
PMDA 2006 Alex T. Makris, MD, CMD. INFLUENZA New Issues and New Challenges.
58
PMDA 2006 PMDA 2006 Alex T. Makris, MD, Alex T. Makris, MD, CMD CMD
-
Upload
domenic-manning -
Category
Documents
-
view
217 -
download
0
Transcript of PMDA 2006 Alex T. Makris, MD, CMD. INFLUENZA New Issues and New Challenges.

PMDA 2006PMDA 2006
Alex T. Makris, MD, CMDAlex T. Makris, MD, CMD
INFLUENZAINFLUENZA
New Issues and New New Issues and New ChallengesChallenges

Centers for Disease Control and Prevention. Influenza Prevention and Control. Influenza. Available at: http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm.
Clinically Relevant Influenza Clinically Relevant Influenza VirusesViruses
Type AType A Potentially severe illnessPotentially severe illness
Epidemics and pandemicsEpidemics and pandemics
Rapidly changingRapidly changing
Type BType B Usually less severe illnessUsually less severe illness
EpidemicsEpidemics
Genetically more stableGenetically more stable
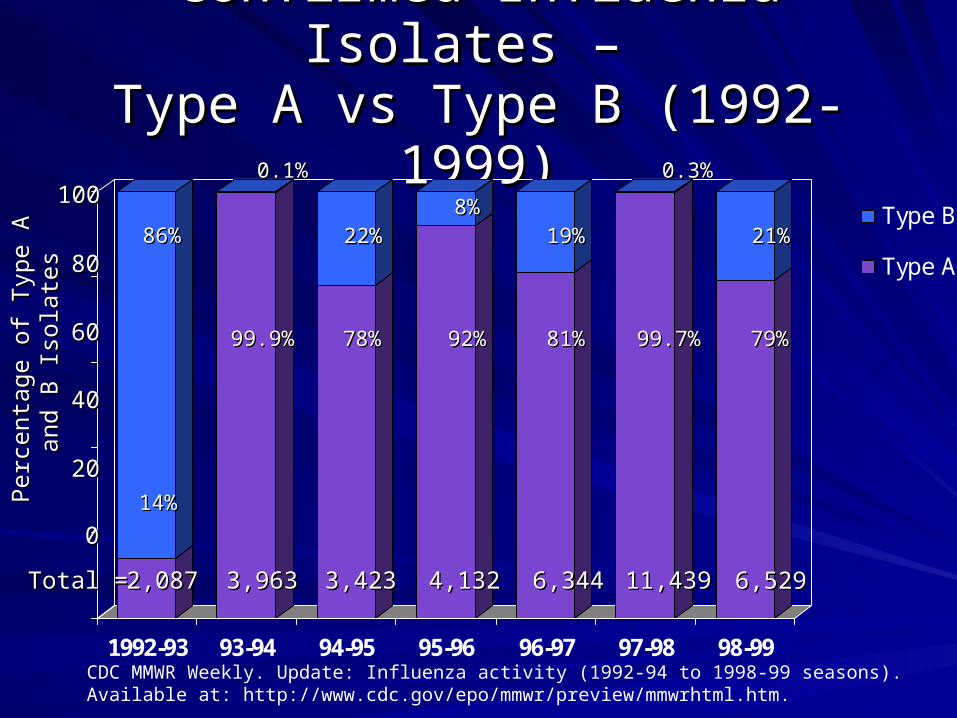
Confirmed Influenza Isolates – Confirmed Influenza Isolates – Type A vs Type B (1992-1999)Type A vs Type B (1992-1999)
CDC MMWR Weekly. Update: Influenza activity (1992-94 to 1998-99 seasons). Available at: http://www.cdc.gov/epo/mmwr/preview/mmwrhtml.htm.
1992-93 93-94 94-95 95-96 96-97 97-98 98-99
Type B
Type A86%86%
Total =Total = 2,0872,087 3,9633,963 3,4233,423 4,1324,132 6,3446,344 11,43911,439 6,5296,529
14%14%
0.1%0.1%
99.9%99.9%
22%22% 19%19% 21%21%8%8%
0.3%0.3%
78%78% 92%92% 81%81% 99.7%99.7% 79%79%
Per
cent
age
of T
ype
A
Per
cent
age
of T
ype
A
and
B I
sola
tes
and
B I
sola
tes
00
2020
4040
6060
8080
100100

YearsYears FluFlu VirusVirus MortalityMortality
1918-191918-19 “Spanish”“Spanish” Type A (H1N1) Type A (H1N1) 20 million worldwide20 million worldwide550,000 US550,000 US
1957-581957-58 “Asian”“Asian” Type A (H2N2)Type A (H2N2) 70,000 US70,000 US
1968-691968-69 “Hong Kong”“Hong Kong” Type A (H3N2)Type A (H3N2) 34,000 US34,000 US
Glezen WP. Epidemiol Rev. 1996;18:65.Centers for Disease Control and Prevention. Influenza Prevention and Control. Influenza. Available at:http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm.
Influenza Pandemics in the 20th Influenza Pandemics in the 20th CenturyCentury

Pneumonia and Influenza Pneumonia and Influenza Mortality Mortality
Rates by AgeRates by Age
0
20
40
60
80
100
120
<5 5-9 10-14 15-19 20-24 25-34 35-44 45-54 55-64 ≥65Age (yr)
Pe
r 1
0,0
00
Glezen WP. Epidemiol Rev. 1996;18:73, with permission.

NeuraminidaseNeuraminidase
HemagglutininHemagglutinin
RNARNA
Influenza Surface ProteinsInfluenza Surface Proteins
MM22 protein protein
(only on type A)(only on type A)

INFLUENZAINFLUENZA
TransmissionTransmission
PathophysiologyPathophysiology
Clinical ManifestationsClinical Manifestations

InfluenzaInfluenzaTransmissionTransmission
Aerosolized droplet spreadAerosolized droplet spread
Incubation period 18 - 72 hoursIncubation period 18 - 72 hours
Attack rate 10% - 50%Attack rate 10% - 50%
Outbreaks generally begin in confined Outbreaks generally begin in confined locationslocations
After initial cases, numbers usually peak After initial cases, numbers usually peak over 2-3 weeksover 2-3 weeks
Usually occurs Dec - AprilUsually occurs Dec - April
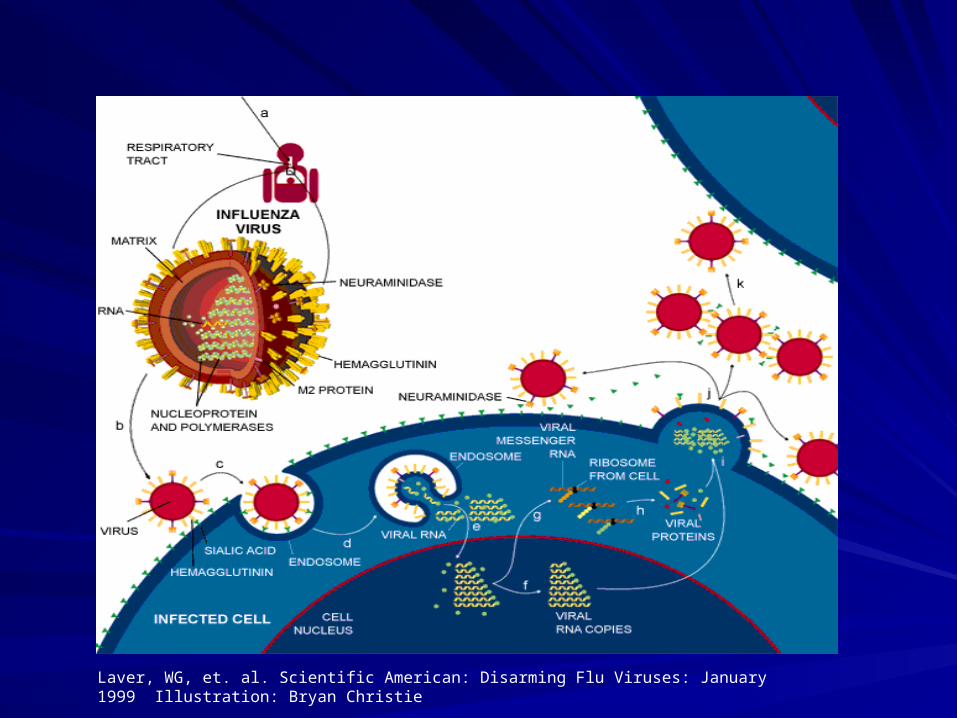
Laver, WG, et. al. Scientific American: Disarming Flu Viruses: January 1999 Illustration: Bryan Christie
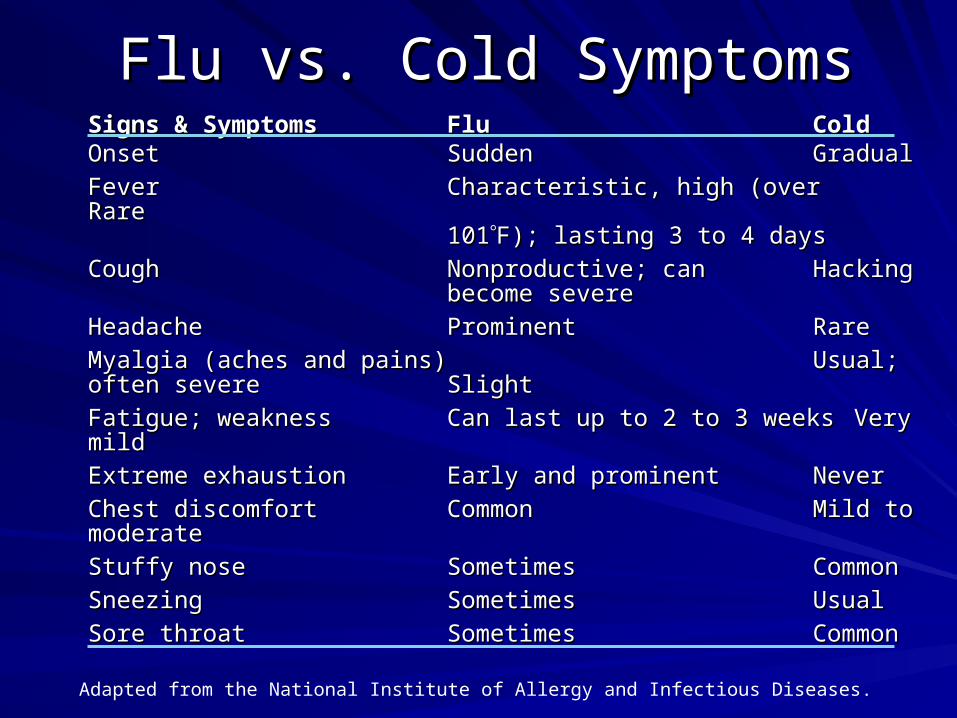
Adapted from the National Institute of Allergy and Infectious Diseases.
Signs & SymptomsSigns & Symptoms FluFlu ColdColdOnsetOnset SuddenSudden GradualGradual
FeverFever Characteristic, high (over Characteristic, high (over RareRare101101F); lasting 3 to 4 daysF); lasting 3 to 4 days
CoughCough Nonproductive; canNonproductive; can HackingHackingbecome severebecome severe
HeadacheHeadache ProminentProminent Rare Rare
Myalgia (aches and pains)Myalgia (aches and pains) Usual; often severeUsual; often severe Slight Slight
Fatigue; weakness Fatigue; weakness Can last up to 2 to 3 weeksCan last up to 2 to 3 weeks Very mildVery mild
Extreme exhaustionExtreme exhaustion Early and prominentEarly and prominent NeverNever
Chest discomfortChest discomfort CommonCommon Mild to Mild to moderatemoderate
Stuffy noseStuffy nose SometimesSometimes CommonCommon
SneezingSneezing SometimesSometimes UsualUsual
Sore throat Sore throat SometimesSometimes CommonCommon
Flu vs. Cold SymptomsFlu vs. Cold Symptoms

Diagnostic ToolsDiagnostic Tools
Weekly CDC activity reportsWeekly CDC activity reports
Clinical suspicionClinical suspicion
Viral isolationViral isolation
SerologySerology
PCRPCR
Immunofluorescence assaysImmunofluorescence assays
Rapid diagnostic testsRapid diagnostic tests

MANAGEMENT OPTIONSMANAGEMENT OPTIONS
Early vaccinationEarly vaccination
Infection Control MeasuresInfection Control Measures
Anti-influenzal agentsAnti-influenzal agents
Prophylaxis with anti-influenzal Prophylaxis with anti-influenzal agentsagents

Influenza & Influenza & Pneumococcal Pneumococcal ImmunizationsImmunizations
Guidance TrainingGuidance TrainingCFR 483.25(n) F334CFR 483.25(n) F334
Effective October 1, 2006Effective October 1, 2006
CMS

Determination of ComplianceDetermination of ComplianceSynopsis of RegulationSynopsis of Regulation
The influenza & pneumococcal vaccination The influenza & pneumococcal vaccination requirement has five aspects:requirement has five aspects:
1.1. The resident is provided education regarding The resident is provided education regarding the benefits & potential side effects of the the benefits & potential side effects of the vaccinations;vaccinations;
2.2. The facility must determine if a resident is The facility must determine if a resident is eligibility to receive the vaccinations.eligibility to receive the vaccinations.
3.3. The resident, or the resident’s legal The resident, or the resident’s legal representative, has the right to refuse the representative, has the right to refuse the vaccinations.vaccinations.
CMS

Determination of ComplianceDetermination of ComplianceCriteria for ComplianceCriteria for Compliance
4.4. Each eligible resident is administered the Each eligible resident is administered the influenza & pneumococcal vaccine (unless influenza & pneumococcal vaccine (unless refused or contraindicated or the resident refused or contraindicated or the resident has already been immunized); and has already been immunized); and
5.5. The facility must document that education The facility must document that education was provided and that the resident either was provided and that the resident either received the vaccine(s) or, if not received, received the vaccine(s) or, if not received, that the vaccine(s) was (were) refused or that the vaccine(s) was (were) refused or medically contraindicated or the resident medically contraindicated or the resident had already been immunized. had already been immunized.
CMS

Vaccination ProgramVaccination Program
Generally, vaccinate in late September, Generally, vaccinate in late September, OctoberOctober
Vaccinate through March Vaccinate through March – New admissions should be offered vaccineNew admissions should be offered vaccine– Generally takes ~ 2 weeks for protectionGenerally takes ~ 2 weeks for protection– If vaccination occurs during high activity levels If vaccination occurs during high activity levels
may need to provide chemoprophylaxis during may need to provide chemoprophylaxis during the 2 weeks after vaccination the 2 weeks after vaccination

MMWR. 1999;48:4.
Efficacy of the Influenza Efficacy of the Influenza VaccineVaccine
Most effective (70%-90%) in preventing Most effective (70%-90%) in preventing illness in persons aged <65 yrsillness in persons aged <65 yrs
30%-70% in preventing P/I hospitalization in 30%-70% in preventing P/I hospitalization in elderly not in chronic care facilityelderly not in chronic care facility
30%-40% in preventing illness in frail elderly30%-40% in preventing illness in frail elderly
50%-60% in preventing P/I hospitalization in 50%-60% in preventing P/I hospitalization in nursing home elderlynursing home elderly
80% in preventing death in nursing home 80% in preventing death in nursing home elderlyelderly

TypeType HemagglutininHemagglutinin NeuraminidaseNeuraminidase OriginOrigin Yr Yr
A (H1N1)/Sydney/5/93A (H1N1)/Sydney/5/93
B/Beijing/B/Beijing/184/93184/93
Naming Influenza VirusesNaming Influenza Viruses
Strain Strain Sequence Sequence
No.No.

2006 – 2007 Vaccine Composition2006 – 2007 Vaccine Composition
A/New Caledonia/20/1999 (H1N1)-likeA/New Caledonia/20/1999 (H1N1)-like
A/Wisconsin/67/2005 (H3N2)-likeA/Wisconsin/67/2005 (H3N2)-like
B/Malaysia/2506/2004-like antigensB/Malaysia/2506/2004-like antigens
Inactivated vaccineInactivated vaccine
Live, Attenuated Influenza Vaccine (LAIV)Live, Attenuated Influenza Vaccine (LAIV)

Characteristics of Influenza Characteristics of Influenza VaccinesVaccines
CharacteristicCharacteristic InactivatedInactivated LAIV (FluMistLAIV (FluMist™)™)
Route of Route of administrationadministration
Intramuscularly - Intramuscularly - annuallyannually
Intranasally - annuallyIntranasally - annually
CompositionComposition Killed virus:Killed virus:
Same antigenic Same antigenic makeupmakeup
Live, attenuatedLive, attenuated
Same antigenic Same antigenic makeupmakeup
IndicationIndication ≥≥ 6 months6 months 5 – 49 years5 – 49 years
Clinical IllnessClinical Illness Mild, localMild, local Mild signs/symptoms Mild signs/symptoms of influenzaof influenza
MMWR July 28, 2006/55(RR10); 1-42 Prevention and Control of Influenza

Avian InfluenzaAvian Influenza
H5N1 epizootic H5N1 epizootic
Human infections from direct contact with Human infections from direct contact with infected poultry/wild birdsinfected poultry/wild birds
Person Person → person transmission→ person transmission– Rare, Limited, UnsustainedRare, Limited, Unsustained
If sustained transmission, pandemic may If sustained transmission, pandemic may resultresult
Little pre-existing immunityLittle pre-existing immunity
CDC August 9, 2006 Avian Influenza: Current Situation

Avian InfluenzaAvian Influenza
No available vaccineNo available vaccineSx & Sx similar to circulating strainsSx & Sx similar to circulating strainsCases/deaths 2003 through August 2006Cases/deaths 2003 through August 2006– 241/141241/141
Cases/deaths 2006Cases/deaths 2006– 96/6496/64
Oseltamivir and Zanamivir are currently Oseltamivir and Zanamivir are currently effective for treatment and effective for treatment and chemoprophylaxischemoprophylaxiswww.who.int/csr/disease/avianinfluenza/en

Infection ControlInfection Control
AndAnd
Outbreak ManagementOutbreak Management

Outbreak ControlOutbreak Control
Recognize when a potential outbreak Recognize when a potential outbreak existsexists– Any activity above the usual for the FacilityAny activity above the usual for the Facility
Manage the active residentsManage the active residentsPrevent transmission to other residents Prevent transmission to other residents and staffand staff– Infection Control MeasuresInfection Control Measures– Treatment of active residentsTreatment of active residents– Chemoprophylaxis of uninfected residentsChemoprophylaxis of uninfected residents
Mode of TransmissionMode of Transmission
DropletsDroplets– Person Person → person→ person– Generated via cough, sneezing ( 3 feet)Generated via cough, sneezing ( 3 feet)
Mucosal surfacesMucosal surfaces
Inanimate surfaces laden with virusInanimate surfaces laden with virus
– Transmission from 24 hours prior and 5 days Transmission from 24 hours prior and 5 days after onsetafter onset
CDC December 23, 2005. Infection Control Measures for Preventing and Controlling Influenza Transmission in Long-Term Care Facilities

General Infection Control MeasuresGeneral Infection Control Measures
Annual influenza vaccinationAnnual influenza vaccinationStandard and Droplet PrecautionsStandard and Droplet PrecautionsPrivate room if possiblePrivate room if possibleCohort when possibleCohort when possibleActive surveillanceActive surveillanceTesting for new casesTesting for new casesLimit visitation Limit visitation Limit communal activitiesLimit communal activitiesLimit admissionsLimit admissionsProphylactic antiviralsProphylactic antiviralsCDC December 23, 2005. Infection Control Measures for Preventing and Controlling Influenza Transmission in Long-Term Care Facilities
Infection Control MeasuresInfection Control MeasuresStaff ManagementStaff Management
Reinforce hand washing importanceReinforce hand washing importanceProvide alcohol based hand gelsProvide alcohol based hand gelsDo not allow ill employees to workDo not allow ill employees to workIf outbreak confined to one unit; limit staff If outbreak confined to one unit; limit staff cross over to other unitscross over to other unitsIf possible, assign care givers to only ill or If possible, assign care givers to only ill or well residentswell residentsIf not, care for well residents first, then ill If not, care for well residents first, then ill residents residents
Influenza TreatmentInfluenza Treatment

Antiviral Agents for InfluenzaAntiviral Agents for Influenza
Amantadine, RimantadineAmantadine, Rimantadine– Only active against influenza AOnly active against influenza A– Significant CNS adverse effectsSignificant CNS adverse effects– Rapid, high levels of resistanceRapid, high levels of resistance
192/209 (92%) influenza A, 26 States192/209 (92%) influenza A, 26 States
– No longer recommended for treatment or No longer recommended for treatment or chemoprophylaxis of influenzachemoprophylaxis of influenza
MMWR July 28, 2006/55(RR10); 1-42 Prevention and Control of Influenza
Antiviral Agents for InfluenzaAntiviral Agents for Influenza
Zanamivir, Oseltamivir phosphateZanamivir, Oseltamivir phosphate– Neuraminidase inhibitorsNeuraminidase inhibitors– Treatment initiated within 48 hours of onset Treatment initiated within 48 hours of onset – Active against A, BActive against A, B– Approved for treatment of acute illnessApproved for treatment of acute illness– Approved for prophylaxisApproved for prophylaxis
Oseltamivir Oseltamivir ≥ 1yr≥ 1yr
Zanamivir ≥ 5 yrsZanamivir ≥ 5 yrs
– Zanamivir – inhalationZanamivir – inhalation– Oseltamivir – oral Oseltamivir – oral

Neuraminidase InhibitionNeuraminidase Inhibition
Influenza TreatmentInfluenza Treatment
Zanamivir (Relenza)Zanamivir (Relenza)– Delivery via inhalationDelivery via inhalation
Diskhaler deviceDiskhaler device
10 mg BID X 5 days10 mg BID X 5 days
Begin within 48 hours of onsetBegin within 48 hours of onset
Oseltamivir phosphate (Tamiflu)Oseltamivir phosphate (Tamiflu)– Delivery via oral route (suspension available)Delivery via oral route (suspension available)
75mg BID X 5days75mg BID X 5days
Begin within 48 hours of onsetBegin within 48 hours of onset

Influenza ProphylaxisInfluenza Prophylaxis
CDC CDC encouragesencourages the use of oseltamivir for the use of oseltamivir for chemoprophylaxischemoprophylaxis– 75 mg daily75 mg daily
Vaccinated elderly in aggregate living Vaccinated elderly in aggregate living settings may develop influenza or be settings may develop influenza or be susceptible to influenzasusceptible to influenza
www. cdc.gov/flu/professionals/treatment/0506antiviralguide.htm. CDC Influenza Antiviral Medications: 2005-06 Interim Chemoprophylaxis and Treatment Guidelines.

Chemoprophylaxis ManagementChemoprophylaxis Management
If confined to one unitIf confined to one unit– Implement infection control measuresImplement infection control measures– Provide chemoprophylaxis to unvaccinated Provide chemoprophylaxis to unvaccinated
staff and uninfected, unvaccinated residents staff and uninfected, unvaccinated residents on the uniton the unit
– If vaccinated residents have Sx & Sx provide If vaccinated residents have Sx & Sx provide chemoprophylaxischemoprophylaxis
– Continue prophylaxis for at least two weeks Continue prophylaxis for at least two weeks and for as long as one week after the last and for as long as one week after the last resident case occurredresident case occurred
CDC December 23, 2005. Infection Control Measures for Preventing and Controlling Influenza Transmission in Long-Term Care Facilities

Chemoprophylaxis ManagementChemoprophylaxis Management
If active cases occur on several unitsIf active cases occur on several units– Implement infection control measuresImplement infection control measures– Provide chemoprophylaxis to all unvaccinated Provide chemoprophylaxis to all unvaccinated
staff and uninfected, unvaccinated residents staff and uninfected, unvaccinated residents – If vaccinated residents have Sx & Sx provide If vaccinated residents have Sx & Sx provide
chemoprophylaxischemoprophylaxis– Continue prophylaxis for at least two weeks Continue prophylaxis for at least two weeks
and for as long as one week after the last and for as long as one week after the last resident case occurredresident case occurred
CDC December 23, 2005. Infection Control Measures for Preventing and Controlling Influenza Transmission in Long-Term Care Facilities

Clostridium difficile InfectionClostridium difficile Infection
New StrainNew Strain
New ChallengesNew Challenges

Clostridium difficileClostridium difficilePrevalencePrevalence
4% - 20% - LTCF without outbreak4% - 20% - LTCF without outbreak¹¹
10% - 20% may acquire during their stay²10% - 20% may acquire during their stay²
Rate of acquisition – 1 yr. follow up Rate of acquisition – 1 yr. follow up 0.52/1,000 rcds³0.52/1,000 rcds³
Incidence - AADIncidence - AAD– 1,600 per 1,000 resident years1,600 per 1,000 resident years¹¹
¹Gerding DN, et al. Infect Control Hosp Epidemiol 1995;16:459. ²Monsieur I, et al. Arch Gerontol Geriatr 1991;13:255. ³Simor AE, et al. Clin Infect Dis 1993;17:672

Clostridium difficileClostridium difficilePrinciples of Treatment - CDAD Principles of Treatment - CDAD Discontinue antimicrobial therapy if Discontinue antimicrobial therapy if possiblepossibleFluids and electrolytesFluids and electrolytesAvoid anti – peristaltic agentsAvoid anti – peristaltic agentsAvoid opiates Avoid opiates Mild casesMild cases– 15% - 20% will resolve with above measures15% - 20% will resolve with above measures¹¹
¹Olson MM et al. Infect Control Hosp Epidemiol 1994;15:371
Clostridium difficileClostridium difficilePrinciples of Treatment - CDADPrinciples of Treatment - CDAD
Specific therapy should be given orally Specific therapy should be given orally when possiblewhen possibleSpecific therapy should be continued for Specific therapy should be continued for 10 days10 daysTest of Cure cultures or toxin assays Test of Cure cultures or toxin assays should not be done in asymptomatic should not be done in asymptomatic patients¹patients¹– Does not predict clinical relapseDoes not predict clinical relapse
¹Fiengold SM Academic Press 1988:341

Clostridium difficileClostridium difficileTreatment Options - CDADTreatment Options - CDAD
Metronidazole Metronidazole
VancomycinVancomycin
Vancomycin + RifampinVancomycin + Rifampin
Probiotics Probiotics – Lactobacillus Lactobacillus – Saccharomyces boulardiiSaccharomyces boulardii
Ion-exchange resins - colestipolIon-exchange resins - colestipol
Clostridium difficile Current Clostridium difficile Current Guidelines forGuidelines for
Treatment - CDADTreatment - CDAD
Initial therapyInitial therapy– Metronidazole PO – 10 days Metronidazole PO – 10 days
1.0 – 1.5 gm/day for 10 days1.0 – 1.5 gm/day for 10 days¹ ¹
– Vancomycin PO – 10 daysVancomycin PO – 10 days500 – 1,000 mg/day for 10 days500 – 1,000 mg/day for 10 days²²
RelapseRelapse– Retreat with initial agentRetreat with initial agent³³
Cures 90% of recurrences Cures 90% of recurrences
¹Peterson LR et al. Verlog 1990:115 ²Gerding DN Infect Control Hosp Epidemiol 1995;15:8:459
3Simor et al Infect Control Hosp Epidemiol 2002;23:696
Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
Clinical improvement 2 – 4 daysClinical improvement 2 – 4 days
Symptoms remit 7 – 10 daysSymptoms remit 7 – 10 days
Relapse rates 10% - 20%Relapse rates 10% - 20%¹¹ ³³׳׳²²׳׳– Metronidazole – 7%Metronidazole – 7%²²,16%,16%³³– Vancomycin – 10%², 16%³Vancomycin – 10%², 16%³
¹Teasley DG et al. Lancet 1983;5: 1043 ²Olson MM et al. Infect Control Hosp Epidemiol 1994;15:371 ³Wenisch C et al. Clin Infect Dis 1996;22:813

Clostridium difficileClostridium difficileAsymptomatic Carriers Asymptomatic Carriers
No increased risk of CDAD in No increased risk of CDAD in asymptomatic carriers vs. non colonized asymptomatic carriers vs. non colonized patientspatients¹¹
Treatment of colonization does not reduce Treatment of colonization does not reduce risk of CDADrisk of CDAD²²
Metronidazole ineffective in eliminating the Metronidazole ineffective in eliminating the carrier statecarrier state³³
Vancomycin may prolong carrier stateVancomycin may prolong carrier state
¹Johnson S et al. Lancet 1990;336:97 ²Bender BS et al. Lancet 1986;ii:11 ³Johnson S et al. Ann Int Med 1992;117:297
Epidemic Strain
New strainNew strain – Appears to produce greater quantities of Appears to produce greater quantities of
toxins A and Btoxins A and B1,21,2
– Is more resistant to fluoroquinolonesIs more resistant to fluoroquinolones3,43,4
– Has a Has a tcdCtcdC gene deletion gene deletion22
– Binary toxin genes are presentBinary toxin genes are present
1. CDC Fact Sheet, July 2005. 2. Warny M, et al. Lancet. 2005;366:1079-1084.3. McDonald LC, et al. 42nd Annual Meeting of the Infectious Diseases Society
of America (IDSA); 2004. Abstract LB-2.4. McDonald LC, et al. N Engl J Med. 2005;353:2433-2441.

Markers of Severe DiseaseMarkers of Severe Disease
Decreased mental statusDecreased mental status
Severe abdominal distension, pain Severe abdominal distension, pain
Marked increase in white blood cell countMarked increase in white blood cell count
Hemodynamic instabilityHemodynamic instability

Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
Jacques Pepin et al. Clin Inf Dis 2005;40:1591Jacques Pepin et al. Clin Inf Dis 2005;40:1591– Retrospective review 1991-2004Retrospective review 1991-2004
Clinical diagnosis + toxin assayClinical diagnosis + toxin assay
Metronidazole therapyMetronidazole therapy– 250 mg QID – 500 mg TID250 mg QID – 500 mg TID
Relapse ratesRelapse rates
Metronidazole Metronidazole → Vancomycin → Vancomycin – Clinical failure Clinical failure
Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
1991-20021991-2002– Treatment failure with MetronidazoleTreatment failure with Metronidazole
9.6% (66/688)9.6% (66/688)
– Recurrence rate Recurrence rate < 60 days< 60 days15.2%15.2%
2003-20042003-2004– Treatment failure with MetronidazoleTreatment failure with Metronidazole
25.7% (112/435)25.7% (112/435)
– Recurrence rate Recurrence rate < 60 days< 60 days47.2%47.2%

Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
Daniel M Musher et al. Clin Infect Dis Daniel M Musher et al. Clin Infect Dis 2005;40:15862005;40:1586– 207 patients treated with Metronidazole207 patients treated with Metronidazole
Clinical cure - 50% (103/207)Clinical cure - 50% (103/207)Persistent symptoms – 22% (46/207)Persistent symptoms – 22% (46/207)Recurrence – 28% (58/207)Recurrence – 28% (58/207)

Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
Jacques Pepin et al. Clin Inf Dis Jacques Pepin et al. Clin Inf Dis 2005;41:12542005;41:1254– 1/1/03 – 6/30/041/1/03 – 6/30/04– All hospital admissionsAll hospital admissions– Clinical CDADClinical CDAD
Clostridium difficileClostridium difficileTreatment Outcomes - CDADTreatment Outcomes - CDAD
293 incident cases CDAD293 incident cases CDAD– 50.5% (148/293) in patients > 80 y.o.50.5% (148/293) in patients > 80 y.o.– 63.5% (186/293) received Fluoroquinolones 63.5% (186/293) received Fluoroquinolones – 21.8% (64/293) mortality < 30 d of diagnosis21.8% (64/293) mortality < 30 d of diagnosis

SummarySummaryExpanding spectrum of diseaseExpanding spectrum of disease
Epidemic strain has been identifiedEpidemic strain has been identified
Await updated guidelines (Spring 2007)Await updated guidelines (Spring 2007)
Role of vancomycin may be re-definedRole of vancomycin may be re-defined
Prevention is key!Prevention is key!– Infection control measuresInfection control measures– Judicious use of antibioticsJudicious use of antibiotics

Treatment – Complicated Treatment – Complicated InfectionsInfections
Vancomycin + Vancomycin + – Saccharomyces boulardiiSaccharomyces boulardii¹¹– Rifampin²Rifampin²– Lactobacillis³Lactobacillis³– Colestipol¹Colestipol¹
¹Feckety R Am J Gastroenterol 1997;92:739 ²Buggy BE J Clin Gastroenterol 1987;9:155 Gorbach SL Lancet 1987;ii:1519

Infection Control

Clostridium difficileClostridium difficileMode of TransmissionMode of Transmission
Direct ContactDirect Contact– Hand carriage - HCWHand carriage - HCW¹¹ ²²׳׳
Most likely plays major roleMost likely plays major role
– Environmental surfacesEnvironmental surfacesSpores – weeks or monthsSpores – weeks or months
Commodes, rectal thermometers Commodes, rectal thermometers
¹McFarland LV et al. N Engl J Med 1989;320:204 ²Fekety R et al. Am J Med1981;70:906

Clostridium difficileClostridium difficileInfection ControlInfection Control
Two major potential reservoirsTwo major potential reservoirs– Infected humansInfected humans
SymptomaticSymptomatic
ColonizedColonized
– Inanimate objectsInanimate objects
Nosocomial acquisition – 20%Nosocomial acquisition – 20%¹¹– Most asymptomaticMost asymptomatic
¹McFarland LV et al. N Engl J Med 1989;320:204

Clostridium difficileClostridium difficileInfection ControlInfection Control
Patients with CDAD and incontinence Patients with CDAD and incontinence should be in private roomsshould be in private rooms
Contact isolationContact isolation– Barriers with direct contactBarriers with direct contact– Barriers when contact with environmentBarriers when contact with environment
Dedicated equipment when possibleDedicated equipment when possible
Simor AE et al. SHEA Position Paper. Clostridium difficile in Long-Term Care Facilities for the Elderly 2002;23:696

Clostridium difficileClostridium difficileInfection ControlInfection Control
Meticulous hand hygieneMeticulous hand hygiene– Alcohol based hand gels are not sporocidal Alcohol based hand gels are not sporocidal
Environmental cleaning with sporocidal Environmental cleaning with sporocidal agents agents
Discontinuation of isolation when diarrhea Discontinuation of isolation when diarrhea subsidessubsides
Do not treat asymptomatic carriersDo not treat asymptomatic carriers
Simor AE et al. SHEA Position Paper. Clostridium difficile in Long-Term Care Facilities for the Elderly 2002;23:696


















