Pneumonia Final Copy

of 68
-
Upload
charles-liong-calma -
Category
Documents
-
view
223 -
download
0
Transcript of Pneumonia Final Copy
-
8/3/2019 Pneumonia Final Copy
1/68
I. INTRODUCTION
Breathing is the greatest pleasure in life.
~Giovanni Papini
Breath is sometimes used as a metaphor for life itself because it takes
in the oxygen needed by the body and the carbon dioxide out of the body. It
is one of the human persons vital functions to maintain and sustain life. One
of the most common illness that disrupts the normal breathing pattern of a
person is Pneumonia.
Pneumonia is an infection and inflammation of the alveoli in the lungs
that is usually caused by infection with bacteria, viruses, fungi or other
organisms. Pneumonia is a particular concern for older adults and people with
chronic illnesses or impaired immune systems, but it can also strike young,
healthy people. Pneumonia may be of bacterial in origin (pneumococcal,
streptococcal, staphylococcal, or chlamydial) or viral in origin, such as
respiratory synctial virus (RSV). (http://mayoclinic.com; August 27, 2008;
6:45pm )
Worldwide, Pneumonia is the 7th leading cause of death in 1999 and
2000 according to CDC. In the United States, the incidence extrapolations of
pneumonia is 4,800,000 per year, 400,000 per month, 92,307 per week,
13,150 per day, 547 per hour, 9 per minute, 0 per second. In the Philippines,
Pneumonia is the 5th cause of mortality according to the 2003 Philippine
Health Statistics with a rate of15,831 for males and 16, 224 for females or
32, 055 per 100, 000 population. ( http://doh.gov.ph; August 28, 2008;
8:30pm)
A study suggests that antipsychotic drugs increase the risks of
developing pneumonia in the elderly. Elderly patients who use antipsychotic
drugs have a 60 percent increased risk of developing pneumonia compared
to non-users. This risk is highest in the first week following prescription and
decreases gradually thereafter. Antipsychotic drugs are frequently used in
elderly patients for the treatment of psychosis and behavioral problems
1
-
8/3/2019 Pneumonia Final Copy
2/68
associated with dementia and delirium. This study is the first to show that the
development of pneumonia is associated with antipsychotic drug use.
(www.sciencedaily.com; Apr. 16, 2008)
Researchers at Children's Hospital of Pittsburgh of UPMC haveidentified a key protein target that may be a crucial factor in the
development of a vaccine to prevent and new therapies to treat pneumonia,
the leading killer of children worldwide. Identified for the first time is the
importance of a protein known as interleukin 22 (IL-22) in the immune
response to a strain of bacterial pneumonia. In the laboratory, the
researchers were able to effectively treat mice with pneumonia by using
purified IL-22. IL-22 and interleukin 17A (IL-17A) are produced by a recently
discovered lineage of cells known as T Helper Type 17 (Th17). Children'sresearchers found evidence that the Th17 cell lineage and its cytokines IL-22
and IL-17A have evolved to promote host defense against certain infections
in the lung caused by extracellular pathogens. (www.sciencedaily.com;
February 12, 2008)
Much of the learning of student nurses is derived from the exposure in
the hospital setting. Reinforcement in the actual setting is important for
learning to be truly effective. As student nurses, it is important that the care
provided bring satisfaction to patients. To be able to provide outmost care,
knowledge about the disease condition must be well founded. It is one of the
objectives of the group to be familiar with the common disease conditions
that may be encountered in the hospital setting. Knowing that Pneumonia is
one of the common cases evident in the area, which is Medical Surgical, the
group decided to make this as their topic for case study.
2
-
8/3/2019 Pneumonia Final Copy
3/68
II. NURSING ASSESSMENT
A. Personal History
To secure confidentiality, the patient would be referred as Monia
throughout the study. Monia is the primary source of information.
Monia is a 31 year old married Filipina who lives in a barrio in San
Vicente, Magalang Pampanga. She was born on August 2, 1974. She is the 2nd
among five siblings. Monia was admitted on August 12, 2008 at 12:05 pm in a
district hospital in Magalang with complaints of fever, chills and cough. The
admitting diagnosis is Community Acquired Pneumonia and was discharged
on August 16, 2008 with a final diagnosis of CAP.
Monia lives in a barrio which has limited accessibility to the hospital.
She and her family earn a living by planting different plant crops like camote.
Her activities of daily living include cooking, cleaning the house, doing the
laundry, taking good care of her five children and helping her husband in
planting and selling crops. Monia was not able to finish her schooling due to
the location of their place. She was only able to reach grade six because the
school in their barrio only offers elementary schooling and her family cannot
send her to high school due to financial constraints. Monia and her family are
devoted Missionaries. At present, they live in a house which has concrete
walls, sawali for the roof and a flooring which is still not cemented. She
describes her community as a peaceful one and her neighbors are hospitable.
One of the cultural practices done in their community is the practice of using
herbal plants like bayabas, bawang, ginger and ampalaya for medicines.
3
-
8/3/2019 Pneumonia Final Copy
4/68
B. Pertinent Family Health-Illness History
Paternal Side Maternal Side
Lolo89 y/o
Lola
85y/o
Papa67 /o
Lolo
Ulcer
1996
Lola
Stroke
2002
Mama62y/o
MONIA
34y/oCAP
LEGEND:
Male
Female
Deceased
S1 S2 S3 S5 S6 S7 S8 S1 S2 S3 S5 S6 S7 S8
S Sibling
4
-
8/3/2019 Pneumonia Final Copy
5/68
Explanation:
The illnesses present in the in the family tree of Monia are ulcer, which
was the cause of death of her grandfather, and stroke, which caused the
death of her grandmother last 2002 both on the mother side.
On her paternal side, Monia stated that her grandparents are still living
and has no known illness.
Monia has no history of pneumonia on both maternal and paternal
sides.
C. History of Past Illness
When Monia was 3 years old, she had tigdas or measles which her
mother treated with some herbal plants. She also had chickenpox when she
was 25 years old. Monia did not experience any major illness in the past and
was never hospitalized before. She only experienced cough, colds and fever
occasionally especially during cold weather. During these situations, she only
self-medicates and uses herbal plants like oregano and takes drugs like
Biogesic and Neozep.
D. History of Present Illness
On July 29, 2008, Monia is supposed to go with her husband to sell
their root crops but her body malaise prevented her from doing so. The
following day, she experienced fever, which subsides after sweating. Her
fever had became recurrent and caused her to have difficulty sleeping at
night. She also lost her appetite, which led to lost of weight of 6.6 pounds
(from 125.4 lbs to 118.8 lbs). She also had cough, which she said gave her
the difficulty of breathing. She felt that there is mucus in her throat but she
cannot cough it out. Her condition prevented her from doing her usual chores
of helping in the planting and selling of their root crops and taking good care
of her five children.
At first, Monia thought that it is just a usual fever which she got
possibly because of the prevalence of fever and cough in their barrio. But
after two weeks of having fever, she decided to ask her husband to bring her
to the district hospital which she had not thought before because of the
5
-
8/3/2019 Pneumonia Final Copy
6/68
distance of their house to the said medical institution and also because of
financial constraints. While on their way to the hospital, her husband had to
carry her because she cannot walk properly due to body malaise and high
fever. So on August 12, 2008, Monia was admitted with an admitting
diagnosis of Community Acquired Pneumonia and was discharged after 5
days on August 16, 2008 with a final diagnosis of Pneumonia.
E. Physical Examination
2 weeks prior to admission (+) fever
1 week prior to admission (+) cough, productive
2 days prior to admission fever on and off
- low appetite
few hours prior to admission (+) chills and fever
- (+) body weakness
Date: August 12, 2006 (Admission) Lifted from the Chart
pink palpebral conjunctiva
anecteric sclerae
adynamic pericardium
(-) murmurs
flabby abdomen
(+) chills and fever with temperature of 40.50C/axilla
(+) body weakness
(+) cough, nonproductive
First Student Nurse-Patient Interaction
(August 12, 2008)
General Survey:
Received patient wearing a white colored shirt and blue jogging pants,
in high fowlers position, awake and conscious,; with an IVF of #1 D5NM 1L
regulated at 30 to 31 gtts/min. at 550 cc level infusing well on the right hand.
6
-
8/3/2019 Pneumonia Final Copy
7/68
Signs and symptoms include (+) nonproductive cough, (+) difficulty of
breathing, febrile.
Vital Signs:
Temperature 37.80C/axilla
Pulse rate 86 bpm
Respiratory rate 34bpm
Blood pressure 110/70 mmHg
Skin:
Brown in color, no altered pigmentation, no edema or swelling upon
palpation.
Head:
Hair and Scalp: Black in color, slightly thick, silky and
resilient and hair equally distributed on scalp area, No infestation or
infection noted.
Skull: Rounded, smooth skull contour and no masses or nodules noted.
Face: symmetrical facial feature and symmetric facial
movements.
Eyes: Eyebrows and eyelashes evenly distributed; eyelids
have no discharge, no discoloration and lids close symmetrically.
Palpebral conjunctiva is pink in color.
Vision: Client can see objects in the periphery.
Illuminated pupil constricts while non-illuminated dilates.
(+)PERRLA
Ear: Color of the auricles same as the facial skin.
Symmetrical and aligned with outer canthus of eye, mobile, firm
and not tender, pinna recoils after it is folded.
Nose: Centrally located, uniform in color, no discharges noted, not
tender, no lesions and air moves with slight difficulty as the client
breaths through the nares because of presence of nasal
secretions.
Mouth: (+) Mild drying of lips and oral mucosa
7
-
8/3/2019 Pneumonia Final Copy
8/68
Neck:
Head is centered, head movement is coordinated with no discomfort.
No swelling and masses noted and no enlargement of lymph nodes
upon palpation.
Thorax:
No tenderness and masses on the chest skin, skin intact and uniform
temperature. (+) Fast shallow breathing.
Lungs:
(+) Rales heard upon auscultation.
Heart:
Normal rhythm and rate noted upon auscultation, no murmurs.
Abdomen:
Flabby, no pain when palpated.
Upper Extremities:
Intact nail beds, good capillary refill, no deformities, no tenderness or
swelling,
Lower Extremities:
Intact toenail beds, has upright posture and steady gait, walks unaided
and maintains balance.
Second Student Nurse-Patient Interaction
(August 13, 2008)
General Survey:
Received patient wearing yellow colored shirt and brown shorts, in
right side-lying position, sleeping; with an IVF of #3 D5NM 1L regulated at 30
to 31 gtts/min. at 650 cc level infusing well on the right hand.
Vital Signs:
Temperature 380C/axilla
Pulse rate 81 bpm
Respiratory rate 26 bpm
Blood pressure 120/70 mmHg
8
-
8/3/2019 Pneumonia Final Copy
9/68
Skin:
Brown in color, no altered pigmentation, no edema or swelling upon
palpation.
Head:
Hair and Scalp: Black in color, slightly thick, silky and
resilient and hair equally distributed on scalp area, No infestation or
infection noted.
Skull: Rounded, smooth skull contour and no masses or nodules noted.
Face: symmetrical facial feature and symmetric facial
movements.
Eyes: Eyebrows and eyelashes evenly distributed; eyelids
have no discharge, no discoloration and lids close symmetrically.
Palpebral conjunctiva is pink in color.
Vision: Client can see objects in the periphery.
Illuminated pupil constricts while non-illuminated dilates.
(+)PERRLA
Ear: Color of the auricles same as the facial skin.
Symmetrical and aligned with outer canthus of eye, mobile, firm
and not tender, pinna recoils after it is folded.
Nose: Centrally located, uniform in color, no discharges noted, not
tender, no lesions and air moves with slight difficulty as the client
breaths through the nares because of presence of nasal
secretions.
Mouth:(+) Mild drying of lips and oral mucosa
Neck:
Head is centered, head movement is coordinated with no discomfort.
No swelling and masses noted and no enlargement of lymph nodes
upon palpation.
Thorax:
No tenderness and masses on the chest skin, skin intact and uniform
temperature. (+) Fast shallow breathing.
Lungs:
9
-
8/3/2019 Pneumonia Final Copy
10/68
(+) Rales heard upon auscultation.
Heart:
Normal rhythm and rate noted upon auscultation, no murmurs.
Abdomen:
Flabby, no pain when palpated.
Upper Extremities:
Intact nail beds, good capillary refill, no deformities, no tenderness or
swelling,
Lower Extremities:
Intact toenail beds, has upright posture and steady gait, walks unaided
and maintains balance.
10
-
8/3/2019 Pneumonia Final Copy
11/68
F. Diagnostic and Laboratory ProceduresDiagnostic/LaboratoryProcedures
Date OrderedDate Results
In
IndicationsOr
Purposes
Results NormalValues
Analysis andInterpretation
of ResultsHemoglobin Date Ordered:
08/12/08Date Results In:
08/12/08
To evaluate thehemoglobin
content, the ironstatus, and
oxygen carrying
capacity of theblood.
10.2 mg% Male: 13.5 18Female: 12-16
Less thannormal. The
Oxygen carryingcapacity of the
blood is
inadequate dueto the
inflammatoryreaction thatoccurs in the
alveoli,producing
exudates thatinterfere with the
diffusion ofoxygen and
carbon dioxide.
Hematocrit Date Ordered:08/12/08
Date Results In:08/12/08
This is tomeasure thepercentage of
the patients redblood cells in thetotal volume ofblood. It aids inthe diagnosis ofany abnormal
status ofpatients
hydration.
33.0 vol. % Male: 40-54Female: 37-47
Less thannormal. Itindicates
insufficient bloodvolume
composed ofRBCs and an
abnormal statusof patients
hydration due tothe excessive
sweatingexperienced by
11
-
8/3/2019 Pneumonia Final Copy
12/68
the patient aftereach onset of
fever.
WBC Count Date Ordered:08/12/08
Date Results In:08/12/08
To determineinfection or
inflammationand also to
determine and
evaluate thebodys
physiologiccapacity toresist andovercomeinfection
10.750/cu. mm. Adult: 5-10 x103
There ispresence of
inflammation orinfection due tothe invasion of
microorganismsin the lungs.
Platelet Count Date Ordered:08/12/08
Date Results In:08/12/08
To determinethe number ofplatelets in thepatient's bloodand to assist inthe diagnosis of
bleedingdisorders
280/cu. mm. Adult: 150 - 450 Value is withinnormal rangewhich could
indicate that thepatient does nothave bleeding
disorders.
Segmenters Date Ordered:08/12/08
Date Results In:08/12/08
To determineinfection or
inflammation
87% 50-70 Increase in valuecan be a result ofbodys response
to infection.Lymphocytes Date Ordered:
08/12/08Date Results In:
08/12/08
To determineviral infection or
inflammation
13% 25-40 Decreasedcapability of
carrying out theactivities of theimmune system
or there is adecreased ability
to produce
12
-
8/3/2019 Pneumonia Final Copy
13/68
antibodies.
Nursing Responsibilities:
Before
1. Explain the procedure to the SO and the purpose of the procedure.
2. Inform the SO that there is no food/fluid restriction needed.
3. Inform the SO that the test requires blood sample, tell who will do the test and when.
4. Inform that there will be a discomfort from needle puncture and pressure from the tourniquet.
During:
1. Support the patients arm upon insertion of the needle.
2. Be sure the patient remains still upon insertion of needle.
After:
1. Apply pressure to the punctured site.
2. Observe the venipuncture site for bleeding.
3. Explain that some bruising, discomfort, and or swelling maybe experienced at the site. Instruct to apply
warm, moist compress.
4. Send the specimen to the laboratory.
Diagnostic/ Date Ordered Indications Results Normal Analysis and
13
-
8/3/2019 Pneumonia Final Copy
14/68
Laboratory
Procedures
Date Results
In
Or
Purposes
Values Interpretation
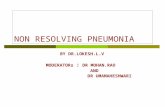
of ResultsChest X-Ray Date Ordered:
08/12/08
Date Results In:
08/12/08
This is done
to obtain or
detect
pulmonary
diseases
and the
status of
respiratory
problems or
trauma
There are hazy
infiltrates in the
Right lower lung
zone. The heart
is normal in size
and
configuration.
Diaphragms,
costophrenic
angles &
visualized bones
are intact.
Impression:
Pneumonitis,
Right Lower
Lung
Clear
lung fields
With continuous
formation of
exudates, the
involved lobe
undergoes
Consolidation of
the tissue
caused by filling
w/ exudates. In
chest x-ray, the
lung should
appear as black
because the lung
is not dense and
it permits the
passage of x-
rays. But in
lungs w/
pneumonia,
consolidated
parts become
dense and
14
-
8/3/2019 Pneumonia Final Copy
15/68
appear as white
areas on the
chest x-ray film.
Nursing Responsibilities:
Before:
1.Explain the procedure to the patient, its purpose and how it is done.
2. Inform the patient that there are no foods or fluid restriction.
3. Remove all jewelries and metal objects from the area to the image.
4. Ask the patient to remove her clothes and put on a hospital gown.
5. Assist the patient.
During:
1. Ensure the patients safety at all times.
2. Position the patient for specific views needed.
3. Ensure that the patient will remain motionless during the imaging.
After:
1. Assist the patient in dismounting from the radiography table and getting dressed.
15
-
8/3/2019 Pneumonia Final Copy
16/68
III. ANATOMY AND PHYSIOLOGY
ANATOMY
1. The SINUSES (frontal, maxillary, and sphenoidal) are hollow spaces in the
bones of the head. Small openings connect them to the nose. The functions
they serve include helping to regulate the temperature and humidity of air
breathed in, as well as to lighten the bone structure of the head and to give
resonance to the voice.
2. The NOSE (nasal cavity) is the preferred entrance for outside air into the
respiratory system. The hairs that line the wall are part of the air-cleaningsystem.
3. Air al so enter through the MOUTH (oral cavity), especially in people who
have a mouth-breathing habit or whose nasal passages may be temporarily
obstructed, as by a cold or during heavy exercise.
16
-
8/3/2019 Pneumonia Final Copy
17/68
4. The ADENOIDS are lymph tissue at the top of the throat. When they
enlarge and interfere with breathing, they may be removed. The lymph
system, consisting of nodes (knots of cells) and connecting vessels, carries
fluid throughout the body. This system helps to resist body infection by
filtering out foreign matter, including germs, and producing cells
(lymphocytes) to fight them.
5. The TONSILS are lymph nodes in the wall of the throat (pharynx) that
often become infected. They are part of the germ-fighting system of the
body.
6. The THROAT (pharynx) collects incoming air from the nose and mouth and
passes it downward to the windpipe (trachea).
7. The EPIGLOTTIS is a flap of tissue that guards the entrance to the
windpipe (trachea), closing when anything is swallowed that should go into
the esophagus and stomach.
8. The VOICE BOX (larynx) contains the vocal chords. It is the place where
moving air being breathed in and out creates voice sounds.
9. The ESOPHAGUS is the passage leading from the mouth and throat to the
stomach.
10. The WINDPIPE (trachea) is the passage leading from the throat
(pharynx) to the lungs.
11. The LYMPH NODES of the lungs are found against the walls of the
bronchial tubes and windpipe.
12. The RIBS are bones supporting and protecting the chest cavity. They
move to a limited degree, helping the lungs to expand and contract.
17
-
8/3/2019 Pneumonia Final Copy
18/68
13. The windpipe divides into the two main BRONCHIAL TUBES, one for
each lung, which subdivide into each lobe of the lungs. These, in turn,
subdivide further.
14. The right lung is divided into three LOBES, or sections. Each lobe is like a
balloon filled with sponge-like tissue. Air moves in and out through one
opening -- a branch of the bronchial tube.
15. The left lung is divided into two LOBES.
16. The PLEURA are the two membranes, actually one continuous one folded
on itself, that surround each lobe of the lungs and separate the lungs from
the chest wall.
17. The bronchial tubes are lines with CILIA (like very small hairs) that have
a wave-like motion. This motion carried MUCUS (sticky phlegm or liquid)
upward and out into the throat, where it is either coughed up or swallowed.
The mucus catches and holds much of the dust, germs, and other unwanted
matte that has invaded the lungs. You get rid of this matter when you cough,
sneeze, clear your throat or swallow.
18. The DIAPHRAGM is the strong wall of muscle that separates the chest
cavity from the abdominal cavity. By moving downward, it creates suction in
the chest to draw in air and expand the lungs.
19. The smallest subdivisions of the bronchial tubes are called
BRONCHIOLES, at the end of which are the air sacs or alveoli (plural of
alveolus).
20. The ALVEOLI are the very small air sacs that are the destination of air
breathed in. The CAPILLARIES are blood vessels that are imbedded in the
walls of the alveoli. Blood passes through the capillaries, brought to them by
the PULMONARY ARTERYand taken away by the PULMONARY VEIN.
18
-
8/3/2019 Pneumonia Final Copy
19/68
While in the capillaries the blood gives off carbon dioxide through the
capillary wall into the alveoli and takes up oxygen from the air in the alveoli.
Physiology
The exchange of gases (O2 & CO2) between the alveoli & the blood
occurs by simple diffusion: O2 diffusing from the alveoli into the blood & CO2
from the blood into the alveoli. Diffusion requires a concentration gradient.
So, the concentration (or pressure) of O2 in the alveoli must be kept at a
higher level than in the blood & the concentration (or pressure) of CO2 in the
alveoli must be kept at a lower lever than in the blood. We do this, of course,
by breathing - continuously bringing fresh air (with lots of O2 & little CO2)
into the lungs & the alveoli.
Breathing is an active process - requiring the contraction of skeletal
muscles. The primary muscles of respiration include the external intercostal
muscles (located between the ribs) and the diaphragm (a sheet of muscle
located between the thoracic & abdominal cavities).
19
http://www.sit.wisc.edu/~edrothen/flash/lungs.htmhttp://sorrel.humboldt.edu/~wva1/images%20respiration/lung_anatomy.gifhttp://www.sit.wisc.edu/~edrothen/flash/lungs.htmhttp://sorrel.humboldt.edu/~wva1/images%20respiration/lung_anatomy.gif -
8/3/2019 Pneumonia Final Copy
20/68
The external intercostals plus the diaphragm contract to bring about
inspiration:
Contraction of external intercostal muscles > elevation of ribs &
sternum > increased front- to-back dimension of thoracic cavity >lowers air pressure in lungs > air moves into lungs
Contraction of diaphragm > diaphragm moves downward >
increases vertical dimension of thoracic cavity > lowers air pressure in
lungs > air moves into lungs:
To exhale:
relaxation of external intercostal muscles & diaphragm > return of
diaphragm, ribs, & sternum to resting position > restores thoracic
cavity to preinspiratory volume > increases pressure in lungs > air is
exhaled
Intra-alveolar pressure during inspiration & expiration
As the external intercostals & diaphragm contract, the lungs expand.
The expansion of the lungs causes the pressure in the lungs (and alveoli) to
become slightly negative relative to atmospheric pressure. As a result, air
moves from an area of higher pressure (the air) to an area of lower pressure
(our lungs & alveoli). During expiration, the respiration muscles relax & lung
volume descreases. This causes pressure in the lungs (and alveoli) to become
slight positive relative to atmospheric pressure. As a result, air leaves the
lungs.
The walls of alveoli are coated with a thin film of water & this
creates a potential problem. Water molecules, including those on the alveolar
walls, are more attracted to each other than to air, and this attraction creates
a force called surface tension. This surface tension increases as water
molecules come closer together, which is what happens when we exhale &
our alveoli become smaller (like air leaving a balloon). Potentially, surface
20
http://sorrel.humboldt.edu/~wva1/images%20respiration/ventilation_diaphragm.gifhttp://sorrel.humboldt.edu/~wva1/images%20respiration/ventilation_diaphragm.gif -
8/3/2019 Pneumonia Final Copy
21/68
tension could cause alveoli to collapse and, in addition, would make it more
difficult to 're-expand' the alveoli (when you inhaled). Both of these would
represent serious problems: if alveoli collapsed they'd contain no air & no
oxygen to diffuse into the blood &, if 're-expansion' was more difficult,
inhalation would be very, very difficult if not impossible. Fortunately, our
alveoli do not collapse & inhalation is relatively easy because the lungs
produce a substance called surfactant that reduces surface tension.
Pulmonary Surfactant
Surfactant decreases surface tension which:
o increases pulmonary compliance (reducing the effort needed to
expand the lungs)
o reduces tendency for alveoli to collapse
Exchange of gases:
External respiration:
o exchange of O2 & CO2 between external environment & the
cells of the body
o efficient because alveoli and capillaries have very thin walls &
are very abundant (your lungs have about 300 million alveoli
with a total surface area of about 75 square meters)
Internal respiration - intracellular use of O2 to make ATP
occurs by simple diffusion along partial pressure gradients
Partial Pressure
it's the individual pressure exerted independently by a particular gas
within a mixture of gasses. The air we breath is a mixture of gasses:
primarily nitrogen, oxygen, & carbon dioxide. So, the air you blow into
a balloon creates pressure that causes the balloon to expand (& this
pressure is generated as all the molecules of nitrogen, oxygen, &
carbon dioxide move about & collide with the walls of the balloon).
21
http://oac.med.jhmi.edu/res_phys/Encyclopedia/Surfactant/Surfactant.HTMLhttp://oac.med.jhmi.edu/res_phys/Encyclopedia/Surfactant/Surfactant.HTML -
8/3/2019 Pneumonia Final Copy
22/68
However, the total pressure generated by the air is due in part to
nitrogen, in part to oxygen, & in part to carbon dioxide. That part of
the total pressure generated by oxygen is the 'partial pressure' of
oxygen, while that generated by carbon dioxide is the 'partial pressure'
of carbon dioxide. A gas's partial pressure, therefore, is a measure of
how much of that gas is present (e.g., in the blood or alveoli).
Factors involved in increasing respiratory rate
Chemoreceptors - located in aorta & carotid arteries (peripheral
chemoreceptors) & in the medulla (central chemoreceptors)
Chemoreceptors (stimulated more by increased CO2 levels than by
decreased O2 levels) > stimulate Rhythmicity Area > Result =
increased rate of respiration
22
-
8/3/2019 Pneumonia Final Copy
23/68
IV. THE PATIENTS ILLNESS (Book-Based)
Synthesis of the Disease
Community Acquired Pneumonia
1. Definition of the disease
Community-acquired pneumonia (CAP) is a disease in which
individuals who have not recently been hospitalized develop an infection of
the lungs (Pneumonia). CAP is a common illness and can affect people of all
ages. CAP often causes problems like breathing, fever, chest pains and a
cough. CAP occurs because the areas of the lung which absorb oxygen
(alveoli) from the atmosphere become filled with fluid and cannot work
effectively.
CAP occurs throughout the world and is a leading cause of illness and death.
Causes of CAP include bacteria, viruses, fungi, and parasites. CAP can be
diagnosed by symptoms and physical examination alone, though x-rays,
examination of the sputum and other tests are often used. Individuals with
CAP sometimes require treatment in a hospital. CAP is primarily treated with
antibiotic medication. Some forms of CAP can be prevented by vaccination.
2. Non-modifiable and Modifiable Factors
Non-modifiable Factors:
>Age
Pneumonia is more common among infants, young children, and the
elderly. With age, mucus accumulates within the respiratory passageways.
The mucus-cilia escalator is less able to move the mucus because it becomes
more viscous and the number of cilia as well as their rate of movement
decreases. This leads to increase susceptibility of the elderly to respiratory
infections such as pneumonia.
In children, their immune system is not yet well developed making
them susceptible in acquiring pneumonia.
23
-
8/3/2019 Pneumonia Final Copy
24/68
>Genetic Factors
A number of genetic disorders can predispose a person to pneumonia,
such as: Sickle cell anemia, cystic fibrosis, and Kartageners syndrome.
Modifiable Factors:
>Smoking and second-hand smoking
People who smoke have a much higher risk of developing pneumonia.
Also, those who regularly exposed to second-hand smoking are at risk for
pneumonia. In the case of the patient, she is exposed to second hand
smoking due to her husband who is a smoker.
>Alcohol and Drug Abuse
Alcohol and drug abuse makes a person more susceptible to
pneumonia.
>Crowded Living Conditions
The risk of pneumonia is increased among people living in crowded
conditions just like the area where the patient is exposed.
>Environmental Factors
Occupation exposure to toxic chemical fumes and smoke can weaken
the lungs defenses making a person susceptible in acquiring pneumonia.
Monia is exposed to smoke because of her husband who is a smoker.
3. Signs and Symptoms
>Fever and chills
An increase in body temperature accompanied by chills is due to the
invasion of microorganisms in the lungs that causes inflammation. The body
increases its temperature in order to kill the microbes. Monia experienced
recurrent fever and chills from July 30, 2008 to August 14, 2008.
>Pleuritic chest pain
24
-
8/3/2019 Pneumonia Final Copy
25/68
This is due to the constant irritation of the pleural membrane brought
about by inflammation, which stimulates the release of prostaglandin (pain
mediator) that acts on the pain receptors that causes pain.
>Cough and sputum production
There is an increase production of mucus due to the constant
inflammation of the epithelial lining of the bronchi and alveoli. Coughing is
the bodys mechanism to get rid of microorganisms and excess mucus. The
patient experienced cough from July 30, 2008 to August 15, 2008.
>Hemoptysis
Forceful coughing brought about by constant irritation of the
respiratory tract and consolidated alveolar exudates; damage the capillaries
in the lungs causing the production of blood-tinge sputum.
>Dyspnea
Difficulty in breathing is due to inflamed and fluid filled alveolar sacs
cannot exchange oxygen and carbon dioxide effectively. The patient
experienced dyspnea from July 30, 2008 to August 15, 2008.
>Headache
Impairment of oxygen and carbon dioxide exchange results in a
decrease in oxygenation in the brain that causes headache.
>Fatigue
Accumulation of lactic acid in tissues and muscles due to poor oxygen
perfusion brought about by impaired gas exchange in the lungs. The patient
experienced fatigue from July 29, 2008 to August 14, 2008.
4. Prevention and Health Promotion
Immunization against influenza and increasingly resistant pneumococci
can play a critical role in the prevention of pneumonia, particularly in
25
-
8/3/2019 Pneumonia Final Copy
26/68
immunocompromised and older adults. The influenza vaccine is formulated
and administered annually. Also, it is recommended that the vaccine be
offered to persons aged > 50 years; residents of chronic-care facilities;
patients who have chronic heart or lung disorders, and patients with chronic
metabolic diseases (including diabetes mellitus), renal dysfunction,
hemoglobinopathies, or immunosuppression.
Consequently, to prevent the development of pneumonia, one should
live a healthy lifestyle. Elimination of smoking habits, alcohol and drug abuse;
wearing of PPEs (such as mask) for persons who are exposed in smoke and
other chemicals; and adapting a regular exercise regimen are indeed a great
help in minimizing the incidence of pneumonia.
Stopping smoking is the best way to prevent pneumonia. Some
pneumonia can be prevented by vaccination. Oseltamivir or zanamivir
can be given to prevent influenza in household contacts of people who have
influenza and in people with heart or lung disorders who have not been
vaccinated because these people would be at risk of severe pneumonia if
they developed influenza.
(http://mayoclinic.com/health/pneumonia)
(http://www.lungusa.org/site)
26
-
8/3/2019 Pneumonia Final Copy
27/68
27
-
8/3/2019 Pneumonia Final Copy
28/68
V. THE PATIENT AND HIS CARE
A. MEDICAL MANAGEMENT
a. IVF
Medical
Management/
Treatment
Date Ordered
Date Performed
Date Changed
General
Description
Indications
Or
Purposes
Clients Response
to Treatment
D5NM 1L x 30 to 31
gtts/min
D.O: 08/12/08
D.P: 08/12/08
D.C: 08/15/08
It is a hypertonic
solution and it
contains Dextrose 5
gm NaCl 234mg,
Potassium Acetate
128mg, Sodium
Bisulfate 30mg.
Multiple electrolyte
maintenance
solution for use in
routine daily IV
therapy. It is given
to Monia in amount
sufficient to meet
her ordinary daily
water needs. It is
also a route of
administration of
her IV medicines.
Monias hydration
status was
maintained and
there were no signs
and symptoms of
hypersensitivity.
Nursing Responsibilities:
Before:
1. Verify the doctors order.
2. Explain the procedure to the patient.
3. Obtain necessary materials. Acquaint the SO and patient with the requirements needed for IV infusion.
28
-
8/3/2019 Pneumonia Final Copy
29/68
During
1. Check IV level.
2. Check for patency of tubing as well as infiltrations.
3. Check if the IVF is infusing well.
4. Practice aseptic technique.
After1. Adjust rate of flow of fluids appropriate to patients needs as prescribed.
2. Monitor IVF flow and patients response.
3. Monitor patient for evidence of local IV complications such as pain, swelling and tenderness.
4. Check for the presence of air in the tubing.
5. Record all procedure done.
b. Drugs
Name of
Drugs:
Date Ordered
Date
Route of
Administration
Indications
Or
Specific Foods
taken
Clients
Response to
29
-
8/3/2019 Pneumonia Final Copy
30/68
Generic Name
Brand Name
Performed
Date Changed
, Dosage and
Frequency of
Administration
Purposes the Meds with
Actual Side
EffectsGeneric Name:
Cefuroxime
Brand Name:
Ceftin
Date Ordered:
August 12, 2008
Dates Taken:
August 12-14,
2008
200 mg IV q 12
hours
Cephalosporin
antibiotics. - It
works by
stopping the
growth of
bacteria which
invades the
lungs causing
pneumonia.
Rice, fish,
vegetable,
meat, banana,
water.
The patient did
not show any
allergic
reactions. After
taking the drug
for 3 days,
Monia was
relieved from
productive
cough which
can be a sign
that the
bacteria that
invades the
lungs was
inhibited.
Nursing Responsibilities:
Before:
1. Explain the action of the drug to the client
30
-
8/3/2019 Pneumonia Final Copy
31/68
2. Check doctors order for the time, dosage and route of the drug.
3. Perform skin testing before administration
4. Obtain specimen for culture and sensitivity test.
During:
1. Re-check doctors order
2. Observe sterile technique3. Slowly push the medication to avoid irritation of the IV line.
After:
1. Educate client about the possible side effects
2. Document the action done
3. Observe for signs and symptoms of adverse or allergic reactions
Name of
Drugs:
Generic Name
Brand Name
Date Ordered
Date
Performed
Date Changed
Route of
Administration
, Dosage and
Frequency of
Indications
Or
Purposes
Specific Foods
taken
Clients
Response to
the Meds with
Actual Side
31
-
8/3/2019 Pneumonia Final Copy
32/68
Administration EffectsGeneric Name:
Paracetamol IV
Acetylcysteine
Brand Name:
Parvolex, Lysox
Date Ordered:
August 12,
2008
Date Taken:
August 12,
2008
Date Changed:
August 13,
2008 (shifted to
tab)
300 mg IV Analgesic and
Antipyretic. -
Thought to
produce
analgesia by
blocking pain
impulses by
inhibiting
synthesis of
prostaglandin in
the CNS or other
substances that
sensitize pain
receptors to
stimulation. The
drug may
relieve fever
through central
action in the
hypothalamic
heat regulatory
center.
This is indicated
for mild pain
and fever
experienced by
the patient.
The patient
responded
positively to the
medication. The
patients
recurrent fever
decreased from
40.50C to 37.80C
to 37.20C on
August 12,
2008.
Generic Name:
Paracetamol,
Date Ordered:
August 13,
500 mg/tab Analgesic and
Antipyretic. -
This is indicated
for mild pain
The patient
responded
32
-
8/3/2019 Pneumonia Final Copy
33/68
Acetaminophen
Brand Name:
Tylenol, Tempra
2008
Dates Taken:
August 13-14,
2008
Thought to
produce
analgesia by
blocking pain
impulses by
inhibiting
synthesis ofprostaglandin in
the CNS or other
substances that
sensitize pain
receptors to
stimulation. The
drug may
relieve fever
through central
action in the
hypothalamic
heat regulatory
center
and fever
experienced by
the patient.
positively to the
medication. The
patients
recurrent fever
decreased from
380C to 37.30C
on August 13,2008 and from
380C to 36.90C
on August 14,
2008.
Nursing Responsibilities:
Before:
1. Obey the 10 rights of giving medications
33
-
8/3/2019 Pneumonia Final Copy
34/68
2. Check the physicians order on the patients chart
3. Identify the patient
4. Warn the patient or SO that high doses or unsupervised long term use can cause liver damage
During:
1. Follow standard precautions during administration of the medication
2. Observe proper sterile technique
3. Administer right dose
After:
1. Check for the presence of adverse reactions such as vomiting, abdominal pain, drowsiness, rash and
urticaria
2. Record all procedures done and time of drug administration
3. Monitor temperature q 15 minutes after administration
Name of
Drugs:
Generic
Name
Brand Name
Date Ordered
Date
Performed
Date
Changed
Route of
Administration
, Dosage and
Frequency of
Administration
Indications
Or
Purposes
Specific Foods
taken
Clients
Response to
the Meds with
Actual Side
Effects
34
-
8/3/2019 Pneumonia Final Copy
35/68
Generic Name:
Ambroxol
Brand Name:
Seropram
Date Ordered:
August 12,
2008
Date Taken:
August 12-15,
2008
30 mg/tab A mucolytic
agent. - Which
hasantioxidant
properties and
stimulates the
release of
pulmonarysurfactant,
against
influenza-virus
proliferation in
the airwaywas
investigated in
mice.
It is administered
for the breakdown
of acid
mucopolysaccharide
fibers and to make
the sputum thinner
and less viscous andtherefore more
easily removed by
coughing.
Patient
responded well
to treatment
without signs of
adverse
reactions or
complicationssuch as
superinfection.
After taking the
drug for 4 days,
the patient was
relieved from
dyspnea and her
respiratory rate
decreases from
34bpm upon
admission to 26
bpm on August
13 to 24 bpm on
August 14 to 21
bpm on August
15 and 19 bpm
upon discharge.
35
-
8/3/2019 Pneumonia Final Copy
36/68
Nursing Responsibilities:
Before:
1. Obey the 10 rights of giving medications
2. Check the physicians order on the patients chart
3. Identify the patient.
4. Make sure that the patient is not pregnant which is one of the contraindications of the drug.
5. Strictly follow aseptic technique in preparation of IV medication
During
1. Caution to patient that the drug could cause gastric ulceration.
2. Observe proper sterile technique.
After:
1. Check for the presence of adverse reaction such as nausea and vomiting and mild gastric irritation.
2. Record all procedures done and time of drug administration.
c. Diet
Type of diet
Date Ordered
Date
Performed
Date Change
General
Description
Indications or
Purposes
Specific food
taken
Clients
Response and
or Reaction to
the DietDAT D.O: 08/12/08
D.P: 08/12/08
Regular diet
based of the 4
basic food
groups as long
For patients
whose condition
does not
necessitate a
Fish, meat,
bread, fruits,
vegetables, and
water.
The patient was
able tolerate the
diet as the
patient did not
36
-
8/3/2019 Pneumonia Final Copy
37/68
as the patient
can tolerate it.
modified diet developed any
allergies. There
is a boost in the
patients energy
level and
nourishment is
increased asevidenced by
patients ability
to perform her
self-care needs
and absence of
body malaise
and fatigue upon
discharge.Nursing Responsibilities:
Before:
1. Explain the diet or type of diet to patient
2. Feed patient in upright-position to prevent aspiration.
3. Give small frequent feeding.
4. Instruct strict compliance on the diet program given.
37
-
8/3/2019 Pneumonia Final Copy
38/68
d. Activity/Exercise
Type of Exercise
Date Ordered
Date PerformedDate Change
General
Description
Indications or
Purposes
Clients Response
and or Reaction tothe Exercise
Bed Rest Date Ordered:
08/12/08
A type of activity
wherein the patient
is in supine position
with his body lying
flat on bed with the
head raised using
This is indicated to
reduce the patients
oxygen demand, to
facilitate fast
recovery and avoid
complications. Rest
The patient was able
to take adequate
amount of rest and
sleep as evidenced
by absence of body
malaise, fatigue and
38
-
8/3/2019 Pneumonia Final Copy
39/68
pillows as support
to the head.
decreases the
bodys metabolic
rate.
normalization of
respiratory rate
from 34bpm upon
admission to 26
bpm on August 13
to 24 bpm on
August 14 to 21bpm on August 15
and 19 bpm upon
discharge.
Nursing Responsibilities:
1. Check for the doctors order
2. Explain to the SO the type of activity needed by the patient and why it is necessary
3. Ensure safety precautions by instructing SO not to leave patient alone at the bed since side rails are
not present or by putting pillows at the side of the patient to prevent the patient from falling
4. Stretch bed linens
5. Assist the patient in position changes to prevent bed sore formation
Type of Exercise
Date Ordered
Date Performed
Date Change
General
Description
Indications or
Purposes
Clients Response
and or Reaction to
the ExerciseDeep Breathing
Exercise
Date Ordered:
08/12/08
Designed to
improve the
To promote
oxygenation and
Monia was able to
demonstrate Deep
39
-
8/3/2019 Pneumonia Final Copy
40/68
efficiency of
ventilation,
decrease the work
of breathing,
increase of
excursion of the
diaphragm, andimprove the gas
exchange and
oxygenation
prevent respiratory
complications.
Breathing
Exercise/DBE and
had relief of her
difficulty of
breathing as
evidenced by
normalization ofrespiratory rate of
34bpm upon
admission to 26
bpm on August 13
to 24 bpm on
August 14 to 21
bpm on August 15
and 19 bpm upon
discharge
Nursing Responsibilities:
1. Explain the reason and rationale and aims of bed rest.
2. For DBE, have the patient assume a comfortable position and looses constrictive clothing.
3. Instruct the patient to place hands below the anterior costal margin and ask the patient to
breathe slowly and deep through the nose. Have patient keep shoulder related and upper chest
quite allowing the abdomen to rise. Tell patient to practice this three to four times for her to rest.
40
-
8/3/2019 Pneumonia Final Copy
41/68
41
-
8/3/2019 Pneumonia Final Copy
42/68
2. NURSING MANAGEMENT
1. Nursing Care Plan
Problem # 1: Ineffective Airway Clearance r/t Retained Secretions AEB Ineffective or Absent Sputum
Assessment Nursing
Diagnosis
Scientific
Explanation
Planning Nursing
Intervention
s
Rationale Expected
Outcome
Subjective
Cues
>
Objective
Cues
Patient
manifested:
> pursed lip
breathing
> increased
respiratory
rate (34 bpm
on August 12,
2008)
>non-
productive
Ineffective
Airway
Clearance
r/t
Retained
Secretions
AEB
Ineffective
or Absent
Sputum
Pneumonia is an
inflammation of
the lung
parenchyma
caused by
various
microorganisms
including
bacteria and
viruses. It affects
both ventilation
and diffusion.
Areas of the
lungs are not
adequately
ventilated
because of
Short Term:
> After 4
hours of NI,
patient will
demonstrate
behaviors to
improve
airway such
as deep
breathing
and
coughing
Long Term:
> After 1 to
3 days of NI,
patient will
1. establish
rapport
2. monitor
vital signs
3. elevate
head of bed
and change
position every
2 hours.
4. encourage
deep
breathing and
coughing
exercises.
5.provided
TSB
1. to gain
cooperation
2. to obtain
baseline
data
3. to
enhance
drainage
and
ventilation
to different
lung
segments.
4. to
maximize
respiratory
effort.
Short Term:
> patient shall
have
demonstrated
behaviors to
improve
airway such as
deep
breathing and
coughing
Long Term:
> patient shall
have
demonstrated
absence of
congestion
42
-
8/3/2019 Pneumonia Final Copy
43/68
cough
> rales heard
upon
auscultation
> irritability
>
restlessness>hyperthermi
a (380C/axilla
on August 12,
2008)
Patient may
manifest:
> difficulty of
breathing
> altered
chest
excursion
> use of
accessory
muscles to
breathe
> nasal
flaring
secretions. If a
patient is unable
to clear
secretions from
the respiratory
tract, ineffective
airway clearanceoccurs. The signs
and symptoms
include (+) DOB
due to the
presence of
secretions,
nonproductive
cough which
indicates
retained
secretions, high
RR which
indicates the
mechanism of
the body to gain
oxygen and fever
which occurs
demonstrate
absence of
congestion
with breath
sounds clear
and
improvedoxygen
exchange.
6. encourage
increase fluid
intake
7. encourage
warm versus
cold liquids
8.demonstrate
pursed lip and
diaphragmatic
breathing
9. encourage
opportunities
for rest
10. regulate
IVF as ordered
11. administer
meds as
ordered.
5. to lessen
fever.
6. to help
liquefy
secretions
7. to help
liquefysecretions
8. to
improve
airway
9. to
prevent or
lessen
fatigue
10. to keep
the patient
properly
hydrated
11. to
comply with
the
with breath
sounds clear
and improved
oxygen
exchange.
43
-
8/3/2019 Pneumonia Final Copy
44/68
> pale
conjuctiva
and mucous
membranes
> cyanosis
because of the
presence of
microbes in the
body. It acts as
the bodys
defense
mechanism.
therapeutic
regimen.
44
-
8/3/2019 Pneumonia Final Copy
45/68
-
8/3/2019 Pneumonia Final Copy
46/68
cough
Patient
may
manifest:
> difficulty
of
breathing> altered
chest
excursion
> use of
accessory
muscles to
breathe
> nasal
flaring
> pale
conjuctiva
and
mucous
membranes
filled lungs are
being covered
with mucus
secretions
causing the air
flow to be
blocked,therefore
difficulty of
breathing
may appear and
to compensate,
the patient will
exert effort to
breath rapidly
causing more
carbon dioxide
to be inhaled
than oxygen
leading cyanotic
manifestations.
evidence by
diminished
rales on
Lung fields
upon
auscultation
andimproved
respirations.
y
6. Encourage
increase fluid
intake
7. Encourageadequate rest
periods
between
activities
8. Assist
client to learn
breathing
exercises
9. Administer
medications
as ordered
cough
5. To mobilize
secretions
6. To facilitate
hydration
7. To limit
fatigue which
would increase
oxygen demand
8. To facilitate
effective
breathing
pattern
9. For
pharmacological
management
rales on
Lung fields
upon
auscultation
and
improved
respirations.
46
-
8/3/2019 Pneumonia Final Copy
47/68
Problem # 3: Hyperthermia
Assessme
nt
Nursing
Diagnosis
Scientific
Explanation
Planning Nursing
Interventions
Rationale Expected
OutcomeSubjective
Cues
>
Objective
Cues
Patient
manifested
:
> pursed
lip
breathing
>
increased
respiratory
rate (34
bpm on
August 12,
2008)
Hyperthermi
a
Pyrogens are
released in the
inflammation
process.
Pyrogens are
chemicals that
stimulate fever
production.
Pyrogens affect
the body
temperature-
regulating
mechanism in
the
hypothalamus
of the brain. As
a
consequence,
heat
Short Term:
>After 3-4
hours of NPI,
patient will
be able to
maintain
body
temperature
within
normal range
Long Term:
>After 5
days of NPI,
patient will
be free from
development
of possible
complication
1. Establish
rapport
2. Monitor vital
signs
3. Ascertain
understanding
of individual
nutritional
needs
4. Explain diet
modifications
such as:
increase protein,
carbohydrates
and vitamin C,
small frequent
1. To gain
patients
confidence and
cooperation in
treatment
regimen
2. Provides
comparative
baseline
3. To determine
what
information to
provide to SO
4. To promote
adequate
nutritional
Short Term:
Patient shall
have been
able to
maintain
body
temperature
within normal
range
Long Term:
Patient shall
have been
free from
development
of possible
complication
s
47
-
8/3/2019 Pneumonia Final Copy
48/68
>non-
productive
cough
Patient
may
manifest:
> difficultyof
breathing
> altered
chest
excursion
> use of
accessory
muscles to
breathe
> nasal
flaring
> pale
conjuctiva
and
mucous
membrane
s
production and
conservation
increase, and
body
temperature
increases.
Feverpromotes the
activities of the
immune
system, such
as
phagocytosis,
and inhibits the
growth of some
microorganism
s. In the
presence of
infection, fever
is concomitant
especially
when it has
become
systemic.
s feedings,
avoidance of
solid foods that
may lead to
indigestion
5. Promotepleasant/relaxin
g environment,
including
socialization
when possible
6. Note
presence and
absence of
sweating as
body attempts
to increase heat
loss by
evaporation,
conduction and
diffusion
intake
5. To promote
rest which
decreases the
metabolic
demand
6. Evaporation is
decreased by
environmental
factors of
humidity and
high ambient
temperature as
well as body
factors
7. To lower body
temperature
8. To facilitate
hydration status
48
-
8/3/2019 Pneumonia Final Copy
49/68
7. Promote
surface cooling
by tepid sponge
baths
8. Discuss
importance ofadequate fluid
intake
9. Administer
medications as
ordered
9. For
pharmacological
management
49
-
8/3/2019 Pneumonia Final Copy
50/68
Problem # 4: Risk for infection r/t to inadequate primary and secondary defenses
Assessme
nt
Nursing
Diagnosis
Scientific
Explanation
Objectives Nursing
Interventions
Rationale Expected
OutcomesS> O
O> Pt.
manifeste
d:
>hyperthe
rmia
>non-
productive
cough
>dyspnea
Patient
may
manifest:
Risk for
infection r/t
to
inadequate
primary and
secondary
defenses.
Pneumonia
involves the
inflammation of
the lung
parenchyma
which
eventually
leads to
decreased
cilliary action
and may
further lead to
stasis of
respiratory
secretions the
client is at risk
for spread of
Short Term:
After 4-6 of
NI the
patient will
be able to
prevent/
reduce risks
of spread of
infection.
Long Term:
After 3 days
of NI the
patient will
achieve
timely
>establish
rapport
>monitor and
recorded V/S
>encourage
proper hand
washing
techniques by all
caregivers
between
therapies/ clients
>provide for
isolation as
>for patient
cooperation
>serve as
baseline data
> a first line
defense against
nosocomial
infections
> reduces risk
of cross
contamination
Short Term:
After 4-6 of
NI, patient
shall have
prevented/
reduced risks
of spread of
infection.
Long Term:
After 3 days
of NI, patient
shall have
achieved
timely
50
-
8/3/2019 Pneumonia Final Copy
51/68
>
irritability
>
restlessne
ss
infection since
the continuous
production of
mucous
secretions is a
perfect
breeding placefor
microorganism.
The secondary
defense
mechanism of
the immune
system is also
inadequate
since the client
is suffering
from a
deceased
hemoglobin
level.
Resolution
of current
infection.
indicated
>change position
every 2 hours
>encourageintake of foods
rich in Vit. C such
as oranges.
>encourage
increase of fluid
intake
>administer/mon
itor medication
regimen
> to facilitate
secretion
movement and
drainage
>to help boost
the immunesystem
>To liquefy
secretion and
to avoid stasis
>To comply
with the
therapeutic
regimen
resolution of
current
infection
without
complications
.
51
-
8/3/2019 Pneumonia Final Copy
52/68
Problem #5: Deficient diversional activity r/t long term hospitalization AEB clients statement of boredom &
inability to perform ADL
Assessment Nursing
Diagnosis
Scientific
Explanation
Planning Nursing
Interventions
Rationale Expected
OutcomeS> maynip na
ku
O> pt. manifest:
Weakness
Irritability
Decrease
performan
ce
Restlessne
ss
Boredom
With VS as
follow:
T- 37 OC
P- 83 bpm
R- 21 bpm
B.P- 110/70
Deficient
diversional
activity r/t
long term
hospitalizatio
n AEB clients
statement of
boredom &
inability to
perform ADL
Prolong
hospitalizatio
n may cause
boredom
especially for
a person who
is use to
doing chores
or ADLs. Any
life change
that requires
numerous
readjustments
can be
perceived as
stressful. The
emotions &
physiological
arousal
Short Term:
After 4 hr. of
N.I, pt. will
engage in
satisfying
activities
within
personal
limitations
such as
chatting with
SO
Long Term:
After 3 days
of NI, pt. will
recognize
own
psychologica
Establish
rapport
Monitor and
record VS
Acknowledge
reality of the
situation &
feelings of pt.
Provide am and
pm care
Note impact of
illness on life
style by
comparing with
precious/norma
To gain trust
To have
baseline data
To establish
therapeutic
relationship
To provide
comfort
To validate
reality of
environment
al deprivation
Short Term:
After 4 hr. of
N.I, pt. shall
have
engaged in
satisfying
activities
within
personal
limitations
such as
chatting with
SO
Long Term:
After 3 days
of NI, pt.
shall have
recognized
52
-
8/3/2019 Pneumonia Final Copy
53/68
mmHg
Pt. may manifest:
Hostility
Withdrawa
l
Crying
Flat affect
Lack of
interest in
eating
created by
stressful
situation are
highly
uncomfortabl
e &
discomfortmotivates the
individuals to
do something
to alleviate it.
l response &
initiate
appropriate
coping
actions
l activity level
Encourage
diversional
activity like
talking to SO
and readingnewspaper
Encourage the
SO to be with
the pt. within
the whole
process of the
situation
Encourage the
SO to provide
the pt.
adequate rest
periods
To lessen
boredom
To provide
comfort andto ensure
that the pt. is
not alone
To prevent
fatigue and
for the pt. to
gain
maximum
strength
own
psychological
response &
initiate
appropriate
coping
actions
53
-
8/3/2019 Pneumonia Final Copy
54/68
2. Actual SOAPIEs
August 12, 2008
S> maskup ku salu
O> Received patient on high fowlers position with an IVF of #1 D5NM 1L
regulated at 30 to 31 gtts/min at 550cc level; signs and symptoms include:
(+)DOB, (+)nonproductive cough; with vital signs taken and recorded as
follows: T- 37.80C/axilla, PR- 86 bpm, RR 34 bpm, BP 110/70mmHg
A>Ineffective Airway Clearance related to Retained Secretions AEB
Ineffective or Absent Sputum.
P> After 4 hours of NI, patient will demonstrate behaviors to improve airway
such as deep breathing and coughing.
I> establish rapport
>monitor vital signs
>elevate head of bed and change position every 2 hours.
>encourage deep breathing and coughing exercises.
>provided TSB
>encourage increase fluid intake
> encourage warm versus cold liquids
>demonstrate pursed lip and diaphragmatic breathing
>encourage opportunities for rest
> regulate IVF as ordered
>administer meds as ordered
E> Goal met AEB patients ability to demonstrate behaviors to improve
airway such as deep breathing and coughing.
August 13, 2008
S>
54
-
8/3/2019 Pneumonia Final Copy
55/68
O>Received patient in right side-lying position, sleeping; with an IVF of #3
D5NM 1L regulated at 30 to 31 gtts/min at 650cc level; infusing well on the
right hand; with Hemoglobin of 10.2mg%; hematocrit 33.0 vol%,
segmenters 87%, lymphocytes 13% as of 08/12/08; with vital signs taken
and recorded as follows: T - 380C/axilla, PR- 81 bpm, RR 19 bpm, BP
120/70mmHg.
A> Risk for Infection related to Inadequate Secondary Defenses (decresed
Hgb, Hct and Lymphocytes level)
P> After 2hours of NI, patient will identify interventions to prevent or reduce
risk for infection.
I> established rapport
>monitored and recorded vital signs
>encouraged deep breathing exercises
>maintained adequate hydration
>emphasized necessity of taking medications (antibiotic)
>encouraged increase intake of Vitamin C rich foods
>encouraged increase fluid intake
>provided adequate rest periods
>due meds given
>needs attended
>referred accordingly
E> Goal met AEB patients ability to identify interventions to prevent or
reduce risk for infection.
VI. CLIENTS DAILY PROGRESS IN THE HOSPITAL
1. Clients Daily Progress Chart
Days Admission
August 12
August 13 August 14 August 15 Discharge
August 16Nursing ProblemsIneffective
55
-
8/3/2019 Pneumonia Final Copy
56/68
Airway
Clearance r/t
Retained
Secretions AEB
Ineffective or
Absent SputumIneffective
Breathing
Pattern r/t
Presence of
secretions
secondary to
Pneumonia
Hyperthermia Deficient
diversional
activity r/t long
term
hospitalization
AEB clients
statement of
boredom &
inability to
perform ADL
Risk for
infection r/t to
inadequate
primary and
secondary
defenses.
56
-
8/3/2019 Pneumonia Final Copy
57/68
Vital SignsTemperature 40.50
C
37.80
C
380C 380C 36.80C 36.90C
Pulse Rate 88bpm 81bpm 83bpm 90bpm 81bpmRespiratory
Rate
34bpm 26bpm 24bpm 21bpm 19bpm
Blood Pressure 110/70mmHg 120/70mmH
g
110/70mmH
g
110/80mmH
g
120/70mmH
gDiagnostic
and
Labora
tory
Proced
uresHemoglobin
Male: 13.5 18
Female: 12-16
10.2 mg%
57
-
8/3/2019 Pneumonia Final Copy
58/68
Hematocrit
Male: 40-54
Female: 37-47
33.0% vol.
WBC Count
Adult: 5-10 x103
10.750/cu.
mm.
Platelet Count
Adult: 150 - 450
280/cu. mm.
Segmenters
50-70%
87%
Lymphocytes
25-40%
13%
Chest X-Ray Medical
Manag
ementD5NM 1L x 30
to
31gtts/
min
DrugsAmbroxol Paracetamol IV Shifted
Cefuroxime Paracetamol
tab
DietDAT ExerciseBed Rest Deep Breathing
VII. DISCHARGE PLANNING
a. General Condition Upon Discharge
58
-
8/3/2019 Pneumonia Final Copy
59/68
Patient was not seen upon discharge on August 16, 2008 at 9:00 in the
morning.
b. METHOD
M>
E> Encouraged to perform deep breathing and coughing exercises, prevent
patient from engaging in strenuous activity or those that may cause fatigue.
T>
H> Instructed patient to wear loose clothes to prevent excessive sweating
> Imposed proper hand washing before and after eating
> Instructed patient to do chest tapping and postural drainage to mobilize
secretions
>Encouraged patient to eat foods rich in Vitamin C
>Encouraged patient to increase fluid intake
>Encouraged patient to always keep the back dry
> Encouraged patient to have adequate rest periods between activities
O> Advised patient to come back 1 week after discharge (August 23, 2008)
at the OPD Department
D> Encouraged patient to eat foods rich in protein such as meats, eggs and
beans.
> Encouraged patient to Include vitamin C in diet such as orange juice,
calamansi and mangoes
> Encouraged increase fluid intake
VIII. CONCLUSION
Learning is not attained by chance, it must be sought for with ardor
and attended to with diligence.
59
http://www.quotationspage.com/quote/3072.htmlhttp://www.quotationspage.com/quote/3072.htmlhttp://www.quotationspage.com/quote/3072.htmlhttp://www.quotationspage.com/quote/3072.html -
8/3/2019 Pneumonia Final Copy
60/68
-Abigail Adams-
Knowledge is not achieved by a mere snap of the fingers. There is so
much to learn learning that is very much important to be able to accomplish
responsibilities and in one way or another, encourage one to be committed in
his chosen profession. The pursuit for knowledge is every persons
responsibility. As student nurses, well-founded background knowledge is
essential so as to be able to render quality care to every patient.
With the completion of this case study, the group has learned a lot
about Pneumonia, which is a very prevalent disease in Philippines justified by
the statistics conducted by different organizations. It is an illness that could
be prevented if precautionary measures are practiced. The group also
learned that pneumonia can be a complication of other respiratory diseases
like tuberculosis.
Early detection and prompt management may drastically lessen the severity
of the disease condition.
There are preventive measures which the group recommends to lessen
the occurrence of pneumonia. The primary prevention is being vaccinated
with pneumococcal vaccine although this vaccine does not offer absolute
protection especially to people with low immunity. Proper hand washing
should also be practiced especially before eating and after using the
bathroom. A daily diet that includes foods rich in antioxidants, such as fresh-
dark-colored fruits and vegetables and other nutrients help boost a persons
immune system. Brisk walking and other aerobic exercises should be
practiced to help increase the lung capacity and breathing exercises which is
the taking of slow, deep, relaxed breaths and exhalation through pursed lips,
may also be helpful. Lastly, a person should avoid smoking.
IX. BIBLIOGRAPHY
Seeley, Rod, et. Al. Essentials of Anatomy and Physiology, 6th ed.
McGraw-Hill Companies, Inc. New York.
60
-
8/3/2019 Pneumonia Final Copy
61/68
Patton, Kevin T. Anatomy and Physiology, 5th ed. Mosby Inc. St. Louis,
Missouri. 2003.
Black, Joyce, and Hawk Jane Hokanson (2005) Medical-Surgical
Nursing
Yuan, Dr. Sara (2004), Hand Book of Diseases 3rd Edition
Professional guide to diagnostic tests, Lippincott Williams and Wilkins
Nurses quick check diagnostic tests, Lippincott and Wilkins
http://www.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=22576
http://people.eku.edu/ritchisong/RITCHISO/301notes6.htm
http://www.childbirths.com/cypress/ivtherapy.htm
http://search.live.com/results.aspx?
q=decreased+hemoglobin+and+hematocrit&FORM=AWRE2
http://www.childbirths.com/cypress/ivtherapy.htm
http://search.live.com/results.aspx?
q=decreased+hemoglobin+and+hematocrit&FORM=AWRE2
http://www.diagnosis.com/p/pneumonia/prevalence.htm
http://doh.gov.ph/data_stat/html/mortality.htm
http://www.sciencedaily.com/releases/2008/02/080213090516.ht
http://www.wddty.com/03363800369751974858/alternative-treatments-for-
pneumonia.html
http://mayoclinic.com/health/pneumonia/DS00135
X. APPENDICES
Appendix A
MORTALITY
61
-
8/3/2019 Pneumonia Final Copy
62/68
Ten Leading Causes of Mortality by Sex
Number, Rate/100,000 Population & Percentage
Philippines, 2003
Cause Male Femal
e
Both SexesNumber Rate Percent*
1. Heart Diseases38,67
729,019 67,696 83.5 17.1
2. Vascular System Diseases29,05
422,814 51,868 64.0 13.1
3. Malignant Neoplasm20,63
418,664 39,298 48.5 9.9
4. Accidents
27,72
0 6,246 33,966 41.9 8.6
5. Pneumonia15,83
116,224 32,055 39.5 8.1
6. Tuberculosis, all forms18,36
78,404 26,771 33.0 6.8
7. Symptoms, signs and
abnormal clinical, laboratory
findings, NEC
10,74
010,623 21,363 26.3 5.4
8. Chronic lower respiratory
diseases
12,99
8 5,907 18,905 23.3 4.8
9. Diabetes Mellitus 6,823 7,373 14,196 17.5 3.6
10. Certain conditions
originating in the perinatal
period
8,397 5,725 14,122 17.4 3.6
Source: The 2003 Philippine Health Statistics
* percent share from total deaths, all causes, Philippines
Last Update: January 11, 2007
Appendix B
Antipsychotic Drugs Increase Risk Of Developing Pneumonia In
Elderly, Study Suggests
62
-
8/3/2019 Pneumonia Final Copy
63/68
ScienceDaily (Apr. 16, 2008) Elderly patients who use antipsychotic drugs
have a 60 percent increased risk of developing pneumonia compared to
non-users. This risk is highest in the first week following prescription and
decreases gradually thereafter. Antipsychotic drugs are frequently used in
elderly patients for the treatment of psychosis and behavioral problems
associated with dementia and delirium. This study is the first to show that
the development of pneumonia is associated with antipsychotic drug use.
The risk of developing pneumonia is not associated with long-term use, but
is the highest shortly after starting the drug, say Drs. Rob van Marum and
Wilma Knol, authors of the study. They caution that all antipsychotic drugs
may be associated with pneumonia in elderly patients.
In nursing homes, up to 40 percent of residents may be prescribed
antipsychotics, according to the study. It has been suggested that, for
residents of nursing homes who receive antipsychotic therapy, more than
half are prescribed for inappropriate reasons.
Although literature shows limited efficacy and effectiveness for
antipsychotic drug use in the treatment of behavioral problems in dementia
patients, these drugs are frequently used for this purpose. In the last few
years it has become clear that the use of antipsychotic drugs in elderlypatients is also associated with an increased risk of death and morbidity.
The underlying mechanism for the association remains unclear. The authors
stress that clinicians may need to monitor patients for sedation after
initiation of antipsychotic medication and that a careful weighing of the
possible risks is recommended before starting antipsychotic treatment in
elderly people.
This study is published in Journal of the American Geriatrics Society.
Adapted from materials provided by Wiley-Blackwell.
Need to cite this story in your essay, paper, or report? Use one of the
following formats:
63
-
8/3/2019 Pneumonia Final Copy
64/68
APA
MLA
Wiley-Blackwell (2008, April 16). Antipsychotic Drugs Increase Risk Of
Developing Pneumonia In Elderly, Study Suggests. ScienceDaily. Retrieved
August 28, 2008, from http://www.sciencedaily.com
/releases/2008/04/080415111640.htm
Possible Target For Prevention And Treatment Of Pneumonia
Identified
ScienceDaily (Feb. 12, 2008) Researchers at Children's Hospital of
Pittsburgh of UPMC have identified a key protein target that may be a crucial
factor in the development of a vaccine to prevent and new therapies to treat
pneumonia, the leading killer of children worldwide.
Research led by Jay K. Kolls, MD, chief of the Division of Pediatric Pulmonary
Medicine, Allergy and Immunology at Children's, identified for the first time
the importance of a protein known as interleukin 22 (IL-22) in the immune
response to a strain of bacterial pneumonia. In the laboratory, the
researchers were able to effectively treat mice with pneumonia by using
purified IL-22.
"Currently there is no vaccine that covers all kinds of pneumonia and
antibiotic treatment is sometimes limited by antibiotic resistance. As acute
respiratory infections are the no. 1 killer of children in the world, progress in
the development of novel vaccines or new, more effective treatments is
critical," said Dr. Kolls, the Neils K. Jerne Professor of Pediatrics and
Immunology at the University of Pittsburgh School of Medicine. "Our results
64
-
8/3/2019 Pneumonia Final Copy
65/68
raise the possibility of developing new protein-based therapies using IL-22 to
limit or prevent pneumonia."
Pneumonia causes almost one in five deaths in children under age 5
worldwide -- more than 2 million children each year, according to the WorldHealth Organization. It kills more children than any other disease -- more
than AIDS and malaria combined.
IL-22 and interleukin 17A (IL-17A) are produced by a recently discovered
lineage of cells known as T Helper Type 17 (Th17). Children's researchers
found evidence that the Th17 cell lineage and its cytokines IL-22 and IL-17A
have evolved to promote host defense against certain infections in the lung
caused by extracellular pathogens.
This is an important discovery because the Children's research team
proposes that by stimulating the Th17 arm of the immune system, they can
more efficiently treat bacterial pneumonia. Furthermore, the researchers
propose that Th17 is a less critical pathway for intracellular bacteria such as
those that cause listeria and tuberculosis -- thus raising the potential to
target this pathway in diseases of chronic inflammation such as rheumatoid
arthritis or inflammatory bowel disease without increasing susceptibility to
these intracellaulr pathogens.
Dr. Kolls' laboratory investigates mechanisms of lung host defenses in
normal and immunocompromised hosts as well as lung immunology in
disease such as cystic fibrosis and asthma. Additional research interests of
Dr. Kolls include gene therapy, lung immunology, lung host defenses, tumor
necrosis factor, pneumocytis carinii pneumonia, ethanol, gene expression,
polymerase chain reaction and molecular biology.
Results of the study are published in the February online issue of Nature
Medicine.
Adapted from materials provided by Children's Hospital of Pittsburgh, via
EurekAlert!, a service of AAAS.
65
http://www.eurekalert.org/http://www.eurekalert.org/ -
8/3/2019 Pneumonia Final Copy
66/68
Need to cite this story in your essay, paper, or report? Use one of the
following formats:
APA
MLA
Children's Hospital of Pittsburgh (2008, February 12). Possible Target For
Prevention And Treatment Of Pneumonia Identified. ScienceDaily. Retrieved
August 28, 2008, from http://www.sciencedaily.com
/releases/2008/02/080211111323.htm
Appendix C
Community-acquired pneumonia
Community-acquired pneumonia (CAP) is a disease in which individuals
who have not recently been hospitalized develop an infection of the lungs
(pneumonia). CAP is a common illness and can affect people of all ages. CAP
often causes problems like breathing, fever, chest pains, and a cough. CAP
occurs because the areas of the lung which absorb oxygen (alveoli) from the
atmosphere become filled with fluid and cannot work effectively.
CAP occurs throughout the world and is a leading cause of illness and death.
Causes of CAP include bacteria, viruses, fungi, and parasites. CAP can be
diagnosed by symptoms and physical examination alone, though x-rays,
examination of the sputum, and other tests are often used. Individuals with
CAP sometimes require treatment in a hospital. CAP is primarily treated with
antibioticmedication. Some forms of CAP can be prevented by vaccination
CAUSES
Typical Bacterial Pathogens in CAP (approximately 85%)
66
http://en.wikipedia.org/wiki/Diseasehttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Pneumoniahttp://en.wikipedia.org/wiki/Breathhttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Chest_painhttp://en.wikipedia.org/wiki/Coughhttp://en.wikipedia.org/wiki/Oxygenhttp://en.wikipedia.org/wiki/Alveolihttp://en.wikipedia.org/wiki/Earth's_atmospherehttp://en.wikipedia.org/wiki/Bacteriahttp://en.wikipedia.org/wiki/Viruseshttp://en.wikipedia.org/wiki/Fungihttp://en.wikipedia.org/wiki/Parasiteshttp://en.wikipedia.org/wiki/Diagnosishttp://en.wikipedia.org/wiki/Symptomhttp://en.wikipedia.org/wiki/Physical_examinationhttp://en.wikipedia.org/wiki/X-rayhttp://en.wikipedia.org/wiki/Sputumhttp://en.wikipedia.org/wiki/Pharmacotherapyhttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Antibiotichttp://en.wikipedia.org/wiki/Medicationhttp://en.wikipedia.org/wiki/Preventive_medicinehttp://en.wikipedia.org/wiki/Vaccinationhttp://en.wikipedia.org/wiki/Diseasehttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Lunghttp://en.wikipedia.org/wiki/Pneumoniahttp://en.wikipedia.org/wiki/Breathhttp://en.wikipedia.org/wiki/Feverhttp://en.wikipedia.org/wiki/Chest_painhttp://en.wikipedia.org/wiki/Coughhttp://en.wikipedia.org/wiki/Oxygenhttp://en.wikipedia.org/wiki/Alveolihttp://en.wikipedia.org/wiki/Earth's_atmospherehttp://en.wikipedia.org/wiki/Bacteriahttp://en.wikipedia.org/wiki/Viruseshttp://en.wikipedia.org/wiki/Fungihttp://en.wikipedia.org/wiki/Parasiteshttp://en.wikipedia.org/wiki/Diagnosishttp://en.wikipedia.org/wiki/Symptomhttp://en.wikipedia.org/wiki/Physical_examinationhttp://en.wikipedia.org/wiki/X-rayhttp://en.wikipedia.org/wiki/Sputumhttp://en.wikipedia.org/wiki/Pharmacotherapyhttp://en.wikipedia.org/wiki/Hospitalhttp://en.wikipedia.org/wiki/Antibiotichttp://en.wikipedia.org/wiki/Medicationhttp://en.wikipedia.org/wiki/Preventive_medicinehttp://en.wikipedia.org/wiki/Vaccination -
8/3/2019 Pneumonia Final Copy
67/68
Streptococcus pneumoniae
Penicillin-sensitive S pneumoniae
Penicillin-resistant S pneumoniae
H influenzae
Ampicillin-sensitive H influenzae
Ampicillin-resistant H influenzae
Moraxella catarrhalis
(all strains penicillin resistant)
Atypical Respiratory Pathogens in CAP (approximately 15%)
Legionella species
Mycoplasma species
C pneumoniae
Rare Bacterial Pathogens in CAP
Klebsiella pneumoniae - Only in those with chronic alcoholism
Staphylococcus aureus - Postviral influenza setting
Pseudomonas aeruginosa - Only in patients with cystic fibrosis or
bronchiectasis
Nonpulmonary Pathogens in Pneumonia
Nonaeruginosa pseudomonads
Stenotrophomonas (Xanthomonas) maltophilia
Citrobacter freundii
Burkholderia (Pseudomonas) cepacia
Citrobacter koseri
Enterobacterspecies
Flavobacterium species
Enterobacter cloacae
Flavobacterium meningisepticum
Enterobacter agglomerans
Enterococcus species
Symptoms
67
-
8/3/2019 Pneumonia Final Copy
68/68
Symptoms of CAP commonly include:
problems breathing
coughing that produces greenish or yellow sputum
a high fever that may be accompanied with sweating, chills, anduncontrollable shaking
sharp or stabbing chest pain
rapid, shallow breathing that is often painful
Less common symptoms include:
the coughing up of blood (hemoptysis)
headaches (including migraine headaches)
loss of appetite
excessive fatigue
blueness of the skin (cyanosis)