Placement of Ureteral Stent After Uncomplicated Ureteroscopy: Do We Really Need It?
9
Endourology and Stones Placement of Ureteral Stent After Uncomplicated Ureteroscopy: Do We Really Need It? Liang Tang, Xu Gao, Bin Xu, Jianguo Hou, Zhensheng Zhang, Chuanliang Xu, Linhui Wang, Yinghao Sun OBJECTIVE To investigate the role of stenting after uncomplicated ureteroscopy. METHODS This was a systematic review and meta-analysis of randomized controlled trials from MEDLINE, the Cochrane Central Search Library, and the EMBASE database. All of the studies reported various outcomes with or without stenting after ureteroscopy. RESULTS Fourteen trials were identified. As there was significant heterogeneity in pain assessment, difference in postoperative pain between the stent and nonstent groups was not clear. The incidence of dysuria, frequency, and hematuria was statistically significantly higher in stent group (relative risk [RR] 1.91, 95% confidence interval [95% CI] 1.18-3.08, dysuria; RR 2.23, 95% CI 1.48-3.36, frequency and urgency; RR 2.26, 95% CI 1.20-4.24, hematuria). There was no statistically significant difference in the postoperative analgesia requirement, urinary tract infections, postoperative fever, stone-free rate, and ureteral stricture between groups. There was a decreased tendency toward unplanned medical visits or hospital readmission in the stent group (RR 0.60, 95% CI .33-1.11), but the difference was not statistically significant. Combined analysis of the trials only used holmium laser or pneumatic lithotripsy showed no statistically significantly difference in unplanned medical visits between groups. Five studies found that ureteral stenting increased the expenses. Operation duration was significantly longer in the stent group (weighted mean difference 4.25, 95% CI 1.10-7.40). CONCLUSIONS A meta-analysis of the present literature revealed much benefit in the nonstent patient group. However, considering different outcome measures, marked clinical heterogeneity and various quality of, including trials, the place of stenting after uncomplicated ureteroscopy remains unclear. UROLOGY 78: 1248 –1256, 2011. © 2011 Elsevier Inc. W ith the development of smaller caliber semi- rigid and flexible ureteroscopes and the intro- duction of improved instrumentation, includ- ing the holmium:YAG laser, ureteroscopy (URS) has evolved into a safer and more efficacious modality for treatment of stones in all locations in the ureter with increasing experience worldwide. 1,2 The routine place- ment of ureteral stents after uncomplicated ureteroscopy is controversial. The main advantage of stenting is its effect of preventing ureteral obstruction and renal colic that may develop after stone retrieval. In addition, ure- teral stenting may help the passage of stone fragments and prevent delayed ureteral stricture. 3 However, many patients complain of flank and bladder discomfort during the process of implanting the ureteral stent. 4 The occurrence of these discomforts is believed to be associated with migration or breakage of the stent, infection, pyelonephritis, encrustation, and stone forma- tion. 5,6 Stent placement also requires additional costs. In addition, unless a pull string is used at the distal end of the stent, secondary cystoscopy is required to remove the stent, which is more costly and may potentially influence patients’ quality of life. The role of stenting in the management of patients after uncomplicated ureteroscopy remains debated. We performed a systemic review and meta-analysis to evalu- ate whether postoperative ureteral stenting is necessary after uncomplicated ureteroscopy. MATERIALS AND METHODS Search Strategy We obtained relevant trials from MEDLINE between 1966 and 2010, the Cochrane Central Search Library, and the EMBASE database between 1980 and 2010. All the studies included were Liang Tang, Xu Gao and Bin Xu share first authorship of this article. From the Department of Urology, Changhai Hospital, Second Military Medical University, Shanghai, China Reprint requests: Yinghao Sun, M.D., Department of Urology, Changhai Hospital, Second Military Medical University, 168 Changhai Road, Shanghai 200433, China. E-mail: [email protected] Submitted: March 6, 2011, accepted (with revisions): May 5, 2011. 1248 © 2011 Elsevier Inc. 0090-4295/11/$36.00 All Rights Reserved doi:10.1016/j.urology.2011.05.004
-
Upload
liang-tang -
Category
Documents
-
view
217 -
download
2
Transcript of Placement of Ureteral Stent After Uncomplicated Ureteroscopy: Do We Really Need It?

Endourology and Stones
Placement of UreteralStent After UncomplicatedUreteroscopy: Do We Really Need It?Liang Tang, Xu Gao, Bin Xu, Jianguo Hou, Zhensheng Zhang, Chuanliang Xu,Linhui Wang, Yinghao Sun
OBJECTIVE To investigate the role of stenting after uncomplicated ureteroscopy.METHODS This was a systematic review and meta-analysis of randomized controlled trials from MEDLINE,
the Cochrane Central Search Library, and the EMBASE database. All of the studies reportedvarious outcomes with or without stenting after ureteroscopy.
RESULTS Fourteen trials were identified. As there was significant heterogeneity in pain assessment,difference in postoperative pain between the stent and nonstent groups was not clear. Theincidence of dysuria, frequency, and hematuria was statistically significantly higher in stent group(relative risk [RR] 1.91, 95% confidence interval [95% CI] 1.18-3.08, dysuria; RR 2.23, 95% CI1.48-3.36, frequency and urgency; RR 2.26, 95% CI 1.20-4.24, hematuria). There was nostatistically significant difference in the postoperative analgesia requirement, urinary tractinfections, postoperative fever, stone-free rate, and ureteral stricture between groups. There wasa decreased tendency toward unplanned medical visits or hospital readmission in the stent group(RR 0.60, 95% CI .33-1.11), but the difference was not statistically significant. Combinedanalysis of the trials only used holmium laser or pneumatic lithotripsy showed no statisticallysignificantly difference in unplanned medical visits between groups. Five studies found thatureteral stenting increased the expenses. Operation duration was significantly longer in the stentgroup (weighted mean difference 4.25, 95% CI 1.10-7.40).
CONCLUSIONS A meta-analysis of the present literature revealed much benefit in the nonstent patient group.However, considering different outcome measures, marked clinical heterogeneity and variousquality of, including trials, the place of stenting after uncomplicated ureteroscopy remains
unclear. UROLOGY 78: 1248–1256, 2011. © 2011 Elsevier Inc.bitatsp
apaa
With the development of smaller caliber semi-rigid and flexible ureteroscopes and the intro-duction of improved instrumentation, includ-
ing the holmium:YAG laser, ureteroscopy (URS) hasevolved into a safer and more efficacious modality fortreatment of stones in all locations in the ureter withincreasing experience worldwide.1,2 The routine place-ment of ureteral stents after uncomplicated ureteroscopyis controversial. The main advantage of stenting is itseffect of preventing ureteral obstruction and renal colicthat may develop after stone retrieval. In addition, ure-teral stenting may help the passage of stone fragmentsand prevent delayed ureteral stricture.3
Liang Tang, Xu Gao and Bin Xu share first authorship of this article.From the Department of Urology, Changhai Hospital, Second Military Medical
University, Shanghai, ChinaReprint requests: Yinghao Sun, M.D., Department of Urology, Changhai Hospital,
Second Military Medical University, 168 Changhai Road, Shanghai 200433, China.
E-mail: [email protected]Submitted: March 6, 2011, accepted (with revisions): May 5, 2011.
1248 © 2011 Elsevier Inc.All Rights Reserved
However, many patients complain of flank and bladderdiscomfort during the process of implanting the ureteralstent.4 The occurrence of these discomforts is believed toe associated with migration or breakage of the stent,nfection, pyelonephritis, encrustation, and stone forma-ion.5,6 Stent placement also requires additional costs. Inddition, unless a pull string is used at the distal end ofhe stent, secondary cystoscopy is required to remove thetent, which is more costly and may potentially influenceatients’ quality of life.The role of stenting in the management of patients
fter uncomplicated ureteroscopy remains debated. Weerformed a systemic review and meta-analysis to evalu-te whether postoperative ureteral stenting is necessaryfter uncomplicated ureteroscopy.
MATERIALS AND METHODS
Search StrategyWe obtained relevant trials from MEDLINE between 1966 and2010, the Cochrane Central Search Library, and the EMBASE
database between 1980 and 2010. All the studies included were0090-4295/11/$36.00doi:10.1016/j.urology.2011.05.004

qaobst
tbt(C
lindi
randomized controlled trials regarding whether double-J stentsshould be placed after uncomplicated ureteroscopy for treat-ment of ureteral stones or diagnostic or therapeutic ureteros-copy for upper tract transitional cell carcinoma in adults (only3 patients in 1 trial accepted ureteroscopy for upper tracttransitional cell carcinoma).
Quality Assessment and Data AbstractionThe articles were retrieved and assessed for inclusion accordingto the prior criteria by 2 researchers independently. Quality ofthe trials was assessed according to the criteria of the CochraneRenal Group 7 (Table 1).
All data from the literature was retrieved by 1 researcher, anduality was controlled by a second researcher with respect tollocation concealment, use of the blind method, completenessf follow-up, and intention-to-treat analysis. Any discrepancyetween the 2 reviewers was evaluated and adjudicated by thetudy group. If important data were lacking, we would attempto contact the author.
Characteristics of the Studyand Quantitative Analysis of the DataA combined quantitative analysis would be performed when 2
Table 1. Assessment of quality criteria for included trials
Study (author andreference)
AllocationConcealment Intention-t
Borboroglu et al.,8
2001Adequate Six participants rand
stents removed franalysis because
Byrne et al.,1
1995NA NA
Chen et al.,10
2002Adequate NA
Cheung et al.,11
2003Inadequate NA
Damiano et al.,12
2004Adequate NA
Denstedt et al.,13
2001Adequate 13 patients exclude
balloon dilatationJeong et al.,14
2004NA NA
Netto et al.,15
2001NA NA
Srivastava et al.,16
2003Adequate NA
Shao et al.,17
2008NA Three patients were
before randomizatperforation duringureteral stricture astone
Ibrahim et al.,18
2008Adequate NA
Kenan et al.,19
2008NA NA
Xu et al.,20 2009 NA Ten patients were rethey did not meetintraoperative elig
Cevik et al.,21
2011NA Two patients had ur
the procedure andlost to follow-up. Texcluded from the
NA � not available (insufficient information provided).* None of the trials provided sufficient information to determine b
or more studies reported the same outcome. Relative risks were
UROLOGY 78 (6), 2011
calculated for dichotomous data and weighted for mean differ-ences, with 95% confidence intervals for continuous data. Afixed effect model (Mantel–Haenszel) was used unless there wasevidence of substantial statistical heterogeneity, in which casethe DerSimonian and Laird random effect model would be used.Statistical heterogeneity of treatment effect between studieswas formally tested with Cochran’s test for heterogeneity (P �.1). The I2 statistic was also examined.
Possible sources of heterogeneity, including participants,reatments and study quality were explored. Data that could note combined for quantitative analysis were assessed qualita-ively. All meta-analyses were performed using Review ManagerRevMan 4.2.10, The Nordic Cochrane Centre, The Cochraneollaboration, 2006, Copenhagen, Denmark).
RESULTSOf 490 potentially related articles retrieved, 461 werenonrandomized studies and excluded. The remaining 39articles were evaluated in detail, of which 25 were alsoexcluded because they did not meet our inclusion crite-ria. Finally, 14 articles were used for meta-analysis. The14 clinical trial research articles were published between
at AnalysisCompleteness of
Follow-up Blinding*
zed to group withoutrotocol andtraoperative injury
Reported NA
Reported NA
Reported NA
Reported NA
Reported NA
m trial because of Reported NA
Reported NA
Reported Surgeon
Reported NA
uded from study1 for ureteralration and 2 forciated with the
Reported NA
Reported Patients andsurgeons
Reported NA
ed from study assecondaryy criteria
reported NA
l perforation duringther patients weree 4 patients werey
Reported NA
ng of participants or outcome assessors.
o-Tre
omiom pof in
d fro
exclion,opesso
movtheibilitetera2 ohesstud
2001 and 2010. The reported length of hospital stay after
1249

t
7d
urFt
dcb
1
tsw
s
sph9dtC
UFt
uabuh(w
mi9otug
UU
ureteroscopy varied from a few hours for outpatients9,13
to 2-3 days.14,16,19 In 2 trials, the length of hospital stayvaried on a case-to-case basis.8,11 Two trials reported a1-day hospital stay,10,12 and 5 trials did not report post-operative hospital stay.15,17,20,21 In 1 trial, 80% of pa-tients in the stent group and 83% in nonstent group weredischarged home the day of ureteroscopy. Lithotripsydevices and unplanned medical visits or readmission in 2groups are listed in Table 2. Of the 14 studies, 7 includedpatients irrespective of the stone site in the ureter,9-15
whereas some studies selected participants with stones inthe lower ureter,8,16,18,19 and other studies selected pa-ients with stones in the middle and lower ureters.17,20,21
There was no significant difference in stone size betweenthe groups with versus without stents. Patients who useddouble-J stents because of intraoperative ureteral perfo-ration or other complications had already been excludedfrom these studies. The types of double-J stents included4.7-Fr,17 4.8-Fr gauge,19-21 6-Fr gauge,8,9,11,12,16,18,20 and-Fr gauges.10,14 Two studies did not detail the type ofouble-J stents used.13,15 One study used fexible ureter-
oscopy of 7.4-Fr gauge for management of upper ureteralstones routinely,13 and still another study used flexiblereteroscopic occasionally.9 The other studies used semi-igid or rigid ureteroscopes ranging in size from 6.0 to 11r. Three studies performed ureteral dilation before ure-eroscopy,8,16,18 One study excluded patients who under-
went ureteral dilation before ureteroscopy.9 Six studiesid not perform ureteral dilation before ureteros-opy.10,11,15,17,19,20 One study performed ureteral dilationefore ureteroscopy when necessary.18
RESULTS
Pain Scoring and Requirement for AnalgesiaSome studies used a 10-cm visual analogue scale to mea-sure pain at variable intervals after ureteroscopy: at day1,16 at days 1 and 3,11 only at day 3,10 at days 3, 7, and5,12 at days 1 and 6 and week 12,13 at days 1, 3, 7, and
15,18 and at days 2, 7, and 28.20 One study used a linearpain scale to measure pain after ureteroscopy at days 2, 7,and 28.8 There was no statistically significant difference inpain scores within the first 3 days after the procedure be-tween different groups in 3 studies.10,16,18 One study re-ported that the mean visual analog pain score in the stentgroup was statistically significantly higher than that in thenonstent group at day 3 (P � .05).12 One study reportedhat the pain score of the stent group was statisticallyignificantly higher than that of the nonstent group at 4eeks after ureteroscopy.8 Three studies reported that there
was no statistically significant difference in the pain score atweek 2 and 12 weeks after the procedure between the stentand nonstent groups.12,13,18 One study reported that therewas no statistically significant difference at weeks 1 and 4.20
Another study reported that there was no statistically sig-nificant difference in pain perception between the stent andnonstent groups, although the method of pain measurement
was not clearly indicated.14 As there was significant heter- i1250
ogeneity in postoperative pain scores between these studies,we were unable to perform meta-analysis on these data.
Seven studies reported patient requirements for analgesiaafter ureteroscopy.8,10,15,16,19-21 Three studies provided datauitable for meta-analysis.10,15,20 There was no statistically
significant difference in use of analgesics between the stentand nonstent groups (relative risk [RR] 1.10, 95% confi-dence interval [95% CI) 84-1.45) (Fig. 1A).
Lower Urinary Tract SymptomsData from 13 studies showed lower urinary tract symptomsduring follow-up.8-14,16-21 Combined analysis of 7 of the 15tudies showed that the urinary frequency or urgency rate inatients of the stent group was statistically significantlyigher than that in those of the nonstent group (RR 2.23,5% CI 1.48-3.36; Fig. 1B), and that the hematuria andysuria rates were also statistically significantly higher inhese patients (RR 2.26, 95% CI 1.20-4.24; RR 1.91, 95%I 1.18-3.08) (Fig. 1C and Fig. 1D).
rinary Tract Infection and Postoperative Feverour studies reported urinary tract infections in 430 pa-ients.11,12,16,18 There was no statistically significant differ-
ence in urinary tract infection between the stent and non-stent groups (RR 1.20, 95% CI .62-2.32; Fig. 1E). Data from1 study showed that there was a statistically significantlyhigher rate of pyuria in the initial postoperative period inpatients of the stent group, although all cases of pyuria werecured completely by day 28 after operation.10
Of the 669 patients in 6 studies, 70 (10.5%) developedpostoperative fever.7,11-13,17,18 There was no statistically sig-nificant difference in the percentage of patients with post-operative fever between the stent and nonstent groups (Fig.1F).
Unplanned Medical Visits and ReadmissionOf 1103 patients in 11 studies, 52 patients (4.7%) soughtunplanned medical visits or hospital admission.8-
13,15,16,18,19,21 Of 52 patients in 11 studies who soughtnplanned medical visits, 15 patients in the stent groupnd 37 patients in the nonstent group (Table 2). Com-ined analysis of these studies showed that the rate ofnplanned medical visits or hospital admission wasigher in nonstent patients than that in stent patientsRR 0.60, 95% CI .33-1.11; Fig. 1G), but this differenceas not statistically significant.Combined analysis of the trials that only used hol-ium laser showed no statistically significantly difference
n unplanned medical visits or readmission (RR 0.93,5% CI .39-2.21; Fig. 1H). Metaanalysis was performedn trials that only used pneumatic lithotripsy, we foundhat there was no statistically significantly difference innplanned medical visits or readmission between the 2roups (RR 0.46, 95% CI .10-2.19; Fig. 1I).
reteral Stricture and the Stone-Free Ratereteral stricture was reported in 10 of the 14 stud-
es.8,11,12,13,15-20 There was no statistically significant dif-
UROLOGY 78 (6), 2011

Table 2. Lithotripsy devices and unplanned medical visits or readmission in 2 groups
First Author andReference
No. of PatientsStented/Nonstented Energy Source Unplanned Medical Visits in Nonstented Group
No. Unplanned MedicalVisits in Stented Group
No; Requested for a Second Stenting No; Conservative Treatment
Borboroglu etal.,8 2001
53/54 Holmium laser electrohydraulic 2 (severe flank pain) 2 (Severe flank pain) 0
Byrne et al.,1
199522/28 Holmium laser causing
obstruction requiredcystoscopic removal)
1 (Renal colic) 1 (Pyelonephritis) 1 (Distally migratedstent)
Chen et al.,10
200230/30 Electrohydraulic 0 1 (Severe flank pain) 0
Cheung etal.,11 2003
29/29 Holmium laser 5 (Treatment not clear) 6 (Severe flank pain, treatmentnot clear)
Damiano etal.,12 2004
52/52 Swiss lithoclast 6 (severe flank pain) 6 (severe flankpain) 0
Denstedt etal.,13 2001
29/29 Holmium laser electrohydraulicfor one patient
0 1 (Vomiting) 1 (Genitourinary sepsis,received intravenousantibiotics)
Jeong et al.,14
200423/22 Electromechanical lithotripter
Netto et al.,15
2001133/162 Ultrasonic 0 0
Srivastava etal.,16 2003
26/22 Swiss lithoclast 0 1
Shao et al.,17
200858/57 Holmium laser
Ibrahim etal.,18 2008
110/110 Holmium laser and Swisslithoclast
0 5 (Severe flank pain) 2 (Severe flank pain,treated conservatively)
Kenan et al.,19
20081/22 Pneumatic lithotripter (Karl
Storz, Calcusplit 27630020, Germany)
0 1 (Severe flank pain with fever) 1 (Proximal stentmigration requiredcystoscopic removal)
Xu et al.,20
200955/55 Pneumatic lithotripsy
Cevik et al.,21
201130/30 Pneumatic lithotripsy (Vibrolith,
Elmed Lithotripsy Systems,Ankara, Turkey)
0 6 (Severe flank pain) 3 (Severe flank pain,received injectableanalgesics)
UR
OLO
GY
78(6),2011
12
51

Figure 1. Continued
1252 UROLOGY 78 (6), 2011

t
wt
ioggi
rwwvrw
ference in the occurrence of ureteral stricture betweenthe stent and nonstent groups. The stone-free status wasnot statistically significantly different between the 2groups.
Return to Normal Physical ActivitiesTwo studies reported that there was no significant differ-ence in return to normal physical activities between thestent and nonstent groups.10,18
Health-Related Quality ofLife and Health EconomicsThe results of 1 study17 showed the Ureteric Stent Symp-
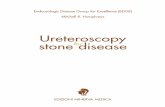
Figure 1. Forest plots. (A) Patient requirements for analgesate in patients with and without stents. (C) Hematuria in paithout stents. (E) Urinary tract infection in patients with aithout stents. (G) Unplanned medical visits and readmissisits or readmission in patients accepting holmium laseadmission in patients accepting pneumatic lithotripsy wiithout stents.
om Questionnaire (USSQ) domain score in the second
UROLOGY 78 (6), 2011
eek. The stent group was statistically significantly worsehan the nonstent group (P � .0001).17 The other studies
did not mention the quality of life of the patients.Five studies reported the cost per patient in the stent and
nonstent groups,9,15,16,17,21 showing that ureteral stentingncreased the expenses in all the 5 trials. Combined analysisf 10 studies showed that the operation duration in the stentroup was significantly longer than that in the nonstentroup (weighted mean difference 4.25, 95% confidencenterval 1.10-7.40, Fig. 1J).9,11-13,16-21
Impact of Ureteral Stent DiameterMeta-analysis was performed on trials applying stents �6
patients between groups. (B) Urinary frequency or urgencyts with and without stents. (D) Dysuria in patients with andithout stents. (F) Postoperative fever in patients with and
n patients with and without stents. (H) Unplanned medicalith and without stents. (I) Unplanned medical visits ornd without stents. (J) Operation time in patients with and
ia intiennd wion ier wth a
Fr. We founded that the incidence of dysuria, frequency
1253

F
psuittt
rCov
br
egcAtrdo
es
atshItopcmtfabpmw
uapdsssgnu
twct
and hematuria was statistically significantly higher in thestent (using stent �6 Fr) group. The meta-analysis alsoshowed that there was no statistically significant differ-ence in the urinary tract infections, postoperative fever,unplanned medical visits, or readmission between groupsin trials applying stents �6 Fr. Studies applying stents �5r were insufficient to be analyzed.
COMMENT
Principal FindingsThe issue of ureteral stenting after uncomplicated uret-eroscopy is still debated. The rationale for the routine useof ureteral stents after ureteroscopy originates from as-sumptions, rather than from evidence-based medicine.This widely held belief is based on the presumption thatstent placement serves to eliminate clinically significantobstruction and prevent ureteral stricture formation.3,22
The reported published data have clearly demonstratedthat ureteral stents have been routinely placed after treat-ment for urinary stone disease in most ureteroscopy se-ries.3,6,23 Nevertheless, some trials suggest that stentlacement may cause significant symptoms and that theymptoms persist until the stent is removed. However,reteral stenting may cause significant morbidity, such asrritative voiding symptoms, pain, and hematuria. Fur-hermore, it may be associated with various complica-ions, such as migration or breakage of the stent, infec-ion, pyelonephritis, encrustation, and stone formation.
In this systematic review, we considered data from 14andomized controlled trials of moderate to poor quality.linical heterogeneity included the use of different sizesf ureteroscopes, different intracorporeal lithotripsy de-ices, and variations in practice and experience.None of the included studies reported relationships
etween ureteral stent design and patient comfort. In 1andomized study,24 236 patients were randomized in a
1:1:1:1 ratio to the short loop tail stent, the long loop tailstent,59, the Percuflex Plus stent64 and the Polaris stent.53
Patients who underwent stenting with the short loop tailhad lower questionnaire pain scores on day 4 after place-ment and lower pain medication use on day 1 afterplacement, although it was not statistically significant.
LimitationsThe research quality of most of these trials included waspoor, probably because of their low level of methodolog-ical quality.25,26 The assessment of quality became im-possible without adequate reporting,27 and the drive tonsure adherence to standardized conduct and reportinguidelines for randomized controlled trials has much toommend it from the systematic reviewer’s point of view.llocation concealment was unclear in 9 trials, and 1
rial used an inadequate approach for concealment ofandomization. This increases the risk of selection bias byisrupting the assignment sequence and may result in loss
f the advantages of randomization, generating biased1254
stimates of results.27,28 Some trials had small sampleizes.
There was a lack of criteria for the length of the studynd the duration of stenting. There were also inconsis-encies in the use of preoperative antibiotics, study de-ign, stent material, patient population, evaluation ofealth-related quality of life, and cost-effectiveness data.n all, 50% of the studies included stones at any site inhe ureter. Success of ureterolithotripsy partly dependedn the proximal or distal location. Ureterolithotripsy inroximal ureteral stones may be associated with signifi-antly higher intraoperative complication and retreat-ent rates compared with distal stones. Ureterolitho-
ripsy in distal ureteral stones may result in higher stone-ree rate than with proximal ureteral stones. Some trialsllowed patients to draw from study after randomizationecause of intraoperative complications,8,12 leading tootential reporting bias. The longest follow-up was 49onths, but most of the included trials’ follow-up timesere too short.18
Definition of Uncomplicated UreteroscopyMost of these trials lacked a standard definition of un-complicated ureteroscopy, Only Ibrahim et al18 definedncomplicated ureteroscopy as ureteroscopy in personsged 18 years or more with stones located in the distalart of the ureter below the iliac vessels, a largest stoneiameter of less than 1.5 cm, and no multiple complextones or distal ureteral pathology. In addition, therehould have been no intraoperative major complications,uch as ureteral perforation, or incomplete stone disinte-ration or removal. Other trials lacked a standard defi-ition but showed exclusion criteria for uncomplicatedreteroscopy (Table 3).10-13,16-21 Ureteroscopy without
the above exclusion criteria can be defined as uncompli-cated ureteroscopy.
Postoperative Unplanned MedicalVisits or Readmission to the HospitalThe cost savings, operation time savings, and improvedpatient comfort seen in patients without stent must bebalanced against the risk of postoperative readmission ormedical visit to the hospital. In this meta-analysis, wefounded that there was a decreased tendency towardunplanned medical visits or hospital admission in thestent group, but this difference was not statistically sig-nificant. Of the 11 studies that reported unplanned med-ical visits or hospital admission, 1 study reported that therate of unplanned admission was statistically significantlyhigher in nonstent patients.12 The reason may be thathey used the Swiss Lithoclast ballistic lithotriptor,hich is more likely to leave larger residual fragmentsompared with holmium:YAG laser. However, Srivas-ava et al16 also used pneumatic lithotripsy (Swiss Litho-
clast), and showed that there was no statistically signif-icant difference in the rate of unplanned admission
between the stent and nonstent groups. The other 9 trialsUROLOGY 78 (6), 2011

all showed that there was no statistically significant dif-ference in the rate of unplanned admission between the2 groups.
In our experience, the completeness of stone fragmen-tation may be a more critical factor for whether ureteralstent placement is necessary. Ureteroscopic Holmium:YAG laser lithotripsy is believed to be the “gold standard”in ureteroscopy for management of ureteral stone. The hol-mium laser produced smaller (�2-mm) stone fragmentsthan the other common intracorporeal lithotriptors. Weperformed meta-analysis on trials that only used holmiumlaser, the results showed the unplanned readmission rate wasnearly the same between groups, and the difference was notstatistically significant. Pneumatic lithotripsy produceslarger fragments (at least 3-4 mm) that may potentiallycause more problems in terms of spontaneous passage. Meta-analysis was performed on trials that used only pneumaticlithotripsy, and a decreased tendency of unplanned medicalvisits or hospital admission in the stent group was founded;however the difference between groups was also not statis-tically significant.
In another study,29 276 uncomplicated ureteroscopieswere performed for ureteral calculi. Double-J stent insertionwas needed on an emergent basis in 23 patients with intol-
Table 3. Exclusion criteria for uncomplicated ureteroscopy
Chen10 Cheung11 Damiano12 D
Ureteral obstruction(stricture)
● ● ●
Ureteral perforation ● ●Radiolucent stone ● ●Solitary functioning
kidney● ●
Concomitantipsilateral renalstone load thatrequired furtherintervention afterureteroscopy
●
Ureteralsteinstrasse
●
Preoperativeureteral stenting
●
Stone size �2 cm ●History of sepsis ●Previous
ureteroscopy forthe same stoneand failed
●
Renal failure ●Pregnancy ●History of urinary
tract infectionStone size �1.5 cmBilateral ureteral
stonesSuspicion of
urothelial cancer●
Multiple ureteralstones
Filled circle (●) denotes that the trial included this criterion.
erable colic pain and extreme discomfort. All 276 patients
UROLOGY 78 (6), 2011
had accepted an uncomplicated procedure with no compli-cation. The trial showed that a longer operative time, re-peated access, management of a large stone, impacted cal-culi with ureteral wall edema, a mildly narrowed ureteralsegment, ignored caliceal small calculi, and a recent historyof urinary tract infection contributed to the need for post-operative stent placement. The study recommended thatplacement of a ureteral catheter, at least transiently (over-night stenting), might prevent ureteral obstruction causingpatient extreme postoperative discomfort with evident colicpain in selected patients.
Future EffortsConclusions drawn from our meta-analysis should beinterpreted cautiously. Although there is some evidenceof benefits in the nonstent group after uncomplicatedureteroscopy, more high-quality confirmatory trials arewarranted before final clinical recommendations can bemade.
CONCLUSIONSMeta-analysis of the present literature detected muchbenefit in the nonstent group. However, considering dif-
first author of study and reference
tedt13 Srivastava16 Shao17 Kenan20 Xu21 Cevik23
● ●
● ● ●●
● ● ● ● ●
●
●
● ● ●
● ●● ● ● ●
● ●
● ● ● ●● ● ●
●● ●
●
● ●
, by
ens
●
●
●●●
●●●
ferent outcome measures, marked clinical heterogeneity,
1255

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
withdrawal after randomization, imprecision in measure-ment of outcomes (large confidence intervals), and poorreporting of the included trials, the place of stenting inthe management of patients after uncomplicated ureter-oscopy remains unclear.
References1. Francesca F, Scattoni V, Nava L, et al. Failures and complications
of transurethral ureteroscopy in 297 cases: conventional rigid in-struments vs. small caliber semirigid ureteroscopes. Eur Urol. 1995;28:112-115.
2. Yaycioglu O, Guvel S, Kilinc F, et al. Results with 7.5F versus 10Frigid ureteroscopes in treatment of ureteral calculi. Urology. 2004;64:643-646; discussion 646-647.
3. Gettman MT, Segura JW. Management of ureteric stones: issuesand controversies. BJU Int. 2005;95(Suppl 2):85-93.
4. Harmon WJ, Sershon PD, Blute ML, et al. Ureteroscopy: current practiceand long-term complications. J Urol. 1997;157:28-32.
5. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuringinconsistency in meta-analyses. BMJ. 2003;327:557-560.
6. Hosking DH, McColm SE, Smith WE. Is stenting following uret-eroscopy for removal of distal ureteral calculi necessary? J Urol.1999;161:48-50.
7. Sun Y, Xu C, Wen X, et al. Is endoscopic management suitable forlong ureteral fibroepithelial polyps? J Endourol. 2008;22:1459-1462.
8. Borboroglu PG, Amling CL, Schenkman NS, et al. Ureteral stent-ing after ureteroscopy for distal ureteral calculi: a multi-institu-tional prospective randomized controlled study assessing pain, out-comes and complications. J Urol. 2001;166:1651-1657.
9. Byrne RR, Auge BK, Kourambas J, et al. Routine ureteral stentingis not necessary after ureteroscopy and ureteropyeloscopy: a ran-domized trial. J Endourol. 2002;16:9-13.
0. Chen YT, Chen J, Wong WY, et al. Is ureteral stenting necessaryafter uncomplicated ureteroscopic lithotripsy? A prospective, ran-domized controlled trial. J Urol. 2002;167:1977-1980.
1. Cheung MC, Lee F, Leung YL, et al. A prospective randomizedcontrolled trial on ureteral stenting after ureteroscopic holmiumlaser lithotripsy. J Urol. 2003;169:1257-1260.
2. Damiano R, Autorino R, Esposito C, et al. Stent positioning afterureteroscopy for urinary calculi: the question is still open. Eur Urol.2004;46:381-387; discussion:387-388.
3. Denstedt JD, Wollin TA, Sofer M, et al. A prospective randomizedcontrolled trial comparing nonstented versus stented ureteroscopiclithotripsy. J Urol. 2001;165:1419-1422.
4. Jeong H, Kwak C, Lee SE. Ureteric stenting after ureteroscopy
for ureteric stones: a prospective randomized study assessing1256
symptoms and complications. BJU Int. 2004;93:1032-1034;discussion 1034-1035.
5. Netto NR Jr., Ikonomidis J, Zillo C. Routine ureteral stenting afterureteroscopy for ureteral lithiasis: is it really necessary? J Urol.2001;166:1252-1254.
6. Srivastava A, Gupta R, Kumar A, et al. Routine stenting afterureteroscopy for distal ureteral calculi is unnecessary: results of arandomized controlled trial. J Endourol. 2003;17:871-874.
7. Shao Y, Zhuo J, Sun XW, et al. Nonstented versus routine stentedureteroscopic holmium laser lithotripsy: a prospective randomizedtrial. Urol Res. 2008;36:259-263.
8. Ibrahim HM, Al-Kandari AM, Shaaban HS, Elshebini YH, ShokeirAA. Role of ureteral stenting after uncomplicated ureteroscopy fordistal ureteral stones: a randomized, controlled trial. J Urol. 2008;180:961-965.
9. Isen K, Bogatekin S, Em S, et al. Is routine ureteral stentingnecessary after uncomplicated ureteroscopic lithotripsy for lowerureteral stones larger than 1 cm? Urol Res. 2008;36:115-119.
0. Xu Y, Wei Q, Liu LR. A prospective randomized trial comparingnon-stented versus routine stented ureteroscopic holmium laserlithotripsy. Saudi Med J. 2009;30:1276-1280.
1. Cevik I, Dillioglugil O, Akdas A, et al. Is stent placement necessaryafter uncomplicated ureteroscopy for removal of impacted ureteralstones? J Endourol. 2011;24:1263-1267.
2. Richter S, Ringel A, Shalev M, et al. The indwelling ureteric stent:a “friendly” procedure with unfriendly high morbidity. BJU Int.2000;85:408-411.
3. Blute ML, Segura JW, Patterson DE. Ureteroscopy. J Urol. 1988;139:510-512.
4. Lingeman JE, Preminger GM, Goldfischer ER, et al. Assessing theimpact of ureteral stent design on patient comfort. J Urol. 2009;181:2581-2587.
5. Newcombe RG. Towards a reduction in publication bias. Br Med JClin Res Ed. 1987;295:656-659.
6. Juni P, Altman DG, Egger M. Systematic reviews in health care:assessing the quality of controlled clinical trials. BMJ. 2001;323:42-46.
7. Schulz KF, Chalmers I, Hayes RJ, et al. Empirical evidence ofbias. Dimensions of methodological quality associated with es-timates of treatment effects in controlled trials. JAMA. 1995;273:408-412.
8. Schulz KF. Assessing allocation concealment and blinding in ran-domised controlled trials: why bother? Evid Based Nurs. 2001;4:4-6.
9. Tanriverdi O, Yencilek F, Koyuncu H, et al. Emergent stentingafter uncomplicated ureteroscopy: evaluation of 23 patients. Urol-
ogy. 2011;77:305-308.UROLOGY 78 (6), 2011