POINSETT PSYCHIATRIC INNOVATIONS, PA · Poinsett PSYCHIATrIC INNOVATIONS, PA Page 4 of 4 ......
10
Poinsett PSYCHIATrIC INNOVATIONS, PA Page 1 of 4 1/1/2016 POINSETT PSYCHIATRIC INNOVATIONS, PA 414 Pettigru St., Suite C ▪ Greenville, SC 29601 ▪ Phone: 864.404.9706 ▪ Fax: 864.438.4744 Adult Intake Form Place Patient Label Here
Transcript of POINSETT PSYCHIATRIC INNOVATIONS, PA · Poinsett PSYCHIATrIC INNOVATIONS, PA Page 4 of 4 ......

Poinsett PSYCHIATrIC INNOVATIONS, PA Page 1 of 4 1/1/2016
POINSETT PSYCHIATRIC INNOVATIONS, PA
414 Pettigru St., Suite C ▪ Greenville, SC 29601 ▪ Phone: 864.404.9706 ▪ Fax: 864.438.4744
Adult Intake Form Place Patient
Label Here

Poinsett PSYCHIATrIC INNOVATIONS, PA Page 2 of 4 1/1/2016
Name: __________________________________
Place patient
Label here
Poinsett PSYCHIATrIC INNOVATIONS, PA Page 3 of 4 1/1/2016
Name: __________________________________
Place patient
Label here

Poinsett PSYCHIATrIC INNOVATIONS, PA Page 4 of 4 1/1/2016
Name: __________________________________
Place patient
Label here

PPI New Patient Information Form.dotx 1/1/2016
POINSETT PSYCHIATRIC INNOVATIONS, PA
414 Pettigru St., Suite C ▪ Greenville, SC 29601 ▪ Phone: 864.404.9706 ▪ Fax: 864.438.4744
New Patient Information (Please PRINT information below)
Preferred
Name: _____________________________________________________ Name: ______________________ First Middle Initial Last
Street Address: _______________________________________________________________________________________
City: _____________________________________ State: ________________ Zip Code: ___________________________
Main Phone: ( ) _______________________ Home Work Cell Other ____________________
Birthdate: _______________________________ Social Security Number: __________________________________
Driver’s License or Government Issued ID: _____________________________________________________________ Issuing State / License or ID number License or ID?
Marital Status: Single Married Widowed Partnered Sex: Male Female
Legally Separated Divorced Other
INSURANCE INFORMATION: We do not accept direct payment from any insurance companies, but we keep
your insurance information on file in case of medication preauthorization. PLEASE BRING YOUR INSURANCE
CARD WITH YOU TO YOUR APPOINTMENT.
Insurance Company: ________________________________ Type: Group Non-Group Supplement
ID Number: _________________________________________ Group Number: ______________________________
Subscriber Name: ____________________________________________ Birthdate: ________________________
Relationship to Subscriber: Self Spouse Parent Other
ADDITIONAL CONTACT INFORMATION
Secondary Phone: ( ) _______________________ Home Work Cell Other
Home E-mail: _________________________________ Work E-mail: _______________________________________
Emergency Contact Name: ________________________________________________________________________
Emergency Contact Phone: ___________________________________ Home Work Cell Other
Relationship to you: __________________________________________
Your Primary Care Provider: _________________________________________ Phone: _______________________
Other Provider: _____________________________________________________ Phone: _______________________
Pharmacy Name: ___________________________________________________ Phone: _______________________
Pharmacy Location: _______________________________________________________________________________ Street name City
APPOINTMENT REMINDER METHOD (Check all that apply)
Home E-mail Work E-mail Phone: Home Work Cell: Call OR Text
FOR OFFICE USE ONLY: Driver’s License copy Insurance Card copy PI PI/S TMS
Information entered to EMR by__________________________________________________________ on __________________________

414-C Pettigru St., Greenville, SC 29601
Tel. 864.404.9706 Fax 864.438.4744
Poinsett Psychiatric Innovations, PA Place Patient
Label Here
Clinician
Use
Very False or
Often False
Sometimes or
Somewhat
False
Sometimes or
Somewhat
True
Very True or
Often True
Item
Score
1 People would describe me as reckless. 0 1 2 3
2 I feel like I act totally on impulse. 0 1 2 3
3 Even though I know better, I can't stop making rash decisions. 0 1 2 3
4 I often feel like nothing I do really matters. 0 1 2 3
5 Others see me as irresponsible. 0 1 2 3
6 I'm not good at planning ahead. 0 1 2 3
7 My thoughts often don't make sense to others. 0 1 2 3
8 I worry about almost everything. 0 1 2 3
9 I get emotional easily, often for very little reason. 0 1 2 3
10 I fear being alone in life more than anything else. 0 1 2 3
11I get stuck on one way of doing things, even when it's clear it
won't work.0 1 2 3
12 I have seen things that weren't really there. 0 1 2 3
13 I steer clear of romantic relationships. 0 1 2 3
14 I'm not interested in making friends. 0 1 2 3
15 I get irritated easily by all sorts of things. 0 1 2 3
16 I don't like to get too close to people. 0 1 2 3
17 It's no big deal if I hurt other peoples' feelings. 0 1 2 3
18 I rarely get enthusiastic about anything. 0 1 2 3
19 I crave attention. 0 1 2 3
20I often have to deal with people who are less important than me.
0 1 2 3
21I often have thoughts that make sense to me but that other
people say are strange.0 1 2 3
22 I use people to get what I want. 0 1 2 3
23I often "zone out" and then suddenly come to and realize that a
lot of time has passed.0 1 2 3
24 Things around me often feel unreal, or more real than usual. 0 1 2 3
25 It is easy for me to take advantage of others. 0 1 2 3
Total/Partial Raw Score:
Prorated Total Score: (if 1-6 items left unanswered)
Krueger, RF, Derringer J, Markon KE, Watson D, Skodol AE.
Copyright © 2013 American Psychiatric Association. All Rights Reserved.
This material can be reproduced without permission by researchers and by clinicians for use with their patients.
The Personality Inventory for DSM-5 -- Brief Form (PID-5-BF) -- Adult
Name: ___________________________________________ Age: _______ Sex: Male Female Date: _____________________
Average Total Score:
Instructions: This is a list of things different people might say about themselves. We are interested in how you would describe
yourself. There is no right or wrong answers. So you can describe yourself as honestly as possible, we will keep your responses
confidential. We'd like you to take your time and read each statement carefully, selecting the response that best describes you.
PPI New Patient Personality Inventory for DSM 5.xlsx
414-C Pettigru St., Greenville, SC 29601
Tel. 864.404.9706 Fax 864.438.4744
Poinsett Psychiatric Innovations, PA Place Patient
Label Here
Clinician
Use
In the past SEVEN (7) days . . . Never Rarely Sometimes Often Always Item Score
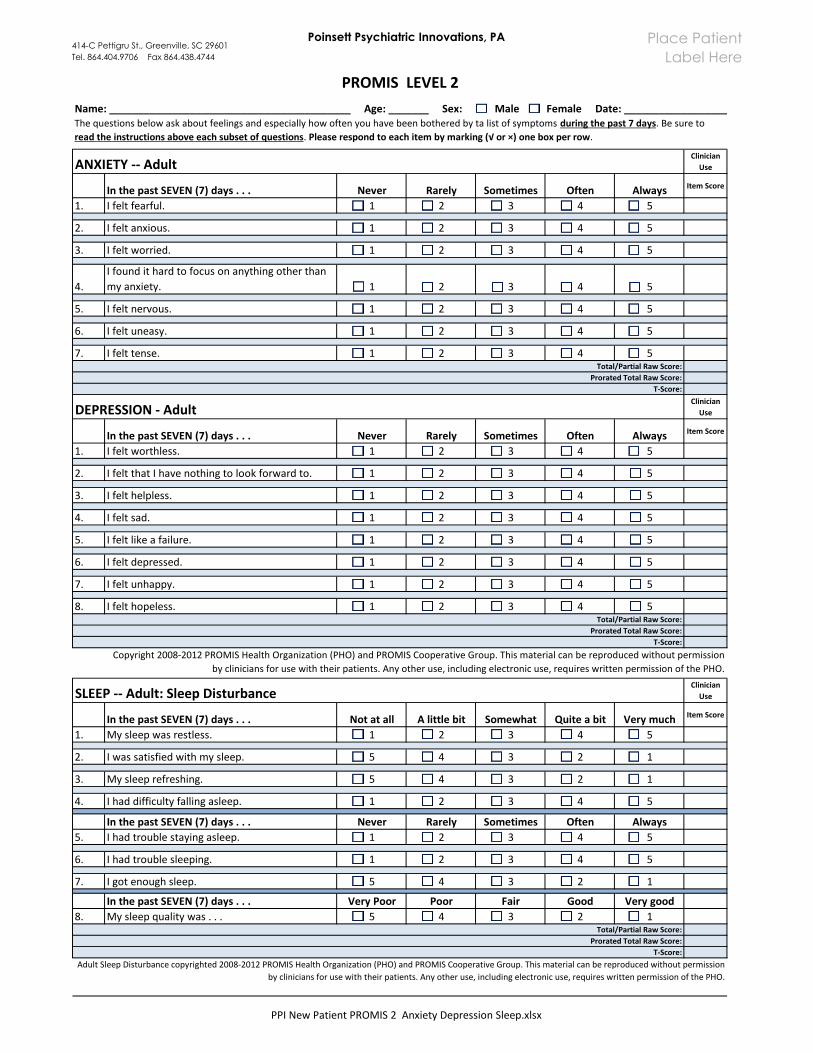
1. I felt fearful. 1 2 3 4 5
2. I felt anxious. 1 2 3 4 5
3. I felt worried. 1 2 3 4 5
4.
I found it hard to focus on anything other than
my anxiety. 1 2 3 4 5
5. I felt nervous. 1 2 3 4 5
6. I felt uneasy. 1 2 3 4 5
7. I felt tense. 1 2 3 4 5
Clinician
Use
In the past SEVEN (7) days . . . Never Rarely Sometimes Often Always Item Score
1. I felt worthless. 1 2 3 4 5
2. I felt that I have nothing to look forward to. 1 2 3 4 5
3. I felt helpless. 1 2 3 4 5
4. I felt sad. 1 2 3 4 5
5. I felt like a failure. 1 2 3 4 5
6. I felt depressed. 1 2 3 4 5
7. I felt unhappy. 1 2 3 4 5
8. I felt hopeless. 1 2 3 4 5
Clinician
Use
In the past SEVEN (7) days . . . Not at all A little bit Somewhat Quite a bit Very much Item Score
1. My sleep was restless. 1 2 3 4 5
2. I was satisfied with my sleep. 5 4 3 2 1
3. My sleep refreshing. 5 4 3 2 1
4. I had difficulty falling asleep. 1 2 3 4 5
In the past SEVEN (7) days . . . Never Rarely Sometimes Often Always
5. I had trouble staying asleep. 1 2 3 4 5
6. I had trouble sleeping. 1 2 3 4 5
7. I got enough sleep. 5 4 3 2 1
In the past SEVEN (7) days . . . Very Poor Poor Fair Good Very good
8. My sleep quality was . . . 5 4 3 2 1
Copyright 2008-2012 PROMIS Health Organization (PHO) and PROMIS Cooperative Group. This material can be reproduced without permission
by clinicians for use with their patients. Any other use, including electronic use, requires written permission of the PHO.
Total/Partial Raw Score:
Total/Partial Raw Score:
Prorated Total Raw Score:
T-Score:
SLEEP -- Adult: Sleep Disturbance
T-Score:
Adult Sleep Disturbance copyrighted 2008-2012 PROMIS Health Organization (PHO) and PROMIS Cooperative Group. This material can be reproduced without permission
by clinicians for use with their patients. Any other use, including electronic use, requires written permission of the PHO.
Total/Partial Raw Score:
Prorated Total Raw Score:
PROMIS LEVEL 2
The questions below ask about feelings and especially how often you have been bothered by ta list of symptoms during the past 7 days. Be sure to
read the instructions above each subset of questions. Please respond to each item by marking (√ or ×) one box per row.
Name: __________________________________________ Age: _______ Sex: Male Female Date: _____________________
Prorated Total Raw Score:
T-Score:
ANXIETY -- Adult
DEPRESSION - Adult
PPI New Patient PROMIS 2 Anxiety Depression Sleep.xlsx

414-C Pettigru St., Greenville, SC 29601
Tel. 864.404.9706 Fax 864.438.4744
Poinsett Psychiatric Innovations, PA
Not at all
One or two
days Several daysMore than half
the days
Nearly every
dayItem
Score
a. Painkillers (like Vicodin) 0 1 2 3 4
b. Stimulants (like Ritalin, Adderall) 0 1 2 3 4
c. Sedatives or tranquillizers (like sleeping pills or 0 1 2 3 4
d. Alcohol (like beer, wine, liquor) 0 1 2 3 4
e. Nicotine (like cigarettes, e-cigarettes, chewing 0 1 2 3 4
f. Marijuana 0 1 2 3 4
g. Cocaine or crack 0 1 2 3 4
h. Club drugs (like ecstasy) 0 1 2 3 4
i. Hallucinogens (like LSD) 0 1 2 3 4
j. Heroin 0 1 2 3 4
k. Inhalants or solvents (like glue) 0 1 2 3 4
l. Methamphetamine (like speed) 0 1 2 3 4
Clinician
Use
In the past SEVEN (7) days . . . Never Rarely Sometimes Often AlwaysItem
Score
1. I was irritated more than people knew. 1 2 3 4 5
2. I felt angry. 1 2 3 4 5
3. I felt like I was ready to explode. 1 2 3 4 5
4. I was grouchy. 1 2 3 4 5
5. I felt annoyed. 1 2 3 4 5
©2008-2012 PROMIS Health Organization (PHO) and PROMIS Cooperative Group.
This material can be reproduced without permission by clinicians for use with their patients.
ANGER -- Adult: Emotional Distress
The questions below ask about feelings and especially how often you have been bothered by a list of symptoms during the
past 7 days. Be sure to read the instructions above each subset of questions.
Please respond to each item by marking (√ or ×) one box per row.
Place Patient
Label Here
Total/Partial Raw Score:Prorated Total Raw Score:
T-Score:
Courtesy of National Institute on Drug Abuse.
Name: ___________________________________________ Age: _______ Sex: Male Female Date: _____________________
Or drugs like:
Total Score:
SUBSTANCE USE -- Adult: Adapted from the NIDA-Modified ASSISTDuring the past TWO (2) WEEKS, about how often did you use any of the following medicines ON YOUR OWN, that is, without a
doctor's prescription, in greater amount or longer than prescribed?
PPI New Patient PROMIS 2 Anger Substance.xlsx

1.2.3.
4.
Clinician Use
Item Score
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
Copyright 1997, with permission from Elsevier.
Not
bothered
at all (0)
Bothered
a little (1)
Always
(2)
Clinician Use
Item Score
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Total/Partial Raw Score:
Prorated Total Raw Score:
I have often been more active than usual.
SOMATIC SYMPTOMS -- Adult
I often feel happier or more cheerful than usual.
I feel happier or more cheerful than usual most of the time.
Question I
I have frequently been more active than usual.
I am constantly more active or on the go all the time.
Name: ______________________________________ Age: _______ Sex: Male Female Date: _____________
Reprinted from Altman EG, Hedeker D, Peterson JL, Davis JM: The Altman Self-Rating Mania Scale. Biological Psychiatry 42: 948-955, 1977
The questions below ask about these feelings in more detail and especially how often you have been bothered by a list of
symptoms during the past SEVEN (7) days. Please respond to each item by marking (√ or X) one box per row.
Please read each group of statements/question carefully.
Choose the one statement in each group that best describes the way you have been feeling for the past week.
Please note: The word "occaionally" when used here means once or twice; "often" means several times or more and "frequently"
means most of the time.
Question 2
I do not feel more self-confident than usual.
I occasionally feel more self-confident than usual.
I often feel more self-confident than usual.
I frequently feel more self-confident than usual.
I feel lextremely self-confident all of the time.
Question 3
I do not need sleep less than usual.
I occasionally need less sleep than usual.
I occasionally feel happier or more cheerful than usual.
Check the box (√ or X) next to the number/statement selected.
I talk constantly and cannot be interrupted.
Question 5
I have not been more active (either socially, sexually, at work, home, or school) than usual.
I have occasionally been more active than usual.
Question 4
I do not talk more than usual.
I occasionally talk more than usual.
I often talk more than usual.
I frequently talk more than usual.
I feel happier or more cheerful than usual all of the time.
I often feel need less sleep than usual.
I frequently need less sleep than usual.
I can go all day and all night without any sleep and still not feel tired.
MANIA -- Adult
I do not feel happier or more cheerful than usual.
Stomach pain
Back pain
Pain in your arms, legs, or joints (knees, hips, etc.)
Menstral cramps or other problems with your periods (WOMEN ONLY)
Headaches
Chest pain
Dizziness
Fainting spells
Feeling your heart pound or race
Shortness of breath
Adapted from Physical Symptoms (PHQ-15) for research and evaluation purposes.
Prorated Total Raw Score (if 1-3 items left unanswered):
Pain or problems during sexual intercourse
Constipation, loose bowels, or diarrhea
Nausea, gas, or indigestion
Feeling tired or having low energy
Trouble sleepingTotal/Partial Raw Score:
PPI New Patient PROMIS 2 Mania Somatic Symptom.xlsx
Place Patient
Label Here
Poinsett Psychiatric Innovations, PA414-C Pettigru St., Greenville, SC 29601
Tel. 864.404.9706 Fax 864.438.4744

Poinsett Psychiatric Innovations, PA
PPI New Patient Repetitive Thoughts Acute Stress.dotx 1/1/2016
414-C Pettigru St., Suite C, Greenville, SC 29601
Tel. 864.404.9706 Fax 864.438.4744
Name: ________________________________________________ Age: ______ Sex: Male Female
Date: _______________________
Severity of Acute Stress Symptoms – Adult* Instructions: People sometimes have problems after extremely stressful events or experiences. How much have you been bother during the PAST SEVEN (7) DAYS by each of the following problems that occurred or became worse after an extremely stressful event/experience? Please respond to each item by marking (√ or x) one box per row.
*National Stressful Events Survey Acute Stress Disorder Short Scale (NSESS), Kilpatrick DG, Resnick, HS, Friedman, MJ Copyright © 2013 American Psychiatric Association. All rights reserved.
This measure can be reproduced without permission by researchers and by clinicians for use with their patients.
PROMIS—Repetitive Thoughts and Behaviors—Adult* Instructions: The questions below ask about these feelings and especially how often you have been bothered by the list of symptoms during the past 7 days. Please respond to each item by marking (√or x) one box per row.
*Adapted from the Florida Obsessive-Compulsive Inventory (FOCI) Severity Scale (Part B) © 1994 Wayne K. Goodman, MD and Eric Storch, PhD. This material can be reproduced withoutpermission by clinicians for use with their own patients. Any other use, including electronic use, requires written permission from Dr. Goodman ([email protected])
Please list the traumatic event that you experienced: __________________________________________________________ Clinician Use
Date of the traumatic event: ______________________ Not
at all A little
bit Moderately
Quite a bit
Extremely Item Score
1 Having “flashbacks,” that is, you suddenly acted or felt as if a stressful experience from the past was happening all over again (for example, you re-experienced parts of a stressful experience by seeing, hearing, smelling, or physically feeling parts of the experience)? 1 2 3 4 5
2 Feeling very emotionally upset when something reminded you of a stressful experience? 1 2 3 4 5
3 Feeling detached or distant from yourself, your body, your physical surroundings, or your memories? 1 2 3 4 5
4 Trying to avoid thoughts, feelings, or physical sensations that reminded you of a stressful experience? 1 2 3 4 5
5 Being “super alert,” on guard, or constantly on the lookout for danger? 1 2 3 4 5
6 Feeling jumpy or easily startled when you hear an unexpected noise? 1 2 3 4 5
7 Being extremely irritable or angry to the point where you yelled at other people, got into fights, or destroyed things? 1 2 3 4 5
Total/Partial Raw Score:
Prorated Total Raw Score: (if 1 item left unanswered)
Average Total Score:
Clinician Use
During the past SEVEN (7) DAYS . . . Item Score
1. On average, how much time is occupied by these thoughts or behaviors each day? 0 -- None
1 – Mild (Less than an hour a day)
2 – Moderate (1 to 3 hours a day)
3 – Severe (3 to 8 hours a day)
4 – Extreme (more than 8 hours a day)
2. How much distress do these thoughts or behaviors cause you?
0 -- None 1 – Mild (slightly
disturbing)
2 – Moderate (disturbing but still
manageable) 3 – Severe (very
disturbing)
4 – Extreme (overwhelming
distress)
3. How hard is it for you to control these thoughts or behaviors?
0 – Complete
control
1 – Much control (usually able to
control thoughts or behaviors)
2 – Moderate control (sometimes able to control thoughts or
behaviors)
3 – Little control (infrequently able to control thoughts or
behaviors)
4 – No control (unable to control
thoughts or behaviors)
4. How much do these thoughts or behaviors cause you to avoid doinganything, going anyplace, or beingwith anyone?
0 – No avoidance
1 – Mild (occasional avoidance)
2 – Moderate (regularly avoid doing
these things)
3 – Severe (frequent and extensive
avoidance)
4 – Extreme (nearly complete avoidance;
house-bound)
5. How much do these thoughts or behaviors interfere with school, work,or your social or family life?
0 -- None 1 – Mild
(slight interference)
2 – Moderate; (definite interference with
functioning, but still manageable)
3 – Severe (substantial
interference)
4 – Extreme (near-total interference;
incapacitated)
Total/Partial Raw Score:
Prorated Total Raw Score (if 1 item is left unanswered):
Average Total Score:
Place Patient
Label Here