PLANT POISONING
29
PLANT POISONING Dr. Hisham Zein Alabdin
description
PLANT POISONING. Dr. Hisham Zein Alabdin. POISONOUS PLANTS. The active principles in most of these plants are alkaloids but glycosides ( digitales ) and resinous materials, as cannabis also exist. - PowerPoint PPT Presentation
Transcript of PLANT POISONING
PLANT POISONING
Dr. Hisham Zein Alabdin
POISONOUS PLANTS
The active principles in most of these plants are alkaloids but glycosides (digitales) and resinous materials, as cannabis also exist.
The plant poisons have mainly remote action after their absorption. The route of poisoning is usually the oral one, so gastric lavage is indicated . each plant poison has its specific physiological antidote.
Atropine poisoning
Atropa belladonnas. Datura fastiosa, Datura strammonium ( thorn apple),
Plant contains ; atropine, hyoscine and hyoscayamine. All parts of the plant contain the active substance.
Atropine has 2 actions:1. central action causes stimulation of the CNS . In
large toxic doses it causes depression.2. peripheral action anticholenergic: atropine blocks
nicotinic and muscarinic effects of acetycholine.

Uses
A- Therapeutic:o Pre- anesthetic.o Antispasmodics.o In the treatment of peptic ulcer.o Ophthalmic use.o Nocturnal enuresis o Toxicological use: as antidote in phosphate esters,
digitalis, aconite poison.B- Non therapeutic: by addicts.
Toxicokinetics
Absorption : slowly absorbed from the gut.Metabolism: is in the liver and muscle to
tropine tropic acid.Excretion: is via the kidney in the urine, partly
unchanged and partly metabolized.
Pathophysiology
A- Central action: stimulation followed by depression of CNS.
Except hyoscine has depressant action only.B- Peripheral action:By blocking the muscarinic action of
acetylcholine at the post ganglionic nerves whether parasympathetic or sympathetic (sweat glands)
Clinical picture 1- Central effects:A- Stimulation phase:1-Delirium ,disorientation, confusion, loss of short
term memory, talkativeness(acute toxic psychosis).2-Ataxia, in-coordination, hallucination(Lilliputian
type)3-Occupational purposeless movements (picking or
grasping)4- Tremors and convulsions.
B- Depressant phase: it follows pre-existing stimulation phase . Patient is calm and falls into sleep then into stupor and coma. The respiration becomes slow and irregular. The end result will be central asphyxia and death.
II- Peripheral effects:
1- Vital signs:o Increased respiration.o Increased blood pressure.o Increased temperature up to atropine fever
resulting from anhydrosis.o Rapid pulse and may be cardiac arrhythmia.
2- Diminished secretion:o saliva dryness of the mouth with
dysarthria and dysphagia.o Sweat dry skino GIT constipation (decreased secretion and
motility)o Urinary oliguria and retention of urine
3- Blood vessels: Peripheral vasodilatation to increase heat loss , leading to atropine flush which may be misdiagnosed as scarlet fever.
4-Eye changes: o Dilation and fixed pupils blurred vision.o Loss of accommodation due to cycloplegia
(ciliary muscle paralysis)o Diplopia and photophobiao Loss of light reflex.
• The eye symptoms may be the earliest ones, thus the anticholinergic syndrome of parasympathetic paralysis can be remembered
Blind as a Bat.Red as a Beet.Dry as a Bone.Hot as a Hare.Mad as a Hen.
Treatment
Support respiration.Control convulsion if present by diazepam.Stop further absorption by inducing emesis or
by gastric lavage.The physiological antidotes ( physostigmine,
pilocarpine.).Treat hyperthermia by ice packsIV fluids to maintain urine output
DIGITALIS (FOX GLOVE)
Uses: As cardiac tonic for cases of congestive heart
failure.As diuretic.As an anti-arrhythmic especially in atrial
flutter and. fibrillation as well as in paroxysmal tachycardia
Toxicokinetics
• Digitalis preparations are rapidly absorbed from the GIT and injection sites . Metabolism takes place in the liver . Excretion is via the renal route mainly, a small part in the bile ( enterohepatic circulation).
Pathophysiology
Digitalis toxicity is an exacerbation of the drug Pharmacological actions:
Positive inotropic action: it increases the force and velocity of myocardial contraction by increasing intracellular Ca++ . This increase in the excitability and contractility of the atria and ventricles may result in extrasystoles and tachyarrhythmias.
Negative chronotropic action: (rate) It increases the vagal tone in the early stage leading to decreased heart rate.
Negative dromotropic action: (conduction velocity) It slows AV node conduction velocity that can be depressed resulting in Saor AV block.
It increases the refractory periods of AV node and depresses that of the atria and ventricles, resulting in prolonged PR interval , AV block and shortened QT interval.
Alteration of impulse formation with suppressant and excitatory effects.
Mechanism of action:
Digitalis inhibit active transport of Na+ ,K+ across cell membranes by binding to the Na+ - K+ ATP ase , and inhibiting Na+ - K+ pumps .
The net result Increase extracellular potassium Increase intracellular sodium. Increase intracellular calcium
Predisposing factors
Patient factor: (old age, myocardial infarction, core pulmonale, renal failure.)
Electrolyte abnormalities: ( hypo and hyperkalemia, hypomagnesemia, hyper and hypocalcemia.)
Drug interaction: (diuretics, antibiotics, quinidine , reserpine.)
Clinical picture Asymptomatic period of several minutes to
several hours follows a single oral toxic dose. The toxic effects include non cardiac and cardiac effects
A- Non cardiac :o GIT: may be the first complaints. (nausea,
vomiting, abduminal pain and diarrhea)o CNS: headache, trigeminal neuralgia, confusion,
delirium, disorientation, drowsiness and hallucination.
o Visual transient amblyopia, diplopia, blurring, scotoma and abnormal colour vision including yellow halos (xanthopsia).
o Endocrine : Gynecomastia.o Allergic : Urticaria.
B- Cardiac:Early slow full pulse (vagus) , with hypotension,
followed by any type of dysrhythmia (altration in cardiac rate and rhythm):
o AV block.o Atrial tachycardia with AV block.o Sino-atrial block.o Atrial flutter, fibrillation.o Ventricular premature extrasystoles , flutter.
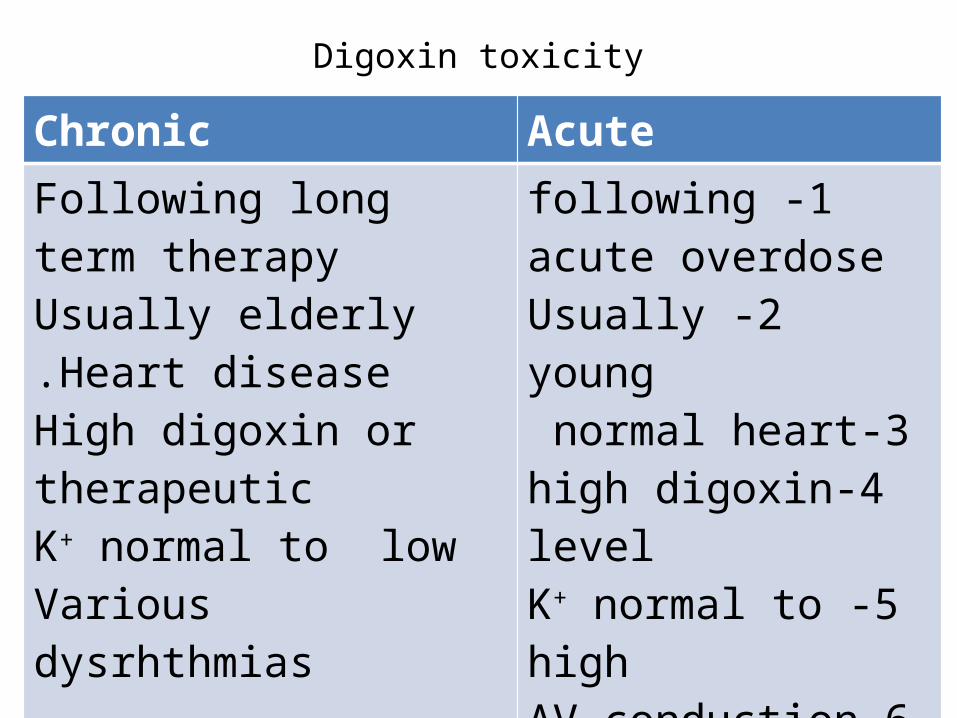
Digoxin toxicity
Chronic AcuteFollowing long term therapyUsually elderlyHeart disease.
High digoxin or therapeuticK+ normal to lowVarious dysrhthmias
Non cardiac symptoms prominent
1 -following acute overdose
2 -Usually young3-normal heart
4-high digoxin level5 -K+ normal to high
6-AV conduction blocks more common
7-Lessnon cardiac manifestations
MANAGEMENT
Investigations:1-ECG: o Prolonged PR intervalo Shortened QT intervalo ST segment depression, inverted T wave.2- Laboratory :o Electrolytes (K+ )o Serum digoxin: toxic level is above 2ng/ml and
is above 25ng/ml for digitoxin.
Treatment
Stop drug administration. monitor the patient in an ICU.Establishment of respiration.Dicontamination.Atropine sulphate 1-2mg IM for bradycardia.Phenytoin or diphenyl hydantoin is the drug of
choice for tachyarrhythmia. Cholestyramine help excretion of digitalis
Determine electrolytes hourly and correct electrolytes and acid base disturbances.
o For hypokalaemia: potassium chloride5g in fruit juice every hour until ECG show improvement or peaking of T wave.
o For hyperkalaemia : give 20 units of insulin with 5% Dextrose.
o For hypocalcemia: avoid replacement because intracellular calcium is very high.
Antidotal therapy: Digoxin specific antibody (Digibind ).They bind to the free digoxin and increase the renal excretion of digoxin bound to FAB fragment.
Indications for (DIGIBIND ) Hyperkalaemia (k + > 5 mEq/L). Bradyarrhythmias unresponsive to atropine.High degree AV block.Life threatenting ventricular tachycardia and
ventricular fibrillation.
THANK YOU