
Post-Partum Complications SG # 8 Prof. Unn Hidle Updated Spring 2010.
85
Post- Partum Complicati ons SG # 8 Prof. Unn Hidle Updated Spring 2010
-
date post
22-Dec-2015 -
Category
Documents
-
view
220 -
download
2
Transcript of Post-Partum Complications SG # 8 Prof. Unn Hidle Updated Spring 2010.

Post-Partum Complications
SG # 8Prof. Unn Hidle
Updated Spring 2010

HEMORRHAGE

HEMORRHAGE Description: (overall category of
hemorrhage) Bleeding of 500 mL or more following delivery Traditional definition vs. “new” definition:
Traditional: NVD => 500cc C-section => 1000cc
“New” criteria: Decreased Hct of 10 points OR The need for fluid replacement after birth

Early PP Hemorrhage Assessment
Hemorrhage occurs during first 24 hours after delivery >500cc of blood loss
Caused by: retained fragments of placenta UTERINE ATONY
80-90% of the cases Blood may be expelled or retained in the vagina
perineal injuries/lacerations inversion of uterus Episiotomy Hematomas: vulvar, vaginal, subperitoneal Coagulation disorders (i.e. hemophilia, thalassemia)

HEMORRHAGE

Predisposing factors Multiparity Multiple gestations Anesthesia (relaxes the uterus) Uterine infections Pitocin used for induction or augmentation of labor Trauma from forceps delivery Malnutrition (esp. decreased Folic Acid and iron) Anemia PIH

Most Common Causes of Hemorrhage Residual placenta
Bleeding from placenta accreata – parts of the placenta adhers to the endometrium, in this case the chorionic villi attaches directly to the myometrium of the uterus (accounts for 80% of adherent placenta to the endometrium)
Placenta accreata may cause: Maternal hemorrhage Failure of the placenta to separate
Less common to bleed from placenta increta or placenta percreta (other placenta adherences)
Abdominal hysterectomy may be necessary, depending on involvement
Retained placenta: Surgical removal (D&C)

Uterine Atony

D&C: Dilitation & Curettage

Early PP hemorrhage Laceration of the birth canal
If there is post-partum hemorrhage and the fundus is firm, suspect laceration
Vaginal lacerations: Surgical repair Cervical laceration:
Repair is usually accomplished by turning the cervix inside out and suturing
Assessment of Early PP Hemorrhage
In what order? Bradycardia Tachycardia Tachypnea with shallow respirations Diaphoretic Cool, clammy skin Hypotension
Overall: signs of hypovolemic shock

Treatment Remember, this is immediately PP! FIRST… Externally massage fundus if
boggy – DON’T over-massage Bimanual massage? What if it is a C-section? Oxytocin / Pitocin PRBC transfusion or other blood products

HEMORRHAGE

Possible Medications Pitocin Methylergonivine maleate (Metergine) Prostaglandins (PGF2a); Prostin:
Uterine stimulant – increase contraction of uterus
Most effective if hemorrhage is caused by uterine atony
Used if Pitocin is not successful

Prostaglandin SE and interventions Fever & chills:
Temp Q1-2 hours Antipyretics
Respiratory: Wheezing, cough, bronchospasms: Auscultate lungs and treat accordingly
CV: flushing, headaches, bradycardia, arrhythmias, increased DBP, edema: Frequent assessment Correct any electrolyte imbalance ?diuretics
Metabolic: Hypocalcemia, hypokalemia or hyperkalemia, hypoglycemia: Correct electrolyte imbalance via IV
GI: N/V, diarrhea: Antiemetic &/or antidiarrheal – pre-med.
What else is Prostaglandins used for? Induction (PGE2) – cervical ripening

Late PP Hemorrhage Definition:
Hemorrhage occurs after the first 24 hours following delivery
Usually within 1-2 weeks after childbirth

Etiology: Late PP Hemorrhage Subinvolution of the placenta site (due to):
Retained placental fragments
Signs of subinvolution: Fundal height is greater than expected
Makes sure the woman ambulates and empties bladder Lochia rubra fails to progress from
RUBRA----SEROSA----ALBA Lochia rubra that persists > 2 weeks PP is highly
suggestive of subinvolution

LOCHIA FLOW

Other assessment Blood loss may be excessive, but rarely poses the same risk as
early PP hemorrhage Generalized signs of SHOCK:
Early s/s of shock: Tachycardia leading into bradycardia Thready pulse Shallow respirations hypotension
Late s/s of shock: Cool, clammy Pale skin “Air hunger” May lapse into unconsciousness Death without proper interventions

Treatment D&C: Removal of retained fragments Fluid replacement Possible blood transfusion Fe supplementation Antibiotic therapy

NURSING VS – How often? Externally massage uterus to stimulate
contractions (DON’T overmassage) Stimulate contractions
Express any clots – gentle downward pressure ABCs:
Assess airway and breathing Oxygen supplementation (6-8L via mask) Maintain O2 saturation >95%

NURSING Strict I&O
Maintain urine output >30cc/h (adult) Possibly insert Foley catheter Assess for need of IV fluid boluses
Monitor CVP if CVL in place Normal 10-12 mmHg Monitor for intravascular depletion
CBC: H/H Observe if Hct is <30 Transfuse if Hct is <21
Rest

INFECTION

INFECTION Description
Any infection of the reproductive organs that occurs within 28 days of delivery or abortion
Categories of Infections: Puerperal infection: overall category
An infection of the reproductive tract associated with childbirth that occurs up to 6 weeks PP
1) Endometritis or metritis 2) Pelvic cellulites / Parametritis 3) Peritonitis 4) Salpinitis


PUEPERAL INFECTIONS Infection of the reproductive tract associated with childbirth Occurs any time up to 6 weeks PP Standard definition of puerperal morbidity:
Temperature =>38.0 C (100.4F) - check hospital policy Occurring on any 2 of the first 10 PP days excluding the first 24
hours The vagina and cervix of approximately 70% of all healthy
pregnant women contain pathogenic bacteria that are sufficiently virulent to cause excessive infection Other factors MUST be present for infection to occur Pathogens may include:
Proteus mirabills, Pseudomonas, Clostridium, E. coli, Strep., Staph., Perfingins………..

PREVENTION of infection GOOD HYGIENE!!!!!!! PREVENT cross-bacterial contamination! Aseptic technique Proper use of peri-bottle Do not use fingers to separate labia Limit vaginal exam to two during L&D Masks, hats and gloves in DR Proper nutrition Decrease PP stress

1) ENDOMETRITIS / METRITIS Inflammation of the endometrium 48-72
hours post-delivery Placental site (after the expulsion of
placenta) provides an excellent culture media for bacterial growth
Causative organisms: Genital mycoplasm Chlamydia trachomatis*

Signs / Symptoms Lochia: reddish-brown with FOUL odor
(if infection caused by beta-hemolytic strep, lochia may be odorless)
Temp >100 with “high’s and lows” in terms of temperature spikes……. Chills
CBC: Elevated WBC Tachycardia Headaches, malaise Anorexia Backache Prolonged after-pains with enlarged, tender uterus

TREATMENT HIGH FOWLER’S POSITION!!!!!
Prevent spreading Promote drainage….. gravity
Antibiotics Increase fluids Oral oxytocics (increase contractions), i.e. Metergin PO Rest “Isolation” …… private room STOP “direct” breastfeeding:
Preserver energy Express milk mechanically/manually to prevent loosing
production

2) PELVIC CELLULITIS / PARAMETRITIS Infection involving the connective tissue of the
broad ligament …….. OR In more severe cases, the connective tissue of
ALL the pelvic structures Ascending infection in the pelvis by way of the
LYMPHATICS in the uterine wall May also occur if pathogenic organisms invade a
CERVICAL LACERATION that extend upward = DIRECT PATHWAY INTO THE PELVIS

Signs and Symptoms High fevers: 102-104 F (39-40C) Chills Tachycardia Malaise, lethargy Abdominal pain Subinvolution of the uterus Local and referred rebound tenderness **

Treatment Obtain blood cultures for sensitivity Antibiotics Monitor fluid status: I&O Pain management: Analgesics HIGH FOWLER’S POSITION I&D for abscess in cul-de-sac of Douglas to
prevent rupture of fluid

3) PERITONITIS “Infection spreading through the lymphatics” Involves the peritoneal cavity:
Uterine ligaments Cul-de-sac of Douglas Subdiaphragmatic space
S/S: ACUTELY ILL!!!!! Severe pain, high fevers, altered respiratory status (rapid /
shallow), tachycardia, excessive thirst, N/V, abdominal distension and marked anxiety
Treatment: Same as with parametritis

4) SALPINGITIS Tubal infection: Fallopean tubes Always a risk of INFERTILITY as a result of occlusion of the
fallopean tubes Cause:
Ascending infection S/S:
ACUTELY ILL!!!! ----- similar to peritonitis Treatment:
Antibiotics Analgesics and sedatives to promote rest Fluid – I&O



THROMBO EMBOLIC DISEASE

THROMBOPHLEBITIS Thrombus = clot Phlebitis = inflammation of the wall of a
vein Inflammation of a vein with clot formation Usually firmly attached to vessel wall Thrombophlebites versus phleothrombosis

Thrombophlebitis: INFLAMMATORY Thrombus formed secondary to inflammation of the vein
wall More firmly attached (decreased risk of “traveling”) No embolism (only if in pelvis)
Phleothrombosis = venous thrombosis NON-INFLAMMATORY Clot formed by venous stasis More loosely attached (increased risk of “traveling”) Increased risk for embolism

Increased risk with: DIC Anemia Existing varicose veins ---- venous stasis Increased blood clotting factors Thrombocytosis: Increased platelets (viscous) Release of thromboplastin: from the tissue of the
decidua placenta and fetal membranes Increased amounts of fibrinolysis inhibitors

Risks (continued) Increased maternal age >30 years Obesity Multiparity Endometritis Anesthesia and surgery with trauma to vessels Existing cardiac disease (Previously: estrogen for supression of lactation)

Different types: Superficial Thrombophlebitis Femoral Thrombophlebitis Pelvic Thrombophlebitis

Superficial Thrombophlebitis More common PP than during pregnancy Clot often involves the smaller saphenous veins Common in women with pre-existing varicose
veins S/S: Usually present after 3-4 days PP
Tenderness and pain in the affected lower extremity Positive Homan sign Warm and pinkish-red color over thrombus area Palpable thrombus that feels bumpy and hard Slightly elevated pulse rate Temperature normal to low grade fever

Superficial Thrombophlebitis

Treatment: Local heat Elevate affected leg Bedrest, analgesics Ted stocking or venodyne boots
Yes, verified that even with thrombus they are used!!!!! Usually NOT anticoagulant unless complications develop
(remember, embolism is EXTREMELY RARE) Occasionally the involved veins have incompetent
valves and as a result, the problem may spread to the deeper leg veins such as the femoral vein……….

Femoral & pelvic thrombophlebitis Included in the overall category DVT More frequently seen in women with history
of thrombosis Obstetrical complications (hydramnios, PIH
and C/S are putting women at risk

Signs and symptoms: Depends on the vein involved
Femoral: Chills and fever Malaise Pain, stiffness, and swelling of the affected leg Shiny, white skin over the affected area Homans’ sign is usually NEGATIVE but in some cases
may be positive (depending on the vein involved) Diminished peripheral pulses
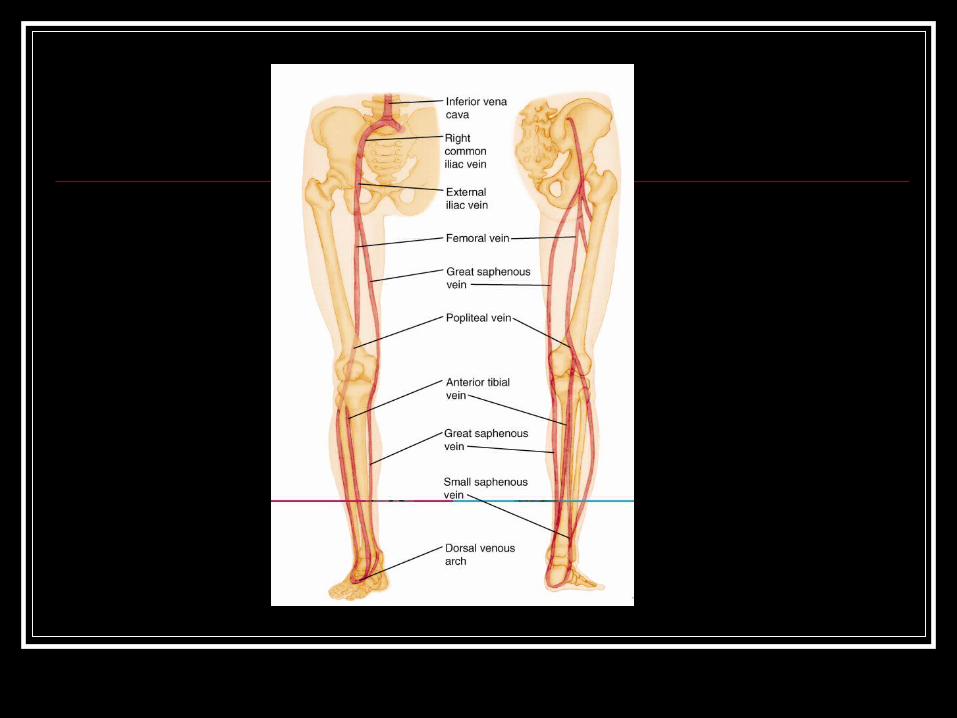
Popliteal: Pain in popliteal and lateral tibial area
Anterior and posterior tibial veins: Pain in ENTIRE lower leg and foot
Iliofemoral veins: Pain in LOWER ABDOMEN
OVERALL s/s: Fever is usually LOW GRADE Homan sign is USUALLY NEGATIVE but may in some cases be
positive. Pain is often the result from calf pressure Pale and cool limb to touch due to reflex arterial spasm:
Referred to as “MILK LEG” or “PHLEGMASIA ALBA DOLENS” Peripheral pulses decreased

Deep Vein Thrombosis

TREATMENT Assess lower extremities for edema, tenderness,
varices, and increased skin temperature Evaluate legs for Homans’ sign by extending the legs
with the knees slightly flexed and dorsiflexing the foot Maintain bedrest – activity can loosen clot Elevate the affected leg Apply a bed cradle and keep bedclothes off affected
leg; TED stockings or Venodyne boots NEVER massage the leg or “try to stretch it out” Monitor for manifestations of pulmonary embolism

Specific treatment for conditionsSuperficial Thrombophlebitis
Provide rest Elevate affected leg Apply hot packs to the affected site as
prescribed Apply elastic stockings or Venodynes Administer analgesics as prescribed

Femoral Thrombophlebitis Provide bedrest Elevate affected leg Apply moist heat continuously to affected area if
prescribed to alleviate discomfort Administer analgesics as prescribed Administer antibiotics if prescribed Prepare to administer intravenous heparin to
prevent further thrombus formation if prescribed

Pelvic Thrombophlebitis Provide bedrest Administer analgesics as prescribed Administer antibiotics if prescribed Prepare to administer intravenous
heparin if prescribed

THROMBOPHLEBITIS

Pelvic Thrombophlebitis Affects the uterine veins and ovarian veins Usually later occurrence: 2nd PP week Usually caused by anaerobic strep organism S/S:
High fevers and severe chills Dramatic body temperature changes The occurrence of pulmonary embolism may be the first
sign: Dyspnea, SOB, desaturation, chest pain (unilateral)

Treatment: Anticoagulants:
Heparin (antidote = Protamine) Coumadin (antidote = Vitamin K)
Antimicrobial: Based on C&S Broad spectrum to start with
Transfusions: PRBC for decreased hematocrit/hemoglobin

CLIENT EDUCATION FOR THROMBOPHLEBITIS PREVENTION!!! Avoid pressure behind the knees Avoid prolonged sitting Avoid constrictive clothing i.e. knee-highs Avoid crossing the legs…… only at ankles Elevate legs, including foot of bed Never massage the leg Ambulate ASAP PP or do PROM in bed How to apply support hose if prescribed The importance of anticoagulant therapy as prescribed The importance of follow-up

Discharge teaching for Coumadin S/S of bleeding: Call MD/CMW immediately
Gums, epistaxis, petechia/ecchymosis, melena (blood in stool), hematuria
Avoid aspirin and NSAID: Aspirin, advil, ibuprofin, motrin, etc
Keep appointments for lab studies PT (Normal = 11-15 seconds) PTT (Normal = 30-40 seconds) Goal: stretch PT to 1 - 1 1/2 times normal (16-21 seconds) in
order to prevent clotting *** NO BREASTFEEDING when on COUMADIN***
Pregnancy risk category X

PULMONARY EMBOLISM Description
The passage of thrombus, often originating in one of the uterine or other pelvic veins, into the lungs, where it disrupts the circulation of blood
Fat, blood, air or debris


PULMONARY EMBOLISM Assessment:
Dyspnea (usually sudden onset) Tachypnea Cough, rales Tachycardia Pallor, cyanosis SOB, chest pain Pressure in bowl / rectum Arrhythmia (gallop) Hemoptysis Pleuritic chest pain Feeling of impending doom – “fear of death”
PULMONARY EMBOLISM Implementation:
Administer oxygen as prescribed Position client with the head of the bed elevated to promote comfort Monitor vital signs frequently Treat arrhythmias according to the origin Frequently assess respiratory rate, breath sounds, and for signs of
increasing hypoxemia Monitor for signs of respiratory distress as tachypnea, tachycardia,
restlessness, cool and clammy skin, cyanosis, and the use of accessory muscles
Treat respiratory conditions: bronchodilators (Albuterol, Xopenex), antispasmodics (racemic epinephrine)

Treatment continued Pain management: opioids (Morphine = respiratory
depression; Demerol) Increase IV fluids as prescribed Administer anticoagulants as prescribed Prepare to assist physician to administer
streptokinase to dissolve the clot if prescribed Now often Alteplase is used instead
Last resort: embolectomy

SUBINVOLUTION OF UTERUS Description
Incomplete involution or failure of the uterus to return to its normal size and condition
Cause Infection Retained placenta fragments

Assessment Uterine pain on palpation Uterus is larger than expected Fundus is higher in the abdomen Greater than normal vaginal bleeding Lochia does not follow normal pattern i.e.:
RUBRA – SEROSA -- RUBRA Backache Leucorrhea if infection (white, creamy discharge)

Implementation Assess vital signs, uterus, and fundus Monitor for vaginal bleeding Elevate the legs to promote venous return Encourage frequent voiding Monitor hemoglobin and hematocrit Prepare to administer methylergonovine maleate
(Methergine) or ergonovine maleate (Ergotrate) as prescribed

Treatment Methergin 0.2 mg Q3-4H PO for 24-48 hours Antibiotics Possibly D&C
Nursing interventions Medications as ordered Assessment of fundus Safety and comfort needs

MASTITIS Description
Inflammation of the breast as a result of infection Primarily seen in breast-feeding mothers 2 to 4 weeks after
delivery
Cause Staph aureus Hemolytic strep How it is transmitted:
Baby’s nose and throat Mother’s or health care providers’ hands Cracked nipples

MASTITIS Assessment
Localized heat and swelling Pain: redness, warmth and firm to touch with areas of
lumpiness Elevated temperature and chills Tachycardia Headache Complaints of flu-like symptoms

MASTITIS Implementation
Promote comfort of the client Instruct mother in good hand-washing and breast hygiene Apply heat to enhance inflammatory process (kill microbes) Maintain lactation in breast-feeding mothers Encourage manual expression of breast milk or use of breast
pump every 4 hours REMEMBER, during EARLY stages of mastitis, the mother is
encouraged to breast-feed DIRECTLY Encourage mother to support breasts with supportive bra Administer analgesics as prescribed Administer antibiotics as prescribed Possibly I&D

MASTITIS

Urinary Tract Infections Description
An infection of the urinary tract / bladder Caused by:
Decreased bladder sensitivity Increased bladder capacity to accommodate
increased blood volume Inhibitory neural control of bladder after
anesthesia Poor sterile technique with catheterization Residual problems = stasis

Assessment Burning and pain on urination Lower abdominal pain Increased frequency of urination Costovertebral angle tenderness (“flank pain”) Fever Proteinuria, hematuria, bacteriuria, WBCs in urine

Nursing Void within 6-(8) hours PP (if not, straight cath.) Assess bladder status – distension Assess perineum
Edema Injuries
If Foley catheterization Assess urine output and if >750cc during catheterization, clamp X
30 minutes and reassess Send urine for:
Urinalysis, C&S

Common UTI’s in PP clients Pyelonephritis
Infection of the kidney pelvis S/S:
High fevers, chills Flank pain N/V
Treatment: Antibiotics based on C&S Bedrest Increase fluid intake, I&O Analgesics Antispasmodics (Ditropan) Empty bladder and change pads frequently Teaching and follow-up care

Cystitis Infection of the bladder S/S:
Dysuria at end of urination Urgency and frequency Low grade fever Hematuria CBC: abnormal number of leukocytes and bacteria
Treatment: Sulfa drugs: trimethoprim/trimethoprim,
sulfamethoxazole/sulfisoxazole (Bactrim) Ciprofloxacin is commonly used today
Nursing: Teach good hygiene: Wipe front to back Increase fluid Acid fluids such as Cranberry juice and Vitamin C Antibiotic therapy
VULVAR HEMATOMA Description
The formation of a hematoma following the escape of blood into the tissues of the reproductive sac after the delivery
Predisposing conditions include operative delivery with forceps or injury to a blood vessel
A life-threatening condition

Assessment Abnormal severe pain; pressure in perineal area,
including rectal pressure Sensitive “tumor” / “cyst” in perineal area with
discolored skin Inability to void Palpable tumor Reddish or blue discoloration of the skin Decreased hemoglobin and hematocrit (H&H) Signs of shock such as pallor, tachycardia, and
hypotension if significant blood loss has occurred

VULVAR HEMATOMA Implementation
Monitor vital signs Monitor client for abnormal pain especially when
forceps delivery has occurred Place ice to the hematoma site followed by warm sitz
baths later (general rule: Ice X 12-24 hours, then heat)
Administer analgesics as prescribed Monitor I&O Encourage fluids Encourage voiding

HEMATOMA Implementation
Prepare for urinary catheterization if client is unable to void
Administer blood replacements as prescribed Monitor for signs of infection such as increased
temperature, pulse rate, and WBC count Administer antibiotics as prescribed as infection is
common following hematoma formation Prepare for incision and evacuation of hematoma if
necessary

HEMATOMA

THE END!!!


















