Plastic surgery in the United States of America: A comparative view
9
PLASTIC SURGERY IN THE UNITED STATES OF AMERICA: A COMPARATIVE VIEW 1 By NOEL THOMPSON, F.R.C.S. 2 Stoke Mandeville Hospital, Aylesbury, Bucks. " The national motto should fit the national facts. What I should write under America's flapping eagle would be: 'Vitality, Prosperity, Modernity'."--ALDOUS HUXLEY, 1926. " The Americano dreams vast dreams--challenges fate at every step and his whole life is a struggle."--H. L. MENCKEN, 1933. THE visiting of a score or so of major plastic surgical centres in the northern part of the United States of America over a period of six months, though allowing of little more than the collection of superficial impressions, has served to correct a sufficient number of the writer's preconceptions to prove of possible interest to others. It is implicit in any brief account such as this that many expressed views should be personal and all generalisations have occasional notable exceptions. It may be stated that any surgical centre of the first rank should have significant contributions to make in three integrated spheres of activity: clinical practice, post-graduate instruction, and medical research. This basic subdivision has, for convenience, been preserved in this discussion. CLINICAL PRACTICE Everyday plastic surgical practice differs fundamentally little on either side of the Atlantic. The free exchange of surgical knowledge and ideas between the United States and Britain resulting from the travels of peripatetic surgeons, and the interchange of professional journals using a shared language, has served to perpetuate a common background to surgical thinking having its inception at the time of the First World War, when American surgeons--of whom Dr George Webster Pierce (San Francisco) is still surgically and most hospitably active-- worked alongside our own founders of modern plastic surgery in Europe. Perhaps for the same reason the charge of slow operative technique so often levelled by British surgeons at their American colleagues (Ogilvie, 1937) and attributed to the influence of Halsted, would appear to have little relevance in the context of plastic surgery; for precise and celeritous surgery, leading American plastic surgeons can clearly compare with any in the world. Minor differences in national practice are usually attributable to the delay inevitably preceding acceptance of any advance, and may be expected to prove transitory. In this category may be cited the principle of "shaving" and skin grafting (Mr W. Hynes, Sheffield) which has contributed significantly to the treatment of certain types of extensive scars in Britain ; the onlay autogenous 1 This report is written in accordance with the terms of award, in the Junior Classification, 1959 Essay Contest of the Foundation of the American Society of Plastic and Reconstructive Surgery. 2 Present Address : Middlesex Hospital, London, W.I. 2 A io 9
-
Upload
noel-thompson -
Category
Documents
-
view
214 -
download
0
Transcript of Plastic surgery in the United States of America: A comparative view

PLASTIC SURGERY IN THE UNITED STATES OF AMERICA: A COMPARATIVE VIEW 1
By NOEL THOMPSON, F.R.C.S. 2
Stoke Mandeville Hospital, Aylesbury, Bucks.
" The national motto should fit the national facts. What I should write under America's flapping eagle would be: 'Vitality, Prosperity, Modernity'."--ALDOUS HUXLEY, 1926.
" The Americano dreams vast dreams--challenges fate at every step and his whole life is a struggle."--H. L. MENCKEN, 1933.
THE visiting of a score or so of major plastic surgical centres in the northern part of the United States of America over a period of six months, though allowing of little more than the collection of superficial impressions, has served to correct a sufficient number of the writer's preconceptions to prove of possible interest to others.
It is implicit in any brief account such as this that many expressed views should be personal and all generalisations have occasional notable exceptions.
It may be stated that any surgical centre of the first rank should have significant contributions to make in three integrated spheres of activity: clinical practice, post-graduate instruction, and medical research. This basic subdivision has, for convenience, been preserved in this discussion.
CLINICAL PRACTICE
Everyday plastic surgical practice differs fundamentally little on either side of the Atlantic. The free exchange of surgical knowledge and ideas between the United States and Britain resulting from the travels of peripatetic surgeons, and the interchange of professional journals using a shared language, has served to perpetuate a common background to surgical thinking having its inception at the time of the First World War, when American surgeons--of whom Dr George Webster Pierce (San Francisco) is still surgically and most hospitably active-- worked alongside our own founders of modern plastic surgery in Europe. Perhaps for the same reason the charge of slow operative technique so often levelled by British surgeons at their American colleagues (Ogilvie, 1937) and attributed to the influence of Halsted, would appear to have little relevance in the context of plastic surgery; for precise and celeritous surgery, leading American plastic surgeons can clearly compare with any in the world.
Minor differences in national practice are usually attributable to the delay inevitably preceding acceptance of any advance, and may be expected to prove transitory. In this category may be cited the principle of "shaving" and skin grafting (Mr W. Hynes, Sheffield) which has contributed significantly to the treatment of certain types of extensive scars in Britain ; the onlay autogenous
1 This report is written in accordance with the terms of award, in the Junior Classification, 1959 Essay Contest of the Foundation of the American Society of Plastic and Reconstructive Surgery.
2 Present Address : Middlesex Hospital, London, W.I.
2 A io 9

IIO BRITISH JOURNAL OF PLASTIC SURGERY
rib bone graft in children (Dr J. J. Longacre, Cincinnati); and the impressive use of direct composite flaps incorporating muscle for simultaneous reconstruction following radical malignant jaw resections (Drs F. S. Hoffmeister and V. Bakamjian, Buffalo).
The self-contained plastic surgery unit so often met with in Britain, with wards, operating theatre, dental department, and permanent surgical and nursing staff compactly concentrated in one hospital, has no exact parallel in the United States at present, although a trend in this direction can be discerned in the larger units. In the vast majority of instances, the American patient is situated in hospital in accordance with his fee-paying capacity rather than the anatomical or pathological nature of his illness, so that the American plastic surgeon visits all levels of the hospital on his rounds, and not infrequently three or four different hospitals in the same city.
A n inevitable sequel is the loss of specialised pre-operative and post-operative nursing care, as understood in Britain. All surgical dressings and wound care become the province of the attending surgeon or his surgical residents, the nursing staff in any one part of the hospital having little opportunity to experience the special problems involved in the care of the plastic surgical patient. Not infrequently the same may be said of the operating theatre, which may vary in situation and staffing from day to day.
It is usual for burned patients to be similarly scattered throughout all levels o f the building ; however, the modern construction of almost all American hospitals, with agolition of the open ward, immensely enhances the control able to be exercised over hospital wound infections, as compared with most British institutions, and of such importance in the treatment of the burned patient.
The usually harmonious liaison with dental colleagues in a closely integrated dental department traditional in British units was rarely paralleled on the American scene, and it was not unusual to find the simple but adequate intra-oral fixation of fractured jaws replaced by complex methods of internal fixation in order to eliminate the necessity for dental collaboration ; in one Middle Western centre eleven transfixing Kirschner wires were demonstrated in a single patient with multiple fractures of facial and jaw bones. Similarly limited was the contribution of the dental surgeon in the pre-operative phase of the primary cleft palate, which has done so much to simplify the surgical stage of repair in Britain.
Somewhat unexpectedly, surgical specialisation in the United States failed in many instances to reach a level ordinarily accepted in Britain. It is probably fair to state that in this country specialisation in medicine has been accepted with some reluctance and only as a demonstrable necessity in modern times. With the rapidly and constantly expanding frontiers of medical knowledge and the increasing complexity of therapeutic and diagnostic techniques, until the next evolutionary advance predicted by Metchnikoff (:9oI) has resulted in an extension of the human life span to something approaching 200 years, specialisation erected on a rational basis of general knowledge and experience has appeared the most logical of available alternatives : it is certainly likely to increase in Britain (Godber, :96:).
In the American cities visited, general anaesthesia continued to be administered by specially trained nurses in about one-third; radiotherapy was not a separate speciality in the vast majority, and the use of X-irradiation by the physician dermatologist in h i s" office "was common, so that radio-dermatitis was a frequently

PLASTIC SURGERY IN THE UNITED STATES OF AMERICA I i I
recurring lesion in American operating lists. An interesting and illuminating survey of the standing of plastic surgery as a recognised surgical speciality has shown that of the medical schools in the United States, only 43 per cent. have established full departments of plastic surgery, and 64 per cent. have plastic surgery out-patient clinics (Conway, i96I).
Peer (I96O) has recently criticised the resistance of American general surgeons to the growth of specialisation. It was noteworthy that in the Boston school of surgery--as well as in surgical centres elsewhere in which products of this school controlled departments of surgery--the growth of sub-specialities within J the field of surgery was being resisted in an attempt to perpetuate the myth of the general surgeon: a form of " flat-earthism" resulting in failure to establish a plastic surgery service under available plastic surgeons of vast experience and competence, such for example as Dr Bradford Cannon (Boston), who tended as a result to be used to salvage the plastic surgical failures referred from the general surgical service.
The high incidence of medico-legal actions brought by American patients against their medical attendants has introduced a degree of tension affecting adversely most phases of the patient-doctor relationship, from which British medicine has thus far remained blessedly free. It has been said that statistically every medical practitioner in the United States may expect to be involved in such legal actions once in every seven years. The annual premiums paid by American surgeons to insure against such actions varied from 35 ~ dollars (s in the Middle West, to as much as 73o dollars (~26o) in New York, and may be compared with the s s. (9 dollars) annual subscription standard in Britain.
On both sides of the Atlantic a serious shortage of nursing staff exists outside the major training schools, but it is noteworthy that in the United States more energetic measures have been adopted to alleviate this by relieving the nurse of all duties not immediately concerned with the skilled care of the sick patient. This is accomplished by the delegation of all unskilled aspects of nursing to dieticians, ward secretaries, nursing aides, and licensed vocational nurses, all of whom have a short training in the relevant practical techniques. Central Sterile Supply Departments are the rule in American hospitals (and the exception in Britain) with further conservation of nursing reserves (Lancet, I96I a), additional contributions directed to the same end being made by recovery wards attached to operating theatre suites, intensive nursing-care units where all seriously ill patients of whatever type may be concentrated, and the delegation of all intravenous procedures on patients to trained technicians. Further relief of stress on the nursing staff derives in the most modern hospitals from such measures as pneumatic- tube communication between wards and departments for the automatic transmission of clinical notes, drugs, etc. ; soiled-linen chutes direct from all foors to a basement laundry ; electric power-operated beds for patients and piped oxygen and suction to all beds. The universal use of the dictaphone in operating theatres, out-patient departments and wards, serves the double purpose of largely eliminating the doubtfully legible clinical note and conserving secretarial reserves.
POST-GRADUATE TRAINING
When conceding the better quality of American post-graduate surgical instruction, Sir Heneage Ogilvie, in I937, wrote words still applicable more than

I 1 2 B R I T I S H JOURNAL OF PLASTIC SURGERY
two decades later: " i n England we do not really teach our graduates at all ; once on the register they have to pick up what information they can working as house-surgeons, clinical assistants, or registrars, but there is no attempt to make them think or read, and no instruction apart from cramming courses for particular degrees." More recently a physician, Sir George Pickering (z962), has confirmed the persisting superiority of current North American post-graduate education. Specialist practice in the United States involves satisfying the speciality boards of the American Medical Association and Colleges, whose examinations can only be attempted after set periods of residency training in hospitals whose training
480 220 20
420 200 I~
360 ~lBO 16(
_o
_ o_ u J
L/I
mo & izo ~ ioo. C ~ n,,
.,='z = 120 ~ I00 80.
60 80
0 O0
,~ ,~" ~--PRACTITIONERS U.5./~ ~ " ~ ' .-/PLASTIC
,,._..=,.,,,~ , / ~ USA.
" / "~ULATION U,S,A.
/ 7
/ /
/ /
i / / /
60 .~- . . . . . ~"'. ~" PRACTITI0NERS ~...~.~..~...~"" . .G_T~. _ . ~ t l T I ~
. . . . . . . . . . . . . . "~ PLASTIC Si,IRGEONS . f " ~ - " ' - - - - " ~ POPULATION GT, BRITIAN
4C . . . . . " " , , _ ,GT, BRITIAN 194,$ 1948 1951 "lg54 19437 i960
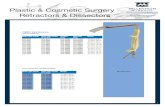
T h e relative rates of expansion of medical practitioners, plastic surgeons, and general population, in the United States and in
Great Britain during the period Z945-T960.
programmes and facilities have satisfied inspection by the Board. In recent times the Board in plastic surgery has demonstrated its determination that neither the seniority nor reputation of individuals can prevent the disapproval of training programmes falling below its established standards on inspection.
The very considerable thought and careful planning traditionally expended on the creation of systems of post-graduate training in the surgical centres of the United States is currently intensified by the urgent need for more trained surgeons of all types. A recent survey showed that in some States almost 3o per cent. of surgical operations were performed either by general practitioners or osteopaths (Coller, x957). The growth of specialisation and the increasing complexity of medical practice in modern times has rendered necessary a basic increase in the proportion of doctors in civilised communities. It may be seen (see illus.) that the slope of increase of medical practitioners since the Second World War is roughly comparable in both Great Britain and the United States, but whereas the population of Great Britain has remained essentially static during this period,

P L A S T I C SURGERY IN THE U N I T E D STATES OF AMERICA 113
that of the United States has expanded at a rate rendering the increase in medical graduates quite inadequate to the increased need. As a result exceptional career opportunities await the American medical graduate (Moore, I96o), especially in the case of the well-trained young plastic surgeon, for despite the dramatic rise in the numbers of plastic surgeons certified by the American College of Surgeons during the past fifteen years, this does not approach the rate of increase of general surgeons, which is itself quite inadequate to the expanding population requirements (Conway, I96I).
The shortage of doctors in the United States is intensified by the decrease in the number of applicants to American medical schools, which has declined by 37 per cent. during the decade ending in I959 (J. Amer. med. Ass., I96I), and is only partially relieved by the 8,392 emigrant doctors from foreign countries who were last year seeking United States registration (Lancet, I96r b).
This is in direct contrast with conditions in Great Brkain, where although the need for more surgical consultants is believed to exist (Platt, I96I ; Seale, I96I a), it cannot be met within the rigid constitution of the National Health Service functioning under the conditions of a relatively static population and fixed national economy. The only existing statistics show that during the five-year period ending in I96o an average of 6oo British doctors (about one- third of the output of the medical schools) emigrated annually, almost one-third of these going to the United States (Seale, I962), for reasons attributable to professional frustration, dissatisfaction, lack of research oppor- tunities (Lancet, I96I b), and in the opinion of one eminent but anonymous surgeon, " t h e tendency to-day for the top jobs, the top salaries, and the honours to go to the administrators rather than the clinicians and the researchers," in Britain (Harris, I96I).
To such basic differences in the state of medicine in the two countries may possibly also be attributed certain aspects of the contrasts in post-graduate surgical training methods. Where few consultant appointments are available it may be suspected to constitute an instrument of policy that the post-graduate training of the plastic surgeon should be prolonged in Britain (to four years in general surgery and a similar period in plastic surgery), while the antipodal state there existing results in its reduction in the United States (to three years general surgical and two or three years plastic surgical appointments).
However, the claim of the leading American training units to produce an adequately trained young plastic surgeon at the end of so limited a period is not lightly to be disregarded. The post-graduate instruction in such centres is not only intensive but carefully planned to achieve a balanced and integrated programme not seen in Britain, where the excessive clinical pressures exerted on under-staffed departments, as well as the obsessional concern of many senior British surgeons with routine operating lists and other clinical duties readily capable of delegation, must be held in major degree responsible. A Harvard professor of surgery has recently pointed out that he has in his department four times as many staff surgeons as a British teaching hospital unit of comparable size, his permanent staff being consequently relieved of the necessity of constantly operating on ward service patients, and so able to maintain adequate teaching and research activities (Moore, I96O). I f the British teaching hospital suffers in such a comparison, Picketing (I962) has underlined how much worse are the educational and research facilities in the regional hospitals where are to be found two-thirds of the junior trainee

114 BRITISH JOURNAL OF PLASTIC SURGERY
posts in British medicine--and in which, incidentally, are sited the great majority of British plastic surgical units.
As in Britain, so it not infrequently happens in American plastic surgical centres that the association of a special surgical interest with the chief of the clinic lends a special strength to the training of residents in one subsection of their speciality : brilliant examples are Dr Reed Dingman (Ann Arbor) in maxillo-facial surgery, Dr Henry Royster (Philadelphia) in malignant jaw surgery, and Dr William White (Pittsburgh) in hand surgery. It is, however, noteworthy that in many major American clinics, by virtue of associate surgeons developing alternative fields of special interest (often centred on a weekly clinic: that on cleft palates by Dr John Curtin with the dental collaboration of Dr S. Pruzansky, in Chicago, is a notable example) balance as well as completeness of graduate training results. Instances of the success attending such methods are afforded by the training units in New York Hospital--Cornell Medical College (New York), and in the University of Pittsburgh ; and though to his loss not able to be visited by the writer, Duke University (Durham, North Carolina) may justly be included in this company. In such centres the surgery of jaw malignancy, trauma, congenital deformity, the hand, and cosmetic disability tend to receive the specialised interest of a single associate.
In contrast to these units, and much more reminiscent of British plastic surgical centres in its eschewal of formal teaching and adherence to traditional surgical disciplines, may be cited the longest-established and famous clinic founded by Dr Vilray P. Blair in St Louis (Missouri), now under the dominion of Dr Barrett Brown. Here the writer observed no less than ten post-graduate trainees in plastic surgery, themselves observing an immense mass of varied but selected clinical material, treated--at a rate averaging about 3oo operations per month m with exemplary skill and despatch by four surgical associates, but with minimal opportunities for practical experience in any phase of therapy during training.
Difficulties remain to be surmounted in many American clinics in ensuring adequate practical experience for the surgical resident in training. The growth of voluntary hospitals and medical insurance schemes has resulted in the near extinction of the charity or service patient, so that the surgeon is placed in " a difficult moral and ethical posture when he undertakes to discharge his responsibilities for post-graduate education in relation to the care of people who are, after all, private patients " (Moore, I96o). Moreover, since the surgeon visits his private patients daily, and the senior resident sees all service patients daily, there is frequently little delegation of responsibility amongst the remaining, often numerous, residents in training.
MEDICAL RESEARCH
Sir Charles Snow (1959) has recently stated his belief that the scientific revolution in which we have lived for the past forty years is as pregnant with potential benefits for mankind, when compared with the antecedent industrial revolution, as was the latter by comparison with the agricultural revolution which preceded it.
There is evidence to suggest that the significance of the impact of the scientific revolution on modern medicine has received more enlightened recognition in the

P L A S T I C SURGERY IN THE U N I T E D STATES OF AMERICA I 1 5
United States than in Britain. In a Harvard symposium, attended by thewriter in Boston, in March I96I, Dr G. W. Thorn (Professor of Medicine) expressed the view that medical advances made during the past forty years exceeded in value the sum total of those made in the whole history of medicine prior to that time, and Dr E. D. Churchill (Professor. of Surgery) stated his conviction that a new renaissance in medicine is imminent, capable of producing revolutionary advances of greater significance than anything so far achieved.
That such views receive authoritative American recognition may be judged from the fact that in I96o the National Institutes of Health expended 2oo million dollars (s million) from Federal sources for medical research in the United States (Shannon, I96I); during the same year the Medical Research Council received from Parliament a grant of just less than s189 million for medical research in Great Britain (Report of the M.R.C., I959-6o). This contrast in official attitudes may be better appreciated when it is further realised that only half the monies spent on medical research in the United States derives from Federal sources, the remainder being contributed by industry, the foundations, voluntary agencies, etc. (Shannon, I96I).
It has been justly suggested that " in some fields of research in the United States brains are scarcer than money" (Brit. med. J., I96I), and it is probable that the American grants system, by making financial support over-dependent on published results, may tend to diminish the general level of research publications : it does, however, ensure that research ideas and talent can be subjected to the only valid test, that of practical trial. In Britain, by contrast, where with a high population and largely exhausted natural resources, " the only real assets we have, in fact, are our wits " (Snow, I959), it is difficult to avoid the conclusion that the failure of established authority adequately to appreciate the importance of medical research, rather than limited financial resources alone, is in major degree responsible for our failure to capitalise on what wits we have. In the National Health Service the natural tendency of government and society to expect the doctor to serve a strictly utilitarian end has gained a disproportionate ascendancy ; "cura t ive" medicine ministering to the immediate needs of sick individuals, dominates to the virtual exclusion of " progressive" medicine concerned with the advancement of knowledge. A distinguished British medical correspondent, writing in an American newspaper, confessed recently that " clinical research is neglected in British hospitals and not encouraged by the Ministry" (Marcus, I96o), and in I96o governmental grants to the Medical Research Council totalled the equivalent of about �89 per cent. of the cost of the National Health Service (Brit. med. J., I96I).
Plastic surgical centres visited by the writer in the United States almost without exception provided research facilities for even junior surgical staff, and a recent American survey has shown that more than 90 per cent. of medical schools in the United States either have established, or plan soon to introduce, research programmes on subjects related to plastic and reconstructive surgery (Conway, I96I).
The symbiotic association of the research laboratory with the plastic surgery clinic and training unit is remarkably illustrated in the major laboratories of Dr Lyndon Peer (Newark, N.J.)mwhose laboratory staff alone totals fourteen individuals, Dr Herbert Conway (New York) and Dr John M. Converse (New York), all of whom number pure scientists amongst their st~ff. The principle

I I 6 BRITISH JOURNAL OF PLASTIC SURGERY
of maintaining complementary contributions to both clinical and research fields is widely accepted, and has been successfully inherited by a second generation of young plastic surgeons, represented amongst many others by Dr Richard Stark (New York), Dr Blair Rogers (New York), Dr H. Griffith (Chicago), and Dr Peter Randall (Philadelphia). In many American training centres the residents in plastic surgery are, or soon will be, expected to spend a part of their training in the laboratory as an integral part of their surgical apprenticeship. By this means all may learn what contribution laboratory disciplines may make towards the solution of plastic surgical problems, and the scientific as well as the surgical potentialities of the individual may be developed.
Tissue transplantation is an ubiquitous subject for research investigation in American plastic surgery centres, with principal attention directed to the homograft. It is of melancholy interest to note by way of contrast that in Britain almost the whole of the considerable national contribution made in the field of homotransplantation research has been made outside plastic surgery units by others than plastic surgeons : and in many instances, as in the case of the most productive laboratory, with predominantly American financialaid (Medawar, 1962). Although much of the future of plastic surgery must be linked with advances in tissue transplantation, only one British plastic surgical unit is seriously engaged in such research at the present time ; due solely to the vision of the late Sir Archibald McIndoe, this venture is quite unsupported by the National Health Service.
In the context of the present world-wide shortage of doctors the current exodus of indigenous medical graduates from Britain is regarded by many authorities as likely soon to precipitate a critical situation in the National Health Service (Brit. med. J . , I962 ; Seale, I96I b). Realisation is not lacking that many emigrate to seek research opportunities not available at home, thereby limiting the possibility of future medical progress and creating difficulties in the filling of higher academic appointments in Britain (Lancet, I96I c). To those who have observed the American medical scene, it must appear confirmed that only if the will to break the deeply ingrained complacency of traditional attitudes exists amongst those having authority in the National Health Service, can the dynamic impetus which medical research might impart to practical therapy be sufficiently realised in British medicine.
My most grateful thanks are offered to my American hosts, too numerous for individual mention, whose unfailing courtesy and overwhelming kindness colour all recollections of this American tour.
REFERENCES
British Medical Journal (I96I), 2, 364. British Medicalffournal (1962), I, 1325. COLLER, F. A. (1957). Report to the American Surgical Association. CONWAY, H. (1961). Plast. reconstr. Surg., 28, 155. Golm~R, C. B. (1961). Brit. reed. ft., 2, 843. HARRIS, K. (1961). Observer., i l t h June. HUXLEY, A. (1926). " Jesting Pilate. The Diary of a Journey." London : Chatto
and Windus. Journal of the American Medical Association (1961), i76 , 292. Lancet (1961 a), z, 152. Lancet (1961 b), I, 43.

PLASTIC SURGERY IN THE UNITED STATES OF AMERICA
Lancet (1961 c), 2, 1298. MARCUS, A. (I96O). New York Herald Tribune, 2oth November. MEDAWAR, P. B. (1962). Personal communication. MENGKEN, H. L. (1933). Reprinted in " T he Vintage Mencken." Ed. A Cooke.
New York : Vintage Books Inc., 1959. METCHNIKOFF, E. (19Ol). " The Nature of Man ." London : Watts (English
translation), 1938. MOORE, F. D. (196o). Lancet, 2, 1339. OGILVIE, W. H. (1937). Reprinted in " Surgery Orthodox and Heterodox." Oxford :
Blackwell, 1948. PEER, L. A. (I96o). Plast. reconstr. Surg., 26, 341. PICKERING, G. (1962). Brit. med. ft., z, 421. PLATT, R. (I961). Brit. med. ft., Suppl., x, 290. Report of the Medical Research Council for the Year 1959-6o (1961). London : H.M.
Stationery Office. SEALE, J. R. (1961 a). Brit. med. ft., Suppl., 2, 171. - - - - (1961 b). Brit. med. ft., 2, 1554. - - (1962). Brit. med. ft., x, 782. SHANNON, J. A. (1961). Bull. N . Y . Acad. Med., 37, 3. SNow, C. P. (1959). " The Two Cultures and the Scientific Revolution." New
York : Cambridge University Press.
I I7
Submitted for publication, July I962.