despite high
incidence (90%) of nodal metastases
– 55% of nodal metastases < 5mm (Noguchi,
Cancer, 1970)

Thyroid cancer incidence and mortality, 1973-2002
Davies, Welch, JAMA, 2006

Thyroid CA:
trends
Type
Size
Davies, Welch, JAMA, 2006

And it’s accelerating: Morris, Sikora, Tosteson, Davies. The increasing incidence of thyroid cancer:
the influence of access to care. Thyroid, Nov 2013.

Thyroid-Cancer Incidence and Related Mortality in South Korea,
1993–2011
Ahn HS et al. N Engl J Med 2014;371:1765-1767.
• 50 fold increase incidence, 1993-2011
• Most common CA dx (> 40K, 2011)
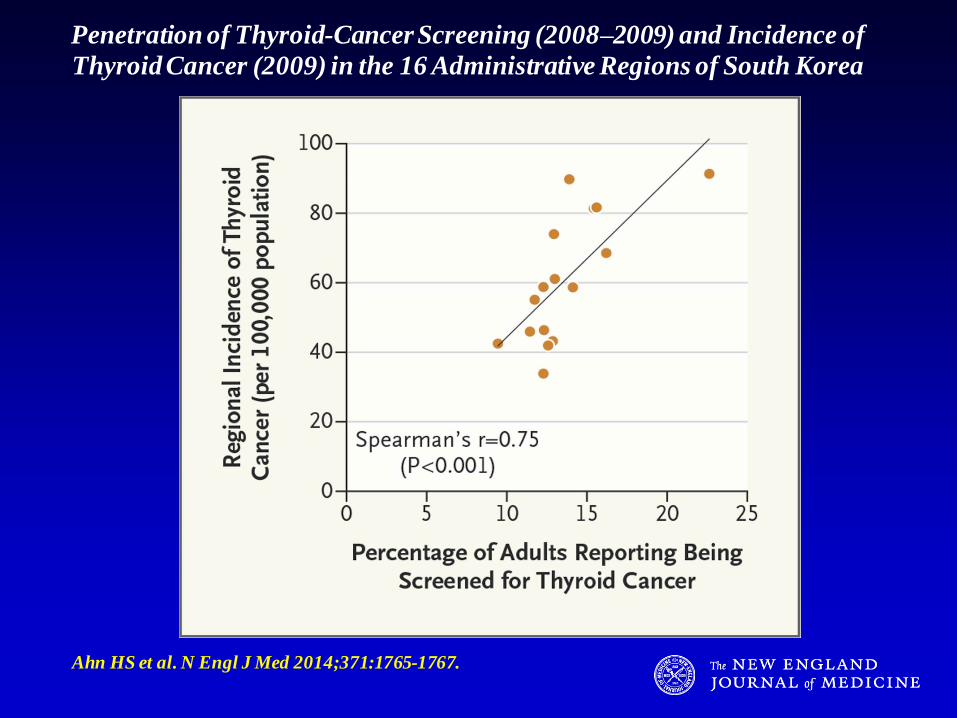
Penetration of Thyroid-Cancer Screening (2008–2009) and Incidence of
Thyroid Cancer (2009) in the 16 Administrative Regions of South Korea
Ahn HS et al. N Engl J Med 2014;371:1765-1767.
Ultrasound surveillance of DTC:
practical impact
• Increased incidence of thyroid carcinoma and improved detection of recurrent or residualdisease largely due to ultrasound
• Aggressive surveillance advocated – yearly Tg and neck ultrasound
• Repeated nodal dissections for low volume locoregional recurrence/residual often performed
– Patient anxiety
– $$$$$

Ultrasound surveillance of DTC:
practical impact
• ? Improved survival with aggressive
surveillance and tx of typically indolent tumor
• The cynic:
– “First, do no harm”
– “Don’t ask, don’t tell”
– “What you don’t know won’t hurt you”
– “Turn the machines off”
Cronan, “Thyroid Nodules: Is it time to
turn of the US machines?” Radiology,
2008

34 y.o. female: 3.6 cm tall cell variant, post
thyroidectomy/ablation, 3 yrs prior. Tg 19.
FNA: 7 mm L6 pap ca nodal recurrence.
Difficult resection despite sono localization.

The real (but unspoken) debate
Should we do any postoperative surveillance at all????
Answer: yes, but…

Ultrasound surveillance of DTC:
practical impact
• Biologic variability
• Small subset of even “nano” papillary
carcinoma may be aggressive
Kuffner : Microfoci of papillary carcinoma are
frequent and can be metastatic. Retrospective
analysis of a cohort of patients from the University
of Pittsburgh Thyroid Cancer Database

32 y.o. female, 6mm
micropapillary carcinoma.
Right neck dissection.
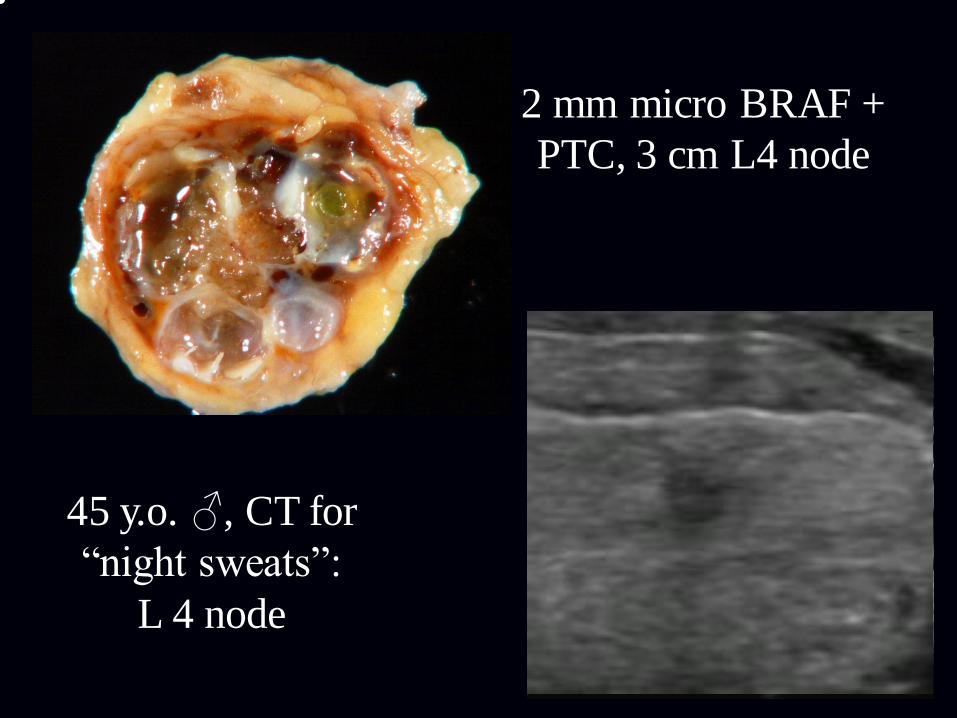
45 y.o. ♂, CT for
“night sweats”:
L 4 node
2 mm micro BRAF +
PTC, 3 cm L4 node

Surveillance of DTC: observations from a
recovering cynic
• We’re learning and adapting
• Machines still on, but improved pathology lexicon, molecular diagnostics, risk stratification, radiology/endocrinology decision trees must be making a difference
• I’m seeing it locally

UPMC Multidisciplinary Thyroid Clinic
• Paradox
• RVU centric: intervention driven
• Marketing bonanza
• Broad Western PA referral base
• Volume originally not an issue
• Stated goal: rational utilization of resources for indolent dz

UPMC Multidisciplinary Thyroid Clinic
• High volume practice early on
• A great clinical model: expertise leveraged
• Victim of our own success
• Tailored clinical pathways, built upon high impact,
collaborative research
• Volume down….a lot• 43% ↓ total FNAs since 2010 (1400 – 800)
• Clinic largely dissolved: many of original core
have left
• Radiology (me) no longer physically on site: tele-
sonography

De-escalating management of patients
with thyroid nodules and cancer
• Fewer FNAs (ATA, and increasingly ACR
TIRADS)
• Molecular diagnostics (Thryoseq 1,2,3)
• Fewer diagnostic lobectomies
• Fewer completion thyroidectomy
• More conservative staging
• Active surveillance for small PTC
• Cancer nomenclature revision
• Encapsulated follicular variant of PTC → Non-
invasive follicular thyroid neoplasm with
papillary-like nuclear features (NIFTP)

2015 ATA Risk of Structural Disease Recurrence
Low Risk
Intermediate Risk
High Risk
FTC, extensive vascular invasion (≈ 30-55%)
pT4a gross ETE (≈ 30-40%)
pN1, any LN > 3 cm (≈ 30%)
BRAF mutated, not intrathyroidal (≈ 10-40%)
PTC, vascular invasion (≈ 15-30%)
Clinical N1 (≈20%)
pN1, > 5 LN involved (≈20%)
BRAF mutated, intrathyroidal, < 4 cm (≈10%)
pT3 minor ETE (≈ 3-8%)
pN1, all LN < 0.2 cm (≈5%)
pN1, < 5 LN involved (≈5%)
Intrathyroidal 2-4 cm PTC (≈ 5%)
Multifocal PMC (≈ 4-6%)
Minimally invasive FTC (≈ 2-3%)
BRAF wild type, intrathyroidal, < 4 cm (≈ 1-2%)
BRAF mutated, intrathyroidal unifocal PMC (≈ 1%)
Intrathyroidal, encapsulated, FV-PTC (≈ 1-2%)
Unifocal PMC (≈ 1-2%)Slide courtesy of
Steven Hodak, MD

Molecular Signature
BRAF+TERT, RAS+TERT
Multiple driver mutations
(eg. NRAS and PIK3CA or TP53)
TERT
ALK fusions
NTRK1 fusions
NTRK3 fusions
BRAF V600E
RET/PTC
RAS
BRAF K601E
PAX8/PPARG
RAS-like
mutations
BRAF
V600E- like
mutations
Molecular markers for cancer risk stratification
High RiskGross extrathyroidal extension,
incomplete tumor resection, distant metastases,
or lymph node >3cm
Intermediate RiskAggressive histology, minor extrathyroidal extension,
vascular invasion,
or > 5 involved lymph nodes (0.2-3 cm)
Low RiskIntrathyroidal DTC
≤ 5 LN micrometastases (< 0.2 cm)
Risk of Structural Disease Recurrence
(In patients without structurally identifiable disease after initial therapy)
PTC, >1 cm, TERT mutated ± BRAF mutated* (>40%)
PTC, extrathyroidal, BRAF mutated* (≈ 10-40%)
Intrathyroidal PTC, < 4 cm, BRAF mutated* (≈10%)
Intrathyroidal, < 4 cm, BRAF wild type* (≈ 1-2%)
Intrathyroidal unifocal PTMC, BRAF mutated*, (≈ 1-2%)
FTC, extensive vascular invasion (≈ 30-55%)
pT4a gross ETE (≈ 30-40%)
pN1 with extranodal extension, >3 LN involved (≈ 40%)
pN1, any LN > 3 cm (≈ 30%)
PTC, vascular invasion (≈ 15-30%)
Clinical N1 (≈20%)
pN1, > 5 LN involved (≈20%)
pT3 minor ETE (≈ 3-8%)
pN1, all LN < 0.2 cm (≈5%)
pN1, ≤ 5 LN involved (≈5%)
Intrathyroidal PTC, 2-4 cm (≈ 5%)
Multifocal PMC (≈ 4-6%)
pN1 without extranodal extension, ≤ 3 LN involved (2%)
Minimally invasive FTC (≈ 2-3%)
Unifocal PMC (≈ 1-2%)
Intrathyroidal, encapsulated, FV-PTC (≈1-2%)
NIFTP (<1%)
Haugen BR et al. Thyroid. 2016, 26:1-133

❑ A distinct class of thyroid tumors:• Clonal process driven by distinct oncogenic mutations (RAS and
RAS-like gene mutations) • Non-invasive, follicular-patterned, moderately to well developed
nuclear features of PTC (nuclear score 2-3)• Highly favorable outcome (<1% risk of recurrence in 15 y)
❑ Recommended new terminology:
“Non-Invasive Follicular Thyroid neoplasm with Papillary-like nuclear features“ (NIFTP)
Nikiforov et al. JAMA Oncology 2016; 2:1023-9.


Molecular Markers Predict Cancer Risk
n=1510
1. Yip L Ann Surg 2015; 262: 519
2. Song YS Cancer 2016; 122: 1370
p<0.001
DTC, n=1510
High Risk for Recurrence2Markers of Low and
Intermediate Recurrence
Risk1
DTC, n=551
p<0.001

Bethesda III-IV
Cytology
N/A
Observation Lobectomy
Test result
Probability of Cancer or NIFTP
Tumor type, risk of recurrence
Patient management
3-4% 40-80%
NIFTP or low-risk cancer
Active surveillance
<10%
ThyroSeq GC
Positive: RAS-like
mutations,CNA, GEA
Negative: no mutations
Currently Negative:
LR mutations
NIFTP or low-risk cancer
Total thyroidor lobectomy
95-100%
Positive: BRAF-like mutations
Intermediate-risk cancer
Total thyroid+/- LND
98-100%
Positive: HR mutation
High-risk cancer
MTC, PT, Non-FCL
28% 6% 2%7%55%
2%
Nikiforov YE et al. Real world experience with ThyroSeq v3 Genomic Classifier in thyroid nodules with indeterminate
cytology: Results of testing of the first 3,734 consecutive samples. American Association of Clinical Endocrinologists
Annual meeting 2018
Patient Management Informed by Molecular Testing

2014
2016
2017
2018

Conclusions
• Increased incidence of thyroid carcinoma over
past thirty years largely due to imaging
• DTC usually indolent dz, but local recurrence or
detection of previously unrecognized tumor may
occur long after initial presentation
• TG and ultrasound currently best combination for
regional surveillance
• Sensitivity/specificity of sono improved when
multiple discriminatory criteria used; FNAC still
necessary

Conclusions
• Impact of intensive surveillance/tx difficult
to assess…but it’s probably not good
• Improvements in imaging have to now
outpaced our understanding of DTC tumor
biology
• More rational approach needed, and it will
be driven by recent advances in molecular
diagnostics (and insurers)
Surveillance of DTC: future
• New guidelines for surveillance intensity likely given better understanding of tumor biology
• Expect less surveillance ultrasound volume
• Healthy cynicism can be a good thing