
Policy Choices and Practical Problems in Health Economics · Policy Choices and Practical Problems...
246
I G 2 G4 Sa lEconomic Development Institute 11 5U of The World Bank Policy Choices and Practical Problems in Health Economics Cases from Latin America and the Caribbean Edited by Catherine A. Overholt Margaret K. Saunders EDI LEARNING RESOURCES SERIES Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of Policy Choices and Practical Problems in Health Economics · Policy Choices and Practical Problems...

I G 2 G4
Sa lEconomic Development Institute11 5U of The World Bank
Policy Choicesand Practical Problemsin Health Economics
Cases from Latin Americaand the Caribbean
Edited by
Catherine A. OverholtMargaret K. Saunders
EDI LEARNING RESOURCES SERIES
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized


EDI LEARNING RESOURCES SERIES
Policy Choicesand Practical Problemsin Health Economics
Cases from Latin Americaand the Caribbean
Edited by
Catherine A. OverholtMargaret K. Saunders
The World BankWashington, D. C.

C 1996The International Bank for Reconstructionand Development / THE WORLD BANK1818 H Street, N.W.Washington, D.C. 20433, U.S.A.
All rights reservedManufactured in the United States of AmericaFirst printing December 1996
The Economic Development Institute (EDI) was established by the World Bank in 1955 to train officials concemed withdevelopment planning, policymaking, investment analysis, and project implementation in member developing countries.At present the substance of the EDI's work emphasizes macroeconomic and sectoral economic policy analysis. Througha variety of courses, seminars, and workshops, most of which are given overseas in cooperation with local institutions, theEDI seeks to sharpen analytical skills used in policy analysis and to broaden understanding of the experience of individualcountries with economic development. Although the EDI's publications are designed to support its training activities, manyare of interest to a much broader audience. EDI materials, including any findings, interpretations, and conclusions, areentirely those of the authors and should not be attributed in any manner to the World Bank, to its affiliated organizations,or to members of its Board of Executive Directors or the countries they represent.
Because of the informality of this series and to make the publication available with the least possible delay, the manuscripthas not been edited as fully as would be the case with a more formal document, and the World Bank accepts no responsibilityfor errors. Some sources cited in this paper may be informal documents that are not readily available.
The material in this publication is copyrighted. Requests for permission to reproduce portions of it should be sent to theOffice of the Publisher at the address shown in the copyright notice above. The World Bank encourages dissemination ofits work and will normally give permission promptly and, when the reproduction is for noncommercial purposes, withoutasking a fee. Permission to photocopy portions for classroom use is granted through the Copyright Clearance Center, Inc.,Suite 910, 222 Rosewood Drive, Danvers, Massachusetts 01923, U.S.A.
The complete backlist of publications from the World Bank is shown in the annual Index of Publications, which containsan alphabetical title list (with full ordering information) and indexes of subjects, authors, and countries and regions. Thelatest edition is available free of charge from the Distribution Unit, Office of the Publisher, The World Bank, 1818 H Street,N.W., Washington, D.C. 20433, U.S.A., or from Publications, Banque mondiale, 66, avenue d'1ena, 75116 Paris, France.
Margaret K. Saunders is a population and health specialist in the Human Resources and Poverty Division of the WorldBank's Economic Development Institute. Catherine A. Overholt is vice president of the Collaborative for DevelopmentAction, Inc. in Boston, Massachusetts.
Library of Congress Cataloging-in-Publcation Data
Policy choices and practical problems in health economics: cases fromLatin America and the Caribbean / edited by Catherine A. Overholt,Margaret K. Saunders.
p. cm.-(EDI learning resources series, ISSN 1020-3842)ISBN 0-8213-3012-81. Medical economics-Latin America-Case studies. 2. Medical
economics-Caribbean Area-Case studies. 3. Medical care-LatinAmerica-Finance-Case studies. 4. Medical care-Caribbean Area-Finance-Case studies. 1. Overholt, Catherine A., 1942-II. Saunders, Margaret K., 1957- . III. Series.RA410.55.L29P65 1996338.4'73621'098-dc2O 94-29559
CIP

Contents
Foreword vAcknowledgments vii
Section One: Issues and Concepts in Health Economicsand Financing
1. Overview of Concepts and Tools for Economic Decisionmaking 3
2. Economic Development and the Health Sector 5
3. Financing the Health Sector: Expenditure Analysis and Affordability 13
4. Basic Concepts of Demand 18
5. Production and Cost Analysis in the Health Sector 22
6. Mobilizing Resources for Health Services 26
7. Economic Evaluation and Health Care Interventions 32
8. Further Readings and References 36
Section Two: Applied Experiences in Health Economicsand Financing
Overview: Using the Case Method 41
Economic Development and the Health Sector
Case 1. Macroeconomics and Health: The Case of Mexico 46Catherine A. Overholt
Financing the Health Sector: Expenditure Analysis and Affordability
Case 2. Primary Health Care in Honduras 70James E. Austin
,ii

iv Contents
Case 3. Financing the St. Lucian Health Sector 90Maggie Huff-Rousselle
Basic Concepts of Demand
Case 4. Planning for Health Services in El Salvador: Need and Demand 108Catherine A. Overholt
Production and Cost Analysis in the Health Sector
Case 5. Hospital Jose Maria Cabral y Baez 132Linda Harder and Michael Reich
Case 6. The AGAPCO Financial Plan 158James E. Austin
Mobilizing Resources for Health Services
Case 7. After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 172Maggie Huff-Rousselle
Case 8. PROSALUD: Marketing and Financing Primary Health Care 190Maggie Huff-Rousselle and Catherine A. Overholt
Economic Evaluation and Health Care Interventions
Case 9. Antimalaria Program in Northwest Brazil: A Cost-Benefit Analysis 210Antonio Campino

Foreword
In 1986 EDI's Human Resources and Poverty Division initiated a program ofwork in the area of health economics and financing in Latin America and theCaribbean. The work has been carried out in collaboration with the World Bank'soperational departments for Latin America and the Caribbean, and with the Pan-American Health Organization. The first stage of the program comprised a seriesof seminars that brought together high-level policymakers from ministries ofhealth, finance, and planning, as well as senior officials from social securityinstitutes, training institutes, and universities, to promote a better understanding offundamental concepts in health economics and financing, and to apply basic toolsfor improved problem solving and decisionmaking. The second stage of theprogram includes the establishment of a Network on Health Economics andFinancing to further promote training in this field, and to encourage thedevelopment of greater expertise at the national level.
This book covers the main issues and concepts in health economics andfinancing. More importantly, it includes a broad range of case studies that applythese concepts to actual situations faced by many health managers, planners, andhuman resource economists as they struggle to balance the needs for greater equityand expansion of services, while faced with financial constraints that requirecareful attention to issues of resource allocation and improved efficiency.
The book is intended primarily for use in short-term training of adults alreadyin senior or mid-level positions who would like to gain experience in usingeconomic and financing analysis to solve problems in the health sector. It may alsoprovide useful material for master's degree programs in health economics andfinancing in Latin America. A list of readings and references is provided for thosewishing to pursue the topic in more depth.
Vinod Thomas, DirectorEconomic Development Institute
v


AcknowledgmentsThe editors would like to thank the reviewers of this book from "outside" the
World Bank, Gerald D. Rosenthal and John Ickis, for their insightful and highlypertinent comments. We believe that their careful work helped make thispublication of even greater value to a much wider audience. In addition, within theWorld Bank, helpful commnents and guidance were provided by Armand VanNimmnen, Maureen Lewis, Philip Musgrove, and John Didier. We would like tothank Alice Dowsett for her editorial contributions. Thanks are also due to ShawnFarrell who handled the initial graphic design work, and to Annette De Mattos forher thorough, diligent work as a graphic designer during the publication process.
vii


Section One
Issues and Concepts in HealthEconomics and Financing


1. Overview of Concepts and Tools forEconomic Decisionmaking
Between 1987 and 1991, the Human Resources Development Division of theEconomic Development Institute of the World Bank (EDIHR), in collaboration withthe Pan-American Health Organization (PAHO), designed and presented a series ofseminars on health economics and financing in Latin American and the Caribbean. Theorigin of the seminars grew out of discussions with task managers within the WorldBank and PAHO that indicated growing discrepancies between the traditional educationof health personnel and the increasingly complicated resource allocation decisions thatrequired understanding of a range of economic analyses and tools. Further discussionby EDIHR and PAHO with high-ranking health care policymakers, advisors, andmanagers from countries in the region identified problems in communication witheconomists and planners over questions of resource allocation and issues related toimproving efficiency and effectiveness in an era of greater economic austerity. Inaddition, economists and planners in the region expressed an interest in improving theirknowledge of the application of economics to the health sector. A final group ofpersons interviewed were associated with universities or training institutes in theregion; they asked to be associated with the seminars so that they might develop similarprograms for national and regional audiences.
The seminars were designed to address three objectives. First, the participantswould acquire general knowledge and understanding of fundamental economic andfinancing concepts and techniques and how to apply them to health issues. Second,participants would practice using these analytical skills to solve problems and makedecisions through the study and discussion of cases based on health sector issues. Theseminars recognized that participants had considerable experience and educationalbackground, and sought to enhance the acquisition of knowledge and judgmentregarding the use of particular analytical approaches, their underlying assumptions andtechnical implications. It was necessary that the seminars be as relevant as possible tocurrent situations faced by participants in the demands of their jobs, rather thantheoretical in nature or drawn from experience that bore little similarity to the region.Third, the seminars provided an opportunity for participants who worked on policyprograms in the health sector to exchange views with others who had economics andfinancing backgrounds.
3

4 Section One: Issues and Concepts in Health Economics and Financing
The economists and health planners from the World Bank and PAHO whodesigned the original seminars felt that it was fundamental for the seminar to developboth an understanding of economic reality and an appreciation for the critical rolethat markets play in resource allocation in any setfing. The goal was to develop realeconomic problem-solving skills in a structured learning environment withoutattempting to cover too much ground in a short seminar experience.
To design the technical content of the seminars, the group identified several basicconcepts and analytical tools used in economic and financial thinking that could helphealth practitioners to identify issues and problems and to structure alternatives withgreater clarity and specificity. The concepts and tools judged to be the most basic andessential were organized into six fundamental and interrelated themes that providedthe framework for the seminars. These themes cover the range of issues thatpractitioners in the health sector are most likely to face and present dimensions ofeconomic thinking. They also represent different perspectives on economic andfinancing issues. The themes combine conceptual ideas used to clarify broadeconomic questions, such as the relationship between macroeconomics anddevelopment, and analytical tools, such as those used in estimations of demand oreconomic evaluation. Collectively, the themes provide a clearer understanding of therelationship and priority of these topics in economic decisionmaking.
The designated themes are (1) economic development and the health sector; (2)financing the health sector: expenditure analysis and affordabilty; (3) basic conceptsof demand; (4) production and cost analysis in the health sector; (5) mobilizingresources for health services; and (6) economic evaluation. The themes and theconcepts and ideas they embody are each discussed below. The purpose of thediscussion is to enable the reader to become familiar with useful concepts and toolsrelevant to the health sector. The presentation is a nontechnical discussion. It doesnot provide the reader with everything one needs to know and understand abouteconomic theory and its basic assumptions. It is not intended as an economictextbook. Additional readings are suggested in each theme for the reader who seeksa more advanced and comprehensive understanding in a particular area.
A more thorough understanding about how to use the conceptual ideas andanalytical tools to improve decsionmaking can be gained by applying them to thehealth sector situations that are described in the cases in Section Two. The cases varyconsiderably in the degree to which the issues fall readily into a single category ortheme, although they do follow roughly the order of economic topics. While eachcase emphasizes one or two key themes, the nature of the problems addressed cutsacross many of the economic themes presented earlier. Each case study is precededby an introductory paragraph that orients the reader to the key themes in the case.A set of study questions provides the reader with guidance for analysis.

2. Economic Development and theHealth Sector
In considering the process of economic development and its relationship to thehealth sector, several questions are relevant for public health professionals:
* What are some of the key basic macroeconomic concepts?
* How is the health sector affected by and interrelated with macroeconomicphenomena?
e What is the impact of the economic crises on the health sector?
Basic Macroeconomic Concepts
Macroeconomics helps us understand economic phenomena at an aggregate nationallevel. It enables us to measure the economic development of a nation in terms of itsgrowth of production and generation of income. The most common measure ofeconomic growth is gross national product, or GNP, which is the value of the totalannual output of final goods and services in the nation.
The basic elements of GNP provide the basis for understanding macroeconomicphenomena. The output of final goods and services embodies four categories:
* Consumption(C), which are those items private consumers purchase as part oftheir personal expenditures, for example, food or entertainment
* Investment (I), which are those items the private sector uses to produce othergoods and services, for example, machines, buildings, or roads
* Government (G), which are those expenditures the government sector makes forconsumption of or investment in goods and services
* Net Exports (X), which are the goods and services produced for export lessthose imported
5

6 Section One: Issues and Concepts in Health Economics and Financing
These four components make up GNP and give rise to the common, simpleequation:
GNP = C + I + G + X
GNP measures the value of what a country produces and consumes each year.Its expansion is a basic indicator of economic growth. GNP measures the valueof the output, but real growth means an increase in the physical output. If acountry produced the same amount of goods this year as last, but inflationcaused the prices of those goods to rise, the nominal value of the GNP would behigher. However, the country is clearly not better off because it has no moreoutput than before. To avoid this illusion, economists deflate the GNP's nominalfigures to remove the price increases and specify GNP in real terms, that is, asa measure of the increase or decrease in the actual output of goods and services.Thus, if the GNP in real terms increased, then we can say the countryexperienced economic growth.
GNP reveals how a nation spends its money, but to spend you need income.Gross national income (GNI) is the other side of the circular macroeconomicpicture. GNP measures what a country produces and spends its money on, andGNI measures what it earns by producing those goods and services. The demandfor goods and services creates the demand by companies and the government toemploy people, borrow money, and rent land and buildings. The correspondingpayments of wages, interest, and rents create the incomes used to buy the goodsand services. Economists refer to these as payments to the factors of production,that is, labor, capital, and land. In the aggregate, expenditure requires income,so by definition GNP = GNI. Because different forces affect incomes andexpenditures, it is important to recognize, understand, and examine both sides ofthe macroeconomic circle as well as their interrelationships.
An elaboration of these flows reveals some additional linkages. Part of theincome that individuals receive is used to pay government taxes. Companiesmake similar expenditures. Thus, taxes become the income flow to a governmentthat enables it to make the expenditures that constitute G in the GNP equation.
Another linkage between government, business, and households flows in theopposite direction from taxes. Governments make a variety of transfer paymentsto households and businesses, for example, social security or unemploymentbenefits and various direct subsidies. Transfer payments "rearrange" incomes toachieve social and/or political objectives by taking money (taxes) from one groupand giving it to another. By themselves, transfer payments do not create a netincrease in output, and so do not affect GNP. HoWever, different recipients ofsuch payments might use them in different ways (for example, spend, save, orinvest), and these uses may ultimately have different effects on the economy.
Businesses, and this includes health facilities such as hospitals, also incuranother cost, which is depreciation. Their buildings and machines wear out andneed to be replaced. Thus, part of what a business earns needs to be set aside to

Economic Development and the Health Sector 7
enable reinvestment. These and other investments that businesses need to make(the I in GNP) in order to grow require more funds than they have been able toset aside in the depreciation allowances or have been able to generate in profits.To obtain these additional funds they must borrow from financial institutions orindividuals. These funds come from savings. Individuals can spend all theirincome or save a portion of it. The portion they spend goes into the C in GNP,the portion they save goes into the I in GNP.
The circular linkages between national income and national expenditures aresummarized in Exhibit 1.
On the surface, it appears to be a virtuous circle: higher incomes lead togreater expenditures that in turn lead to yet higher incomes, generating ever-rising economic growth. Of course, experience tells us that it can also be avicious circle, with lower incomes causing lower expenditures and growth. Thereis no guarantee of economic development; it depends on the forces that affecteach of the components in the macroeconomic circle and how these componentsinteract.
To illustrate, let us examine some of the dynamics and linkages. Given thatGNP = C + I + G + X, then if consumption (C) went up and othercomponents stayed the same, GNP would grow. However, the linkages in thecircular flow mean that other components would likely be affected. If householdsspend more of their incomes on consumption, they will have less to save. Ifsavings drop then companies may not be able to get enough funds to invest, andso the investment (I) component of GNP might decrease, thereby offsetting thegain in C. Or if the factories were already working at full capacity and did nothave the funds to expand, they would not be able to produce the additional goodsdemanded by the consumers. This would mean that more consumers werebidding for the same amount of goods and the price of those goods wouldincrease (inflation). The nominal value of C, and therefore of GNP, would behigher, but there would have been no actual increase in goods produced so therewould be no real increase in GNP. Let us assume that households increased theirsavings, thereby increasing the funds available for businesses to borrow andinvest. However, this will not happen automatically because businesses considermany other variables when deciding to invest, such as the prospects forincreasing demand for their products, the possible actions of their competitors,or the country's political stability. These examples remind us that macroeconomicflows ultimately depend on the aggregated decisions of millions of individualconsumers and business people.
Governments can formulate policies and actions that directly and indirectlyaffect macroeconomic flows and the decisionmaking of individuals andbusinesses. For example, the government's fiscal policies determine the size ofgovernment expenditures (G), and hence the level of GNP. On the income sideof the circle, these expenditures affect the revenues of companies selling goodsand services to the government and the wages of employees working directly forthe government. Thus, a rise in G could stimulate demand and subsequent

EXHIBIT 1CIRCULAR FLOW OF NATIONAL INCOME AND EXPENDITURES
Housz3hod Payments Housaehold /
unessdTaxes Purd7asesot Wagvemmn Gov rnment Goods_° Ptd
InvestmentB Rents, GoodB &I/
Rets Sevi
1 ~~~~Interest &
Income~~~~~~~~~~~~~~~~
\ \ ~~~~~Transhr \|
(HOUSEHOLDS )( BSNS
-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ ~~~~~~~~~~~~CL
\ ~~~~~-h Household Purchases dof \ ~~~~~Good, Swnsces & Investrnents/- -_ Hueod
1-lousahold ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~~~~oseod
/ wdls Buins
Business PTPments oo W agm,c G"vernmenttRent, Interest and DMdrnds

Economic Development and the Health Sector 9
economic growth. The other side of fiscal policy is the revenue to pay for theexpenditures. If these come from taxes, they can reduce incomes and reducedemand. If the government spends more than it obtains in taxes, it incurs adeficit. It can cover this by borrowing the difference as long as willing lendersare available, either domestically or internationally. Continued fiscal deficits cancreate inflationary pressures.
Monetary policy is a related concept. Governments affect the total supply ofmoney through their power to create money and regulate the banking system,including interest rates. For our purpose, it is sufficient to say that monetarypolicy can significantly affect savings and investment through its effects oninterest rates, credit availability, and inflation. For example, to control inflationthe monetary policy might cut back on the supply of money and increase,accordingly, interest rates (a tight money policy). This circumstance would meanthat credit to businesses and consumers would be less available and moreexpensive. The immediate effect might reduce investment (1) and consumption(C), which would have dampening effects on the GNP. A decline in consumerdemand can lead to cutbacks in production and worker layoffs, which in turnreduce incomes and consumption.
Another policy area related directly to GNP is trade policy. Governments canaffect a country's exports and imports through regulations such as import orexport taxes, quotas, and foreign exchange controls. In the aggregate, if exportsexceed imports (net exports are positive), GNP will increase accordingly. Ifimports exceed exports, this trade deficit has to be covered by obtaining foreigncapital in the form of international loans, investments, or grants. The country'sexchange rate will be affected fundamentally by these trade and capital flows. Ifa country's currency suffers a devaluation, then imports will be more expensive,that is, it will take more local currency to acquire the same imported good.
The preceding discussion about the basic macroeconomic phenomena and theirrelationship to a country's economic growth indicates that GNP and GNI andtheir interrelationships are helpful in identifying and understanding themacroeconomic linkages and dynamics that affect economic performance. It isimportant also to recognize, however, that GNP is not a fully adequate measureof development. For example, goods or services that are not sold are not countedin the GNP. The value of unpaid labor of household members is an importantexample. GNP does not judge the purpose or quality of output. For example,some production may produce pollution that reduces quality of life or createsproducts of low social utility. GNP, or even GNP per capita, reveals nothingabout the equity of the distribution of goods and services produced. Thus,economic indicators only constitute one part of a country's development report.
Macroeconomic Linkages with Health
The health status of a country's people is an important noneconomic indicatorof human welfare and national development. For example, infant and maternal

10 Section One: Issues and Concepts in Health Economics and Financing
mortality rates, morbidity rates, longevity, and the number of children peoplehave reveal the quality of life of the population. Health status both affects and isaffected by macroeconomic phenomena, and the way that national income isspent affects the welfare of the population.
Expenditures for health care are important because they contribute to humanwelfare both directly and indirectly. Health sector expenditures include theresources that the government applies to health care activities as well as theprivate expenditures for health care made by households from their owndisposable incomes. These health expenditures can improve the health status ofthe population directly by reducing mortality, fertility, and morbidity. Healthexpenditures improve social welfare indirectly via the effects on per capita GNPthat derive from increasing labor productivity and decreasing population growth.These factors determine the quantity and the quality of the nation's labor supply,which in turn affect total output and national income.
In economic terms, the population is a factor of production. Human capitalis one of the fundamental determinants of economic growth. Health status affectsboth the quality and quantity of this economic resource. Reduction of mortalityrates increases the person days of economic activity available to the economy.Reduction of morbidity rates increases the number of days as well as theproductivity of the work force, and productivity improvement is a key factor ineconomic growth.
As part of the economy, the health sector also directly affects the GNP.Expenditures on health products and services by consumers or by the governmentincrease C and G in the GNP equation. Investments in equipment and facilitiesby private or public health care institutions similarly contribute to GNP. On theincome side, the economic behavior of their public or private sector employersdetermines the income of health sector employees.
The overall condition of the economy has significant effects on the healthsector. If the economy is growing, jobs are generated and incomes rise, therebyincreasing the consumers' ability to pay for health goods and services. Higherincomes, if appropriately distributed, may also mean that more vulnerableeconomic groups are better able to obtain their basic nutritional needs, therebyreducing their health risks. A growing economy and incomes usually also meanrising tax revenues for the government. Greater government revenues permitincreases in national health budgets. As a nation's income rises, it spends a largershare of GNP on health care. A strong economy is healthy for the health sector,but the opposite is also true.
Economic Crises and the Health Sector
During the past decade most developing countries have suffered economiccrises, often characterized by stagnating or negative economic growth,burgeoning unemployment, trade deficits and high inflation. These problems are

Economic Development and the Health Sector 11
caused in part by fiscal deficits, loose monetary policy, and excessive foreign debtor by trade-related conditions, such as skyrocketing prices of oil imports orplummeting prices of export commodities. Economies had gone out of controlbecause of both these external shocks and because of internal mismanagement ofmacroeconomic policies.
These extreme economic problems and the subsequent economic adjustmentmeasures required to correct them carried severe repercussions for the health sector.The impact of economic crises and the effects of stabilization and adjustmentprograms on the financing and performance of the public health sector were issuesof major concern to the public health authorities in developing countries. Economicor structural adjustment programs affected the health of the population in two ways:they reduced household incomes, particularly of poorer groups in the population, andthey reduced the health services provided by the government.
Lower economic growth resulted in unemployment and lower incomes. With lessincome, people, particularly those at the lowest income levels, experienceddeterioration in their diets and nutritional status and increased morbidity risk. Theywere less able to pay for private medical care or medicines, and they turnedincreasingly to the public sector health care system because of its free or cheapercare. Unfortunately, this increase in demand encountered a public sector healthsystem with a decreasing ability to respond.
The decline in national incomes meant a reduction in the flow of revenue togovernment coffers, and international banks were unwilling to lend additional moneyto governments to cover their fiscal deficits. The international agencies providedfmancial assistance contingent upon governments reducing or eliminating their fiscaland trade deficits and inflation. This meant that government budgets were slashed,usually including ministry of health expenditures. This decrease in governmentexpenditures (G) further depressed GNP and national incomes, and in particularreduced the response capability of public health care providers. Devaluations andforeign exchange scarcity cut imports, including health supplies. The quantity andquality of health care services generally declined just as needs were increasing.
Governments have taken a variety of economic adjustment actions to deal with thecrises, often in collaboration with the International Monetary Fund, the World Bank,and other international agencies. Stabilization measures are intended to correct thefiscal and balance of payments deficits and to reduce the inflation rate. They realignand balance resource supply and derrmand. Structural adjustment measures focusprimarily on reformulating macroeconomic policies and institutional interventions soas to improve over time a country's capability to allocate and use resourcesefficiently and expand its growth potential. They expand and balance theresource base. Sectoral adjustment concentrates on specific sectors, suchas agriculture or health, and attempts to correct economic distortions andstrengthen sectoral institutions. Although these adjustment measures mayput adverse pressure on the health sector in the short run, the

12 Section One: Issues and Concepts In Health Economics and Financing
rationale is that the long-run effect stabilizes and strengthens the economy, withpositive macroeconomic linkages to the health sector as discussed previously.
Public health authorities face major challenges in operating effectively duringthese difficult periods of economic crisis and adjustment. Even after a countryhas emerged from the crisis, continued economic health clearly requires a moredisciplined, efficient, and productive use of scarce resources. An understandingof the macroeconomic linkages to the health sector is increasingly critical forpublic health leaders.

3. Financing the Health Sector:Expenditure Analysis and Affordability
In considering the characteristics and trends of national health care expendituresand how these relate to issues of financing and affordability, several questions areimportant for public health professionals:
* What are the prevailing expenditure allocation patterns and sources of financefor the health sector?
- What concepts and tools are useful for analyzing financial flows in the healthsector?
* How can analyses of financial flows help improve planning and resourcemanagement in the health sector?
Institutional and Service Mix and Financial Flows
The health sector in developing countries consists of a mixture of government andnongovernment activities that provide a broad range of health and medical services.Governments finance and direct the public health services that control vector-bornedisease, carry out water and sanitation projects, and provide primary health care tothe general population. Governments also provide free or low-priced curative careto the general public through ministry of health institutions and to insured populationsthrough social security institutions. On the nongovernment side, independentphysicians dominate the provision of private, modern, curative services andtraditional practitioners deliver fee-for-service. Various nonprofit, voluntary, orreligious organizations provide low-priced or free curative and preventive services.Employers may provide direct care for employees or finance its purchase fromprivate practitioners. Communities may organize and finance the delivery of certainservices for its citizens. Also operating in the nongovernment arena are pharmacies,laboratories, and other providers of allied health products and services. A detailedanalysis of the financing of the health sector by services and institutions is animportant step for health planners that seek to orient health services to a moreequitable and efficient use of resources.
13

14 Section One: Issues and Concepts in Health Economics and Flnancing
Financing mechanisms for the health sector need to be considered asinterdependent elements. The conceptualization of financial flows in the healthsector presented in Exhibit 2 (de Ferranti 1983) illustrates these importantlinkages between providers, institutions, and financing mechanisms. It makes thecrucial distinction between govermnent as a service provider through publicfacilities, and government as a source of financing for both the public and privateproviders. It also distinguishes government financing as a subsidy that can bedirected in a variety of ways. This depiction of financial flows also introduces theidea of risk-sharing arrangements.
Expenditure Allocation Pafferns
The examination of the current expenditures and sources of finance involvedin these national health efforts provides an essential understanding of resourceflows in the health sector. This perspective is necessary for planning futureexpenditures, for redeploying resources and improving efficiency, and forclarifying the impact of present or future policies. Brief and low-cost assessmentscan provide a basis for
* Identifying where health policy objectives are being promoted or frustratedbecause of their size, appropriateness, source of funding, or othercharacteristics
* Revealing where resources can be used more efficiently
* Drawing attention to lack a of equity in the use of resources in the publicor private sector
* Distinguishing gaps between available resources, existing policies, andresources required to move toward national health goals (Mach and Abel-Smith 1983).
To obtain a clear picture of the current use of financial and material resourcesin the health sector, the health planner or analyst begins by identifying themagnitude of total national expenditures and their public-private composition, andassesses how both the level and the composition of expenditures are changing.Estimates of total health expenditures in developing countries, for example, rangefrom less that 1 percent of GNP in the poorest countries to 5 to 7 percent ofGNP in middle-income countries. The government's share of these expendituresmay account for only 30 percent of total health expenditures or may be as largeas 70 percent. Per capita spending around the world varies from less than US$1to more than US$800. The proportion of central government expendituresdevoted to health and medical care varies from a low of 1 percent to a high of32 percent. In absolute terms, health budgets in most countries have increased.However, slow economic growth and high population growth rates have producednegative real growth in government health budgets and in per capita healthexpenditures.

EXHIBIT 2FINANCIAL FLOWS IN THE HEALTH SECTOR
Loans and( ~~~~~graaV,"
~~~~~~GOVERNMET)_ ,
graf Sutskl Tax" ~~Tx uSb
\ / / } SutSdles \ l I~~~~~~~~~~~~~~~Sbsdi
Taxes Su\dO
PROVIDERS OF FINANCINGHEALTH SERVICES INTERMEDtARIES
PROVIDER 0
REIMBURSEMENTS U RIA
Utser \ / / Paym to 1bchrgs SerArb/Clhn have coverage
\ \* < * ~~~~~~~~~~~~~~~eimbursemns
( HOUSEHOLDS j
Source: de Ferranti (I 984).

16 Section One: Issues and Concepts in Health Economics and Financing
Next, the analyst identifies the patterns of expenditures among distinctcategories and classes of service, thereby developing a comprehensive accountingof what is spent and by which agencies to provide particular health services orhealth-related activities. This examination of all the material and financialresources involves data collection from ministries of health, other nationalgovernment departments, local governments, compulsory health insuranceagencies, industry and commercial enterprises, voluntary and religious groups,and other areas of the private sector. In most countries information aboutexpenditures in the private sector may be limited and incomplete. In the publicsector the full costs of health programs are not always known because someexpenditures may fall within other ministries. Maintenance and utilityexpenditures, for example, may fall outside the jurisdiction of the ministry ofhealth and be financed by other ministries. The analyst must remember thatbudgets reflect only the intention to spend rather than actual expenditures. Theamount spent is ascertainable only at the end of a fiscal year.
The structure for summarizing expenditures that ministries of health andnongovernment providers usually use includes only such categories as personnel,supplies and equipment, transportation, and training. The analyst must ascertainhow these expenditures relate to health programs and services. It is important todetermine how expenditures are allocated
e Among service activities: curative versus preventive, primary versussecondary/tertiary, low-technology versus high technology
* Among population groups: rural versus urban, within and acrossdistricts/regions/provinces, across ethnic groups and income levels
* Among input combinations: personnel, maintenance and repair of buildingsand equipment, medical and nonmedical supplies, and so on
i Among current andfuture services: recurrent versus capital costs
* Among disease patterns and categories: infectious versus chronic diseaseconditions.
Stating what the ideal allocation of expenditures for any of the abovecategories is not possible. The appropriate expenditure allocation for any countryis constantly changing. Decisionmakers must consider what allocations arereasonable and appropriate given national health goals and resource availability.
Affordability
Affordability is a necessary condition for achieving efficient and effectiveresource use (de Ferranti, Prescott, and Over 1991). Financing constraintsundermine the effectiveness and the continuity of health sector activities. Healthprograms and activities are affordable only if the financial contributions necessary

Financing the Health Sector: Expenditure Analysis and Affordability 17
for their continued operation, on the scale expected, can be made available.Sources of financial support can include the central government, localgovernments, other quasi-public providers such as social security or healthinsurance programs, communities, employers, private households, and externaldonors. A realistic, quantitative assessment of these sources of financial supportand the prospects for the continuity and growth of their financial commitmentsin relation to trends in the recurrent expenditures of health programs andactivities can be sobering. The potential for growth in the recurrent budgets thatcentral governments allocate to ministries is limited for most developingcountries. Given the large role that governments already play in financingpublicly provided health services, the capacity to meet the requirements of newinvestments may be restricted. Analysis of affordability stresses the need foradjustments in policies or programs to close resource gaps.

4. Basic Concepts of DemandTo appreciate how the basic economic concepts of consumer demand are
related to people's demand for health and medical care, several questions arerelevant for public health professionals:
* How is demand different from need and use?
- What factors or circumstances influence or determine demand?
- How can an improved understanding of the demand for health and medicalservices be helpful in planning and providing these services?
Need versus Demand
The need for medical care is generally viewed as the amount of medical carethat medical experts believe is necessary for a person to remain or becomehealthy, that is, what a doctor thinks a patient ought to have for a given healthcondition. The demand for medical care is what people select from the array ofpossible choices given their own perception of their health condition and theirsocioeconomic circumstances.
To base planning decisions regarding the quantity, type, and distribution ofhealth facilities and health personnel solely upon estimates of the need formedical care assumes that need itself is the main determinant of a consumer's useof health services. Need is only one factor affecting the consumer demand forhealth care. Resource allocations for health services based on need alone canresult in misallocations and an inefficient use of health resources. If, forexample, the amount of services that experts regard as necessary to meet medicalneed exceeds the amount that consumers actually choose to use, health facilitiesand service providers will be underutilized. These resources could be used moreproductively in another activity. Alternatively, if consumers use more medicalcare than would be provided on the basis of a need criterion, demand will exceedthe available services. The shortage of services will increase waiting time, createcongestion, and waste patients' time that could be spent in a more productiveuse.
18

Basic Concepts of Demand 19
According to standard economic theory, the demand for any good or servicestems from the income consumers have to spend, the prices they must pay, andthe wants or desires they wish to satisfy. Four major elements delineated instandard economic theory hold true for consumer demand of health and medicalcare:
* Consumers themselves decide what they need.
* Different individuals may make different demands even when their medicalcircumstances are the same.
* Demand, unlike need, depends on income.
* Demand depends on prices that include not only the monetary cost ofservices, but also the time required to travel and wait for services(Musgrove 1988).
The demand for health care and medical services represents what individualswant. Several factors are considered influential in the quantity or amount ofhealth services that a person consumes. These include the prices the individualor the family must pay for the services; certain socioeconomic, demographic, andepidemiological characteristics of the person; and the person's own perception ofthe need for medical care. A person's judgment about the quality of the serviceand characteristics of the medical provider and the environment are alsoimportant. Beliefs and tastes that further characterize consumers also have abearing on the quantity and type of health services they use.
Analysis of Demand for Health Care
The analysis of demand for health and medical care is an examination ofconsumer behavior or choice. An important purpose of an analysis of demand,therefore, is to identify those factors that are most influential in determining aperson's use of health and medical care services. Analyses of the choices thatconsumers make about their use of health services can help policymakers,planners, and managers to answer such questions as:
* What factors influence who will seek care?
* What factors explain underutilization or congestion of services?
* What factors determine the type of provider consulted?
* What barriers to utilization exist?
* What changes in the structure and organization of service delivery wouldenhance utilization?

20 Section One: Issues and Concepts in Health Economics and Financing
Perceptions of Illness
An individual's perception of illness is an important determinant of who seekscare and who responds to preventive and promotive activities. Where endemicdiseases have not been eradicated, substantial discrepancies may exist betweenthe judgments about illness that are made by medical professionals and those thatare made by the nonexpert consumer. People who live in communities wheremedically defined pathologies and impairments are common may recognize andseek treatment for fewer symptoms than people living in communities wherethese conditions are less prevalent.
The perception of illness depends on other circumstances as well.Urbanization and schooling, that is, whether a person is literate and what levelof education that person has attained, are important factors in how an individualperceives illness. Young children depend upon the perceptions and judgments oftheir parents about illness in order to receive medical care and treatment. Amother's level of education and literacy is an influential factor in seekingpreventive and curative services for her children. By itself, however, theperception of illness is insufficient motivation for seeking care.
Prices and Incomes
Prices and incomes are fundamental to the demand for health and medicalservices. Two economic principles are central and logical elements of demand:
* As the price of a service or good goes up, purchases and consumptiondecline.
* People with higher incomes can purchase and consume more ofeverything.
While these two principles predict the direction of the effects on consumptioncaused by differences in income levels or by changes in prices, they do notdetermine the magnitude of the effects.
An additional economic concept is relevant here. Price and income elasticitiesprovide essential information about the sensitivity of the quantity of goods andservices that consumers will demand when faced with changes in the prices ofthese items or in their incomes. The quantifiable nature of elasticities makes themuseful for predicting the response or change in demand that will result whenpolicies or market conditions generate changes in prices or incomes.
The price elasticity of demand measures the percentage change in the quantityof a good or service consumed for a given percentage change in price. If theprice elasticity of demand is high, demand is said to be price elastic. Smallincreases (decreases) in price will cause large reductions (increases) in thequantity consumed. If the price elasticity of demand is low, demand is price

Basic Concepts of Demand 21
inelastic, and demand for a good or service remains largely unaffected bychanges in price.
Similarly, the income elasticity of demand measures the effects of changes inincome on demand. Luxury goods tend to have high income elasticities whilenecessities have low income elasticities. This concept is important because itprovides information about demand responses from different income groups. Ifthe demand for health services is income elastic, it means that demand is veryresponsive to changes in income. The introduction of fees at public facilities, forexample, will cause different consumption responses by low-income and upper-income consumers.
Quality and Competition
Although prices, incomes, and the perceived need for health or medical careare important factors in understanding the demand for health services, otherfactors also play an important role in shaping consumer behavior. The role thatthe quality of medical services plays in influencing demand deserves specialattention. Quality is hard to measure. Often discrepancies exist between whathealth professionals and the general population consider to be essential elementsof good treatment. A typical example is that of patients who regard outpatientvisits to providers who do not give a prescription for a drug or injection asinferior to visits to a provider who does, even though the provider may considerthe medication ineffective.
Consumers' decisions are influenced by the choices available to them via thearray of health care providers. In effect, the extent of competition within thehealth sector can influence relative prices and quality options. The market forhealth and medical services may consist of consumer segments that have differentgeographic and income characteristics, and different providers may service thesesegments.
Traditionally, planning for the supply of health services within the publicsector has been based on medically defined, professionally determined need. Thisapproach results in poor resource allocation when what people want to consumedoes not coincide with what medical experts believe they should consume.Demand analysis-the study of consumer behavior-can promote and facilitateplanning based on demand information and resources, which will contribute toa more efficient and effective use of resources.

5. Production and Cost Analysis in theHealth Sector
Health services can be looked at from the same vantage point as any otherindustry or enterprise, that is, as a process for producing goods and services.This perspective raises two important questions for health professionals regardinghow "products" (health service and programs) can be produced at a lower costand with greater efficiency:
* What is production analysis in the health sector?
* What is cost analysis?
Production Analysis
Three interrelated, but conceptually distinct, components are common to allproductive activities: inputs, process, and outputs. Inputs include resources suchas people (labor), facilities, and equipment (capital) that are available for use ina productive activity. Process refers to the productive technique or technologythat changes inputs into outputs, and the current state of technology determineshow inputs are used. Outputs are the end result of production. Theserelationships are referred to as the production function, which is simply a wayof representing the relationship between inputs and outputs given thecharacteristics of technology. This relationship can be expressed bothqualitatively and quantitatively. Thus a production function indicates thecombination of inputs required to produce various levels of output in atechnically efficient manner, and it describes the productivity of the inputs. Usinginputs in different proportions or configurations will have different effects onoutputs.
In the health sector, several factors make the examination of productiverelationships somewhat problematic. Health care systems are complex productiveunits that use a wide range of different resources and produce many differenttypes of outputs simultaneously. Measuring and valuing both the inputs and theoutputs poses problems. Ministries of health, for example, allocate an array ofresources (inputs) among programs, hospitals, and primary health care services(production processes) to reduce morbidity and mortality or increase healthy days
22

Production and Cost Analysis in the Health Sector 23
of life (outputs). Relating a particular output to any one production activity isdifficult because multiple inputs interact to produce a variety of health outcomes.Nonetheless, relationships between inputs and outputs can be examined to assessthe productivity of some intermediate operations, for example, outpatient visitsper doctor, bed turnover rates per year, maternal child health visits per nurse,and so on.
Cost Analysis
Of all the popularized concepts in economics, costs and prices can be amongthe most confusing. The distinction between the two is a matter of vantage point.Individuals and organizations face both costs and prices depending on thedirection in which they are looking. An individual or organization can be botha buyer and seller at the same time. Thus any particular monetary value can beviewed as a cost or as a price, depending upon whether one is buyer or seller.Costs are associated with the monies used to buy, while prices are associatedwith offering supply for sale. Thus factor prices are the prices of inputsnecessary to produce a good or service. Costs of production are the costs tosellers of producing goods and services.
Costs represent the resources that are used up to obtain a good or service.These resources may be in the form of money, goods, leisure, time, income,security, power, or prestige. Cost analysis can focus on many different issues.Costs of production can be classified and analyzed in many ways for a variety ofpurposes. One essential purpose in examining costs is to assist decisionmaking.
A set of cost concepts used in economics explains the supply curve of a firmor industry, in this case the supply of health services. These concepts include thefollowing:
* Total cost is the value of resources used to produce a good or service. Itis primarily influenced by the state of technology and the prices for labor,materials, and other production inputs. Total cost varies directly with thelevel of output.
* Fixed and variable costs are components of total cost. Fixed costs arethose incurred regardless of the level of output and can only be decreasedin the long run. Variable costs are those that vary with the level of outputand can be changed by management in the short run.
* Average (unit) cost measures the resource requirements of productionassociated with each unit of output (total cost/total units of output).Average cost first decreases as output increases, and then begins to rise asthe marginal cost of producing more output rises.

24 Section One: Issues and Concepts in Health Economics and Financing
Marginal cost measures the rate of change in costs as output changes (thecost associated with increasing output by one unit). Marginal costdecreases at first as output increases and then rises because of economiesof scale. Marginal cost begins to rise before average cost does.
The relationship between production costs and varying levels of output isreferred to as a cost function. It expresses the impact on cost of producingdifferent amounts of output. The use of inputs in different proportions andconfigurations has an effect on cost as well as output. A cost function can beempirically derived from the observation of actual costs over some period oftime. Both economic and accounting approaches are commonly used. A statisticalapproach uses multiple correlation and regression analysis to relate cost to size,output, and fluctuations in input quantities or prices. An accounting approachuses accounting records to generate estimates of average costs at a point in time.
Two further concepts that relate to both the timeframe and function of costsare recurrent and capital costs. Recurrent costs, also called operating costs, referto the cost of the inputs connected with running an enterprise or delivering aservice. Recurrent costs vary with the level of output and are usually calculatedon an annual basis. Capital costs, also known as investment costs or replacementcosts, are the cost of employing durable goods and stocks of raw materials. Ineconomic terms, it is the rate of return foregone by not using the funds spent onparticular durable goods in other ways. In accounting conventions, it is themoney expenditure that is required to purchase goods that have a life of morethan one year. Understanding the relationship between capital and recurrent costsis important for health professionals. Capital costs generate recurrent costs, andthe r-coefficient is a ratio between a project's annual recurrent cost and its totalinvestment cost. The r-coefficients estimated for health are higher than thoseestimated for other sectors because health services are more intensive in their useof recurrent cost items such as staff, drugs, and supplies.
Other cost concepts in economics and accounting include the following:
* Opportunity cost is an economic concept that refers to the value of thebenefit that is given up when a choice is made to use resources in oneparticular way rather than in an alternative way.
* The concept of indirect costs applies in both an accounting and aneconomic sense. The use of resources for more than one activity, forexample, rent, electricity, administration, is an accounting concept.Managers refer to these costs as overhead costs. As an economic concept,indirect costs are associated with productivity losses associated with illnessor work time taken up by medical treatment.
* Direct costs are an accounting concept and are those costs that are tracedor attached to carrying out a single activity, for example, an immunizationprogram.

Production and Cost Analysis In the Heafth Sector 25
Efficiency and effectiveness are related to cost concepts. They are definedhere, but are taken up for a more comprehensive examination in the section thatdiscusses economic evaluation. Effectiveness is concerned with the technicalrelationship between input and output. It identifies the technical possibilities fortransforming inputs into a given level of output. Efficiency requires that one takeinto account the costs of the resources used in production and compare them withthe value of the output produced. It ranks alternative technical possibilities bycomparing the costs of the inputs with the value of the outputs.

6. Mobilizing Resources for HealthServices
As governments try to grapple with the difficult issues of the appropriate levelof funding for health and medical care and the appropriate allocation ofgovernment resources to health activities, health professionals may weighalternative approaches for mobilizing resources for health and medical services.Questions to consider include the following:
* What is the appropriate role for government in the financing and provisionof health and medical services?
* What are alternative mechanisms for mobilizing resources for the healthsector?
* What advantages and disadvantages do alternative mechanisms present?
Experts and governments have examined the following approaches to mobilizemore resources for health:
* Introducing charges (user fees) for curative care at government healthfacilities
* Providing health insurance or other risk coverage
* Expanding nongovernment and private providers.
Some basic principles underlying these approaches and historical experiences arebriefly described below.
User Fees
The prevailing wisdom argues that user fees at public facilities would increasethe resources available to the government health sector, permit greater spendingon health activities that are underfunded, encourage better quality of services, andimprove efficiency. When governments decide to charge fees at public facilities,they must
26

Mobilizing Resources for Health Services 27
* Set up a mechanism to collect and manage fees; health workers cannotnecessarily add this task to their responsibilities;
* Improve the quality of care so that utilization will not be reduced;
* Make decisions regarding who will spend the collected revenue and howit will be spent.
In designing a user fee system, governments must consider where as well ashow to introduce charges. Conventional wisdom dictates that economic principlesand administrative considerations should prevail. Exhibit 3 (Griffin 1988)presents a framework for thinking about where to introduce charges based onthese considerations.
A few countries have had user fees for decades. Many other countries haveestablished fee schedules, but few collect significant revenues. Very fewcountries recover more than 15 percent of health expenditures through fees. Themost common practices are to charge fees at hospitals for inpatient care, specialaccommodations, and outpatient visits. Most pricing policies incorporateexemptions and/or special prices for certain categories of patients or illnesses.
Social Insurance and Other Risk Coverage
An insurance program can be an additional source of revenue for the healthsector. It differs from the user fee concept in two ways. First, payment for andconsumption of health services are separated. An individual or a family purchasesthe insurance and then consumes the health service when someone is ill. Second,insurance spreads the risk of extreme illness over a group rather than having theindividual bear the full cost. Those enrolled in an insurance program pay theaverage cost of care for all those enrolled, but the person who becomes ill istreated at no extra cost.
Insurance programs face two difficult problems. First, sick people who areinsured are likely to consume more medical care than they would if they had topay for each unit of care. This extra use increases the cost of providing care anddrives up the payment that the insurance program must charge its enrollees. Thesecond problem is that of adverse selection: insurance programs are moreattractive to people who think they are likely to become ill. These problems canbe controlled by requiring partial payment from consumers at the time of service(copayments and deductibles) and by making enrollment in an insurance programmandatory for a predefined group. A health maintenance organization or aprepaid group plan combines the features of an insurance program with those ofa health care provider in a single organization. This type of an organization hasan incentive to minimize the cost of care without compromising quality care.

28 Section One: Issues and Concepts in Health Economics and Financing
EXHIBIT 3ECONOMIC AND ADMINISTRATIVE CONSIDERATIONS IN
INTRODUCING USER FEES
Economic Issues
Efficiency of use* Where are waiting times high?* Where are high-cost services used inappropriately?
Equity* What ability is there to exempt the poor?* What is the rural versus urban distribution of public resources?
Signaling* What are the criteria for resource allocation?* What does demand signal to system planners?
Price discrimination* Can revenues be enhanced?* Where is the potential for cross subsidies?* What are the equity effects?
Private versus public goods* Where are preventive services provided?• Where are curative services provided?
Risk and insurance
Administrative Issues
* Can patient flow be controlled?* What accounting mechanisms are already in place for collecting
fees?* Where are trained personnel available?* What supervision and control mechanisms exist for fee collection?* How will fee collection affect or be affected by decentralization?* What are the ready supply needs (for example, equipment or
drugs)?* What is the revenue potential from number of transactions, size of
fees, and third-party payments?

Mobilizing Resources for Health Services 29
Special problems arise for extending health insurance programs in developingcountries. The payment or premium that a health insurance program wouldrequire to cover the average cost of providing care is likely to be beyond thecapacity of low-income groups. Although governments could subsidize thepremium, the size of the subsidy is likely to be indistinguishable from whatgovernments currently pay for providing free care. Finally, a large proportionof the population in developing countries is rural and self-employed, raisingadministrative costs and making adverse selection hard to control.
The details of medical care under social insurance systems differ greatly fromcountry to country. The common features include the following:
* Coverage is generally limited to those with relatively stable wage-basedemployment whose dependents may or may not be included.
* Marginal wage earners and subsistence farmers are generally excluded.
* Most systems provide services directly through their own facilities, whichare generally better equipped, have better trained staff, and are lesscrowded than public facilities.
X Participants pay flat, regular contributions deducted from their paycheckswith few provisions for copayments or deductibles. Participation may becompulsory.
* Few incentives for efficient resource allocation are built into the system.
Expansion of the Private Sector
In terms of expenditures and quantities, the private sector is already involvedas a major provider of health services in most developing countries. Similarly,the private sector plays a major role in producing and supplying health productsand allied or logistical services. Private is defined here to include for-profitproviders and suppliers as well as voluntary, religious, charitable, and other non-profit operations.
It is argued that private provision widens choices for consumers, results inmore efficient use of inputs, and improves technology. A conceptual view of theprivate sector and its role in the health sector and the larger economicdevelopment process can provide an appropriate framework for developinginitiatives for private enterprise development in the health sector. Developmentor expansion of the private sector is not an end in itself, but a means to facilitateand promote the achievement of wider development goals. To be effective, aprivate sector strategy or portfolio for the health sector needs to be carefullyintegrated and synergistic with government health policies and objectives andwith policies for the general development of the private sector. Understanding theoperating environment for both health and private sector activities can help

30 Section One: Issues and Concepts in Health Economics and Financing
generate program and policy options and potential implementing partners andagents. The following sets of questions are suggested as a means of mapping theprivate sector and generating options.
Description
* How is government included in the health sector? What roles does it play?
* Who provides services in the private sector (for example, private practicedoctors, paraprofessionals, nurses, midwives, traditional healers, clinics,hospitals, employer-based facilities)?
* Who supplies products and allied goods and services (for example,pharmacy outlets, laboratories, housekeeping and laundry services, foodservices, maintenance services)?
* Who finances the purchase and provision of services (for example,individuals, households, private insurance, social insurance, employers,cooperatives, communities, religious groups, local and centralgovernment)?
* Where are private sector health activities located (for example, urban,peri-urban, rural, other distinct geographic areas)
* How large are these private sector activities?
Diagnosis
• How has the private health sector performed over time?
* What effects have public policies and regulation had?
* What are the major constraints impeding the expansion of private sectorhealth activities (for example, government policies; resources such ascapital, credit, technology, information, managerial expertise,infrastructure)?
* What is the private sector's perception of its opportunities and constraints?
Prescription
* What specific programs and projects will most effectively achieve thegovernment's goals and objectives?
* What set of criteria should be used to evaluate options?
* What initiatives is the private sector already undertaking?

Mobilizing Resources for Health Services 31
* How does what is desirable fit with what is feasible given thecompetencies and resources in both the government and private sectors?

7. Economic Evaluation and Health CareInterventions
The economic evaluation of health investments and programs can providehealth professionals and policymakers with responses to two fundamentalquestions:
- Are limited resources being used in the best way possible'?
e What is the value received from the resources expended'?
Economic evaluations are essential because resources are limited and must beallocated among competing alternatives. An essential purpose of any economicevaluation is to determine whether a project or program is a worthwhileinvestment. The criterion of economic efficiency requires that available resourcesbe used in a way that obtains the most output for the least cost. An economicevaluation is a way of assessing the array of possible choices with regard to thevalue of the output that can be expected against the resource costs that will benecessary.
Used as a tool in the process of identifying, designing, and selecting healthprograms and projects, economic evaluations help decisionmakers to make betterchoices. The question the health planning analyst must address is whether theexpected health outcomes (outputs) from a project or program are sufficientlyvaluable to warrant the expenditure of scarce resources for this as opposed toalternative uses. Any alternative allocation of these same resources for programsor projects that would result in a healthier population should be preferred. Thus,economic evaluations help health planners and government policymakers ensurethat they will get the most health benefits possible from the scarce resources attheir disposal.
Approaches to Economic Evaluation
Any economic evaluation concerns choices between alternatives, and alleconomic evaluations compare the real benefits with the real resource costs forthe proposed undertaking.
32

Economic Evaluation and Health Care Interventions 33
Economic evaluations r-ly or-i two basic analytical techniques: cost-effectiveness analysis and cud,t b. nef;t analysis. As is evident from their names,both approaches start with deternmining the costs of the alternative healthinterventions being considered. ( onsequently, the first step in either approach isto determine the direct operatinE costs and capital costs and the indirect costsincurred by the patients (suclh as imne lost from work or travel expenses). Wherethe two approaches differ i:; in the measurement of the consequences of theinterventions. Each appruac i s tiisc.issed below.
Cost-Effectiveness Analysis
Cost-effectiveness analysi,is Lan n'e a powerful tool for choosing betweendifferent techniqlues tor aichievi hg ilie same narrowly defined goal. Under thisapproach. effectiveness men-i u t art stated in terms of health outcomes, such asyears of life gained, days nin= hidity saved, or percentage reduction inmortality rates or disease incidlv- . ['he costs are related to these consequencesor outcomes. Cost etfectivenes, sunmmarizes all program costs into one numberand program benefits into a second oiumber. For example, the cost-effectivenessof different approaches to) oral rei yd ratio )n therapy compares different techniquesfor achieving the same output - I educing the number of deaths of children underfive years old---or the cost-el fect ver-ess of different medical techniques comparesthese techniques in relation to the iiumber of healthy years of life gained. Theintervention with the lower c st-efctiveness ratio is preferred, that is, thealternative that takes fewe! re out -es to achieve the same or greater healthbenefits.
A companion measure !I at _in I c used when outcome measurements are notavailable or are considered uinm Aii!71e would he a cost-efficiency or least-costindicator. This approach calculi-tes the costs to deliver a unit of health care, forexample, cost per iminunizatitn l r cost per contraceptive device delivered.Under the assumption that tht li alth care units delivered under alternativemethods of intervention would :est It in the same health improvement outcome,the one with the lower dJelive.r% cois per health care unit is preferred.
Cost-Benefit Analysis
In cost-benefit analysis the hea,th improvement outcomes derived from theproject or program are translated in,-o) monetary terms. For example, added yearsof life can be valued as the addittio ial net income that would be earned throughthe individuals' extendedi work ner od. Decreases in morbidity can be quantifiedin terms of recaptured work, da s productivity improvements. One could alsoadd in any savings in ongoomg he<,lSh care costs that would have been needed tocontinue to treat the illnes-. 1 "se figures are often difficult to estimate, but ifone is able to. then as Iong tS . /c economic benefits exceed the costs, theprogram is beneficial. I hose v itth ower costs relative to the benefits generatedare preferred when choosliig ai-n,or alternatives.

34 Section One: Issues and Concepts in Health Economics and Financing
Discounting
In both approaches, the analyses need to consider the timing of the costs andthe health outcomes. Obtaining the benefits sooner rather than later is usuallypreferable, but the pattern of when benefits occur and when expenditures areincurred can vary across type of intervention. The way to make these differenttime patterns comparable is to use an economic discount rate, which expressessociety's time preferences. You might consider this like an interest rate. Forexample, US$100 earned five years from now is less valuable to you thanUS$100 earned today, because you could put that in a bank and earn interest forfive years, thereby accumulating more than US$100. Thus, the cost and benefitstreams should be discounted and the present value compared to determine thepreferred alternative.
Sensitivity Analysis
Many of the costs and consequences used in these economic evaluationapproaches are difficult to estimate precisely. Therefore, in consideringalternatives it is useful to use a range of estimates, for example, low, high, andexpected, to test the results to such variations. Some alternatives might be moresensitive than others, and this could influence their relative desirability. Also, ifsuch calculations reveal that the results are relatively insensitive to suchvariations, then one's confidence in the likelihood of the outcomes should begreater. If some variables are revealed as being particularly sensitive, thenfurther investigation into these variables might be warranted to examineassumptions, or even to adjust the intervention's design to reduce this variability.
Nonquantifiables
Many health outcomes are difficult to quantify and even more difficult toattach economic values to. For example, a patient's life might be saved throughan intervention but the patient remains handicapped in some significant way. Thevalue of those added years of life are not equal to those of added years withoutsuch an impediment. Consequently, valuation will require some subjectivejudgment that incorporates quality of life considerations.
At the outset of the economic evaluation, health planners must have a clearunderstanding of what they are trying to achieve as well as how to compare theamount and value of resources with the amount and value of the output. Whereoutputs can be converted easily to monetary terms, an economic analysis providesone measure by which to compare and evaluate projects. If outputs arequantifiable, but not easily reduced to monetary values, economic analysis allowspolicymakers to make judgments about projects based on the real resource costsper unit of output. Where outputs cannot be quantified, economic analysisprovides a basis for making choices between competing alternatives on a least-cost basis. An evaluation of projects that focuses on economic analysis enablesdecisionmakers to select from among alternative options as well as to chooseamong different projects in the same sector or from different sectors.

Economic Evaluation and Health Care Interventions 35
Although economic evaluation cannot always be entirely precise and accurate,these approaches do enable us to make the difficult choices inherent in allocatingscarce health resources more systematically and rationally.

8. Further Readings and References
Economic Development and the Health Sector
Belassa, B. 1987. "Structural Adjustment Policies in Developing Economies."World Development 15(10):23-38.
Bell D., and M. Reich. 1988. Health, Nutrition and Economic Crisis:Approaches to Policy in the Third World. Dover, Massachusetts: Auburn House.
Heilbroner, R., and L. Thurow. 1978. Understanding Macroeconomics, 6th ed.Englewood Cliffs, New Jersey: Prentice-Hall.
Leslie, J. 1986. Weathering Economic Crises: The Crucial Role of Women inHealth. Washington D.C.: International Center for Research on Women.
Musgrove, P. 1986. "The Impact of the Economic Crisis on Health and HealthCare in Latin America and the Caribbean." WHO Chronicle 40(4):152-57.
Samuelson, P. 1973. Economics. New York: McGraw-Hill.
Basic Concepts of Demand
Mills, A., and L. Gilson. 1988. Health Economics for Developing Countries: ASurvival Kit. London: London School of Hygiene and Tropical Medicine,Evaluation and Planning Centre for Health Care.
Musgrove, Philip. 1988. "Some Reflections on Demand for Health in LatinAmerica." Cuadernos de Economia (66):99.293-305.
Over, Mead, ed. 1991. Economics for Health Sector Analysis: Concepts andCases. Washington, D.C.: Economic Development Institute of the World Bank.
Stigler, J. 1966. The Theory of Price. New York: Macmillan.
36

Further Readings and References 37
Financing the Health Sector: Expenditure Analysis andAffordability
de Ferranti, D. 1984. Strategies for Paying for Health Services in DevelopingCountries. PHN Technical Notes GEN 25. Washington, D.C.: World Bank.
de Ferranti, D., N. Prescott, and M. Over. 1991. 'Affordability and theFinancing of Health Projects." In M. Over, ed., Economics for Health SectorAnalysis: Concepts and Cases. Washington, D.C.: Economic DevelopmentInstitute of the World Bank.
Mach, E.P., and B. Abel-Smith. 1983. Planning the Finances of the HealthSector: A Manualfor Developing Countries. Geneva: World Health Organization.
Mills, A., and L. Gilson. 1988. Health Economics for Developing Countries. ASurvival Kit. London: London School of Hygiene and Tropical Medicine,Evaluation and Planning Centre for Health Care.
Over, M., ed. 1991. Economics for Health Sector Analysis: Concepts and Cases.Washington, D.C.: Economic Development Institute of the World Bank.
World Bank. 1987. Financing Health Services in Developing Countries: AnAgenda for Reform. Washington, D.C.
Production and Cost Analysis in the Health Sector
Heller, P. 1979. "The Underfinancing of Recurrent Development Costs.'Financing and Development 16(1):38.
Over, M. 1991. Economics for Health Sector Analysis: Concepts and Cases.Washington, D. C.: Economic Development Institute of the World Bank.


Section Two
Applied Experiences in Health Economicsand Financing


Overview: Using the Case Method
Since one of the purposes of the seminar series on health economics andfinancing in Latin America and the Caribbean was to acquaint high-levelpolicymakers with the latest thinking on the relevant issues, a search wasundertaken to identify pertinent articles and background reading sources. At thetime, there were few readings that went beyond theory to application ofprinciples to the health sector of developing countries. What was available largelyfocused on regions other than Latin America and the Caribbean, and was onlymarginally useful. Furthermore, almost nothing was available in Spanish. Toaddress this problem, EDIHR first translated a core selection of reading materialsinto Spanish, and then began a process of commissioning papers and case studiesthat more closely aligned with the educational needs of the audience.
The cases included in this book were written to help health practitionersacquire practice and experience in using economic and financing tools andanalyses to solve problems and make decisions in the health sector. The goal isto increase the understanding of economics and financing issues by using cases.Because the use of the term case or case study is widespread and can refer tolegal or medical cases, to business cases, to social workers' cases, to case studiesthat are historical accounts or documents, or to social science researchinvestigations, it is useful to establish what we mean by the term. Cases as usedin this book refer to descriptions of real-life situations or problems that requireanalysis, decision, and action. They are intended for use as tools for learning andteaching, and can be further characterized as vehicles for case method teaching.
Cases may be used in many ways. They may serve as exercises or assignedreadings to illustrate a principle that a resource person has introduced in anoverview presentation. However, the case method refers to discussions of aplanned sequence of cases whose purpose is to assist health, planning, andfinance professionals to
* Gain an understanding of the principal economic and financing problemsand issues, and concepts pertinent to the health sector;
41

42 Section Two: Applied Experiences in Health Economics and Financing
* Develop proficiency in producing and evaluating ideas about ways tomanage effectively the economics and financing problems encounteredduring their professional work;
* Acquire skills in selecting and implementing alternative courses of action.
Case method teaching and learning has a long history as an effectivepedagogical approach to developing problem-solving and decisionmaking skills.It is based on the philosophy that seminar participants learn most effectivelywhen they take an active part in and responsibility for the learning process. Acase discussion is a highly participatory form of learning, especially suited toadult education, in which participants and session leaders work as partners andshare the responsibility for the learning process. Students, in fact, have a greatdeal of control over what they learn from cases.
The case method approach to learning has proven to be particularly useful inhelping policymakers, planners, and managers to develop new skills andperspectives for conducting their work. Three basic characteristics of the casemethod render it particularly effective for training executives and practicingprofessionals, namely:
* It is based on reality and is applied rather than theoretical.
* It facilitates the exchange of ideas, perspectives, and analyses.
* It develops new techniques and skills while drawing on the participants'experience.
Cases are the pedagogical vehicles through which participant involvement isgenerated. As used at many institutions of higher learning, they are factualdescriptions of actual circumstances that decisionmakers in business, government,or other situations have faced. Generally, case studies focus on a specificdecisionmaker confronted with a set of alternatives. However, some cases focuson the macro appraisal of the country and the health sector situation, as in thefirst case in Mexico, or the overall appraisal of the health sector andidentification of policy options, as in case three on St. Lucia or case four on ElSalvador. As educational tools, cases are designed to facilitate discussions. Theydo not set forth theories or hypotheses, but present pieces of the real world in aform that allows individuals, either on their own or within the context of aseminar or training session, to think purposefully about issues that are relevantto their work. Cases do not include an analysis or evaluation of the situation, butprovide the raw material from which individuals can engage in their own analysisand draw their own conclusions.
The content, scope, organization, and orientation of all cases are designed tofit an overall plan for the use of materials, a blueprint or strategy that is laid outto achieve certain learning objectives. Each of the cases in this book is preceded

Overview: Using the Case Method 43
by a brief introductory paragraph that relates the case to the economic themespresented in Section One. Technical readings or lectures that transmit conceptualor technical material and provide basic information on relevant substantive topicsthat will be applied in the case discussions can supplement the cases.
The case method requires that an individual read the case and undertake hisor her own analysis. Study questions prefacing each case will facilitate and guidethis process. In some seminar settings participants may have an opportunity tomeet in small groups to share ideas and analyses and seek clarification on anyconfusing points. These discussions allow participants to exchange insights andpreliminary analyses. A structured discussion involving all the participants andled by a resource person or facilitator usually enhances and builds on small groupdiscussions.
The responsibility of seminar participants in this process is to participateactively. They should try to build on other participants' comments and be willingto venture a different perspective or idea, even though it seems far from howothers have been looking at the situation. Such contributions often open newavenues of discussion and insight. Challenging other participants' proposals oranalyses to ascertain their validity is also appropriate. For an individual,defending your own analysis or recommendations helps develop greater analyticaldepth. The learning process is continuous and occurs at each stage. The learningprocess does not end with the completion of a discussion because the case raisesquestions and creates new avenues for exploration. It is the process of explorationthat is the unending journey of decisionnakers.
In preparing for a case discussion, the critical first step is for each participantto read and analyze the case. A useful discussion will be impossible if theparticipants have only cursorily read the case. Thorough preparation pays biglearning dividends.
As a process, participants should start by skimming through the case to geta feel for the nature of the problem situation and the components of the case.Study questions presented at the beginning of each case provide guidance for amore careful and thorough reading. In subsequent readings, participants shouldtry to
* Identify what critical problems or issues confront the sector and/or thedecisionmakers
* Identify and assess the causes of those problems
* Formulate alternative ways to deal with the problems
* Assess the advantages and disadvantages of each alternative
* Specify recommendations and implementation steps that are realistic andfeasible.

44 Section Two: Applied Experiences In Heath Economis and Financing
Discussion promotes rigorous thinking and helps develop communicationskills. It encourages people to "think on their feet." For participants, talking ina seminar, expressing and defending their views, is one of the most valuableparts of an educational experience. It is also important for all to listen to theviews of others. The measure of a case discussion should not be based on aperson's assessment of whether his or her ideas were right, but instead should berelated to the greater understanding of concepts and analysis taken from a wide-ranging discussion of viewpoints.

Case Studies

Case 1. Macroeconomics and Health:The Case of Mexico
Study Questions
This first case focuses on a macro appraisal of the Mexican economy inrelation to the health sector. It provides an opportunity to consider and examinethe issues and economic concepts presented in Section One's discussion ofEconomic Development and the Health Sector as they apply in the Mexicancontext. The case describes Mexico's development strategies, policies, andmacroeconomic performance during the 1965-88 period. Information is alsoprovided on health sector expenditures and health status. An analysis of theMexican experience reveals the linkages between macroeconomic policies andhealth. The national income and expenditures model presented in Section Onewill facilitate this analysis. The case permits an examination of the causes andcures of economic crises and their impact on the health sector. The reader shouldtry to identify what critical problems confront the health sector, what kinds ofalternatives can be formulated, and who can or should make decisions about thechoice of alternatives.
1. What conclusions do you draw regarding (a) the growth of Mexico's economybetween 1965 and 1982, and (b) the gains in health during the same period?
2. How do you evaluate the economic sustainability of the health gains?
3. What policies and forces contributed to the economic crises of 1976 and 1983and how?
4. What forces affected health status during Mexico's economic crises? By whatmechanisms did they do so?
5. How did economic crises affect institutions that deliver health services?
6. How did macroeconomic policy actions taken to correct Mexico's economiccrises affect health status and health service institutions?
7. How important is having a healthy economy to achieving a healthypopulation?
8. What should health service institutions do in economic good times to preparethemselves to cope with economic bad times?
46

Macroeconomics and Health: The Case of Mexico 47
Macroeconomics and Health: The Case of Mexico
On December 1, 1988, Carlos Salinas de Gortari succeeded Miguel de laMadrid as president of Mexico. The new president had narrowly won the mostkeenly disputed election in Mexico's history. President Salinas used hisinstallation address to broadcast his intention to continue his predecessor'seconomic adjustment policies and to restore the country to a path of sustainableeconomic growth.
President de la Madrid was the first president in modern Mexican history whowas forced to grapple with negative economic growth rates. When he took officesix years earlier, de la Madrid was confronted with annual inflation that hadsoared to nearly 100 percent, a government budget deficit that had reached arecord high, and a worldwide reaction to Mexico's announcement that it couldnot pay the interest on its foreign loans. To correct these macroeconomicproblems and restore economic growth and stability, de la Madrid'sadministration entered into a stabilization agreement with the InternationalMonetary Fund (IMF). Under the terms of this agreement, Mexico agreed tocarry out structural adjustments that would shift the country's developmentstrategy from import substitution to export promotion. This shift compelled thecountry to diversify exports so as to reduce its dependence on oil, lower its tradebarriers to create pressure for international competitiveness, reduce governmentsubsidies, and renegotiate the servicing of foreign debt.
As Carlos de Gortari Salinas assumed his new presidential role and de laMadrid concluded his administrative tenure, inflation was reduced by half,modest economic growth was restored, debt servicing resumed, and the budgetdeficit was curtailed. These economic achievements were not wrought withoutpain and anguish. Real wages plummeted nearly 40 percent during this period ofeconomic stress, and per capita income dropped 15 percent. The administrationof the new president would need to address these effects as it continuedimplementing the economic stabilization policies.
Early Development Strategies and MacroeconomicPolicies
During the late 1950s and 1960s, Mexico pursued an industrial developmentstrategy that was based on protecting its newly emerging manufacturing sectorfrom foreign competition through government import tariffs and quotas. Thegovernment gave long-term loans to industry at subsidized interest rates,developed infrastructure, and even invested directly in some basic industries.Policies focused mostly on developing large manufacturing, although they also
This case was written by Catherine A. Overholt, Collaborative for Development Action, Inc., with fundingprvidedby the Economic Development Institute of the World Bank. The case is intended for use as a basisfor classroom discussion rather as an illustration of either effective or ineffective handling of a managerialor development situaton.

48 Section Two: Applied Experiences in Health Economics and Financing
stimulated commercial agricultural exports through extensive irrigation projectsand modern production technology.
The growth of Mexico's economy during this period was based on rapidindustrialization by developing the domestic market. Three elements critical tothe economic strategy were trade protection, a system of relative prices andsubsidies that favored industry over the primary sector, and direct economicparticipation by the government in infrastructure investments and parastatalenterprises. In addition to railroads and oil, which traditionally had beengovernment owned, other industries such as electricity, telephones,petrochemicals, and steel came under public control. Foreign investmentincreased between 1950 and 1970 as large firms established predominantpositions in the protected manufacturing sector.
A key feature of the development strategy from 1954 to 1970 was fiscal andmonetary discipline, that is, relatively tight fiscal and monetary policies to ensuremacroeconomic stability. Although there were modest fiscal deficits, they did notpose financing problems because domestic and foreign savings were sufficient tocover them without exerting pressures on the financial markets.
This development strategy was successful in attaining rapid economic growth.Between 1961 and 1973, Gross Domestic Product (GDP) increased on average6.6 percent annually in real terms. Public debt as a proportion of GDP remainedstable. Foreign indebtedness was relatively modest, inflation was low, and theexchange rate in relation to the US dollar remained stable.
Mexico During the 1970s
The incoming administration of President Luis Echeveria in 1970 faced alteredmacroeconomic and social circumstances. Economic growth rates had slowed andagricultural output was running behind population growth. The developmentstrategy had succeeded in reducing imports of consumer goods, but not of capitalgoods, and exports of manufactured goods were not growing. By 1970 thecurrent account deficit had risen to almost US$1 billion, a 157 percent increaseover 1965.
On the social side, Mexicans migrated to the cities in increasing numbers. In1950, 43 percent of the population was urban, but by 1970 this proportion hadrisen to 59 percent and would rise to 70 percent by 1988. Mexico City attractedmore than one-third of the population and it grew faster than the nationalpopulation. Per capita incomes rose, but the distribution of income became moreskewed.
The administration of President Echeverfa responded with more expansivefiscal and monetary policies. To improve income distribution the governmentexpanded subsidies for food and other basic commodities and also increasedspending on health and education. It invested in and promoted import substitution

Macroeconomics and Health: The Case of Mexico 49
in capital goods to counter the effects of a slow growth rate and infrastructurebottlenecks. The direct participation of the government in the economy grewdramatically. Total public sector expenditures rose from 18.5 percent of GDP in1965 to 28.9 percent by 1975. The number of parastatal enterprises tripled to845, and their total expenditures expanded to 52 percent of overall publicexpenditures.
Control of government expenditure became more difficult and spendingoutpaced revenues. Fiscal and current account deficits continued to grow, andinflation ballooned to 30 percent. The government met deficits by increasinglevels of foreign indebtedness. Public debt rose to 9.9 percent of GDP. Thesemacroeconomic imbalances reached crisis proportions in 1976. Curtailment offoreign financing and the loss of international reserves forced Echeveria todevalue the peso in August 1976, the first time the peso had been devalued since1954. Mexico turned to the IMF for a standby loan agreement.
President Jose Lopez Portillo implemented an austerity program when he wasinaugurated in December 1976. By 1978 the balance of payments had improved,the fiscal deficit had been reduced, and inflation fell. External economicconditions enhanced the effect of this austerity program. The international priceof oil rose, thus improving the terms of trade for what was becoming Mexico'smajor export. At the same time, major new oil discoveries placed Mexico as thefourth largest oil-producing nation in the world. This position provided Mexicoeasy access to foreign credit. Lopez Portillo ended the IMF stabilizationagreement and launched an aggressive growth strategy that expanded Mexico'seconomy at an unprecedented annual rate of 8.5 percent annually between 1978and 1981.
Government expenditures grew rapidly. The wages and salaries of governmentemployees were increased, subsidies for basic commodities continued to grow,and the government invested in oil exploration and production as well as in steeland seaports. The number of parastatals rose to more than 1,200 and publicsector expenditures grew by more than 40 percent between 1975 and 1980.Central government expenditures for health more than doubled, in real terms,between 1976 and 1979.
Health Sector Finance and Structure
In Mexico, four institutions were federally financed to deliver health servicesto the general population: the Secretariat of Health (SSA), the System forIntegrated Development of the Family (DIF), the Medical Services Departmentof the Federal District (DDF), and the General Program Coordination for theNational Plan for Deprived Zones and Marginalized Groups(IMSS-COPLAMAR). The Mexican Institute of Social Security (IMSS) providedhealth services to a large percentage of the population in the formal wage laborsector, and the Institute of Security and Social Services for State Workers(ISSSTE) provided health services to government bureaucrats. The IMSS was

50 Section Two: Applied Experiences in Health Economics and Financing
financed by contributions from the government, employers, and employees. TheISSSTE was financed by contributions from workers and the government.
The budgets of these health institutions continued to grow between 1976 and1981 (see Exhibit 1). During the early 1980s, the National Health System wasestablished to consolidate the health sector and pursue two major objectives:expand the coverage of health services to the population at large, with priorityfocused on rural and marginal population groups; and raise the quality ofservices. Exhibit 2 presents an overview of health status indicators during the1960s and 1970s.
Economic Crisis
Imports poured into the country faster than the pace of exports as Mexicobecame increasingly dependent on revenues from its oil exports and non-oilexports deteriorated. The expansionary government spending pushed the fiscaldeficit from 3 percent to 8 percent of GDP by the early 1980s. To cover thegrowing fiscal and balance of payments deficits the country doubled its publicforeign debt between 1979 and 1981 to US$78 billion. External shocksexacerbated the country's situation. Rising interest rates abroad and fallinginternational oil prices made it difficult for the government to continue fundingits rising deficits with new loans. The fixed exchange rate became increasinglyovervalued, and real negative interest rates triggered massive capital flight. In1982 the economy stagnated and inflation soared toward 100 percent. On August15, Mexico announced to the world that it could not make its foreign debtinterest payments, which were twice its liquid reserves. Lopez Portillonationalized the banks on September 1 and instituted foreign exchange controls.By December, when de la Madrid assumed the presidency, the foreign debt hadballooned to US$91 billion.
Adjustment and Macrostabilization
De la Madrid, whose public career had been in the Treasury and the CentralBank, regarded control of public finances as the backbone of an economicadjustment program. He regarded curbing inflation as a prerequisite to renewedeconomic growth. His new administration implemented a three-year stabilizationprogram formally agreed upon with the IMF in late 1982. The program consistedof two phases: an initial shock relying on tight monetary and fiscal policiesfollowed by a gradualist approach to restore economic stability.
Budget cutting was fierce during the first two years of de la Madrid'spresidency. Subsidies on basic price-controlled commodities were slashed. Thevalue added tax and prices for public sector goods and services, such aselectricity and gasoline, were rapidly increased. The government's investmentbudget plummeted to 1960 levels. The public sector borrowing rate was reducedfrom 17.9 percent in 1982 to 7.1 percent by 1984. To further combat inflation,the government held increases in the minimum wage to rates that were lower than

Macroeconomics and Health: The Case of Mexico 51
inflation. The peso was sharply devalued with the intent to spark growth andnon-oil exports. The real devaluation of the free exchange rate was on the orderof 160 percent.
The results in terms of inflation were not as promising as expected. The actual1983 inflation rate was 81 percent compared with the expected rate of 55 percent.Output also had contracted more than was anticipated, and the GDP declined 4.2percent. The gradualist approach to restraining inflation set key prices in theeconomy-the minimum wage, the exchange rate, public prices-to expectedinflation rather than past inflation. This strategy aimed to curb the public'sinflationary expectations. The minimum wage, officially determined by thegovernment and used as a benchmark for wages throughout the country, was setto an inflation rate that was expected to be lower than historical rates of inflation.Inflation continued a downward trend through 1985, but less rapidly thanexpected. Exhibit 3 provides an overview of the performance of the Mexicaneconomy.
The GDP recovered to a 3.6 percent growth rate in 1984. When fiscaltightening eased in 1985, the deficit increased, inflation accelerated, and the pesobecame overvalued. Several circumstances combined to provoke a balance ofpayments problem: international oil prices collapsed, the terms of trade turneddownward, a massive earthquake rocked Mexico City, and capital flightincreased. High interest rates and decreased demand from the deep cuts in realwages reduced the incentive to invest and led to rising unemployment and aneconomic contraction. The devaluations necessary to encourage exports inflatedthe peso price of imports.
The collapse of the Mexican stock market in 1987 and skyrocketing three-digitinflation in the face of an economic contraction led the Mexican government toseek alternative policies. In December 1987 business, labor, and governmentformulated the Economic Solidarity Pact, which was based on the idea thattoday's inflation is passed on from yesterday through wage and price contracts.To break this cycle the government, labor, and the private sector agreed toimpose a wage and price freeze. The peso was devalued by 22 percent, and themaximum tariff on imports was cut in half to 20 percent. To achieve a budgetsurplus, government expenditures were reduced and revenues increased. Creditbecame extremely tight.
By the end of 1988 when de la Madrid turned the presidency over to Salinasde Gortari, GDP growth had started again, the balance of trade was in surplus(despite falling oil prices), and the share of nonpetroleum goods in exports hadrisen from 22 percent in 1982 to 68 percent. There was a fiscal budget operatingsurplus, foreign debt levels had stabilized, and interest payments on that debt hadfallen as a share of GDP. Inflation had been slashed from the 1987 peak of 140percent, but remained high at 52 percent.

52 Section Two: Applied Experiences in Health Economics and Financing
Adjustment, Welfare, and Health
The crisis and adjustment process entailed major cuts in governmentexpenditures. As the share of public expenditures allocated to debt servicing rosefrom 25 percent in 1980-81 to more than 40 percent in 1983-84, the governmentcut back expenditures in all other categories (see Exhibits 4 and 5). To reducepublic outlays the government eliminated general food subsidies for items suchas cooking oil, bread, and eggs. Some food subsidies were replaced withsubsidies targeted to particular population groups. CONASUPO, thegovernment's food distribution chain, for example, sold a cheaper tortilla, thestaple of the popular diet. With the reductions in food subsidies, the cost of abasic food basket as a percentage of the minimum wage rose from 30 percent in1982 to 50 percent by 1985. Total consumption of beef declined by 45 percentbetween 1982 and 1988, and bean consumption, the primary source of proteinfor Mexico's poor, fell by 34 percent.
Government social expenditures, which include health, education, and socialsecurity, had fallen in relative terms since 1975, when they were 21 percent oftotal expenditures. In 1985 social expenditures fell to about 13 percent of totalgovernment expenditures, and were 23 percent lower than in 1982 (see Exhibit6). Exhibits 7 and 8 depict the evolution of the budgets and sources of financefor the public institutions of the health sector between 1979 and 1988. Exhibit 9provides estimates of population coverage. Exhibit 10 summarizes hospitaldischarges and outpatient visits for each of the health sector institutions over aten-year period. Exhibits 11 and 12 summarize the changes in budget allocationsto preventive, curative, and administrative activities and the availability ofresources within health institutions.
Real wages for public providers of health services declined. The cumulativedecline equaled 31 percent in 1985 and contributed to a decline in the share ofwages in total institutional income (see Exhibit 13). The drop in real wages fordoctors, nurses, and other employees, combined with the decline in grossinvestment, contributed to reducing health expenditures. In the agriculturalsector, output grew, employment rose, but real wages declined substantially. Therelative weights of the two sources of rural household income-wage andnonwage-determined the effect of the crisis on the rural family.
Nonwage earnings for practically all sectors increased in 1984. The nonwageincome category includes profits, rents, and interest. This income accrues to thewealthier segment of the population and to households that earn mixed incomesfrom small shops, home factories, and self-employment. Sectors with largeinformal employment experienced a smaller improvement in total nonwageincome. The rate of open unemployment was 2.4 percentage points higher in1983 than 1981.
Before the 1983 crisis, Mexico's poor already lived in precarious conditions.At the start of the decade, 35 to 40 percent of all households earned a total

Macroeconomis and Health: The Case of Mexico 53
income below the prevailing minimum wage. About 45 percent of the populationdid not receive adequate health care; 50 percent of households had no runningwater and sewage services and 25 percent lacked electricity; 22 percent hadneither water, sewage services, and or electricity. Approximately 20 percent ofthe population was estimated to suffer from malnutrition.
Between 1982 and 1985 the countrywide infant mortality rate did not rise.Exhibit 14 compares the causes of infant mortality during the last two decades,and Exhibit 15 indicates the percentage change in causes of death between thetwo decades. Infant deaths caused by avitaminosis and other nutritionaldeficiencies increased in 1982 after declining steadily prior to 1981. The ISSSTErecorded an increase in the total number of infants who suffered from slow fetalgrowth. The absolute number of children served by the ISSSTE who died ofnutritional deficiency also increased after 1982. Exhibit 16 provides an overviewof preschool mortality by region.

54 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 1HEALTH SECTOR BUDGET BY INSTITUTION, 1976-79
(millions of 1980 pesos)
Institution 1976 1977 1978 1979
Secretariat for Health (SSA) 11,478 17,712 19,489 21,020
System for Integrated N/A 1,104 3,165 3,544Development of the Family(DIF)
Medical Services Department N/A N/A N/A 3,632of the federal District (DDF)
National Plan for Deprived 1,180Zones and MarginalizedGroups (IMSS-COPLAMAR)a
Total 11,478 18,816 22,654 29,376
Populations (millions) 62.0 63.8 65.7 67.5
N/A: Not availablea. Program began in 1979.Source: Cruz, Lozano, and Querol (1990).
EXHIBIT 2BASIC HEALTH INDICATORS, 1965 and 1984
Indicator 1965 1984
Life expectancy at birth (years) 59 66Males (years) 58 64Females (years) 61 68
Crude birth rate (per 1,000 population) 45 36
Crude death rate (per 1,000 population) 12 7
Infant mortality (per 1,000 population) 91 54
Child death rate 10 4
Population per physician 1,830 1,260
Source: World Bank (1985).

EXHIBIT 3AGGREGATE PERFORMANCE OF THE MEXICAN ECONOMY, 1978-88
Yearly averageEconomicindicator 1978to 1981 1982 1983 1984 1985 1986 1987 1988
Gross Domestic Product (% annual growthrate) 8.5 -0.6 -4.2 3.6 2.5 -3.7 1.5 1.1Population (millions) 71.4a 73.1 74.9 76.7 78.5 80.1 81.7 83.2GDP per capita (% annual growth rate) 6.0 -3.0 -6.5 1.1 0.1 -5.9 -0.5 -0.6Average annual inflation (%) 28.7a 98.8 80.8a 59.2 63.7 107.0 159.2 51.7Gross Fixed Investment (% of GDP) 26.4a 23.0 17.5 17. ga 19.1 19.5 18.4 19.0Total consumption (% of annual growth rate) 7,7a 1.2 -6.8 3.0 2.0 -1.8 -0.3 2.0Non-oil exports (% of annual growth rate) 3.1 11.3 34.0 20.6 -7.9 40.9 23.7 16.0 9Imports (% of annual growth rate) 25.9 -37.1 -41.7 19.7 11.8 -11.7 5.6 44.7Public Deficit (% of GDP) 14.18 16.9 8.6a 8.5 9.6 15.2 16.0 12.3 oCurrent account surplus (% of GDP) -5.88 3.7 3.8 2.58 0.7 -1.3 2.8 -1.4 oTotal foreign debt (end of period in US$ Obillion) 74,9a 87.6 93.8 96.7 97.88 101.0 107.5 100.4Real free exchange rate (1978 = 100) 91.1 208.8 161.8 123.7 140.0 N/A N/A N/ATerms of trade (1980 = 100) 103.08 97.0 77.0 77.0 73.0 N/A N/A N/A EUnemployment rate (%) 5 3b 42 6.6b 5.7 b 443 b 395b I
Real average wages (% of annual growthrate) 4.2 -2.4 -26.5 -4.9 1.0 N/A N/A N/AReal minimum wages (% of annual growth =r
rate) 1,3a 3.3 -25.2 -8.3 -1.28 N/A N/A N/A 0O
N/A: Not available.a. For 1981. x.b. For 1984 and 1985 weighted average of sixteen cities. The rest of the years include only Mexico City, Guadalajara, and Monterey. 0Source: Cruz, Lozano, and Querol (1990), Lustig (1990); World Bank (1990). en
(1

56 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 4PUBLIC EXPENDITURE PER CAPITA, 1970-87
7
6 - A0Ua 5
a)
3 ~ ~ ~ ~
0 2
0
- Public expenditure
-4- Public expenditure (adjusted for debt service)
Sourcew: Instituto Nacional de Salud Puiblica (11990).

Macroeconomics and Health: The Case of Mexico 57
EXHIBIT 5PER CAPITAL INVESTMENT IN HEALTH, 1970-87
350
e~ 300
e0@ 150
c 150
so
1970 1971 1972 1973 1974 1975 1976 1977 1978 1979 1980 1981 1982 1983 1984 1985 1986 1987
Year
-0-- SSASource: Instituto Nacional de Salud POblica (1990). - MSSA
A ISSSTE

58 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 6EVOLUTION OF PUBLIC SOCIAL EXPENDITURES, 1981-85
Expenditure category 1981 1982 1983 1984 1985
Total expenditure on social
development (millions of
1980 pesos)ab 353,663 359,440 265,455 270,326 277,932
As a percentage of total
public expenditure 18.85 14.84 17.21 12.44 13.30
Per capita growth rate (%) 16.2 -0.7 -27.8 -0.3 0.7
Public education
expenditure (% per capita
growth rate) 21.7 1.7 -31.9 4.1 0.7
Health care expenditure
(% per capita growth rate)c 13.1 -3.4 -31.2 4.5 2.8
Social security expenditure
(% per capita growth rate)d 13.5 -2.6 -21.4 -1.4 -23.2
a. Expenditures converted into real expenditures using the GDP implicit deflator with 1980 as abase.b. Includes expenditures on public education, health care, social security, and other categories.c. Does not include ISSSTE and IMSS.d. ISSSTE and IMSS.Source: Lustig (1990).

EXHIBIT 7ANNUAL HEALTH SECTOR BUDGET BY INSTITUTION, 1979-88
(thousands of 1980 pesos)
Institution 1979 1980 1981 1982 1983 1984 1985 1986 1987 1988
Institutions with servicesopen to general populabon
SSAS 21,020 19,486 22,092 16,952 11,791 12,111 13,526 9,378 11,470 20,011DIF 3,544 3,385 3,394 2,356 968 1,902 2,344 1,869 873 2,864DDF 3,632 1,281 1,273 822 814 N/A N/A N/A N/A N/ACOPLAMAR 1,180 1,712 3,519 1,283 2,485 1,365 1,879 1,429 938 2,551
Total 29,376 25,864 30,278 21,413 16,058 15,378 17,749 12,676 13,281 25,426
Institutions with servicesrestrcted to membership
populationsIMSS 91,458 99,448 111,584 92,138 75,102 73,172 77,171 64,221 56,790 125,211ISSSTE 34,319 35,091 43,251 24,485 16,868 19,551 18,346 19,618 19,128 41,116ISSFAM 2,176 1,666 850 497 814 N/A N/A N/A N/A N/APEMEX 2,657 2,388 3,407 3,358 2,557 1,659 N/A N/A N/A N/A
Total 130,610 138,593 159,092 120,478 95,341 94,382 95,517 83,839 75,918 166,327R
N/A: Not available.Source: Cruz, Lozano, and Querol (1990). 0

EXHIBIT 8SOURCES OF FINANCE: IMSS AND ISSSTE, 1978-88
(percent)(D
Source 1978 1979 1980 1981 1982 1983 1984 1985 1986 1987 1988
IMSS~~~~~~~~~~~~~~~~~~~~~~
Employees 20.5 20.7 21.6 22.1 21.5 21.5 21.5 21.4 21.7 21.6 21.5 Employers 62.1 64.4 66.8 68.7 67.3 66.9 66.5 67.0 70.1 72.7 72.4 0Government 17.4 14.9 11.6 9.3 11.2 11.7 12.0 11.7 8.3 5.7 6.1 3C
U)
ISSSTE"DEmployees 39.6 38.7 38.7 39.3 49.6 56.8 50.6 48.9 37.4 35.2 30.3 :3Government 60.4 61.3 61.3 60.7 50.4 43.2 49.4 51.1 62.6 64.9 69.7
Source: Cruz, Lozano, and Querol (1 99).

Macroeconomics and Health: The Case of Mexico 61
EXHIBIT 9ANNUAL INSTITUTIONAL COVERAGE, 1978-88
(thousands of people)
Year SSA3 IMSS ISSSTE Total
1978 40,800 19,790 5,000 65,5901979 41,440 20,990 4,880 67,3101980 36,540 24,130 4,990 65,6601981 38,970 26,920 5,320 71,2101982 41,570 26,890 5,470 73,9301983 39,540 26,980 5,610 72,1301984 40,320 29,390 6,080 75,7901985 41,130 31,530 6,450 79,1101986 41,940 31,060 6,960 79,9601987 42,750 34,340 7,360 84,4501988 43,200 35,870 7,670 86,740
a. Estimated population coverage, including individuals also covered by IMSSand ISSSTE.Source: Cruz, Lozano, and Querol (1990).

62 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 10VOLUME OF SERVICES BY INSTITUTION, 1978-88
Number of outpatient consultations Number of hospitaldischarges
Year SSA IMSS ISSSTE Total SSA IMSS ISSSTE Total
1978 24,124 58,639 12,511 96,274 666 1,476 224 2,3661979 22,614 54,303 12,522 89,439 447 1,576 237 2,2601980 13,591 56,568 12,575 82,734 447 1,650 248 2,3451981 14,140 58,764 12,439 85,343 458 1,727 264 2,4491982 17,430 59,834 12,873 90,137 638 1,890 286 2,8141983 16,355 66,263 14,393 97,011 438 1,948 310 2,6961984 16,796 71,416 14,844 103,056 490 1,894 300 2,6841985 18,888 71,687 14,575 105,150 566 1,765 277 2,6081986 23,415 71,579 16,899 111,893 660 1,791 305 2,7561987 26,748 76,391 17,572 120,711 726 1,811 356 2,8931988 29,374 75,921 19,586 124,811 802 1,408 216 2,426
Source: Cruz, Lozano, and Querol (1980).

Macroeconomics and Health: The Case of Medco 63
EXHIBIT 1 1HEALTH SECTOR BUDGET ALLOCATIONS, 1978-87
(percentage of total government health budget)
Preventive Curative AdministrationYear services services and support
1978 2.7 75.2 22.11979 4.9 59.5 35.61980 6.6 64.7 28.71981 6.4 62.6 31.01982 6.5 74.7 18.81983 8.0 75.2 16.81984 6.4 66.4 27.21985 8.6 57.1 34.31986 9.3 63.1 27.61987 8.9 63.8 27.3
Source: Cruz, Lozano, and Querol (1990).

EXHIBIT 12HUMAN AND PHYSICAL RESOURCES BY HEALTH INSTITUTION, 1978-88
Resource 1978 1979 1980 1981 1982 1983 1984 1985 1986 1987 1988
Hospital beds (number)SSA 24,043 24,704 20,216 12,655 15,251 11,768 18,169 17,296 17,206 44,350 44,793 a
mIMSS 25,495 26,671 22,334 23,123 24,644 31,268 31,318 26,828 26,851 26,657 28,110ISSSTE 4,529 4,721 5,315 5,257 5,477 5,615 6,133 6,135 6,148 6,198 6,244
Doctors (number)XSSA 11,427 13,633 19,772 15,918 10,396 12,630 15,428 17,263 18,453 20,296 20,498
IMSS 21,132 25,389 25,445 29,635 24,054 29,699 23,325 22,045 23,922 25,587 26,604ISSSTE 6,358 7,336 7,686 8,125 9,015 9,252 10,488 10,772 11,559 11,480 11,620
Doctors (per 1,000 personsserved by the institution)SSA 0.28 0.33 0.54 0.41 0.25 0.32 0.38 0.42 0.44 0.47 0.47IMSS 1.07 1.20 1.05 1.10 0.89 1.10 0.79 0.70 0.77 0.75 0.72ISSSTE 1.27 1.50 1.58 1.52 1.65 1.65 1.72 1.67 1.66 1.56 1.51
Nurses per doctor (number)SSA 1.79 1.53 1.15 1.16 1.19 1.64 1.36 1.78 1.86 1.86 1.86IMSS 1.62 1.54 1.65 1.50 1.88 1.60 2.12 2.37 2.24 2.17 2.17ISSSTE 1.24 1.68 1.04 1.10 1.20 1.18 1.26 1.26 1.10 1.20 1.20
Source: Cruz, Lozano, and Querol (1990).

Macroeconomics and HeaKth: The Case of Mexico 65
EXHIBIT 13WAGE AND NONWAGE SHARES AND DISTRIBUTIONOF INCOME BY INSTITUTIONAL CATAGORY, 1981-85
(percent)
Share and category 1981 1982 1983 1984 1985
Wage share 42.7 38.2 31.7 30.8 31.2Nonwage share 57.3 61.8 68.3 69.2 68.8
Total 100.0 100.0 100.0 100.0 100.0
Private sector 81.5 79.6 76.3 78.1 78.2Public sector 15.2 15.1 18.0 16.2 17.6Foreign sector 3.3 5.3 5.7 5.7 4.2
Source: Lustig (1990).

66 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 14INFANT MORTALITY BY CAUSE, 1970s and 1980s
Respiratory infection
Intestinal infection _
Perinatal mortality
Accidents
Malnutrition
Immuno-preventable
Congenital anomalies
Circulatory AP
0 2 4 6 8 10 12 14 16 18Rates per 1,000 live births ___
I °1970s~
S C 1980s
Source. Cruz, Lozano, and Querol (1990).

Macroeconomics and Health: The Case of Mexico 67
EXHIBIT 15PERCENTAGE CHANGE IN CAUSES OF DEATH IN CHILDREN
YOUNGER THAN 1 YEAR OF AGE, 1970s and 1980s
Acute respiratory Iinfection
Dysentery
Anemia
Malnutrition
Pneumonia
Diarrhea
Perinatal
Total
-60 -50 -40 -30 -20 -10 0 to 20 30 40Percent
O 1970s
Sourco: Cruz, Lozano, and Querol (1990).

68 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 16PRESCHOOL MORTALITY BY REGION, 1978 and 1984
North
Central-North
Central-South
C
Gulf
Federal District
South
National
0 1 2 3 4 5 6Rate per 1,000 habitants a 1978
Source: Cruz, Lozano, and Querol (1990).

Macroeconomics and Health: The Case of Mexico 69
Source Documents
Cruz, C., R. Lozano A., and J. Querol V. 1990. "Consecuencias de la Crisis ylas Politicas de Ajuste Sobre la Salud de la Poblacion y la Organizacion de losServicios de Salud en Mexico." Cuernavaca, Mexico: Institutio Nacional deSalud Publica. Draft.
Instituto Nacional de Salud Publica. 1990. Personal Communication.
Lustig, N. 1990. 'Economic Crisis, Adjustment and Living Standards in Mexico,1982-1985." World Development 18(10). Pergamon Press, Oxford.
Pan-American Health Organization, Directing Council. 1984. "The EconomicCrisis in Latin America and the Caribbean and Its Repercussions in the HealthSector." Provisional Agenda Item 24. XXX Meeting, Washington, D.C.,September - October.
Pan-American Health Organization, Executive Committee of the DirectingCouncil, Subcommittee on Planning and Programming. 1985. "The EconomicCrisis and Its Impact on Health and Health Care in Latin America and theCaribbean." Provisional Agenda Item 6. Washington, D.C., December 11 - 13.
Ortiz, Guillermo, and Carlos Noriega. 1990. Rationalizing the Public Sector: theMexican Experience in 1982-1990. Senior Policy Seminar, Latin America: Facingthe Challenges of Adjustment and Growth, Caracas, Venezuela, July 19-22.EDI/IESA.
Shapiro, Helen. 1990. Mexico: Escaping from the Debt Crisis? Boston: HarvardBusiness School.
World Bank. 1985. World Development Report 1985. Washington, D.C.
World Bank. 1990. World Development Report 1990. Washington, D.C.

Case 2. Primary Health Care in Honduras
Study Questions
The next two cases, Primary Health Care in Honduras and Financing the St. LucianHealth Sector, focus on affordability issues and how the characteristics, trends, anddistribution of national health care expenditures relate to existing policies, strategies,and the resources required to move toward national health goals. Together, the casesprovide an opportunity to apply and assess the tools and concepts presented in SectionOne's discussion of Financing the Health Sector: Expenditure Analysis andAffordability. The Honduras case raises the question of how to balance the delivery ofprimary health care and hospital services with limited resources. The ministry of healthseeks to extend a health sector project under the constraint that irreversible decisionsabout hospital services have been made elsewhere in the government. The affordabilityof both approaches is in question, and the decisionmaker must assess the underlyinganalytical assumptions and formulate alternative courses of action.
1. What were the strengths and weaknesses of the past health strategies of thegovernment of Honduras?
2. What financial forces shaped these strategies? How and why?
3. What are the most serious financial constraints that the MPH faces in expandingHSI?
4. Do you agree with the economists' projections for hospital recurrent costs aftercompletion of construction? Why or why not?
5. What recommendations would you make to the MPH? To the Ministry of Finance?To external donors?
6. What conclusions do you draw with regard to balancing primary health care andhospital services?
70

Primary Health Care in Honduras 71
Primary Health Care in Honduras
Working within the public sector is a constant series of battles, and this is no less truewithin the Ministry of Public Health in Honduras. There are many different points ofview ... political, economical, social . .. and decisions are influenced by a variety offorces ... The battle may be between a new building for the Post Office and a programfor potable water throughout the rural areas of the countiy ... or between a program forhospital construction and one for primary care clinics. The problem becomes even morecomplicated because people can see a hospital as representing health, but cannot seesuch a clear relationship between the lack of potable water and diarrhea. Medicalgroups, one of the more powerful lobbies in the country, want hospitals.
Carlos Guzman, Director General of Health for the Ministry of Public Health in
Honduras, was commenting on the dilemma he faced as he assembled his notes in
preparation for an upcoming meeting with the director of an international donor agency.
At stake was the continued success of the multimillion dollar program in primary health
care in Honduras, known as Health Sector Initiatives (HSI). As he reflected on the task
before him, he realized that the problems confronting him were political as well as
organizational and required concrete analysis. Not only would he have to propose an
approach for continuing HSI that was acceptable to the various parties involved, but
his proposal would need to be supported with hard numbers to show that HSI's
recuring costs could be met by the Honduran government.
Country Context and Health Status
Honduras, the second largest country in Central America, had a low population
density and was one of the region's least urbanized countries in the early 1980s. Sixty-
five percent of its 4.2 million people lived in rural areas. Its mountainous terrain and
lack of all-weather roads made transportation in rural areas difficult, especially during
the rainy season when flooding was common.
Per capita Gross National Product (GNP) was US$700 in 1984, placing Honduras
among the poorest countries in Latin America. More than 60 percent of its work force
was employed in subsistence farming, forestry, hunting, or fishing. Only 40 percent of
the population over ten years of age was literate.
A fertility rate of 7.3 children per woman contributed to an annual population
growth rate of 3.5 percent, well above the 2.7 average for Latin America during the
early 1980s. Forty-eight percent of the population was under the age of fifteen. The
crude death rate had declined by 43 percent since 1965, and in 1984 general mortality
stood at 10 per 1,000 population. Infant mortality was 72 per 1,000 live births, third
This case was written by James E. Austin, Harvard Business School, with funding provided by the U.S.Agency for Intemational Development. It first appeared in "Proceedings of the LAC Health OfficersConference." November 1984, and was based on Primary Health Care in Honduras (A) by David Young,Harvard School of Public Health. While the case is based on actual data, all names and some perpheralfacts have been disguised. the case was prepared for use as the basis for classroom discussion ratherthan to illustrate either effective or ineffective handlng of a managerial or development situaton.

72 Section Two: Applied Experiences in Health Economics and Financing
highest in Latin America, and the rates in the rural areas were about 1.5 times those incities. Nearly 40 percent of all deaths occurred among children less than five years old.
The leading causes of infant mortality by order of importance were diarrhea,perinatal diseases, prematurity diseases, pneumonia, bronchitis, other respiratoryillnesses, perinatal infections, pertussis, cardiac arrhythmia, and measles. The principalreasons for hospitalization were complications in pregnancy, delivery, and puerperium;infectious diseases and parasites; accidents and violence; respiratory disease; anddigestive system disease.
The Honduran Health System
The government health system under the Ministry of Public Health (MPH) assumedresponsibility for providing health services to 85 percent of the population who wereconsidered to have no access to other sources of health care. Actual coverage wasestimated at around 60 percent in 1981. The MPH had six levels of service (see Exhibit1). The main features of each are as follows.
* Level 1: At the lowest level, communities of less than 500 people selectedunpaid volunteers to be trained and supervised by the MPH. These communityworkers became health guardians, midwives, malaria volunteers, and healthrepresentatives who attended to common illnesses, made referrals to MPH facilities,carried out vector control, and organized local health services.
* Level 2: At the next level, 429 rural health centers served populations of 2,000to 3,000 people. Full-time MPH employees at these clinics included an auxiliarynurse (with one year of training) who provided direct care and supervisedcommunity health workers in four to eight surrounding communities, a healthpromoter who assisted communities with health education and sanitation projects,and an auxiliary who was responsible for vector control.
* Level 3: This level consisted of 119 clinics that provided ambulatory care topopulations of 10,000 people. These clinics were staffed by a medical doctor,nursing auxiliaries, a lab technician, and administrative support staff.
* Level 4: This level consisted of seven emergency hospital units with fifty ormore beds that were staffed by up to nine doctors, five nurses, forty-five nursingauxiliaries, and administrative personnel. These hospitals supervised the urban andrural clinics and each served an area of 100,000 people.
* Level 5: Six regional hospitals with 200 to 500 beds offered a full rangeof services, including specialties.
* Level 6: The national hospital in Tegucigalpa topped the health system pyramid.It had 1,200 beds and was equipped to handle referrals from all other levels. Otherspecialized hospitals at this level provided specific services for tuberculosis, mentalhealth, and maternal-infant care.

Primary Health Care in Honduras 73
Exhibit 2 provides an overview of MPH budgets between 1972 and 1984.
Of the forty-four hospitals in the country in 1982, twenty-five were private. Privatehospitals, laboratories, physicians, nurses, and dentists were concentrated inTegucigalpa, the capital, and in the next largest city, San Pedro Sula. They servedapproximately 9 percent of the population, principally higher-income groups whosemorbidity patterns were quite different from the national profile.
In the rural areas traditional healers were common. Many rural people believedillness was caused by external and often supernatural forces. Traditional healersincorporated these dimensions into their practices, and they had high credibility. Peopleoften consulted them before or concurrent with other sources. Traditional midwiveswere private practitioners who had been incorporated into the public health system aspart of the community health worker program for many years. In 1983 the governmenttrained 7,500 midwives. Families paid a midwife L25 for assisting a birth.'
The pharmaceutical system had twenty-eight private laboratories and a mixedenterprise, the Hondulab Farmoquimica Internacional S.A.2 Hondulab was formed in1979 with plans to supply forty-seven products, ranging from antibiotics to vitamins,to the MPH and the Honduras Social Security Institute (HSSI). Only six of its productswere expected to duplicate products produced by the national laboratory (PANI).Hondulab had not reached its production or sales objectives by 1984, and it wasexperiencing some financial difficulties. Private pharmacies and other local storeshandled the retail distribution of drugs.
Most family planning services were provided through the Honduran FamilyPlanning Association. There were 40,000 users in 1982. Services were provided in theassociation's clinics in Tegucigalpa and San Pedro Sula as well as through 1,100community-run rural distribution posts. Under the association's auspices sterilizationswere performed in thirteen MPH and three private hospitals. A social marketing projectdistributed contraceptives through 600 commercial retail outlets.
1. In 1984, one U.S. dollar was equivalent to two lempiras.2. All but four of the private laboratories were Honduran owned, and only four laboratories made
pharmaceuticals found on the MPH's essential drugs list. Hondulab was a joint investment of the NationalInvestment Corporation of the Honduran govemment (64 percent), the Argentine government (30 percent),and three local price investors (6 percent).

74 Section Two: Applied Experiences in Health Economics and Financing
Government Health Strategy and Performance
Between 1974 and 1984 the Honduran government's approach to the delivery ofhealth services featured three distinct strategies. The period from 1974 to 1978 stressedexpansion of primary health care coverage. The years between 1978 and 1981 sawrenewed interest in hospital-based services. During 1982-84 the government renewedits emphasis on primary health care, and a health project supported by donor fundsbecame the focus of MPH efforts and activities.
Expanded Coverage Program, 1974-78
In response to the results of an MPH evaluation of the country's health situation in1973, the government reached a policy decision to undertake a national health project.The fundamental objective of the Expanded Coverage Program, supported financiallyby international donors, was to extend basic health services to the entire population.The strategy was fourfold:
* To focus on providing services to individuals who did not have access to healthcare, giving particular attention to rural areas and subgroups such as thematernal-child population
* To decentralize health services, relying on community participation as anessential component
* To place emphasis on preventive health services, including both primary careand environmental health
* To reorganize the basic structure of the health care system, establishing definedlevels of care and strengthening the referral system from one level to the next.
To implement this strategy, the MPH diverted resources from hospital expansionto the rural-based primary health care delivery systems. Health sector expenditureswere approximately 2.5 percent of GNP and recurrent health expenditures for thisperiod ranged from 8.5 percent of the national recurrent budget to 12.6 percent. Healthclinics were constructed and auxiliary and community workers trained. Reducedattention, however, was given to developing management support activities. The MPH'sadministrative budget declined from 10 percent to 2 percent of the overall healthbudget.
The results of the strategy were marked. The number of ambulatory consultationsper person rose from 0.25 to 1.00 and health guardians and midwives reported acombined average of 254 consultations per worker per year. Coverage forimmunizations of children under two years old reached 96 percent for polio and 79percent for DPT. The death rate then dropped from an average of 16 per 1,000 during1965-70 to 12 per 1,000. Morbidity rates for several

Primary Health Care in Honduras 75
common diseases generally increased, but many felt that this was caused by improvedreporting rather than a higher actual incidence rate.
Hospital Expansion, 1978-81
Personnel changes at the policymaking level within the MPH that came with a newadministration altered the health policy focus. Although extension of primary healthcare services remained the official policy, the MPH embarked upon an ambitiousprogram of construction to add seven emergency and two regional hospitals (1,060additional beds) to its existing stock of thirteen hospitals (3,100 beds). The Inter-American Development Bank (IDB) provided the funding.
During this period the MPH budget grew from 10.2 percent to 11.1 percent of thetotal government budget. Overall health expenditures per capita increased 25 percent,growing from US$15.60 to US$19.60. Annual recurrent expenditures per hospital bedrose by 6.9 percent per year, in real terms, between 1978 and 1980.
Many health gains under the previous strategy were eroded. Immunization coveragedropped by over half. Conmmunity workers' productivity plummeted 90 percent andmany of them abandoned their positions. Morbidity and mortality rates did not showsignificant improvement.
By 1980 several problems stood out. Under the MPH's organizational structure,those who developed objectives had little control over implementation, theimnplementors had little control over the needed resources, and the resource providershad little input into setting objectives. The only office that could provide coordinationwas that of the director general, and it was staffed by only two people. Coordinationwas poor, overlap common, and conflict intense. Most auxiliary nurses in rural clinicsreceived one supervisory visit during the year. The community workers and clinics werefrequently out of supplies. Half of the MPH's vehicles were inoperative and many clinicrefrigerators were also not working. Although construction of the nine new hospitalsremained uncompleted, 500 beds were added to the hospital system.
Health Sector Initiatives Project, 1981-84
A new president brought changes in personnel and policies to the MPH. A newnational health plan revived the earlier strategic thrusts toward primary health care forhigh-risk groups who lacked access to health care, and stressed a decentralizedorganizational structure. Hospital construction and capital investments weretemporarily halted and then cut in half. The MPH embarked on a four-year, US$32million HSI project that was financed by loans and grants from donors. The project hadfour major components:

76 Section Two: Applied Experiences in Health Economics and Financing
* Health technologies provided resources for the control of malaria anddiarrhea (emphasizing oral rehydration), the promotion of maternal and childhealth, and the support of an expanded immunization program.
* Logistics and maintenance supported training, facility construction,equipment, management, and technical advice aimed at ensuring that suppliesreached the peripheral areas and that equipment was kept operational.
* Management and planning redressed the problems generated by a rapidgrowth in the scope and complexity of the health care system in the previousten years without a concomitant increase in management resources.
* Human resources development improved the supervision and continuingeducation of community and MPH workers, the public health training ofmedical and nursing school teachers, and mass media support for village-levelworkers.
The MPH made the strategic decision to focus on diseases that had the highestimpact on mortality and for which effective and relatively inexpensiveinterventions existed. Priorities were assigned to immunopreventible diseases,diarrheal diseases, TB and respiratory diseases, malaria, birthing services,nutrition services, education, and family planning and maternal and child healthservices.
To address the previous organizational problems, the MPH established a seriesof working groups that cut across several departments and levels to supervisevarious activities. A new formal organization structure was approved (see Exhibit3). These changes increased the ministry's effectiveness. When an outbreak ofpolio occurred in mid-1984, a national coordinating committee was formed. Itsactions were a major factor in controlling the outbreak within six weeks of itsdetection.
Technical assistance to the MPH through a team of nine resident advisors,financed by one of the major donor agencies, contributed to progress on severalfronts. A logistics system was designed, 1,000 MPH personnel were trained, andthe central and regional warehouses were reorganized. These activities resultedin improvements in inventory management and supply dependability for clinicsand community workers. The maintenance department was reorganized andpersonnel were trained. Ninety-five percent of the refrigerators were working and50 percent more MPH vehicles were on the road. Document flow time wasreduced by 25 percent, and budgetary controls were instituted usingmicrocomputers, cost indicators, and cost centers. Training curricula for thecommunity health workers were designed for use at the local level. Thesupervision model was revised and simplified to focus on the priority diseases.MPH personnel were trained in using the supervision manual.
By 1984 immunization coverage had returned to high levels: 95 percent forpolio and 70 percent for other diseases. Ambulatory consultations returned to 1.0

Primary Health Care in Honduras 77
per inhabitant. The midwives increased their consultations to 101 per year and healthguardians to 240 per worker per year. The infant mortality rate was reduced by 30percent during the four-year period.
Exhibits 2 and 4 provide an overview of total expenditures. The MPH'sexpenditures in real terms increased 42 percent between 1979 and 1982, an increaseof 28 percent on a per capita basis. The annual recurrent costs of a hospital bed, net ofinflation, more than doubled (see Exhibit 5). The country experienced significantinflation during these years and a recession forced budget cutbacks in 1983-84. In 1983real expenditures declined by 15 percent, but primary health care expendituresexperienced significant growth (see Exhibit 6).
Health Sector Initiatives Project Extension
In late 1984, staff of the director's office with officials from a major donor agencyprepared a proposal for a three-year extension of the HSI project. Their initial draftcalled for the continued support of the original objectives of HSI. In addition, theproject was to help the governnent expand the social security system into rural areasand to move basic drug production toward self-sufficiency. The project proposalrequested funding of US$5.7 million in loans and US$4 million in grants.
The draft proposal, however, raised major questions as to whether the projectedfinancial position of the government of Honduras (GOH) would allow it to sustain anexpansion of the HSI project activities that were proposed. The GOH recently hadbegun to implement a series of austerity initiatives that would constrain governmentoutlays over the next five years. The pessimistic outlook for the general economicfuture of Honduras was coupled with indications that the health priorities of thegovernment might be shifting.
Officials of the Inter-American Development Bank (IDB) had already persuaded theGOH to resume the construction of the unfinished hospitals and to staff themappropriately, although not all of the senior staff of the MPH agreed with this decision.However, the government was under strong political pressure to come up with highvisibility projects such as hospitals prior to the 1985 elections. The IDB agreed toprovide the necessary funds for construction. Any scenario projecting the availabilityof funds to finance recurrent costs and in-kind contributions for the HSI projectextension had to account for the increases in costs that would result from the proposedcompletion of the hospital construction program.
Projections by economist advisors to the MPH, which assumed completion ofhospital construction as well as staffing and equipping the new hospitals, revealed thatthe associated costs the MPH would incur for the new hospitals would leavenothing for primary care. All other health programs would have to experiencesignificant cuts (see Exhibit 7). They argued that it was not possible to goahead with an expanded primary health care project in light of this information. Others

78 Section Two: Applied Experiences in Health Economics and Financing
within the MPH believed that there were acceptable answers to the problem ofrecurring costs, but felt that if some arrangements were not made soon, fundswould run out and the HSI project and its accomplishments would be set backseveral years.
The donor was concerned about the future of primary care in the country, andwas reconsidering its involvement in supporting HSI. The MPH was counting onthis project as a strong bargaining chip for protecting its budget negotiations withthe Ministry of Finance. Carlos Guzman provided his perspective on thesituation.
Our decision about the IDB loan . . . was just one of many battles that we haveevery day. We lost that one, but [if the donor] pulls out [on the extension of theHSI project] it would mean losing not only the battle but the war. . . . Overall,what we need is a balanced development of the health sector. Hospitals are not thedevils . .. But we must balance the construction of hospitals with the developmentof primary care and other public activities.
The donor saw the situation somewhat differently.
We're not threatening to pull out of primary care activities, but we are saying tothe MPH, "This is your issue. How do you want to deal with it?" We can't wakeup three or four years from now facing a recurrent cost crisis for our on-goingproject because we have funded the development of a primary care system whichis too expensive for the ministry to operate.
Dr. Guzman was planning to address these concerns in his meeting with thedirector of the donor agency. He commented on the analytical effort his staffwould need to undertake in preparation for that meeting.
I know there has to be another way to approach this problem. For one thing, wehad been thinking about charging patients more for hospital care than in the past.In January I sent a memorandum to all hospital directors instructing them to revisetheir user fees to achieve greater cost recovery [see Exhibit 81. But we are notsure by how much these fees can feasibly be raised. A [consultant's] survey [ofhousehold expenditures] found that expenses for "health protection" represented5.2 percent of total family costs in rural areas and 4.8 percent in urban areas. Thesurvey showed that the mean overall expense for an illness episode was L20.However, the median expense of L2 indicated that there were a relatively smallnumber of families with very high expenses . . . [perhaps] . . . incurred becausethe illness was perceived as relatively serious." [See Exhibits 9 and 10 for studyresults by type of illness and by source of treatment.]
If user fees alone will not suffice to finance the recurring costs, other alternativeswill have to be proposed and we will have to undertake some concrete financialanalyses of each ... [we expect to prepare for the MPH] some viable alternativesas well as the structure for an analysis of their financial consequences.

Primary Health Care in Honduras 79
EXHIBIT 1THE HONDURAS HEALTH SYSTEM: PUBLIC SECTOR
Level 6 National Medical
Level 5 6 Regional Hospitals
Level 4 7 Emergency Hospital Centers
Level 3 119 Health Centers
Level 2 429 Rural Health Centers
Level 1 Community Health Workers
Source: Ministry of Public Health (1982).
Honduran Social Security Institute (HSSI): The institute served about 7.5percent of the population through its four hospitals and four clinics in thetwo major cities of Tegucigalpa and San Pedro Sula. The HSSI wasestablished in 1959 as an autonomous public entity to providecomprehensive health care to certain categories of wage and salariedworkers. Services were considered to be high quality and the hospitalsefficiently run, but the population coverage had not changed in ten years.The HSSI was entirely funded through employer and employee payrolldeductions. Employee contributions amounted to 2.5 percent of salary upto L600 and the employers paid 5 percent of salaries. The averageunskilled worker's income was so low as to preclude participation in thesystem. The HSSI purchased 13 percent of its pharmaceuticals in 1983from Honduran producers and directly imported the majority of its needsfrom Mexico and Central American producers.
National Laboratory (PANI): PANI was established as an autonomousagency in the mid-1960s to provide low cost essential medications to theMPH and the HSSI. It produced about fifty medications on the WorldHealth Organization's essential drugs list and supplied 20 percent of theMPH's requirements. PANI was financed by the national lottery andreturned more funds to the Treasury than it used. Its products were of highquality, but involved only minimal value added manufacturing operations.
National Water and Sanitation Service: This agency was responsible forthe potable water supply for communities with more than 2,000 inhabitantsand the MPH for those with less than 2,000. In practice, there wasconsiderable overlap.

80 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 2MPH HEALTH BUDGETS, 1972-84
Percentage of Percentage ofYear MPH budget government recurrent
(millions of current US$) budget government budget
1972 10.7 7.9 N/A1973 11.5 8.4 N/A1974 14.1 8.5 N/A1975 24.9 12.6 N/A1976 26.1 10.1 8.61977 33.7 10.8 12.11978 42.3 10.2 12.31979 54.7 10.9 12.21980 62.3 11.0 N/A1981 74.6 11.1 N/A1982 85.1 11.0 N/A1983 92.6 11.1 N/A1984 84.7 9.8 N/A
N/A: Not available.Source: Ministry of Public Health.

EXHIBIT 3THE ORGANIZATION OF THE MPH, 1978 and 1983
1983 1978
SecretarySecretary Subsecretary
Executive Director SDirector GeneralCoordination General Projects&Subdirector General
Group & Ppnecng UIInstitutionaI GpsciT Statistics Department
BasIc Technical Support I IlBasic Technical Support Complementary Administration Hean Care Environment AdministrationPrograms Programs Programs Section Section Section
I I IIUDivisions Divisions Divisions Divisions Divisions Food Divisions Departments
Control* Epidemiology * Human * Hospitals * Personnel * Hospital Maintenance * Sanitation - Personnel* MCH Resources * Food * Payments * Epidemiology * Vector Control * Purchasing* Vector Control * Laboratories * Mental Health * Supplies * MCH - Oral Health *Accounting* Sanitation * Maintenance * Oral Health * Transport - Nutrition * Graphic Arts 0* Nutrition * Science & * Accounting * Human Resources
Technology Unit * Graphic Arts * Nursing* Medications * Laboratories Regional*Equipment * Mental Health* Education * Education* Emergency &
Mobile HealthRegions
Source: Ministry of Public Health.

EXHIBIT 4TOTAL HEALTH EXPENDITURES BY PROGRAM, 1979-84
(millions of current US$)0
Program 1979 1980 1981 1982 1983 1984
Operating programs 30.4 37.5 50.2 57.0 59.0 61 2
Health Promotion and Environmental Program 3.2 4.3 6.0 6.3 6.6 5.7Control of Communicable Diseases 7.7 9.9 14.5 17.1 19.0 21.7 mHospital Care 17.4 20.4 24.4 28.5 28.9 29.0Central Administration 0.4 0.7 2.7 2.6 2.4 2.7
0Normative Health Services 1.7 2.2 2.6 2.5 2.1 2.1
Current transfer to domesticand international organizations 0.3 0.04 0.6 0.7 0.8 0.7
0Investment program 13.4 14.0 9.8 11.1 18.7 7.5 m
Capital transfers to domestic institutions' 11.2 10.5 14.0 16.4 14.0 15.3 O
Total 55.3 62.3 74.6 85.2 92.5 84.7
Percentage of foreign financing 31.4 23.1 70.8 16.5 23.2 32.8 ,
N/A: Not availablea. Includes external financingSource: Ministry of Public Health.

Primary Health Care in Honduras 83
EXHIBIT 5HOSPITAL EXPENDITURES BY BED, 1977-80 and 1983-84
Number of Expenditures Annual expendituresYear hospital beds (millions of US$) per bed (US$)
1977 3,117 11.1 3,561
1978 3,082 14.9 4,835
1979 3,521 16.8 4,771
1980 3,579 20.4 5,700
1983 3,437 28.9 8,408
1984 3,495 29.0 8,298
a. In 1977, occupancy rates were 81 percent for national hospitals, 71 percent for regionalhospRals, and 50 percent for area hospitals.b. HospRal discharges totaled 109,584 and patient days came to 1,222,700.c. Budgeted rather than actual expendRtures.d. Hospital discharges totaled 111,024 and patient days came to 1,222,700.Source: Ministry of Public Health.

co
EXHIBIT 6 mBUDGETED HEALTH EXPENDITURES BY PROGRAM, 1979-84 O
(percent)
Program 1979 1980 1981 1982 1983 1984 >
Operating Programs 54.42 60.10 67.28 66.81 63.73 72.28m
Health Promotion and Environmental Program 5.86 6.83 8.06 7.37 7.09 6.79Control of Communicable Diseases 14.05 15.91 19.42 20.03 20.56 25.62Hospital Care 30.60 32.77 32.69 33.52 31.21 34.27 2Central Administration 0.74 1.09 3.58 2.99 2.53 3,13 5
Normative Health Services 3.15 3.49 3.50 2.88 2.31 2.46 I
P1m
Current transfer to domestic 8and international organizations 0.68 0.66 0.75 0.81 0.85 0.81
Investment program 24.48 22.44 13.13 13.05 20.23 8.80
Capital transfers to domestic institutions 20.41 16.78 18.82 19.30 15.16 18.09
Total 100.00 100.00 100.00 100.00 100.00 100.00
Note: includes external financing.Source: Ministry of Public Health.

Primary Health Care in Honduras 85
EXHIBIT 7PROJECTED HEALTH BUDGET BY PROGRAM
TO BE FINANCED WITH DOMESTIC FUNDS, 1984-89(millions of current US$)
Program 1984a 1985 1986 1987 1988 1989
Operating programs 53.8 54.3 55.4 59.3 66.2 72.4
Health Promotion and
Environmental Program 5.7 5.1 4.5 4.7 5.4 5.9Control of Communicable Disease 14.5 13.9 13.4 13.5 14.1 14.8Hospital Careb 29.0 31.9 35.1 38.6 42.5 46.7Central Administration 2.6 2.0 1.4 1.6 2.3 2.8Normative Health Services 2.0 1.4 0.9 1.0 1.7 2.2
Current transfer to domestic
and international organizations 0.6 0.02 N/A 0.1 0.9 1.4
Investment program' 3.3 4.0 3.4 4.1 2.3 2.3
Capital transfers to
domestic institutions 2.8 2.2 1.7 1.8 2.5 3.0
Totald 60.5 60.5 60.5 65.3 71.9 79.1
N/A: Not availableNotes: All Inter-American Development Bank hospitals will be contracted and staffed and willopen upon completion of construction. San Pedro Sule Hospital will open on schedule and willoperate at 100 percent capacity.a. Adjusted for US$1.25 million budgeted cut, of which US$0.85 million is a reduction intransfers to domestic institutions and the rest is distributed evenly among all programs excepthospital care.b. Assumes 10 percent yearly growth in expendituresc. For 1985-89 the figure used is 40 percent of the overall investment plan, that is, anassumption is made that 60 percent of the plan will be financed with external funds.d. The MOH budget is assumed to remain at the same level for 1985 and 1986 and to grow 8percent in 1987 and 10 percent thereafter.Source: Ministry of Public Heafth.

86 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 8DIRECTOR GENERAL OF HEALTH
Circular No. 1-84 Tegucigalpa, D.C.
31 January, 1984
Hospital Directors:
As was discussed in the recent meeting of Hospital Directors, allow meto reiterate the following:
1) Each hospital will design a plan for cost recovery that permits theprogressive financing of the operational costs of the hospital in the area ofmedications, surgical supplies, fuel, and food. It is estimated that theseareas represent about 30 percent of hospital costs.
2) In order to comply with the foregoing you must effect a substantialrevision of the fees and collection mechanisms that the hospital currentlyuses. It will be important to develop a plan which specifies a progressiveapproach to increasing collections, with the objective of developing asystematic collection control system.
3) We remind you that each Hospital Director must initiate contact withorganized groups from the nearby community in order to establishagreements about the health services offered, as a transitional means tothe eventual extension of the services of The Social Security Institute.
4) Also, you must consider other mechanisms such as the installation ofboarding facilities, the integration of Health Committees for hospital supportwith the participation of the vital forces of the community, and substitutionof services. We would like to remind you that you are managers of aninstitution that, besides being an efficient institution administratively, mustguarantee its proper social mission in matters and activities concerned withhealth.
Sincerely,
Dr. Carlos Guzman C.Director General
cc. Minister of Public Healthcc. Deputy Director Generalcc. Health Region Heads

EXHIBIT 9OUT-OF-POCKET EXPENDITURES FOR ILLNESS
Costs (US$)Consultabon Medicabon Other Total
Illness cases Percent Median Mean Median Mean Median Mean Median Mean
Respiratory, other 361 21.9 0.50 4.15 0.25 5.35 0.25 1.10 1.00 9.05Upper respiratory infection 280 17.0 0.25 1.45 0.50 2.15 0.25 0.18 0.50 3.10Diarrhea 205 12.4 0.50 3.25 0.50 3.00 0.25 1.45 1.50 6.70Fever/malaria 184 11.2 0.50 4.15 0.50 4.85 0.25 1.00 1.00 9.00Pregnancy/birth 113 6.9 0.25 3.60 0.25 3.80 0.25 3.65 1.50 12.60Othergastrointestinal 87 5.3 0.50 5.15 0.25 3.50 0.25 1.90 1.50 10.60Arthritis 79 4.8 1.00 6.20 2.00 8.20 0.25 1.60 3.00 15.20Headache 71 4.2 0.50 4.65 0.25 5.70 0.25 2.60 2.50 12.95Anemia/malnutrition 39 2.4 0.50 2.90 1.50 6.85 0.25 1.15 3.00 11.00Other 229 13.9 N/A N/A N/A N/A N/A N/A N/A N/A
Total 1,648 100 0.50 4.80 0.50 4.70 0.25 1.65 1.00 10.20
N/A: Not Available.Note: L2=US$1.Source: Unpublished report on the Honduran Health System by Management Sciences for Health (1984).
OD
41

co
EXHIBIT 10EXPENDITURES FOR ILLNESS BY SOURCE OF TREATMENT
Costs (US$) Consultation Medication Transport Other Total
No. of~~~~~~~~~~~~~~~~~~~~~~~
Sources N.ocases Percent Median Mean Median Mean Median Mean Median Mean Median Mean
Family 508 31 N/A N/A 0.50 1.85 N/A N/A 0.25 0.20 0.50 2.00Self 250 15 N/A N/A 0.50 3.20 N/A N/A 0.25 0.15 0.50 3.25
rn
mPrivate M.D. 223 14 7.50 13.65 7.50 13.65 2.00 15.25 0.25 4.35 25.00 35.35
0
Rural center 223 14 0.25 0.25 0.25 2.45 0.25 0.20 0.25 0.45 0.25 2.25
0
Rural clinic with M.D. 149 9 0.50 0.85 0.25 1.40 0.25 2.15 0.25 1.30 2.00 5.55
m
MPH hospital 126 8 0.50 1.51 0.35 2.50 0.25 4.90 0.25 5.75 4.00 14.05 :C
Guardian 53 3 0.25 0.13 0.25 1.05 0.25 0.05 0.25 0.06 0.25 1.25 -Others 102 6 0.25 3.85 1.00 7.35 0.25 2.20 0.25 3.15 2.50 15.30 10
5
Total 1,634 100 1.00 4.30 1.00 4.30 0.25 2.40 0.25 3.00 1.00 9.13
N/A: Not available.Note: L2= US$1.Source: Unpublished report on the Honduran Health System by Management Sciences for Heafth (1 984).

Case 3. Financing the St. LucianHealth Sector

Case 3. Financing the St. LucianHealth Sector
Study Questions
This case on St. Lucia extends the analyses covered in the preceding case onHonduras regarding affordability and national health care expenditures. The St. Luciasituation focuses on how to finance health services in the face of rising costs, increasingdemand, and evidence that the current health services are inadequate and perhapsinefficient. Its orientation is on macro appraisal and identification of viable policyoptions. Both cases also raise issues covered under other themes, particularly that ofMobilizing Resources for Health Services as described in Section One.
1. What are the strengths and weaknesses of the existing methods and mechanisms forfunding the St. Lucian public health system?
2. What are the strengths and weaknesses of using funds within the public healthsystem for achieving positive health outcomes?
3. What are the MOH's most serious problems in keeping health services affordableto the government?
4. What opportunities exist for alternative methods of financing the health caresystem?
5. What constraints might impede or facilitate the implementation of alternativemethods? Why?
6. What recommendations would you make to the goverrnent?
90

Financing the St. Lucian Health Sector 91
Financing the St. Lucian Health Sector
In late 1987, Cornelius Lubin, the Permanent Secretary in the Ministry ofHealth, was seeking alternatives to the government of St. Lucia's currentmethods for financing its health care delivery system. Mr. Lubin had been thePermanent Secretary for roughly a decade. Prior to his appointment, he had beenthe hospital administrator at Victoria Hospital, the government's major hospital.His formal training was in hospital administration. Mr Lubin was in the processof considering the contents of a number of health sector and financial reports onboth St. Lucia and the Eastern Caribbean subregion.
The nation's health problems had changed over the past decade and were nowmore closely aligned to those of high income countries. Critical health indicatorsfor St. Lucia established life expectancy at birth at 70 years and infant mortalitywas 23.6 per 1,000, compared to 54.2 in 1972. The Ministry of Health (MOH)budget, excluding the costs of sanitation, was expected to consume 12 percent ofgovernment expenditures and 5 percent of the Gross Domestic Product (GDP) infiscal year 1986-87, a level that approximated health expenditures in the UnitedKingdom. Health services were considered inadequate, and demand for them wasrising. One government study indicated that perceived need to see a doctor hadincreased by 78 percent in a two-year period. Given constraints on the nationalbudget and other national priorities that required public funding, MOH programsand budget were in danger of becoming less adequate.
Background
St. Lucia, one of seven independent English-speaking countries in the EasternCaribbean (see Exhibit 1), gained its independence in February 1979. With theexception of a brief period in the late 1970s, the same political party and thesame prime minister have been in power since independence. During the colonialperiod the French and English exchanged control of St. Lucia fourteen times.English was the official language, but most St. Lucians spoke Creole or Patois,a melange of French, English, and African dialects. Creole until recently wasunwritten. This situation was partially responsible for the high functionalilliteracy rate, estimated at 33 percent for all St. Lucians and 60 percent ofadults.
St. Lucia is a beautiful Caribbean island: white sand beaches, clear turquoisewaters, waterfalls, sulfur springs, rain forests, and scenic vistas abound.Thesmall volcanic island is 238 square miles in size, 27 miles long and 14 miles atits widest point. In 1987 St. Lucia had approximately 142,000 inhabitants,predominantly the descendants of African slaves brought to the region during the
This case was written by Maggie Huff-Rousselle, Social Sectors Development Strategies, Inc., withfunding by the Economic Development Institute of the Wolrd Bank. The case was prepared for use asthe basis of classroom discussion rather than to illustrate effective or ineffective handling of amanagerial or development situation.

92 Section Two: Applied Experiences in Health Economics and Financing
colonial period. The descendants of colonial and East Indian immigrants made up asmall portion of the population, as did expatriates from other Caribbean islands orexpatriates from high-income countries who had come to work or retire. Roughly 90percent of the population belonged to the Catholic church. Approximately 40 percentof the population lived in Castries, the capital city situated at the northern end of theisland on the Caribbean Sea. The area surrounding Vieux Fort, to the south,contained 8 percent of the population. Soufriere on the west coast and Dennery onthe east each contained less than 10 percent of the population.
Traditionally, St. Lucia's economy depended heavily on agricultural activities.Agriculture represented 17 percent of GDP in 1986 and absorbed 40 percent of theemployed population. More than 10,000 acres (71 percent of all arable land) wereunder banana cultivation. The banana industry injected close to EC$ 1 million (US$370,300) into the economy every week, and more than half the population directlydepended on it. Bananas accounted for approximately 90 percent of agricultureexports. The industry, although buoyant in recent years, was affected by a widerange of natural conditions, particularly hurricanes and tropical storms. GeestIndustries was the sole purchaser of bananas. The government of St. Lucia, likeother banana producers in the Eastern Caribbean, was very concerned that the tradeagreements due to take effect in Europe in 1992 might have dire consequences forthe economy, because the United Kingdom protected the banana industry. The issuewas discussed frequently in the media.
Twelve percent of the employed population worked in the tourist industry and 7to 8 percent were employed in manufacturing jobs, such as assembling clothing forexport. The tourist industry and related communications and transportation industrieswere developing rapidly. In 1986 hotels and restaurants contributed 12 percent toGDP and transportation and communications contributed 15 percent. Even thoughtourism was expanding, St. Lucia competed with other Caribbean islands and pricecompetition was an increasingly important factor.
Manufacturing accounted for 9 percent of GDP. Industrial wages tended to behigher than in many of the other Caribbean and Central American countries, and thisfact, combined with a largely unskilled labor force, did not encourage rapiddevelopment in the industrial sector. The government was a major employer andgovernment services accounted for 20 percent of GDP.
The growth rate of real GDP over the past several years was positive, achievinga 5 to 6 percent annual increase. Current account deficits were reversed during1985-86 and 1986-87. However the capital account remained in deficit, and theMinistry of Finance (MOF) estimated that approximately 12 percent of annualrecurrent expenditures were for debt service. Debt payments continued to be inarrears. Annual inflation during recent years was estimated at 1.5 percent. Thisinflation rate was typical of the Eastern Caribbean; their currency was probably themost stable in Latin America and the Caribbean.

Financing the St. Lucian Health Sector 93
Rising unemployment was a major problem for St. Lucia. Approximately 25percent of the working age population was unemployed, up from 14 percent in1975, and the number was still rising. The economy needed to create 2,000 to3,000 jobs annually just to keep the unemployment rate stable, but this target hadgenerally not been attained. Half of the work force was in the informal sector,where wages and job security were low. Often the most skilled St. Luciansemigrated to other countries inside and outside the region.
Per capita income was EC$ 3,057 (US$1,132) in 1986 and rising. An InternalRevenue audit survey reported that 23,000 residents had filed income tax returns,primarily those working in the formal employment sector or government service.A 1982 household survey indicated that 23 percent of the population had annualincomes of less than EC$ 2,000.
Approximately 81 percent of children five to fourteen years old were enrolledin primary school, and 43 percent of the fifteen- to nineteen-year-olds wereenrolled in secondary school. Nevertheless, only 39 percent of adults had morethan four years of schooling.
Health and Social Problems
A decline in the birth rate between 1970 and 1985, coupled with emigration,had limited net population growth to two percent per year since 1977. Thepopulation was young; forty-four percent were under fifteen years old. Seventypercent of St. Lucians had access (perhaps at some distance) to potable water,with the other 30 percent dependent on river water, while 60 percent had waterclosets, with the remainder still relying on pit latrines.
For adults, chronic and noncommunicable diseases occurring in the middleand later years with patterns similar to those of industrial countries were nowsignificant causes of mortality and morbidity. Hypertension, diabetes mellitus,cancer, and cerebrovascular disease were prominent. Traffic and other accidentswere growing in importance. A relatively high number of deaths attributable toill-defined conditions and symptoms suggested some weaknesses in the reportingprocedures, and had placed this "cause" of death among the top four in everyyear since 1976.
Infant mortality rates were reduced through a combination of improvedimmunization and diarrhea control programs. However, diarrheal diseaseremained an important cause of mortality and morbidity. Worms were a majorcause of morbidity in children. One study indicated that St. Lucia had aprevalence rate of more than 80 percent for trichuriasis and, in at least onecommunity, 10 to 15 percent of the two- to six-year-olds had associated colitisand growth stunting. Much progress had been made in reducing protein-energymalnutrition, but there were still indications that it was a problem, particularlyat lower socioeconomic levels. Respiratory infections were also a major healthproblem for children.

94 Section Two: Applied Experiences in Health Economics and Financing
AIDS was a growing problem in the Caribbean. Gonorrhea and syphilis rankedsecond and fourth among communicable diseases in a 1986 study. Gastroenteritis,influenza, and dengue fever were among the other top five communicable diseases.Schistosomiasis had occurred frequently in St. Lucia, but was now well controlledfollowing a Rockefeller Foundation project that the MOH had continued.
In 1985, the National Research and Development Foundation (NRDF) in St.Lucia conducted a health profile study of three rural communities. Between 13 and40 percent of mothers identified malnutrition as a problem in their children,depending on the community. Twenty-seven to 45 percent of people in the threecommunities reported that they used folk medicine and 50 to 100 percent used it totreat high blood pressure. Of these, 62 percent felt it was effective and 30 percentused it because it was cheaper than the alternatives. Poor sanitation was a majorcomplaint for respondents.
More than 70 percent of the people interviewed identified teenage pregnancy asa major social problem. It resulted in early termination of education, illegalabortions, inadequate parenting, and disorganized families. In 1986, 28 percent ofthe births in St. Lucia were to women between the ages of fifteen and nineteen and33 percent of all births were to women between the ages of twenty and twenty-four.
A number of socioeconomic factors created family disorganization. The relativelyfluid nature of male-female relationships both resulted in and perpetuated familydisorganization. Women headed more than half of all households. Socioeconomicinsecurity among women heads of households encouraged them to have additionalchildren to establish a stable relationship. Alcohol and other forms of drug abusewere serious problems, particularly for men, and were related to other socialproblems (early termination of education, unemployment and underemployment,disorganized families, destructive child-rearing practices, family violence, risingcrime rates, and rising traffic accidents).
The Ministry of Health
The government of St. Lucia had a strong commitment to public health care. TheMOH supported health service delivery through four facilities: Victoria Hospital andGolden Hope (the mental health hospital) in Castries, and two district hospitals inSoufriere and Dennery (see Exhibit 2). The MOH also provided a building andsubsidized the costs of St. Jude's Hospital in Vieux Fort, a private mission-runfacility. In addition, the MOH supported thirty-two health centers throughout thecountry. Public transportation, although often less than comfortable, was generallyquite accessible, and patients did not normally have to walk to a health center. Theservices available at the two district hospitals were limited and their bed occupancyrates were consistently low. Health centers normally offered one clinic a week. Otherservices were more limited.

Financing the St. Lucian Health Sector 95
Public revenues provided the major source of financing for health care in St.Lucia. In constant prices, per capita spending on health had increased by nearly 64percent over the past decade. In fiscal year 1986-87, the recurrent budget for theMinistry of Health and Labour was EC$ 19,957,424 (see Exhibit 3). After transfersto the Department of Labour and Sanitation, the remaining EC$ 17,560,810 wasdevoted to administration and health service delivery. The line item 'contributions'was primarily for the recurrent expenditures of St. Jude's Hospital. MOH capitalexpenditure estimates for 1986-87 were modest (see Exhibit 4).
Victoria Hospital
One of the popular carnival hits of 1987 was a calypso poking fun at VictoriaHospital. The 100-year-old building was antiquated and services were inadequate.Victoria Hospital was the major referral hospital, and it generally operated beyondits capacity. Bed occupancy rates were consistently high. The casualty service atVictoria Hospital was frequently used for regular, nonurgent visits. A national healthpolicy dictated that women with first pregnancies should deliver in hospitals. Giventhe limited services at the district hospitals and women's preference for what theyperceived as better quality and more reliable services at Victoria Hospital, the bedoccupancy rate was 96.5 percent in the matermity ward during 1986. The gynecologyward had occupancy rates of more than 90 percent. An appropriateness evaluationprotocol conducted as part of the hospital cost study indicated that 14 percent ofadmissions and 20 percent of days of care in the maternity ward were inappropriate.Both were higher than established and accepted rates.
Exhibit 5 provides a distribution of the hospital's recurrent expenditures. A 1987cost study of Victoria Hospital found that the full operating costs of the hospital weresignificantly higher than those estimated in the MOH's line item for VictoriaHospital's budget. Some of the costs of Victoria Hospital's operations were includedin the MOH budgets for other facilities (for example, medical stores) and were underthe budgets for other ministries. Victoria Hospital also financed some of itsoperations with off-budget resources. When depreciation of buildings and the capitalcosts of land were included, the total costs were even higher.
The cost study noted that about 20 percent of the costs were under the hospital'scontrol, including instruments, equipment, maintenance and other items. Personnelrepresented nearly 70 percent of total costs, and the average government wagesettlements for 1984 and 1986 had been, respectively, 20.8 and 18.0 percent. Thestudy recommended that an independent hospital board be created and that VictoriaHospital consider contracting out services such as meals and laundry.
Half of the medical doctors in the country were employed by Victoria Hospital.Only eight of the twenty-nine doctors were St. Lucian. The others represented six

96 Section Two: Applied Experiences in Health Economics and Financing
different nationalities, leading to variations in medical practice standards. Theshortage of nursing staff was a worsening problem and the existing nursing staff wasoverburdened.
Health User Fees
In St. Lucia user fees generally were set far below the actual costs of deliveringservices and categories of patients who were exempted from payment were broadlydefined. The government estimated that 92 percent of the population was exemptunder existing policies, which excluded the elderly, schoolchildren, other heavyhealth care users, and most public employees. Combined with other policies, thesituation decreased the incentive to collect fees from the few who were not exemptand supported a widespread attitude that free health care was the citizen's right. Allrevenues collected by the MOH (see Exhibit 6) were returned to the consolidatedfund. These revenues were not available for use by the MOH. Some considered thisa further disincentive for collection.
In Victoria Hospital, revenue from most wards covered between 9 and 17 percentof actual costs. For emergency room services, radiology, the operating theater, andthe private wing, fees were about 50 percent of costs. Only the laboratory andphysiotherapy had fees that were close to the actual costs of providing services (seeExhibit 7). Aside from the low level of fees, the value of services not billed becauseof exemptions was approximately 90 percent for Victoria Hospital. Nevertheless,apart from a contribution from the National Insurance Scheme (NIS), hospital userfees were the largest component of MOH revenues.
At St. Jude's Hospital, 96 percent of outpatients and 86 percent of inpatients didnot pay for services, even though all in-patients were billed and the hospital wasallowed to retain any earned revenues.
User fees for drugs were consistently less than the recurrent revenue estimates.A recent study in Grenada, where health and fiscal problems were similar to thosein St. Lucia, indicated that 25 percent of those receiving free drugs from governmentfacilities had paid the doctor who wrote the prescription. Some considered this anindication that patients were able and willing to pay for health services. The situationin St. Lucia was considered similar. In Dominica, where health and fiscal problemswere also similar, patients who received a prescription from a private practice werenot allowed to fill the prescription in a government facility. St. Lucia had both anational formulary and a regional formulary produced by the Eastern CaribbeanDrug Service, an agent that provided pooled tendering and drug procurementservices to seven of the ministries of health in the region. However, health ministriesdid not adhere firmly to these formularies in purchasing or prescribing.

Financing the St. Lucian Health Sector 97
Health Insurance
The National Health Insurance Scheme (NIS) covered 14 percent of thepopulation. Members contributed 5 percent of their salaries, and their employersmatched this. The NIS's contribution to the MOH was EC$ 1,500,000 in 1986-87.It was not clear whether the NIS subvention was appropriate under current legislationor adequate for health coverage of the NIS' s enrollees. Although the NIS maintaineda manual system for recording the names of active contributors, there was no wayof linking this system to users at the health care facilities. Active membership and thecosts of health care services provided to members could not be confirmed.
Another option that was being discussed was a health levy, similar to that used inBarbados, which would perhaps be connected to Internal Revenue.
Approximately 5 percent of the population held private health insurance policies.The payout ratio for private insurance in St. Lucia was very low, and the types ofservices for which policyholders were reimbursed were unknown (see Exhibit 8).The reasons for the low payout ratio were unclear, but some possibilities included thefollowing: (a) policyholders did not bother to file claims because of minimal chargesfor services; (b) determining liability for accidents was difficult; and (c) hospitaldocumentation was considered inadequate by insurance companies.
Private Sector
There were fifty-five doctors practicing in St. Lucia, seven in full-time privatepractice and forty-eight in the public service. All but two of the public servicedoctors also had private practices, and this situation was accepted by the governmentas compensation for the modest salaries that it provided. Only one of the privatepractices was a joint practice.
St. Lucia had approximately ten private pharmacies, seven of them in Castries.They generally carried a wider range of drugs than the Central Stores, although thesewere not limited to essential drugs. Two private laboratories operated in addition tothe laboratory at Victoria Hospital. One laboratory provided a wider range of teststhan did Victoria Hospital. The other laboratory had services similar to VictoriaHospital, but held a wider range of off-island contracts for special services.
In addition to these private sector services, St. Jude's Hospital was generallyconsidered private, although it received government subsidies. St. Jude's providedservices to individuals outside its defined service area. In order to raise its bedoccupancy rate, it had recently started to experiment with a preferred providerarrangement (a form of prepayment insurance program) with selected companies. Itsbed occupancy rate remained just over 50 percent.

98 Section Two: Applied Experiences in Health Economics and Financing
A recent study indicated that 2.3 percent of St. Lucians' disposable householdincome was spent on health: 1.2 percent was spent on pharmaceuticals, 0.7 percenton doctors' visits, and 0.4 percent on other products or services. When the 2.3percent was applied to estimates of total private consumption, it appeared that St.Lucians, on average, were spending EC$ 42 per capita on health care. Selected dataon health expenditure suggested that, in general, payments for hospital care were notmade.
As Mr. Lubin pondered the studies available to him, he was reminded thatalternative methods for financing the St. Lucian health sector presented complex anddifficult choices that might be politically sensitive.

Financing the St. Lucian Health Sector 99
EXHIBIT 1The Eastern Caribbean
ICI 96&TWD0103
68S Oritish Virgin Is. 68' 69'
7.s Y;rgin is lp AnguillaD, o0 U.S. Virgin is. isl
Puerto Rico Barbuda
St. Kitts'N Nevts Antigua
Monserrati Guadeloupe
Dominica1-16'
C A R R I B E A N Martinique%
S E A St.L ucia
St. Vincent
Barbados
o so loo 150 200 0
MItES Gronadaj 12*-
* Commonwealth Members and British Colonies

0
EXHIBIT 2ST. LUCIA'S HOSPITALS, COMPARATIVE STATISTICS, 1984
GoldenCategory Victoria St. Judes' Soufriere b Dennery' Hope Total
Number of beds 211 107 20 22 162 522Number of admissions 8,164 3,983 857 344 405 13,753
0
Number of patient days 60,088 23,066 3,906 1,370 N/A N/AAverage length of stay 7.4 5.8 4.6 4.0 N/A N/A z
Percentage occupancy 78 59 54 1 7 N/A N/A
00
N/A: Not available.Note: Estimated population of 134,100.a. A January 1988 study sponsored by the Pan-American Heafth Organization reported 114 beds at St. Judes. Cb. During a site visit at Soufriere Hospital in October 1987, the study team found twenty-nine beds and three cots. The inpatient census that day wasten patients (34 percent occupancy).
O.
c. During the same site visi there were twenty beds, of which, two were occupied (10 percent occupancy). Source: Ministry of Finance (18986); Stanton (34988).

Financing the St. Lucian Health Sector 101
EXHIBIT 3RECURRENT EXPENDITURE
MINISTRY OF HEALTH AND LABOUR, 1984/85 - 1988/89(EC$)
Actual Actual Estimates Estimates EstimatesCategory 1984-85 1985-86 1986-87 1987-88 1988-89
Administration 645,554 662,031 739,890 776,882 813,876Contributions' 1,742,000 1,982,837 2,026,840 2,128,182 2,229,524
Subtotal 2,387,554 2,644,868 2,766,730 2,905,064 3,043,400
Health and medicalcare
Administration 54,192 124,718 334,121 350,825 367,532Medical care 2,675,701 2,792,159 2,684,884 2,819,126 2,953,370Dental service 125,921 214,538 282,833 296,973 311,115Medical stores 2,155,682 2,205,961 1,592,721 1,672,357 1,751,993Sanitation 1,912,931 2,185,101 1,962,377 2,060,495 2,158,613Engineering 296,326 148,653 0 0 0Mosquito program 147,049 183,743 173,510 182,185 190,861Victoria Hospital 5,706,075 6,412,246 6,297,560 6,612,437 6,927,315Soufriere Hospital 277,074 327,072 363,425 381,595 399,767Dennery Hospital 166,802 174,581 200,776 210,813 220,852Golden Hope
Hospital 783,456 815,775 890,169 934,677 979,185Dispensaries 120,751 133,619 163,347 171,512 179,680Health education 205,330 200,821 608,384 638,802 669,222World Food
Program 308,783 403,708 339,685 356,668 373,653Training 524,189 656,218 862,665 905,798 948,931UJN.F.P.A.b 21,899 0 0 0 0Research and
control 260,841 109,579 0 0 0
Subtotal 15,743,002 17,088,492 16,756,457 17,594,263 18,432,089
Labour Department 0 314,084 434,237 455,948 477,659
Total 18,130,556 20,047,444 19,957,424 20,955,275 21,953,148
a. Contributions, listed under General Administration, represent funding provided to St. Jude'sHospital.b. United Nations Population Fund.Source: Govemment of St. Lucia (1 987).

102 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 4CAPITAL EXPENDITURE ESTIMATES,
MINISTRY OF HEALTH AND LABOUR, 1986-87
(EC$)
Category Estimates Local Grants Loans
St. Jude's Hospital 150,000 150,000 0 0
Health centers 100,000 100,000 0 0
Victoria HospitalLaboratory 100,000 100,000 0 0Operating theaters 25,000 25,000 0 0X-ray 22,900 0 22,900 0Standby generator 120,000 0 120,000 0
Subtotal 267,900 125,000 142,900 0
Golden Hope Hospital 603,000 0 603,000 0
Kellogg Project 710,000 0 710,000 0
SanitationWater development 400,000 400,000 0 0Water development 1,000,000 0 1,000,000 0Water distribution 2,500,000 0 0 2,500,000Roseau Dam 1,000,000 0 1,000,000 0Intake access road 250,000 250,000 0 0Sewage systems 250,000 0 250,000 0Sewage systems 249,448 0 249,448 0
Subtotal 5,649,448 650,000 2,499,448 2,500,000
Total 7,480,348 1,025,000 3,955,348 2,500,000
Health-related 1,830,900 375,000 1,455,900 0
a. Canadian International Development Agency.b. Friends of Golden Hope.c. Kellqgg.d. United Kingdom.e. Caribbean Development Bank.f. France.g. Urban Development Ccooperation.Source: Government of St. Lucia (1987).

Financing the St. Lucian Health Sector 103
EXHIBIT 5COST ALLOCATION FOR VICTORIA HOSPITAL, 1986-87
Other1.2%
Instruments16.7%
Utilities2.5%
Maintenance0.9%
Drugs
PersonnelEquipment 68.7%
1 S9%
Source: Stanton (1 988).

EXHIBIT 6REVENUE ESTIMATES, MINISTRY OF HEALTH AND LABOUR, 1984/85 - 1988/89
(EC$)
Actual Estimates Estimates Estmates EstmatesCategory 1984-85 1985-86 1986-87 1987-88 1988-89 aHospital fees 106,874 190,000 265,820 267,820 270,320Nurses' board 14,675 15,000 15,000 16,000 17,000Sale of drugs 13,417 33,000 104,750 106,750 108,000Confinement fee 1,430 11,400 30,000 30,200 30,500Sludge disposala 34,910 7,200 0 0 0Other sales 6,540 6,390 0 0 0 iInspectionsa 275 2,100 2,500 3,000 3,500Licensesa 1,554 6,500 15,000 16,000 17,000Regulabon of food handlersa 884 0 5,000 5,000 5,000Other receipts 5,043 12,000 18,000 18,500 18,600NIS contribution 1,000,586 1,000,000 1,500,000 1,500,000 1,500,000Ophthalmology 9,618 13,200 22,000 23,000 24,000Medical school 700 196,500 196,500 196,500 196,500Medical fees 10,569 22,000 25,000 25,200 25,400Work permitsb 0 300,000 350,000 355,000 360,000
Total 1,207,075 1,815,290 2,549,570 2,562,970 2,575,820a. Fees related to sanitation and restaurant/hotel sector.b. Fees related to the Labour DepartmentNote: Figures are based on anticipated surplus in 1986-89 and an increase in withholding.Source: Government of St. Lucia (1987).

Financing the St. Lucian Health Sector 105
EXHIBIT 7FEES IN RELATION TO UNIT COSTS
(EXCLUDING LABORATORY AND PHYSIOTHERAPY)
Maternity Y 107
Gynecology 3
Private 146
Medical 103
Surgical 96
Pediatric
Opthalmology 1 15 | 174
Theater I 27- i n I~~~~~~~~~~~~~r n ~~~~~ 611
Radiology 49
Casualty 3
0 100 200 300 400 500 600 700
ECS
S SaCosts
.Source: Stanton (I1988).

106 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 8PRIVATE ACCIDENT AND SICKNESS INSURANCE
PAYOUT RATIOS, SELECTED COUNTRIES
Claims paidCountry Gross and Payout ratio
premiums outstanding (percent)
Barbados (BDS$) 6,896,000 4,840,000 70.19Jamaica (J$) 46,382,933 36,380,355 78.43St. Lucia (EC$) 1,305,170 410,031 31.42Trinidad and Tobago 24,800,000 12,100,000 48.79
Source: St. Lucia Ministry of Finance

Financing the St. Lucian Health Sector 107
Source Documents
Huff-Rousselle, Maggie A. 1989. "Eastern Caribbean Health Sector Assessment& Strategic Alternatives: Anguilla, Antigua and Barbuda, British Virgin Islands,Dominica, Grenada, Montserrat, St. Kitts and Nevis, St. Lucia, St. Vincent andthe Grenadines." Ottawa: Canadian International Development Agency.
Stanton-Russell, S., G. Gwynne and M. Trisolini. 1988. "Health Care Financingin St. Lucia and Costs of Victoria Hospital." Health Care Financing in LatinAmerica and the Caribbean, Research Report No. 5. Stony Brook, New York:State University of New York.
Saint Lucia, Ministry of Health. 1986. Estimates of St. Lucia, 1986/87. Castries,St. Lucia.

Case 4. Planning for Health Services inEl Salvador: Need and Demand
Study Questions
The perspective in this case is a macro appraisal one rather than that of anindividual decisionmaker. The staff in the health planning unit of El Salvador's ministryof health face the task of how to make use of household survey information in theirplanning process. The concepts discussed in Section One's Basic Concepts of Demandare fundamental in grappling with the case's broad focus and the information containedin its exhibits. The study questions and the information regarding the interpretation ofmultiple regression analysis contained in the case's appendix provide the reader withguidance for using need and demand data to improve planning and investment decisionsabout health services.
1. How would you define health care need?
2. What differences might exist between a health care need as perceived by anindividual and one perceived by a medical professional?
3. What is health care demand?
4. What factors might influence an individual's decision about when and where to seekmedical care?
5. How is utilization of health services related to need and demand?
6. What consequences result from discrepancies between need, demand, andutilization?
7. How can or should policymakers and health planners accommodate discrepanciesbetween need, demand, and utilization?
108

Planning for Health Services in El Salvador: Need and Demand 109
Planning for Health Services in El Salvador: Need andDemand
In mid-1990, the Ministry of Health (MOH) in El Salvador received the analyticalresults of a household survey that was undertaken to determine the household demandfor health care in the country. The report was prepared by the team of consultants whocarried out a nationwide household survey and analyzed the data on behalf of thegovernment. The findings and policy implications were thoroughly discussed at aworkshop seminar attended by senior level officials from various ministries and severaloutside experts. The discussion of the need for health services versus the demand forand utilization of these services, and the implications of the survey's results for healthpolicy and planning had generated considerable debate. In early 199 1, the staff of thePlanning Unit of the MOH faced the task of how to make best use of this informationin their planning process.
Population and Health
The population of El Salvador was a young and growing one, increasing at 1.5percent per year. Of the country's 5 million inhabitants in 1988, more than 45 percentwere less than fifteen years old, and only 17 percent were older than forty-five. Duringthe previous two decades, El Salvador had achieved considerable progress in improvingthe health status of its population. The infant mortality rate fell from 1 18 per 1.000 livebirths to 55, and the general mortality rate declined to 6.4 per 1,000 inhabitants.Childhood deaths attributable to immuno-preventible illnesses were reduced to 4.8percent. However, 60 percent of deaths among children under one year old were causedby infectious diseases-especially diarrhea-and parasites. Thirty-five percent of allbirths were attended by health staff, and about 15 percent of babies were born with lowbirth weights. Overall, the leading causes of death were as follows: diseases of theperinatal period, intestinal infections, homicides and intentionally inflicted lesions,accidents, malignant tumors, and cerebral-vascular and ischemic heart diseases.
Per capita income in 1988 was US$940. Forty-five percent of the country'sinhabitants earned US$20 per month, while 15 percent had monthly incomes of morethan US$80. Illiteracy was still a serious problem: 31 percent of adults could notread or write. Although 79 percent of the children of school age wereenrolled in primary school, fewer than 60 percent completed four years of
This case was written by CatheHne A. Overholt, Collaborative for Development Action, Inc., with fundingprovided by the Economic Development Institute of the Wor/d Bank. Case material was drawn from analysesand reports by R. Bitran, J. Fied/er, and L. C. Gomez as well as from conversatons with them. While thecase is based on actual data, all names, places, and some peripheral facts have been disguised. The casewas prepared for use as a basis for classroom discussion rather than to illustrate either effective orineffective handling of a management of development situation.

110 Section Two: Applied Experiences in Health Economics and Financing
schooling. The urban population was growing at about 2 percent per year, and 44percent of the nation's inhabitants lived in urban settings.
The Structure of Health Services
The constitution of El Salvador conferred the responsibility for the health of itsinhabitants on the MOH. While about seventy nongovermment institutions had healthprograms, the MOH assumed the responsibility of providing preventive and curativecare to more than 85 percent of the population. Primary care was the priority policy andstrategy through which the MOH expected to attain an improved level of nationalhealth. Exhibit 1 provides an overview of the MOH's infrastructure.
The decade of the 1980s was one of mounting economic pressure on thegovernment's health care delivery system. The system, financed through central budgetallocation, was confronted with growth in the demand for health services stimulated bya constantly expanding and increasingly sophisticated medical technology that raisedthe cost of providing care. The number of MOH salaried positions grew by more than6.5 percent during the decade, and personnel expenditures swelled from 78 percent ofoperating expenditures in 1980 to 93 percent in 1988. Hospitals received 60 percentof the MOH's budget allocation, but annual recurrent costs for operating the system orindividual facilities could not be determined. By the end of the decade, financiallimitations constrained the quality and availability of government health services.
The average annual growth rates of real GDP were negative for most of the decade.Public health expenditure as a percentage of GDP fell from a high of 2.1 percent in1981 to 1.1 percent by 1988. The MOH's share of central government expendituredecreased from 10.8 percent in 1980 to 7.0 percent by 1988. Declining overallresources and competing pressures among national priorities foreclosed the option ofincreasing public resources for health services.
Limited off-budget resources were generated through an informal schedule ofvoluntary contributions at local government health facilities. Fee revenues collected foroutpatient services at health centers, units, posts, and hospitals and for inpatientcharges at hospitals (primarily higher quality room and board services) constituted 75to 80 percent of total off-budget revenues. Monies raised from various fundraisingactivities and philanthropic contributions augmented fee revenues. These resourcesgrew from 5.0 percent of operating expenditures in 1980 to 8.5 percent in 1988.Revenues were under the control and authority of local community health boards ratherthan the MOH. Fee revenues at hospitals represented 5 percent of their operatingexpenses. On a per patient consultation basis, hospitals raised less than any of the otherfacilities.
The Institute for Social Security of El Salvador (ISSS) provided health servicesto 11.6 percent of the economically active population (6.0 percent of the totalpopulation). The ISSS relied on services from nineteen MOH hospitals, but it

Planning for Health Services in El Salvador: Need and Demand 111
also maintained its own network of facilities. Financing for the ISSS was tripartite: 25percent by employers, 25 percent by workers, and 50 percent by the government.
The military offered its own preventive and curative health services to its membersand their families. Similarly, other government and private institutions provided healthservices to their employees. The National Administration of Telecommunications, forexample, had its own hospital, and the Ministry of Education contracted with privatephysicians and hospitals for health services for its employees.
While the telephone directory of the capital city, Santa Marta, listed more than 400doctors in private practice and dozens of private clinics, not much is known about thedelivery of private health services. Officials of the MOH believed that these serviceswere not widely used by families with modest incomes.
Health Policy, Planning, and Reform
The MOH's strategy at the beginning of the 1990s was to focus on improving theefficiency of resource use and to attempt to develop altemative sources of financing,such as user fees and other cost recovery mechanisms. At the same time, the MOH wascommitted to implementing the Pan-American Health Organization's (PAHO's) schemefor Local Systems of Health and to protecting the substantial proportion of Salvadoranswho were impoverished and medically indigent.
The MOH's financial position remained tenuous in mid-1990. Financial assistancefrom several international donor agencies was directed at assisting the MOH toimplement strategies for improving efficiency. A five-year project initiated in 1985 andfunded by a bilateral donor agency provided assistance to make managementimprovements within the MOH. Under this project, strategies were developed andimplemented for improving the organization and functioning of several key logisticsystems, for example, maintenance of vehicle fleet and biomedical equipment systems,availability and distribution of pharmaceutical and medical supplies, and developmentof a modem information system.
In response to PAHO's Local Systems of Health program, decentralizationstrategies were developed. The chief of the Department of Planning of the MOH wasa proponent of "districtization and decentralization." This plan proposed to groupdifferent types of MOH health facilities in a pyramidal referral structure within thirty-six demarcated geographic areas or districts of the country. A nonspecialty hospital orhealth center would form the pinnacle of the pyramid, and the lowerlayer would consist of all other facilities: health units, posts, and dispensaries.To implement this plan, the large teaching hospital located at the university'smedical school would form the peak of the pyramid in the capital city. Eachof the nine regional hospitals would cap nine other districts, and the

112 Section Two: Applied Experiences in Health Economics and Financing
existing health centers would serve as the pinnacle for fifteen districts. Anadditional eleven centers would be required to cap the remaining districts. Thisplan would boost the number of health centers by 75 percent and increase theMOH's total operating expenditures for 1989 by 18 percent.
The financial expert of the Institution Development Unit of the MOH'sPlanning Department proposed an alternative districtization scheme. This planwould create fifty district offices, but would not require building new healthcenters. Appropriately located health units would be remodeled to accommodateregional offices. This plan would increase the MOH's total operatingexpenditures for 1989 by 8.6 percent.
An external assessment of these proposals was contemplated before anydecisions were made on decentralization.
The Household Survey of Health Care Seeking Behavior
As part of its program of assistance to strengthen El Salvador's nationalcapacity to generate and manage health resources effectively, a bilateral donoragency promoted the idea of undertaking a study of the health care-seekingbehavior of the Salvadoran population. The agency officials knew of consumerbehavior or demand studies, based on nationally representative surveys ofhouseholds, that had been carried out in a few other countries. The premise ofthese studies was that individuals who have a health problem face two types ofdecisions. First they must decide whether to seek care outside the home, and ifthey do, they must then decide which provider they will visit. The studies hadcollected and analyzed information about the consumers' decisionmakingprocesses for meeting their individually perceived health needs and helpedprovide a better understanding of what factors were important in determiningwhen and where people would seek health services.
In discussions between officers of the MOH's Planning Office, representativesof the ISSS, and the bilateral agency, the participants concluded thatunderstanding what factors influence whether individuals seek health care servicesand where they will obtain them was important. The ministry's staff believed thatthe MOH provided all the preventive services in the country, and that it coveredat least 85 percent of the Salvadoran population for curative services. Yet it hadlittle understanding of where facilities and services might be inadequate, and ithad no knowledge of what was happening in the private sector. Knowing howhouseholds decide to seek health care services and what provider characteristicsare important to them could help decisionmakers determine what policies to adoptto improve the population's health status and achieve public health goals. TheMOH Planning Office and the ISSS concurred that a household survey andanalysis of the data collected could help develop this knowledge.
The study of the demand for health services in El Salvador was funded by thebilateral agency and carried out during 1989 and 1990. Survey data were

Planning for Health Services in El Salvador: Need and Demand 113
gathered from 2,885 households in El Salvador (13,896 people) betweenFebruary and March 1989 from three major strata of the country: MetropolitanSanta Marta, other urban centers, and rural areas. Households were chosen to beinterviewed from a probabilistic sampling procedure elaborated by the SalvadoranDemographic Association and the study team. This procedure ensured that thehouseholds would be representative of the total population, and the results couldthus be inferred to the whole country.
The survey questionnaire was jointly developed by the study team, thePlanning Office of the MOH, the Programming and Control Section of the ISSS,and external advisors to the MOH. The questionnaire gathered data about eachmember of a household on occupation, income, age, gender, health insurancecoverage and affiliation to social security or other welfare systems, health status,the occurrence of health problems in the two-week period prior to the survey,and the use of ambulatory health services in response to these health problems.The objective was to discern the patterns of utilization of health services bygeographic location, demographic and socioeconomic characteristics ofconsumers, and consumers' perception of their illness. Individuals who soughthealth care outside the household were asked to identify the type of health careprovider they visited and to specify the amount paid to each provider. Theamount of time and money spent on travel as well as the amount of time thepatient had to wait at the provider's facility were also recorded.
After the survey data were collected, they were assembled into tables andgraphs that described the utilization patterns according to various characteristicsof both consumers and providers. The application of an econometric model tothese data helped to establish the relative importance of each of these distinctfactors for individuals in making a decision whether and where to seek healthcare.
The survey revealed that the average number of outpatient consultations perperson per year in El Salvador was 2.5. Private providers delivered 45 percentof outpatient consultations, the MOH delivered 40 percent, the ISSS 13 percent,and other government institutions 2 percent.
The principal reason (74 percent) that individuals gave for seeking outpatientcare during the two-week period prior to the survey was illness. Accidents anddental problems accounted for an additional 7 percent of outpatient visits.Preventive reasons, such as prenatal care, immunization, or other preventivecheckups, were responsible for 19 percent of all outpatient visits.
Preventive consultations for children were 25 percent of all visits for childrenunder five years old and 9 percent of those of children between five andfourteen. Preventive visits for adults were 20 percent of all consultations amongthose fifteen to forty-four years old and 17 percent for those over age forty-five.Preventive care accounted for 13 percent of male and 14 percent of femaleoutpatient visits. Of all the outpatient visits that took place at MOH facilities, 35percent were for preventive reasons; 29 percent of the reported visits to the ISSS

1 14 Section Two: Applied Experiences in Health Economics and Financing
were for preventive care; and 15 percent of private consultations werepreventive.
Approximately 53 percent of the country's population-about 2.2 millionpeople-reported that they had had a health problem during the survey's two-week recall period. Twelve percent of these individuals sought curativeambulatory care from a health care provider. Eighty-one percent of those seekingcare saw a medical doctor, and 39 percent of these visits took place at MOHfacilities. Of those who fell ill but did not seek care, 46 percent treatedthemselves, 27 percent considered treatment was unnecessary, and 7 percent didnot seek care for economic reasons. Exhibits 2-4 summarize people's perceptionof illness and their decision to seek care by geographic area of the country,Exhibit 5 describes health care-seeking behavior according to characteristics ofthe consumer, Exhibit 6 provides information about the choice of the providerand Exhibit 7 reports waiting and travel time for those who sought health careservices.
Of the total outpatient consultations during the two week period, sixty-sixpercent involved some direct payment. Exhibits 8 and 9 indicate the consumer'sout-of-pocket expenditures associated with seeking health services.
These exhibits can provide only a description of what people do. They reveallittle about the relative importance of factors that affect health care-seekingbehavior. The external advisors to the MOH used econometric multipleregression analysis to measure the independent effect of factors on an individual'sdecision to seek health care. Appendix 1 provides a fuller explanation ofeconometric multiple regression analysis and its interpretation.
The analysis revealed that for individuals with a perceived illness, theprobability of seeking care outside the home was higher for individuals whosemain activities, such as employment, school, or care of the household, wereinterrupted by their illness. Among those who reported that illness interruptedtheir activities, 39.5 percent sought care, while for those whose illness did notinterrupt their activities 17.5 percent sought care. The probability was 44 percentfor choosing an MOH facility and 51 percent for selecting a private facility.
The likelihood of seeking care outside the home did not vary in any importantway across age groups, but the probability of choosing a private provider didincrease with age. This increase was greater among households in rural and otherareas than it was in Santa Marta. While the likelihood of seeking care outside thehome did not vary in any important way with gender, the analysis revealed thatwomen were more likely to go to nonprofit private facilities than men. Theanalysis did not find that schooling affected the likelihood of seeking care. Aseducational levels increased, however, so did the preference for seeking a privateprovider.
Travel time had a negative effect on both the probability of seeking care andon the choice of provider. Those within twenty minutes travel time of an MOH

Planning for Health Services in El Salvador: Need and Demand 1 15
facility were likely to seek care 19 percent of the time; 56 percent chose anMOH facility, 39 percent chose a private facility, and 5 percent went to the ISSS.Among those individuals living more than an hour away from an MOH facility,17 percent sought care; 32 percent chose an MOH facility while 59 percentselected a private provider. Similar effects were observed when consideringtravel time to either private providers or ISSS facilities.
Exhibits 10 and 11 provide additional results of the analyses. Exhibit 12shows what health care demand would be if all providers had the same price,waiting time, and travel time as those of the MOH, and if all people werebeneficiaries of ISSS. See Appendix I for an explanation of the assumptions usedfor the econometric analyses.
The Workshop Seminar
The workshop seminar convened in Santa Marta during August 1990 todiscuss the concepts, methods, and results of the survey. It was jointly organizedby the Ministry of Health, the ISSS, the Ministry of Planning, the university, theSalvadoran College of Physicians, and the bilateral donor agency. The workshopparticipants included senior government staff from the Ministry of Health, theSalvadoran Institute of Social Security, and the Ministry of Planning.Representatives from the university community, the Medical Association of ElSalvador, and the private health sector were also invited. International expertsfrom the bilateral donor agencies, the World Bank, the Pan American HealthOrganization, and private consultants also attended.
The descriptive and analytical findings of the study were presented by thestudy team. In their presentation, they suggested that a principal implication ofthe study was that patients perceived MOH services to be of poor quality. If theMOH wanted to capture a greater share of patients and obtain higher revenuesthrough an increase in its prices, it first would have to improve the quality of itsservices. Given the strong preference for private sector services that the studyrevealed, the team also suggested that the government could set policies toencourage a greater role for the private sector in service delivery to improve theaccessibility of health services. The four areas for policy options suggested bythe team were (a) improving the quality of MOH services, (b) changing MOHprices, (c) expanding the role of the private sector, and (d) expanding ISSScoverage and service quality.
In considering and evaluating these options, the workshop participantsdiscussed the relative importance of need and demand in health planning, theunderlying assumptions used in the econometric analysis, and the interpretationand implications of the study for health policy.

1 16 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 1THE MOH's INFRASTRUCTURE, SELECTED YEARS
(number)
Category 1979 1984 1986 1989
FacilitiesHospitals 14 14 14 14Centers 9 12 12 15Unitsa 109 100 105 110Postsb 159 215 221 203
PersonnelDoctors 1,327 1,523 1,527 1,609Nurses 1,307 1,261 1,274 1,369Auxiliary nurses 2,496 2,635 2,674 2,751
Total medical visits perclass of medicalprovider
Doctors 2,853,442 2,883,818 2,894,384 2,962,853Nurses 485,484 602,804 684,234 753,789Auxiliary nurses 141,770 178,327 185,894 232,632
Ambulatory visitsHospitals
Doctors N/A N/A 1,230,216 1,189,786Nurses N/A N/A 51,315 26,463
Health centersDoctors N/A N/A 369,415 481,841Nurses N/A N/A 71,933 42,125
Units and postsNurses N/A N/A 746,885 892,688
N/A: Not available.a. Units include health units and mobile community units.b. Posts include health posts, vaccination posts, community posts, and health dispensaries.c. Figures are for 1988.Source: Feidler (1990).

Planning for Health Services in El Salvador: Need and Demand 11 7
EXHIBIT 2HEALTH STATUS AS PERCEIVED
BY PEOPLE INTERVIEWED
People not PeopleLocation experiencing experiencing
health problems health problems
Metropolitan SantaMarta 542 (52%) 503 (48%)
Other urban areas 700 (46%) 835 (54%)
Rural areas 742 (46%) 886 (54%)
Total 1,984 (47%) 2,224 (53%)
Source: Bitran (1990).
EXHIBIT 3DECISION TO SEEK CARE
People not People seekingLocation seeking curative
curative care ambulatory care
Metropolitan SantaMarta 417 (83%) 86 (17%)
Other urban areas 730 (87%) 105 (1 3%)
Rural areas 805 (91%) 81 (9%)
Total 1,984 (47%) 2,224 (53%)
Source: Bitran (1990).

118 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 4REASONS GIVEN FOR NOT SEEKING CARE
(percentage)
Metropolitan OtherReason Santa Marta urban areas Rural areas
Thought no treatmentwas required 35 31 20
Self-treatment 34 46 51
Economic reasons 6 5 9
Other reasonsa 25 18 20
a. Lack of time, lack of permission from work, dislike of consultation or unsatisfactoryprior experience, distance of place of care and transport problems, place of care closed,missedappointment or consultation programmed for another date, permanent illnessSource: Gomez (1990a).

Planning for Health Services in El Salvador: Need and Demand 119
EXHIBIT 5CHARACTERISTICS OF INDIVIDUALS
AND DECISION TO SEEK CARE(percentage)
Metropolitan Other urban RuralSanta Marta areas areas
Care Care Carenot Care not Care not Care
Characteristics sought sought sought sought sought sought
GenderMale (45%) 83 17 87 13 92 8Female (55%) 82 18 87 13 90 10
Age group (years)Less than 1 (3%) 62 38 71 29 76 241 to4(12%) 81 19 85 15 91 95 to 14 (23%) 90 10 92 8 94 615 to 44 (38%) 81 19 87 13 90 1045 or older (24%) 83 17 85 15 90 10
Educational level (years)Oto6(76%) 85 15 87 13 91 97to12(20%) 81 19 86 14 89 1113 or more (4%) 73 27 87 13 100 0
Household annual income(March 1989 pesos)
4,000 or less (28%) 82 18 90 10 92 84,001-7,500 (23%) 83 12 90 10 91 97,500-15,000 (24%) 82 18 82 18 93 715,000ormore(25%) 81 19 83 17 89 11
Beneficiary statusNo insurance (92%) 84 16 89 11 91 9ISSS only (7%) 73 27 73 27 71 29Private insurance only (0.7%) 90 10 67 33 73 27ISSS and pnvate insurance (0.3%) 76 24 52 48 100 0
Health problemRespiratory 86 14 90 10 92 8Intestinal 79 21 88 12 89 11Accident 61 39 84 16 74 26Two conditions 79 21 83 17 90 10AJI three 84 16 78 22 100 0Other problems 83 17 85 15 89 11
Note: Percentages in parentheses in the first column indicate percentage of total population in thatcategorySource: Bitran (1990).

120 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 6PATIENT CHARACTERISTICS AND CHOICE OF PROVIDER
Ipercentage)
Characteristics Ministry of Health ISSS Private
Geographic locationMetro Santa Marta 26 1 6 58Other urban areas 43 14 42Rural areas 54 4 43
Average for all areas 42 12 46
Household annual income(March 1989 pesos)
1-500 28 0 72501-4,000 66 1 334,001-7,500 52 4 437,500-15,000 36 16 471 5,000 or more 23 22 56
Mean income 8,000 18,000 15,100
GenderMale 38 12 50Female 44 11 45
Age group (years)Less than 1 55 1 441 to4 55 0 455to 14 42 0 5815 to 44 38 22 4045 or older 36 9 56
Mean age 25 36 29
Educational level (years)0 to 6 48 9 427 to 12 25 17 5813 or more 23 15 61
Mean years of education 3.7 6.8 5.7
BeneficiaryProvider used 100 79 3Payment made 83 1 47
NonbeneficiaryProvider used N/A 21 97Payment made N/A 15 79
N/A: Not applicable.Source: Bitran (1990).

Planning for Health Services in El Salvador: Need and Demand 121
EXHIBIT 7TRAVEL AND WAITING TIME ACCORDING TO
PROVIDER AND GEOGRAPHIC LOCATION(average number of minutes)
Metropolitan Santa Other urban areas Rural areas
Waiting Travel Waiting Travel Waiting TravelProvider time time time time time time
Ministry of Health 158 40 157 51 169 69
ISSS 124 47 95 42 71 55
Private 62 40 57 53 62 82
a. Nineteen percent of patients waited less than 30 minutes and 19 percent waited less than 240minutes (4 hours).b. Twenty-nine percent of patients waited less than 30 minutes and 7 percent waited less than 240minutes (4 hours)c. Fifty-seven percent of patients waited less than 30 minutes and 2 percent waited less than 240minutes (4 hours).Source: Birtran (1990).
EXHIBIT 8OUT-OF-POCKET EXPENSES PAID BY INDIVIDUALS
TO PROVIDER FORCONSULTATIONS, EXAMINATIONS, AND MEDICATION
Expenditure Ministry of Health Social Security Private
Distribution (percent)0 15 96 191-5 68 3 86-20 12 1 2921-100 4 0 34101 ormore 0 0 10
Total 100 100 100
Average (March 1989 pesos)Santa Marta Metropolitan Area 3.6 0.3 52.5Other urban areas 6.4 0.2 37.6Rural areas 4.1 N/A 40.4
Total 5.0 0.2 43.9
N/A: Not applicable.Source: Bitran (1990).

122 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 9TOTAL OUT-OF-POCKET EXPENSES PAID
BY INDIVIDUALS PER EPISODE OF ILLNESS(all provider payments and purchases)
Ministry of Social PrivateExpenditure Health Security
Distribution (percent)0 16 88 191-5 48 5 106-20 21 4 1421-100 15 2 31101 or more 0 0 26
Total 100 99 100
Average (March 1989 pesos)Santa Marta
Metropolitan Area 10.8 2.7 79.9Other urban areas 19.4 0.4 71.5Rural areas 10.8 N/A 67.3
Total 14.4 1.3 73.3
N/A: Not applicableSource: Bitran (1 990).

EXHIBIT 10DECISION TO SEEK CARE AND CHOICE OF PROVIDER AS A FUNCTION OF PRICE
(percent)Price at Ministry of Health Facility (April 1989 pesos)
0 2.5 5.0 () 7.5 10.0
Decision Decision Decision Decision Decisionto seek Provider to seek Provider to seek Provider to seek Provider to seek Provider
care choice care choice care choice care choice care choiceRegion m~
Santa Marta Metropolitan AreaNo medical care 81.9 82.3 82.8 83.2 83.5Medical care 18.1 17.7 17.2 16.8 16.5
Ministry of Health 52.2 48.7 45.3 42.1 38.4 ICD
Social Security 5.0 5 3 5.7 5.0 6.4 IPrivate-for-profit 37.5 40.3 42.9 45.5 48.2 =
Private nonprofit 5.3 5.7 6.0 6.4 7.0 coOther urban areas o
CDNo medical care 84.7 85.2 85.6 86.0 86.3Medical care 15.3 14.8 14.4 14.0 13.7
Ministry of Health 58.1 54.7 51.3 47.9 44.2 rnSocial Security 4.5 4.9 5.3 5.6 6.3 CnPrivate-for-profit 35.8 38.8 41.6 44.5 47.3 m
a.Private nonprofit 1.6 1.7 1.8 1.9 2.2 Q
Rural areas zNo medical care 85.7 86.1 86.5 86.9 87.2 CD
Medical care 14.3 13.9 13.5 13.1 12.8 E
Ministry of Health 56.0 52.6 49.2 45.9 42.6 Q
Social Security 1.8 1.9 2.0 2.2 2.3 0Private-for-profit 40.1 43.2 46.3 49.4 52.3Private nonprofit 2.1 2.1 2.5 2.6 2.8 X
E.
Source: Cruz, Lozano, and Querol (1990).

EXHIBIT 10(continued)
Price at Private-for-Profit Facility (April 1989 pesos)
0 38 77() 115
Decision Decision Decision Decisionto seek Provider to seek Provider to seek Provider to seek Provider '
Region care choice care choice care choice care choice aSanta Marta Metropolitan Area
No medical care 63.0 77.7 82.8 84.1Medical care 37.0 22.3 17.2 15.9
Ministry of Health 4.9 22.9 45.6 55.2Social Security 0.6 2.9 5.7 6.9Private-for-profit 93.8 71 2 42.6 30.5Private nonprofit 0.7 3.0 6.1 7.3
Other urban areas mC)
No medical care 68.1 81 .3 85.6 86.7Medical care 31.9 18.7 14.4 13.3
Ministry of Health 5.7 26.2 51.5 62.0Social Security 0.6 2.7 5.3 6.4Private-for-profit 93.5 70.1 41.4 29.4Private nonprofit 0.2 0.9 1.8 2.2
Rural areasNo medical care 68.7 82.1 86.6 87.7Medical care 31.3 17.9 13.4 12.3
Ministry of Health 5.0 23.9 49.4 60.9Social Security 0.2 1.0 2.0 2.5Private-for-profit 94.6 74.0 46.0 33.5Private nonprofit 0.2 1.2 2.5 3.0
Note: Assumptions used for analysis are presented in Appendix 1.Source: Bitran (1990).

EXHIBIT 1 1DECISION TO SEEK CARE AND CHOICE OF PROVIDER AS A FUNCTION OF PRICE AND INCOME
(percent)
Price at Ministry of Health Facility (April 1989 pesos)
0 2.5 5.0(*) 7.5 10
Annual household Decision to Provider Decision to Provider Decision to Provider Decision to Provider Decision to Providerincome quintile seek care choice seek care choice seek care choice seek care choice seek care choice0-2,876 pesos :No medical care 82.0 82.5 82.9 83.3 83.7 5Medical care 18.0 17.5 17.1 16.7 16.3
Ministry of Health 53.1 49 6 46.2 42.9 37.7 ISocial Security 5.1 5.4 5.8 6.2 6.5Private for profit 36.5 39.2 41.9 44.5 47.0 =Private nonprofit 5.3 5.7 6.1 6.5 6.9 cn
5,181-7,800 pesosNo medical care 81.6 82.1 82.5 82.9 83.2Medical care 18.4 17.9 17.5 17.1 16.8 3
Ministry of Health 50.4 47.0 43.7 40.5 37m5 mSocial Security 4.8 5.1 5.5 5.8 6.1 gnPrivate for profit 39.6 42.3 45.0 47.5 50.0 XPrivate nonprofit 5.2 5.5 5.9 6.2 6.5 o
14,801-176,400 zpesosNo medical care 80.1 80.5 80.8 81.1 81.3Medical care 19.9 19.5 19.2 18.9 18.7 a.
Ministry of Health 40.9 38.0 35.3 32.7 30.2 3Social Security 3.9 4.1 4.3 4.5 4.6Private for profit 50.7 53.2 55.5 57.8 59.9 .
Private nonprofit 4.5 4.7 4.9 5.1 5.3 _VI

EXHIBIT 1 1(continued) 0
Price at Private-for-Profit Facility (April 1989 pesos)
0 38 77(*) 115
Decision Decision Decision Decision >to seek Provider to seek Provider tc ;eek Provider to seek Provider '
Annual care choice care choice care choice care choice o.mx0-2,876 pesos
No medical care 63.0 77.9 83.0 84.2 (DMedical care 37.0 22.1 17.0 15.8 3
Ministry of Health 4.9 23.2 46.4 56.3 oSocial Security 0.6 2.9 5.8 7.1 5Private-for-profit 93.8 70.8 41.6 29.1 I
Private nonprofit 0.6 3.1 6.2 7.55,181-7,800 pesos m
0No medical care 62.9 77.5 82.5 83.8 0Medical care 37.1 22.5 17.5 16.2 0
Ministry of Health 4.9 22.2 43.9 53.0 .Social Security 0.6 2.8 5.5 6.6Private-for-profit 93.8 72.0 44.7 33.3Private nonprofit 0.7 3.0 5.9 7.1 m
14,801-176,400 pesosNo medical care 62.9 76.0 80.8 81.8 o
Medical care 37.1 24.0 19.2 18.2Ministry of Health 5.1 19.2 35.4 40.5Social Security 0.6 2.3 4.3 4.9Private-for-profit 93.6 75.8 55.4 49.0Private nonprofit 0.7 2.7 4.9 5.7
Note: Assumptions used for analysis are presented in Appendix 1.Source: Bitran (1990).

Planning for Health Services in El Salvador: Need and Demand 127
EXHIBIT 12DECISION TO SEEK CARE AND CHOICE OF PROVIDER WHEN
PRICE, TRAVEL TIME, AND WAITING TIME ARE THE SAME(percent)
Gender
Male Female
Decision Decisionto seek Provider to seek Provider
Region care choice care choice
Santa Marta Metropolitan AreaNo medical care 49.30 47.00Medical care 50.70 53.00
Ministry of Health 24.20 2.51Social Security 26.80 36.41Private-for-profit 70.32 60.19Private nonprofit 0.46 0.89
Other urban areasNo medical care 55.10 52.90Medical care 44.90 47.10
Ministry of Health 2.86 2.98Social Security 25.88 35.43Private-for-profit 71.12 61.31Private nonprofit 0.14 0.28
Rural areasNo medical care 58.00 56.70Medical care 42.00 43.30
Ministry of Health 2.98 3.36Social Security 10.85 16.06Private-for-profit 85.96 80.13Private nonprofit 0.21 0.45
Note: Assumptions used for analsis are presented in Appendix 1.Source: Bitran (1990).

128 Section Two: Applied Experiences in Health Economics and Financing
Appendix 1
Econometric multiple regression is a statistical means of analyzing behavioralphenomena. Any observable and measurable trait is subject to multiple causes,and statistical techniques enable us to analyze the relationship between adependent variable and a set of independent variables.
In the traditional economic theory of demand, we presume that an individualhas preferences and can choose between different bundles of goods. The theoryprovides the basis for examining the effect on an individual's consumption ofthese goods given changes in other factors. In demand theory we concentrate ona handful of variables that are useful in explaining differences in quantities ofgoods consumed, in this instance, health services. The quantity of health servicesdemanded (the dependent variable) depends on many elements (the independentvariables). While economic theory is an enormous simplification of a complicatedreality, it allows the researcher to extract important elements that can explain alarge part of the observed phenomena.
To assess the effect of particular variables on the demand for health services,one must keep constant all other factors that affect demand. For example, if onewants to assess the extent to which gender influences demand, one must keepconstant, that is, fix the value of each of the other variables such as education,age, prices, travel and waiting time, income, and beneficiary status. By fixingthese variables, one can prevent them from having their own effect on demand,and the effect of a particular variable can be isolated.
The values (or assumptions) that were fixed to identify the effect of thevariables discussed in the text are as follows:
Activity interruption noAccident noSocial security beneficiary noAge 25-44 yearsGender maleEducation 3 yearsIncome 6,016 pesos (yearly)

Planning for Health Services in El Salvador: Need and Demand 129
The values (assumptions) for variables used in the analysis in Exhibits 10-12follow:
Assumptions for Exhibit 10Activity interruption noAccident noSocial security beneficiary noAge 25-44 yearsGender maleEducation 3 yearsIncome 2,876 colones (yearly)
Private- PrivateEXHIBIT 10 MOH SS for-profit non-profit
Price n.a. 0.2 n.a. 11.7
Travel time 56 45 52 44
Wait time 162 104 56 94n.a. not applicable 1 56 94
Assumptions for Exhibit 11Activity interruption noAccident noAge 25-44 yearsGender maleEducation 3 yearsRegion Santa Marta Metropolitan Area
Private- PrivateEXHIBIT 11 MOH SS for-profit non-profit
Price 5 0.2 76.5 11.7
Travel time 56 45 52 44
Wait time 162 104 56 94

130 Section Two: Applied Experiences in Health Economics and Financing
Assumptions for Exhibit 12Activity interruption noAccident noSocial security beneficiary yesAge 25-44 yearsGender see tableEducation 3 yearsIncome 7,800 colones (yearly)
Private- PrivateEXHIBIT 12 MOH SS for-profit non-profit
Price 5 5 5 5
Travel time 56 56 56 56
Wait time 162 162 162 162

Planning for Health Services in El Salvador: Need and Demand 131
Source Documents
Bitran, Ricardo. 1990. Household Demand for Health Care in El Salvador:Determinants of Household Demand for Curative Ambulatory Medical Care.Vol. II. Arlington, Virginia: REACH Project, John Snow, Inc.
. 1991. Health Care Demand in Latin America: Lessons Drawn from theDominican Republic and El Salvador. Washington, D.C.: EconomicDevelopment Institute and Abt Associates.
Fiedler, John. 1990. "Contributions to the Mid-Term Evaluation of theUSAID/EI Salvador APSISA Project. Arlington, Virginia: United States Agencyfor International Development.
. 1991. Increasing Reliance on User Fees as a Response to Public HealthFinancing Crises: a Case Study of El Salvador. Arlington, Virginia: UnitedStates Agency for International Development.
Gomez, Luis Carlos. 1990a. Household Demand for Health Care in El Salvador:Household Survey Methodology and Findings. Vol. I. Arlington, Virginia:REACH Project, John Snow, Inc.
. 1990b. Seminario-Taller Sobre Demanda de Servicios de Salud en ElSalvador, del 27 al 29 de Agosto de 1990. Arlington, Virginia: Clapp & Mayne,Inc. Association of University Programs in Health Administration.
Pan-American Health Organization (PAHO). 1990. Las Condiciones de Salud enlas Americas. Vol. II Washington, D.C.

Case 5. Hospital Jose Maria Cabral y Baez
Study Questions
The following two cases, Hospital Jose Maria Cabral y Baez and TheAGAPCO Financial Plan, provide an opportunity to consider how health servicesand products can be produced and delivered with greater efficiency, that is, at alower cost. The concepts discussed in Section One's Production and CostAnalysis in the Health Sector provide a departure point for the case analysis.However, the reader will also find the concepts and tools discussed under BasicConcepts of Demand and Financing the Health Sector useful in the case analysis.The problem facing Dr. Estevez in the Dominican Republic is how to minimizethe impact on hospital operations of a sudden, large, and unexpected increase inthe cost of pharmaceuticals.
1. What are Dr. Estevez's most serious problems? Why'?
2. What are the underlying causes of these problems?
3. What should Dr. Estevez do to address the current crisis caused by theincreased cost of medicines and supplies?
4. What actions should he take over the long term to improve the quality ofhealth services in the hospital? In the region?
5. How can he improve efficiency in the use of health resources in the hospitals?In the region?
6. What actions would you recommend the Secretary of Health take to improvehospital management and resource use in public facilities?
132

Hospgal Jos6 Maria Cabral y Biez 133
Hospital Jose Maria Cabral y Baez
Dr. Rafael Estevez, Director of the Jose Maria Cabral y Baez Hospital, the mostmodern and well-endowed hospital in the Dominican Republic, hung up the phoneand paused to reflect on the significance of what he had just heard. It was 6 p.m.,April 16, 1984, and he had just been told by Dr. Amiro Perez Mera, the Secretaryof Health, that tonight President Salvador Jorge Blanco would announce that theCentral Bank' s preferential exchange rate for imports of food and medicines wouldno longer be used. The Secretary of Health had informed him that all importedmedicines would be transferred from the official exchange rate of one peso per U.S.dollar to the "parallel market," where the exchange rate was approximately 2.8 pesosper dollar.
It had been a typically hectic day. Dr. Estevez had spent much of the morningvisiting an area hospital in his role as Director of Region II for the Secretariat ofHealth and Social Assistance (SESPAS). Returning to the hospital at noon, he hadspent the last few hours attending to the steady stream of visitors and calls to hisoffice from department heads, the press, doctors, and even a few patients. Now itlooked like a new crisis would demand his attention. Dr. Estevez, a thin, dark,handsome man perpetually dressed in a white coat, was greatly concerned about theimpact of an almost 300 percent increase in the price of medicines, since they madeup more than half of the hospital expenditures that were under his direct control.SESPAS administered the hospital's personnel budget.
As Dr. Estevez contemplated the possible steps he could take to deal with thecrisis, he considered the list of budget goals he had presented to the board ofdirectors the previous August:
1. Petition SESPAS for an increase in the hospital's monthly income
2. Raise money via board members
3. Recover one month's income that SESPAS had not paid to the hospital in 1982
4. Increase occupancy on the private patient floor to increase income
5. Initiate a charge for inpatient surgical services
6. Increase existing charges.
This case was written by Linda S. Harder, MBA, under the supervision of Michael R. Reich, AssociateProfbssor, Harvard School of Pubic Health. The case was developed with the support of the Pew MemorialTrust and the Takenry Program in Intemational Health, and with the cooperation of Jos0 Marla Cabral y BaezHospital and the coDlaboarion of the Centro de Administraci6n del DesarroDlo Rural of the Instituto Superiorde Agricultura. The case was prepared as the basis for classroom discussion rather than to iustrate eithereffective orineffective handling of a managerial or development situation.

134 Section Two: Applied Experiences in Health Economics and Financing
Dr. Estevez wondered which of these plans might help him deal with theimmediate crisis, and what other actions might be needed. He did not wish toincrease the hospital's 'debt" (the hospital was legally barred from incurring adebt, but carried long-outstanding accounts payable). He was proud of his abilityto keep it at the level that he had inherited from his predecessor. Before Dr.Estevez could think any further about the problem, he was interrupted.
"Dr. Estevez," called his secretary, "you're needed in surgery for anemergency." As he walked through the corridors, Dr. Estevez reflected on thehealth care situation in the country since he had become director of the hospitala year and a half ago, the problems his hospital faced, the measures he hadalready taken to economize and improve financial control, and the steps he couldtake to deal with this new fiscal crisis. He was aware of many limitations in hisown ability to deal with the impact of the foreign exchange crisis on the publichealth system and on his hospital. Certain solutions could only come fromSESPAS, and he wondered what recommendations, if any, he should make to thesecretariat. Devising a plan to increase revenues or decrease costs so as toprevent a decline in the quality or quantity of the hospital's services wouldpresent a challenge.
SESPAS Region 11
The Jose Maria Cabral y Baez Hospital (JMCB) was located in Santiago, themajor city in SESPAS Region II and the second largest city in the DominicanRepublic. The five provinces in the Cibao Valley comprised Region II, one ofeight SESPAS regions (see Exhibit 1), Twenty-five percent of the country'spopulation, about 1.4 million people, lived in Region II.
Private health services in Region II served privately insured individuals andpeople who paid out-of-pocket expenses for services, mostly the upper 10 percentof the population. Forty-six small clinics and 210 pharmacies comprised theprivate sector for health services. The public health facilities under SESPAS'sdirection provided health services to the poor and uninsured, roughly consideredto be 80 percent of the population. Other health coverage was provided by thesocial security and armed forces sectors, which together served 8 to 9 percent ofthe population, mostly from the lower-middle class.
In 1983, SESPAS Region II operated 1,565 beds that were distributed amongthe regional hospital (JMCB), one children's hospital, seven area hospitals, andnine subcenters. SESPAS also maintained six urban clinics and sixty-seven ruralclinics in Region II.U In principle, SESPAS services were provided hierarchically,with patients referred to the area and regional hospitals only after visiting theclinics and subcenters (see Exhibit 2). In reality, patients tended to bypass the
1. Nationwide, SESPAS institutions include 337 urban and rural clinics; 7,486 beds in 48hospitals, 55 subcenters, and 13 specialty facilities; and 6,000 local health representativesproviding preventive health care services to their communities.

Hospital Jos6 Maria Cabral y Biez 135
clinics and subcenters because these facilities often lacked equipment, personnel, orsupplies. Exhibits 3-5 present the major causes of mortality in hospitals, the majorreasons for seeking medical care from SESPAS physicians in 1983 for Region II andthe principal causes of mortality nationwide. The organizational objectives of theSESPAS reflected the priorities of the Minister of Health appointed in 1982 (seeExhibit 6).
Each of the SESPAS regions had a regional office whose interdisciplinary teamwas responsible for carrying out national policies, directing and coordinating regionalservices, and maintaining regional statistics. The office had limited influence overSESPAS institutions in the region because it did not control their supply of funds,which came directly from the central office. In 1984, the administrative director ofSESPAS Region II was Dr. Estevez. This was the first time a hospital director hadalso been regional director.
Hospital Jose Maria Cabral y Baez
The original JMCB hospital was founded in 1946 with 250 beds, and wasexpanded in 1953 to 350 beds. A new six-story building housing 417 beds wasconstructed in 1977 at a final cost of RD$ 12.4 million, of which RD$ 10 million wasspent on construction costs and 2.4 million on major movable equipment. With theinauguration of President Salvador Jorge Blanco in August 1982, Dr. Rafael Estevezwas appointed director.
In 1984 the hospital was considered unique among public hospitals in theDominican Republic. Among its distinguishing characteristics it boasted a teachingaffiliation with the medical school of the University Cat6lica Madre y Maestra inSantiago, and it housed the largest and most sophisticated range of services andequipment in the country. Dr. Perez Mera described the hospital's uniqueness in thefollowing way:
Jose Maria Cabral y Baez is not a typical Dominican hospital. It is a copy in someways of a Puerto Rican hospital. The architect was from Puerto Rico. It is also amixture of the U.S. and the Dominican Republic in that the past and current directorsare Philadelphia trained surgeons. The hospital is unusual in its equipment, thebuilding design, and its human resources, all of which are superior to any otherhospital in our country. However, its relationship to the Secretariat and itsadministration are more or less the same as other hospitals in the country.
The hospital was spaciously designed, but sparsely furnished. During the morninghours, a visitor was likely to be impressed by the numbers of patients crowding thebenches that lined the outpatient clinic waiting areas. In the afternoons the clinicswere closed, and even the inpatient area appeared quiet. Equipment was limited. Theradiology department, for example, was awaiting arrival of its first ultrasoundmachine, but had been unsuccessful in its request to the Secretary of Health for a CTscan machine.

136 Section Two: Applied Experiences in Health Economics and Financing
The JMCB's Mission and Scope of Services
The hospital's mission was to provide general and specialized health servicesand medical care to the community without discrimination. Like other SESPAShospitals, the majority of its patients were the poor and uninsured who could notafford private clinics or were not eligible for social security or armed forcesmedical services. The hospital generally provided services free of charge, and nopatient was refused service on the basis of inability to pay.
As the regional hospital for Region II, the JMCB was at the apex of servicecomplexity in the region. It was the only regional hospital in the SESPAS systemthat provided the quantity and complexity of services implied by its role. Itoffered a full range of medical services, with twenty-two specialties, includingradiology, nuclear medicine, internal medicine, cardiac surgery, cardiology, or-thopedics, urology, psychiatry, neurosurgery, obstetrics/gynecology, andnephrology. It also provided a wide range of outpatient services and anemergency room. A recent study found that most other regional hospitals offereda level of services comparable to what would be expected at lower-level areahospitals.
As the most well-endowed public hospital in the country, the JMCB'sinfluence extended beyond the regional boundaries. Partly for this reason, somehospital personnel questioned the appropriateness of the hospital's role as aprovider of care to the poor. One doctor commented:
The hospital should not treat only the poor. We provide services here that eventhe private clinics cannot provide. We should serve all patients, developing apatient income test and then charging patients according to their ability to pay.The hospital is also burdened with social security patients who use this hospitalbecause it is better maintained than the social security hospital in Santiago.
In 1984 general medicine accounted for approximately 20 percent of all theJMCB's admissions and surgery for 12 percent. Obstetrics and pediatrics eachcontributed 6 percent to total admissions. The principal surgical operations werebiopsies, obstetrics, abdominal procedures, and orthopedic procedures. Each daythe hospital performed approximately 40 deliveries and the emergency roomtreated about 200 patients. The outpatient service saw over 500 patients per day,app.oximately two patients per physician per hour (see Exhibit 7).
Information on patient profiles was limited. The hospital's department ofsocial services maintained a monthly record of all patients who were referredfrom other institutions, including name, age, sex, reason for referral, andtreatment received. The department head estimated that approximately 100patients were referred monthly from other institutions, such as the SantiagoChildren's Hospital, which lacked the specialized services and equipmentavailable at the JMCB.

Hospital Jos6 Maria Cabral y Bdez 137
The monthly report of all referred patients was sent to the director, butinformation was not compiled in summary form. The head of the statisticsdepartment noted that a medical student had conducted a study that compiledpatient profile data from the hospital, but the hospital was still waiting to receivea copy of this study.
Role of the Hospital Director
The JMCB's director was appointed by the secretary of SESPAS andanswered to a nineteen-member board of directors headed by the secretary. Theboard met quarterly and during emergencies. Board functions included approvingthe budget for each fiscal year, overseeing plant and equipment maintenance, andshaping internal hospital policy.
The hospital director was both the medical and administrative director of thehospital and presided over the medical, nursing, administrative, and maintenancedivisions. He was assisted by an administrator. All the administrative departmentheads (including personnel, pharmacy, kitchen, and statistics) and each of themedical department heads (including social services) considered Dr. Estevez tobe their direct supervisor. Other personnel, such as the head of health educationand the Peace Corps volunteer assigned to food services management, alsoregarded him as their immediate supervisor. All expenditure requests were firstapproved by the administrator and then sent to the hospital director for finalapproval.
Dr. Estevez noted with pride that his administrator, Gladys Ortiz, was acertified accountant. She was one of only three public administrators in thecountry to hold a bachelor's degree. Dr. Estevez himself had recently receivedtraining in management skills at a three-week course conducted by aninternational health management firm. He described his approach to hospitalmanagement and the priority he placed on communication and on economy:
For the first five months I spent much of my time talking with staff, includinghousekeeping and laundry staff. You have to find out what they do. Many peopledon't know the importance of the work they do. I explain to them that they areas important as doctors. I do that because most of our problems are incommunication. Improving communication is critical for any institution, especiallyin Latin America . . . Good administration of economic resources, this isimportant. Even though prices have been increasing while our monthly incomefrom SESPAS stays the same, we have kept the debt the same. We are using themoney collected in a better way. This has not affected the quality of services.How do we do this? I don't know.
The hospital did not have formal policies or long-range goals, and Dr.Estevez noted that there were no staff evaluations, although each departmentmaintained a set of job descriptions. Many staff believed that Dr. Estevez hadgreatly improved the control systems to prevent loss of supplies and equipmentand that he had made some important personnel changes. However, they

138 Section Two: Applied Experiences in Health Economics and Financing
commented that he no longer visited the floors as much as he did initially, andsome staff had resorted to communicating with him through memorandums,because his time was limited. One department head stated that since Dr. Estevezhad become director, department head meetings were scheduled only on an as-needed basis.
Hospital Personnel
All JMCB personnel were public sector employees who were hired, trans-ferred, and fired by the secretariat, whose approval was required for all suchdecisions. Employees were paid directly by SESPAS, and JMCB's director, asall SESPAS hospital directors, did not have direct control over personnelbudgets.
In 1984 the JMCB employed 1,382 people, including its medical residents.Dr. Perez Mera regarded personnel as one of the greatest problems in SESPAShospitals for several reasons:
One, there is an excess of physicians whose productivity is poor. Second, thereare many nurse auxiliaries who work hard, but who function at a very low skilllevel. Third, the administration is not modem at most hospitals, even at JMCB.We are running hospitals with 1,916 administrative practices. Also, we cannotcompete, due to the poor salary levels. There are no legal fringe benefits.
Most personnel (excluding physicians who only worked until noon) workedMonday through Friday until 1:00 or 2:00 p.m. and alternate Saturday mornings.Some employees reportedly worked two jobs to compensate for the low salary.Dr. Estevez stated that there were more employees than there should be and theirwork was often less than productive. One observer pointed out that the employeetime clock had been broken, allegedly by the employees themselves.
The appointments of many public health personnel had traditionally beenlinked to political connections. Dr. Estevez commented:
Many people work in the hospital because of their political connections. Thesecretary or president may call up and request placement for a person. I try tosend that person to the personnel department so that at least the best match can bemade. The director has to have control.
Regarding physicians, Dr. Estevez commented:
Many doctors have private clinics. At least 10 percent of them consider thehospital a very low priority. One form of control is the residents. They're tryingto learn and do the best for the patient . . . they observe the doctor and askquestions about the usage of medicines.

Hospital Jos6 Maria Cabral y Baez 139
Income and Expenses
The JMCB, like all other SESPAS hospitals and subcenters, received a monthlyallocation of its assigned budget from the SESPAS central office (see Exhibit 8).Clinics and local hospitals received between RD$ 1,500 and RD$ 20,000 per month.These sums were expected to cover all operating expenses except salaries, whichwere paid directly by SESPAS. Average salaries for all personnel, including manage-ment staff, were low compared to those for comparable positions in the privatesector. The salaries of JMCB personnel totaled RD$ 328,000 per month (see Exhibit9).
The JMCB was atypical among SESPAS hospitals in that it had several additionalsources of income. Revenue generated from its "private" twenty-eight bed unit forpaying patients on the sixth floor was its major source of additional income. Althoughpublic patients received most services and all supplies free, private patients werecharged for all services and supplies. The amount charged varied according to thenumber of beds per room (see Exhibit 10). In addition to fees for room, board, andsupplies, private patients were charged for each specialist who provided medicalattention while they were hospitalized. Twenty percent of the amount paid to thespecialist went to the hospital.
Little was known about why private patients selected the JMCB, and noinformation on patient characteristics or origins was kept in summary form. Ms.Ortiz believed that patients were attracted to the hospital's private floor because itscosts were at least 25 percent lower than those private clinics charged.
Another source of off-budget income for the hospital was the fee charged forsome ancillary services. All inpatients and outpatients were charged for nuclearmedicine and radiology services. Charges for these services were lower for publicpatients than for the hospital's private floor patients. For an electrocardiogram, forexample, a public patient was charged RD$ 2, but a private patient paid RD$ 15 in1984. Outpatients were also charged for laboratory exams.
Patients who claimed to be unable to pay for the ancillary services wereinterviewed by Social Services Department staff to determine their ability to pay.There were no reliable methods for determining payment ability and the department'sstaff acknowledged that they had to depend on the patient to supply valid information.Ms. Ortiz estimated that as many as 50 percent of public patients paid nothing forancillary services, and that another 30 percent paid only a portion of their fullcharge.
The JMCB prepared monthly income statements that recorded income andexpenditures (see Exhibit 11), but did not maintain balance sheets to keep trackof inventory, cash, plant assets, or debt. The accounting department did preparea monthly record of bills owed to hospital suppliers. The hospital spent nearlyhalf of its income on medicines and medical supplies and about 30 percent on

140 Section Two: Applied Experiences in Health Economics and Financing
food. Meals were provided free of charge to patients and to hospital staff whowere involved in direct patient care. Four percent of the budget was assigned tomaintenance.
SESPAS did not allow depreciation allowances for equipment used in itsfacilities. Instead, hospitals were expected to request new or replacementequipment from the secretariat or solicit equipment funds from private sources.
Problems and Alternatives Facing Dr. Estevez
As Dr. Estevez examined a summary of his monthly income statements (seeExhibit 12), he considered what alternatives he had to avoid facing shortages inessential medicines and supplies during the coming weeks. He wondered howmuch additional income he would need or what cost savings could be generatedto keep supplies at the same level after price increases.
One alternative was to continue to purchase medicines and medical suppliesover the short run on credit. Pharmacies and suppliers had proven reluctant tosell to the hospital on other than a cash and carry basis because of the hospital'slarge backlog of accounts payable (see Exhibit 13). Dr. Estevez doubted that hewould be able to procure much more on credit. Even if this were a viablealternative, he felt it would only be a temporary measure, and he turned to therevenue side of his income statement.
To ensure funds for medical supplies, Dr. Estevez could request an increasein his monthly budget allocation from SESPAS. This might be difficult givenSESPAS's own shortage of funds and the administration's view of hospitalefficiency. Dr. Perez Mera had commented:
I see hospitals as sieves which can accept as much money as we pour into them.I give them as much support as I can, but I am pushing them to be more efficientand controlled. At the present time, we do not have a way to evaluate theirperformance. If a hospital wants to justify an increase in its allocations, it mustpresent proof of the legal use of its funds.
To request additional funds, Dr. Estevez felt he would need strong justification,and he was not certain he had the necessary information.
Another option was to begin charging public patients for surgical services. Dr.Estevez could charge for both elective and nonelective operations, but was notcertain on what to base the charge. He knew that many patients were too poorto afford even a small fee, and he was aware of the importance of the hospital'smission to serve patients without discrimination. He also knew that this actionwould mean that the hospital's Social Services Department would have tointerview all surgical patients who claimed they were unable to pay.
Dr. Estevez also considered increasing the charges to private patients whomight be better able to afford the increase, but he was unsure whether this action

Hospital JosA Maria Cabral y BNez 141
would conflict with another plan he had presented to the board of directors inAugust 1983. He wanted to increase the occupancy rate on the private floor,which had always experienced great fluctuations, but since early 1984 had showna steady decline (see Exhibit 7). Dr. Estevez realized he did not know how muchprofit this floor made, because some medicine and supply costs for publicpatients were assigned to this floor. He did know that the floor had contributedbetween RD$ 19,000 and RD$ 51,000 in revenues per month in the past year(see Exhibit 14), but he did not know what attracted paying patients to theJMCB.
A fourth option for Dr. Estevez was to increase the prices of ancillaryservices. While nuclear medicine regularly earned enough money to cover thedirect costs of materials and physicians' fees, the laboratory and radiologydepartments recovered only about half of their direct costs (see Exhibit 15). Hewas aware that the director of radiology based his prices on those charged byprivate clinics, because the cost of materials changed too quickly to calculatecharges independently. Radiology prices at the JMCB were usually about halfthose charged by private clinics. If he were to raise prices for these departments,Dr. Estevez wondered what criteria he should use to establish a new feeschedule. Should the hospital try to recover all direct personnel and materialcosts? Would patients be able to afford such prices?
A final thought was to develop some kind of fund raising campaign througha direct appeal to the Santiago community, or through activities such as a fair.The latter approach had been used successfully by the director of the children'shospital in previous years. Dr. Estevez had never tried such an approach,although the JMCB did have a foundation that included a group of patrons, manyof whom were prominent community leaders.
Dr. Estevez doubted whether income-generating alternatives could provide thefull amount of resources that he would need during the coming months. Helooked at the expense side of his income statement.
Many observers believed that the JMCB was overstaffed, and one alternativeused by private hospitals to reduce costs was to reduce personnel. However,personnel expenses did not even appear in Dr. Estevez's budget. They werecontrolled directly by SESPAS in Santo Domingo. A proposal to reduce staffcould be politically problematic, and reducing staff would not increase Dr.Estevez's resources under the present system unless savings generated by cuts inpersonnel were transferred to Dr. Estevez's hospital budget. This action seemedunlikely in the short term.
Dr. Estevez looked at the line item for medical honoraria, but did not see away to reduce these expenses without also decreasing hospital income. Thehospital charged private patients for the specialty visits made to them by hospitalphysicians while they were hospitalized, and it returned 80 percent of the amountcollected to the physician while retaining 20 percent as income. Although itmight be possible to decrease the percentage share going to the doctors, Dr.

142 Section Two: Applied Experiences in Health Economics and Financing
Estevez was uncertain what effect this would have on the doctor's willingness tosee private patients.
Expenditures such as electricity, maintenance, telephone, water, laundry,cleaning, and supplies averaged about RD$ 45,000 to RD$ 50,000 per month.Underfunding in maintenance had already resulted in disrepair, and a number ofmachines were out of service, but Dr. Estevez felt that perhaps economies of upto 10 percent a month in these categories could be achieved.
The presidential decree affecting medicines would also increase prices forimported foods, but food costs could be reduced by ending the provision of freemeals to hospital service personnel or initiating a joint purchasing system withother Region 11 hospitals. A cost reduction of about 10 percent in the food budgetwould save RD$ 3,000 to RD$ 4,000 per month.
Dr. Estevez thought that another way he could reduce costs was to decreaseinappropriate use of specialized and regional hospitals by dividing Region II intofourteen areas and installing a pediatrician, an internist, a gynecologist, and anurse in medical centers in each of these areas. This approach was being tried inseven areas and the children's hospital had already experienced a 25 percentdecline in outpatient visits. Ms. Ortiz anticipated that the JMCB would soon seesome results, hopefully a 5 to 10 percent reduction in nonemergency visits. Dr.Estevez wondered what actions he could take as either hospital or regionaldirector to improve further the regional referral system. One problem with tryingto determine the appropriateness of outpatient visits and patient admissions wasthe limited availability of data on patient origins and characteristics. Furthermore,the hospital's mission was broadly defined rather than limited to secondary ortertiary care.
Dr. Estevez finally turned to the largest category in his budget, medicines andmedical supplies. Only 25 to 30 percent of the pharmaceutical products thehospital used were produced in the Dominican Republic, and local production ofmedicines also relied heavily on imported raw materials. Cost increases wouldaffect most of the pharmaceutical items that the hospital purchased. Dr. Estevezcontemplated some alternatives to temper these increases.
One possibility was to augment hospital control procedures by instituting anexchange system for supplies. If a doctor requested five syringes, for example,the hospital pharmacy would only issue two, and the doctor would have to returnthe used syringes before being issued more. In this way the hospital could assurethe appropriate use of its supplies.
Another option was to change the procedures for supplying pharmaceuticalsto the floors. The pharmacy currently provided medicines to the floors in bulkto meet the daily needs of all patients. In a new system, the pharmacy wouldrequest a separate prescription for each patient and send only enough to supplyone dose for each patient. Subsequent doses would be supplied upon receipt ofa new prescription signed by the doctor, if the medicine were still available.

Hospital Jose Maria Cabral y Baez 143
Monthly summaries could be compiled to identify the medicines ordered by eachdoctor and permit corroboration with the patient's medical record. Stricter controlson the prescription process might help reduce the flow of free hospital medicines thatwere reportedly being sold outside the hospital.
Dr. Estevez also considered sending the physicians a memorandum that woulddescribe the effects of the crisis and request that physicians prescribe only from a listof about 100 "essential medicines" that were mostly generic products. He was awarethat physicians were influenced by the promotional efforts of the drug manufacturers'representatives and by past training and habits. They tended to demand a wide rangeof more expensive, brand-name drugs. He was not sure how he could enforce thememorandum unless he took a hard line approach and declared an official pharmacypolicy that drug purchases would be strictly limited to the list of essential drugs. Hefeared this approach might alienate some physicians or decrease the quality of patientcare.
The hospital could pressure suppliers for lower prices or to improve theeconomies in the current procurement system. Currently, the hospital pharmacy wasresponsible for purchasing medicines and supplies used by the medical staff forhospital inpatients. The pharmacy manager noted that her department purchased fromboth wholesalers and retailers. Whenever possible, drugs were purchased fromwholesalers to avoid the 30 percent retailer's markup. Wholesalers marked upmedicines 20 to 30 percent above cost. Pharmaceutical supplies generally werepurchased on a monthly basis, in accordance with the monthly flow of income to thehospital. Accounts payable were usually paid after 30 days, although the hospital hadlong-standing accounts payable with several major suppliers.
Recently, the hospital had experienced more difficulty purchasing a sufficientquantity of drugs for its patients. Dr. Pdrez believed that one reason was thatpharmaceutical suppliers needed additional working capital to pay for the higherpriced medicines that would result from the new foreign exchange policy. Lack ofsupply among wholesalers, and perhaps the hospital's backlog on accounts payable,required the pharmacy to purchase medicines more frequently from a wider varietyof sources, including retailers.
One executive in a pharmaceutical company suggested that hospital directors dothe following:
First, the way for hospitals to get better prices is to devise a plan, a system, for theyear ahead to deternine the amount of medicines needed. Then he should contact thesuppliers and arrange a contract for long-term purchases and the timing of payments.If a supplier knows when he will be paid and what quantity the hospital will purchaseover the long term, he can reduce prices. The contract should also include anegotiation to pay off the current debt, with perhaps one-half the monthly paymentgoing towards purchases and one-half towards debt repayment.

144 Section Two: Applied Experiences in Health Economics and Financing
Dr. Estevez was under increasing pressure from several drug companies(including one that was owed more than RD$ 50,000) to negotiate a contract forpayment of long-standing accounts payable. A contract would help the hospitalobtain a more secure supply source, but the hospital would have to predict itsneeds in advance and promise prompt payment.
A last alternative for reducing procurement costs would be to make volumepurchases through SESPAS for the bulk of the public sector's medicine andsupply purchases. Dr. Estevez could lend his support to a plan being consideredby the secretariat to reinstitute a central purchasing office that would ask pharm-aceutical companies to bid on large orders of medical supplies. SESPAS wouldsupply medicines to hospitals with only a 5 percent markup over costs, andsubtract the expenditures from the hospital's monthly budget allocation. Underthe plan, SESPAS would work in cooperation with the influential DominicanMedical Association to establish a list of 150 to 200 essential generic medicinesand limit purchases to these items.
Developing a Plan of Action
Dr. Estevez realized that he had many options available to him, but he feltthat some actions might be beyond his control and might require the power ofSESPAS. His initial brief list seemed to have expanded, and he wondered howhe might prioritize and organize that list. Where should he begin? What actionscould help immediately to ameliorate the impending price increase and whatactions would require a longer timeframe?
He also wondered what additional information he needed to implement futureactions or whether there were other areas that he had not yet considered.

Hospital Jose Maria Cabral y Baez 145
EXHIBIT 1DOMINICAN REPUBLIC AND EIGHT REGIONS OF SESPAS
NIL ~~~~~~~~~ArLANTICMON I I X A r t SJ. N r i C 2~~SAJATIA
ELMIS RD _, OVATE ->
HAITI "s' I - -LA ;A _
IMONg fATA N JIO '
VI V( - - \ AlGA EEAAVLA ---
I .OVOSCO - SX DSEUTTO -AOIr LA SA TAEAOCAa ,
\N~~~~~~~~~~~~~~~~~~~~~~~~A NO.50/ DO
/TJEEEENE/C/A S' I
i-I

0)
0
-1
EXHIBIT 2 >THE SESPAS REGIONAL SYSTEM
Number of m-oPopulation Location Level of care Type of institution institutions S
O
National population National District National level General and 10 O
(Santo Domingo) specialty hospitals 5-
250,000-1 million Regional capital Regional level Regional hospitals 7=
40,000-250,000 Provincial capital Area level Area hospitals 18 0
0
20,000-40,000 Municipalities Local level B Local hospitals 11 C,
3,500-20,000 Municipalities Local level A Subcenters 55 m
1,500-3,00 Rural towns Rural level B Rural clinics 327 )
1,500 Rural towns Rural level A' Heafth promoters 6,000
Source: Memoria SESPAS (1983).

Hospital Jose Maria Cabral y Baez 147
EXHIBIT 3PRINCIPAL CAUSES OF DEATH IN HOSPITALS,
SESPAS REGION II, 1982
No. ofCause cases Percent
Cerebrovascular accidents (stroke) 130 2.6Enteritis and other diarrheal diseases 112 2.3Heart disease 111 2.3Accidents 53 1.1Nutritional deficiencies 45 1.0Diabetes mellitus 40 0.8Homicide 29 0.6Meningitis 27 0.5Arterial hypertension 21 0.4Other causes 4,338 88.4
Total 4,906 100.0
Source: Memoria SESPAS (1983).
EXHIBIT 4PRINCIPLE REASONS FOR SEEKING
AMBULATORY CARE NATIONWIDE, 1983
Cause No. ofcases
Gastroenteritis 10,685Intestinal parasites 9,758Anemia 8,551Bronchitis 7,308Influenza/cold 6,224Heart disease 5,026Gastritis 4,484Amigdalitis 4,426
Source: Memoria SESPAS (1983).

148 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 5PRINCIPAL CAUSES OF MORTALITY, NATIONWIDE, 1982
No. of Rate perCause cases 100,000
Pulmonary disease, circulatoryand other heart disease 1,871 32.1
Intestinal infections 1,355 23.3Perinatal disorders 1,297 22.3Cardiovascular disease 1,236 21.2Myocardial infarction 1,196 20.5Maldefined symptoms, signs, and morbidity 5,713 N/A
Note: These figures should be regarded as estimates because of poor record and classificationsystemsSource: Memoria SESPAS (1983).

Hospital Jose Maria Cabral y Bez 149
EXHIBIT 6OBJECTIVES OF THE SECRETARY OF HEALTH, 1983-86
1. Establish vaccination campaigns to control and/or eradicate polio,diptheria, tetanus, measles, tuberculosis, and scarlet fever.
2. Strengthen malaria eradication services.
3. Develop a national program to control diarrheal diseases throughoral rehydration, provide sanitation education, and increase thepotable water supply.
4. Develop the primary health care system through health promotersand health education.
5. Implement a program to rehabilitate hospitals with the followingcomponents:*Supply basic medicines*Supply basic equiment and instruments*Improve emergency services
6. Improve and expand potable water services and waste disposalservices, especially in rural and marginal urban areas.
7. Provide adequate maintenance for the physical plants and existingequipment of SESPAS's health facilities.
Source: SESPAS (1983).

zn1
0
EXHIBIT 7a-
PATIENT STATISTICS, 1981-April 1984 m
1984Category 1981 1982 1983 January February March April 8
Beds (number) 429 433 433 433 433 433 433 I
Admissions (number) 23,179 23,718 23,339 1,955 1,750 1,828 1,729 5
Patient days 11,663 128,836 129,057 11,221 10,699 11,476 10,204 8Average length of stay (days) 4.8 5.4 5.5 5.7 6.1 7.6 5.9 oOccupancy (percent) 70.7 81.5 81.6 83.6 82.2 85.5 78.5Outpatient visits (number) 122,620 158,858 171,886 13,113 13,029 14,849 10,165Emergency visits (number) 68,817 72,781 73,881 7,325 6,264 7,175 6,197 Q.
Private floor occupancy (percent) N/A N/A N/A 72 70 57 50
N/A: Not available. C
Source: Hospital records.

EXHIBIT 8MONTHLY BUDGET FOR HOSPITAL JOSE MARIA CABRAL Y BAEZ
AND OTHER SELECTED SESPAS HOSPITALS, 1977-83(RD$ thousands)
No. of 1977 1978 1979 1980 1981 1982 1983Hospital beds
Jose Maria Cabral 417 20 20 20 150 150 150 150
Robert Reid Cabral (children's) 315 23 30 30 45 55 55 55
Padre Billini 500 25 25 28 32 40 40 40
Arturo Grullon (children's) 282 18 18 28 40 40 40 40
Luis Aybar 290 25 33 33 45 50 50 50
Ricardo Limardo 235 12 12 15 18 18 18 18_
Exchange rate (Dominican peso/US$) 1.00 1.00 1.00 1.00 1.00 1.00 1.00 o
Source: SESPAS data (1984). 0to0*
0)
w'en.

152 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 9NUMBER OF JMCB PERSONNEL ANDAVERAGE MONTHLY SALARIES, 1984
Total AverageNumber monthly monthlyof active salaries salaries
Department personnel (RD$) (RD$)
Physicians 123 69,052 561Nurses 413 88,575 214Others 747 121,312 162
Total 1,283 278,939 217
Medical residents 99 49,075 495
Total with residents 1,382 328,014 237
Note: Department heads earn RD$ 330 to RD$ 500 per month. The administrator earns RD$500 per month.Source: Hospital records, Personnel Department (1984).
EXHIBIT 10PRIVATE FLOOR CHARGES
(RD$)
Beds per roomCharge Private Two Four
Per diem room and board 25 20 10Per diem per medical specialist 25 20 10Surgical procedure fee 100 80 50Electrocardiogram 15 15 15Chest X-ray 20 20 20
Source: Hospital records.

Hospital Jose Maria Cabral y Biez 153
EXHIBIT 1 1MONTHLY INCOME/EXPENSE STATEMENT, October 1983
Category RD$
IncomeSESPAS 150,000Other (private floor, radiology, laboratory, nuclearmedicine, cafeteria) 63,641
Total revenues 213,641
ExpensesMonthly operating expenses 192,990Physicians honoraria 18,806Salaries to other personnel 3,000
Total expenses 214,796
Surplus (deficit) (1,155)
Details of monthly expensesMedicines/medical supplies 110,263Food 30,752Gas/oil 10,271Electricity 20,000Maintenance contracts 2,375Telephone 525Water 1,600Fumigation 200Oxygen 4,935Paper 4,167Gasoline (vehicles) 1,439Laundry 3,391Cleaning supplies 3,072
Total 192,990
Source: Hospital records.

C,'
co
EXHIBIT 120
(RD$ thousands)Categoy May Jun. Jul. Aug. Sep. Oct. Nov. Dec. Jan. Feb. Mar. A,p-r.
Income
~0
SESPAS 150 150 150 150 150 150 150 150 150 150 150 150 '
Othera 79 55 59 59 62 64 41 49 52 63 48 48Total 229 205 209 209 212 214 191 199 202 213 198 198
CD
a'
Expenditures
=r
Medicines and medical rnsupplies 133 128 124 123 112 110 97 108 111 86 107 111 0
Food 33 34 32 33 32 31 32 38 37 33 36 34 3
Medical honoraria 20 19 20 19 17 19 12 20 16 21 16 16 2In
Other 40 33 49 32 44 52 56 36 39 71 35 40 a.
Total 226 214 225 207 205 212 197 202 203 211 194 201 ~a'
0
Surplus (Deficit) 3 (9) (16) 2 7 2 (6) (3) (1) 2 4 (3) :30
a. Includes Income from private floor and ancillary services.b. Personnel expenditures were not included because salaries were paid directly to personnel from SESPAS's central officeSource: Hospital records.

EXHIBIT 13OUTSTANDING ACCOUNTS PAYABLE
(RD$)
1981 1982 1983 1984Category November August August January February March April
Beginning balance 292,595 785,531 730,399 765,570 774,302 781,553 769,329
Plus purchases 178,277 161,688 152,309 159,798
Subtotal 943,847 935,990 933,862 929,127
Less payments 169,545 154,437 164,533 137,777
Ending balance 774,302 781,553 769,329 791,350 C-
Note: Purchase and payment information was not available for 1981-83.Source: Hospital records.
to
N
c,'

CDa0:
EXHIBIT 14xI,
PRIVATE FLOOR INCOME AND EXPENDITURES, May 1983-April 1984(RD$) _.
Category May Jun. Jul. Aug. Sep. Oct. Nov. Dec. Jan. Feb. Mar. Apr.
Income fromprivate floor 50,911 30,823 40,267 34,688 40,388 32,953 19,006 30,019 31,519 40,491 24,596 31,993 8
Expenditures from 3
private floora 54,438 34,343 37,330 34,200 36,572 33,599 22,065 28,494 33,123 40,114 28,855 32,889 0
a. Expenditures assigned to this floor also incude some medical supplies costs for public patients. Real expenditures for the private floors were difficult to ascertain, but m
were lower than these figures would indicate.Source: Hospital records.

Hospital Josh Maria Cabral y Biez 157
EXHIBIT 15TYPICAL INCOME/EXPENDITURE STATEMENTS
FOR INCOME-GENERATING DEPARTMENTS, October1983
NuclearCategory Radiology medicine Laboratory
Income (RD$) 10,766 2,080 5,713
Expenses (RD$)' 17,822 1,790 12,455
Difference (RD$) (7,056) 290 (6,742)
Number of patients 2,334 126 1,888
Cost per patient (RD$) 7.63 14.21 6.59
Percentage of direct costs recovered 60.0 116.2 45.0
a. Does not include cost of salaries or depreciation of equipment or any overhead. Includes only directexpenses for materials and doctors' fees.Source: Hospital records.
Source Documents
Memoria SESPAS. 1983. Annual Report of the Ministry of Health. SantoDomingo, Dominican Republic.
SESPAS. 1983. "Statement of Objectives of the Secretary of Health, 1983-86."Santo Domingo, Dominican Republic. Unpublished memorandum.

Case 6. The AGAPCO Financial Plan
Study Questions
This case deals with the efficiency and effectiveness of Haiti's pharmaceuticaldelivery system. It extends the examination of production and cost raised in theprevious case and elaborates on demand concepts as well. The tools and conceptsin Mobilizing Resources for Health Services will also be helpful in analyzing thiscase. The problem facing Marie Laurent is to determine whether AGAPCO, aquasi-private enterprise engaged in packaging, distributing and sellingpharmaceuticals to clients of health services provided by the ministry of health,is financially viable.
1. What are the key costs in the budget projections?
2. What are the assumptions underlying the cost projections? Are the costprojections reasonable? Why or why not?
3. Can AGAPCO sell what it projects? What factors will determine salesperformance?
4. What are the capital requirements? Are the estimates reasonable?
5. Should the financial plan be approved? Why or why not?
6. How is the development of financial plans and budgets for AGAPCO similarto or different from the development of those for the ministry of healthprograms?
158

The AGAPCO Financial Plan 159
The AGAPCO Financial Plan
In early 1982 the minister had asked Marie Laurent, special advisor to the ministerof health in Haiti, to review and evaluate the 1983-86 financial plan for AGAPCO.This newly established revolving drug fund constituted a major innovation in Haiti'sefforts to establish a financially viable means of delivering needed drugs to thepopulation. The AGAPCO concept had both ardent supporters and critics, so Marieplanned to scrutinize the various components of the financial plan with extra care.
Revenue Projections
Sales
AGAPCO would wholesale its drugs to community pharmacies, the Ministry ofHealth (MOH), and nongovernmental organizations (NGOs). Exhibit 1 presents salesand cost projections and indicates revenues rising from US$459,000 in 1983 toUS$2,420,000 in 1986. Exhibit 2 presents the projected breakdown of sales betweenthe pharmacies, MOH, and NGOs.'
Community Pharmacies
The community pharmacies were expected to expand from those existing in 1982to 130 by 1985 (see Exhibit 3). AGAPCO would help organize the pharmacies, trainthe clerks, and assist with problems that might arise. AGAPCO would either consignor sell to the community an initial stock of medicines sufficient to start communitypharmacies. The communities in which pharmacies were to be located were responsiblefor covering all the pharmacies' costs. AGAPCO estimated the costs to be US$50 permonth for the clerk. Other costs were expected to be 5 percent of the cost of goods sold.The pharmacies were obligated to sell at the official AGAPCO retail prices, whichallowed an average markup over wholesale of 25 percent. Commercial pharmacies solddrugs in single unit doses, but AGAPCO's community pharmacies would sell the drugsonly in prepackaged course-of-therapy units, that is, the number of single doses neededto cover the full treatment of the illness. The average retail price per course-of-therapyunit was projected at US$0.25. One hundred forty-three private pharmacies operatedin the country, and 114 of them were in Port-au-Prince. About 80 percent of Haiti'sannual US$8 million supply of drugs went through the commercial pharmacies, while20 percent went through the MOH and NGOs.
This case was witen by James E Austin, Harvard Business School, for Management Sciences for Healthwith funding from the Pew Charitable Trust. While the case is based on actual data, all names and someperipheral facts have been disguised. It was prepared for use as a basis for classroom discussion ratherthan to illustrate either effective in ineffectve handling of management or development situabions.
1. The MOH operated 178 clinics and the NGOs operated 159 clinics located in small towns and ruralareas. About 20 percent of the national drug supply went through these two channels.

160 Section Two: Applied Experiences in Health Economics and Financing
Pricing
The wholesale prices of the drugs were based on a markup that would coverAGAPCO's operating costs as well as the replacement cost of the drugs sold.The markups varied by product and supplier. The overall average was 28 percentover the original cost of the drugs purchased for resale by AGAPCO (see Exhibit4). The products to be sold were from the standard list of generic drugs basedon the assessed health needs of the population, rather than from a market studyof actual use or prescriber practices. They were sold only with a prescription.Unlike the commercial pharmacies, AGAPCO would sell no over-the-counter,nonprescription drugs.
Costs
Cost of Goods Sold
The figures used for the cost of goods sold were the cost of replacing thosestocks and are estimated in Exhibit 1. The estimate was calculated as the originalcost of stock purchased, including a projected 5 percent stock loss resulting fromexpiration, damage, or pilferage (see footnote in Exhibit 1) multiplied by theexpected rate of inflation over the period during which the stocks would be in thepipeline.2 The annual inflation rate was estimated at 12 percent and the averagepipeline time was calculated as sixteen months, giving a 16 percent inflation rateover the time the drugs would be in the pipeline.
Personnel Costs
AGAPCO's staff was to increase from twenty-three to thirty-three over thethree-year period. The salary budget amounted to US$87,960 by the third year.The largest single employee category was packers (see Exhibit 5).
Other Operating Costs
Exhibit 6 presents the budget for transportation, packaging, office supplies,telephone, and postage. Utilities and space rental were excluded under theassumption that these services were to be provided free by the Ministry ofHealth.
Capital Requirements and Sources
The capital required to finance AGAPCO's sales over the three-year periodtotaled US$2.46 million and is detailed in Exhibit 7. Exhibit 8 shows that thesources of capital for the project were to come from the Ministry of Health, the
2. The pipeline refers to the amount of time that transpires between the sale of the drugs andtheir replacement by the next shipment, for example, after the collection on invoices, letters ofcredit, order placement, transport, customs clearance, receipt, storage, packaging, and delivery.

The AGAPCO Financial Plan 161
U.S. Agency for International Development (USAID), and the United NationsChildren's Fund (UNICEF).3
As Marie reviewed the different elements of the financial plan, she focusedon three questions:
* Was AGAPCO financially viable?
* What were the key assumptions underlying the budget projections?
* If those assumptions were altered, what affect would they have on thefinancial projections?
3. The source of funds the MOH would draw on would be the proceeds from the local sale offood aid commodities received by the government of Haiti through the PL-480 program, a specialU.S. Agency for International Development program.

162 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 1AGAPCO FINANCIAL PROJECTIONS, 1983-86
(US$)
Category 1983 1984 1985 1986
Sales 458,695 1,264,435 2,123,097 2,419,824- Replacement costa 437,571 1,206,131 2,025,323 2,308,390= Gross margin 21,124 58,304 97,774 111,434-Operating costs 79,102 99,848 105,181 107,246= Surplus (deficit) (57,978) (41,544) (7,407) 4,188
Original cost of drugs sold 358,356 987,780 1,658,670 1,890,492Stock losses 18,861 51,988 87,298 99,500
Original cost ofdrugs purchased 377,217 1,039,768 1,745,968 1,989,992
a Replacement costs equal original cost of drugs, including stock losses, multiplied by the inflation rate.Source: AGAPCO data (1982).
EXHIBIT 2PROJECTED SALES BY OUTLET TYPE, 1983-85
(US$)
Outlet 1983 1984 1985
Pharmacies 290,695 1,058,035 1,917,024MOH 84,000 103,200 103,200NGOs 84,000 103,200 103,200
Total 374,695 1,161,235 2,020,224
Source: AGAPCO data (1982).

The AGAPCO Financial Plan 163
EXHIBIT 3PROJECTED COMMUNITY PHARMACY OPENINGS, 1983-85
Institutional affiliation 1983k 1984 1985 Total
Hospitals 3 3 3 9Health centers 11 15 11 37Health posts 31 25 28 84
Total 45 43 42 130
a. Includes twenty-three outlets in existence in 1982.Source: AGAPCO data (1982).

EXHIBIT 4coWHOLESALE PRICES SUGGESTED BY AGAPCO
Cost Price MarkupName of product Form Unit Source (US$) (US$) (%)
ANAESTHETICS o
1 Ether Bottle 120 cc 120 cc Haiti 2.20 2.42 10
2 Sodium pentathol Ampule 500 mg 500 mg US 2.11 2.50 18 _
3 Lidocaine 2% Vial 50 cc 50 cc US 0.60 1.50 150 8
ANALGESICS
4 Asprin Tablet 350 mg 1,000 Haiti 2.00 3.00 50 ID
5 Codeine phosphate Tablet 30 mg 100 Haiti 8.00 9.00 13 mC)
GASTRO-INTESTINAL DRUGS o0
6 Tincture of Belladonna Bottle Gallon Gallon Haiti 14.00 15.40 10 3
7 Magnesium trisilicate Tablet 500 mg 1,000 Haiti 4.00 6.50 63
8 Mineral oil Bottle Gallon Gallon Haiti 6.10 10.00 64 a
ANTI ALLERGICS0
9 Diphenhydramine Tablet 50 mg 1,000 Haiti 2.00 3.00 50
10 Dimenhydrinate, injection Vial 10 cc 10 cc US 1.10 2.00 82
SEDATIVES
11 Diazepen Ampule 2 cc 12 cc Haiti 0.58 0.64 10
12 Phenobarbitol Tablet 30 mg 1,000 Haiti 2.00 3.00 50

EXHIBIT 4WHOLESALE PRICES SUGGESTED BY AGAPCO
(continued)Cost Price Markup
Name of product Form Unit Source (US$) (US$) (%)
ANTIHELMINTIC
13 Metronidazole Tablet 250 mg 1,000 Haiti 7.39 20.00 171
14 Mebendazole Tablet 100 mg 100 UNICEF 3.90 8.00 105
15 Piperazine, tablets Tablet 500 mg 1,000 UNICEF 3.45 10.00 190
16 Piperazine, syrup Bottle Fallon Gallon Haiti 6.00 8.00 33
ANTITUBERCULOSIS
17 INH, adult Tablet 200 mg 1,000 Haiti 3.00 3.30 1 0
18 INH, child Tablet 100 mg 1,000 Haiti 1.60 1.76 10
19 Thiazina, aduit Tablet 300/15 1,000 Haiti 8.00 8.80 10
20 Thiazina, child Tablet 100/50 1,000 Haiti 3.00 3.30 10
21 Ethambutal Tablet 400 mg 1,000 Haiti 27.00 29.81 1 0 ^-4
22 Streptomycin Vial 5 gm 5 gm Haiti 0.46 0.50 9
ANTIMALARIALS C)
23 Cloroquine, phosphate Tablet 250 mg 1,000 Haiti 10.80 15.00 39 c0
24 Cloroquine, injection Ampule Ampule UNICEF 0.07 1.50 2,043 -n
ANTIBIOTICS
25 Penicillin, tablets Tablet 250 mg 1,000 Haiti 20.00 22.00 10
26 Penicillin, powder for susp. Bottle, 100 cc 100 cc US 1.20 1.50 25
27 Procaine penicillin, injection Vial 10 cc 10 cc Haiti 0.57 .06 11U'

00)
EXHIBIT 4 CaWHiOLESALE PRICES SUGGESTED BY AGAPCOa
(continued)
Cost Price MarkupName of product Form Unit Source (US$) (US$) (%
ANTIBIOTICS (continued) 0.
28 Penicillin in oil, injection Vial 10 cc 10 cc Haiti 0.57 0.63 11
toQ
29 Benzathine penicillin, inj. Vial 10 cc 10 cc Haiti 1.76 2.00 14
C-
30 Sulfamethoxazole Tablet 500 mg 1,000 Haiti 35.00 50.00 43
31 Chloramphenicol, capsule Capsule 350 1,000 Hafti 26.85 29.00 8
I
32 Chloramphenicol, in susp. Bottle Gallon Gallon Haiti 19.85 26.00 31 D
33 Tetracycline Capsule 250 1,000 us 13.50 20.00 48
m
VITAMINS AND MINERALS 0C034 Multivitamins, tablets Tablet 1,000 UNICEF 2.91 6.00 106a
35 Multivitamins, syrup Bottle Gallon Gallon Haiti 8.00 10.00 25
9)
36 Iron sulfate Bottle 300 mg 1,000 UNICEF 1.27 3.00 136 C.
37 Vitamin A
DRUGS FOR RESPIRATORY TRACT
38 Phenylephrine 1 % Bottle Gallon Gallon us 8.80 10.00 14
39 Epinephrine Ampule 1 cc 1 cc us 0.14 0.20 4340 Aminophyllin Vial 10 cc 1,000 Haiti 12.00 15.00 25
41 Cough syrup Bottle Gallon Gallon Haiti 6.30 8.50 35

EXHIBIT 4WHOLESALE PRICES SUGGESTED BY AGAPCO
(continued)Cost Price Markup
Name of product Form Unit Source (US$) (US$) (%)
OPTHALMOLOGICAL PREPARATIONS
42 Silver nitrate Ampule 0.3 cc 0.3 cc Us 0.17 0.19 12
43 Eye ointment Tube 5 gr 5 gr UNICEF 0.11 0.30 173
DERMATOLOGICAL PREPARATIONS
44 Gentian violet Bottle Ounce Ounce US 0.55 0.60 9
45 Benxyl benzacte Bottle Gallon Gallon UNICEF 4.37 10.00 129
46 Calamine lotion Bottle Gallon Gallon US 6.35 9.00 42
CARDIOVASCULAR DRUGS
47 Digitoxin, tablet Tablet 0.1 mg 1,000 US 3.60 4.00 11
48 Digitoxin, injection Ampule 2 cc 2 cc US 0.18 0.30 67
49 Clauden Vial 10 cc 10 cc Haiti 1.00 1.57 57
50 Vitamin K Ampule I cc 1 cc US 0.31 0.41 32
ANTIHYPERTENSIVE DRUGS
51 Resperne, tablet Tablet 0.25 mg 1,000 US 2.90 6.00 107 00
52 Resperne, injection Vial 10 cc 10 cc Us 0.75 0.80 7 n5.
53 Chlorothiazide Tablet 250 mg 1,000 US 26.50 50.00 89
HORMONES
54 Insuline, regular Vial 10 cc 10 cc US 2.09 3.75 79
55 Cortisone Vial 10 cc 10 cc US 1.75 2.00 14-J)

mEXHIBIT 4 i
WHOLESALE PRICES SUGGESTED BY AGAPCO(continued)
Form Unit Source Cost Price MarkupName of product (US$) (US$) (%)
rnOXYTOXICS 856 Ergometrine maleate, tablet Tablet 1,000 US 3.76 4.10 9
57 Ergometrine maleate, inj. Ampule 1 cc 1 cc US 0.12 0.12 0
BLOOD SUBSTITUTES
58 Dextran 70 BoHtle 500 cc 500 cc UNICEF 3.14 5.00 59
ELECTROLYTIC SOLUTIONS
59 Rehydration salts Pouch Pouch Haiti 0.10 .01 10
60 Dextrose 5% Bottle 500 cc 500cc UNICEF 1.08 1.70 57
61 Ringers solutions BoHtle 500 cc 500cc UNICEF 0.88 1.70 93
62 Normal saline BoHtle 500 cc 500 cc Haiti 1.75 1.90 9
63 DLtrs, 10% Rnttle 500 cc 500rc , Haiti 1 as 2 00 l
Source: AGAPCO data (1982).

EXHIBIT 5AGAPCO PERSONNEL PROJECTIONS, 1983-85
Number of staff Cost (US$)Position 1983 1984 1985 1983 1984 1985
Director 1 1 1 9,600 9,600 9,600Assistant director 1 1 1 8,400 8,400 8,400Accountant 1 2 2 5,400 10,800 10,800Secretary 1 1 1 4,800 4,800 4,800Store manager 1 1 1 5,400 5,400 5,400Pharmacist 1 1 1 5,400 5,400 5,400Community development expert 1 1 1 7,200 7,200 7,200Packer 7 14 14 8,400 16,800 16,800Store clerk, central level 2 4 4 2,400 4,800 4,800 -Driver 1 1 1 2,160 2,160 2,160Regional director 3 3 3 9,000 9,000 9,000Store clerk, regional level 3 3 3 3,600 3,600 3,600 o
0
Total 20 30 30 68,160 84,360 84,360 -
Source: AGAPCO data (1982).
e0

170 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 6PROJECTED OPERATING COSTS, AGAPCO, 1983-86
(US$)
Category 1983 1984 1985 1986
Personnel 71,760 87,960 87,960 87,960Transportation/per diem 1,980 2,220 2,490 2,788Packaging and labels 1,162 4,052 7,675 8,596Office supplies and printing 2,400 3,600 4,800 5,376Telphone and telegraph 1,200 1,244 1,500 1,680Postal services 600 672 756 846
Total 79,102 99,748 105,181 107,246
Source: AGAPCO data (1982).

The AGAPCO Financial Plan 171
EXHIBIT 7PROJECTED PIPELINE CAPITAL NEEDED,
AGAPCO, 1983-85(US$)
Sales category 1983 1984 1985
Hospital pharmacies 161,556 181,719 201,615Community pharmacies
Health centers 196,460 300,045 246,345Health posts 138,179 124,725 156,324
Direct SalesMOH 109,480 134,504 134,504NGOs 109,480 134,504 134,504
Total pharmacy 496,195 606,489 604,284Total direct sales 218,960 269,008 269,008Total for all sales 715,155 875,497 873,292
Total for three years 2,463,944
Source: AGAPCO data (1982).
EXHIBIT 8PROJECTED FINANCING SOURCES FOR AGAPCO, 1983-85
(US$)
Organization 1983 1984 1985
MOH (PL-480) 400,000 500,000 500,000USAID 322,000 322,000 323,000UNICEF 0 56,000 56,000
Total 722,000 822,000 879,000
Source: AGAPCO data (1982).

Case 7. After the Election: A Fresh Look atPharmaceutical Supply in Jamaica
Study Questions
The cases "After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica"and "PROSALUD: Marketing and Financing Primary Health Care" provide anopportunity to consider the issues of the appropriate role for government in financingand providing health services. They also allow the reader to assess the advantages anddisadvantages of alternative mechanisms outside the government for providing healthservices and assuring the quality and availability of medical and pharmaceuticalsupplies. The minister of health in Jamaica faces severe deficiencies in thephannaceutical and medical supply system and wishes to consider non-ministry supplyalternatives. The discussions in Section One's "Mobilizing Resources for HealthServices" provide a departure point for analysis. However, the reader will also want torely on concepts and tools provided under many of the other themes.
1. What are the strengths and weaknesses in the Jamaican MOH pharnaceuticalsupply system for selecting and using (prescribing and patient compliance)pharmaceutical products?
2. What are the strengths and weaknesses of the procedures and agencies involved inprocuring, warehousing, and distributing pharmaceutical products for the JamaicanMOH?
3. What features of the BDS and/or ECDS systems for selecting and using drugs havepotential to improve selection and use in the Jamaican MOH? Why?
4. What features used by the BDS and/or ECDS for procuring, warehousing, anddistributing pharmaceutical supplies have potential to improve Jamaica'spharmaceutical supply system? Why?
5. What actions would you recommend that the minister take to improve the MOHpharmaceutical supply system in Jamaica?
6. What recommendations should the minister make to other individuals or institutionswithin the government?
7. How would you prioritize and implement these actions?
172

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 173
After the Election: A Fresh Look at Pharmaceutical Supplyin Jamaica
In November 1989, just after Prime Minister Manley's party had been re-elected after a long absence from power, Jamaica's new minister of healthreceived a consultant's report on the Ministry of Health's (MOH's)pharmaceutical supply system. Although the MOH was plagued by a myriad ofcomplex and related difficulties, the minister was particularly interested in thepharmaceutical and medical supply problems. The MOH budget allocation forthese commodities had been increased from J$ 38 to A$ 56 million during thepast three years.' As the second largest line item after personnel, pharmaceuticalsrepresented roughly 13 percent of the MOH budget, and annual per capita publicsector expenditures were approximately J$ 20. Since many pharmaceuticalproducts were imported, their purchase also required scarce foreign exchange.
In 1986, Island Medical Stores (IMS), the central warehouse for the MOH,provided an estimated 20 percent of the supplies required to accommodatepatients fully. Despite the increased commitment of resources, IMS was stillunable to supply the MOH system adequately. The absence of adequate drug andmedical supplies demoralized MOH personnel and eroded public confidence inthe MOH system.
The problems in the MOH supply system were not only public healthproblems, they had become political problems. The public health system haddeteriorated over the years and was considered to be in an embarrassing state.The population was demanding improvements. The new Minister wanted to findways to correct these deficiencies as quickly as possible, although the newManley government was not unique in its attempt to analyze and improvepharmaceutical supply.
A two-person Canadian consultant team had been selected to review theJamaican pharmaceutical sector because of the consultants' extensive experiencewith public sector pharmaceutical programs in the English-speaking Caribbean.One consultant had been responsible for establishing the Barbados Drug Service,which served both the public and private sectors in Barbados. The otherconsultant had been responsible for establishing the Eastern Caribbean DrugService, an organization that served seven ministries of health in membercountries of the Organization of Eastern Caribbean States. Both theseorganizations had excellent reputations in the region and the minister was
This case was written by Maggie Huff-Rousselle, Social Sectors Development Strategies, Inc., withfunding provided by the World Bank. Case material was obtained from "Assessment of JamaicanPublic Sector Pharmaceutical System" prepared by Maggie Huff-Rousselle and John Tumbull. Thecase is intended for use as the basis for classroom discussion rather than to illustrate either effectiveor ineffective handling of a managerial or development situaton.
1. In November 1989, 1 U.S. Dollar was equivalent to 6.50 Jamaican dollars; in 1986 one U.S.dollar was equivalent to 5.48 Jamaican dollars.

174 Section Two: Applied Experiences in Health Economics and Financing
interested in understanding how the Jamaican Ministry of Health could benefitfrom their experience. See Exhibit 1 for a description of the organizations.
The Jamaican Health Sector
With a population of 2.5 million and an area of 11,000 square kilometers,Jamaica was the most populous and largest of the English-speaking islands in theCaribbean. In terms of socioeconomic development, Jamaica was sliding behindthe other islands. During the previous decade, the government of Jamaica hadbeen operating under severe economic constraints. A declining gross domesticproduct (GDP), an unfavorable trade balance, very high debt servicing, steadydevaluation of the Jamaican dollar, an increasing population with risingexpectations, and International Monetary Fund restrictions put additionalconstraints on health and education programs.
The government's economic difficulties had kept government salaries low incomparison to similar private sector jobs. This situation resulted in a generalexodus from the public service. Remaining managers were often burdened withresponsibilities beyond their capacity. The shortage of nurses was most acute, asit was throughout the English-speaking Caribbean, but vacancy rates were highfor all allied health workers. There were adequate numbers of MOH physicians,but they devoted most of their attention to private practices they had set up tosupplement their MOH incomes. Given the low salaries, poor support systems,and an absence of faith in the potential for change, staff who remained in theservice were demoralized. The situation offered MOH staff little incentive toattempt constructive changes in their own work routines. Absentee rates and staffturnover were high. The attitudinal problems of health system staff contributedto the erosion of public confidence in the MOH system. While the MOH wasable to contract some services to the private sector or take selected positions outof the civil service, International Monetary Fund restrictions and other constraintslimited these and other options.
Health statistics for the English-speaking Caribbean islands reflected atransition from infectious to chronic diseases as the predominant causes ofmorbidity and mortality. Jamaica was no exception. Life expectancy at birth wasapproximately 70 years, and infant mortality was approximately 27 per 1,000 livebirths. The major health problems were chronic degenerative diseases(hypertension, diabetes), traumas (traffic accidents, gun and knife wounds),sexually transmitted diseases, AIDS, teenage pregnancies, substance abuse, andother life-style related problems.
Although Jamaica had moved through a transition to a health care profilemore typical of high-income countries, the infectious and tropical diseasesassociated with poverty and underdevelopment still plagued the 25 percent of thepopulation that hovered at the poverty line. The government's health caredelivery system struggled to provide services that responded to both the diseasesof affluence and the diseases of poverty. Services offered through the MOH,

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 175
often the only source of care for the most disadvantaged groups, were woefullyinadequate.
Despite Jamaica's economic stagnation, the number of health centers haddoubled during the 1970s and the number of general hospital beds had increasedby 20 percent. The MOH primary health care (PHC) system of approximately375 PHC centers was organized and administered geographically according toJamaica's fourteen parishes, with each parish divided into health districts. Therewere five different classes of PHC centers, and the supply link for drugs andmedical supplies was theoretically based on deliveries from IMS to those thatwere parish centers. In practice, because of weaknesses in the delivery system,about one-third of all PHC orders were picked up at IMS by PHC staff. Thetwenty-two secondary and tertiary care hospitals, with three differentclassifications, were organized according to ten regions that did not correspondgeographically to the fourteen parishes. With the exception of UniversityHospital, which functioned as a relatively independent entity, IMS directlysupplied all hospitals regardless of their classification. Sometimes the hospitalscame to IMS for smaller deliveries, but most orders were large and requireddelivery by one of IMS's ten-ton trucks.
Private health care services in Jamaica included six small private hospitals, anunknown number of private physicians' offices, and more than 200 pharmacies.Private hospitals experienced severe financial problems, but the number of patientvisits to private doctors offices, compared to visits to government hospitaloutpatient clinics, was rising. The number of private pharmacies had increasedby 25 to 35 percent during the last few years.
Jamaica's public sector pharmaceutical system included three separatesystems: the University Hospital, the National Family Planning Board (NFPB),and the MOH. University Hospital and the NFPB operated with relativeautonomy, and problems in these two separate systems were minimal in contrastto the MOH system with IMS at its hub. A number of institutions were involvedin the MOH's supply system, and the consultants' report described and assessedthe complex decisionmaking, procedures and processes, organizational incentives,and communication issues that were involved in the interactions between theseinstitutions.
Drug Formulary Process
Under the 1975 Food and Drugs Act, the Office of the Director of PharmacyServices was responsible for registering pharmaceuticals considered acceptableto the government. Registration was usually based on World Health Organizationcertification.
Any product registered in the country could be included in the nationalformulary. The latest edition of the Jamaica National Formulary had beencompiled nearly two years previously with the input of a very large committee.

176 Section Two: Applied Experiences in Health Economics and Financing
It was still not published and had been delayed at the government printer fornearly six months. It was a very open formulary, listing and briefly describingmore than 2,000 items registered in Jamaica. The draft document was the sizeof a New York City telephone directory.
A separate vital, essential and necessary (VEN) list had been compiled for thepublic sector (Exhibit 2 provides definitions of selected technical terms). The listwas developed to restrict the variety of drugs in the MOH system and toconcentrate scarce resources on those drugs that were most critical to providinggood health. There were 219 vital items, 158 essential items, and 147 necessaryitems. Unlike the national formulary, the VEN list did not include additionalinformation on products. It simply listed them by therapeutic category. The VENlist was developed for the MOH, but it had not been widely circulated within theMOH system. Most MOH staff were unaware of its existence, and IMS did notnecessarily adhere to the VEN list when planning its purchases.
Pharmaceutical Procurement
IMS was responsible for planning and placing pharmaceutical purchase orders,but many other organizations were also involved in the process (see Exhibit 3).By law, the Ministry of Finance (MOF) Supply Division acted as the centralpurchasing agency and was responsible for all government local procurement. Italso assisted with some foreign procurement. Drugs and medical suppliesrepresented 26 percent of the value of all goods procured by the MOF SupplyDivision during 1988. The MOF Supply Division charged the MOH a 5.0percent administrative fee for all foreign supply purchases and 2.5 percent forlocal procurements. It added a transportation charge that was 5 percent of actualtransportation costs. All fees reverted to the government's consolidated fund. TheMOF Supply Division's operating budget was based on its anticipated feerevenues, and it always covered its actual operating costs through fee revenues.
The staff vacancy rate in the MOF Supply Division was 40 percent, and itwas at a nascent stage in computerizing its inventory systems. Despite its legalauthority, the Supply Division's role in pharmaceutical procurement had beensignificantly diminished over time. The MOF Supply Division received ordersfrom the MOH Finance Department along with a check to pay for the order andthe associated administrative fees. This process of reviewing the orders andassigning an indent number normally took one month.
The MOF Supply Division also cleared imported goods through customs.Shipments could be delayed in customs for many months, but on average, it tooksix weeks before they reached IMS. Private agents could expedite customsclearance more rapidly than the MOF Supply Division. The cost of wharfcharges, storage, opening containers, and demurrage often exceeded thecomparative cost of contracting out customs clearance to an agent. Delays incustoms shortened the available shelf life of products.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 177
The Jamaica Commodity Trading Company (JCTC) had taken over virtuallyall the activities of the MOF Supply Division related to pharmaceutical imports.The MOF Supply Division retained responsibilities for customs clearance and fortransport from customs to Island Medical Stores. The JCTC procured all MOHforeign purchases and about 17 percent of the private sector' s needs. The JCTCoperated as a private company, but the government owned 100 percent of itsshares. It was one of the most profitable of the government-owned companies,and had paid regular dividends to the government in the past.2
The Pharmaceutical Section was a small part of the JCTC's overall operations.As employees of a private company, the section's staff received significantlyhigher salaries than comparable MOH positions, and the PharmaceuticalDivision's access to computer technology and expertise was excellent comparedwith that of the MOH and the MOF.
The Pharmaceutical Section conducted a restricted international tender (seeExhibit 2), inviting approximately 150 suppliers to bid on 800 to 900 differentdosage forms. The tender invitations listed products by generic name andprovided estimated demand figures for each item. The Tenders Committee usedthe unit prices for individual products quoted by suppliers as one criterion foradjudication. Other criteria for deciding contract awards included preference forbrand names, convenience packaging, promised lead times for delivery, and typeof payment mechanism (letter of credit, sight draft, and so on).
The Tenders Committee was a multidisciplinary group of about ten personsthat included representatives from both the public and private sectors. After thetenders had been adjudicated, eighteen-month contracts for specific items wereawarded to the selected suppliers. Approximately 50 percent of the contractawards were for branded products. Contractual prices were denominated in U.S.dollars, but the duration of the contracts increased the relative risk of fluctuationsin foreign exchange rates for suppliers in Europe and Asia. Suppliers tended toincrease quoted prices to reduce this risk. The JCTC did not publish or makereadily available to individual parties any information on quoted or contractedprices.
During the contract period, the JCTC would place orders for the MOH,University Hospital, the National Family Planning Board, and privateorganizations. For MOH purchases, the JCTC charged a fee of 8 percent on allorders.' It charged private organizations an 8 percent fee for generics and a 4percent fee for brand names because the base price of brand names was typicallymuch higher. These fees generally allowed the JCTC Pharmaceutical Section to
2. As a powerful influence in the Jamaican economy with monopolistic powers over manyimports, the JCTC was criticized for apparent inefficiencies or perverse effects on incomedistribution created by some of its pricing controls and cross-subsidies.
3. Because diabetes was a widespread chronic disease with an expensive therapy, there wasno JCTC fee for insulin in either sector.

178 Section Two: Applied Experiences in Health Economics and Financing
break even financially. Shipments took approximately three months or more toarrive in Jamaica. The JCTC monitored the progress of these shipments untiltheir arrival. Once a shipment arrived in port, the JCTC took no furtherresponsibility for it.4
The JCTC assured quality by screening suppliers before inviting them to bidthrough a public restricted tender. Once awards were made, it monitored theperformance of contracted suppliers by using criteria that ranged from adherenceto English-language labeling and promised delivery lead times to more seriousquality issues related to product efficacy. It also used the Caribbean RegionalDrug Testing Laboratory based in Jamaica to test new products, new suppliers,or suspect products.
The MOH spent more than 50 percent of its pharmaceutical budget throughlocal suppliers, who included roughly thirty wholesalers and six manufacturers.Local manufacturing processes were very simple.5 Because of the low volume ofdemand and limited competition, these processes were not very efficient.Approximately 70 percent of the MOH local purchases came from one localsupplier who was also the most sophisticated manufacturer. The governmentprotected local manufacturers because they contributed to the development of thelocal economy. In general, if a pharmaceutical product was manufactured inJamaica, it could not be imported. Local wholesalers could purchase products notmanufactured in Jamaica from the JCTC or import them directly.
For local procurements, the MOH and IMS made phone calls to select a localsupplier. During the phone calls they arranged the terms of credit and delivery.The suppliers provided transportation to IMS. Suppliers were often willing toprovide the MOH with liberal credit terms and would deliver orders before theyhad received official documents from the MOF Supply Division. Many invoicesfrom local suppliers were not paid for six months, although the MOH generallyreceived the orders within three weeks and, in emergencies, within a few hoursof a phone order.
The MOH Office of Pharmaceutical Services was responsible for checking theaccuracy and appropriateness of the requisitions initiated by IMS from both atechnical and financial perspective. The Office of Pharmaceutical Services couldnot forward an order to either the JCTC or to local suppliers without firstobtaining a check from the MOH Finance Department and then forwarding theorder through the MOF Supply Division. If no cash flow problems occurred, thisprocess took two to three weeks. The process took two to three months whencash flow was a problem, as was frequently the case.
4. In rare cases, such as vaccines for immunizations, the JCTC provided customs clearance.
5. These simple processes were generally limited to forming capsules or tablets from bulkcompounds that had been imported or repackaging other preparations that had been purchased inbulk.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 179
An informal comparison of drug purchase prices in the English-speakingCaribbean indicated that the Jamaican MOH could double its purchasing powerby changing its procurement methods. The costs of locally procuredpharmaceuticals appeared to be particularly high.
Warehouse and Distribution for Pharmaceutical Supplies
IMS operated as the hub of the supply system. It was responsible, directly orindirectly, for inventory management and distribution of pharmaceuticals to 22hospitals, 6 prisons, 4 infirmaries, and the 375 PHC centers in the MOH system.IMS had a smaller vehicle fleet than the National Family Planning Board, and itsoperating budget was 3.3 percent of the total costs of drugs and medical suppliespurchased for the MOH system in 1988.
Frequent stock-outs and shortages had plagued the system for many years.These problems appeared to be increasing with the passage of time. Leakagefrom the supply system through pilferage was a major problem. Improvedsecurity of the physical facilities, particularly at IMS's two warehouses, wasprovided through a project funded by the United States Agency for InternationalDevelopment, but these improvements had little initial impact. IMS staff wereapparently responsible for much of the pilferage. The MOH and IMS removedsuspected staff members, and security at the IMS level apparently improvedsubstantially. How much pilferage continued at the facility level in hospitals andPHC centers was not clear.
Computerized inventory management systems were installed in IMS, but thedata could not be processed or printed at IMS. IMS sent data on disks to theCentral Data Processing Unit. This unit had a backlog of work, and IMSreceived their processed reports several months after diskettes had beensubmitted.
After the delay for processing, IMS would receive reports on inventory levels,quantities of stock issued to facilities, and cost information for total purchases.These data were not completely accurate, and they had never been used to do anABC analysis or a vital, essential and necessary analysis (see Exhibit 2). Therewas no costing information at the facility level, and it was not possible tocalculate costs per patient visit or per service population and make comparisonsacross facilities in the MOH network.
Providers at facilities generally did not have complete information about whatitems were available through IMS, and they had no information about the course-of-therapy costs of items they prescribed or dispensed. Facility staff tended tohoard stock and inflate their order quantities in anticipation of stock-outs orshortages at IMS. No one in the MOH had ever conducted a complete pipelineanalysis of the IMS supply system.

180 Section Two: Applied Experiences in Health Economics and Financing
The vacancy rate for pharmacists was higher than the average 50 percentMOH personnel vacancy rate. Sixty-two of the 152 MOH positions were filled,and only half of the pharmacy posts were filled at University Hospital, IMS, andthe MOH Supply Division. The 200 private pharmacies employed mostpharmacists. Salaries were often twice the standard MOH salary levels. Allninety-five of the pharmacy assistant posts in the MOH were filled, and manyassistants were acting as pharmacists.
Pharmacists received a three-year diploma from the College of Arts, Scienceand Technology, and the college was training adequate numbers of pharmaciststo supply the MOH system. Pharmacy technicians, who filled the assistant posts,received four months of formal training from the MOH and eight months of on-the-job training.
The Use of Pharmaceuticals
Personnel shortages and weak record keeping systems contributed to anabsence of statistics and quantitative data regarding prescribing patterns and druguse within the Jamaican MOH system. It was well known that doctors tended tooverprescribe or "poly-prescribe." Poly-prescribing was a reaction to a lack ofdependable laboratory and other testing techniques that would confirm adiagnosis, but it was also a result of poor diagnostic skills and prescribing habits.Doctors said they prescribed when nothing was needed because they felt thatpatients expected to receive something. They commonly prescribed placebos likeparacetemol and vitamin B. Overprescribing of antibiotics was common andtroubling because it fostered the development of resistant strains of infection,particularly for sexually transmitted diseases, which were among the top tencommunicable diseases in most areas of Jamaica.
Doctors in Jamaica also prescribed expensive brand names because they didnot know the generic equivalents or were dubious about their quality. Doctorsreceived little information about the drugs that were available through the MOH.Their main source of current drug information was the pharmaceutical industry.This information came in the form of brochures and samples, but primarily fromthe "detail men" who paid personal visits, usually to doctor's private offices.
Less was known about patient compliance than about prescribing habits, butample anecdotal evidence indicated that patient compliance was poor. Compliancewas considered to be particularly poor among patients requiring treatment forchronic diseases that did not manifest painful symptoms (hypertension, diabetes).These diseases were the major causes of morbidity and mortality throughout theEnglish-speaking Caribbean.
Financing Pharmaceutical Supply
Pharmaceuticals were the major target for increasing user fees in the healthsector. A recent study reported that the collection of user fees had increased in

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 181
a number of hospitals after the government had reinterpreted the law regarding theiruse. Policies based on this reinterpretation allowed facilities to claim part or all of thefees they collected rather than returning them to the central treasury, as was previouslythe case. Some MOH officials believed that this change would boost the motivation forfacility staff to enforce user fee policies.
The charges for drugs in the MOH were much lower than the MOH's costs, and feeswere collected only in hospital outpatient clinics. Patients with chronic conditions(diabetes, hypertension, arthritis, mental patients) paid an annual prescription fee ofJ$5. The charge for others was J$5 per item on a prescription slip. Charges were thesame for privately insured patients and physicians' private patients. MOH physicianswith private practices also had relatively easy access to MOH pharmaceuticals. Manycategories of patients and/or drugs were exempt from charges, for example, familyplanning, immunizations, food aid recipients, women with high risk pregnancies, anddental treatments for children. The total amount of user fees collected by the MOHcovered 1.5 percent of the MOH's total costs, and about 20 percent of the total feeswere earned from prescriptions.
Most Jamaicans filled their prescriptions in the private sector. Private supplierspreferred to cany brand name products. In addition to the JCTC's import fees, they paida 15 percent customs duty, a 5 percent consumption tax, and a 2 percent handlingcharge that the MOH was not required to pay. For most pharmaceutical products, retailprices were controlled. Wholesalers could charge a maximum of 20 percent for ethicalproducts, and retailers could charge an additional 30 percent. Over-the-counterproducts carried a maximum wholesaler margin of 20 percent, and the retail marginwas set at 25 percent. Retailers charged a "professional fee" or dispensing fee of J$4per item.
Pharmaceuticals were a popular target for the introduction of user fees into publichealth systems, not only in Jamaica, but throughout the developing world. Accordingto numerous household expenditure surveys on health, pharmaceuticals represented alarge portion (25 to 50 percent) of household expenditures. This provided credence toeconomists' belief that people were willing and able to pay for pharmaceuticals. Manyhealth professionals believed that the practice of charging for drugs was apt to increasepatient compliance, because patients would value their prescriptions more if they hadpaid for them.
The Social Sectors Development Project, a World Bank-funded loan to Jamaica,included a budget of approximately US$15 million for the procurement ofpharmaceuticals. The expectation was that these funds would be used as a capitalinvestment to top up the stock levels in the MOH system, help the MOH and IMS tomove out of a crisis management mode, and implement good procurement planning andinventory control techniques. The new minister was concerned that these loan fundswould be spent on pharmaceuticals, but that within two or three years IMS and theMOH would be back in the same situation.
The new minister had been in office for only a few months. From his businessbackground he knew that there were many ways in which private sector management

182 Section Two: Applied Experiences in Health Economics and Financing
techniques could improve the MOH's performance. At the same time, he was aware thathe had to deal with constraints that were less apparent or did not exist in the privatesector. The MOH's mandate was to increase equity and access to health care, and thisconstraint was not one that the minister wished to change. However, he felt that thehealth delivery system was inhibited by the machinery of government, ranging fromredundant procedures and regulations to public service salary limitations.
Some of these constraints were factors that he might be able to change, others werenot. The lack of financial resources was a major impediment, and motivating thedemoralized staff was perhaps a greater challenge. He had to decide which problemsto address, in what sequence, and how to attack them.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 183
EXHIBIT 1THE BARBADOS DRUG SERVICE AND
THE EASTERN CARIBBEAN DRUG SERVICE
The Barbados Drug Service (BDS) operated in both the public and private sectors ofBarbados. The Eastern Caribbean Drug Service (ECDS) served member states of theOrganisation of Eastern Caribbean States through participating MOHs. In 1989, the islandsserved by ECDS included the British Virgin Islands, Dominica, Grenada, Montserrat, St.Kitts, St. Lucia, and St. Vincent. The combined population of these island nations wasroughly 500,000. The population of Barbados, a single island, was 350,000. Average publicsector per capita pharmaceutical expenditure in the Organisation of Eastern CaribbeanStates' countries was J$24, and in Barbados it was J$145.'
Per capita expenditure in Dominica, one of the islands served by ECDS, was the lowest inthe Eastern Caribbean region. The Dominican MOH was very cost conscious about howit used its scarce health dollars. It had an extremely restricted formulary list. For example,symptomatic treatments such as cough syrups were not purchased by the MOH. Drugswere budgeted for at the individual facility level, and cost accounting systems were usedto charge the facilities and monitor their performance against the budget. Periodic ABCanalyses (see Exhibit 2) were done of drug expenditures by facility and for the system asa whole. These analyses identified major discrepancies in use patterns or per patientexpenditure. The MOH did not allow MOH physicians to use MOH pharmaceuticals in theirprivate practices, nor could patients obtain pharmaceuticals from the MOH without an MOHprescription. A list of the course-of-therapy costs of each item carried by the MOH wasfrequently up-dated and circulated to prescribers in all MOH facilities. Dominica purchasedpharmaceuticals through the ECDS, which generally had lower prices than the BDS or theJCTC. The Dominica pharmaceutical supply system generally had a shorter pipeline, lowerstock-out rates, and higher service levels than any of the other English-speaking Caribbeancountries.
Selection and Drug Formularies
Both the BDS and the ECDS published formularies annually. Their formulary committeeswere relatively small and stable in membership, but they consulted noncommitteemembers who had recognized expertise in specific areas. The committees reviewed andrevised the formulary list by adding and deleting a few items each year. This processensured that information was technically current and accurate, and it kept influentialindividuals in the medical community engaged and committed to the formulary.
The published manuals were small enough to fit in a prescriber's shirt pocket, but theycontained all the key reference information needed to inform prescribing choices: genericname (and common brand names), indications, contraindications, precautions, adversereactions, drug interactions, use during pregnancy and lactation, advice to give to thepatient on how and when to take, dosage, and so on.
Both the BDS and the ECDS formularies had a number of comprehensive indexes,including all the commonly used brand names in the Caribbean cross-referenced togeneric names. This feature was particularly important, because most prescribers onlyknew pharmaceuticals by their common brand names. The ECDS manual also includedbar charts that compared the cost of therapy for alternative therapies listed in theformulary (for example, daily cost of analgesic or antipyretic agents); and other
1. Organization of Eastem Carribean States costs include the 15 percent ECDS service charge.

184 Section Two: Applied Experiences in Health Economics and Financing
prescribing information (for example, the efficacy of selected anthelminthic preparationson specific worm infestations).
The ECDS formulary contained just over 300 items. The BDS formulary contained morethan 500 items, but Barbados had a teaching hospital and per capita expenditure onpharmaceuticals was six times that of the countries served by the ECDS. Both the BDSand the ECDS formulary manuals werewidely distributed throughout the EasternCaribbean, and neither agency purchased anything that was not on its formulary.
Pharmaceutical Procurement
The core services offered by the BDS and the ECDS were very similar to the services theJamaican Commodity Trading Company (JCTC) provided to the Jamaican MOH. TheECDS charged participating MOHs 1 5 percent of the value of drug orders as anadministrative fee that would cover its own operating costs. The BDS was a departmentof the Barbados MOH, and there were no service charges. Its own operating costs werejust under 20 percent of Barbados' total drug costs.
Both the BDS and the ECDS operated twelve-month restricted tendering-contractingcycles, and both invited approximately 100 suppliers to bid. The ECDS did not publishor make its quoted or contracted prices readily available to interested parties, but theBDS did. The BDS also guaranteed suppliers minimum quantities, while the ECDS onlygave an indication of estimated quantities in the tender solicitations. Branded productsreceived 75 percent of the BDS's awards and 25 percent of the ECDS's awards. Brandnames were often two or three times the cost of generic equivalents. Both the BDS andthe ECDS guaranteed suppliers prompt payment in foreign exchange within roughly sixweeks of delivery.
The BDS had a 100 percent market share of Barbados' public sector. The ECDS hadroughly 85 percent of the public sector markets in the seven countries it served.Through a sole source commitment developed by the ministers of health, the MOHscould not purchase brand name or generic equivalents of any products contracted by theECDS.
A 1988 study compared procurement prices obtained by BDS, ECDS, and JCTC for asmall sample of drugs that were high demand items (antibiotics, and treatments forhypertension and diabetes).2 Cost insurance and freight (CIF) prices for the ECDS weregenerally lower than for either the BDS or the JCTC even given the low volume of demandand high transportation costs in the small Eastern Caribbean islands.3 This comparisonincluded the ECDS's 15 percent administrative fee, but not the JCTC's 8 percent fee or theBDS's operating costs. The sample was too small to draw firm conclusions, but it raisedquestions about pharmaceutical procurement practices in both Barbados and Jamaica.
2. Huff-Rousselle, Maggie. 1988. 'Public Tendering for Pharmaceuticals in the English-Speaking Caribbean: Barbados, Jamaica, and the OECS Countries." Paper presented at the Pan-American Health Organization Essential Drugs Policy Programme Seminar for the Government ofTrinidad, Port-of-Spain, Trinidad.
3. The participating islands had a population of less than 500,000 and suppliers had to shipdirectly to each country. For a country as small as Montserrat, with a population of 12,000, thisoften meant that transportation costs exceeded manufacturing production costs for the smallvolume of pharmaceuticals.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 185
Warehouse and Distribution Systems
Neither the BDS nor the ECDS did any warehousing. The BDS paid local suppliers anadditional 32 percent over CIF prices to provide this service to the MOH. Barbados is asmall, flat island with good transportation systems, and suppliers were contracted by theBDS to maintain sufficient reserve stocks and to deliver directly to MOH facilities whenthe BDS placed an order with them. This system was working smoothly in Barbados.
In the Organisation of Eastern Caribbean States' countries, pharmaceutical shipmentsordered through the ECDS were delivered directly to the central medical stores of theMOHs in each island. The costs of warehousing and distribution were borne by theindividual MOHs.
Although the project that had established the ECDS had made substantial contributionsto the MOH formulary and procurement processes, the warehousing and distributionsystems had changed little. Under the project, computers and inventory control programshad been installed in the central medical stores, but the programs were either notfunctioning properly or managers were not using data to plan procurement anddistribution. The central medical stores had encountered technical problems, such asinadequate documentation for the software, but the lack of employee motivation to usethe programs was a greater deterrent to progress.
Neither the Barbados MOH nor the MOHs served by the ECDS had personnel problemsas severe as those in Jamaica's MOH.
Use of Pharmaceuticals
The BDS and the ECDS assured quality through preventive strategies. Both agenciesscreened suppliers before inviting them to bid through the restricted public tender.Screening was a major advantage to a restricted tendering system because it providedquality assurance by eliminating substandard suppliers and reduced the volume ofinformation presented to the adjudication committee. The two services also monitoredcontracted suppliers' performance, using criteria ranging from adherence to English-language labeling and promised delivery lead times to more serious quality issues relatedto the efficacy of the products. Both agencies used the Caribbean Regional Drug TestingLaboratory based in Jamaica to test new products, new suppliers, or suspect products.
The BDS and the ECDS attempted to improve physicians' prescribing habits through drugnews letters or occasional seminars, but their major vehicle for disseminating informationthat might improve prescribing habits was widespread distribution of the publishedformularies. None of the island nations had dependable data on prescribing patterns.
Patient compliance was suspected to be poor in Barbados and the islands served by theECDS. Given the high incidence of hypertension and diabetes, this was a critical publichealth problem for all the island nations. Although patient compliance was a topic ofconcern at numerous meetings for health professionals, actions that improved healtheducation or promotion in this area were very limited throughout the English-speakingCaribbean.
Financing Pharmaceutical Supply
Under Barbados' Special Benefits Service, the MOH reimbursed the private sectorpharmacies for the cost plus a profit margin on BDS formulary drugs. The identicalproducts (same brand, same package) were available free of charge through the MOH,where they only cost the government the base price, excluding the private sector profitmargin. Initially the Special Benefit Service had included a copayment in the private

186 Section Two: Applied Experiences in Health Economics and Financing
pharmacies. When the copayment was eliminated, the cost of pharmaceutical supply forthe MOH in Barbados doubled during a three-year period.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 187
EXHIBIT 2DEFINITIONS OF TECHNICAL TERMS
ABC Analysis
An ABC analysis is a technique used in pharmaceutical supply management to identifythose products that, either because of volume of use or because of unit costs (or both),represent the largest share of the costs for all drug products in a supply system.
The quantity of each product procured during a given period is multiplied by theproduct's price to calculate each product's significance in terms of total costs. Productsare then ranked in terms of total costs. As a rule of thumb, the top 20 percent of theproducts, the "A Class" items, normally account for approximately 80 percent of totalinventory investment. If managers focus attention on better management of the A Classitems, they are apt to show a greater impact on the whole system than they would ifthey focused on the whole system.
Pipeline Analysis
A pharmaceutical pipeline analysis estimates the average amount of time (in months)that elapses between the point when an order is placed for pharmaceuticals and thepoint at which drugs from tCat order are dispensed to patients. The length of the pipelinecan be influenced by a number of factors: slowdowns in the procurement process,transportation difficulties in delivering goods to a country, the time required to clearcustoms, the number of levels in the delivery system, and the average safety stock ateach level of the system.
The length of the pipeline provides some indication of the required capital investment tofill the pipeline without any bubbles or stock-outs. It also provides an indication of thelikely risk of expiration and spoilage, given the average length of time that a product willtake to move through the complete pipeline. A pipeline analysis can identify pointswhere the length of the pipeline can be reduced, thus reducing the capital investmentand the potential for wastage through expiration or leakage.
Restricted Tender
In a restricted tender, suppliers bid against each other for the contract, but participationis limited to those suppliers who have registered with the agency inviting the tender.Usually these suppliers have met established prerequisites. This screening process,followed by invitations to bid addressed only to suppliers who have passed thescreening, distinguishes a restricted public tendering process from an open publictendering process.
The effect of a restricted tender on price is generally favorable, although not asfavorable as an open tender might be. However, a restricted tender both reduces theworkload associated with processing and adjudicating bids and provides good preventivequality assurance by screening out questionable suppliers. It is particularly valuable forproducts where bioequivalence, sterility, and precise formulation are important, or forlarge volume, standard items when reliable suppliers are known.
Vital Essential Necessary (VEN) Analysis
A VEN analysis is a technique used in pharmaceutical supply management to identifythose products that are considered vital, essential, and necessary. (The necessarycategory is sometimes known as nonessential, and includes items such as cough syrups

188 Section Two: Applied Experiences in Health Economics and Financing
and most vitamins.) An expert committee can discuss and assign drug products to oneof the three categories, based on the dominant health problems and the relevance ofeach product to those problems. A life saving drug may not, for example, be classifiedas vital if the disease it treats is rare or unheard of in the area being served by a healthcare system.
When combined with an ABC analysis, a VEN analysis can be useful in highlighting areaswhere funds are being allocated for the purchase of products that are neither vital noressential. If, for example, these are a number of necessary category products that arealso A class in an ABC analysis, this would indicate wastage of resources and poorprescribing habits.
The Drug Supply Cycle
SaLEcrioN
4 2
USE PROCUREE/ T
Note: For a more expansive discussion of these and other technical terms, see Management Sciencesfor Health, Inc. 1982. Managing Drug Supply.

After the Election: A Fresh Look at Pharmaceutical Supply in Jamaica 189
EXHIBIT 3MINISTRY OF HEALTH DRUG SUPPLY SYSTEM
INTERNATIONAL LOCAL SUPPLIERSSUPPLIERS (approximately 30)
(approximately 150) andMANUFACTURERS(approximately 6)
JAMAICACOMMODITY
TRADINGCOMPANY
MINISTRY OFFINANCE
SUPPLY DIVISION
MINISTRY OFHEALTH
FINANCEDEPARTMENT
ISLANDMEDICALSTORES
REGIONALHOSPITALS
(approximately 22)
PRISONS (6),HOSPITALS (4),
andOTHER
MINISTRIES PHC CENTERSTYPE IV and V
(approximately 30)
PHC CENTERSTYPE 1, 11 and III
Source: Huff-Rouselle, M., and J. Turnbull. 1989."Assessment of the Jamaican Public Sector PharmaceuticalSystem." Unpublished report.

Case 8. PROSALUD: Marketing andFinancing Primary Health Care
Study Questions
The PROSALUD case extends the previous case's assessment of alternativemechanisms to delivering and financing basic health services to low incomegroups. Carlos Cuellar of PROSALUD must assess what factors and conditionshave been essential to the success of PROSALUD, whether these can bereplicated in another setting, and how expansion is likely to contribute to long-term financial sustainability. The reader will want to rely on concepts and toolsdiscussed under many of the other themes.
1. What are the characteristics of the market for health services in Bolivia? InSanta Cruz?
2. What factors or market forces worked in favor of the development ofPROSALUD?
3. What factors or forces presented obstacles for PROSALUD'!
4. What characteristics differentiate PROSALUD from other available healthservices?
5. What advantages and disadvantages are there for collaboration betweenPROSALUD and the MOH? PROSALUD and the private sector'?
6. Is it possible to expand or replicate PROSALUD in other areas of Bolivia?Why or why not?
7. What conclusions do you draw for the potential of PROSALUD-typeendeavors beyond Bolivia?
190

PROSALUD: Marketing and Financing Primary Health Care 191
PROSALUD: Marketing and Financing Primary Health Care
Toward the end of 1989 Carlos Cuellar, the director of PROSALUD, receiveda draft copy of the final evaluation report on the Bolivia Self-Financing PrimaryHealth Care Project. This was the project, now six years old, supported by the U.S.Agency for International Development (USAID) under which PROSALUD had beenestablished with technical assistance from Management Sciences for Health. Theproject intended to improve the health status of semi-urban and low-income ruralworkers and their families in selected areas of the Department of Santa Cruz, Boliviaand to become financially self-sufficient.
Dr. Cuellar had been working with PROSALUD since it was established,although he had not been the director during the early years. He was a doctor in hismid-thirties, and his energy and enthusiasm were contagious. He had previouslymanaged a rural service for the Bolivian government, and the service had becomefinancially self-sufficient based on revenues generated through user fees.
At the time, PROSALUD operated thirteen primary health care (PHC) centers(see Exhibit 1), and fifteen were to be opened under the PROSALUD system by theend of 1989. By the third quarter of 1989, the existing PHC centers had achieved anaverage self-financing level of 87 percent, but costs of the Management Services Unit(MSU) were not included in this self-sufficiency calculation (see Exhibit 2).PROSALUD estimated that it was providing services to approximately 125,000people in the Santa Cruz area.
Carlos considered the evolution of PROSALUD over the past years, and the manyturns along a road that were never mapped out in the original project design. Thelengthy evaluation report contained no surprises for him and it was effusive in itspraise of PROSALUD's accomplishments. The evaluation report called for furtherexpansion of the PROSALUD system in the Santa Cruz area, replication of thePROSALUD model in other parts of Bolivia, and an annual external funding ofUS$80,000 and US$90,000 to support these activities.Carlos realized that the futurecourse of PROSALUD might provide even more complex choices for theorganization than those it had confronted at past junctures.
Bolivian Health Sector
Approximately 30 percent of the 6.5 million Bolivians did not have access tomodern health care. The Ministry of Social Welfare and Public Health (MPSSP),
This case was written by Maggie Huff-Rousselle and Catherine A. Overholt with funding provided by theEconomic Development Inslitute of the Worid Bank through John Snow, Inc., Initiatives, Inc., and CARICANInitiatves, Inc. Case material was obtained from documents and reports on the Bolivia Self-FinancingPrimary Health Care Project, as well as from conversations with Carios Cuellar, John Fiedler, PaulHartenberger, Rafael Indaburu, Patricia Moser, and Pamela Putney. The case was preapred as a basis forclassroom discussion rather than to illustrate either effectve or ineffective handling or managerial ordevelopment situatons.

192 Section Two: Applied Experiences in Health Economics and Financing
although officially charged with providing services to 80 percent of the Bolivianpopulation, was providing coverage to an estimated 38 percent. The socialsecurity system was estimated to be providing coverage for 26 percent at anannual per capita cost of US$36; the private sector covered approximately 5percent; and other organizations provided coverage to 1 percent.
Prior to the severe and prolonged economic crisis of the 1980s, the NationalTreasury (TGN) had provided approximately 90 percent of health sector fundingin Bolivia. However, from 1980 to 1987, the MPSSP's share of that funding hadshrunk from 4.5 percent to 2.0 percent. MPSSP expenditures declined fromUS$37 million to less than US$17 million. Funding for the MPSSP had shiftedincreasingly toward reliance on user fees. Exhibit 3 provides detail onexpenditures and sources of funding.
MPSSP expenditures were allocated toward central-level activities and thehospital sector. Between 1984 and 1989, central headquarters expenditures hadincreased by nearly 300 percent, while regional office budgets grew by 17percent. Hospitals accounted for approximately 75 percent of the MPSSPexpenditures, although occupancy rates were generally less than 50 percent.MPSSP salaries had fallen in real terms by 43 percent between 1984 and 1988.The turnover rate averaged 30 percent, absenteeism and tardiness were majorproblems, and most staff now worked six- rather than eight-hour days.
Santa Cruz Health Sector
Santa Cruz had been a growing metropolitan area for nearly twenty years,sustaining an immigration rate of 10 percent for more than a decade. Theestimated population of the Department of Santa Cruz in 1988 was approximately1I.1 million. Roughly half of the residents lived in the department's urban areas.Education and income levels in Santa Cruz were higher than in the rest of Bolivia(see Exhibit 4). The formal business sector was growing rapidly.
The trend toward user fees in the Santa Cruz health sector was even morepronounced. The MPSSP's Santa Cruz Regional Health Unit received 48 percentof its total income from user fees in 1987 and 57 percent in 1988 (see Exhibit 5).Private sector health care in Santa Cruz grew from 35 to 40 percent between1984 and 1988.
Evolution of PROSALUD
The Self-Financing Primary Health Care Project, as designed and approvedin mid-1983, was intended to serve the members of three cooperatives in SantaCruz on the basis of a prepayment scheme. The absence of marketing studies,other planning techniques, and preliminary organizational work with the threecooperatives led to the collapse of the original agreement in 1985.

PROSALUD: Marketing and Financing Primary Health Care 193
The MSU, originally intended to operate through one of the cooperatives,became an independent legal entity, PROSALUD, in August 1985. PROSALUDwas able to establish its first six clinics during 1986 by working enthusiasticallywith the communities and other institutions to generate interest in and support forPROSALUD clinics.
PROSALUD based its method for selecting a site on seven criteria: (1)population size, (2) geographic accessibility, (3) absence of other health services,(4) existing physical and human health resources, (5) community organization,(6) financial capacity, and (7) possibilities for expansion.
In addition to these criteria, the guidelines for selecting a site identified thetypes of people and institutions with whom PROSALUD staff should confer.According to PROSALUD's director,
Nothing can substitute for learning about and taking into account the psychologyof the people and the sociology of the community. . . The different medical needsof different neighborhoods or different communities are simply technical issues.They are not as difficult as the social questions . . . figuring out how to gain theconfidence of the people. The trick is to learn what motivates people, what turnsthem on . . . You have to gain people's faith, and faith is believing in somethingyou can't see.
PROSALUD reached another critical juncture when it developed a marketanalysis model in early 1987 and tested it during the following year. This modelput into place basic elements of the PROSALUD system as it existed in late1989. It helped PROSALUD to reduce costs in both the centers and the MSU(see Exhibit 6), and to assess better the financial viability of operating centerswithin specific communities. Exhibit 7 contains market survey results oncommunities served by PROSALUD.
According to PROSALUD market studies, approximately one-third of thepopulation of Santa Cruz was not served by the government health care system.PROSALUD estimated that its market share of clinics in communities it servedwas less than 40 percent.
In June 1987, the MPSSP offered PROSALUD the opportunity to administerthe rural primary health care facility in El Paurito, near Santa Cruz.Demographic and economic data were gathered and analyzed. Using its marketmodel, PROSALUD estimated that the El Paurito center would recover less than50 percent of its costs during its second and third years of operation. The offerwas rejected.
Structure and Staffing
The PROSALUD service delivery developed into a three-tiered system. Itbegan with Level 1, which consisted of health promoters. PROSALUD hadselected 160 persons from their communities and trained them between 1985 and

194 Section Two: Applied Experiences in Health Economics and Financing
1989. Three Level II facilities, basically sanitary posts, were staffed by afull-time auxiliary nurse. These evolved into feeder posts for the Level IIIfacilities. The ten Level III facilities (with two more planned prior to the end of1989) were placed in both urban and rural areas. By late 1989, approximatelythirty-five of these health promoters remained actively in the system, working outof the Level III facilities and successfully promoting each center's services.Incentive schemes had been developed to retain and motivate the healthpromoters.
For urban centers, full-time staff included a medical director/physician, agraduate nurse, two nurse auxiliaries, and one dentist; part-time staff included alaboratory technician, an obstetrician/gynecologist, and a pediatrician. In therural centers the specialty services (dentistry, pediatrics, and obstet-rics/gynecology) were not available.
Exhibit 8 gives personnel costs for the clinics operating during 1988. A majorfocus of the cost reduction activities that resulted from the development of themarket analysis model was on the elimination and/or redesignation of staffpositions. Night watchmen, for example, were replaced by auxiliary nurses,allowing the provision of twenty-four hour services. Laboratory technicians wereshared between clinics and serviced private physicians during slack periods.Productive staff members were assigned to new clinics where they could establishPROSALUD's work ethic with new staff. By the end of 1989, PROSALUDhealth teams were approaching a maximum level of efficiency, but patientvolume could still be increased at the current staffing levels. At the same time,an internal project review earlier in the year called for increasing the quality ofcare through peer review systems, in-service education, and efforts to reducepoly-prescribing practices. PROSALUD had been prompt in responding to thefindings of this internal evaluation.
An employee incentive system was introduced in July 1988. Employeesreceived a base salary, and in addition they received a bonus based on increasesin the center's revenues. Revenues collected in cost centers, excludingpharmacies, were used to evaluate a center's performance. The first and lastquarters of the previous year's revenues for a clinic were averaged, and therevenues in a current period were compared to this benchmark. Thirty percentof the earned revenues that exceeded this benchmark were returned to thecenter's staff as an incentive. Of this 30 percent, 30 percent went to the full-timephysician, and the remaining 70 percent was divided among the rest of the staffin direct proportion to the share their salary represented in the center's total basesalary costs. Generally this incentive plan represented approximately 10 percentof the staff's salary. PROSALUD paid its nonspecialist physicians, all of whomwere former MPSSP employees, approximately 25 percent more than theMPSSP, although private physicians could earn considerably more.
In the case of new facilities, 10 percent of the income from medicalconsultations was paid to the physician for the first six months. This six-month

PROSALUD: Marketing and Financing Primary Health Care 195
period was then used as the initial benchmark to move to the standard incentivescheme.
Medical specialists did not receive salaries from PROSALUD, but worked ona fee-sharing basis. Pediatricians and gynecologists received half of the fees theygenerated, while dentists, who were responsible for providing their own materialsand equipment, received 80 percent of the fees they generated.
Pharmaceutical Products
PROSALUD carried 134 essential drugs that were procured up to four timesa year from twenty suppliers in Bolivia. In 1987 PROSALUD realized thatpharmacy services represented more than 28 percent of revenues generated, butthe costs of delivering these services were greater. PROSALUD's pricing policyfor pharmaceuticals was a mark-up of 15 to 25 percent over wholesale cost.Private sector establishments charged a 50 percent mark-up. PROSALUDreduced its average medication cost per consultation at each clinic between 1987and 1988. Pharmacies became net revenue generators and accounted for nearly35 percent of total system revenues. Poly-prescribing practices still existed insome clinics (see Exhibit 9).
Services
PROSALUD provided a range of preventive and curative services (see Exhibit10). These services were used to categorize indicators for each center thatallowed PROSALUD to monitor and evaluate performance.
Dentistry had recently been added at the request of the communities. Familyplanning services, normally subject to political and religious resistance in Bolivia,were also added at some risk to PROSALUD's image within Santa Cruz. Theevaluation report called for the expansion of family planning activities, as wellas further efforts in nutrition education and the introduction of a breastfeedingpromotion program.
Most preventive services were provided free of charge, and approximately 8percent of patients were provided with free care for all services. Exhibit 10shows trends in the level and mix of services provided by PROSALUD.
Financing
The initial source of funding for PROSALUD was the USAID grant providedunder the terms of Bolivia Self-Financing Primary Health Care Project. Overtime, grant support was reduced in line with the system's ability to cover someof its own costs through revenue generation. In late 1989, 20 percent of theMSU's costs were allocated to the clinics, prorated on the basis of the total costsof each clinic. Other MSU costs, including marketing, training, and clinic deficitswere covered by the USAID grant, additional smaller grants, and the

196 Section Two: Applied Experiences in Health Economics and Financing
income-generating consulting and research activities of PROSALUD staff. Ingeneral, the MSU had been able to maintain its costs at close to the 1988 level (seeExhibit 6).
The buildings in which PROSALUD clinics were based and the operating costsof the buildings were contributed by the communities or other organizations (seeExhibit 2).
We say our clinics, but they're not PROSALUD's. They belong to the communities.Community ownership is important. People will take pride in their responsibility forthe destiny of the clinics.
In the Cotoca facility, the MPSSP continued to pay salaries, which PROSALUDsupplemented. A major turnaround in net revenue generation at Cotoca occurred ingeneral medical consultations when the physician incentive plan was introduced andthe nurse and doorman were terminated. The MPSSP also subsidized salaries at LosTajibos, Montero Hoyos, and Puerto Pailas. None of the peri-urban clinics receivedany subsidies.
The Alcaldfa had expressed interest in turning over seven of its remaining clinicsto PROSALUD management. Both the MPSSP and the Caja Nacional, the largestsubprogram of social security, had also expressed interest in further cooperativearrangements with PROSALUD.
In 1986 PROSALUD offered both a prepaid and fee-for-service plan in the oneurban and five rural clinics then in existence. For the prepaid plan, individualparticipants paid the equivalent of US$20 per year for an unrestricted number ofvisits. Utilization rates were much higher for prepaid plan members than forfee-for-service users, and this plan had to be phased out because of financial losses.In mid-1988 PROSALUD began an experiment with a deferred payment programintended to serve approximately 1,300 employees of twenty-six business enterprises.The plan offered the businesses a single source of care as an alternative to theobligatory social security system. However, payments from the businesses were notcollected easily or quickly, and the resultant cash flow crisis caused PROSALUD toabandon the program a year later. The free provision of medicines was generallyregarded as a critical factor in the failure of both the prepayment and deferredpayment programs.
In 1989, the cost accounting system included nine cost/revenue centers: (1) thepharmacy; (2) medical consultations; (3) nursing services; (4) laboratoryexaminations; (5) births and deliveries; (6) community organization and training; (7)dental services; (8) changes in medicines, office supplies, and lab supplies, and (9)changes in office furniture and equipment, medical and lab equipment, vehicles, andany improvements in physical plants.
1. One U.S. dollar was equivalent to Bs 2.86.

PROSALUD: Marketing and Financing Primary Health Care 197
PROSALUD's financial systems had evolved over time. Cost accountingcategories had been eliminated or redefined to conform with shifting operatingrealities. Because past categories might overlap, partially duplicate, or simply notexist when compared with more recent categories, this made it difficult tocompare trends over time.
Many cost categories could not be matched exactly with the costs related toservices that also generated revenues. Costs that at least partially supported otherrevenue-generating activities were not allocated to the services they supported.Nursing services were one example. Although nurses provided reception andtriage for all activities, including assistance in the labs, their costs were collectedand compared with revenues generated by nursing services. As most directnursing services were preventive care (immunization, etc.), this cost centershowed the largest deficit. Other cost centers, such as dentistry, were viewed asnet revenue generators, but had no system support costs allocated to them.Pharmacy costs only included costs directly associated with the pharmaceuticals.
Information generated by these financial systems indicated that five serviceswere net positive revenue generators (see Exhibit 11). Births and deliveries wereestimated to generate from two-and-a-half to three-and-a-half times their costs inrevenues.
Promoting PROSALUD
PROSALUD had used various promotional techniques to increase demand forservices. Since clients valued the services of physicians, deliveries now wereperformed by physicians rather than midwives. The number of drugs availablewas increased and their presentation made more attractive. Preferential prices fordrugs were used for clients served by PROSALUD physicians and nurses. Radiospots and brochures were developed, and a video was tested on PROSALUDstaff, but not used for promotion. Another approach to promotion was the healthfair that was conducted at some clinics. It combined health education in the formof posters, measured children's heights and weights, and used educationalentertainment such as cooking competitions between mother's clubs. Theshort-run increase in patient volume was impressive and paid for the costs of thehealth fair, but it was short-lived and the fairs were generally not repeated. Eachof the centers also designated its largest room as the space for other organizedneighborhood activities, and these rooms were decorated with plants andpaintings. PROSALUD believed that generally word-of-mouth advertising wasits best promotional vehicle.
Medical Community Perspective
The College of Medicine's register indicated that nearly 1,200 physicianslived and/or practiced in Santa Cruz. Of these, the president of the collegeestimated that half were unemployed. Approximately 400 worked in permanentpositions with the MPSSP or social security. Only 50 percent worked full time,

198 Section Two: Applied Experiences in Health Economics and Financing
and the remaining 200 worked half or three-quarters-time. There had been nodiscernible change in the prices charged by private physicians. The college,which acted as a trade association, published a fee schedule to which thepresident believed private physicians generally adhered. Various pressures werebrought to bear on those who did not, and the president made it clear that he feltthe lower prices of the PROSALUD system (see Exhibit 12) exacerbated theunemployment problem for physicians, undermined physician solidarity, andcreated economic insecurity for individual physicians by making it difficult forthem to earn what the college felt were appropriate salaries. Private solopractices and polyclinics in the areas immediately surrounding PROSALUDfacilities were reported to be charging prices far below the minimum schedulerecommended by the college.
The MPSSP, the social security, the Alcaldia, and other organizations' viewof PROSALUD was generally very supportive. PROSALUD had maintainedclose cooperative relationships with other institutions, including completing thereporting forms normally required in the MPSSP system. PROSALUD wasgenerally seen as a vehicle to assist the MPSSP in providing health services.PROSALUD prices were almost identical to those of the MPSSP.
Carlos considered what expansion efforts PROSALUD might want toundertake in the Santa Cruz area and whether replication was possible in otherareas of Bolivia. He had little information available that would allow him tocompare the health sector situation in Santa Cruz to other parts of Bolivia and toassess whether the PROSALUD system could succeed. Was it in fact replicable?While he felt that PROSALUD should explore possible options for expansion,he also was concerned about how to improve the system already in place as wellas how to assure the long-term viability of PROSALUD.

EXHIBIT 1ORGANIZATIONAL STRUCTURE OF THE PROSALUD SYSTEM
' ~~~PROSALUDMANAGEMENT SERVICES UNIT
< (MlS,U)
0LEVELIII EVELIII LVEL II LVEL II LEEL II LEVL II LEVL IIILEVLIIIILEVEL III LEVEL III
Rural PHC Rural PHC Rural PHC s
a.t~~~~~~~~~~~~~~~-
3*1r-~~~~~~~~~~~~~_ _ _ _ _ _ _ _ _ _ _ _ _ _ U,
LEVELI 1(Health Promoters) J-
COMMUNITY ]Source: PROSALUD.
to

N)O
EXHIBIT 2PROGRESS OF CLINICS TOWARD SELF FINANCING, 1988-September 1989a O
1988 1989'
Health centers esablshentf 01 02 03 04 0Q1 2 03 Facility supportb
URBANVilla Pllin 3/86 82 63 74 90 94 100 108 Community & USAIDEl Carmen 7/87 90 89 125 137 134 130 138 La Alcaldia Municipal CLa Morita 10/87 95 82 99 87 97 95 104 La Alcaldia Municipal La Madre 5/88 77 83 99 108 103 95 La Alcaldia Municipal Los Lotes 11/88 39 53 52 66 Fondo Social de Emergencia (Fioanini 7189 40 Fondo Social de Emergencia La Cuchilla 7/89 53 Fondo Social de EmergenciaLas Pampitas 7189 57 Fondo Social de Emergencia
CD
Ismael SuardezHeroes del Chaco E
xm
Urban average 89 78 97 99 104 102 88 mRURAL El Pailon 3/86 60 41 48 54 47 55 53 Community 0
Montero Hoyos 6/86 50 53 40 42 59 64 47 Community 0Cotoca 8/86 57 56 54 57 86 97 101 MPSSPLos Tajibos 10/86 30 36 43 48 73 67 92 Community C
-n
Puerto Pailas 10/86 89 82 91 79 77 79 84 CORDECRUZRural average 61 53 56 58 68 76 78Overall average 85 81 91 92 95 96 87
to
0: QuarterNote: The cost of the MSU are excludeda, Averages are weighted by clinic size. Quarter 3, 1989, wieghted urban clinic average excluding the three clinics opened that quarterwas 107 percent. The overall weighted average was 101 percent.b. Facility Support refers to the ownership or construction of the building. LaAlcaldia Municipal is the Santa Cruz municipal government.Fondo Social de Emergencia is one of the numerous government mutual aid funds. CORDECRUZ is the Regional Cooperation Source: PROSALUD.

PROSALUD: Marketing and Financing Primary Health Care 201
EXHIBIT 3TRENDS IN BOLIVIAN
PUBLIC HEALTH SECTOR FINANCING, 1984-88
Source 1984 1985 1986 1987 1988
National treasury andothers 92.2 62.2 48.8 60.2 50.1
User fee 5.6 17.2 30.1 25.4 22.1External aid 2.2 20.6 21.1 14.4 27.8
Total 100 100 100 100 100
Source: MPSSP data; World Bank (1989).
EXHIBIT 4SOCIOECONOMIC INDICATORS
Indicator Level
Total population, 1988 (millions) 6.9Population residing in urban areas, 1988 (percent) 50GNP per capita, 1988 (US$) 570Average growth of GNP, 1965-88 (percent) -0.6Average growth in GDP, 1980-88 (percent) -1.6Average annual inflation, 1980-88 (percent) 483Unemployment rate, 1980 (percent) 5.8Unemployment rate, 1986 (percent) 20Population with income insufficient to satisfy 70% of basic
needs, 1975 (percent) 80Share of central government health expenditures, 1972
(percent) 6.3Share of central government health expenditures, 1988
(percent) 1.9Life expectancy, 1988 (years) 53Infant mortality rate, 1988 (per 1,000 live births) 108Adult illiteracy rate, 1985 (percent) 26
Source: World Bank (1990).

202 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 5SOURCES AND USES OF MPSSP HEALTH
EXPENDITURES IN SANTA CRUZ, 1987
ExpendituresFunding source Personnel Operations Investment Total
National treasury (US$) 2,522,182 354,405 0 2,876,590Percentage of source 88 12 0 100Percentage of total 55 13 0 31
User fees (US$) 2,052,736 2,202,596 233,876 4,489,208Percentage of source 46 49 5 100Percentage of total 45 84 11 48
Subtotal 457,492 2,557,001 233,876 7,365,79862 35 3 100
100 97 11 79
DONATIONSMunicipal (US$) 0 29,028 551,426 580,454Percentage of source 0 5 95 100Percentage of total 0 1 27 6
Regional (US$) 0 11,000 466,624 477,624Percentage of source 0 2 98 100Percentage of total 0 0 22 5
International (US$) 0 31,177 823,463 854,640Percentage of source 0 4 96 100Percentage of total 0 1 40 9
Subtotal 0 71,205 1,841,513 1,912,7180 4 96 1000 3 89 21
Total 4,574,921 2,628,206 2,075,389 9,278,51649 28 22 100
100 100 100 100
Source: MPSSP data; World Bank (1989).

PROSALUD: Marketing and Financing Primary Health Care 203
EXHIBIT 6COMPARISON OF MSU COSTS
FIRST QUARTERS OF 1987 AND 1988
March 1987 Bs
PercentageCosts 1987 1988 change
VARIABLE COSTSaOffice supplies 1,218 676 -44.5Communications 696 123 -82.3
Fuel and maintenance 836 698 -16.5Transportation and travel 1,066 326 -69.4
Training 594 313 -47.3Utilities 190 181 -4.7Other 1,944 923 -52.5
Subtotal 6,544 3,240 -50.5
FIXED COSTS3
Personnel 24,100 16,151 -33Rent 1,800 1,303 -27.6Vehicle depreciation 632 1,986 214.2
Subtotal 26,532 19,440 -26.7
Total 33,076 22,680 -31.4
a. Variable and fixed cost categories were established by the study team during the development ofthe market analysis model.Source: PROSALUD

EXHIBIT 7PROSALUD MARKET SURVEY DATA RESULTS
Percent O
Mother's education Average Less than Less than M
Number of Total family 2 years in 2 years in Formal Own Health .>
Center families population size area Santa Cruz employment None Basic home insurance
URBAN rnPetrolero 1,299 6,427 4.9 65 79 22 14 46 63 28 XPampitas 1,383 7,066 5.1 49 50 14 20 41 72 8 _Chichilla 1,822 8,796 4.8 56 58 12 5 44 62 7Foianini 1,764 9,623 5.5 65 62 38 4 40 63 19 5Heroes 1,726 9,447 5.5 56 66 26 14 40 69 21 I
Lotes 1,478 7,265 4.9 49 11 73 11 XMadre 1,665 6,565 3.9 53 20 40 16 mMorita 1,798 7,832 4.4 55 23 44 22 8Carmen 2,608 15,885 6.1 68 21 51 21 O
Villi Pillin 1,402 8,065 5.8 66 23 74 20 C
Subtotal 86,971
RURAL mCotoca 442 2,479 5.6 86 13 28 !Tajibos 800 77 15 _
Pto.Pailas 162 909 5.6 5 CDPailon 353 1,861 5.3 93Monetero 147 750 5.1 94
Subtotal 6,799
Note: For blank cells information was not available.Source: PROSALUD.

PROSALUD: Marketing and Financing Primary Health Care 205
EXHIBIT 8PERSONNEL COSTS AS A PROPORTION
OF CLINIC COSTS, 1988
Costs of Percentage ofpersonnel operating Percentage of
Health centers (1988US$) costsa total costsb
URBANVilla Pillin 23,613 68.5 53.7El Carmen 18,313 69.5 53.3La Morita 17,320 63.7 52.2La Madra 9,740 67.5 65.4
RURALEl Pailon 10,353 64.1 61.1Montero Hoyos 2,010 68.1 64.1Cotoca 1,971 64.0 61.2Los Tajibos 3,163 39.3 37.4Puerto Pailas 9,213 61.1 56.6
Overall average 64.8 54.9
Note: MSU costs are included in calculations for both operating and total costsbecause most MSU costs are personnel costs and disaggregation was notpossible. MSU personnel totalled twenty-four persons in 1986, but were reducedto only nineteen persons by late 1988.a. Operating costs include medicines, medical and laboratory supplies, officesupplies, personnel and transportation.b. Total costs include operating costs, plus marketing costs and depreciation.Source: PROSALUD.

206 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 9MEDICATION DISPENSED BY PROSALUD CLINICS, 1988
1988 US$
Revenue Percentage ofNumber of Cost of Cost per from drug Drug sales PROSALUD's
visits drugs visit sales surplus income
URBAN
Villa Pillin 4,932 4,826 0.98 6,660 2,834 25.1El Carmen 8,322 6,547 0.79 10,341 3,794 25.2La Morita 6,750 8,095 1.2 10,377 2,282 33.1La Madre 4,855 1,601 0.33 3,229 1,628 25.4
Subtotal 24,859 21,069 0.85 30,607 9,538 27.4
RURAL
El Pailon 987 3,612 3.66 4,947 1,335 59.9Montero 679 819 1.21 1,152 333 65.1HoyosCotoca 2,048 4,552 2.22 5,783 1,231 48.8Los Tajibos 315 642 2.04 972 330 63.2Puerto Pailas 1,071 3,433 3.21 5,296 1,863 77.9
Subtotal 5,100 13,058 2.56 18,150 5,092 60.1
Total 29,959 34,127 1.14 48,757 14,630 34.4
Source: PROSALUD.

EXHIBIT 1 0TRENDS IN LEVEL AND MIX OF SERVICES, 1987-SEPTEMBER 1989
(average number of visits for all active clinics)1987 1988 1989
Service Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3
PREVENTIVEPrenatal 51 49 63 84 98 68 84 78 82 100 115Births 12 10 14 15 22 18 21 23 30 37 36Pernatal 11 6 10 12 22 19 30 21 30 37 59Well-child 107 90 89 95 86 78 86 85 67 104 137Vaccinations' 161 813 291 341 229 296 533 290 288 381 844House calls 90 115 37 34 42 40 50 34 40 52 64
Subtotal 432 1,083 504 581 499 519 794 531 537 711 1,255
CURATIVEGeneral consultation 557 427 638 784 813 540 864 822 777 854 848Diarrhoeal 42 37 37 72 39 26 38 60 43 33 46Acute respiratory 46 66 69 63 58 47 105 86 100 88 107TB treatments 13 9 7 5 6 1 16 4 5 5 4
Subtotal 658 539 751 924 916 614 1,023 972 925 880 1,005
Total 1,090 1,622 1,255 1,505 1,415 1,133 1,817 1,503 1,462 1,591 2,260
Q. Quartera. DPT, BCG, tetanus, toxoid, polio, and Measles. 0Source: PROSALUD.

EXHIBIT 1 1KEY NET REVENUE GENERATING SERVICES
January -June 1988
Service January February March April May June
Pharmacy (US$) 1,529 1,420 2,349 1,606 1,506 1,818Laboratory tests (US$) 2,849 1,688 2,105 1,962 1,097 5,007
I
Subtotal (US$) 4,378 3,108 4,454 3,568 2,603 6,825Percentage 47 42 42 38 32 5o0C
00Dentistry (US$) 851 729 937 1,182 1,093 982
Births and deliveries (US$) 1,224 1,062 2,282 1,356 2,399 3,163 Pediatrics (US$) 2,855 2,426 2,859 3,228 1,997 2,644
-TnSubtotal (US$) 4,930 4,217 6,078 5,766 5,489 6,789Percentage 53 58 58 62 68 50_
Total 9,308 7,325 10,532 9,334 8,092 13,614
Source: PROSALUD.

PROSALUD: Marketing and Financing Primary Health Care 209
EXHIBIT 12CHARGES FOR SELECTIVE MEDICAL PROCEDURES,
PRIVATE MEDICAL MARKET STANDARD AND PROSALUD(Bs)
PROSALUD price Minimum prdce________________ recommended by
Rural Urban the College
Procedure clinic clinic of Medicine'
ConsultationGeneral or family 5 5.0-6.0 15pracbtionerSpecialist N/A 7.5-8.0 22.5
Birth and deliveryb 50-60 110 450
SuturesUp to 4 points 8 8 45Upto 10 cm.Additional points 2 2More than 1 0cm. 75
N/A: Not applicablea. These are the minimum prices suggested by the college, which suggests that six additionalconsiderations should justify an increase in these prices by as much as threefold.b. Birth and delivery charges in PROSALUD clinics cover attendance by a gynecologist, two to threeInpatient days, medicines, a nightgown for the baby, and one pediatrician visRt.Source: Colegio Medico (1989).
Source Documents
Colegio Medico. 1989. Memorandum on Price Lists Santa Cruz, Bolivia.Unpublished.
World Bank. 1989. "Integrated Health Development Project-Bolivia." StaffAppraisal Report 8001. Washington, D.C.
. 1990. World Development Report 1990. Washington, D.C.

Case 9. Antimalaria Program inNorthwest Brazil: A Cost-Benefit
Analysis
Study Questions
This last case deals directly with issues of economic evaluation and health careinterventions. There is a clear decision to be made, with significant consequencesfor the health of the people of Rondonia, Brazil. Information provided on costsand benefits leads to a conclusion about whether or not the project is aworthwhile investment. Further information, around which the central issues ofthe case revolve, includes benefits not considered in the cost-benefit calculations.It is important to consider whether limited resources are being used in the bestway possible to eliminate malaria, and whether value will be received from theresources to be expended. The reader should have a clear understanding of whathe or she would like to achieve in Rondonia as well as how to compare theamount and value of resources to the amount and value of the potential project'soutput.
1. Why is malaria a health problem? Why might it be considered an economicproblem?
2. What are the known strategies for dealing with malaria and what inputs arerequired for these strategies? Which alternatives are most appropriate fornorthwest Brazil?
3. What are the underlying assumptions in the approaches to the cost-benefitanalysis in northwest Brazil? What is your evaluation of the appropriatenessof these assumptions?
4. What recommendations would you make regarding the estimation of costs andbenefits?
5. How would you use the cost-benefit analysis to make decisions about theproposed project?
6. What other criteria would you recommend?
210

Antimalaria Program in Northwestern Brazil: A Cost-Benefit Analysis 211
Antimalaria Program in Northwest Brazil: A Cost-BenefitAnalysis
Esteban Pachuco was trying to decide what recommendations he should maketo the World Bank about financing an antimalaria program in northwest Brazil.He was pressed by two opposing arguments. Some economists at the World Bankopposed financing the program because a preliminary cost-benefit analysisindicated that in each year of the period 1984-2000 the costs would be greaterthan the benefits (see Exhibit 1). Countering this argument were many medicaldoctors and the Superintendency of Public Health Campaigns (SUCAM), anoperationally autonomous entity under the umbrella of the Ministry of Health thatwas responsible for the control of malaria and other endemic diseases. SUCAMregarded health programs in general, and antimalaria programs in particular, asgovernment obligations that did not require economic justification for theirimplementation.
The debate over financing this antimalaria program arose during thepreparation for the World Bank's participation in the Brazil Northwest RegionIntegrated Development Program (POLONOROESTE). The Bank's proposedinvolvement included the financing of a highway construction project that wouldlink the state of Mato Grosso with the state of Rondonia and support for anagricultural development and environmental protection project. The proposedhighway would link rich agricultural areas and connect areas of abundant mineralresources to the rest of Brazil, but the areas through which the highway wouldpass were afflicted with health problems, one of which was malaria. For thisreason one of the components of the proposed loan was a health project. Thehealth project called for the construction of thirty-nine health posts and supportto SUCAM for its antimalaria program in the region.
Malaria in Northwest Brazil
Although the proportion of the population in the Americas living withinmalaria infested areas had steadily declined since the late 1950s, five countriesin the Americas, Brazil among them, attracted attention from health experts atthe Pan-American Health Organization and the World Bank in the early 1980s.The transmission of malaria and the risk of infection had increased in thesecountries. Northwest Brazil was an area plagued by high prevalence of malaria,and the disease was especially troublesome in the state of Rondonia.'
This case was written by Antonio Campino, Pan-American Health Organization, for the EconomicDevelopment Insitute of the World Bank. Case matenal was obtained from attic/es and reports of theWodd Bank. The case is intended for use as a basis for classroom discussion rather than to illustrateeither effective or ineffectve handling of a managerial or development situation.
1. Ninety-seven percent of Brazil's malaria cases were in Amazonia, where 15 percent of thepopulation lived. The states of Rondonia and Para accounted for 70 percent of all reported cases andfour municipalities within each of these states accounted for 60 percent of all cases.

212 Section Two: Applied Experiences in Health Economics and Financing
The annual parasitology index (API) is an indicator that represents the number ofpeople per thousand population infected with malaria in a given area during a year.It measured 120 per 1,000 population in Rondonia in 1980. A survey in the countyof Ariquemes, Rondonia, indicated that 62.8 percent of men and 53.4 percent ofwomen had at a least one bout of malaria during a year; 10 percent of men and 6percent of women experienced more than twenty bouts of illness in the previous fiveyears (see Exhibit 2). Rondonia suffered the highest mortality rates from malaria (seeExhibit 3). In 1980, malaria was the fourth leading cause of general mortality and thefifth cause of infant mortality, causing 5 percent of all deaths among children underthe age of one.
Rondonia, located in the Amazon jungle region of Brazil, was colonized throughmigration supported by government incentives for agricultural development and cattleraising. In 1981, the population of Rondonia was growing at a rate of approximately16 percent per year due to in-migration (see Exhibit 4). Estimates indicated that thepopulation of 500,000 would double by 1986. People with little money, but lookingfor better living and economic conditions or quick wealth from mining for gold,arrived in Rondonia. They settled on small pieces of land, built temporary houses,and came into contact with the Anopheles mosquito, the malaria vector. Increases inmalaria in Rondonia at the beginning of the 1980s were attributed to the increase inpopulation; the type of houses built (94 percent of the houses in one county,Machadinho, had either incomplete or no walls and no screens); ineffectivetherapeutic schemes; and inadequate health services for the growing population.
In Rondonia, the type and location of dwellings-without walls and nearstreams-favored the spread of malaria. The transformation of the environment causedby implementing agricultural and mining projects furthered the spread of malaria.Tree cutting and deforestation, the partial obstruction of rivers and streams, and theleveling of roads without drainage all contributed to increasing the density of themalaria vector. In addition, the housing and minimal clothing habits common in theAmazon area made contact between humans and mosquitoes more pronounced.Control of malaria was made more difficult by the population's lack of knowledgeabout malaria transmission and the benefits of spraying. In a survey of the Rondonianarea, fewer than 40 percent of the inhabitants thought the mosquito was responsiblefor malaria transmission. More than 20 percent did not want their houses to besprayed.
The incidence of malaria varied seasonally. Fewer cases occurred during therainy months. At the end of the rainy season, lingering pockets of water increasedthe number of places for mosquitoes to develop. In Machadinho county in the stateof Rondonia, for example, there were usually fewer than 1,000 cases of malariareported between January and June, but between July and December thousands ofcases were reported. In 1980, a total of 62,000 cases were identified in Rondonia,resulting in a loss of about 1 million workdays. Forty percent of all cases were thelife-threatening P. falciparum infections. An increase of P. falciparum malaria casesin relation to the number of P. vivax cases signaled a deterioration in the healthsituation.

Antimalaria Program in Northwestem Brazil: A Cost-Benefit Analysis 213
Malaria and Productivity
Malaria is a debilitating disease that impairs productivity. Recurrent infectionswith attacks or fevers frequently occur during the season of peak demand foragricultural work. Disability in terms of days of work lost is estimated to rangefrom five to twenty days. According to a survey in the Amazon area of Humaita,a person lost 5.6 days per year on average (see Exhibit 5). Another influence onproductivity includes the effects on output or land cleared. Malaria may alsocontribute to severe anemia and result in a loss of physical ability.
Dissemination of malaria to other noninfected areas is an ongoing concern.People infected with malaria who travel to noninfected areas can transmit thedisease to mosquitoes and then to the human population in the noninfected area.In Brazil, there was concern that the spread of malaria to the south of thecountry, where labor productivity was high, would have negative economicconsequences (see Exhibit 6).
Etiology of Malaria
Malaria is a collective name for different diseases that can result frominfection by any of four species of malaria parasites: Plasmodiumfalciparum, P.vivax, P. malariae, and P. ovale. The malaria parasite is transmitted betweenhumans through the saliva of a biting female Anopheles mosquito. The femalemosquito requires a blood feed from humans or animals to produce her eggs.Thus, when a human infected by malaria is bitten by a mosquito, the parasite ispassed to the mosquito, which after a period of seven to ten days, may transmitmalaria to its next victim. Human dwellings and domestic animalshelters-particularly those with thatched roofs, dark corners, and many cracksin the walls-provide preferred resting places for the mosquito to digest theblood she has consumed so that her eggs may mature.
The mosquito lays her eggs on the surface of water or at its edge. Larvaehatch in two to four days and develop in the water through five stages to produceflying adult mosquitoes. The adult female may live from a few days to over amonth repeating the cycle of blood feeds and egg laying every three to four days.Breeding places vary for each of the thirty species of Anopheles mosquitoes thatare major vectors for malaria, and reflect the evolutionary adaptability ofmosquitoes. Water habitats include permanent or transient bodies of water; freshor brackish water; standing water or flowing canals and open streams; open sunor deep shade; shallow pools or deep wells; clean drinking water or water highlypolluted with organic matter; and open marshes or pools that collect on plantsand in rock holes, cattle footprints, or discarded containers. Weather conditionsinfluence the activity and survival of mosquitoes and result in marked seasonalcycles for mosquito population densities and malaria transmission.
The characteristics of the disease vary with the intensity of the infection, thehost's level of immunity, the adequacy of an opportunity for treatment, and theparasite's susceptibility to it. The chief symptom of malaria is fever lasting eight

214 Section Two: Applied Experiences in Health Economics and Financing
to twelve hours. Periodic bouts of fever tend to alternate with days of less or nofever. This pattern is typical of P. vivax cases. P. falciparum infections usuallyinvolve prostrating fever with brief and incomplete remissions. Repeatedinfections give rise to a partial immune status. Untreated or incompletely treatedinfections will produce repeated relapses. Common antimalarial drugs may clearthe blood of parasites, but different drugs are required to eliminate parasites thatlodge in the liver. Acute severity and mortality occur almost exclusively in P.
falciparum infections, which can lead to death in two to three weeks. Those atsevere risk of malaria in highly endemic areas include the following:
* Children older than three to six months and younger than five years whohave lost the immunity transferred from their mother at birth
* Adult immigrants from nonendemic or low endemic areas
* Laborers concentrated in camps or overcrowded living conditions
* Pregnant women, because their natural immunity is depressed.
Most deaths from malaria occur in young children and pregnant women. Malariaalso may contribute to abortion, prematurity, or low birthweight and to theseverity of other childhood diseases. Among semi-immune pregnant womenliving in highly endemic areas, malaria represents a serious risk for complicationsof pregnancy and delivery. During labor, the severe anemia caused by repeatedinfections can result in extreme hemorrhaging. There also is a high neonatalmortality risk.
Malaria Control Strategies
The traditional strategies for malaria control include spraying house walls withDDT to kill the Anopheles mosquito, the vector for the malaria parasite, andtreating those people infected with chloroquine at health centers. In the 1980s,SUCAM was the organization in Brazil directly responsible for the control andtreatment of malaria. It was obligated to
* Spray houses, camps, and work areas biannually
* Train microscopists for enterprises that held government contracts, suchas mining or highway construction
* Provide education regarding elimination of mosquito breeding areas andreduction of the mosquito density
* Supply antimalarial drugs to treat those infected
* Train personnel working in private firms on spraying techniques

Antimalaria Program in Northwestern Brazil: A Cost-Beneft Analysis 215
* Provide contractors with information on the materials and equipmentneeded.
SUCAM also was responsible for providing the biannual orientation fortherapeutic schemes, supplying medication to institutions, and centralizing theregistration of malaria cases.
SUCAM scheduled houses for spaying with DDT biannually, but inadequatehuman resources, transportation, or DDT supplies often interfered with thecompletion of this schedule. About 10 percent of households were not sprayedbecause the occupants refused to allow spraying of their dwellings, or becausethe houses had no exterior walls. In one year during the early 1980s, only 43percent of the targeted houses were actually sprayed. In some instances, dwellerswashed the walls to remove the "poison."
DDT spraying did not always result in a reduced incidence of malaria. In1980, there was an increase in the incidence of malaria cases after very goodcoverage by DDT spraying in 1979. However, the incidence of malaria in 1981was the lowest for the 1978-81 period even though only a small percentage ofhouses had been sprayed that year.
Alternative strategies to spraying were tried, including
- The use of fish to eat mosquito larvae in places of high transmission rates
- The use of larvicide hiicroorganisms such as bacillus turigiensis vv israelliand Bacillls esphericus
* The use of an ultra low volume of DDT in localities of high transmissionrates.
No information was available as to the effectiveness of these strategies.
Health Services
Basic health services were available to the 40 percent of the Rondonianpopulation living in Porto Velho and other towns. The main health agencies werethe Territorial Secretariat of Health in charge of health policy and coordinationof services for the region; the health departments of the municipalities,responsible for primary health care with the secretariat; the Foundation for PublicHealth Services, providing hospital, health center, and water supply services; andSUCAM. Rondonia had sixty-two health posts and twenty-six health centers.Twelve of the health centers were in urban areas, as were the five referral healthcenters and three public hospitals. The health posts and centers operated bySUCAM functioned in old buildings, all requiring repair and renovation.Although SUCAM's microscope technicians were experienced and capable of

216 Section Two: Applied Experiences in Health Economics and Financing
making accurate diagnoses, the microscopes available for their use worked onlyon daylight and needed upgrading.
Chloroquine medications were readily available at SUCAM health posts.Although chloroquine was administered appropriately and in the correct quantitiesfrom the health facility, it was not effective in controlling either P. vivax or P.falciparum malaria. Health workers were aware that patients stopped taking thechloroquine once they felt better, but before they were completely cured. Theseactions were believed to be contributing to chloroquine-resistant species of bothP. vivax and P. falciparum. Primaquine, a more expensive drug used againsthepatic forms of P. vivax, was administered, but in insufficient quantities. Morethan 30 percent of the malaria patients treated in Machadinho needed to behospitalized.
SUCAM had one doctor assigned to Rondonia and few professionals withuniversity training. The territorial secretary of health and the secretaries of healthof the counties had several doctors in different health posts who were experiencedin treating malaria. SUCAM worked with the other public health entities, butreports by outsiders noted the need for integration and joint operation of thevarious public health entities operating in Rondonia to achieve better results inthe campaign against malaria.
SUCAM was a vertical and centralized organization. It had the advantage ofbeing less susceptible to local political pressures than were the secretaries ofhealth, who may have been influenced to hire public workers on the basis of theirpolitical affiliations rather than their job skills. SUCAM requested a budgetallocation of US$112 million in 1981, of which US$3 million was for malariacontrol operations in Rondonia. The amount actually approved was half theamount required to maintain control efforts. Supplementary funding was providedby the Territory of Rondonia.
The Northwest Region Development Process
POLONOROESTE was established by presidential decree in May 1981 as ameans of ensuring the orderly development and settlement of Brazil's northwestregion, which comprised the Territory of Rondonia and the state of Mato Grosso.Because the region was an important potential source of agricultural productionand employment, its development was one of the govermnent's highest priorities.POLONOROESTE had four objectives: to integrate marginal regions into thenational economy; to ensure orderly settlement; to increase the productivity,incomes, health, and social welfare of migrants; and to protect indigenouscommunities, land resources, and the environment. Three overlapping phases ofthe POLONOROESTE program included five interdependent projects. The totalcost of the entire POLONOROESTE program was estimated at around US$1billion (see Exhibit 7). Fifty-three percent of the funds was intended for roads;40 percent would be spent on rural development and settlement; and the balancewas to be directed to health, protection of indigenous peoples and the

Antimalaria Program in Northwestern Brazil: A Cost-Benefit Analysis 217
environment, and administration. During the program's first phase, theNorthwest Highway Project was to pave the highway between the cities ofCuiaba and Porto Velho, strengthen Rondonia's Highway Department, andconstruct the feeder road network. The Agricultural Development andEnvironmental Protection Project was to support settlement consolidation,environmental protection, ecological research, and land tenure regularization. TheHealth Project was expected to strengthen malaria control, establish a limitednetwork of primary rural health facilities in Rondonia with trained staff, andsupport health research.
The proposed malaria control component of the health project was designedto identify transmission areas, provide surveillance of malaria incidence, reducethe population of infected mosquitoes, and treat the sick. The project wouldsupport the expansion of SUCAM's malaria control program and strengthen itsmanagement and controls systems. It would support the recruitment of 330additional field workers and provide them with the proper spray equipment,DDT, and vehicles. The project also would finance incremental salaries, someoperating costs, and consulting services. The development of health servicesinvolved the construction of thirty-nine health centers and fifty health posts in themunicipalities, as well as training for 100 rural health workers and 200 healthauxiliaries to be assigned to these new facilities. Research on malaria wasintended to be an ongoing component of the health project. Exhibits 7 and 8provide details regarding project costs.
Malaria Program Cost Benefit Analysis
A preliminary cost-benefit analysis performed by the World Bank was madeunder the following assumptions:
* The API would be reduced from 120/1,000 to 35/1,000 by 1986 withmaintenance at that level until 2000.
* The economically active population aged fifteen to sixty-four yearscorresponded to 53.5 percent of the population of the state of Rondonia.2
* The average value of daily earnings in Rondonia, based on monthly wagesconverted to daily wages using a thirty-day month, were US$5.00 per dayfor rural areas, US$8.65 per day for urban areas, and US$6.02 per daystatewide.
* Sixty percent of the days in the year were working days.
2. If the economically active population were defined as those aged 10 to 64 years becauseRondonia is an agricultural state, the corresponding population would be 65.8 percent of the total(see Exhibit 2).

218 Section Two: Applied Experiences in Health Economics and Financing
* Fifty percent of the malaria cases affected men and women older thanfourteen.
The Institute of Economic Research at the University of Sao Paulo calculated twobenefit-cost ratios using different assumptions about the economically activepopulation, the daily wage, and the possible reduction in the API (see Exhibit 9).The rates of return obtained for each of these analyses were negative for theperiod 1981-84, and although the rate of return would improve, it would continueto be negative through the year 2000. Exhibit 10 presents the rates of return andExhibit 11 provides details on the cost-benefit analysis.
Economic Analysis and the Ministry of Health
The Ministry of Health regarded health as a merit good and the decision toinvest in health was justifiable without need of further scrutiny or economicanalysis.3 This position was supported by SUCAM, the Ministry of the Interior,and also a group of influential doctors.
The Institute of Economic Research at the University of Sao Paulo assumeda moderate and intermediate position in the debate. Economists at the instituteemphasized that other instruments could be used in place of a cost-benefitanalysis, and they suggested that a cost-effectiveness analysis of the malariaproposal was warranted. In any event, a cost-benefit analysis could provide animportant, but not the only, basis for taking a decision. They advocated takinginto account a full evaluation of benefits that could result from an antimalarialprogram. One professor in the Department of Economics thought that a betterway to assess the benefits of the antimalaria program would be to consider thefamily as a producing unit and associate monetary value to the activities of allfamily members.
Pachuco recalled that a secretary of health in Rondonia had once stated thatthe press would 'give more importance to four cases of malaria in Guaruja [atourist beach in the state of Sao Paulol than to 170,00 cases of malaria inRondonia." A colleague of Pachuco's at the Pan-American Health Organizationemphasized that malaria becomes a problem when there is an inadequate systemof health protection. His vision required developing the capacity for thepopulation to care for its own health. In the opinion of others, more effectivemeasures to control malaria would be to require new economic projects to beimplemented with the effective participation of public health units and preventpeople with malaria from entering an area.
3. Merit goods or services are those that a government believes individuals should not havefree choice in consumption, because consumers may lack information about the good or badeffects inherent in the consumption of the goods or services.

Antimalaria Program in Northwestern Brazil: A Cost-Benefit Analysis 219
As Pachuco reflected on these views, two aspects concerned him. One was theadequacy of the cost-benefit analysis. The second concerned the adequacy of theproposed strategy for the malaria program: spraying and chloroquine distribution.

Cn
EXHIBIT 1BENEFITS AND COSTS OF THE ANTIMALARIA PROGRAM, 1981-2000
D
Year 1981 1982 1983 1984 1985 1986 1987 1988 1989 1990Population (1,000) 764 887 1,024 1,175 1,340 1,510 1,685 1,866 2,052 2,244 mxMalaria cases avoided (1,000) 16.81 38.14 40.96 41.12 46.90 52.85 58.96 65.31 71.82 78.54 X
Gains in working days (1,000) 39.80 90.30 96.98 97.37 111.04 125.13 139.65 154.63 170.05 185.96Value of the working days gained 199.00 451.50 484.90 486.85 555.20 625.65 698.25 773.15 850.25 929.80(US$ 1,000) 5Costs (US$1,000) 1,572.70 1,931.20 2,563.40 3,243.00 4,159.20 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70Benefit-cost ratio 0.127 0.234 0.189 0.150 0.133 0.165 0.184 0.203 0.224 0.245 _
M
Year 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 0Population (1,000) 2,446 2,666 2,906 3,167 3,452 3,763 4,101 4,470 4,875 5,511 o
a)Malaria cases avoided (1,000) 85.61 93.31 101.71 110.85 120.82 131.71 143.54 156.45 170.56 185.59 Qa.Gains in working days (1,000) 202.70 220.93 240.82 262.46 286.07 311.85 339.86 370.43 403.83 440.13 m
Value of the working days gained 1,013.50 1,104.65 1,204.09 1,312.03 1,430.35 1,559.25 1,699.30 1,852.15 2,019.15 2,220.65(US$ 1,000) o
Costs (US$1,000) 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70 3,800.70Benefit-cost ratio 0.267 0.291 0.317 0.345 0.376 0.410 0.447 0.487 0.531 0.579
Source: World Bank (1 981); Institute of Economic Research (1 982).

EXHIBIT 2EPISODES OF MALARIA BY SEX AND OCCUPATION IN ARIQUEMES, RONDONIA, 1977-82
Sex Occupation
Number of Men Women Farming Nonfarmingepisodes Number Percentage Number Percentage Number Percentage Number Percentage
0
0 88 36.21 94 46.31 4 8.70 178 44.50 z
1-3 69 28.40 46 22.66 12 26.09 101 25.25
4-10 41 16.87 34 16.75 10 21.74 66 16.503
11-20 19 7.82 17 8.37 8 17.39 28 7.00
More than 20 26 10.70 12 5.91 12 26.09 27 6.75
Source: Boulos, Gryschek, and Segurado (1986).

222 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 3MALARIA MORTALITY BY STATE, 1977-82
Average mortalityper 100,000
State population
Acre 8.3Rondonia 24.6Amazonas 1.8Roraima 1 1.9Para 6.9Amapa 8.0Maranhao 2.2Mato Grosso 1.9Golas 1.5
Source: Fiuza Lima (1985).

Antimalaria Program in Northwestern Brazil: A Cost-Benefit Analysis 223
EXHIBIT 4FLOW OF MIGRANTS TO RONDONIA, 1981
'S~~~~
-I- ~ ~ ~ 1-
~~~~~~~Z ~ ~ ~ ~ ;
-/ fORAS - t *-- (l9&lWD1l1-
Source:'Mii o H =1===j j:;, ACRE hA 5 ,' P A HAO ) X AD
) , X A (i)~~~~~~~~~~~~~~~~~~~~~~~~,
$ SAflT CATARINA
Source: MinistLry of Health (1982).

224 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 5DURATION OF MALARIA SPELLS ACCORDING TO
ETIOLOGY IN PATIENTS LOCATED IN HUMAITA, AMAZON
Duration in days
Etiology O to 3 4 to 6 7 to 16 Total
Plasmodium vivax 12 6 11 29
Plasmodium falciparum 15 6 7 28
Plasmodium vivax and falciparum 0 1 0 1
Total 27 13 18 58
Source: Meira (1982), cited in Institue of Economic Research (1982).

Antimalara Program in Northwestern Brazil: A Cost-Benefit Analysis 225
EXHIBIT 6PRINCIPLE FLOW OF MALARIA CASES, 1977
PANAMA So. P.C,A,.N.
\/ t , A C Of AT
'N~~~~.
Souce MityW of Helt 1982).
CAM *
- A I t-2 I"
Source: Minstry of Helth (1982)

226 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 7TOTAL COST OF POLONOROESTE PROGRAM, 1981
Project costProject/component (US$ millions)
PHASE I
Highway Project 487.7
1. Highway construction and operation
2. Strengthening DER-RO
3. Feeder roads in Mato Grosso and Rondonia
Agricultural Development and Environmental Protection Project 199.31. Settlement consolidation
2. Environmental protection
3. Ecological research
4. Assistance to INCRA for land tenure regularization
5. Assistance to INCRA for identification of future
settlements
6. Strengthening of program coordination and monitoring
Health Project 25.3
1. Malaria control
2. Health services department
3. Training and supervision
4. Research and evaluation
PHASE II
Mato Grosso Rural Development Project 76.8
PHASE IlIl
New Settlement Project 182.0
Total POLONOROESTE program cost 971.1Source: World Bank (1981); Institute of Economic Research (1981).

Antimalaria Program in Northwestem Brazil: A Cost-Benefit Analysis 227
EXHIBIT 8HEALTH PROJECT EXPENDITURES BY ACCOUNT CATEGORY
Expenditure category Year 1 Year 2 Year 3 Year 4 Year 5 Total
Capital costs
Equipment 61.0 70.0 80.0 92.0 104.9 407.9
Vehicles 94.1 61.3 53.7 61.4 53.5 324.0
Technical assistance 72.0 0.0 0.0 0.0 0.0 72.0
Research 300.0 300.0 300.0 300.0 300.0 1,500.0
Total capital costswithout 227.1 131.3 133.7 153.4 158.4 803.9research
Total capital costs with 527.1 431.3 433.7 453.4 458.4 2,303.9research
Recurrent costs
Drugs and DDT 364.0 415.1 473.2 540.1 615.1 2,407.5
Increment in salaries 322.6 469.4 685.0 897.9 1,328.9 3,703.8
Travel 426.5 650.3 969.3 1,307.1 1,664.1 5,017.3
Vehicle maintenance 232.5 265.1 302.2 344.5 392.7 1,537.0
Total recurrent costs 1,345.6 1,799.9 2,429.7 3,089.6 4,000.8 12,665.6
Contingencies
Physical (10%) 187.3 223.1 286.3 354.3 445.9 1,496.9
Pricea 298.5 580.3 1,057.4 1,684.4 2,391.5 6,012.1
Total contingencies 485.8 803.4 1,343.7 2,038.7 2,837.4 7,509.0
Total project costs
Capital + recurrent +contingencies 2,358.5 3,034.6 4,207.1 5,581.7 7,296.6 22,478.5
Capital without research +recurrent + contingencies 2,028.5 2,704.6 3,877.1 5,251.7 6,966.6 20,828.5
Capital without research +recurrent 1,572.7 1,931.2 2,563.4 3,243.0 4,159.2 13,469.5
Note: Physical contingencies were calculated prorating the value for physical contingencies for the entire healthproject. The same procedure was used for price contingencies. The total for capital without research +recurrent + contingencies was calculated, excluding US$300,000 for research and US$30,000 for physicalcontingencies.a. Price contingencies are based on the following annual percentage escalations: 9.0 in 1981, 8.5 in 1982, 7.5in 1983-85, and 6.0 thereafter.Source: World Bank (1981); Institute of Economic Research (1982).

cCDEXHIBIT 9
ASSUMPTIONS USED BY ANALYSTS FOR CALCULATION OF RATES OF RETURN
Institute for Economic ResearchParameter World Bank Hypothesis 1 Hypothesis 2
Annual parisitology index (per 1,000) Reduced from 110 in Reduced from 98 in 1981 to 761980 to 30 in 1986 in 1982, 80 in 1983, and 85 in
and remains at that level. 1984 through the year 2000.
rnDays lost by malaria 6.00 6.00 6.0
0
Economically active population (percent) 50.00 50.00 65.8-n
Proportion of active days (percent) 60.00 60.00 60.0 _
Average wage per day (US$) 6.02 6.02 5.0
Source: Internal World Bank document(1 982); Institue of Economic Research (1982).

Antimalaria Program in Northwestern Brazil: A Cost-Beneft Analysis 229
EXHIBIT 10ALTERNATIVE RATES OF RETURN FOR THE
ANTIMALARIA PROGRAM, 1981-84 and 1981-2000
Rate of return for Rate of return for1981-84 1981-2000
Alternative (percent) (percent)
World Bank -233.42 -51.05
Institute for Economic Research
Hypothesis 1 -212.19 -195.99Hypothesis 2 -212.81 -195.40
Source: Internal World Bank document (1982); Institute of Economic Research (1982).

230 Section Two: Applied Experiences in Health Economics and Financing
EXHIBIT 1 1COST-BENEFIT ANALYSIS
The internal rate of return of the incremental expenditures in the antimalariaprogram was calculated according to the formula:
n B, - C,= O
t-1(1 +r) t
where:
Bt= value of the benefits in year t (monetary value of the additional days ofwork gained because of the antimalaria program);
Ct = value of the costs in year t (sum of the incremental costs of theantimalaria program);
t year
r internal rate of return
To determine the value of the benefits the following hypotheses were made inconstructing Exhibit 1:
a. The annual parasitology index (API) would be reduced to 22 per 1,000(0.022) in 1981, 0.043 in 1982, 0.040 in 1983, and 0.035 from 1984 until2000;
b. The number of days of work lost due to malaria spells was on the averagesix per year;
c. The economically active population (EAP) corresponded to 65.77 percent ofthe total population;
d. The number of working days corresponded on the average in Rondonia to 60percent of the total number of days in a year;
e. The average daily wage was US$5.00 per day;
f. The incremental costs of the antimalaria program were calculated bySUCAM. They are equal to the sum of recurrent and capital costs. Theyconsist of the additional costs of spraying DDT, paying additional personnelto be recruited to implement the additional activities, the costs of newvehicles needed and the costs of their maintenance, and the costs ofadditional medicines needed.

Antimalaria Program in Northwestern Brazil: A Cost-Benefit Analysis 231
EXHIBIT 1 1COST-BENEFIT ANALYSIS
(continued)
Having these hypotheses in mind, the numbers in Exhibit 1 were derived in thefollowing manner:
a. The number of cases of malaria avoided was determined by multiplying thereduction in the API by the estimated population. For example, for 1985 thenumber of cases of malaria avoided, 46.90, was equal to 0.035 times 1,340.
b. The same parameter 0.035 holds true for the period 1986-2000 (you can doan exercise for the years 1981-1984 using the information given in a).
c. The product of the number of working days lost due to malaria (6) times theproportion of the total population that is economically active (0.6577) timesthe proportion of days of the calendar year that are working days (0.6)multiplied by the number of cases of malaria avoided will produce anestimate of days of work gained because of the antimalaria program. Forexample, for 1985: 6 x 0.6577 x 0.6 x 46.90 = 111 .04.
d. The monetary value of the number of working days gained is obtained bymultiplying the number of days by US$5.00. Thus for 1985 we have:111.04 x US$5.00 = US$555.20.

232 Section Two: Applied Experiences in Health Economics and Financing
Source Documents
Boulos, Marcos, Ronaldo Gryschek, and Segurado Aluisio. 1986. "I - Evaluation ofthe Malaria Control Project; n - Evaluation of the Health Services and Health Policyin Rondonia." University of Sao Paulo, Institute of Economic Research. Processed.In Portuguese.
Fivza Lima, J.T., 1985. XXII Congress of the Brazilian Society of TropicalMedicine.
Institute of Economic Research. 1981. "Cost-Benefit Analysis for the MalariaControl Program." Sao Paulo, Brazil: University of Sao Paulo. In Portuguese.
Ministry of Health. 1982. Illnesses and Human Migration. Brasilia, Brazil. InPortuguese.
World Bank. 1981. "Staff Appraisal Report: Brazil Northwest Region IntegratedDevelopment Program, First Phase, Health Project," Washington, D.C.

fl*cI-r4
h.ifnrc of COLOMBIA HONG KONGh MACAO JAMAICA NIGERIA RUSSIAN FEDERATION ADECO Van Dermen Edilons
Distrbutors of llnoenlace Ltda. Asia 2000 Ltd Ian Randle Pubitshers Ltd. University Press Limited lsdatelsato <Ves Mir, Technique
'W orld Bank Carrera 6 No. 51-21 Sales & Circulation Department 206 Old Hope Road Three Crowns Building Jericho 9a, Lopachniy Pereulok Ch. de Lacuez 41
Apartado Aereo 34270 Seabird House, unt 1101-02 Kingtson 6 Private Mail Bag 5095 Moscow 101831 CHl607Blonay
Publications Santate de Bogota, D.C. 22-28 Wyndham Street Central Tel: 809-927-2085 ltadan Tel: (7 095) 917 87 49 Tet: (41 2t) 943 2673
Prices and credit terms vary T el (57 1)285-2798 Hong Kong Fax: 8098977-0243 Tet: (234 22) 41-1306 Fun: (7095) 9t7 9259 Fa: (41 2t) 943 3605
frmcutyto coontry. Fan: (57 1) 285-2798 Tel: (852) 2530-1409 E-mail: [email protected] Fee: (234 22) 41-2056SIGPR,TWA,ANNAfrom countrft Iy Fax: (852) 2526-1107 SNGAPORE TAIWAN TANZANIA
Consult your local distributor CYPRUS E-mait saIesOasia2000.com.hk JAPAN NORWAY MYANMAR, BRUNEI Oxford Universay Press
before placing an order. Center lor Applied Research URL: rtpJtww/ asia2008.coM.hk Eastern Book Service NIC Into AVS Asahgate Piblishing Asia Maktaba Street
Cyprus College 3-13 Hongo 3-chome, Bunkyo-k" Book Department Pacifc Pte. Ltd. PO Boo 5299
6, Diogenes Street, Engomi INDIA Tokyo 113 PO. Box 6125 Enerstad 41 Kallang Pudding Road 004-03 Dar es Salaam
ARGENTINA PO. Box 2006 Alled Pubdishers Ltd. Tel: ()1 3) 3818-0861 N-0602 Oslo 6 Golden Wheel Building Tel: (255 S1) 29209
Oficina del Lbro Internacional Nicosia 751 Mount Road Fax (81 3) 3818B0864 Tel: (47 22) 57-3300 Singapore 349316 Fax: (255 S1) 46822
Av. Cordoba 1877 . Tel: (3572)44-1730 Madras - 608 002 E-mail: svt-ebsOppp.bekkoame.or.p Fax: (47 22) 68-1901 Tel: (65) 741-5166
1120 Baenos Ares Far (3572) 46-2051 Tel: (91 44)852-3938 URL: hlttpAww.bekkoame.or.9V-svt-ebs Fan: (65)742-9358 THAILAND
Tel (54 1)815-8354 Fax: (91 44)852-0849 PAKISTAN E-mail: [email protected] CentalBonesDiebibatle
Fax (54 1) 815-8156 CZECH REPUBUC KENYA Mirza Book Agercy 306 Silom Road
Nabonal lnlormafbon Center INDONESIA Atrica Book Service (E.A) Ld. 65, Shahrahle-Oaaid-e-Azam SLOVENIA Bangkok 10500
AUSTRAUA, FJ, PAPUA NEW GUINEA, prodeiaa, KornikMa S Pt lnd a Lemaed Ouaran House, Mtangano Street Lahore 54000 GospDdarslb Vestnik Pubitshing Group Tel: (6 2) 235-5400
SOLOMON ISLANDS, VANUATU, AND CS- 113 57 Praguee JalanBorobudur20 PO. Box 45245 Tel: (9242)7353801 Dunakacesta S Fax: (682)237-8321
WESTERN SAMOA Tel: (42 2) 2422-9433 PO. Box 181 Nairobi Fax: (92 42) 758 5283 1000 Lkjudana
D.A. lnformatin Services Fax (422)2422-1484 Jakarta 10320 Tel: (2542)223 641 Tel: (3886 1)1338347; 1321230 TRINIDAD & TOBAGO
648 Wtehorse Road URL htptiww.anS.czt Tel: (62 21) 390-4290 Fao (2542)330 272 Oxford University Press Far (386 61) 133 8030 AND THE CARRIBBEAN
Mftcham 3132 Fax: (6221)421-4289 5 Bangalore Town E-mail: belicd@gvestrksi Systemabc SWtaes LInt
Victoria DENMARK KOREA, REPUBUC OF Sharae Fasal 9 Wae Street
Tel: (61) 39210 7777 SamfundseLatur IRAN Daepon Tracbng Co. Ltd. PO Box 13033 SOUTH AFRICA, BOTSWANA Curepe
Far (61)392107788 Roseeoaemsa Al 11 Ketab Sara Co. Publtshers PO. Box 34, Youida Karachim75350 Forsinrgle Uas: Trnkada, Wesa Indes
E-mail: [email protected] DK-1970 Frederikbeng C Khaled Eslambo Ave., 706 SeounBldg Tel: (92 21) 440307 Oxford University Press Tel: (809)662-5654
URL: hletil:ndadirectcom.au Tel: (4531) 351942 6h Strees 44-6 Youido-Dorng, Yeongchengpo-Ku Fax: (92 21) 4547640 Southem Africa Fax: (809)662-58654
Fax (4531)357822 KurIheh Delatrooz Nc. 8 Send E-maail:[email protected] PO. Box1141 E-madl: [email protected]
AIJSTRIA PO. Box 15745-733 Tel: (822)785-163V14 Cape Town 8000
Gerald rand Co. EGYPT ARAB REPUBUC OF Tehran Fax (82 2) 784-8315 Pak Book Corporation Tel: (27 21) 45-7266 UGANDA
Weihburggasse 26 Al Ahram DiEsbune Agerry Tel: (9821) 8717819; 8716104 Aziz Chafbers 21 Fax (2721)45-7265 GuatraLtd.
A-10 I Wien Al Galaa Streel Fax: (9821)8712479 MALAYSIA Queens Road PO Box 9997
Tel (431) 512-47-3140 Cairo E-maitl: [email protected] UnrverayofMalyaCooperateve Lahore Formsubscriion orders: MadtianiiBuildirrg
Fax: (43 1) 512-47-31-29 Tel: (202) 578883 Bookshop, Ufnted Tel: (9242)6363222; 638 0885 lntematonal Subscr5pVeSernic Plot 614JirjaRd.
URL: htpilnwA.g&rold.colatonflire Far (202)578-683 KowkabPublhers PO. Box1127 Fax: (9242)6362328 PO. Box 41095 Kampala
PO. Box 19575-t11 Jala nPantai Baru E-mail: pbcobrain.net.pk Craigha1 Teo: (25641)254 763
BANGLADESH The Middle East ObseNer Tehran 59780 Kuala Lumpr Johannesburg 2024 Fax: (256 41) 251 468
MicrolndustriesDeweloprrent 41, SheritSLeet Tel: (982t)258-3723 Tel (603)756-5000 PERU Tel: (27 1t)880-t448
Assistance Society (MIDAS) Cairo Fax: (98 21) 258-3723 Fax: (603) 755-4424 Editorial Desarrollo SA Far (27 11)880-6248 UNWEDKINGDOM
House 5, Road 16 Tel: (20 2) 393-9732 Apartado 3824 E-mail: isesis.co.za Microinto Ltd.
Dhaamondi FlArea Fax: (202)393-9732 IRELAND MEXICO Lima 1 PO. Box 3
Dhaka 1209 Govemment Supplies Agercy INFOTEC Tel: (51 14) 285380 SPAIN Aton, Hampshire GU34 2PG
Tel: (8802) 326427 RNLAND Ortig an tSolathair Av. San Famando No. 37 Fax: (51 14) 286628 MundiPrensa Libros, SA. England
Fax: (8802) 811185 Akateerrinren Kirialaappa 4-5 Harcourt Road Co. Toriello Guerra Castello 37 Tel: (44 t420) 86848
PO Box 128 Dublin 2 14050 Mexico, D F PHIUPPINES 28061 Madrid Fax: (44 1420) 689
BELGIUM FIN-D0101 Helaid Tel: (353 1)681-311I Tel: (52 5)624-2800 interanaeonal Booksource Coler Inc Tel. (34 1) 431-3399 E-mail: wbank@ukminlo demon co uk
Jean De Lannoy Tel: (3580) t2141 Fax: (353 1)475-2670 Far (52 5)624-2822 1127-A Antipolo St. Fax: (34 1)575-3998 URL. httpJtnwwrmcroinao.co.uk
Av. du Roi 202 Far (358 0) t21-4441 E-mail: [email protected] Barangay, Venezuela E-mail: libreria@mundiprensa es
1060 Banmes URL: hapJ1ookinetcultnet.flakl ISRAEL URL: hftpJlrtn.net.mx MakhCity URL: htpihww.mundiprensa.esf VENEZUELA
Tel: (32 2( 538-5168 Yozmot Uteratare Ltd. Tel: (622)69 8 6501; 6505; 6507 TecralCientcia Lbros, S.A.
Far (32 2) 538-084 FRANCE PO. Box 58055 NEPAL Fax: (63 2) 896 1741 Munhd-Preesa Barcelona Ceare Caidad Comcral Tamaaco
Word Bank Pdticabons 3 Yohanan Hasandlar Street Everest Media Intemabonal Consell de Cent 391 Nivel C2
BRAZIL 68, avenue dlna Tel A"! 61580 Services (P) Ltd. POLAND 08009 Barcelona Caracas
Publicacoes Tecnicas laternacionars 75116 Pars Tel: (9723)5285-397 GPO Box 5443 international Publishing Service Tel: (343)488-3492 Tel: (582)9595547;5035, 0016
LUda. Tel: (33 1) 40469-30-56/57 Fax: (9723)5285-397 Kathmandu Ul. Piekna 337 Fax: (34 3)487-7659 Fax: (582) 959 5636
Rua PeLxoto Gomride, 209 Far (33 1) 404-9-30-68 Tel: (977 1) 472 152 00-677 Warzawa
01409 Sao Pauli, SP R.O.Y Intemartonal Far (977 1) 224 431 Tel (48 2) 628-6089 SRI LANKA, THE MALDIVES ZAMBIA
Tel (55 11) 25-6644 GERMANY PO Box 13056 Fax: (48 2) 621-7255 Lake Hout Bookshop University Bookshop
Fan: (55SIt) 256-6880 IUNO-Vedag Tel A"! 61130 NETHERLANDS E-mail: books%pseikp.atm.com.pl 100, Sir Chittampalam GardmneoMawatha Universly ofZarrbe
E-mail: [email protected] Poppeldtter Mee 55 Tel: (972 3)5461423 De LindeboomAnOr-Publikaties URL htpJwwwip009.waWpveiaXpoC(1 Colombo2 GreatEastRoadCairus
URL: htrpJAhww.ul.br 531t5 Bon Fax: (9723)5481442 PO. Box 202 Tel: (94 1) 32105 PO. Box 32379
Tel: (49228)212940 E-malt [email protected] 7480 AE Haaksbergen PORTUGAL Far (94 1)432104 Lusaka
CANADA Fax (49228) 217492 Tel: (31 53)574-0D04 Lvraria Portugal Tel: (280 1)252576
Renout PubitEhng Co. Ltd. Paleman Authority/Middle East Far (31 53) 572-9296 Apartado 2681 SWEDEN Fax: (260 1)253952
5369 Canotek Road GREECE Irdex loenrmatbn SerANc E-man: lindlboowordlonline.rn Rua Do Camao 70-74 Wennergren-W8liarms AB
Onawa, Ontario KIJ 9J3 Papasonriou S.A. PO.B. 19502 Jerunalem URL: httpJiww.wonrdnine.nl-Ideb0oo 1208Lsbon P[e. Box 1305 ZIMBABWE
Tel: (613) 745-2665 35, Stoumara tr. Tel: (972 2) 6271219 Tel: (1) 347-4982 S-171 25 Solna Longman Zimbabwe (Pte.)Ltd.
Far (613)745-7660 106 82Arhens Fax: (9722)6271634 NEWZEALAND Fax: (1)347-0264 Tel: (468)705-97-50 Toude Road, Adbennie
E-mail: [email protected] Tel: (301) 364-182 EBSCO NZ Ltd. Far (458)27-00-71 PO. Box STt25
URL: htpJ wwtfox.rstr.cal-renout Far (301)364-8254 ITALY Privale Mad Bag 999t4 ROMANIA Southenton
Licosa ComrrisiDnaria Sansoni SPA New Market Compani De Lbrarii Bucuresb S.A. SWITZERLAND Hararare
CHtNA HAITM Via Duca Di Caobrta, it Aucidand Str Lipscani no. 26, sector 3 Lbairie Payot ket (263 4) 6216617
Chinra Fnarcil&Economk CLnjreeDffdaon Caelb Posate 552 Tel: (649)524-8119 Bucharest Serace lnstiturionnel Fax: (2634)621670
Pubieshig Hea B, Rue Capals 50125 Firenze Far (64 9) 524-07 Tel: (40 t) 613 9645 Cotea-de-Montbenon 30
8, Da FoSi Dong Jie C.P 257 Tel: (55)645-415 Fax: (4031)32440800 1002Lausanne
Beijing Pon-au-Pdrce Fax: (5() 641-257 Tel: (41 21) 341-3229
Tel: (86 10) 6333-8257 Te3: (509 1) 3 9280 E-edit [email protected] Far (41 21) 34t-3235
Far (86 10) 640t-7365 ULd: htprJywi.ltbc.tlicosa ru



31The World Bank
I~~~~~ I
; i . | ' I. *
! ! !~ ! S S _ .5 Si.5 z
.,5.5 .* .
_ 5 l' S
*:^w - * S
Sll Z b b ' S
I OS . 'S S; 5
is iS S - - L5
S i. itii
111 r I IISsa 302IIjlIIIlI
9l31_40 1 95
ISB 08 13-3012-8w1




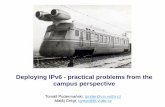




![[] Practical Problems in Soil Mechanics and Foundation](https://static.fdocuments.us/doc/165x107/577c807b1a28abe054a8e138/-practical-problems-in-soil-mechanics-and-foundation.jpg)







