Poliomyelitis Surveillance in Ireland
22
Poliomyelitis Surveillance in Ireland 4 th April, 2014
description
Poliomyelitis Surveillance in Ireland. 4 th April, 2014. Acknowledgement. - PowerPoint PPT Presentation
Transcript of Poliomyelitis Surveillance in Ireland

Poliomyelitis Surveillance in Ireland
4th April, 2014

Acknowledgement
The health Protection Surveillance Centre (HPSC) would like to thank all those who have contributed to polio surveillance, the National Virus Reference Laboratory, the Irish Paediatric Surveillance Unit (IPSU), paediatricians and all others who have provided data in relation to polio surveillance.
Rationale for polio surveillance• Europe has been polio free since 2002, but poliomyelitis
virus continues to circulate in other countries• In 2013, polio was identified in
– Afghanistan, Nigeria and Pakistan – endemic – Syria, the Horn of Africa, Cameroon, Somalia , other African
countries – outbreaks – Egypt, Israel, the West Bank and Gaza Strip – environmental or
asymptomatic individuals • As long as a single child remains infected, children in all
countries are at risk of contracting polio.

Cases of polio in Ireland
The last notified case of polio was in 1984
1948
1950
1952
1954
1956
1958
1960
1962
1964
1966
1968
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
0
100
200
300
400
500
600
Number Polio Cases Notified in Republic of Ireland 1948-2013, and year of vaccine in-troduction
Year
Num
ber o
f Cas
es N
otifi
ed Polio vaccine, 1957

Irish surveillance for Poliomyelitis- methods
• Acute flaccid paralysis (AFP) in ALL children < 15 years of age
• Investigation of suspect cases of CNS infection (e.g. meningitis, encephalitis, AFP) of all ages if travel or epi-links to contacts from areas where polio virus circulating,

Definition of AFP
Acute flaccid Paralysis (AFP) is a clinical syndrome characterised by rapid onset of weakness, including (less frequently) weakness of respiratory and swallowing, progressing to maximum severity within several days to weeks.AFP is a complex clinical syndrome with a broad array of potential aetiologies.
AFP surveillance and Polio
• Surveillance of AFP is used in surveillance for poliomyelitis in the context of the global polio eradication initiative
• Polio is caused by a human enterovirus called the poliovirus. Wild polioviruses are those that occur naturally. There are three serotypes of wild poliovirus – type 1, type 2, and type 3
• Polio is one of only a limited number of diseases that can be eradicated as there are no long-term carriers of the disease and an inexpensive vaccine is available

Potential aetiologies associated with AFP
Includes possible illness due to: • Guillian-Barré syndrome • Transverse myelitis • Traumatic neuritis • Viral infections caused by other enteroviruses
toxins and tumours
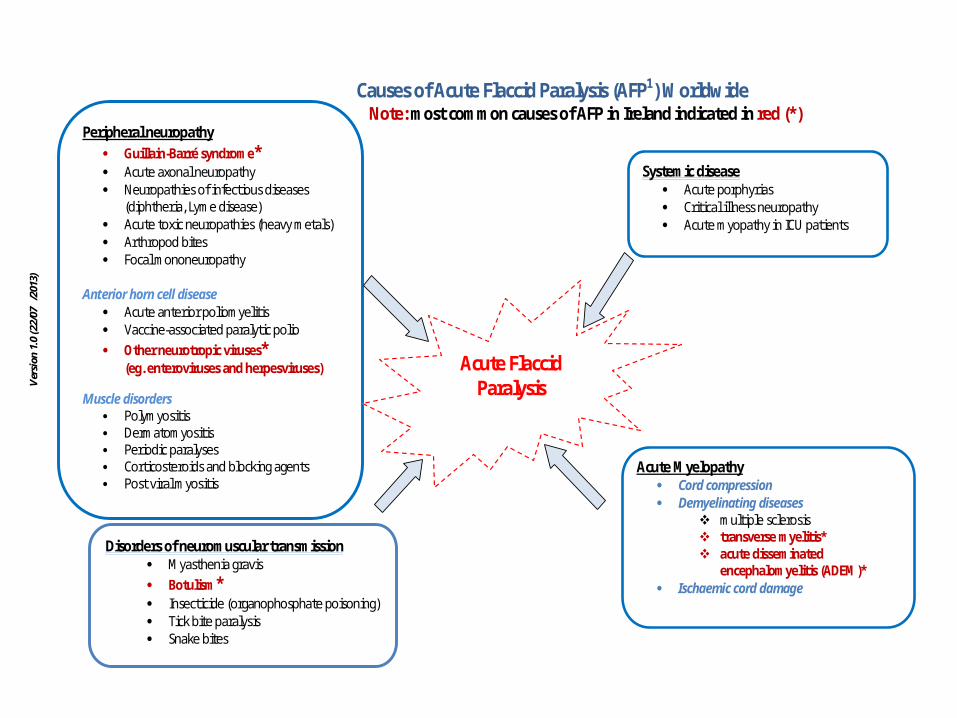
Causes of Acute Flaccid Paralysis (AFP1) Worldwide Note: most common causes of AFP in Ireland indicated in red (*)
Peripheral neuropathy Guillain-Barré syndrome* Acute axonal neuropathy Neuropathies of infectious diseases
(diphtheria, Lyme disease) Acute toxic neuropathies (heavy metals) Arthropod bites Focal mononeuropathy
Anterior horn cell disease Acute anterior poliomyelitis Vaccine-associated paralytic polio Other neurotropic viruses*
(eg. enteroviruses and herpesviruses)
Muscle disorders Polymyositis Dermatomyositis Periodic paralyses Corticosteroids and blocking agents Post viral myositis
Acute Myelopathy Cord compression Demyelinating diseases
multiple sclerosis transverse myelitis* acute disseminated
encephalomyelitis (ADEM)* Ischaemic cord damage
Systemic disease Acute porphyrias Critical illness neuropathy Acute myopathy in ICU patients
Acute Flaccid Paralysis
Disorders of neuromuscular transmission Myasthenia gravis Botulism* Insecticide (organophosphate poisoning) Tick bite paralysis Snake bites
Ver
sion
1.0
(22/
07/2
013)

Objectives of AFP surveillance
• To rapidly detect re-importation of poliovirus into polio-free areas
• To ensure that robust surveillance systems are in place so that if AFP caused by polio virus that it would be identified quickly

Investigation of AFP in children < 15 years of age
1. AFP case admitted to hospital2. Collect 2 stool specimens as early as possible, 24 hours apart, within 2
weeks of paralysis onset and send to National Virus Reference Laboratory (NVRL)
3. Complete AFP enhanced surveillance form and return to Paula Flanagan, HPSC, 25‐27 Middle Gardiner Street, Dublin 1, Tel: 01 876 5300, Fax: 01 856 1299
4. Surveillance forms available on ward or available at http://www.hpsc.ie/hpsc/A-Z/VaccinePreventable/Polio/AcuteFlaccidParalysisAFP/
5. When returning your monthly IPSU (Irish Paediatric Surveillance Unit) card indicate if you have seen a case in previous month
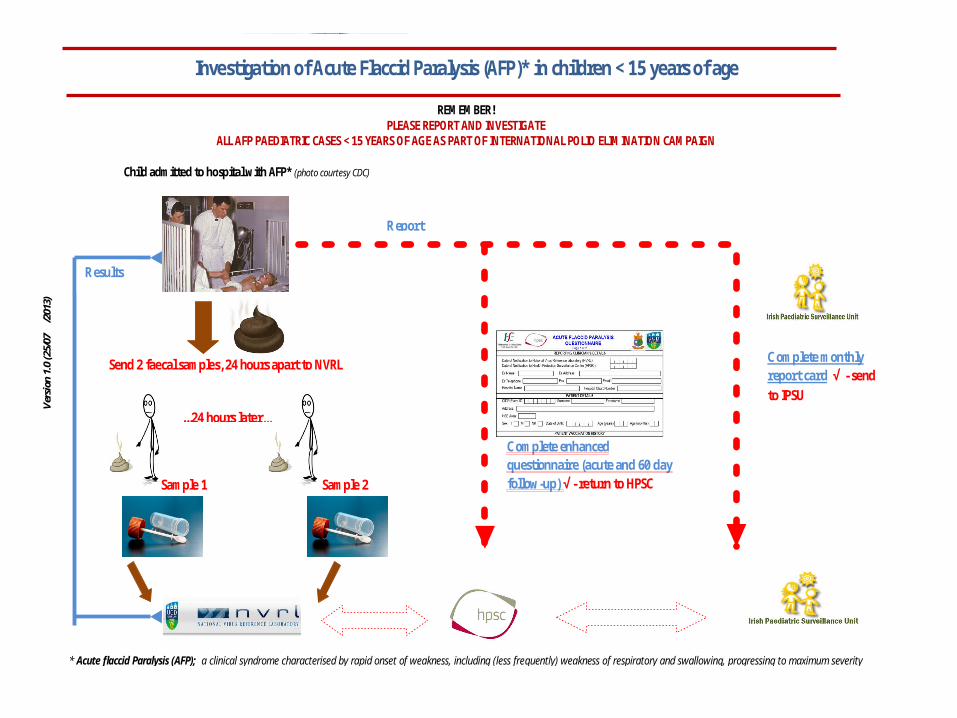
* Acute flaccid Paralysis (AFP); a clinical syndrome characterised by rapid onset of weakness, including (less frequently) weakness of respiratory and swallowing, progressing to maximum severity
Investigation of Acute Flaccid Paralysis (AFP)* in children < 15 years of age
REMEMBER!
PLEASE REPORT AND INVESTIGATE ALL AFP PAEDIATRIC CASES < 15 YEARS OF AGE AS PART OF INTERNATIONAL POLIO ELIMINATION CAMPAIGN
Child admitted to hospital with AFP* (photo courtesy CDC)
Send 2 faecal samples, 24 hours apart to NVRL
Sample 1 Sample 2
...24 hours later...
Report
Results
Complete monthly report card √ - send to IPSU
Complete enhanced questionnaire (acute and 60 day follow-up) √ - return to HPSC
Ver
sion
2.0
(24/
07/2
013)
V
ersi
on 1
.0 (2
5/07
/201
3)
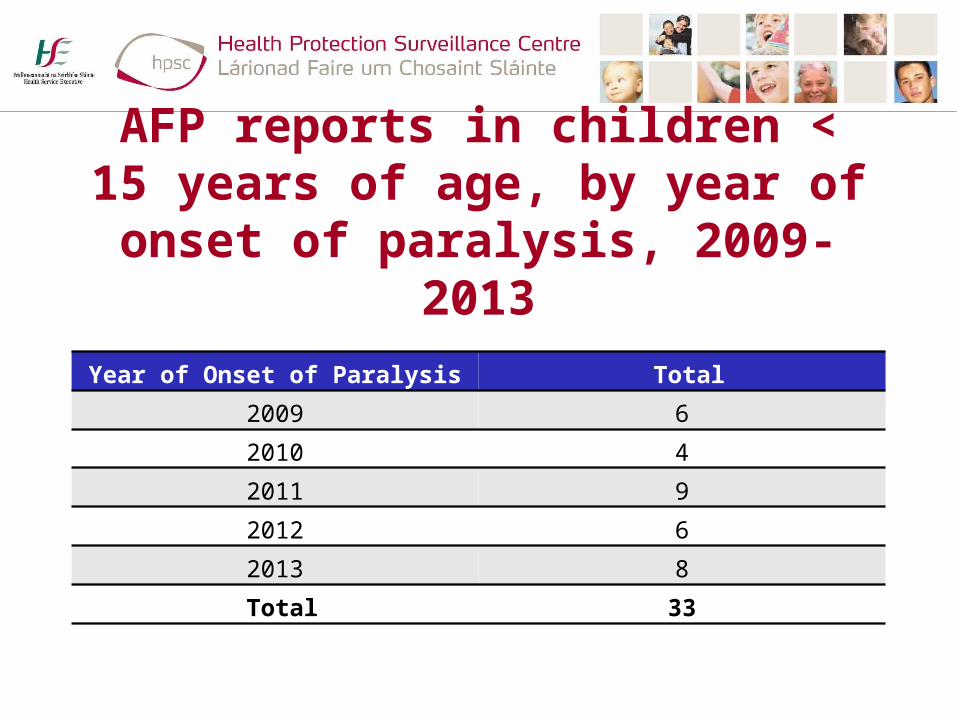
AFP reports in children < 15 years of age, by year of onset of paralysis,
2009-2013
Year of Onset of Paralysis Total2009 6
2010 4
2011 9
2012 6
2013 8
Total 33

AFP cases by Age Group 2009-2013
Age Group Total
0-4 13
5-9 5
10-14 7
Not specified 8
Total 33
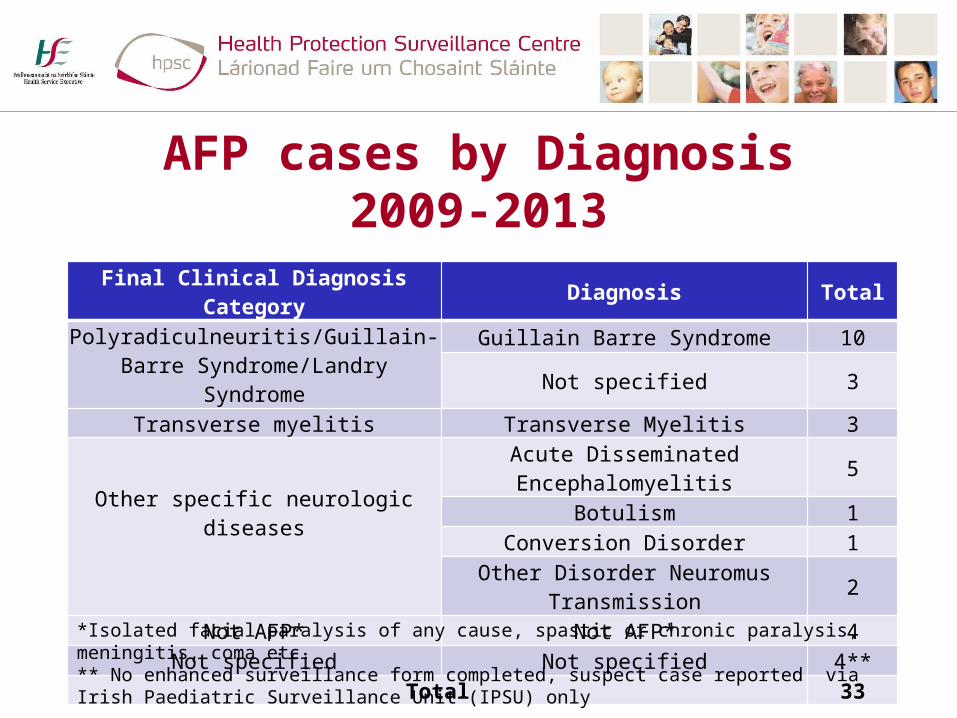
AFP cases by Diagnosis2009-2013
Final Clinical Diagnosis Category Diagnosis Total
Polyradiculneuritis/Guillain-Barre Syndrome/Landry Syndrome
Guillain Barre Syndrome 10
Not specified 3
Transverse myelitis Transverse Myelitis 3
Other specific neurologic diseases
Acute Disseminated Encephalomyelitis 5Botulism 1
Conversion Disorder 1Other Disorder Neuromus Transmission 2
Not AFP* Not AFP* 4Not specified Not specified 4**
Total 33
*Isolated facial paralysis of any cause, spastic or chronic paralysis, meningitis, coma etc.** No enhanced surveillance form completed, suspect case reported via Irish Paediatric Surveillance Unit (IPSU) only

Vaccination uptake of 3 doses polio vaccine at 12 months, by LHO, Q3 2013*
*Source: HPSC Q3 2013 report located at http://www.hpsc.ie
National uptake = 92% (range 88%-95%)
N
EW
S
No Data95 - 10090 - 9485 - 8980 - 840 - 79
% Immunisation Uptake
G
L
DL
KY
MO
CE
TS
RN
NC
MH
NSL
WX
LS/OY
WC
SO/LM
WD
KE/WW
LD/WH
LHCN/MN
CW/KKTN/EL
WW
DN
DW
DN W
DSW DSDSE
DN C
DSC
DSC
DNC
DSE DSDSW
DNW
DW
DN
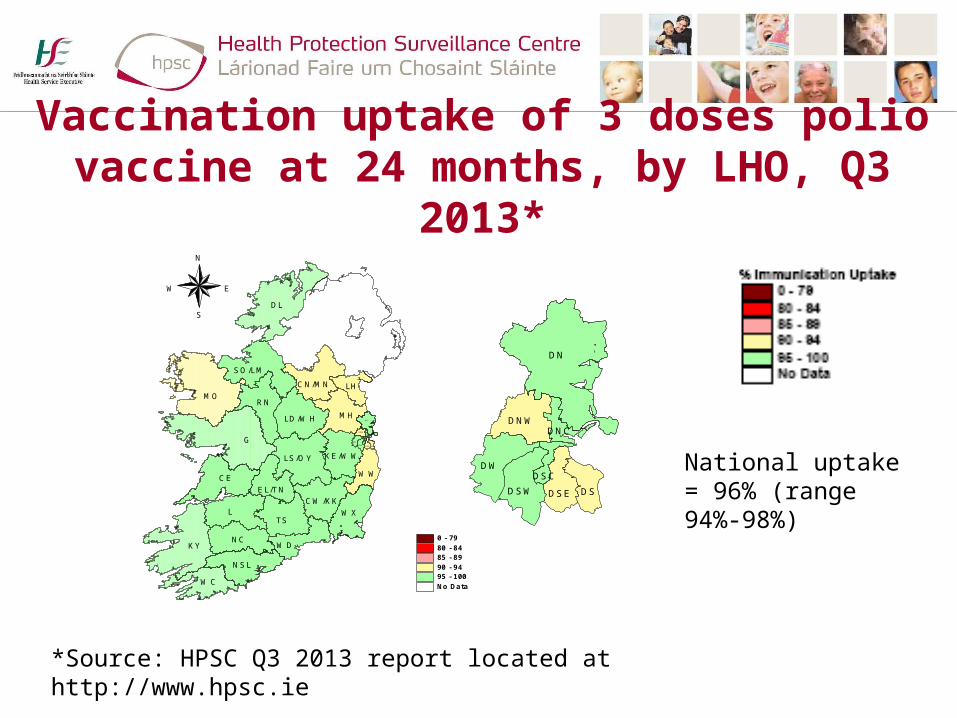
Vaccination uptake of 3 doses polio vaccine at 24 months, by LHO, Q3 2013*
*Source: HPSC Q3 2013 report located at http://www.hpsc.ie
National uptake = 96% (range 94%-98%)
N
EW
S
0 - 7980 - 8485 - 8990 - 9495 - 100No Data
G
L
DL
KY
MO
CE
TS
RN
NC
MH
NSL
WX
LS/OY
WC
SO/LM
WD
LD/WH
LHCN/MN
CW/KK
WW
EL/TN
KE/WW
DN
DW
DNW
DSW DSDSE
DNC
DSC
DN
DW
DNW
DSW DSDSE
DNC
DSC

WHO recommendations to decrease risk of Wild Polio Virus (WPV) importation and possible
spread and diseaseVaccination recommendations• Maintain national vaccination
coverage with completed polio vaccination > 90%
• Identify those at risk of low immunisation and implement vaccination as needed
National data • 3 doses at 12 months is
92% (Q3 2013)• 3 doses at 24 months is
96% (Q2 2013)
• Currently national data is not available by ethnicity, migrant or other risk factor status

Recommendations to decrease the risk of WPV importation and possible spread and disease in Ireland(2)
• Improve surveillance- Paediatric AFP surveillance – All AFP cases in children < 15 years of age (regardless
of presumed diagnosis) should be investigated for enteroviral/polio virus specific infection
– Children < 15 years of age who present with aseptic meningitis, encephalitis, other neurological symptoms (non-AFP) should be systematically tested for polio virus IF they have links (direct travel or contact with individuals from these countries where wild polio has been identified)

For older child and adult surveillance for polio virus
• Older children (> 15 years) and adult patients, with a history of travel to, or contact with individuals from, countries where wild polio has been identified AND who present with AFP, aseptic meningitis, encephalitis, other neurological symptoms (non-AFP) should be systematically tested for polio virus.

Laboratory investigation (NVRL) - Summary
Two stool samples should be taken as soon as possible (at least within 2 weeks of onset and 24 hours apart) and sent to the NVRL with clinical detail to facilitate rapid investigation and feedback
– All paediatric cases of AFP – All cases of AFP, aseptic meningitis, encephalitis, other
neurological symptoms (non-AFP) especially IF there are epi-links to countries (or individuals returned from these countries) where polio virus is circulating

Thank you
For more information http://www.hpsc.ie/hpsc/A-Z/
VaccinePreventable/Polio/