post insertion proplem in complete denture 2016
51
-
Upload
ali-al-karawey -
Category
Education
-
view
44 -
download
4
Transcript of post insertion proplem in complete denture 2016


Ahmed haiderMohammed hassan aliMohammed abd almortafeaMuntadher abd alnaserAli ihsanAli jasimAmeer Basheer
Dr. Hussein Almasoodi

comfort esthetics common
phonetic function Un common
Classification of post insertion problem


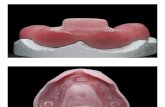
Sore spot :in vestibule, posterior limit of maxillary denture , soreness over ridge , under labial and lingual flanges .
Causes and treatment :1- overextension of borders or flanges T/ : Adjust denture borders using disclosing wax 2- high occlusion in certain area T/ : Adjust occlusion using articulating paper

3- unpolished or sharp edge T/: polish denture borders

Burning sensation 1- ant. Hard palate and ant. Alveolar ridge Cause : pressure over anterior palatine foramen 2- upper posterior ridgeCause : pressure over posterior palatine foramen
3- lower ant. Ridge Cause : pressure on mental foramen
Treatment : Relief the area over foramen

Redness :1- All tissue contact by denture (denture stomatitis)Cause: denture base allergy Treatment : remake the denture use metallic denture base


Pain in TMJ :Cause 1 :Insufficient vertical dimension of occlusion Treatment : increase vertical dimension .
Cause 2 : arthritis Treatment : analgesics


Gaging :
A- Immediately upon denture placement :
Maxillary : - over extension on palate - Too thick posterior border Mandibular : the flange is too thick .
Treatment : adjust the denture and remove thickness .Psychogenic factors : treated by prescribe a mild tranquilizer .

B- Delayed for 2 weeks or months :
- Incomplete border seal allowing saliva to enter under the denture Treated by : improve border seal .
- Faulty occlusion causing denture to loosen Treated by : correct occlusion .

Tongue and cheek biting : cause 1 : loss of muscle tonus(lax cheek) leads to cheek bitingT/ build out thin denture base or extent the under-extended borders Cause 2 : Over closureT/ restore the vertical dimension .
Cause 3 : Tongue biting may occur in patient with epilepsyT/ treat the cause .

Cause 4 : Change in the occlusal plan leading to cheek and tongue bitingT/- new denture with proper occlusal height
Cause 5 : posterior teeth too far lingually leading to tongue bitingT/ re-establish adequate tongue space .
Cause 6 : posterior teeth too far bucally leading to cheek biting T/ re-contour the buccal surface.

Fatigue of the muscles of mastication :
Caused by problem in Vertical dimension
A- excessive vertical dimension of occlusion Treatment : reduce vertical dimension
B- insufficient vertical dimension of occlusionTreatment : increase vertical dimension

Swallowing and sore throat :
A- maxillary denture Cause and treatment - posterior border is over extension or too thick * Adjust posterior border

B - mandibular denture Cause and treatment - overextension of the posterior lingual flange area - too thick lingual posterior flange . * reduce thickness or adjust posterior lingual flange area
C- Decrease vertical dimension of occlusion .* increase vertical dimension

D- excessive vertical dimension of occlusion
* reduce vertical dimension
E- posterior teeth set Lingually (tongue is crowded )
* re- set teeth in correct position

Difficulty in swallowing and eating

• Over extended mandibular denture in the retromylohyoid area
• Increased vertical dimension of Occlusion

Unstable dentures. Check thatretentive forces are maximized anddisplacing forces minimized and allavailable support has been used

Check for over extension and correctAccordingly
Construct dentures to maximizeretention and minimize displacingforces.

Cannot open mouth wide enough for food .

Excessive OVD

Can remove up to 1.5 mm fromocclusal plane by grinding, but ifmore is required, remake dentures

clicking

1_excessive vertical dimension Treat/reduse vertical dimension
2_denture with poor retention Treat/rebasing and remarking the denture
3_ cuspal interference Treat/ eliminate cuspal interference

4_excessive incisal guidanceTreat/correction occlusion

Dislodgement of maxillary denture during function

Overfilled buccal vestibule.T/ Allow proper flange thickness

Over extension in the hamular notch area.T/correct border extention.

Inadequte notches for frenum attachment.T/Allow sufficient clearance for frenum attachments

Placing the maxillary anterior teeth too far labial.T/Reset the teeth .
Lack of occlusal haemony.T/Correct occlusal disharmony by selective grinding

When talkingInadequate posterior palatal seal.T/Increase posterior palatal seal with auto-polymerizing acrylic resin

When talkingOverextension in the posterior regionT/Adjust the posterior overextention


PHONETIC Speech problems Uncommon, but• presence is of great concern to
patient.• May affect sibilant (eg s),
bilabial• (eg p,b), labiodental (eg f.v)

Cause may not be obvious. May be check that problem not present with old dentures

Check for vertical dimension accuracy, and that vertical incisor overlap not excessive. Palatal contour should not allow excessive tongue contact or air leakage - assess using disclosing paste over denture palate while sound is made. It is recommended that thePatient, s speech is assessed at trialinsertion visit

Dentures making clicking sound when the patient tries to speak

This is the result of increased vertical dimension of occlusion

If the increase is slight, correct it using selectivegrinding. If the increase is gross, remaking of thedentures may be required

phonetic• Whistling• When the patient wears the denture for the
first time, the patient may complain of whistling while talking which could be because of increased palatal vault depth and compressed arch form.
• Failure to duplicate the rugae could also lead to this problem

Lowering the palatal contour should help the condition.




Blunt teeth

• Broad posterior occlusal surfaces which replaced narrow teeth on previous denture.
• Non anatomical type teeth used where cusped teeth previously used