Positional-dependent changes in glenohumeral joint contact pressure and force: Possible...
6
Positional-dependent changes in glenohumeral joint contact pressure and force: Possible biomechanical etiology of posterior glenoid wear Ranjan Gupta, MD, a,b and Thay Q. Lee, PhD, a,b Long Beach and Irvine, CA The purpose of this study was to simulate the forces in the individual periscapular muscles and investigate the possi- ble biomechanical etiology of posterior erosion of the glenoid. Twelve fresh-frozen human cadaveric shoulders were used with a custom shoulder jig that uses indepen- dently controlled pneumatic cylinders to apply forces across the tendon of each muscle. The simulated muscle forces included the rotator cuff, the deltoid, the latissimus dorsi, and the pectoralis major. The shoulders were tested in 12 overhead activity positions. A 6 – degree-of- freedom load cell was used to measure the glenohumeral joint forces, and the glenohumeral contact pressures and areas were measured by use of Fuji pressure-sensitive film. There were no significant differences in glenohu- meral joint forces between 60° and 90° of vertical ab- duction or between 60° and 90° of external rotation. At 70° of horizontal adduction from the scapular plane, there was a significant decrease in superior force, a sig- nificant increase in posteriorly directed force, and a sig- nificant decrease in compression when compared with 30° and 50° of horizontal adduction (P .05). Similar statistical trends were seen for 60° of vertical adduction. For the glenohumeral contact area and pressure, a signif- icant decrease in contact area was seen between 30° of horizontal adduction and 70° of horizontal adduction for both 60° and 90° of vertical adduction (P .05). A sig- nificant increase in contact pressure was seen at 70° of horizontal adduction compared with 50° and 30° (P .05). The contribution of the humerothoracic muscles is significant and should be considered for proper restora- tion of glenohumeral joint biomechanics. Furthermore, asymmetric loading with excessive or repetitive overhead activities may eventually lead to posterior glenoid ero- sion. (J Shoulder Elbow Surg 2005;14:105S-110S.) A s the glenohumeral joint has a tremendous range of motion, it also has a tremendous propensity for instability that is resisted with a combination of active and dynamic joint stabilizers. The dynamic stabilizers are primarily the 4 muscles of the rotator cuff and the long head of the biceps. These muscles serve not only to provide joint stability but also to transmit joint reaction forces that directly affect glenohumeral biomechanics. Along with the deltoid and other humerothoracic muscles, these muscles influence both glenohumeral biomechanics and gle- nohumeral contact area and pressures throughout the shoulder’s range of motion. Several anatomic biomechanical studies have evaluated the effect of altering the magnitudes of muscle forces across the glenohumeral joint. 1,5,8,9,15,18,19 These studies have shown that the magnitude of glenohumeral joint reaction forces varies according to both the position of the glenohumeral joint and the ratio of forces between the supraspinatus and deltoid mus- cles. Other investigators have reported that the glenohumeral joint has a slight articular mismatch when the normal shoulder is adducted, producing reduced contact area. 25 As the shoulder is ab- ducted to 90°, the joint becomes more congruent with a subsequent increase in joint contact area. 25 Furthermore, there is a shift in glenohumeral con- tact area posteriorly with increasing forward flex- ion of the glenohumeral joint. 22 These data all point to the idea that there are positional-dependent changes in glenohumeral joint force, contact area, and contact pressure. Alterations in joint forces, contact area, and contact pressure have been implicated in the development of arthritis in other joints such as the hip and knee. In a recent study from Japan, the incidence of primary gle- nohumeral arthritis was reported to be 0.4% in the patients with orthopaedic issues and 4.6% in the pa- tients who had shoulder diseases, with glenohumeral arthritis, which causes both pain and disability, devel- From the Orthopaedic Biomechanics Laboratory VA Long Beach Healthcare System, a and University of California Irvine. b This work was supported in part by the John C. Griswold Founda- tion and Veterans Affairs Rehabilitation Research and Develop- ment. Reprint requests: Thay Q. Lee, PhD, Orthopaedic Biomechanics Laboratory, Long Beach VA Healthcare System (09/151), 5901 E 7th St, Long Beach, CA 90822 (E-mail: [email protected]). Copyright © 2005 by Journal of Shoulder and Elbow Surgery Board of Trustees. 1058-2746/2005/$30.00 doi:10.1016/j.jse.2004.10.005 105S
-
Upload
ranjan-gupta -
Category
Documents
-
view
215 -
download
0
Transcript of Positional-dependent changes in glenohumeral joint contact pressure and force: Possible...

Ppp
R
Tibgwdafdtfjafimd7tnn3sFihbnh.st
F
T
R
C
1d
ositional-dependent changes in glenohumeral joint contactressure and force: Possible biomechanical etiology ofosterior glenoid wear
anjan Gupta, MD,a,b and Thay Q. Lee, PhD,a,b Long Beach and Irvine, CA
aas
AoiascstgaintbaghjpfcgwrdwFtitca
parnpt
he purpose of this study was to simulate the forces in thendividual periscapular muscles and investigate the possi-le biomechanical etiology of posterior erosion of thelenoid. Twelve fresh-frozen human cadaveric shouldersere used with a custom shoulder jig that uses indepen-ently controlled pneumatic cylinders to apply forcescross the tendon of each muscle. The simulated muscleorces included the rotator cuff, the deltoid, the latissimusorsi, and the pectoralis major. The shoulders were
ested in 12 overhead activity positions. A 6–degree-of-reedom load cell was used to measure the glenohumeraloint forces, and the glenohumeral contact pressures andreas were measured by use of Fuji pressure-sensitivelm. There were no significant differences in glenohu-eral joint forces between 60° and 90° of vertical ab-uction or between 60° and 90° of external rotation. At0° of horizontal adduction from the scapular plane,
here was a significant decrease in superior force, a sig-ificant increase in posteriorly directed force, and a sig-ificant decrease in compression when compared with0° and 50° of horizontal adduction (P � .05). Similartatistical trends were seen for 60° of vertical adduction.or the glenohumeral contact area and pressure, a signif-cant decrease in contact area was seen between 30° oforizontal adduction and 70° of horizontal adduction foroth 60° and 90° of vertical adduction (P � .05). A sig-ificant increase in contact pressure was seen at 70° oforizontal adduction compared with 50° and 30° (P �05). The contribution of the humerothoracic muscles isignificant and should be considered for proper restora-ion of glenohumeral joint biomechanics. Furthermore,
rom the Orthopaedic Biomechanics Laboratory VA Long BeachHealthcare System,a and University of California Irvine.b
his work was supported in part by the John C. Griswold Founda-tion and Veterans Affairs Rehabilitation Research and Develop-ment.
eprint requests: Thay Q. Lee, PhD, Orthopaedic BiomechanicsLaboratory, Long Beach VA Healthcare System (09/151), 5901E 7th St, Long Beach, CA 90822 (E-mail: [email protected]).opyright © 2005 by Journal of Shoulder and Elbow SurgeryBoard of Trustees.
058-2746/2005/$30.00
aoi:10.1016/j.jse.2004.10.005symmetric loading with excessive or repetitive overheadctivities may eventually lead to posterior glenoid ero-ion. (J Shoulder Elbow Surg 2005;14:105S-110S.)
s the glenohumeral joint has a tremendous rangef motion, it also has a tremendous propensity fornstability that is resisted with a combination ofctive and dynamic joint stabilizers. The dynamictabilizers are primarily the 4 muscles of the rotatoruff and the long head of the biceps. These muscleserve not only to provide joint stability but also toransmit joint reaction forces that directly affectlenohumeral biomechanics. Along with the deltoidnd other humerothoracic muscles, these muscles
nfluence both glenohumeral biomechanics and gle-ohumeral contact area and pressures throughouthe shoulder’s range of motion. Several anatomiciomechanical studies have evaluated the effect ofltering the magnitudes of muscle forces across thelenohumeral joint.1,5,8,9,15,18,19 These studiesave shown that the magnitude of glenohumeraloint reaction forces varies according to both theosition of the glenohumeral joint and the ratio oforces between the supraspinatus and deltoid mus-les. Other investigators have reported that thelenohumeral joint has a slight articular mismatchhen the normal shoulder is adducted, producing
educed contact area.25 As the shoulder is ab-ucted to 90°, the joint becomes more congruentith a subsequent increase in joint contact area.25
urthermore, there is a shift in glenohumeral con-act area posteriorly with increasing forward flex-on of the glenohumeral joint.22 These data all pointo the idea that there are positional-dependenthanges in glenohumeral joint force, contact area,nd contact pressure.Alterations in joint forces, contact area, and contact
ressure have been implicated in the development ofrthritis in other joints such as the hip and knee. In aecent study from Japan, the incidence of primary gle-ohumeral arthritis was reported to be 0.4% in theatients with orthopaedic issues and 4.6% in the pa-
ients who had shoulder diseases, with glenohumeral
rthritis, which causes both pain and disability, devel-105S

oppotAcldpgtttglhwTs
mmsimhtigmsgot
M
tdbr
oadrwhetmwdtNltN
p9hw9lfrnrz
alpcg22ops2mrlWrtptsuN(ptacpdww
FD
106S Gupta and Lee J Shoulder Elbow SurgJanuary/February 2005
ping in a large number of patients.16 Over time, inatients with glenohumeral arthritis, asymmetric wearatterns of the glenoid will often develop. With primarysteoarthritis of the shoulder, this asymmetric wear pat-
ern often manifests as posterior glenoid erosion.14,23,24
lthough the surgical reconstruction of this pathologicondition has been of recent interest, there remains aimited understanding as to why this pathology actuallyevelops. Recently, Walch et al23,24 performed a mor-hologic study on the glenoid in patients with primarylenohumeral arthritis. After analysis of the computed
omography scans from 113 patients with primary os-eoarthritis of the shoulder, they came to the conclusionhat the position of the humeral head with respect to thelenoid is an important predictor of glenoid morpho-
ogic evolution. Posterior subluxation of the humeralead would lead to asymmetric loading of the glenoid,hich may eventually lead to posterior glenoid wear.his still leaves the question as to why there is posteriorubluxation of the humeral head.
Most studies that have studied glenohumeral bio-echanics have focused on the midrange of glenohu-eral motion. Previous work from our group has
uggested that there are position-dependent changesn glenohumeral joint contact pressures and force thatay be responsible for posterior subluxation of theumeral head and the eventual development of pos-erior glenoid wear. The hypothesis of this study is thatncreasing degrees of horizontal adduction at thelenohumeral joint have profound effects on glenohu-eral joint forces, contact areas, and contact pres-
ures. As such, we evaluated the biomechanics of thelenohumeral joint in 12 positions that simulatedverhead activities and evaluated the role of horizon-
al adduction in glenohumeral joint biomechanics.
ATERIALS AND METHODS
Twelve fresh-frozen human cadaveric shoulders wereested by use of a well-established custom shoulder-testingevice with simulated muscle forces (Figure 1), which haseen described in detail recently.13,21 Before dissection,
igure 1 Photograph of custom shoulder-testing system. DOF,egrees of freedom.
adiographs were obtained to exclude any specimen with A
sseous pathology or soft-tissue abnormality. All soft tissuesround the shoulder were removed, and the muscles wereetached from their scapular origins. The tendons of theotator cuff, deltoid, latissimus dorsi, and pectoralis majorere preserved for all specimens. Any specimen noted toave a deficient rotator cuff at the time of dissection wasxcluded from the study. Osseous structures preserved werehe proximal humerus and the scapula, including the acro-ion and coracoid. For biomechanical testing, the scapulaas fixed to the custom shoulder jig, which uses indepen-ently controlled pneumatic cylinders to apply forces across
he tendon of each of the muscle forces simulated. Fortyewtons of force was applied through the pectoralis major,
atissimus dorsi, and each of the rotator cuff muscles withhe exception of the deltoid, which was loaded with 80.13
The shoulders were tested in 12 different glenohumeralositions that simulate overhead activities. Both 60° and0° of shoulder abduction and 30°, 50°, and 70° oforizontal adduction with respect to the scapular planeere tested. These 6 positions were tested in both 60° and0° of external rotation (Figure 2). A 6–degree-of-freedom
oad cell was used to measure the glenohumeral jointorces, which were resolved into 3 orthogonal componentsepresenting anatomic directions with respect to the gle-oid. Specifically, the x-axis represents the anterior-poste-ior direction, the y-axis represents superior-inferior, and the-axis represents compression.
The measurement of glenohumeral contact pressuresnd areas was accomplished by use of Fuji Prescale super-
ow pressure–sensitive film (Fuji Photo Film Co, Tokyo, Ja-an) with a pressure range of 0.5 to 2.5 MPa. The film wasut to a custom shape to accommodate the concavity of thelenohumeral joint (Figure 3). The Fuji film is composed ofparts, a transfer sheet and a developer sheet. Each of thesheets is approximately 0.10 mm in thickness. The sheets
f Fuji film were wrapped within a polyethylene bag torotect the film from fluid. The total thickness of the pressure-ensitive film in the polyethylene bag was approximately50 �m and was shown to have a negligible effect on theeasurement of contact pressures and areas in the diarth-
odial joint.2 The transfer sheet contains a microcapsuleayer, which contains a translucent color-forming substance.
hen pressure is exerted, the microcapsules break andelease its substance so that it can come into contact withhe developer sheet. The density or shade of the color isroportional to the amount of pressure experienced be-
ween the 2 sheets. A Hewlett-Packard Desk Scan II colorcanner (Palo Alto, CA) with a resolution of 400 dpi wassed to image the Fuji film. After the image was scanned,ational Institutes of Health (NIH) Image Version 1.52
Bethesda, MD) and a Macintosh Power PC (Apple Com-uter Inc, Cupertino, CA) were used to digitize and quantify
he contact pressure and area. The scanned images werenalyzed for total contact area (in square millimeters), totalontact pressure (in megapascals), and 10% peak contactressures (in megapascals). Peak contact pressures wereefined as the mean contact pressure of the contact areaith the highest 10% contact pressure. Analysis of varianceith a P value of .05 was used for statistical analysis.
lthough the NIH recognition imaging software has a 1%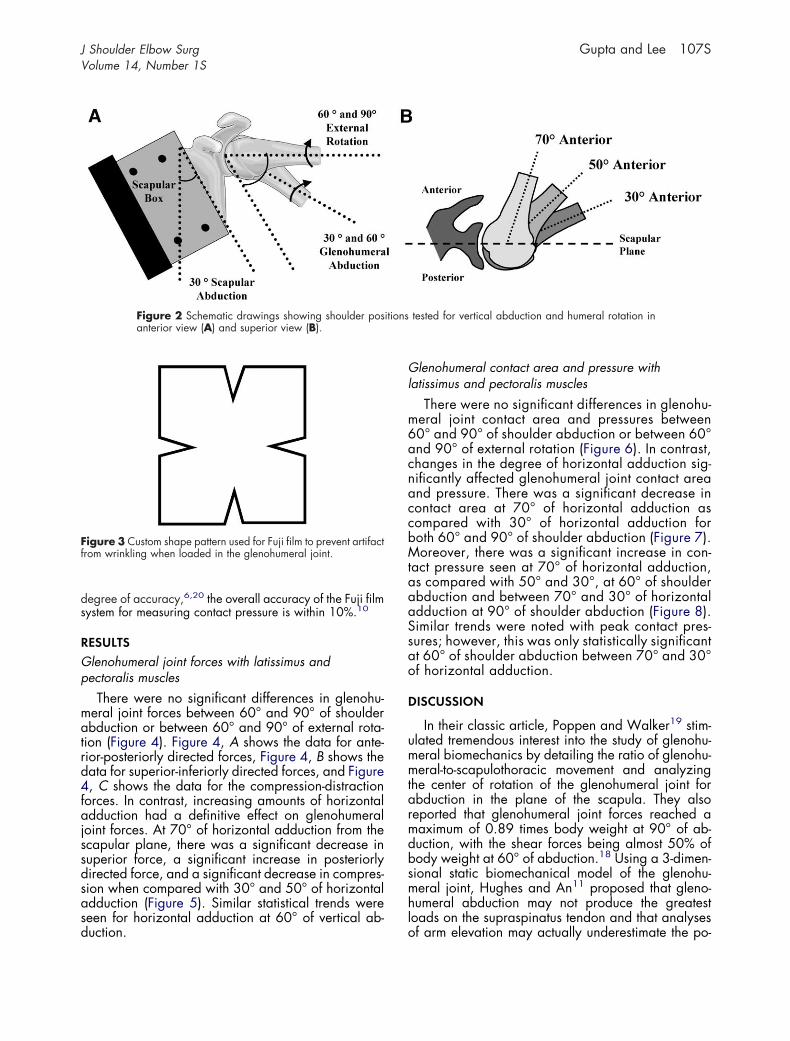
ds
RGp
matrd4fajssdsasd
Gl
m6acnaccbMtaaaSsao
D
ummtarmdbsmhl
itions
Ff
J Shoulder Elbow Surg Gupta and Lee 107SVolume 14, Number 1S
egree of accuracy,6,20 the overall accuracy of the Fuji filmystem for measuring contact pressure is within 10%.10
ESULTSlenohumeral joint forces with latissimus andectoralis muscles
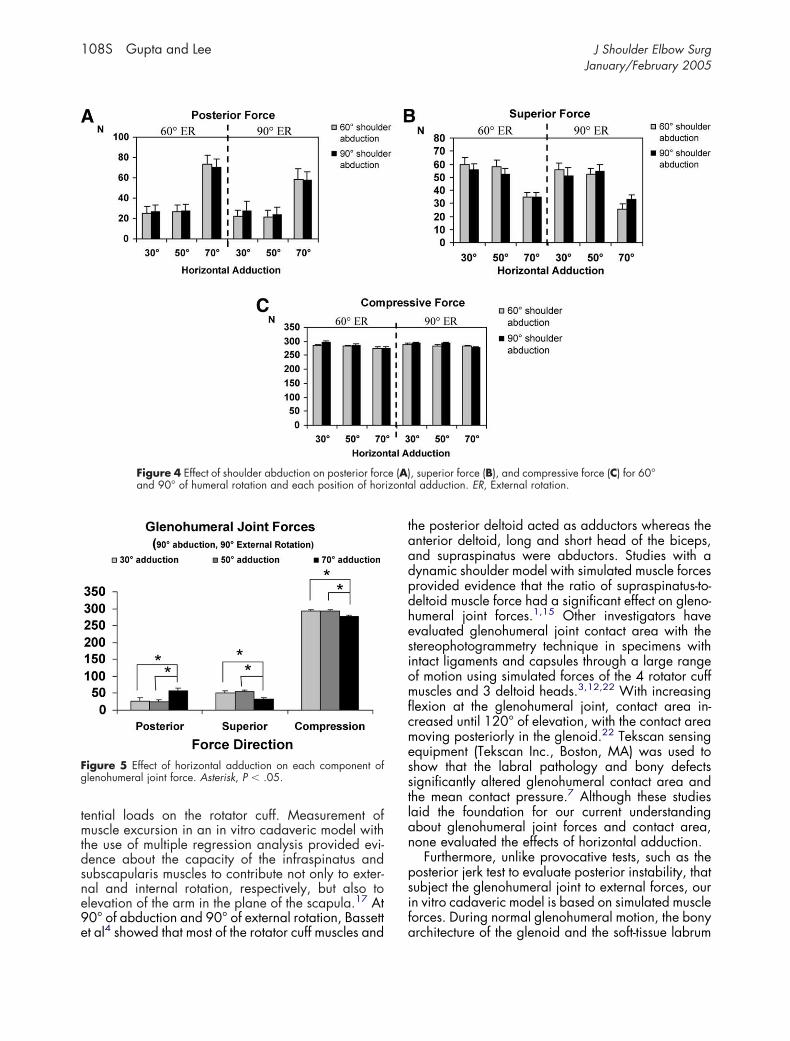
There were no significant differences in glenohu-eral joint forces between 60° and 90° of shoulderbduction or between 60° and 90° of external rota-
ion (Figure 4). Figure 4, A shows the data for ante-ior-posteriorly directed forces, Figure 4, B shows theata for superior-inferiorly directed forces, and Figure, C shows the data for the compression-distraction
orces. In contrast, increasing amounts of horizontaldduction had a definitive effect on glenohumeral
oint forces. At 70° of horizontal adduction from thecapular plane, there was a significant decrease inuperior force, a significant increase in posteriorlyirected force, and a significant decrease in compres-ion when compared with 30° and 50° of horizontaldduction (Figure 5). Similar statistical trends wereeen for horizontal adduction at 60° of vertical ab-
Figure 2 Schematic drawings showing shoulder posanterior view (A) and superior view (B).
igure 3 Custom shape pattern used for Fuji film to prevent artifactrom wrinkling when loaded in the glenohumeral joint.
uction. o
lenohumeral contact area and pressure withatissimus and pectoralis muscles
There were no significant differences in glenohu-eral joint contact area and pressures between0° and 90° of shoulder abduction or between 60°nd 90° of external rotation (Figure 6). In contrast,hanges in the degree of horizontal adduction sig-ificantly affected glenohumeral joint contact areand pressure. There was a significant decrease inontact area at 70° of horizontal adduction asompared with 30° of horizontal adduction foroth 60° and 90° of shoulder abduction (Figure 7).oreover, there was a significant increase in con-
act pressure seen at 70° of horizontal adduction,s compared with 50° and 30°, at 60° of shoulderbduction and between 70° and 30° of horizontaldduction at 90° of shoulder abduction (Figure 8).imilar trends were noted with peak contact pres-ures; however, this was only statistically significantt 60° of shoulder abduction between 70° and 30°f horizontal adduction.
ISCUSSION
In their classic article, Poppen and Walker19 stim-lated tremendous interest into the study of glenohu-eral biomechanics by detailing the ratio of glenohu-eral-to-scapulothoracic movement and analyzing
he center of rotation of the glenohumeral joint forbduction in the plane of the scapula. They alsoeported that glenohumeral joint forces reached aaximum of 0.89 times body weight at 90° of ab-uction, with the shear forces being almost 50% ofody weight at 60° of abduction.18 Using a 3-dimen-ional static biomechanical model of the glenohu-eral joint, Hughes and An11 proposed that gleno-umeral abduction may not produce the greatestoads on the supraspinatus tendon and that analyses
tested for vertical abduction and humeral rotation in
f arm elevation may actually underestimate the po-
tmtdsne9e
taadpdhesiomflcmesstlan
psif
izonta
Fg
108S Gupta and Lee J Shoulder Elbow SurgJanuary/February 2005
ential loads on the rotator cuff. Measurement ofuscle excursion in an in vitro cadaveric model with
he use of multiple regression analysis provided evi-ence about the capacity of the infraspinatus andubscapularis muscles to contribute not only to exter-al and internal rotation, respectively, but also tolevation of the arm in the plane of the scapula.17 At0° of abduction and 90° of external rotation, Bassett
Figure 4 Effect of shoulder abduction on posterior forcand 90° of humeral rotation and each position of hor
igure 5 Effect of horizontal adduction on each component oflenohumeral joint force. Asterisk, P � .05.
t al4 showed that most of the rotator cuff muscles and a
he posterior deltoid acted as adductors whereas thenterior deltoid, long and short head of the biceps,nd supraspinatus were abductors. Studies with aynamic shoulder model with simulated muscle forcesrovided evidence that the ratio of supraspinatus-to-eltoid muscle force had a significant effect on gleno-umeral joint forces.1,15 Other investigators havevaluated glenohumeral joint contact area with thetereophotogrammetry technique in specimens withntact ligaments and capsules through a large rangef motion using simulated forces of the 4 rotator cuffuscles and 3 deltoid heads.3,12,22 With increasingexion at the glenohumeral joint, contact area in-reased until 120° of elevation, with the contact areaoving posteriorly in the glenoid.22 Tekscan sensingquipment (Tekscan Inc., Boston, MA) was used tohow that the labral pathology and bony defectsignificantly altered glenohumeral contact area andhe mean contact pressure.7 Although these studiesaid the foundation for our current understandingbout glenohumeral joint forces and contact area,one evaluated the effects of horizontal adduction.
Furthermore, unlike provocative tests, such as theosterior jerk test to evaluate posterior instability, thatubject the glenohumeral joint to external forces, ourn vitro cadaveric model is based on simulated muscleorces. During normal glenohumeral motion, the bony
, superior force (B), and compressive force (C) for 60°l adduction. ER, External rotation.
e (A)
rchitecture of the glenoid and the soft-tissue labrum

adibshomlecfrjphpazda
ostcsc
sertcdeswnpof
Fj
t preduct
Fj
J Shoulder Elbow Surg Gupta and Lee 109SVolume 14, Number 1S
nd capsule provide limited restraint to posteriorlyirected forces. Rather, it is the muscle forces includ-
ng the rotator cuff, pectoralis major, long head of theiceps, and latissimus dorsi that provide dynamictability for the glenohumeral joint. These musclesave varied effects on contact pressures dependingn the joint position. We used a dynamic shoulderodel with simulated muscle forces, including the
atissimus dorsi and pectoralis major, in this study tovaluate whether there were positional-dependenthanges with glenohumeral biomechanics. The datarom this study showed limited effects of both externalotation and abduction on not only glenohumeraloint forces but also glenohumeral contact area andressure. In direct contrast, increasing degrees oforizontal adduction at the glenohumeral joint hadrofound effects on glenohumeral joint forces, contactreas, and contact pressures. With increased hori-ontal adduction, there is a decrease in superiorlyirected and compressive forces. Strikingly, there is
Figure 6 Effect of shoulder abduction on mean contacof humeral rotation and each position of horizontal ad
igure 7 Effect of horizontal adduction on mean glenohumeraloint contact pressure. Asterisk, P � .05. ER, External rotation.
lso an increase in posteriorly directed forces. Rigor- o
us analysis of glenohumeral contact areas and pres-ures showed that external rotation and abduction ofhe glenohumeral joint had little effect. Again, in-reased shoulder adduction revealed a statisticallyignificant decrease in contact area and increase inontact pressure.
The limitation of this study is that it was a cadaverictudy with simulated muscle forces in a static loadingnvironment. In addition, all shoulders were able toeach required testing positions without any limita-ion; the range of motion and the laxity for eachadaveric shoulder were not documented. Theseata, however, provide a possible biomechanicalxplanation as to why there is posterior wear in nativehoulders with glenohumeral arthritis and posteriorear after glenohumeral joint arthroplasty. Duringormal activities of daily life, individuals routinelylace their arms in space so that they may reachverhead. Wheelchair-bound individuals must per-orm this motion more regularly. On the basis of our
igure 8 Effect of horizontal adduction on mean glenohumeraloint contact area. Asterisk, P � .05. ER, External rotation.
ssure (A) and mean contact area (B) for 60° and 90°ion. ER, External rotation.
bservations (Jacqueline Perry, MD, personal commu-

ntscp7oorahTcwap
gaotdpim
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
110S Gupta and Lee J Shoulder Elbow SurgJanuary/February 2005
ication), we tested specimens in 12 different posi-ions that simulated overhead activities. Our datahowed that there was always a statistically signifi-ant difference when comparing the biomechanicalarameters at 70° versus 30° of adduction. Although0° of horizontal adduction may not regularly bebtained, glenohumeral motion in this direction dem-nstrates significance at some of the measured pa-ameters at 50° of horizontal adduction. Over timend with repeated activities, this position would likelyave similar effects on glenohumeral biomechanics.he increase in posteriorly directed forces with in-reased horizontal adduction may explain why thereould be posterior subluxation of the humeral head,s suggested by Walch et al,23,24 as the etiology ofosterior glenoid wear.
In conclusion, this study highlights changes withlenohumeral biomechanics in positions of overheadctivities. The data showed not only that the posteri-rly directed forces are significantly increased in
hese positions but that there was also a significantecrease in contact area and increase in contactressure in these positions. As such, asymmetric load-
ng with excessive or repetitive overhead activitiesay eventually lead to posterior glenoid erosion.
EFERENCES
1. Apreleva M, Parsons IM IV, Warner JJ, Fu FH, Woo SL. Experi-mental investigation of reaction forces at the glenohumeral jointduring active abduction. J Shoulder Elbow Surg 2000;9:409-17.
2. Ateshian GA, Kwak SD, Soslowsky LJ, Mow VC. A stereophoto-grammetric method for determining in-situ contact pressures indiarthrodial joints: a comparison study. Advances in Bioengineer-ing American Society of Mechanical Engineers–BED Publication1992;22:35-38.
3. Ateshian GA, Kwak SD, Soslowsky LJ, Mow VC. A stereophoto-grammetric method for determining in situ contact areas in diar-throdial joints, and a comparison with other methods. J Biomech1994;27:111-24.
4. Bassett RW, Browne AO, Morrey BF, An KN. Glenohumeralmuscle force and moment mechanics in a position of shoulderinstability. J Biomech 1990;23:405-15.
5. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML. Posteriorglenohumeral subluxation: active and passive stabilization in abiomechanical model. J Bone Joint Surg Am 1997;79:433-40.
6. Glaser F, Gorab R, Lee TQ. Edge loading of the patellar com-ponent in TKA. J Arthroplasty 1999;14:493-9.
7. Greis PE, Scuderi MG, Mohr A, Bachus KN, Burks RT. Glenohu-
meral articular contact areas and pressures following labral andosseous injury to the anteroinferior quadrant of the glenoid.J Shoulder Elbow Surg 2002;11:442-51.
8. Halder AM, Kuhl SG, Zobitz ME, Larson D, An KN. Effects of theglenoid labrum and glenohumeral abduction on stability of theshoulder joint through concavity-compression: an in vitro study.J Bone Joint Surg Am 2001;83:1062-9.
9. Halder AM, O’Driscoll SW, Heers G, et al. Biomechanicalcomparison of effects of supraspinatus tendon detachments, ten-don defects, and muscle retractions. J Bone Joint Surg Am 2002;84:780-5.
0. Hale J, Brown T. Contact stress gradient detection limits ofPressensor film. J Biomech Eng 1992;114:352-7.
1. Hughes RE, An KN. Force analysis of rotator cuff muscles. ClinOrthop 1996;330:75-83.
2. Kelkar R, Wang VM, Flatow EL, et al. Glenohumeral mechanics:a study of articular geometry, contact, and kinematics. J ShoulderElbow Surg 2001;10:73-84.
3. Lee TQ, McMahon PJ. Shoulder biomechanics and muscle plas-ticity: implications in spinal cord injury. Clin Orthop 2002;403(Suppl):S26-36.
4. Levine WN, Djurasovic M, Glasson JM, et al. Hemiarthroplastyfor glenohumeral osteoarthritis: results correlated to degree ofglenoid wear. J Shoulder Elbow Surg 1997;6:449-54.
5. McMahon PJ, Debski RE, Thompson WO, et al. Shoulder muscleforces and tendon excursions during glenohumeral abduction inthe scapular plane. J Shoulder Elbow Surg 1995;4:199-208.
6. Nakagawa Y, Hyakuna K, Otani S, Hashitani M, Nakamura T.Epidemiologic study of glenohumeral osteoarthritis with plainradiography. J Shoulder Elbow Surg 1999;8:580-4.
7. Otis JC, Jiang CC, Wickiewicz TL, et al. Changes in the momentarms of the rotator cuff and deltoid muscles with abduction androtation. J Bone Joint Surg Am 1994;76:667-76.
8. Poppen NK, Walker PS. Forces at the glenohumeral joint inabduction. Clin Orthop 1978;135:165-70.
9. Poppen NK, Walker PS. Normal and abnormal motion of theshoulder. J Bone Joint Surg Am 1976;58:195-201.
0. Powers C, Lilley J, Lee TQ. The effects of axial and multi-planeloading of the extensor mechanism on the patellofemoral joint.Clin Biomech 1998;13:616-24.
1. Sciaroni LN, McMahon PJ, Cheung TG, Lee TQ. Open surgicalrepair restores joint forces that resist glenohumeral dislocation.Clin Orthop 2002;400:58-64.
2. Soslowsky LJ, Flatow EL, Bigliani LU, et al. Quantitation of in situcontact areas at the glenohumeral joint: a biomechanical study.J Orthop Res 1992;10:524-34.
3. Walch G, Badet R, Boulahia A, Khoury A. Morphologic study ofthe glenoid in primary glenohumeral osteoarthritis. J Arthroplasty1999;14:756-60.
4. Walch G, Boulahia A, Boileau P, Kempf JF. Primary glenohu-meral osteoarthritis: clinical and radiographic classification. TheAequalis Group Acta Orthop Belg 1998;64(Suppl 2):46-52.
5. Warner JJ, Bowen MK, Deng XH, et al. Articular contact patternsof the normal glenohumeral joint. J Shoulder Elbow Surg
1998;7:381-8.