Pilot of a DNACPR Form at University Hospital Limerick (Presentation from Acute Hospital Network...
21
Pilot of a DNACPR form at University Hospital Limerick Denis Casey End-of-Life Care Coordinator [email protected] 087 654 4070
-
Upload
irish-hospice-foundation -
Category
Healthcare
-
view
3 -
download
0
Transcript of Pilot of a DNACPR Form at University Hospital Limerick (Presentation from Acute Hospital Network...

Pilot of a DNACPR form at
University Hospital Limerick
Denis Casey
End-of-Life Care Coordinator
[email protected] 087 654 4070

Background
• Part 4 of the National Consent Policy
introduced by the HSE(2013) provides a
decision making framework to facilitate
timely discussions with patients regarding
Cardio-Pulmonary Resuscitation (CPR)
• To ensure decisions are made consistently
transparently and in line with the patients
preferences and best practice
• Recognised need to develop a policy for
ULHG

Policy steering group
• Palliative Medicine Cons (Chair)
• Paediatric Consultant
• Medical Consultants x 3
• ED Consultant
• PALS Manager x 2
• EOLC Coordinator
• Resus CNS x 2
• CNM3 Cancer Services
• Clinical Risk Advisor
• Anaesthetic Consultant
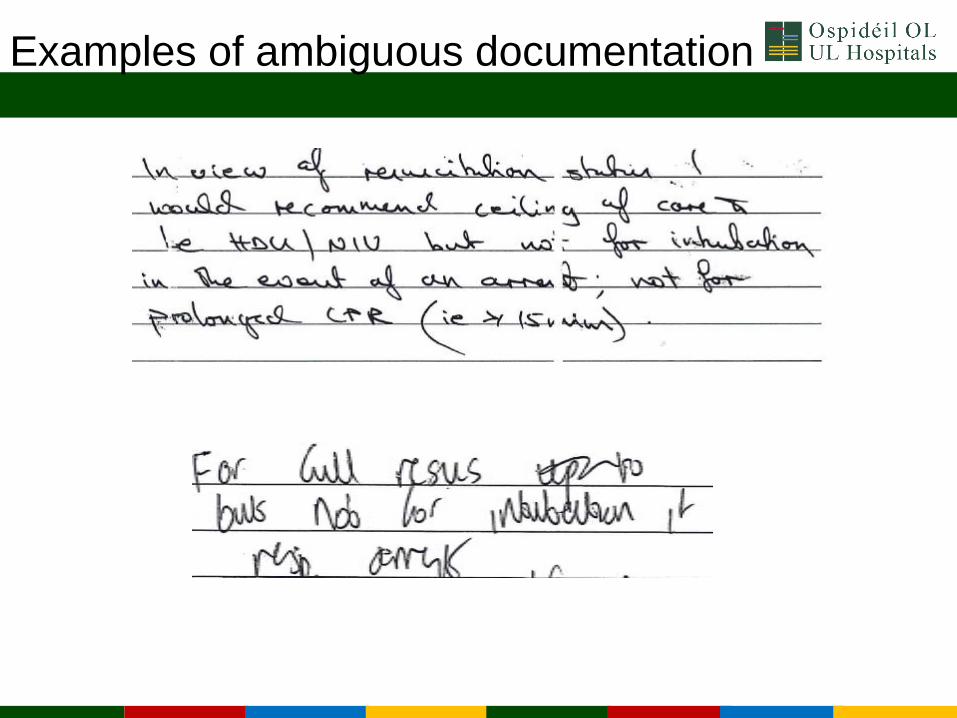
Examples of ambiguous documentation

Principles
• DNACPR decisions only related to CPR
• Presumption in favour of CPR if no decision
• Individual assessment of all cases
• Overall responsibility for decision lies with
consultant in charge
• Communication
• ? Valid advance healthcare directive
• ? Power of attorney
• DNACPR order/decision does not override
clinical judgement of a reversible cause

Policy
• Draft Policy developed
• Draft Adult DNACPR Form developed
• Draft Paediatric Advance healthcare Plan
• Decision Making framework
• Patient and Family information booklet

Decision making framework

DNACPR form

Pilot of Form
• Aim of pilot was to test the DNACPR form for
ease of completion and its adoptability among
staff
• It also sought to identify any potential
deficiencies in the policy before being finalised

Methods
• 12 medical consultants volunteered for pilot
Included: Oncology, GI, Renal,
Care of the Elderly, AMAU
• Pilot on 7 Medical wards, ICU & HDU

Results
• Data collection continued for 20 weeks
•289 patients in medical wards, ICU & HDU
documented “Not for resuscitation”
•100 completed forms

Findings
• Capacity
36% had capacity to discuss their status
No patient reported having AHD
No patient reported having EPA
1 ward of court

• Age
Range 53-97, Mean 79
• Discussion
Status was discussed with 31 patients only
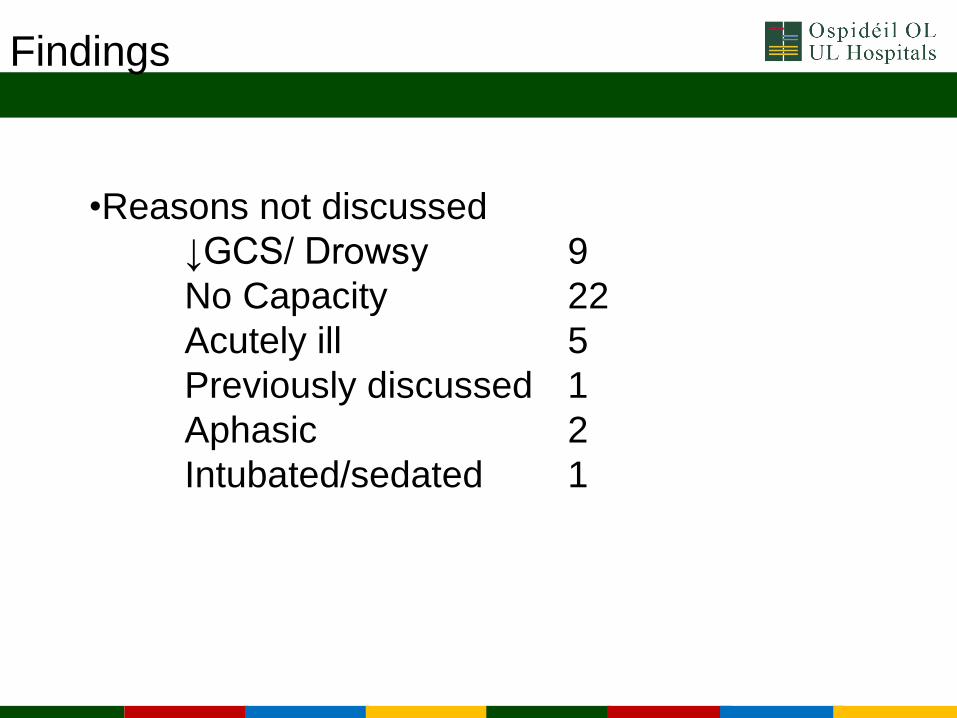
Findings
•Reasons not discussed
↓GCS/ Drowsy 9
No Capacity 22
Acutely ill 5
Previously discussed 1
Aphasic 2
Intubated/sedated 1

Findings – Clinical Problems
Subarachnoid Haemorrhage 4
Fraility 27
Dementia 22
ES COPD 9
Cardiac Arrest 1
Hypoxic Brain Injury 1
Multi-organ failure 2
Age 2
Nursing Home resident 3
Parkinsons Disease 8
Congestive cardiac Failure 12
Previous Coronary Bypass graft 1
Stroke 13
ES Renal Disease 11
Cancer 15
Neuro 2
Acute illnesss 6
ES Liver disease 4
Ms/ MND 2
Not complete 7

Findings
• Reasons not for CPR
72% had an advanced progressive illness
59% unlikely to restart heart & Breathing
• Ceiling of Care
Admission to ICU/ HDU
Yes 7%
No 75%

Findings
• Antibiotics
85% were for antibiotic therapy
• IV Fluids
87% were for IV fluids

Findings
• Other
Not for BiPaP 1
Not for intubation 2
For BiPaP 4
Pain/symptom control 5
Dialysis 1
BiPaP if patient wishes 1
Tx for hyperkalaemia 1
Blood products 1
Usual Medications 1

Findings
• Date
35% not dated – invalid
• Signed by Doctor/ Consultant
12% were not signed – invalid
• Signed by nurse
75% were not signed – for communication

Recommendations
• Update draft policy in light of new ADM act 2015
• Date relocated on form to increase compliance
• Increased options ceiling of care
• Policy to be finalised and approved
• To be implemented hospital group wide

Thank you