
Post PCI Management 20 April 2012
129
Management of Post PCI Patient Dr Ashish Mishra MD,DNB (Cardiology), FACC Fellowship Interventional cardiology Mt Sinai Hospital USA Member American College Of Cardiology
-
Upload
ashishnarayanmishra2541 -
Category
Documents
-
view
111 -
download
1
Transcript of Post PCI Management 20 April 2012
Management of Post PCI Patient
Dr Ashish Mishra MD,DNB (Cardiology), FACC Fellowship Interventional cardiology Mt Sinai Hospital USA Member American College Of Cardiology
CHL Hospitals


Percutaneous coronary intervention (PCI)
an effective revascularization strategy for CAD since its inception in 1977.
1.2 million PCIs performed/yr US, and 45,000 per year in the UK.
India - Exact figures not available but number is increasing day by day due to widening indications
The rapid technological advances & widening
indications for PCI means that
new techniques, along with their new complications, are seen
ever more frequently.
Hence the need for regular review and updates
for clinicians involved in the care of these patients

Immediate post discharge care involves
• Detecting vascular access site complications,
• Dealing with contrast- induced complications,
• & stent thrombosis .
Long -term issues post-PCI
• detection and treatment of recurrent ischemia
• appropriate antiplatelet therapy
• arrhythmias and heart failure
• secondary prevention
•

Today our focus
Detection & T/t of Ischemia after PCI
Dual Anti platelet Therapy
How long & How much
What to do if your pt need Sx while on DAPT

CONTRAST INDUCED NEPHROPATHY
With the use of non ionic dye, this complication has become
less common .
More common in diabetics and
Pts with pre existing renal disease.
DEFINITIONS AND DEFINITIONS AND EPIDEMIOLOGYEPIDEMIOLOGY
No universally accepted definitionNo universally accepted definition Absence of other identifiable causesAbsence of other identifiable causes 25% elevation in serum creatinine25% elevation in serum creatinine Absolute increase of 0.5 mg/dl (44 Absolute increase of 0.5 mg/dl (44
μmol/L), 2 to 7 days laterμmol/L), 2 to 7 days later Adverse short- and long-term Adverse short- and long-term
outcomesoutcomes Unclear causal pathway to adverse Unclear causal pathway to adverse
cardiovascular outcomecardiovascular outcome

Contrast NephropathyContrast Nephropathy
Nonoliguric & reversibleNonoliguric & reversible SCr peaks between 2 and 5 daysSCr peaks between 2 and 5 days SCr returns to normal within 14 SCr returns to normal within 14
daysdays Requiring dialysis: 0.4%Requiring dialysis: 0.4%
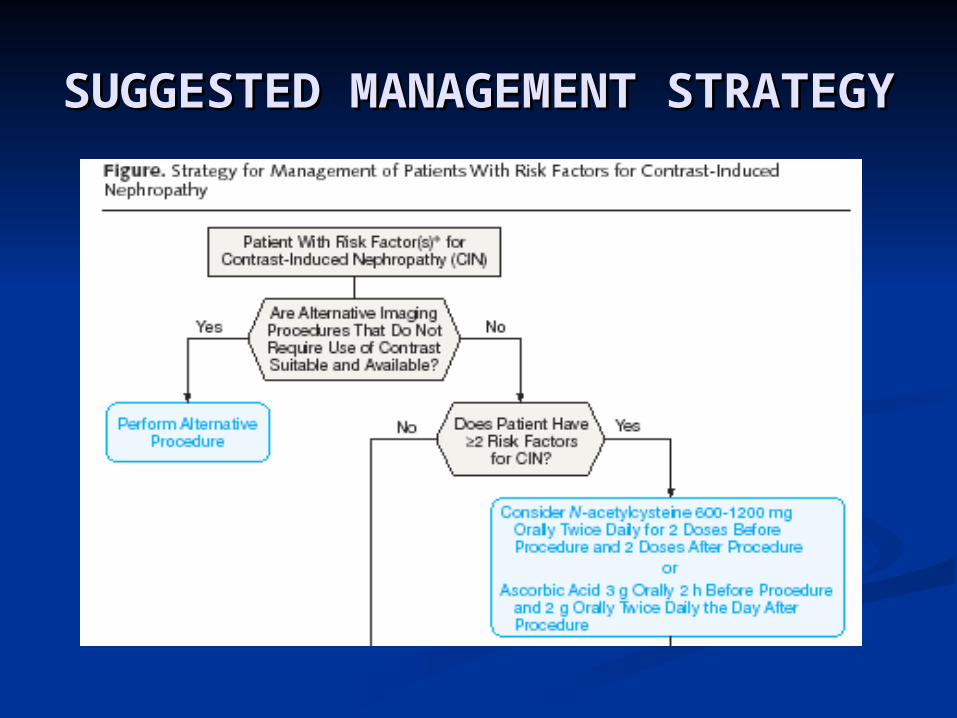
SUGGESTED MANAGEMENT STRATEGYSUGGESTED MANAGEMENT STRATEGY

Management
Recurrent ischemia post-PCI can result from
Restenosis,
Development of progressive disease in the same or a
different coronary territory, OR
Increased myocardial demand from various causes.

Clinical restenosis-
One of the major issues after PCI
With BMSs – around 20 % ( range 10-60%)
With DES – around 5-10%
occurs around 3 months post-PCI & plateaus at 12 months.
Rarely aggressive restenosis can develop sooner but rare in the first month.
Angina that recurs > 12 months post-PCI
• progressive CAD in same or different
• coronary artery
OR
• V. late stent thrombosis
rather than restenosis

Detection of restenosis
symptom status - unreliable index
25% of asymt. Pts had +VE TMT
? routine stress testing in all post-PCI pts- no data
However,
routine stress testing - advisable 6 months post-PCI in selected cases.

Which patients to test
• All the symptomatic patients
• Asymptomatic patients at high risk for future events
- pts with LVEF
- Multivessel CAD and prox LAD stenting Non compliant patients
suboptimal PCI results, Diabetes mellitus, renal failure

Which Test
ExerciseTMT- insensitive predictor of restenosis ( 50% sensitivity),
Stress testing complemented with
either stress echo or nuclear perfusion (MPI)
should be done.

`
Asymptomatic &No High risk features
Atypical chest pain orAsymptomatic withHigh risk features
Continue MaxMedical Therapy
ContinueClinical Follow Up
Normal or LowTo intermediate risk scan
Repeat stress MPI/EchoEvery 1 to 3 yearsIn absence of symptoms
High Risk Scan
CAG &FURTHER M/M
0-3 Months post PCI
Asmptomatic
Ct clinical follow upFor 3-6 months after PCI
StressEcho/MPI
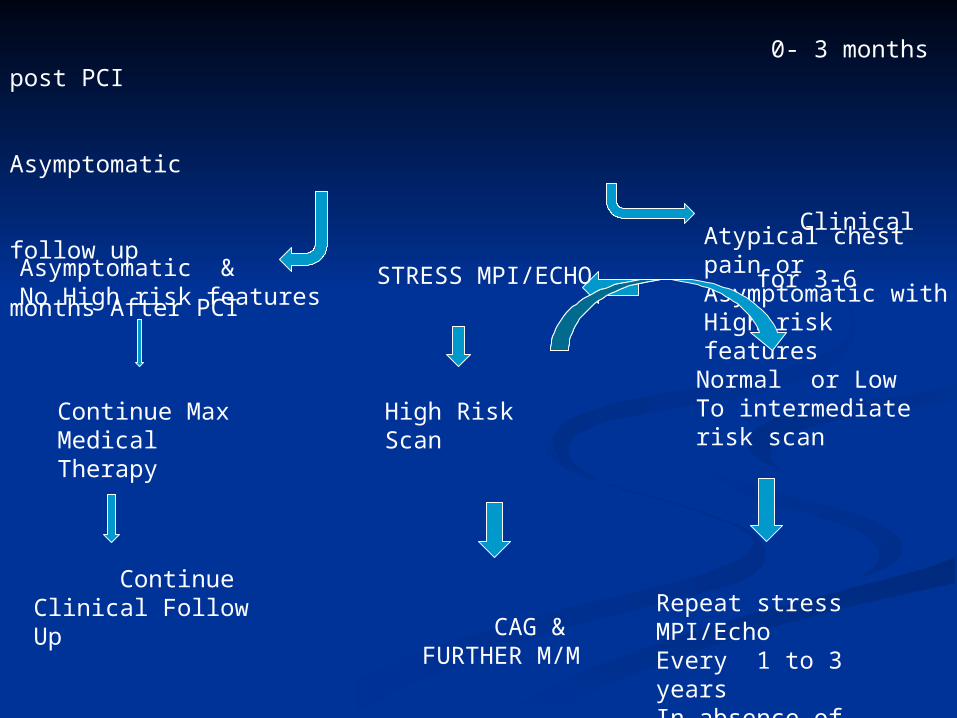
0- 3 months post PCI Asymptomatic Clinical follow up for 3-6 months After PCI `
Asymptomatic &No High risk features
Atypical chest pain orAsymptomatic withHigh risk features
Continue MaxMedical Therapy
ContinueClinical Follow Up
Normal or LowTo intermediate risk scan
Repeat stress MPI/EchoEvery 1 to 3 yearsIn absence of symptoms
High Risk Scan
CAG &FURTHER M/M
STRESS MPI/ECHO

Unchanged ST T Changes
Low Risk
Stress Echo/MPI
CAG & Further Mm
Moderate – high Risk scan
High risk
ECG s/o Acute MI
R/O Stent Thrombosis
Recurrent Angina
Acute Chest Pain ECG
Symptomatic
Post PCI
Repeat Stress Echo/MPIEvery 1 to 3 years
Normal or lowRisk scan

Post PCI
Normal or low Repeat Stress MPI/Echo every 1-3 Years
Unchanged
ST T Changes
Low Risk
Stress Echo/MPI
CAG & Further Mm
Moderate – high Risk scan
High risk
ECG s/o Acute MI
R/O Stent Thrombosis
Recurrent Angina
Acute Chest Pain
ECG
Symptomatic
• Routine follow-up angiography is indicated only in a very few
selected cases.
• patients who have received - left main coronary artery stenting where repeat angiography can be performed in 3-9 months.
• As a part of a protocol or some study
STENT THROMBOSIS
v. imp entity came into lime light because of the
concern raised by certain studies esp. with the use of DES.
has high morbidity and mortality
In one metaanalysis- 80 % presented with MI With 20% mortallty
I Lets first know certain definitions

Time frame of Time frame of ARC ARC definitions of stent definitions of stent
thrombosisthrombosis1 month 1 year
Acute≤1d
Late > 1 mo ≤ 1year
Subacute>1d - ≤1mo
Early ≤ 1 mo Very Late > 1year
0 day to 1 day Acute stent thrombosis>1 day to 1 month Subacute stent thrombosis>1 month to 1 year Late stent thrombosis
> 1 year Very late stent thrombosis
Cutlip D et al. Circulation. 2007;115:2344-2351

Patient/lesion factors in Patient/lesion factors in stent thrombosisstent thrombosis
• Premature discontinuation of dual Premature discontinuation of dual antiplateletsantiplatelets
• Low EFLow EF• DiabetesDiabetes• Renal insufficiencyRenal insufficiency• ACS ACS • Ostial and/or bifurcationOstial and/or bifurcation• In-stent restenosis lesionsIn-stent restenosis lesions• Delayed healingDelayed healing
Luscher T et al. Circulation. 2007;115:1051-1058. Holmes Jr et al. J Am Coll Cardiol. 2007;50:109-108.

Patient• Antiplatelet
noncompliance• Response variability
StentThrombosis
Adapted from Kereiakes DJ et al. Rev Cardiovasc Med. 2004;5:9-15.
Stent Thrombosis: Stent Thrombosis: A Multifactorial ProblemA Multifactorial ProblemLesion • Long lesions • Small diameter• Multivessel • Acute myocardial
infarction (AMI)• Diabetes• Bifurcations
Technical • Underexpansion• Incomplete wall
apposition• Crush technique• Overlapping
Stent • Material• Polymer matrix• Antithrombotic
agent

Mechanism of Stent Thrombosis
After BMS
complete endothelialization - by 3 - 4 months ,
hence ST occurs mostly in first 3 months & esp in first month .
In DES delayed reendothelialization( upto years) and arterial healing
compared with BMS, results in potentially thrombogenicity , hence
potential for ST, hence the need for
Prolonged DAPT, UPTO 1 year or more.

Consequences of Stent Thrombosis
60% Nonfatal MI,
, 24% Death
7% Unstable Angina

Stent Thrombosis:Stent Thrombosis:Clinical OutcomesClinical Outcomes
SESSES
(n=13)(n=13)BMSBMS
(n=15)(n=15)PESPES
(n=22)(n=22)BMS BMS
(n=18)(n=18)
Death (%)Death (%) 4 (31)4 (31) 5 (33)5 (33) 7 (32)7 (32) 5 (28)5 (28)
Myocardial Myocardial infarction (%) infarction (%) 13 (100)13 (100) 13 (87)13 (87) 17 (77)17 (77) 14 (78)14 (78)
Q-wave (%)Q-wave (%) 8 (62)8 (62) 5 (33)5 (33) 7 (32)7 (32) 5 (28)5 (28)
Non—Q-wave Non—Q-wave (%)(%) 5 (39)5 (39) 9 (60)9 (60) 10 (46)10 (46) 10 (56)10 (56)
Mauri L et al. N Engl J Med. 2007;356:1020-1029.
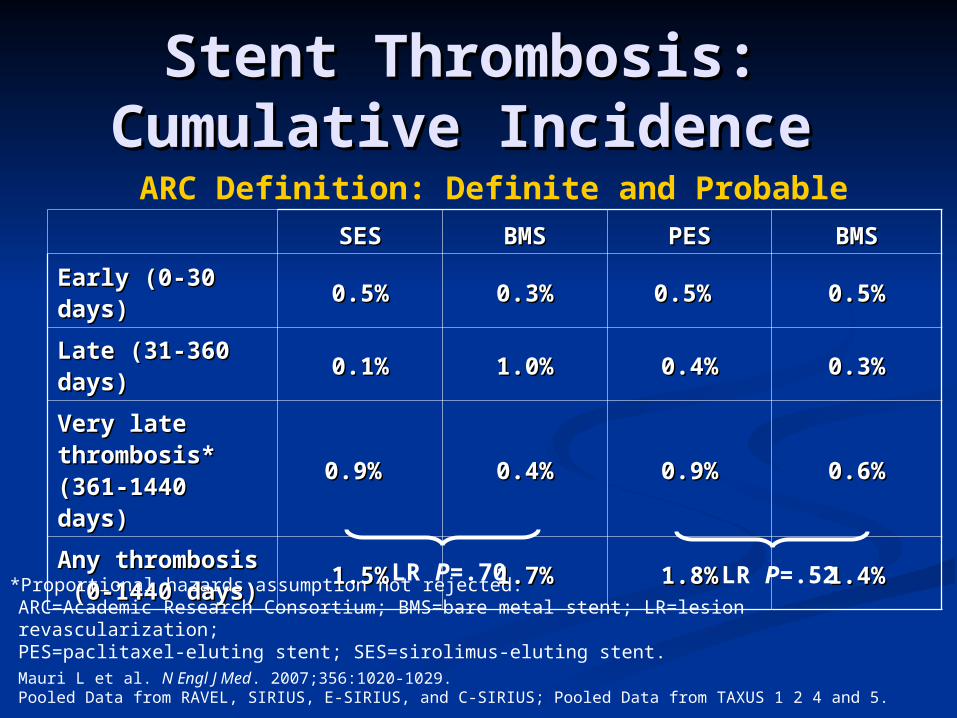
Stent Thrombosis: Stent Thrombosis: Cumulative Incidence Cumulative Incidence
SESSES BMSBMS PESPES BMSBMS
Early (0-30 Early (0-30 days)days)
0.5%0.5% 0.3%0.3% 0.5% 0.5% 0.5%0.5%
Late (31-360 Late (31-360 days)days)
0.1%0.1% 1.0%1.0% 0.4%0.4% 0.3%0.3%
Very late Very late thrombosis* thrombosis* (361-1440 (361-1440 days)days)
0.9% 0.9% 0.4%0.4% 0.9%0.9% 0.6%0.6%
Any thrombosisAny thrombosis (0-1440 days)(0-1440 days)
1.5%1.5% 1.7%1.7% 1.8%1.8% 1.4%1.4%LR P=.70 LR P=.52
ARC Definition: Definite and Probable
*Proportional hazards assumption not rejected.ARC=Academic Research Consortium; BMS=bare metal stent; LR=lesion revascularization; PES=paclitaxel-eluting stent; SES=sirolimus-eluting stent.Mauri L et al. N Engl J Med. 2007;356:1020-1029.Pooled Data from RAVEL, SIRIUS, E-SIRIUS, and C-SIRIUS; Pooled Data from TAXUS 1 2 4 and 5.

Stent thrombosisStent thrombosis
Time (years)210
Cu
mu
lati
ve r
isk
of
sten
t th
rom
bo
sis
% 2
1
0
DES n=21 717BMS n=20 058
Stent type Total cohort
N = 41 775 stents
0.5% per year
Unadjusted
James ESC 2007

Most important conclusions which can be drawn
Up to 1 year after PCI (Ac ,S. A , & LATE PHASE)
Incidence and consequences of Stent thrombosis –
same in BMS and DES.
After 9 months-1 year ,incidence of ST
only slightly higher in DES group &
even this difference does not translate into increased MACE as
compared To BMS .(Kastrati A, Stone G W –NEJM 2007)
Most important and common cause of ST
Premature stopping of clopidogrel( Basket Late trial)

Premature discontinuation of antiplatelet therapy Premature discontinuation of antiplatelet therapy
the most important predictor of stent thrombosis afterthe most important predictor of stent thrombosis after
implantation”*implantation”* At 9 month follow-up, 29 patients had stent thrombosis (1.3%)At 9 month follow-up, 29 patients had stent thrombosis (1.3%)
Among the 29 patients, 13 died (case fatality rate 45%)Among the 29 patients, 13 died (case fatality rate 45%)
Common reasons for discontinuation includedCommon reasons for discontinuation included
41% Surgical procedures41% Surgical procedures
35% Intolerance to bleeding35% Intolerance to bleeding
24% Noncompliance24% Noncompliance

Prevention of ST
Because of High mortality & morbidity associated with
ST, it is imp for clinicians to stratify the individual pt’s risk for ST, restenosis, and bleeding when
selecting appropriate revascularization strategies.

Specifically, if the patient is unlikely to comply with
• long-term clopidogrel therapy,
• is likely to require surgery in the near-term( within 1 year) or
• is at risk of bleeding,
Alternative treatments are preferred, such as
• implanting BMS or doing plain balloon angioplasty
• performing bypass surgery, OR
• managing the patients medically.

Antiplatelet TherapyAntiplatelet TherapyAspirin.Aspirin.
After PCI, in patients without allergy or increased risk of bleeding,After PCI, in patients without allergy or increased risk of bleeding, aspirin 162 mg to 325 mg daily aspirin 162 mg to 325 mg daily
at least 1 month after BMS,at least 1 month after BMS, 3-6 months after DES3-6 months after DES
then, continued indefinitely at a dose ofthen, continued indefinitely at a dose of
75 mg to 162 mg /day75 mg to 162 mg /day

Antiplatelet TherapyAntiplatelet TherapyCLOPIDOGRELCLOPIDOGREL
DESDES
clopidogrel 75 mg daily(clopidogrel 75 mg daily(or prasugrel 10 mg Daily or or prasugrel 10 mg Daily or
ticagrelor 90 mg twice daily)ticagrelor 90 mg twice daily) should be given for at least should be given for at least
12 months if not at high risk of bleeding. 12 months if not at high risk of bleeding.
Continuation of clopidogrel therapy beyond 1 year may Continuation of clopidogrel therapy beyond 1 year may be considered in patients undergoing DES placement.be considered in patients undergoing DES placement.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Antiplatelet Therapy- Cont.
Clopidogrel
If BMS is used
- for Non ACS cases- minimum of 1 month- & ideally up to 12 months (unless at increased risk of bleeding; then it should be given for two weeks).
For ACS cases- given for upto 1 yr unless at increased risk of bleeding; then it should be given for two weeks).

COGENT (Clopidogrel and the Optimization of GI Events) trial randomized pts with
DAPT to clopidogrel and omeprazole or clopidogrel and placebo, no difference in CV events between the 2 groups, GI events were halved in omeprazole group.
Carefully evaluate the indication for PPI therapy in pts treated with clopidogrel, based on the presence or absence of the risk factors . The need for GI Protection with the number of risk factors for bleeding.
Prior upper GI bleeding is the strongest and most consistent risk factor for GI bleeding on antiplatelet therapy.
Patients with ACS and prior upper GI bleeding are at substantial cardiovascularrisk, so DAPT with concomitant use of a PPI may provide theoptimal balance of risk and benefit.

variable Score 0 Score 1 Score 2 Score 3
Age <60 60-79 >80
Shock nil HR< 100SBP>100
SBP <100
Co morbidity
nil CHF,IHDMajor morbity
Renal failure,liverFailure, metastases
Diagnosis Mallory weiss
All other diag
GI malignancy
e/o bleeding
none Blood,adherent clotSpurting vessel
A score less than 3 carries good prognosis but total score more than 8 carries high risk of mortality
Rockall score to identify patients at risk of adverse outcome following acute upper gastrointestinal bleeding.
Post PCI Pt needing non cardiac surgery
There are 2 fundamental questions that each clinician must ask:
1 Is stopping DAPT pharmacotherapy in the
periprocedural period necessary? This question is particularly
relevant in first month post PCI.
2 If DAPT IS interrupted,
what is the optimal timing and duration for temporary
discontinuation?

A Practical Approach to ManagingCardiovascular Risk and Bleeding ComplicationsAvoid cessation of all antiplatelet therapies after PCIwhen possible.
Avoid cessation of clopidogrel (even when aspirin is continued) within the first30 days after PCI and either DES or BMS placement when possible.
Defer elective endoscopic procedures, possibly up to 12 months, if clinicallyacceptable from the time of PCI with DES .
Perform endoscopic procedures, particularly those associated with bleedingrisk, 5–7 days after thienopyridine drug cessation. Aspirin should becontinued when possible.
Resume thienopyridine and aspirin drug therapy after the procedure oncehemostasis is achieved.
Continue platelet-directed therapy in patients undergoing elective endoscopyprocedures associated with a low risk for bleeding.
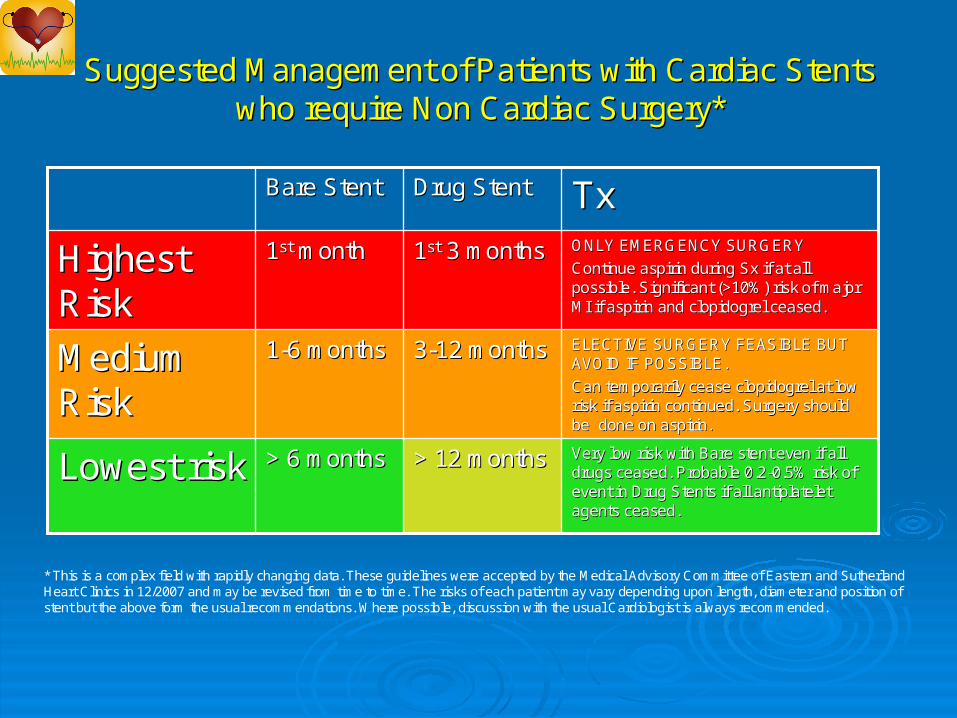
Suggested Management of Patients with Cardiac Stents Suggested Management of Patients with Cardiac Stents who require Non Cardiac Surgery*who require Non Cardiac Surgery*
> 12 months> 12 months
33--12 months12 months
11stst 3 months3 months
Drug StentDrug Stent
Very low risk with Bare stent even if all Very low risk with Bare stent even if all drugs ceased. Probable 0.2drugs ceased. Probable 0.2--0.5% risk of 0.5% risk of event in Drug Stents if all event in Drug Stents if all antiplateletantiplateletagents ceased.agents ceased.
> 6 months> 6 monthsLowest riskLowest risk
ELECTIVE SURGERY FEASIBLE BUT ELECTIVE SURGERY FEASIBLE BUT AVOID IF POSSIBLE.AVOID IF POSSIBLE.
Can temporarily cease Can temporarily cease clopidogrelclopidogrel at low at low risk if aspirin continued. Surgery should risk if aspirin continued. Surgery should be done on aspirin.be done on aspirin.
11--6 months6 monthsMedium Medium RiskRisk
ONLY EMERGENCY SURGERYONLY EMERGENCY SURGERY
Continue aspirin during Continue aspirin during SxSx if at all if at all possible. Significant (>10%) risk of major possible. Significant (>10%) risk of major MI if aspirin and MI if aspirin and clopidogrelclopidogrel ceased.ceased.
11stst monthmonthHighest Highest RiskRisk
TxTxBare StentBare Stent
* This is a complex field with rapidly changing data. These guidelines were accepted by the Medical Advisory Committee of Eastern and Sutherland Heart Clinics in 12/2007 and may be revised from time to time. The risks of each patient may vary depending upon length, diameter and position of stent but the above form the usual recommendations. Where possible, discussion with the usual Cardiologist is always recommended.

Go for it- ct Asp if possible10% risk of MI if both stopped
POST PCINeeding Sx
Emergency ELECTIVE
Days from PCI
< 1 Month 1-6 Months > 6 Months
Defer Sx for Atleast 1month
Type of Stent
BMS
Stop Clop for a weekCt AspirinRestart Clop post Sx
DES
Defer Sx for> 6 months
BMS/DES
Stop Clop for a weekCt AspirinRestart Clop post Sx

Go for it- ct Asp if possible10% risk of MI if both stopped
POST PCINeeding Sx
Emergency ELECTIVE
Days from PCI
< 1 Month 1-6 Months > 6 Months
Defer Sx for Atleast 1month
Type of Stent
BMS
Stop Clop for a weekCt AspirinRestart Clop post Sx
DES
Defer Sx for> 6 months
BMS/DES
Stop Clop for a weekCt AspirinRestart Clop post Sx

Risk of GI BLEED WITH DAPT
is significant – about 2% and as high as 12% in high-risk pts with prior peptic ulcer bleeding.
GI bleed after PCI associated with increased morbidity, mortality, duration of hospitalization and cost.
RISK FACTORS Advanced age a history of peptic ulcer disease, co-administration of NSAIDc, co-administration of anticoagulants, CRF,DM ,Liver disease and physiological stress,

OASIS and CURE
close relation between major bleeding and subsequent MI, stroke and death at 30 days;
10% of patients who got 2 or more units of BT died within 30 days vs 2.5% of those who did not sustain a bleed.
Why -pts who with hemrgic complications are frequently older, with significant comorbidities such as renal insufficiency.
Therefore,bleeding may be a marker of a sicker patient, whichconfers an increased risk of death

Aspirin monotherapyAspirin leads to suppression of mucosal prostaglandinsynthesis and subsequent formation of mucosal erosions.Whereas the inhibition of thromboxane-A2-mediated plateletfunction is dose independent (at least for daily doses N30mg), the impairment of PGE2-mediated cytoprotection in theGI mucosa is dose dependent [14]. Aspirin amplifies the riskof bleeding by causing new mucosal lesions or aggravatingexisting ones, which are associated with a greater relativerisk (four- to sixfold) at the higher doses of aspirin [14]. Ofpatients with a history of peptic ulcer bleeding who continueto take aspirin after ulcer healing and eradication of Helicobacterpylori infection, up to 15% experience recurrentbleeding within a year [15].4.2. Clopidogrel monotherapyWhether clopidogrel causes mucosal injury and bleedingfrom preexisting mucosal lesions is uncertain. In theClopidogrel versus Aspirin in Patients at Risk of IschemicEvents trial, GI hemorrhage (0.52% vs. 0.72%, Pb .05) wassignificantly less frequent with clopidogrel compared withaspirin [16]. Available evidence suggests that clopidogreldoes not induce new ulcer formation but may causerebleeding due to impaired hemostasis only in subjectswith underlying mucosal defects or scarring [17]. Inrandomized controlled trials, among patients with acutecoronary syndrome (ACS), the addition of clopidogrel toaspirin appears to increase the relative risk of all hemorrhagicevents by 50% [18]. However, it must be remembered thatthe patients

4.2. Clopidogrel monotherapyWhether clopidogrel causes mucosal injury and bleedingfrom preexisting mucosal lesions is uncertain. In theClopidogrel versus Aspirin in Patients at Risk of IschemicEvents trial, GI hemorrhage (0.52% vs. 0.72%, Pb .05) wassignificantly less frequent with clopidogrel compared withaspirin [16]. Available evidence suggests that clopidogreldoes not induce new ulcer formation but may causerebleeding due to impaired hemostasis only in subjectswith underlying mucosal defects or scarring [17]. Inrandomized controlled trials, among patients with acutecoronary syndrome (ACS), the addition of clopidogrel toaspirin appears to increase the relative risk of all hemorrhagicevents by 50% [18]. However, it must be remembered thatthe patients
The risk of adverse GI events depends on the dose and duration of antiplatelet therapy.
CURE study- the risk of GI bleeding with combination clopidogrel (75 mg) with high-dose aspirin (N200 mg) was significantly greater than that with low dose aspirin (≤100 mg) (3% vs. 4.9%, P=.0009 APT.
So what to do in a pt with GI BLEED

Therefore, thediscontinuance of DAPT- risk and the initiation of blood transfusion- risk as part of the treatment of post-PCI hemorrhageneed to be thoroughly analyzed on an individual basis.decision to administer BT to a patient should not be based on a hemoglobin level but rather on a pt's symptoms and on the risk of ischemiccomplications from acute anemia such as angina,CHFHypotension etcpatient's risk is defined as the presence of unrevascularizedcoronary artery territory, valvular heart disease andcongestive heart failureJudicious transfusion should begiven for hemodynamically significant blood loss.

variable Score 0 Score 1 Score 2 Score 3
Age <60 60-79 >80
Shock NilHR< 100SBP>100
TachycardiaHR> 100SBP>100
HypotensionSBP <100HR>100
Co morbidity
nil CHF,IHDMajor morbidly
Renal failure,liver Failure, metastases
Diagnosis Mallory weiss
All other diag
GI malignancy
e/o bleeding
none Blood in upper GI,adherent clotSpurting vessel
A score less than 3 carries good prognosis but total score more than 8 carries high risk of mortality
Rockall score to identify patients at risk of adverse outcome following acute upper gastrointestinal bleeding.

Pt with GI Bleed
Features of High Risk Of MortalityMassive Hemmorrhage or shock & /or e/o myocardial ischemia or CCF
Give BT esp if Hb <8 gms%
Start PPIhold antiplatelet for 24 hrsDiagnostic and therapeutic upper GI endoscopy within 24 hrs of admission
Assess risk of ST asso. With Ceassation of APT Assess risk continued GI bleed
Low risk of recurrentBleed(Rockall score <5)
Continue DAPT
High risk of recurrent bleed(Rockall score>5
Stop Aspirin, ct ClopiPlan to restart Aspirin in 2 wks
Continued GI BleedStop both Asp and clopi
Aim to restart clopidogrelIn 1-2 weeks
Start or ct PPI
Assess forHemodynamic stability

Pt with GI Bleed
Start or ct PPIAssess hemod stability
High risk featuresMassive Hrrage or shock&/or e/o myo. Ischemia or CCFEsp if Hb < 8
BT- Packed cells. Hold antiplatelets for 24 hrsDiagnostic and therapeutic Endoscopy within 12-24 hrsAssess risk of ST asso. With
Ceassation of APT vs risk of continued GI bleed
Low risk of recurrentBleed(Rockall score <5)
Continue DAPT
High risk of recurrent bleed(Rockall score>5
Stop Aspirin, ct ClopiPlan to restart Aspirin in 1 wk
Continued GI Bleed or ptNedding SxStop both Asp and clopi
Aim to restart clopidogrelIn 1 week & later aspirin

ScoreVariable0123Age (years)<6060–79 80Shock⩾No shock (systolic BP >100, pulse <100)Tachycardia (systolic BP >100, pulse >100)Hypotension (systolic BP <100, pulse >100)Co-morbidityNil majorCardiac failure, ischaemic heart disease, any major co-morbidityRenal failure, liver failure, disseminated malignancyDiagnosisMallory Weiss tear, no lesion and no SRHAll other diagnosesMalignancy of upper GI tractMajor SRHNone or dark spotBlood in upper GI tract, adherent clot, visible or spurting vesselEach variable is scored and the total score calculated by summing the scores.SRH: stigmata of recent haemorrhage.

THANK YOU
Blood pressure control:GoalLess than 140 over 90 mm Hgorless than 130 over 80 mm Hgif chronic kidney disease or diabetes is present

restenosis, development of progressive disease in the same or a different coronary territory
increased myocardial demand from various causes.

increased myocardial demand can result from the development of anaemia or aortic stenosis

In the BMS era, ST usually presented acutely orsub acutely, before neointimal formation..In randomized trials that compared BMS with DES,rates of acute and sub acute STamong patients receiving dual antiplatelettherapy were similar forboth stent types (1%)

Acute and subacute thrombosis of both BMS and DES
have adverse clinical consequences. In a registry of patients who underwent DES implantation with 9-month follow-up, 24% of ST cases presented as death,
60% as nonfatal MI,
and 7% as unstable angina.
The case fatality rate for ST in this registry was 45%.
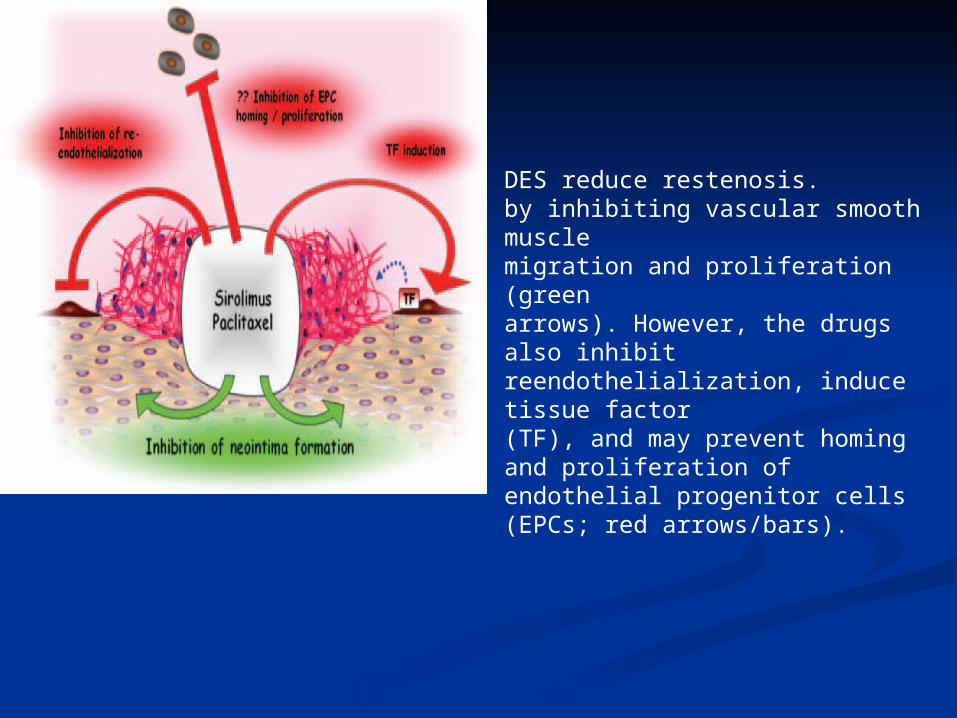
DES reduce restenosis. by inhibiting vascular smooth musclemigration and proliferation (greenarrows). However, the drugs also inhibitreendothelialization, induce tissue factor(TF), and may prevent homing and proliferation of endothelial progenitor cells(EPCs; red arrows/bars).


However, in recentmeta-analyses of DES trials, modest increases in rates oflate and very late ST compared with BMS did not translateinto a worse clinical outcome (3,10). These differencesmight reflect selection bias stemming from different diagnosticcriteria for ST or possibly from implantation of DESin small vessels subtending limited myocardial territory.Stone G W , Kastrati A NEJM 2007

Late BMS thrombosis is an uncommon event (12)This is because of endothelialization of the stent which isAlmost complete by 1 month of PCI

implantation in apatient dying of a non-DES–related cause.52 It has beenproposed that bone marrow–derived endothelial progenitorcells may also be involved in reendothelialization.53,54 Interestingly,rapamycin inhibits proliferation, migration, anddifferentiation of human endothelial progenitor cells invitro.55,56 Hence, drugs loaded on DES may affect the numberas well as the homing and proliferation of endothelialprogenitor cells, thus further preventing proper endothelialhealing (Figure 2).

Impaired ReendothelializationReendothelialization occurs after vascular injury and similarlyafter stent placement. Traditionally, it was believed thatendothelial cells proliferate and migrate from intact neighboringcoronary segments, eventually leading to the reendothelializationof the injured segment. In vitro, rapamycin andpaclitaxel not only inhibit proliferation and migration ofvascular smooth muscle cells but equally suppress endothelialcells,7,35,36,38,49–51 thereby potentially impeding reendothelialization(Figure 2).

DES reduce neointima formationbut may increase stent thrombogenicity.Effect of sirolimus-eluting/paclitaxel-eluting stent strut on the localvessel wall after implantation. Sirolimus/paclitaxel reduces neointima formationby inhibiting vascular smooth musclemigration and proliferation (greenarrows). However, the drugs also inhibitreendothelialization, induce tissue factor(TF), and may prevent homing and proliferationof endothelial progenitor cells(EPCs; red arrows/bars).

988 CONSECUTIVE (non-selected) patients randomized 2:1 DES:BMS
• 746 patients alive without MACE 6 months after coronary stenting; CLOPIDOGREL stopped:BMS Vision stent, Guidant Corp: 281SES: 264PES: 281
• Clopidogrel stopped at 6 months and then followed for another 12 months

Patient• Antiplatelet
noncompliance• Response variability
StentThrombosis
Adapted from Kereiakes DJ et al. Rev Cardiovasc Med. 2004;5:9-15.
Stent Thrombosis: Stent Thrombosis: A Multifactorial ProblemA Multifactorial ProblemLesion • Long lesions • Small diameter• Multivessel • Acute myocardial
infarction (AMI)• Diabetes• Bifurcations
Technical • Underexpansion• Incomplete wall
apposition• Crush technique• Overlapping
Stent • Material• Polymer matrix• Antithrombotic
agent

Technical
Smaller final lumen diameter Underexpansion
Incomplete wall apposition
Stent length
Crush technique
Overlapping and multiple stents
Persistent slow coronary blood flow
Patient related factorsAntiplatelet noncomplianceResponse variabilitylow ejection fraction diabetes mellitus,28 advanced age and stenting in the setting of an acute coronary syndrome.
Lesion characteritics Long lesions
Small diameter vessel , 2.5 mm
Multivessel disease
Acute myocardial infarction (AMI)
Diabetes
Bifurcation lesion

Stent design platelet activationwas greater during the 30 days after implantation of an open-cell versus a closed-cell stentStentMaterialPolymer matrix nonerodable polymers of the Cypher and Taxus DES provoke chronic eosinophilic infiltration of the arterial wall, suggestiveof hypersensitivity reactions in a small number ofcases
Antithrombotic agent
increased risk in patients withacute coronary syndrome could be due to delayed healing,lack of endothelialization, and presence of a pronouncedinflammatory and thrombogenic environment of the exposednecrotic core to flowing blood, accompanied by enhancedplatelet reactivity; furthermore, rapamycin and paclitaxelpotentiate thrombin-induced expression of tissue factor

Thrombogenicity of the StentA predisposition for the development of stent thrombosis hasbeen observed with certain stent materials; for example,platelet activation was greater during the 30 days afterimplantation of an open-cell versus a closed-cell stent.33Stentstrut thickness and polymer type and thickness also play animportant role. It has been reported previously that thenonerodable polymers of the Cypher and Taxus DES provokechronic eosinophilic infiltration of the arterial wall, suggestiveof hypersensitivity reactions in a small number ofcases
Furthermore, drugs loaded on DES may exert a prothrombogeniceffect. Rapamycin (sirolimus), a macrocyclic lactone,is used on DES, because it is known to inhibitproliferation and migration of vascular smooth muscle cells,important factors in the development of neointima formationand restenosis, through interference with cell cycle regulators.35,36 On a subcellular level, rapamycin binds to theFK-binding protein 12 and subsequently inhibits the mammaliantarget of rapamycin. The mammalian target of rapamycinis a downstream target of the phosphatidylinositol-3kinase pathway, which in turn is involved in an inhibitoryfashion in the regulation of tissue factor in endothelial cellsand monocytes.37–39 As a result, rapamycin inhibition of themammalian target of rapamycin increases both thrombin- andtumor necrosis factor-–induced endothelial tissue factorexpression and activity at concentrations of rapamycin thatare encountered in vivo (Figure 1).38,40

Paclitaxel is a lipophilic diterpenoid that binds to the-subunit of the tubulin heterodimer, promoting tubulinpolymerization, cell cycle arrest, and, eventually, inhibitionof vascular smooth muscle cell migration and proliferation.41,42 In addition, paclitaxel is known to activate c-JunNH2-terminal kinase,43,44 an important mediator of endothelialand monocytic tissue factor induction.37,39,45 Consequently,paclitaxel also enhances tissue factor expression andactivity in endothelial cells44

In sirolimus-eluting stents, 80% of the rapamycin haseluted by 30 days, whereas paclitaxel-eluting stents have abiphasic drug release profile in vitro with an initial burstduring the first 48 hours after implantation followed by asustained low-level release for at least 2 weeks.

Thus, both rapamycin- and paclitaxel-inducedtissue factor expression may contribute to a prothromboticenvironment after deployment of DES, particularly in theacute and subacute setting and possibly in late stent thrombosis(Figure 1).

PREMIER Registry of 500 PREMIER Registry of 500 Patients Patients
With AMI and DES With AMI and DES
P<.001.Spertus JA et al. Circulation. 2006;113:2803-2809.
1 in 7 Patients (13%) Stopped Clopidogrel Within 30 Days
Continued
Discontinued
0 1 2 3 4 5 6 7 8 9 10 11 120
5
10
15
Months
Mort
ality
(%
)
No. at RiskNo. at Risk
ContinueContinue 434311
431431 431431 431431 430430 429429 420420
DiscontinuedDiscontinued 6868 6868 6767 6666 6565 6565 6262
Angioplasty in the setting of acutecoronary syndromes could theoretically predispose to STowing to the large thrombotic burden already present,suboptimal stent expansion to avoid the risk of no-reflow, orDES implantation on a thrombus that eventually disappearsleading to malapposition. An SES registry reported increasedrisk of ST in patients who presented with acutecoronary syndromes (28). However, 3 randomized trialscomparing BMS and DES for primary angioplasty in acuteMI found no difference in ST rate between the stent types
(29–31). Some registry reports have suggested increased ST
rates in diabetic patients and patients with renal failure
Optimization of stent deployment (62) and dual antiplatelettherapy with aspirin and a thienopyridine (63–65) haveachieved the currently accepted 30-day ST rate of 1%.Reports of late DES thrombosis, often in association withcessation of antiplatelet therapy (9,13,19,37,38,59), suggestthat long-term combined antiplatelet therapy might beappropriate. A recent science advisory has recommendedlengthening the duration of dual antiplatelet therapy to 1year after PCI and that elective surgery should be postponedfor 1 year (66). The efficacy of increasing the maintenancedose of clopidogrel to 150 mg daily in patients withsuspected clopidogrel resistance is unknown (67).
Percutaneous coronary intervention for emergent ST is often suboptimal, and ST recurs in 12% of these patients
Drug-Eluting Stent Thrombosis2003-2004: Occasional case reports of late stent thrombosis after DES began to emergeFirst big bang: March 2006 ACC AtlantaPresentation of the BASKET-LATE Investigators988 CONSECUTIVE (non-selected) patients randomized 2:1 DES:BMS
746 patients alive without MACE 6 months after coronary stenting; CLOPIDOGREL stopped:BMS Vision stent, Guidant Corp: 281SES: 264PES: 281
Clopidogrel stopped at 6 months and then followed for another 12 months
Current status of DESCurrent status of DES
The data on the two previously approved DES The data on the two previously approved DES have demonstrated a significant reduction in the have demonstrated a significant reduction in the need for repeat revascularization vs BMSneed for repeat revascularization vs BMS
Recently the rare but catastrophic event of late Recently the rare but catastrophic event of late stent thrombosis was shown to be increased with stent thrombosis was shown to be increased with these DES compared to BMSthese DES compared to BMS
However, any increased incidence of LST appears However, any increased incidence of LST appears to be offset by a reduction in downstream to be offset by a reduction in downstream revascularization events prevented by DESrevascularization events prevented by DES

Timing of stent Timing of stent thrombosis with BMSthrombosis with BMS
(A)
0 30 60 120 6000
2
4
6
8
10
n
Days after PCI
Days after PCI0 30 60 12090 600
0
20
40
60
80
100
Per
cen
t o
f p
atie
nts
(B)
Wenaweser P et al. EHJ. 2005;26:1180-1187.
(A) incidence of stent thrombosis (n = number of stent thromboses per day) following bare-metal stent implantation.Acute and subacute stent thrombosis (30 days) are in yellow, late stent thrombosis (> 30 days) in yellow.
(B) Cumulative incidence of stent thrombosis following bare-metal stent implantation.
Days after PCI0 30 60 12090 600
0
20
40
60
80
100
Per
cen
t o
f p
atie
nts
(B)

BASKET-LATE: Late Catch upOverall (0-18 month) rates of death and MI were the same: BMS 7.5% vs DES 8.4% p=0.63First 6 months Death and MI: BMS 12.1% vs DES 7.2% p=0.02AFTER DISCONTINUATION of CLOPIDOGREL (months 7-18)
Death: BMS 0% vs DES 1.2%MI: BMS 1.3% vs DES 4.1%Death and MI: BMS 1.3% vs DES 4.9% (p=0.03)All 6 deaths in the DES group20/23 MI in the DES group
Hypothesis generating, to say the least
Pfisterer et al J Am Coll Cardiol 2006;48:2584-91

Meta analyses presented: ESC European Society of Cardiology meeting Barcelona September 2006
Death/Q wave MI 2.6% TAXUS vs 2.3% BMS (p=0.66)Death/Q wave MI 6.3% Cypher vs 3.9% BMS (p=0.03)Camenzind and Nordmann et al
Industry data: Cordis/Johnson and Johnson and Boston ScientificFDA: Initial Statement on Coronary Drug Eluting Stents, September 14th 2006FDA: Special Expert Advisory Committee, December 7th and 8th 2006New England Journal of Medicine: March 8th 2007

With the introductionof P2Y-receptor antagonists (ie, ticlopidine, clopidogrel)for platelet inhibition in combination with acetylsalicylicacid, the incidence of stent thrombosis decreased substantiallyin stable patients to levels as low as 1%.5 Most of theevents occurred within the first 10 days after implantation;indeed, stent thrombosis after the first month was extremelyrare with BMS.6,7

Numerous reports describe the occurrence of acute (24hours), subacute (30 days), late (30 days), and very late(12 months) stent thrombosis after DES implantation.8,13,16
true incidence of stent thrombosis may beunderestimated in clinical trials and could occur at substantiallyhigher rates in the “real-world” setting, where morecomplex lesions are treated

The most important risk factorsfor acute and subacute stent thrombosis are primary stentingin ST-segment elevation myocardial infarction and acutecoronary syndromes.20,26 Additional risk factors include stentlength, congestive heart failure, and a prothrombogenic state,such as metastatic cancer.19,20,26,27 One of the most significantrisk factors for late and very late stent thrombosis appears tobe discontinuation of antiplatelet therapy.26,27 Other predictorsare stent underexpansion and residual reference segmentstenosis

Outcome after Drug-eluting stent versusBare-metal stent implantation:
A network meta-analysis of 38 trials with 18,023 ptsNo difference in death or myocardial infarction
up to 4 years follow-up
Stettler et al, Lancet 2007:370:937
Antiplatelet Therapy Post PCIStents are foreign bodies in the vessel wall and thus induceplatelet adhesion and balloon inflation causes Vascular injury leading to activation of the coagulation cascade. with exposure ofthrombogenic molecules of the subintima and media (includingplaque material) to the blood stream. As a consequence,only potent platelet inhibition made the procedure feasible,and antiplatelet hyporesponsiveness has been associated withan increased risk for stent thrombosis.31 In line with thisobservation, discontinuation of antiplatelet therapy has beenobserved to be particularly associated with DES thrombosis.8,16,32 The appropriate duration of the long-term antiplateletregimen for prevention of DES thrombosis remains to beassessed in randomized prospective trials; at present, a courseof 12 months of dual-antiplatelet therapy may be consideredespecially in high-risk, real-world patients.

The data on the two previously approved DES have The data on the two previously approved DES have demonstrated a significant reduction in thedemonstrated a significant reduction in the need for repeat revascularization need for repeat revascularization vs BMSvs BMS
Recently the rare but catastrophic event of late Recently the rare but catastrophic event of late stent thrombosis was shown to bestent thrombosis was shown to be increased with these DES compared to BMSincreased with these DES compared to BMS
However, any increased incidence ofHowever, any increased incidence of LST appears to be offset by a reduction in downstreamLST appears to be offset by a reduction in downstream revascularization events prevented by DESrevascularization events prevented by DES


ProcedureProcedure ProcedureProcedure
Stent thrombosis:Stent thrombosis:Procedure, product, patientProcedure, product, patient
Stent thrombosis
Stent appositionStent apposition dissectiondissection
Stent appositionStent apposition dissectiondissection
PatientPatientPatientPatient
Higher riskHigher riskAP complianceAP compliance
Higher riskHigher riskAP complianceAP compliance
ProductProductProductProduct
PolymerPolymerdrugdrug
PolymerPolymerdrugdrug

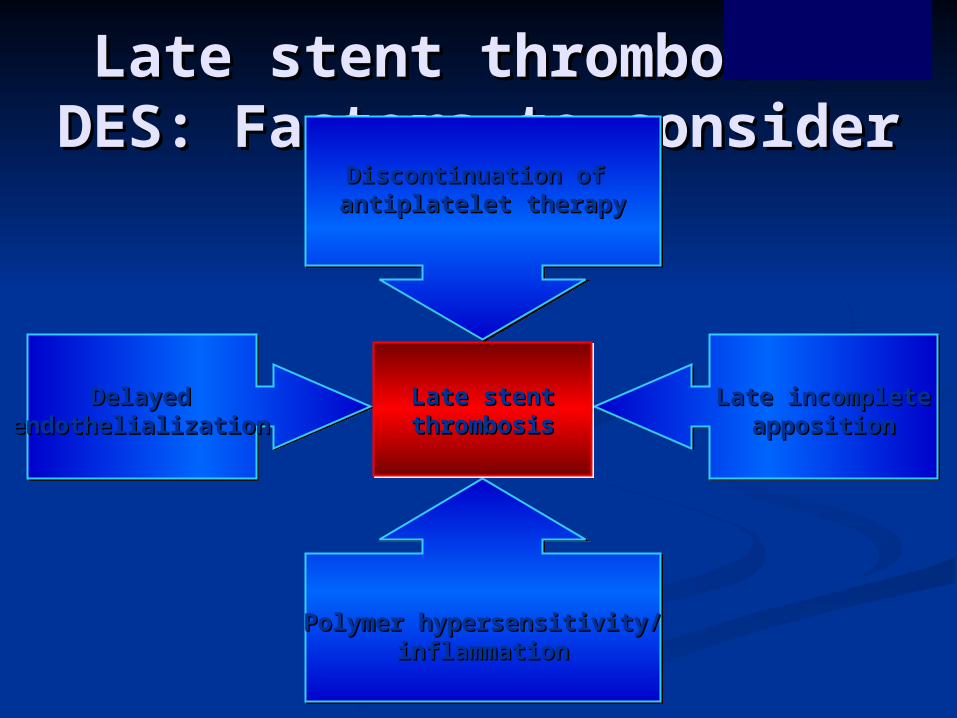
Late stent thrombosis—Late stent thrombosis—DES: Factors to considerDES: Factors to consider
Discontinuation of Discontinuation of antiplatelet therapyantiplatelet therapy
DelayedDelayedendothelializationendothelialization
Late incompleteLate incompleteappositionapposition
Polymer hypersensitivity/Polymer hypersensitivity/inflammationinflammation
Late stentLate stentthrombosisthrombosisLate stentLate stent
thrombosisthrombosis


Stent thrombosis ratesStent thrombosis rates
29.0%
8.7%5.5%
3.5% 3.2% 2.6%1.3%
*Antiplatelet*Antiplatelettherapytherapy
discontinuationdiscontinuation
DiabetesDiabetesPriorPriorbrachybrachy
RenalRenalfailurefailure
BifurcationsBifurcations ULMULM UAUA
*Premature discontinuation.*Iakovou et al. JAMA. 2005;293:2126-2130.
According to select patient characteristicsAccording to select patient characteristics

Premature discontinuation of antiplatelet therapyPremature discontinuation of antiplatelet therapyis the most important predictor of stent thrombosisis the most important predictor of stent thrombosis
after implantation”*after implantation”* Results:Results:
At 9 month follow-up, 29 patients had stent thrombosis (1.3%)At 9 month follow-up, 29 patients had stent thrombosis (1.3%)Among the 29 patients, 13 died (case fatality rate 45%)Among the 29 patients, 13 died (case fatality rate 45%)
Common reasons for discontinuation include:Common reasons for discontinuation include:41% Surgical procedures41% Surgical procedures
35% Intolerance to bleeding35% Intolerance to bleeding24% Noncompliance24% Noncompliance

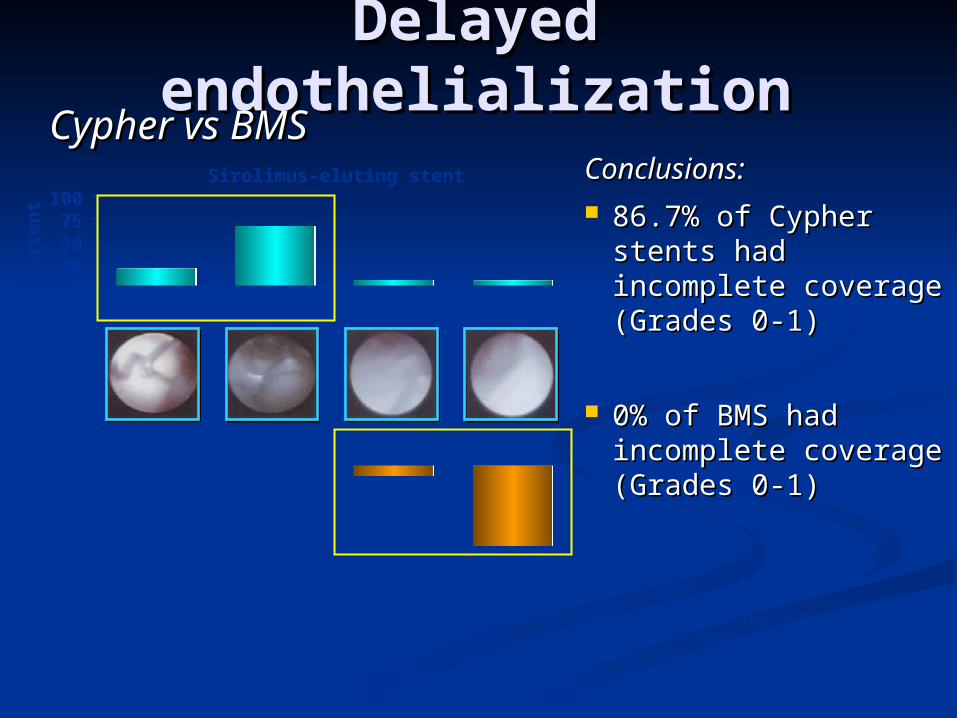
Delayed Delayed endothelializationendothelialization
Conclusions:Conclusions: 86.7% of Cypher 86.7% of Cypher
stents had stents had incomplete coverage incomplete coverage (Grades 0-1)(Grades 0-1)
0% of BMS had 0% of BMS had incomplete coverageincomplete coverage(Grades 0-1)(Grades 0-1)
Cypher vs BMSCypher vs BMS
Grade 0 was defined as stent struts that were fully visible, similar to immediately after implantation.Grade 1 was defined as stent struts that bulged into the lumen and, although covered, were still transparently visible.Grade 2 was defined as stent struts that were visible, but not clearly seen (ie, they were translucent). Grade 3 was defined as stent struts that were not visible by angioscopy (ie, they were embedded in the neointima).Kotani et al. JACC. 2006;47:2108-2111.
0255075
100
Incomplete coverage Complete coverage
Sirolimus-eluting stent
Bare-metal stent
Grade 0 Grade 1 Grade 2 Grade 3
250
5075
100
Per
cen
tP
erce
nt



Causes of Aspirin Resistance
Reduced bioavailability of aspirin Poor compliance Inadequate dose Reduced absorption or increased metabolism
Altered binding to COX-1
Concurrent intake of certain NSAID (ibuprofen, indomethacin)
Other sources of TX production
Not blocked by aspirin (ex. COX-2 in monocytes, macrophages, EC)
Alternative pathways of PLT activation
Not blocked by aspirin (ex. RBC)
Increased PLT sensitivity to collagen & ADP

Increased turnover of PLT By BM in response to stress (ex. CABG) Newly formed PLT unexposed to aspirin during the 24hr dose interval(aspirin half life 20min) Genetic polymorphism COX-1, COX-2, TXA2 synthase etc. PLT Rc (Ia/IIa, Ib/V/IX, IIb/IIIa, collagen,vWF) Factor XIII Loss of the antiplatelet effect of aspirin with prolongedadministration (Tachyphylaxis ) Non-atherothrombotic causes of vascular events

Clopidogrel : mechanism

Causes of Clopidogrel Resistance Absorption Metabolism, Drug interaction CYP3A4 activity (Lau WC, et al. Circulation 2004) CYP3A5 polymorphism (Suh JW, et al. CMAJ 2006) CYP2C19 polymorphism (Hulot JS, et al. Blood 2006) P2Y12 Rc polymorphism Controversial Pro ; Cerebrovascular ds (Ziegler S, Stroke 2005), PAD (Fontana P,Circulation 2003) Cons ; CAD (Smith SM, Platelets 2006/ Angiolillo DJ, Thromb Res 2005)


*Blue – responderΔ aggregation: 27%
*Black- nonresponderΔ aggregation: -1%
Platelet aggregationMaximal percent change in light
transmittance from baseline Platelet rich plasma
Chrono-log 400 series, 500 series ®Pre-treatment Clopidogrel – post 1wk
LTA (light transmittance aggregometry )

Definition of resistance Aspirin resistance
0.5mg/mL AA-induced platelet aggregation ≥20% and 5μM/L ADP-induced platelet aggregation ≥70%
Clopidogrel resistance Absolute difference between baseline and post-treatment aggregation
(Δaggregation) ≤10% in response to both 5 & 20 μM/L ADP

VerifyNowTM (Ultegra) RPFAVerifyNowTM Aspirin Assay VerifyNowTM IIb/ IIIa Assay
VerifyNowTM Clopidogrel Assay

Definition of resistance Aspirin
Aspirin reaction unit (ARU) ≥550 inadequate platelet inhibition by Aspirin

Duration of Dual Antiplatelet TherapyAcute stent thrombosis is a dreaded complication of PCI. It is rare but is typically associated with catastrophic consequences including myocardial infarction and sudden death. Incidence is in general <1% with dual antiplatelet therapy and high-pressure stent deployment. The majority of cases happen early poststenting. Dual antiplatelet therapy with aspirin plus clopidogrel is therefore mandatory initially in patients who had coronary stents implanted.

1. Patients already taking daily long-term aspirin therapy should take2. 75 mg to 3253. mg of aspirin before PCI is performed. (Level of Evidence: A) 4. 2. Patients not already taking daily long-term aspirin therapy should be given 300
mg to 325 mg of aspirin at least 2 hours and preferably 24 hours before PCI is performed. (Level of Evidence: C)
5. 3. After PCI, in patients without allergy or increased risk of bleeding, aspirin 162 mg to 325 mg daily should be given for at least 1 month after BMS implantation, 3 months after sirolimus-eluting stent implantation, and 6 months after paclitaxel-eluting stent implantation, after which daily long-term aspirin use should be continued indefinitely at a dose of 75 mg to 162 mg. (Level of Evidence: B)
A loading dose of clopidogrel,* generally 600 mg, should be administered before or when PCI is performed. (Level of Evidence: C) In patients undergoing PCI within 12 to 24 hours of receiving fibrinolytic therapy, a clopidogrel oral loading dose of 300 mg may be considered. (Level of Evidence: C) For all post-PCI stented patients receiving a DES, clopidogrel 75 mg daily should be given for at least 12 months if patients are not at high risk of bleeding. For post-PCI patients receiving a BMS, clopidogrel should be given for a minimum of 1 month and ideally up to 12 months (unless the patient is at increased risk of bleeding; then it should be given for a minimum of 2 weeks).

1. Continuation of clopidogrel therapy beyond 1 year may be considered2. in3. patients undergoing DES placement. (Level of Evidence: C)

optimal duration of dual antiplatelet therapy is controversial, but a minimum period of 4 weeks for BMSs is widely accepted.

Table 1Relative contraindication to DESs that would favor use of BMSs1. Adherence to prolonged DAPT?Polysubstance abuseDementiaLimited financial means2. Bleeding risk?a. Known bleeding disorderGastric ulcerEsophageal varicesDiverticulosisb. Potential bleeding disorder (lifelong warfarin)Mechanical heart valveAtrial fibrillationProthrombotic disorder3. Surgery within the next year?Many procedures require termination of antiplatelet
PPIs are recommended for 6-8 wk following UGIH and/or endoscopic treatment of PUD to allow for full mucosal healing. Several studies have shown a therapeutic benefit of PPIs in patients using NSAIDs chronically and/or patients with confirmed H. pylori infection[34,35]. After initial mucosal healing has been achieved, is there a benefit to long-term PPI use for secondary prophylaxis? Studies have shown that in patients who have PUD complicated by bleeding, there is a 33% risk of rebleeding in 1-2 years. Furthermore, there is a 40%-50% rebleeding risk over the subsequent 10 years following the initial episode of bleeding[13]. Randomized prospective trials have demonstrated a benefit to long-term acid-suppression therapy in two settings: chronic NSAID users and H. pylori-infected patients. As demonstrated in a 2001 New England Journal of Medicine article by Chan et al[34], in patients taking NSAIDs other than acetylsalicylic acid (ASA) who were concomitantly infected with H. pylori, omeprazole provided added protection above bacterial eradication alone.





















