
PNH: Complications and Long-Term Issuesassets.aamds.org/pdfs/IssuesPNHdeCastro.pdfSlide # 1 PNH:...
22
Slide # 1 PNH: Complications and PNH: Complications and Long Long-Term Issues Term Issues Carlos M. de Castro, MD Duke University Medical Center October 2012 AA&MDSIF Conference PNH: PNH: Comlications Comlications and and Long Long-Term Issues Term Issues What happens to PNH patients? What are the long-term complications of PNH and can they be prevented? – Thrombosis (blood clots) – Renal failure – Pulmonary Hypertension – Development of aplastic anemia, myelodysplastic syndrome, or AML Long term complications of therapy What are some special situations for PNH patients? – Pregnancy – Surgery – Vaccinations What is PNH and what is the long term outlook?
Transcript of PNH: Complications and Long-Term Issuesassets.aamds.org/pdfs/IssuesPNHdeCastro.pdfSlide # 1 PNH:...
Slide # 1
PNH: Complications and PNH: Complications and
LongLong--Term IssuesTerm Issues
Carlos M. de Castro, MD
Duke University Medical Center
October 2012
AA&MDSIF Conference
PNH: PNH: ComlicationsComlications and and
LongLong--Term IssuesTerm Issues
What happens to PNH patients?
What are the long-term complications of PNH and can they be
prevented?
– Thrombosis (blood clots)
– Renal failure
– Pulmonary Hypertension
– Development of aplastic anemia, myelodysplastic syndrome, or AML
Long term complications of therapy
What are some special situations for PNH patients?
– Pregnancy
– Surgery
– Vaccinations
What is PNH and what is the long term outlook?
Slide # 2
Paroxysmal Nocturnal Paroxysmal Nocturnal HemoglobinuriaHemoglobinuria::
Long term outcomesLong term outcomes
100100
8080
6060
4040
2020
00
00 55 1010 1515 2020 2525
Years After DiagnosisYears After Diagnosis
Pati
en
ts S
urv
ivin
g (
%)
Pati
en
ts S
urv
ivin
g (
%)
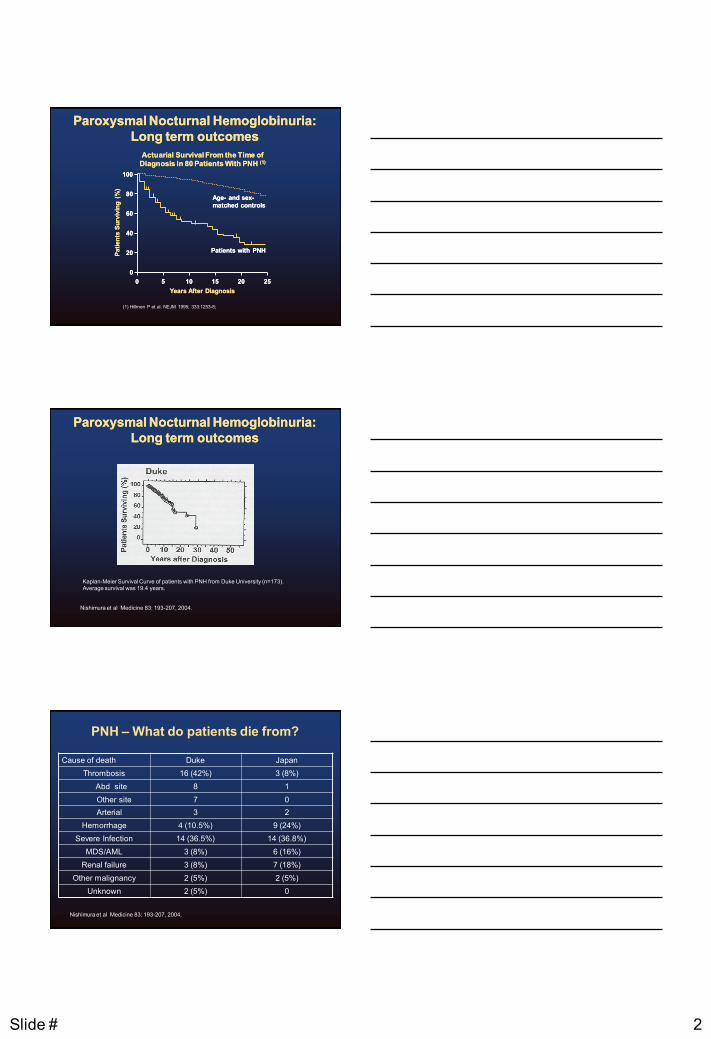
Actuarial Survival From the Time ofActuarial Survival From the Time of
Diagnosis in 80 Patients With PNH Diagnosis in 80 Patients With PNH (1)(1)
AgeAge-- and sexand sex--
matched controlsmatched controls
Patients with PNHPatients with PNH
(1) Hillmen P et al. NEJM 1995; 333:1253-8;
Paroxysmal Nocturnal Hemoglobinuria:Paroxysmal Nocturnal Hemoglobinuria:
Long term outcomesLong term outcomes
Kaplan-Meier Survival Curve of patients with PNH from Duke University (n=173). Average survival was 19.4 years.
Nishimura et al Medicine 83: 193-207, 2004.
PNH – What do patients die from?
Cause of death Duke Japan
Thrombosis 16 (42%) 3 (8%)
Abd site 8 1
Other site 7 0
Arterial 3 2
Hemorrhage 4 (10.5%) 9 (24%)
Severe Infection 14 (36.5%) 14 (36.8%)
MDS/AML 3 (8%) 6 (16%)
Renal failure 3 (8%) 7 (18%)
Other malignancy 2 (5%) 2 (5%)
Unknown 2 (5%) 0
Nishimura et al Medicine 83: 193-207, 2004.

Slide # 3
PNH & Thrombosis
8
PNH & Thrombosis – How do you know if you have a blood clot?
• Symptoms can be quite variable – intense pain, swelling,
shortness of breath, headaches.
• Diagnosis is based on laboratory tests and imaging
studies.
• Ultrasound
• MRI/MR(V or A).
• Blood clots can be life threatening. They require
immediate medical attention.
Thrombosis in PNH
• Recognized early as a problem
• Occurs in ~40% of European-descended populations
– less in East Asian populations
• Is the worst prognostic indicator
• Is the leading cause of death
• Once a thrombosis occurs, no clear evidence that any
anticoagulant will prevent further clots
Slide # 4
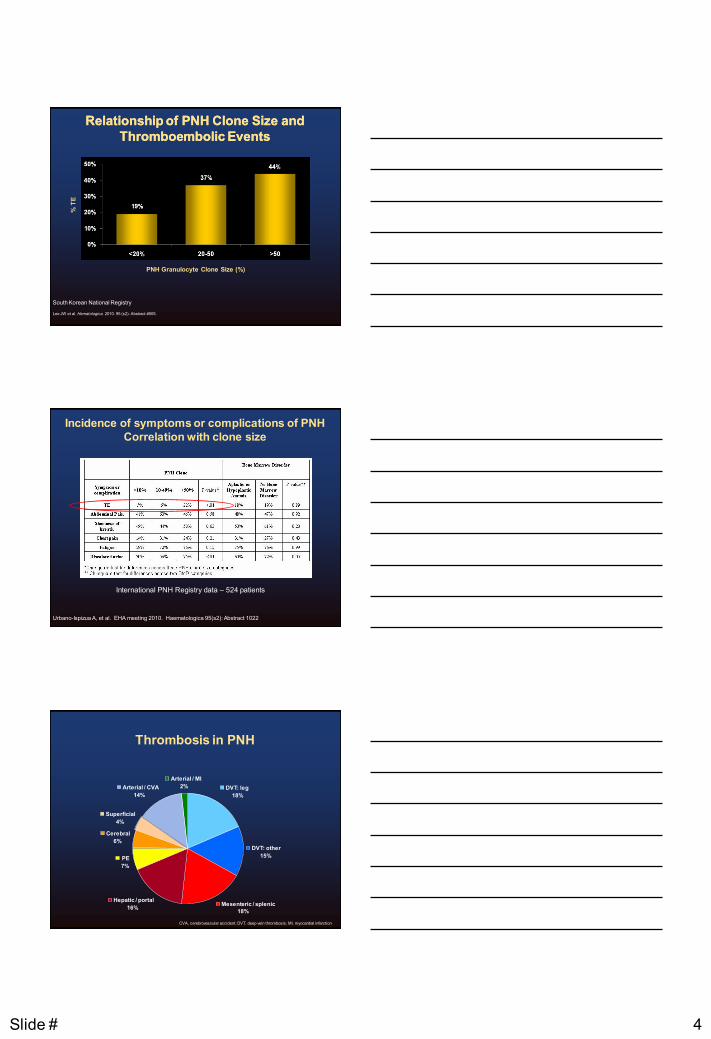
Relationship of PNH Clone Size and Relationship of PNH Clone Size and
Thromboembolic EventsThromboembolic Events
PNH Granulocyte Clone Size (%)
% T
E
Lee JW et al. Hematologica. 2010. 95 (s2): Abstract #505.
South Korean National Registry
Incidence of symptoms or complications of PNH
Correlation with clone size
International PNH Registry data – 524 patients
Urbano-Ispizua A, et al. EHA meeting 2010. Haematologica 95(s2): Abstract 1022
Mesenteric / splenic
18%
Hepatic / portal
16%
PE
7%
Cerebral
6%
Superficial
4%
Arterial / CVA
14%
Arterial / MI
2% DVT: leg
18%
DVT: other
15%
Thrombosis in PNH
CVA, cerebrovascular accident; DVT, deep vein thrombosis; MI, myocardial infarction

Slide # 5
Peculiarities of thrombosis in PNH
• Incidence may be much higher
– small, undetectable thromboses
– D-dimer data
• Once established, tends to recur and continue
– inexorable course of hepatic vein thrombosis
• Incidence lower in East Asian populations
– includes Mexican population
• Role of surgery and pregnancy in initiating thrombosis
• Other risk factors include prolonged immobility, oral contraceptives,
inherited thrombophilia.
Possible causes of thrombosis in PNH
Platelet activation by complement
Role for nitric oxide on platelets and endothelium
ADP release by hemolyzed RBC’s
Reduced expression of urokinase plasminogen activator
receptor
Increased circulating microparticles from lysed RBC’s
How to manage thrombosis in PNHHow to manage thrombosis in PNH
Role of Role of coumadincoumadin prophylaxis to prevent clots remains prophylaxis to prevent clots remains
controversial.controversial.
Patients presenting with an acute clot should undergo Patients presenting with an acute clot should undergo
treatment with a clottreatment with a clot--busting drug busting drug –– TPA, TPA, urokinaseurokinase
Patients should then be on anticoagulant therapy Patients should then be on anticoagulant therapy
((coumadincoumadin, , lovenoxlovenox, , etcetc). ).
Duration Duration -- Probably for their lifetime.Probably for their lifetime.
Patients with a thrombotic event should start Patients with a thrombotic event should start eculizumabeculizumab..
Whether one can stop anticoagulation once Whether one can stop anticoagulation once eculizumabeculizumab is is
started has not been well studied.started has not been well studied.
A bone marrow transplant can be considered.A bone marrow transplant can be considered. 15
Slide # 6
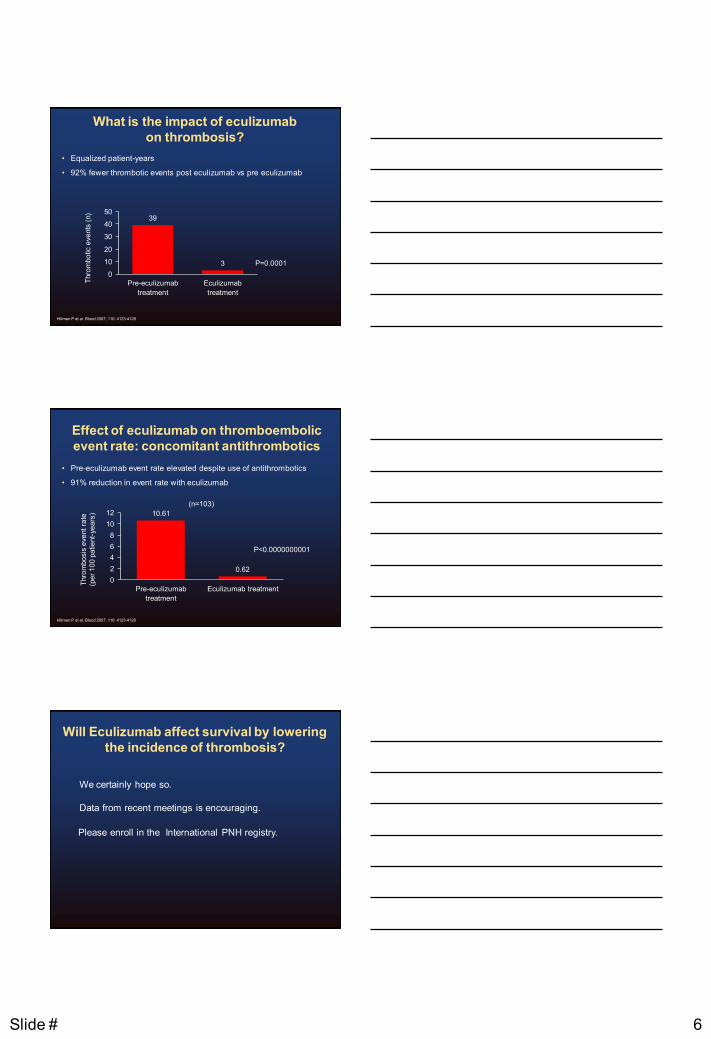
What is the impact of eculizumab
on thrombosis?
• Equalized patient-years
• 92% fewer thrombotic events post eculizumab vs pre eculizumab
39
3
0
10
20
30
40
50
Pre-eculizumab
treatment
Eculizumab
treatment
P=0.0001
Thro
mbo
tic e
ve
nts
(n)
Hillmen P et al. Blood 2007; 110: 4123-4128
Effect of eculizumab on thromboembolic
event rate: concomitant antithrombotics
• Pre-eculizumab event rate elevated despite use of antithrombotics
• 91% reduction in event rate with eculizumab
10.61
0.62
0
2
4
6
8
10
12
Pre-eculizumab
treatment
Eculizumab treatment
P<0.0000000001
Thro
mbo
sis
eve
nt
rate
(pe
r 1
00
pa
tie
nt-
ye
ars
)
(n=103)
Hillmen P et al. Blood 2007; 110: 4123-4128
Will Eculizumab affect survival by lowering
the incidence of thrombosis?
We certainly hope so.
Data from recent meetings is encouraging.
Please enroll in the International PNH registry.
Slide # 7
PNH – Renal Failure
Renal Damage in PNH: BackgroundRenal Damage in PNH: Background
Renal failure has been identified as Renal failure has been identified as
the cause of death in approximately the cause of death in approximately
8 8 –– 18% of PNH patients18% of PNH patients1,21,2
68% have a significant reduction in 68% have a significant reduction in
creatininecreatinine clearanceclearance33
64% of patients with PNH have 64% of patients with PNH have
chronic kidney diseasechronic kidney disease22
Historically underappreciated in PNHHistorically underappreciated in PNH
1. Nishimura JI, et al. Medicine. 2004;83:193-207. 2. Hillmen P et al. Am. J. Hematol. 2010; 85:553–559. 3. Rother RP, et al. JAMA. 2005;293:1653-1662
Renal Damage in PNH: BackgroundRenal Damage in PNH: Background
Chronic haemolysis and cellChronic haemolysis and cell--free plasma haemoglobin lead to free plasma haemoglobin lead to
several serious clinical sequelae in PNHseveral serious clinical sequelae in PNH11––33
Evidence of renal damage is highly prevalent in patients with Evidence of renal damage is highly prevalent in patients with
PNHPNH55––99
May be acute renal failure, which is frequently reversibleMay be acute renal failure, which is frequently reversible44
Associated with haemolysis and/or microvascular thrombosisAssociated with haemolysis and/or microvascular thrombosis2,42,4
Renal damage in PNH may be due to repetitive exposure of Renal damage in PNH may be due to repetitive exposure of
tissue to celltissue to cell--free haemoglobinfree haemoglobin99
1. Parker C et al. Blood 2005; 106:3699-709.; 2. Brodsky RA. Hematology: Basic Principles and Practice. Churchill Livingstone; 2005:419-27.; 3. Rother RP et al. JAMA 2005;293:1653-62.; 4. Clark DA et al. Blood 1981;57:83-9.; 5. Hill A et al. Presented at the 48th ASH Annual Meeting, Dec 9, 2006.; 6. Mulopulos GP
et al. Am J Roentgenol 1986;146:51-2.; 7. Rimola J et al. Br J Radiol 2004;77:953-6.; 8. Tanaka YO et al. J Comput Assist Tomogr 1993;17:749-53; 9. Nishimura J et al. Medicine 2004;83:193-207.

Slide # 8
0 5 10 30 40 20
100
90
80
70
60
50
40
30
20
0
10
Time to Major Clinical Kidney Event Time to Major Clinical Kidney Event
Prior to Prior to EculizumabEculizumab Treatment Treatment
Pro
bab
ilit
y (
%)
of
Main
tain
ing
No
rmal
Kid
ney F
un
cti
on
Time Since PNH Diagnosis (years)
n 195 103 60 21 4
Kaplan-Meier probability of patients progressing to an MCK event.
Hillmen P et al. Am. J. Hematol. 2010; 85:553–559.
Normal
tissue
on the right
Interstitial
scarring
on the left
Clark DA et al. Blood 1981; 57: 83-89
Renal pathology in PNH
Micrograph of a renal biopsy from a PNH patient,
indicative of vascular damage
Chronic Kidney Disease Staging Identifies Chronic Kidney Disease Staging Identifies
Both Function and DamageBoth Function and Damage
Stage GFR
(ml/minute/1.73 m2)
Objective Measure of Kidney Damage
Description Action*
1 ≥ 90 Evidence of proteinuria
Kidney damage with normal GFR
Diagnose and treat
Treat comorbid conditions;
Slow progression;
CVD risk reduction
2 60-89 Evidence of proteinuria
Kidney damage with mild decreased GFR
Estimate progression
3 30-59 No additional evidence necessary
Moderately decreased GFR
Evaluate and treat complications
4 15-29 No additional evidence necessary
Severely decreased GFR
Prep for kidney replacement therapy; Predialysis
5 < 15 (or dialysis) No additional evidence necessary
Kidney Failure Replacement (if uraemia present); Dialysis
Chronic Kidney Disease (CKD) Stages 1-5
*Includes actions from preceding stages. Levey AS et al. Ann Intern Med. 2003;129:137-147.

Slide # 9
64% of Patients Exhibit stage 164% of Patients Exhibit stage 1--5 CKD5 CKD
Among the 22 patients with minimal (0Among the 22 patients with minimal (0--1) transfusion history, 59% exhibited CKD 1) transfusion history, 59% exhibited CKD
Hillmen et al. Long term effect of the complement inhibitor eculizumab on kidney function in patients with paroxysmal nocturnal Hemoglobinuria. Am J Hematol 85:553-559, 2010.
Kidney Function
Stage 3 - 5 CKD
(n=40)
Stage 1 - 2 CKD
(n=84)
No CKD
(n=69)
20.5%
43.1%
35.4%
0
10
20
30
40
50
Pro
po
rtio
n o
f P
ati
en
ts (
%)
Renal Function with Eculizumab in Different
Baseline Populations – 12 Months
Hillmen et al. Long term effect of the complement inhibitor eculizumab on kidney function in patients with paroxysmal nocturnal
Hemoglobinuria. Am J Hematol 85:553-559, 2010.
58.1
23.4
76.9
35.2
71.4
20.5
6.7 5.2 2.6
0
10
20
30
40
50
60
70
80
90
Segment of PNH Population
Pro
po
rtio
n o
f P
ati
en
ts (%
)
P<0.001 P=0.02 P<0.001
No Change Improvement Worsening
Overall
(n=179)
Stage 1 – 2
(n=77)
Stage 3 - 5
(n=39)
How to manage renal complicationsHow to manage renal complications
Stay well hydratedStay well hydrated
Control other conditions which may affect the kidneys Control other conditions which may affect the kidneys
(hypertension, diabetes)(hypertension, diabetes)
Avoid drugs which may cause renal problems (Avoid drugs which may cause renal problems (egeg. Non. Non--
steroidal medications such as ibuprofen)steroidal medications such as ibuprofen)
Monitor kidney function at least once per year.Monitor kidney function at least once per year.
Block hemolysisBlock hemolysis
27

Slide # 10
Renal Function in PNH: Conclusions
Changes in renal function are common in PNH (65% of PNH patients;
6.6-fold more common than in the general population)1
Severe CKD is observed in 21% of PNH patients and appears to be
under-diagnosed in this patient population
21% of patients with CKD prior to eculizumab were no longer classified
with CKD during eculizumab treatment
Administration of eculizumab to patients with more mild baseline kidney
disease was associated with the greatest likelihood of improvement and
prevention of worsening in kidney function
Long-term eculizumab treatment resulted in a significant improvement
and prevention of worsening in CKD at all initial stages of renal disease
PNH & Pulmonary Hypertension
Hemolysis-associated pulmonary
hypertension
An important complication in hereditary hemolytic anemias
such as thalassemia, stomatocytosis, and spherocytosis
A common morbidity in sickle cell disease
Linked to intravascular hemolysis, leading to the term
‘hemolysis-associated pulmonary hypertension’ (PHT)
An independent risk factor for death in sickle cell disease
Gladwin MT et al. N Engl J Med 2004; 350: 886-895
Slide # 11
Brain natriuretic peptide
Elevated levels of BNP:
– released from stretched right heart chambers
– reflect cardiac chamber volume and pressure overload
– indicate increased PHT and right ventricular dysfunction
In patients with hemolytic syndrome, NT-proBNP >160 pg/mL:1
– is a highly positive predictive value for diagnosis of PHT
– is an independent predictor of mortality
TRIUMPH study: 47% of PNH patients had baseline levels of
NT-proBNP >160 pg/mL2
Suggestive of PHT
1Machado RF et al. JAMA 2006; 296: 310-318; 2Hillmen P et al. N Engl J Med 2006; 355: 1233-1243 BNP, brain natriuretic peptide
Change in BNP during eculizumab
treatment
PHT with NT-proBNP ≥160 pg/mL1
Eculizumab vs placebo (P<0.001)
50% reduction
14% increase
Baseline Baseline Week 26 Week 26
52.5
39.4
26.3
43.8
0
10
20
30
40
50
60
Placebo Eculizumab
Treatment group: TRIUMPH (n=73)
Pro
po
rtio
n o
f p
ati
en
ts
wit
h e
vid
en
ce o
f P
HT
Hill A et al. British J Haematol 149: 414-425, 2010
Pulmonary Hypertension - Summary
PHT is a serious and life-threatening complication of hemolytic
disorders
PHT and PNH symptoms are common in patients with hemolytic PNH
PHT may be under-diagnosed clinically in patients with PNH
Hemoglobinemia, NO consumption, and disruption of vasomotor tone
contribute to PHT in patients with PNH
Eculizumab treatment significantly reduces PHT, as measured by BNP,
and PHT-related symptoms in patients with PNH
Eculizumab treatment dramatically reduces hemolysis,
hemoglobinemia, and NO consumption in patients with PNH

Slide # 12
PNH – development of AA or MDS
Sir John V. Dacie (1911 - 2005)
Lewis SM, Dacie JV. The aplastic anemia-paroxysmal nocturnal
hemoglobinuria syndrome. Br J Haematol 13:236, 1967.
William Dameshek 1900-1962
Dameshek W. Riddle:What do aplastic anemia, paroxysmal nocturnal hemoglobinuria
(PNH), and “hypoplastic” leukemia have in common? Blood 30:251, 1967
Slide # 13
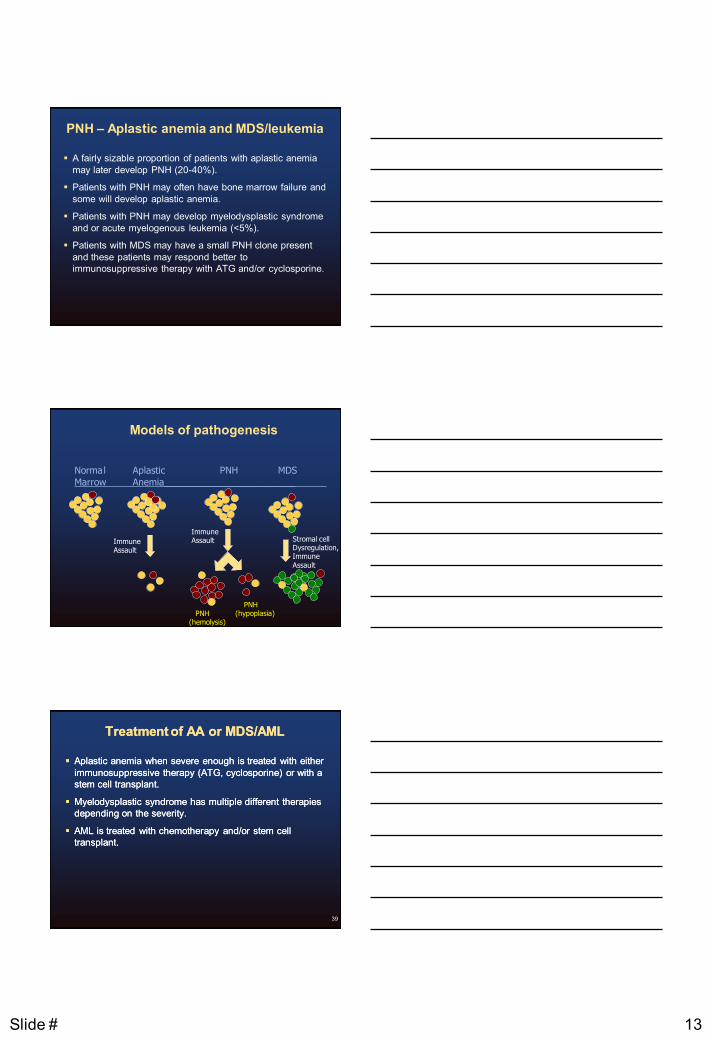
PNH – Aplastic anemia and MDS/leukemia
A fairly sizable proportion of patients with aplastic anemia
may later develop PNH (20-40%).
Patients with PNH may often have bone marrow failure and
some will develop aplastic anemia.
Patients with PNH may develop myelodysplastic syndrome
and or acute myelogenous leukemia (<5%).
Patients with MDS may have a small PNH clone present
and these patients may respond better to
immunosuppressive therapy with ATG and/or cyclosporine.
Models of pathogenesis
Norma l Aplastic PNH MDS
Marrow Anemia_________________________
Immune Assault
Immune Assault
PNH (hemolysis)
PNH (hypoplasia)
Stromal cell Dysregulation, Immune
Assault
Treatment of AA or MDS/AMLTreatment of AA or MDS/AML
Aplastic anemia when severe enough is treated with either Aplastic anemia when severe enough is treated with either
immunosuppressive therapy (ATG, cyclosporine) or with a immunosuppressive therapy (ATG, cyclosporine) or with a
stem cell transplant.stem cell transplant.
MyelodysplasticMyelodysplastic syndrome has multiple different therapies syndrome has multiple different therapies
depending on the severity.depending on the severity.
AML is treated with chemotherapy and/or stem cell AML is treated with chemotherapy and/or stem cell
transplant.transplant.
39

Slide # 14
Complications of PNH Therapy
Complications of PNH Therapy
Eculizumab
– Neisseria infection
– Cost and convenience
– Extravascular hemolysis
ATG/Cyclosporine
– Hospitalization
– Anaphylactic reactions
– Serum sickness
– Immunosuppression / Infection
Bone marrow transplantation
– Allogeneic bone marrow transplant
– Prolonged hospitalization
– Up to 44% mortality at 2 yrs with HLA-matched
sibling donor
– Acute GVHD in 34%; chronic GVHD in 33%
– GVHD-free survival in 14% of patients
Serious Adverse Events:
Clinical Trial Experience
Meningococcal infections are the most important adverse
events that may be experienced by patients receiving
Eculizumab
In PNH clinical studies, 2 patients experienced
meningococcal sepsis
– Both patients had received a meningococcal vaccine
In clinical studies among patients without PNH,
meningococcal meningitis occurred
in 1 unvaccinated patient

Slide # 15
Special Situations in PNHSpecial Situations in PNH
43
Special Situations in PNHSpecial Situations in PNH
Vaccinations
– May activate complement
– Role for Eculizumab
Surgery
– May activate complement
– May lead to thrombosis
– Role for Eculizumab
Pregnancy
PNH and surgeryPNH and surgery
Slide # 16
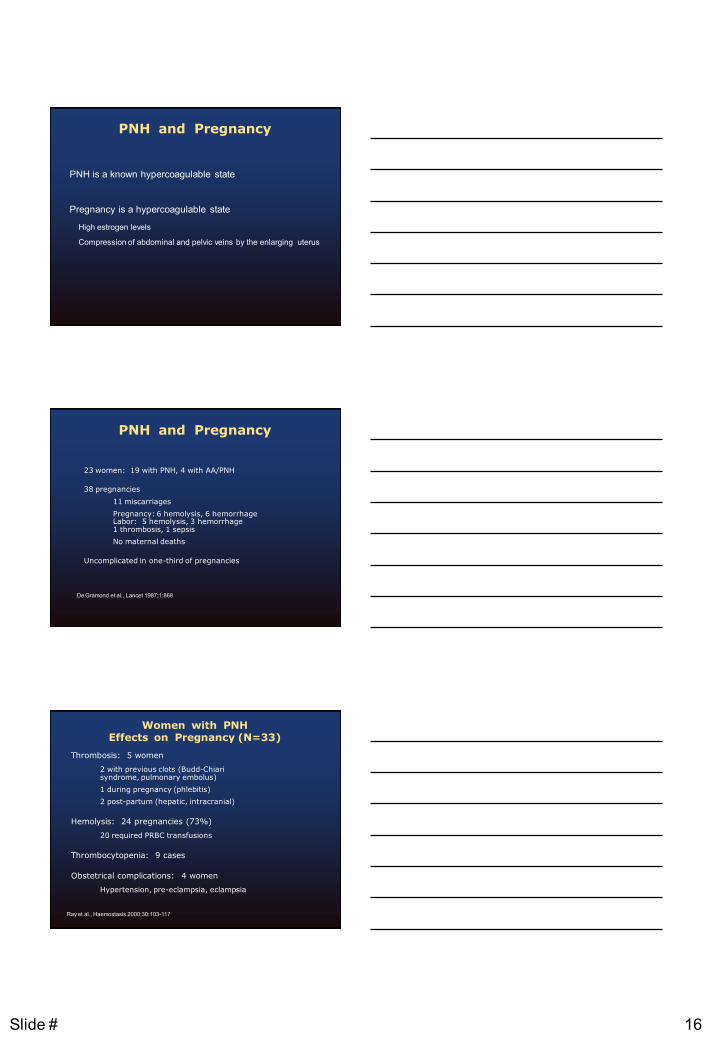
PNH and Pregnancy
PNH is a known hypercoagulable state
Pregnancy is a hypercoagulable state
High estrogen levels
Compression of abdominal and pelvic veins by the enlarging uterus
PNH and Pregnancy
23 women: 19 with PNH, 4 with AA/PNH
38 pregnancies
11 miscarriages
Pregnancy: 6 hemolysis, 6 hemorrhage Labor: 5 hemolysis, 3 hemorrhage 1 thrombosis, 1 sepsis
No maternal deaths
Uncomplicated in one-third of pregnancies
De Gramond et al., Lancet 1987;1:868
Women with PNH Effects on Pregnancy (N=33)
Thrombosis: 5 women
2 with previous clots (Budd-Chiari syndrome, pulmonary embolus)
1 during pregnancy (phlebitis)
2 post-partum (hepatic, intracranial)
Hemolysis: 24 pregnancies (73%)
20 required PRBC transfusions
Thrombocytopenia: 9 cases
Obstetrical complications: 4 women
Hypertension, pre-eclampsia, eclampsia
Ray et al., Haemostasis 2000;30:103-117

Slide # 17
Women with PNH Effects on Infants
Perinatal outcomes of 33 pregnancies
45% of the babies were pre-term
Average birthweight 2800g
Three infant deaths
Two had hemolytic disease of the newborn, not related to PNH
No infant thrombosis
Ray et al., Haemostasis 2000;30:103-117
50
27 pregnancies in 22 PNH patients from 10 different medical centers.
PNH and Pregnancy Summary
Pregnancy is possible for women with PNH, with or without aplastic anemia, but is potentially hazardous for mother and infant.
Pregnancy leads to complications in up to 50% of women: worse cytopenia, transfusion dependency, thrombosis, and the need for anticoagulation or immunosuppressants
Pregnancy for women with PNH is risky, and should be planned carefully with an experienced hematologist and high-risk OB.
There is emerging data on the use of Eculizumab in pregnancy.
Slide # 18
Special situations for patients with PNH
Surgery – Singer A et al. Successful Liver Transplantation for Budd-Chiari Syndrome
in a Patient with Paroxysmal Nocturnal Hemoglobinuria Treated with the
Anti-Complement Antibody Eculizumab. Liver Transplant 15: 540-543, 2009.
Pregnancy – Kelly R, et al. The management of pregnancy in paroxysmal nocturnal
haemoglobinuria on long term eculizumab. Br J Haematol 149: 446-450,
2010.
– Danilov AV, et al. Managing a pregnant patient with paroxysmal nocturnal
hemoglobinuria in the era of eculizumab. Leukemia Research 34: 566-571,
2010.
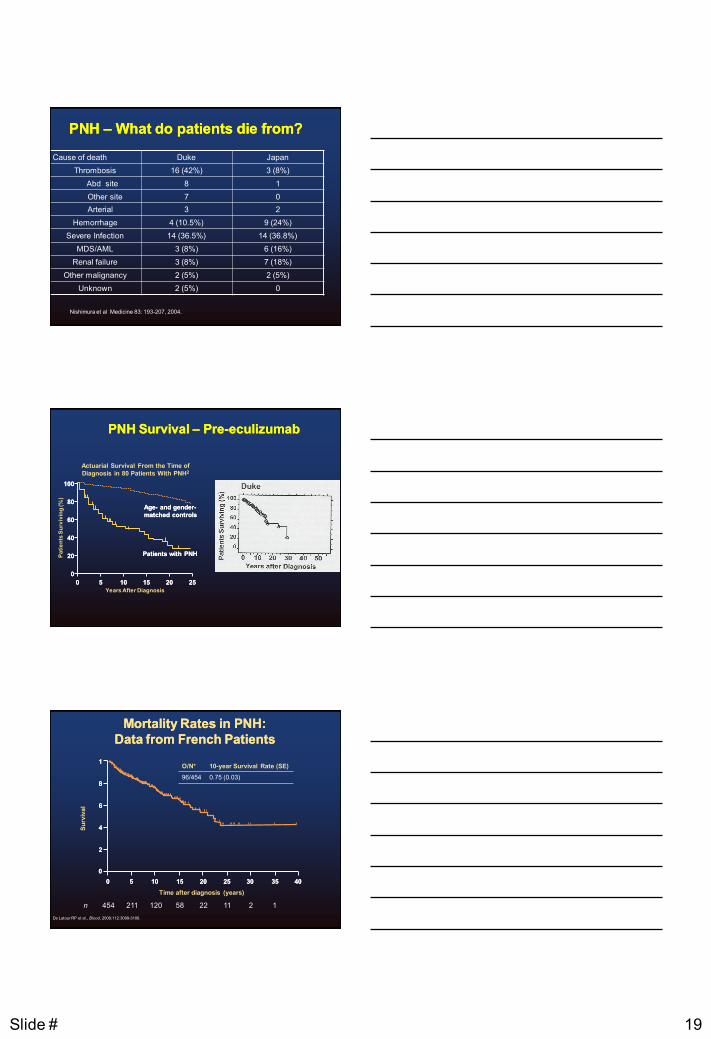
Clinical Impact of Extravascular Haemolysis
Consequences
Increased LDH
Anemia
Fatigue?
Complement-mediated Intravascular Haemolysis
PNH RBC Survival
No Eculizumab Treatment
Eculizumab Treatment
PNH RBC
C3b Deposition, Possible Extravascular
Haemolysis
1. Hill, A et al. Haematologica. 2010; 95:567-573. 2. Risitano, AM. Blood. 2009;113:4094-4100. 3. Hillmen P et al. N Engl J Med. 1995;333:1253-1258.
Consequences
Increased LDH
Anemia
Hemoglobinuria
Nitrous Oxide Squelching
Fatigue
Does Does EculizumabEculizumab improve survival?improve survival?
Slide # 19
PNH PNH –– What do patients die from?What do patients die from?
Cause of death Duke Japan
Thrombosis 16 (42%) 3 (8%)
Abd site 8 1
Other site 7 0
Arterial 3 2
Hemorrhage 4 (10.5%) 9 (24%)
Severe Infection 14 (36.5%) 14 (36.8%)
MDS/AML 3 (8%) 6 (16%)
Renal failure 3 (8%) 7 (18%)
Other malignancy 2 (5%) 2 (5%)
Unknown 2 (5%) 0
Nishimura et al Medicine 83: 193-207, 2004.
PNH Survival PNH Survival –– PrePre--eculizumabeculizumab
100100
8080
6060
4040
2020
00
00 55 1010 1515 2020 2525
Years After Diagnosis
Pati
en
ts S
urv
ivin
g (%
)
Actuarial Survival From the Time of
Diagnosis in 80 Patients With PNH2
AgeAge-- and genderand gender--
matched controlsmatched controls
Patients with PNHPatients with PNH
De Latour RP et al., Blood, 2008;112:3099-3106.
Mortality Rates in PNH: Mortality Rates in PNH:
Data from French Patients Data from French Patients
n 454 211 120 58 22 11 2 1
11
88
66
44
22
00
00 55 1010 2525 3030 4040 1515 2020 3535
Time after diagnosis (years)
O/N* 10-year Survival Rate (SE)
96/454 0.75 (0.03)
Su
rviv
al
Slide # 20
LongLong--term Treatment With term Treatment With EculizumabEculizumab in PNH: in PNH:
Sustained Efficacy and Improved SurvivalSustained Efficacy and Improved Survival
79 consecutive patients with PNH, 79 consecutive patients with PNH,
between May 2002 and July 2010between May 2002 and July 2010
Mortality and disease symptoms were Mortality and disease symptoms were
evaluatedevaluated
Kelly RJ et al. Blood. 117:6786-6792, June 2011
Thrombotic EventsThrombotic Events
Patients (n) 79
Pre-treatment
Thrombotic events (n) 34
Proportion occurring on anticoagulation (%) 47
Patient years (n) 608
Thrombotic event rate (n per 100 patient years)
5.60
Eculizumab Treatment
Thrombotic events (n) 2
Patient years (n) 260
Thrombotic event rate
(n per 100 patient years)
0.8
(P<0.001)
Kelly RJ et al. Blood. 117:6786-6792, June 2011
Eculizumab Has a Major Impact on Survival in PNHEculizumab Has a Major Impact on Survival in PNH
• 96% (76/79) patient survival
• There was no difference in mortality between patients on eculizumab
and the normal population (P=0.46)
Survival is comparable to age and genderSurvival is comparable to age and gender--matched control population out to 8 yearsmatched control population out to 8 years
Cu
mu
lati
ve s
urv
ivin
g (
%)
Time (years)
100100
8080
6060
4040
2020
00
00 11 22 66 77 99 44 55 88 33
n = 79
Age- and sex-matched normal population
Eculizumab treated
Kelly RJ et al. Blood. 117:6786-6792, June 2011

Slide # 21
Mortality in Patients on EculizumabMortality in Patients on Eculizumab
3 Patients Died in the 8 Year Study Period3 Patients Died in the 8 Year Study Period
1.1. 55 year old man died from 55 year old man died from metastaticmetastatic caecalcaecal carcinoma carcinoma
which was diagnosed prior to which was diagnosed prior to eculizumabeculizumab treatmenttreatment
2.2. 76 year old woman died from pneumonia following a long 76 year old woman died from pneumonia following a long
history of recurrent bronchopneumonia prior to starting history of recurrent bronchopneumonia prior to starting
eculizumabeculizumab
3.3. 79 year old man with a preceding history of 79 year old man with a preceding history of ischaemicischaemic
heart disease died from congestive cardiac failureheart disease died from congestive cardiac failure
Kelly RJ et al. Blood. 117:6786-6792, June 2011.
Improved Overall Survival in Patients Improved Overall Survival in Patients
Treated With Treated With EculizumabEculizumab
Time (years)Time (years)
Cu
mu
lati
ve S
urv
ivin
g (%
)
11 22 33 44 55 66 77 88 99
2020
4040
6060
8080
100
00
Kelly RJ et al. Blood. 117:6786-6792, June 2011.
On Eculizumab, n=79
Pre-eculizumab, n=30
Overall survival was 97.6% (95%CI 93.7Overall survival was 97.6% (95%CI 93.7--99.1) at 3 years and was maintained 99.1) at 3 years and was maintained
through 5.5 years of ongoing through 5.5 years of ongoing eculizumabeculizumab treatment (N=195)treatment (N=195)
Patient Survival in the Patient Survival in the EculizumabEculizumab Study PopulationStudy Population
Brodsky R et al. Blood. 2010;116(21) Abstract #4237.
Slide # 22
Where are we going?Where are we going?
Improve current therapyImprove current therapy
–– Oral Oral eculizumabeculizumab
–– Increase treatment intervalsIncrease treatment intervals
Find other ways to inhibit complementFind other ways to inhibit complement
Understand how PNH cells take over the bone marrow Understand how PNH cells take over the bone marrow so we can reverse this process (Restore normal stem so we can reverse this process (Restore normal stem cells)cells)
Gene therapyGene therapy
Stem cell transplantsStem cell transplants
Thank you. Any questions?


















