![Provincial Constituency Reference Map - District Peshawar · T uc l fa j n between ALHASAN [] ... PK - 9 PK - 5 PK - 11 PK - 4 PK - 3 PK - 2 PK - 1 Legend Districts Boundary Provincial](https://static.fdocuments.us/doc/165x107/5c01b81309d3f22b088d1121/provincial-constituency-reference-map-district-t-uc-l-fa-j-n-between-alhasan.jpg)
PK and PD Studies for Systemic Exposure of Locally Acting Drugs Industry View Lester I. Harrison,...
34
PK and PD Studies for Systemic Exposure of Locally Acting Drugs Industry View Lester I. Harrison, PhD Division Scientist 3m Pharmaceuticals
-
Upload
rudolf-charles -
Category
Documents
-
view
213 -
download
0
Transcript of PK and PD Studies for Systemic Exposure of Locally Acting Drugs Industry View Lester I. Harrison,...
PK and PD Studies for Systemic Exposure of Locally Acting Drugs
Industry View
Lester I. Harrison, PhD
Division Scientist
3m Pharmaceuticals
Value of OINDP PK
• Systemic Absorption = Systemic Exposure
• Measure of systemic safety for locally acting drugs
• PK is an Established BE Metric– Standardized– Validated– Discriminating
OINDP PK Concerns
• Low Doses
• Assay LLOQ Limitations
• Variability
• Nose: Drainage of Excess Dose
• Oral Inhalation: Dosing Technique

OINDP PK Concern: Low Doses
• “Low” Dose Relative– Quantitatable
• Therapeutic Dose Range– More dose options
• Nasal Route– May be limited by drainage

OINDP PK Concern: Assay LLOQ
• LLOQ under 100 pg/mL common with LC/MS/MS
• Commercial Availability of Assays– Albuterol– BDP + Active Metabolite– Budesonide– Triamcinolone Acetonide– Cromolyn– Fluticasone Propionate?

OINDP PK Concern: Variability
• Large Inter-Subject Variability
• Large Intra-Subject Variability
• Dosing Technique

Nasal Formoterol VariabilityN = 27
Hochhaus et al, Pharmaceut Res 1992;9:291-297

Nasal Triamcinolone Acetonide Variability N = 12
Argenti et al, J Clin Pharmacol 1994;34:854-858
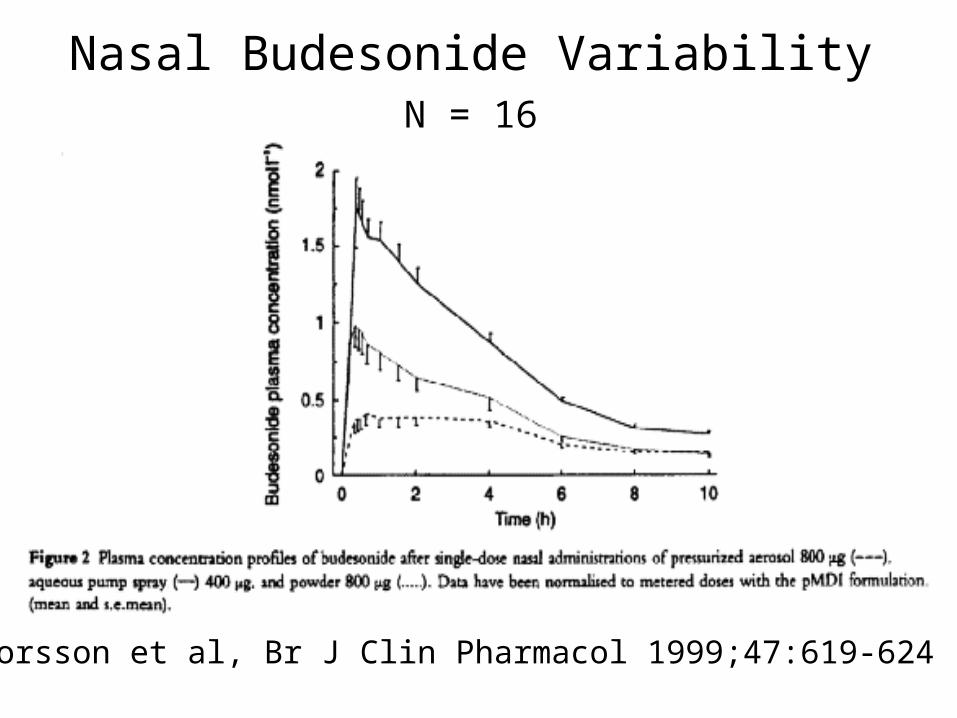
Nasal Budesonide Variability N = 16
Thorsson et al, Br J Clin Pharmacol 1999;47:619-624

Oral Inhalation Fluticasone Variability N = 12
Thorsson et al, Br J Clin Pharmacol 1997;43:155-161

Reducing Variability
• Replicate Study Designs
• Increased N
• Nasal - Reduce Dose
• Oral Inhalation - Inhalation Training– Not real world

BE Limitations of OINDP PK
• No Correlation with Efficacy– Corticosteroids
• Represents a Fraction of Dose– Usually Less Than 30%– Fine Particle Fraction?
• Summary Parameter of Absorption– Represents Mouth + GI + First Pass + Lungs– Different Rates and Extents of Absorption

Nasal Fluticasone PK & EfficacyN = 280
DoseDay 15
SymptomScore
C1
pg/mL
Nasal200 mcg/dy
133 BKGD
Oral5 mg/dy
212 103
Oral10 mg/dy
194 137
Placebo 217 BKGD
Howland et al, Clin Therap 1996;18:1106-1117

Oral Inhaled Fluticasone PK & EfficacyN = 261
DoseWeek 6
AM FEV1
Change, LSymptomScore
Cmaxpg/mL
AUCpg/h/mL
Inhaled200 mcg/dy
0.27 -0.17 BLQ BLQ
Inhaled1000 mcg/dy
0.42 -0.22 116 629
Oral20 mg/dy
-0.2 0.04 248 1230
Placebo -0.19 0.06 BLQ BLQ
Lawrence et al, Am J Respir Crit Care Med 1997;156:744-751
Value of OINDP PK: Conclusions
• PK Useful to Establish Systemic Absorption
• Not a Surrogate for Local Efficacy
• Doable
• Can Reduce Variability
• Systemic BE?

BDP MDI Examples Systemic Absorption Studies
• Formulations: MDI A vs. MDI B
• Study Designs– Single Dose (multiple inhalations)– Asthmatics– Crossover– Good Inhalation Technique

BDP Comparative Absorption StudiesMDI A vs. MDI B
• Q1 …….. ……………… same
• Q2 ………………………… same
• Particle Size Dist ……… essentially same
• Spray Pattern …………… essentially same
• Valve Size …..………… same
• Actuator Dimensions…… essentially same

Oral Inhaled BDP PK Study 1
• Objective: Systemic Comparability
• N = 18 Asthmatics
• Cmax: CI = 0.79 - 1.12; CV = 51%
• AUC: CI = 0.90 - 1.35; CV = 42%

Oral Inhaled BDP PK Study 2
• Objective: Systemic BE
• N = 45 Asthmatics
• CmaxL: CI = 0.85 - 1.01; CV = 30%
• CmaxH: CI = 0.80 - 0.95; CV = 49%
• AUCL; CI = 0.85 - 0.95; CV = 23%
• AUCH; CI = 0.86 - 0.97; CV = 22%
Concluded Systemic Equivalence Ran Local Delivery Study for Efficacy

BDP MDI Examples Systemic Absorption Studies
• Formulations: MDI C vs. MDI D– Different Strengths– Same Dose, Different Number of Puffs
• Study Designs– Single Dose (multiple inhalations)– Asthmatics– Crossover– Good Inhalation Technique

BDP Comparative Absorption StudiesMDI C vs. MDI D
• Q1 …….. ……………… same
• Q2 ………………………… same
• Particle Size Dist ……… same
• Spray Pattern …………… same
• Valve Size …..………… different
• Actuator Dimensions……same
Oral Inhaled BDP PK Study 3
• Objective: Systemic Comparability
• N = 18 Asthmatics
• Cmax: CI = 0.76 - 1.00; CV = 32%
• AUC; CI = 0.86 - 1.19; CV = 37%

Oral Inhaled BDP PK Study 4
• Objective: Systemic BE• N = 30 Asthmatics
• CmaxL: CI = 0.82 - 1.11; CV = 46%
• CmaxH: CI = 0.81 - 1.11; CV = 34%
• AUCH; CI = 0.81 - 1.22; CV = 37%
Concluded Systemic Equivalence Ran Local Delivery Studies on Each MDI

PK Options: Charcoal Block
• Allows Differentiation of Pulmonary and Non-Pulmonary Absorbed Drug
• Utilizes Same Drug Assays and Metrics – Little additional time or cost
• Do Not Have to Alter Reference or Test Products
BE Limitations of Charcoal Block
• No Evidence that Pulmonary Absorbed Drug Correlates with Efficacy
• Does Not Discriminate Potentially Important Product Differences– Oropharayngeal Deposition– Regional Lung Deposition
Very Useful Laboratory Tool– “Pulmonary” Drug Absorption– Potential Surrogate for Local Delivery?
PK Options: Urinary Excretion
• When PK Not Doable
• Reported for– Albuterol– Cromolyn– Nedocromil– Ipratropium

Nasal Ipratropium BromideN = 22
• 24-Hour Urinary Excretion
10.6 1.9 g (mean SE)
CV = 84%
• Percent Dose Excreted
6.3 1.2%
CV = 89%
Wood et al, J Allergy Clin Immunol 1995;95:1111-1116

BE Limitations of Urinary Excretion
• High Variability
• Low Sensitivity
Unlikely to be a Reliable Surrogate

PK Options: PD Measurement
• When PK Not Doable
• Requires Appropriate Study Design– Dose Response Curve– Repeat Administration
BE Limitations of PD
• High Variability
• Low Sensitivity
• Requires Multiple Dose Levels
Difficult Task if PK Not Doable

PK Options: PK-PD
• Allows Correlation of PK with PD– PK Linear– PD Dose Response Curve
• Increased Understanding – Systemic Exposure– Systemic Safety

BE Limitations of PK-PD
• Requires Several Dose Levels, Additional Analyses
• Does Not Increase Ability to Differentiate Products
• Very Useful Laboratory Tool
Development Technique

SUMMARY
• Systemic PK Assessment – Needed to Assure Systemic Safety– Doable for Most Drugs
• PD, Urine Levels – Not Likely Surrogates
• Charcoal Block, PK-PD– Development Tools

FDA Question: Are There Situations Where In Vitro Data + PK + PD Can Be Relied on to Assure Local Efficacy
• Can Be Relied On To Assure Implies Predictability– Beta-Agonists– Corticosteroids– Cromolyn– Anticholinergics– Antihistamines
• Solutions? Need for Caution Until Predictability
Demonstrated