Pilot Case Study in Mauritius for the Treatment of Lymphedema using Complete Decongestive Therapy
17
A Pilot Case Study in Mauritius for the Treatment of Lymphedema using Complete Decongestive Therapy Date of Study: 2 February 2015 – 7 February 2015 Place: Westcare Health Centre, La Mivoie, Black River Therapist: N.A Pearce (CLT) (Norton School of Lymphatic Therapy) With special thanks to: Elizabeth Dalais and all the Staff at Link to Life Thea Van Schoor Dr Bernard Piat
-
Upload
nicole-pearce -
Category
Documents
-
view
232 -
download
2
Transcript of Pilot Case Study in Mauritius for the Treatment of Lymphedema using Complete Decongestive Therapy

A Pilot Case Study in Mauritius for the Treatment of Lymphedema using Complete Decongestive Therapy
Date of Study: 2 February 2015 – 7 February 2015
Place: Westcare Health Centre, La Mivoie, Black River
Therapist: N.A Pearce (CLT) (Norton School of Lymphatic Therapy)
With special thanks to:
Elizabeth Dalais and all the Staff at Link to Life
Thea Van Schoor
Dr Bernard Piat
Lymphedema
Lymphedema is a chronic swelling of a body part usually occurring in the extremities (arms or legs). It can also occur in the face, neck,
abdomen, or genitals. Lymphedema is the result of the abnormal accumulation of protein-rich edema fluid in the affected area. The problems
it creates are poorly understood in the medical community. Lymphedema is classified as either primary or secondary. Primary lymphedema
is the result of lymphatic dysphasia. It may be present at birth but more often develops later in life without obvious cause.
Secondary lymphedema is much more common and is the result of surgery or is a side effect of radiation therapy for cancer. Secondary forms
may also occur after injury, scarring, trauma, or infection of the lymphatic system. Lymphedema has important pathological and clinical
consequences. Lymphedema can present immediately after the event that causes damage to the lymphatic system or many years after the
event. It is important to remember that even if a patient only becomes symptomatic years after (the cancer surgery for instance), the
lymphedema is still directly related to the cancer and its treatment.
In stage 1 lymphedema, the swelling consists of protein-rich fluid and may be temporarily reduced by simple elevation of the limb. If it remains
untreated, however, the lymphedema causes a progressive hardening of the affected tissues which is the result of a proliferation of connective
tissue, adipose tissue, and scarring (stage 2 lymphedema). Stage 3 lymphedema is characterized by a tremendous increase in volume,
hardening of the dermal tissues, hyperkeratosis, and papilloma’s of the skin.
Infections such a cellulitis, erysipelas, and lymphangitis frequently develop in individuals suffering from lymphedema. Infections are most
common in stage II and III lymphedema with each infection contributing to a worsening of the condition making frequent hospitalizations
necessary.
Lymphedema treatment in Mauritius has, to date, been restricted to the prescription of diuretic medications. This does however aggravate
the condition and is contra-indicated in the treatment of lymphedema. Hence no effective treatment has been available to patients with
lymphedema in Mauritius.
Complete Decongestive Therapy is the ‘gold standard’ for the treatment of lymphedema in the United States and Europe. The treatment is
now available in Mauritius.
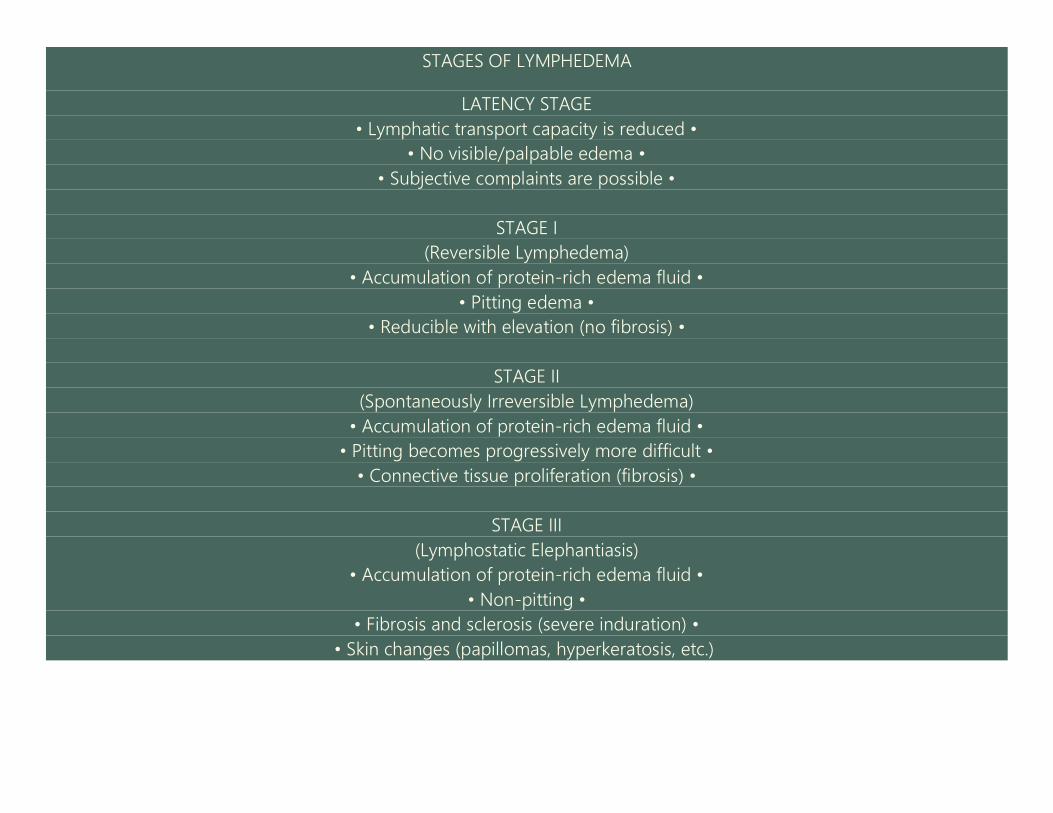
STAGES OF LYMPHEDEMA
LATENCY STAGE
• Lymphatic transport capacity is reduced •
• No visible/palpable edema •
• Subjective complaints are possible •
STAGE I
(Reversible Lymphedema)
• Accumulation of protein-rich edema fluid •
• Pitting edema •
• Reducible with elevation (no fibrosis) •
STAGE II
(Spontaneously Irreversible Lymphedema)
• Accumulation of protein-rich edema fluid •
• Pitting becomes progressively more difficult •
• Connective tissue proliferation (fibrosis) •
STAGE III
(Lymphostatic Elephantiasis)
• Accumulation of protein-rich edema fluid •
• Non-pitting •
• Fibrosis and sclerosis (severe induration) •
• Skin changes (papillomas, hyperkeratosis, etc.)

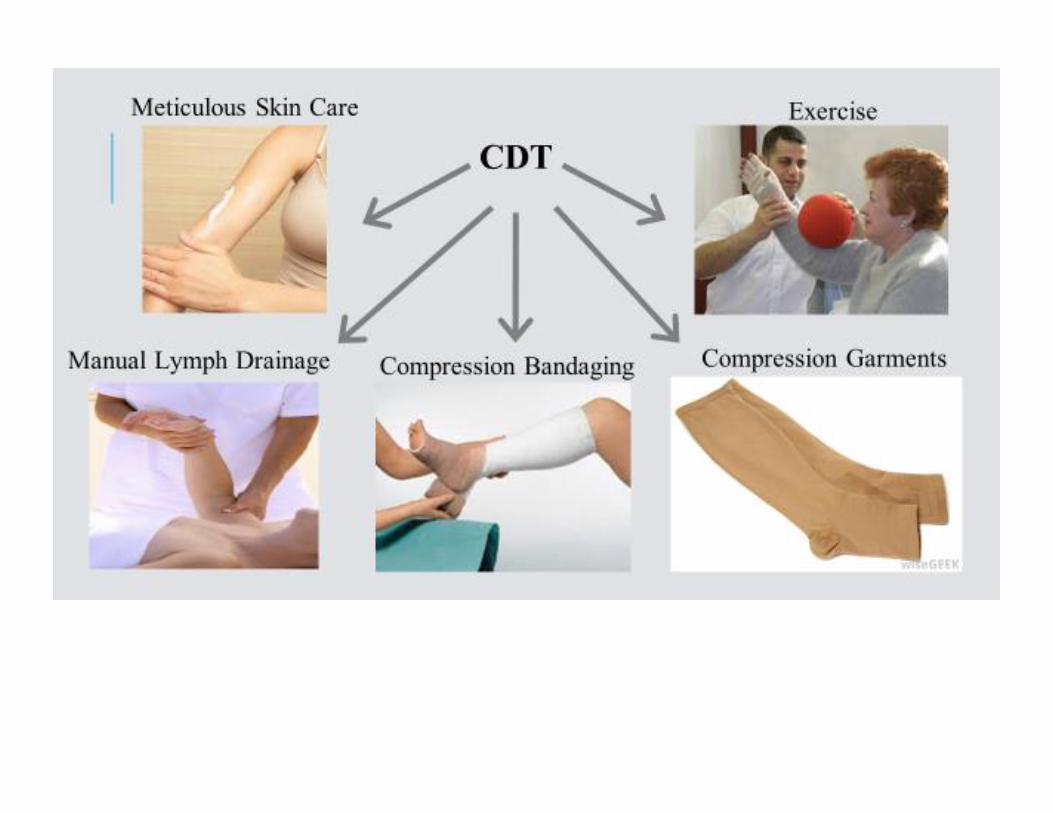
An outline of the treatment Complete Decongestive Therapy (CDT)
CDT is a combination of Manual Lymph Drainage (MLD), bandaging of the affected areas, remedial exercises, and skin and nail care. CDT is
divided into a two-phase program that initially involves an intensive treatment phase and is then followed by a maintenance program
continued by the patient at home. Carried out with great care and consistency by a certified lymphedema therapist, CDT is the treatment of
choice for chronic extremity lymphedema. Even in advanced lymphedema, CDT achieves excellent results with no side effects. Because CDT
is labor intensive, time-consuming, and requires patient compliance, many patients have difficulty committing to the program at first. However,
because the results of CDT are always superior to those achieved with all other treatments, increasing numbers of patients are undergoing
CDT treatment and are consequently able to maintain the reduction of their limbs through diligent participation in a home maintenance
program.
For a lymphedema therapist to be fully competent in treating lymphedema using CDT, it is vital that the CDT training consist of the four
components of CDT: (1) basic and advanced MLD, (2) lymphedema bandaging, (3) remedial exercises, (4) skin and nail care.
The therapist must also have a complete understanding of the anatomy, physiology, and pathophysiology of the lymphatic system, the
treatment of primary and secondary lymphedema, the indications and contraindications of CDT, and the proper measuring techniques for
lymphedema support garments.
Furthermore, lymphedema therapy should not begin unless the patient has been examined and diagnosed by a board-certified physician
who understands lymphedema and its complications. Once the diagnosis of lymphedema has been confirmed and treatment has begun, the
progress must be monitored by the physician. Whereas the clinical diagnosis of lymphedema can most often be established without invasive
testing, and electrocardiogram before the treatment begins and during the course of treatment is sometimes necessary to ensure safe
treatment for each patient.
Lymphangioscintigraphy (LAS), CT scans, and MRIs are also recommended for lymphedema patients before starting CDT. The physician will
be able to decide and inform the patient about the necessity of such procedures at the time of consultation. Because of the complications
associated with lymphedema, the involvement and supervision of a qualified physician is essential for safe and effective lymphedema therapy.

Patient: 50 yr old female diagnosed with cancer in the left breast in November 2004. Patient underwent a radical mastectomy in January 2005 followed
by radiation therapy (Feb-Mar2005) to the affected area. Chemotherapy 1 x per month until Aug 2005.
Patient has a loss of sensation in 3 fingers of the left hand following the mastectomy.
Patient is type 2 diabetic, insulin dependent +Metaformin. Since approx age of 27 years – well controlled.
Weight: 75,3kg
Height: 1m66
BMI: 27.3
Patient underwent a total hysterectomy with bilateral oophorectomy in June 2013 following the discovery of a lesion. No cancer diagnosis at this time.
History of Treatment Received: Patient has never received a diagnosis despite numerous visits to the doctor. She has been prescribed diuretics and
physiotherapy in the past with no noticeable improvements. It was suggested to the patient that surgery to the wrist was needed but she did not go
ahead with this surgery.
Lymphedema Diagnosis: Patient reports the first signs of swelling sometime in 2013. Heaviness in the left arm, inability to wear fitted sleeves. At the time
of meeting this patient (16 Oct 2014) she shows symptoms consistent with Stage 2 Lymphedema. Patient has up to a 7cm difference in arm circumference
on the forearm and a 1cm difference in arm circumference on the upper arm. The forearm and elbow are the worst affected areas with the onset of
fibrosis.
Impact on Quality of Life: Cellulitis infection – last episode December 2014. Diminished use of the arm. Ill-fitting clothes, fatigue in the affected arm due
to heaviness. Disturbed sleep. Embarrassment at comments and attention about her arm in public.
Notes: While there is no doubt that the mastectomy (left breast) and subsequent radiation therapy are the cause of the damage to the lymphatic system
in the affected area and where there is no suggestion that the hysterectomy is the cause of the lymphedema, it should be noted that the onset of symptoms
coincides with the hysterectomy. It would be wise to consider possible trigger factors such as blood pressure cuffs, venipuncture and IV administration to
the left arm at this time.
Suggested Treatment: Complete Decongestive Therapy
Skin and Nail Care
Manual Lymph Drainage
Compression Bandaging
Compression Garments
Materials and Resources: Therapist hours, treatment rooms, foam padding, stockinette, wool pad, finger wraps, short stretch bandages 6cm x 2 8cm x 6
10cm x 2, E45 Lotion, compression sleeve, compression glove including fingers
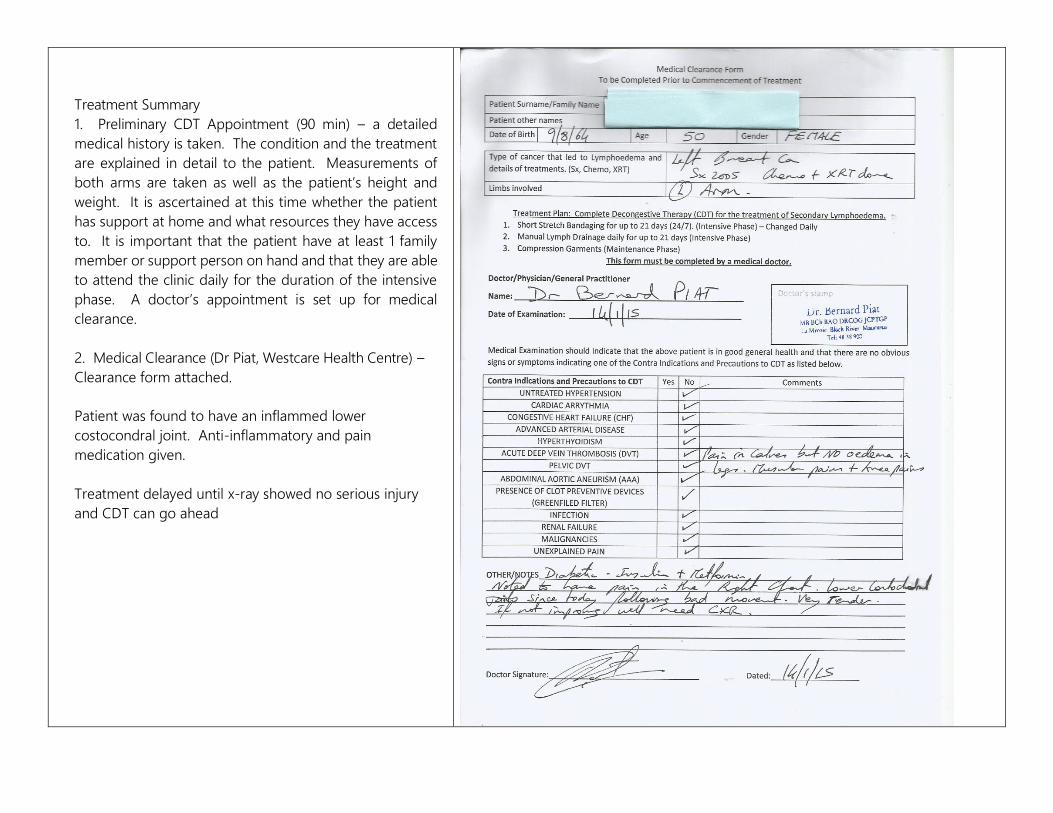
Treatment Summary
1. Preliminary CDT Appointment (90 min) – a detailed
medical history is taken. The condition and the treatment
are explained in detail to the patient. Measurements of
both arms are taken as well as the patient’s height and
weight. It is ascertained at this time whether the patient
has support at home and what resources they have access
to. It is important that the patient have at least 1 family
member or support person on hand and that they are able
to attend the clinic daily for the duration of the intensive
phase. A doctor’s appointment is set up for medical
clearance.
2. Medical Clearance (Dr Piat, Westcare Health Centre) –
Clearance form attached.
Patient was found to have an inflammed lower
costocondral joint. Anti-inflammatory and pain
medication given.
Treatment delayed until x-ray showed no serious injury
and CDT can go ahead

Intensive Phase
Day 1: 2 February 2015 – total treatment time 2h10min
10 minutes skin care
30 minutes MLD – Short neck, rhs axilla prep, lhs inguinal prep, 10 x
diaphragmatic breathing (no MLD to deep abdominal nodes due to
risk factors following abdominal surgery). Anterior interaxillary
anastomoses crossing the midsagittal watershed. Left axillo-inguinal
anastomoses crossing the transverse watershed. Posterior
interaxillary anastomoses crossing the midsagittal watershed.
Drainage of the affected arm is away from the axilla.
60 minutes – cutting foam to size and application of short stretch
compression bandages from fingertips to axilla.
30 minutes – handover of home care instructions and exercise
program (See attached)
Patient showed dismay at the size of the bandaging but otherwise
positive.

Day 2: 3 February 2015 – total treatment time 1h10
Patient tolerated the compression. Bandages stayed in
place. Reduction of up to 2cm in circumference in the
forearm. 1 – 0.5cm reduction in the upper arm.
10 min – bandage removal and skin check
30 min – MLD (as per day 1)
10 min – wash and lotion
20 min – bandage application. Slight increase in
compression.
Patients husband attended and watched bandage
application.
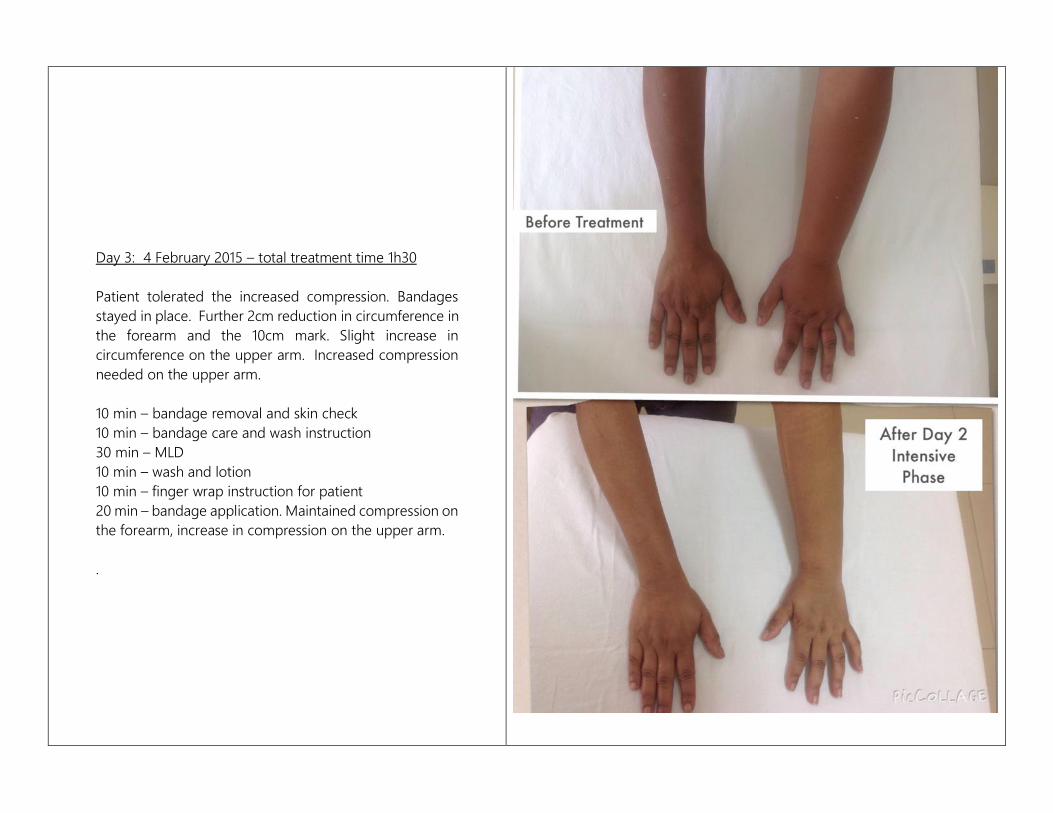
Day 3: 4 February 2015 – total treatment time 1h30
Patient tolerated the increased compression. Bandages
stayed in place. Further 2cm reduction in circumference in
the forearm and the 10cm mark. Slight increase in
circumference on the upper arm. Increased compression
needed on the upper arm.
10 min – bandage removal and skin check
10 min – bandage care and wash instruction
30 min – MLD
10 min – wash and lotion
10 min – finger wrap instruction for patient
20 min – bandage application. Maintained compression on
the forearm, increase in compression on the upper arm.
.
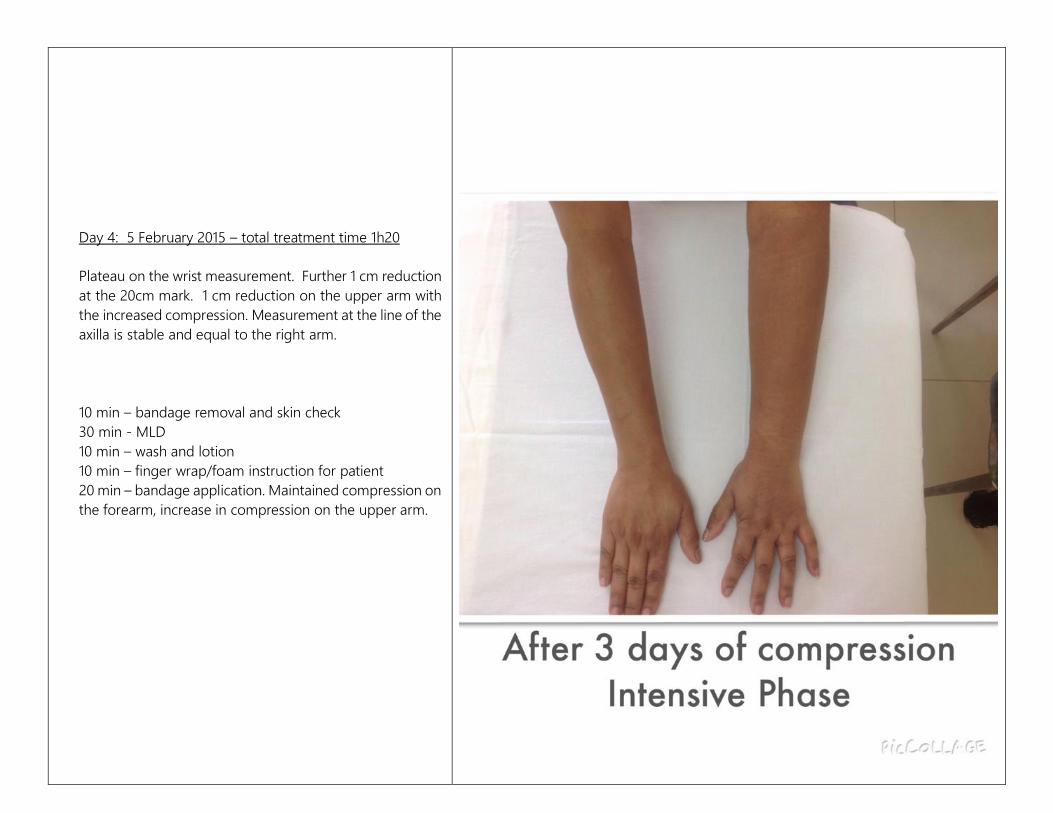
Day 4: 5 February 2015 – total treatment time 1h20
Plateau on the wrist measurement. Further 1 cm reduction
at the 20cm mark. 1 cm reduction on the upper arm with
the increased compression. Measurement at the line of the
axilla is stable and equal to the right arm.
10 min – bandage removal and skin check
30 min - MLD
10 min – wash and lotion
10 min – finger wrap/foam instruction for patient
20 min – bandage application. Maintained compression on
the forearm, increase in compression on the upper arm.
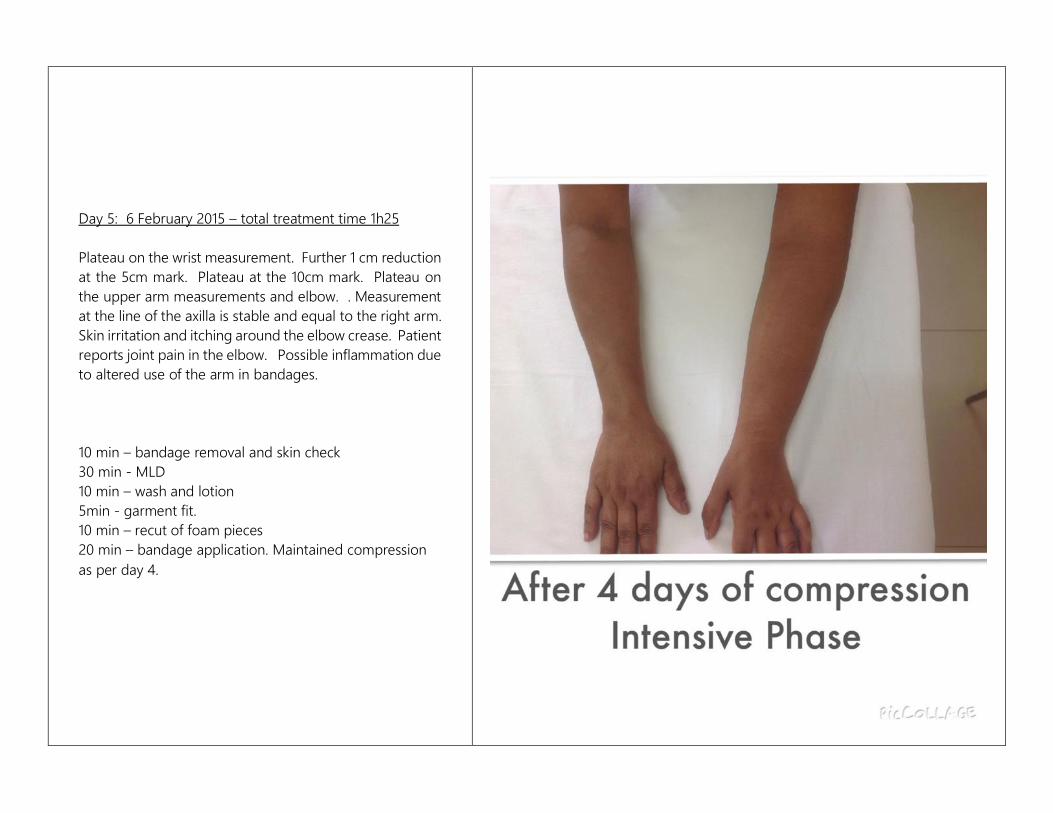
Day 5: 6 February 2015 – total treatment time 1h25
Plateau on the wrist measurement. Further 1 cm reduction
at the 5cm mark. Plateau at the 10cm mark. Plateau on
the upper arm measurements and elbow. . Measurement
at the line of the axilla is stable and equal to the right arm.
Skin irritation and itching around the elbow crease. Patient
reports joint pain in the elbow. Possible inflammation due
to altered use of the arm in bandages.
10 min – bandage removal and skin check
30 min - MLD
10 min – wash and lotion
5min - garment fit.
10 min – recut of foam pieces
20 min – bandage application. Maintained compression
as per day 4.
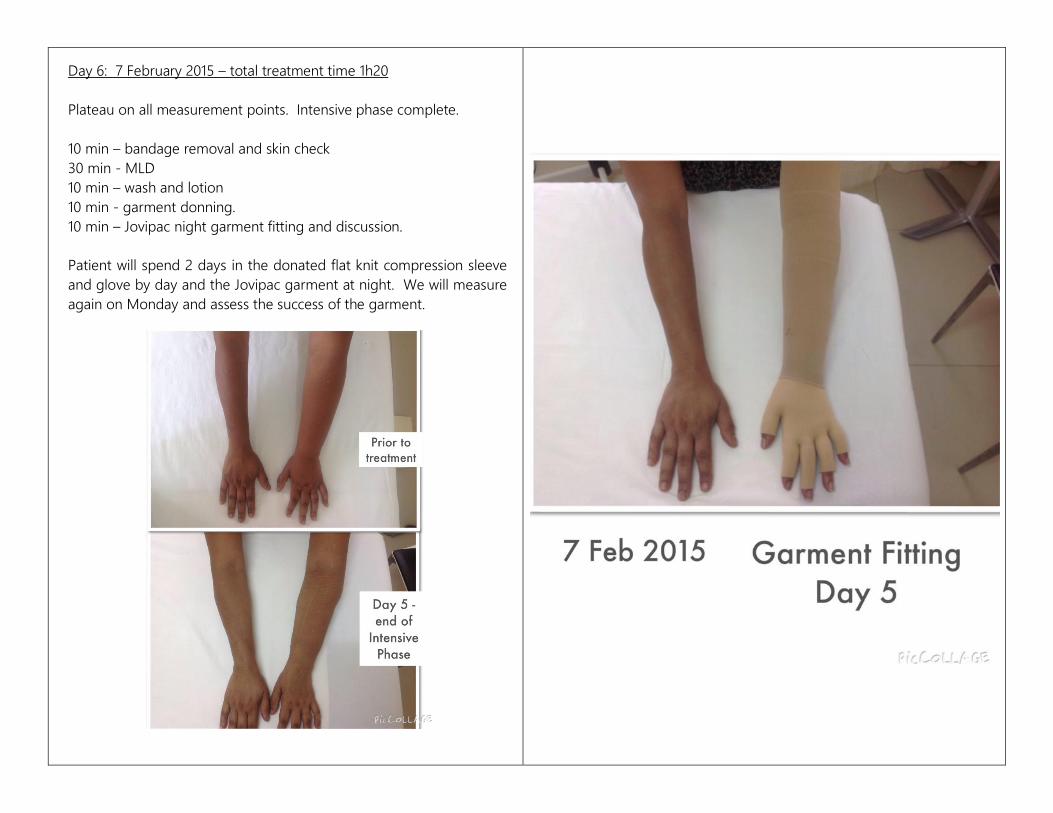
Day 6: 7 February 2015 – total treatment time 1h20
Plateau on all measurement points. Intensive phase complete.
10 min – bandage removal and skin check
30 min - MLD
10 min – wash and lotion
10 min - garment donning.
10 min – Jovipac night garment fitting and discussion.
Patient will spend 2 days in the donated flat knit compression sleeve
and glove by day and the Jovipac garment at night. We will measure
again on Monday and assess the success of the garment.

Measure cm
Patient Case Study
Follow Up Measurements
Date Weight 75.3kg Date Date Date Date Date Date
07-Jan-15
Extremity left / UE 02 February
2015
03 February 2015
04 February
2015
05 February 2015
06 February
2015
07 February 2015
RIGHT LEFT LEFT LEFT LEFT LEFT LEFT LEFT
HAND 21 22 19.5 19 19.3 19 19
WRIST 17.5 20 18.5 18 18 18 18 17.7
5CM 21.4 20.3 20.5
10CM 20 27 26 24 22.7 23.7 23.5 23.4
15CM 27.5 26
20CM 26.5 32 30.5 30 29.3 28.5 29 29.2
Elbow 26 30.5 29 28.5 30 29.5 29.5 29.7
5CM 31 31
10CM 32 33.5 32.5 32 32.5 31.5 31.5 31.5
15CM 33 34
AXILLA 37.5 37.5 37 36 38 37 37 37

Extremity Before CDT After CDT Reduction
RIGHT ARM Unaffected
LEFT ARM Affected LEFT
HAND 21 22 19 2cm
WRIST 17.5 20 17.7 2.3cm
5CM 20.5
10CM 20 27 23.4 3.6cm
15CM 26
20CM 26.5 32 29.2 2.8cm
Elbow 26 30.5 29.7 0.8cm
5CM 31
10CM 32 33.5 31.5 2cm
15CM 34
AXILLA 37.5 37.5 37 0.5cm
Maintenance Phase: In the following week the patient and her husband will be taught the bandaging technique for night-time application. This gives
the best control of swelling and maintenance of the reduction during the intensive treatment. Without adequate night time compression the patient will
be unable to don their day-time compression sleeve and glove. The patient has been fitted with a donated flat knit arm sleeve and glove.
Measurements over the next week will allow us to assess if the grade of garment is correct. If the arm is swelling during the day, we will have to measure
and reorder a garment with a higher grade so as to achieve maintenance of the limb. Should the garment work well, we will re-order same so that the
patient has 2 sets of garments. One needs to be clean and dry at all times.
The patient cannot be without a garment or a compression sleeve/bandages at any time. The arm will begin to fill up with protein rich fluid.
The patient will be taught self MLD techniques and encouraged to keep up the exercise routine and a healthy eating plan.
Conclusion: A 68% reduction in swelling represents a significant improvement in the aesthetics of the arm. Skin care practice and MLD lower the risk of
cellulitis and erysipelas infection. Compliance with treatment will halt the progression of lymphedema meaning that this patient will never progress to
stage 3 with its associated medical costs and complications.
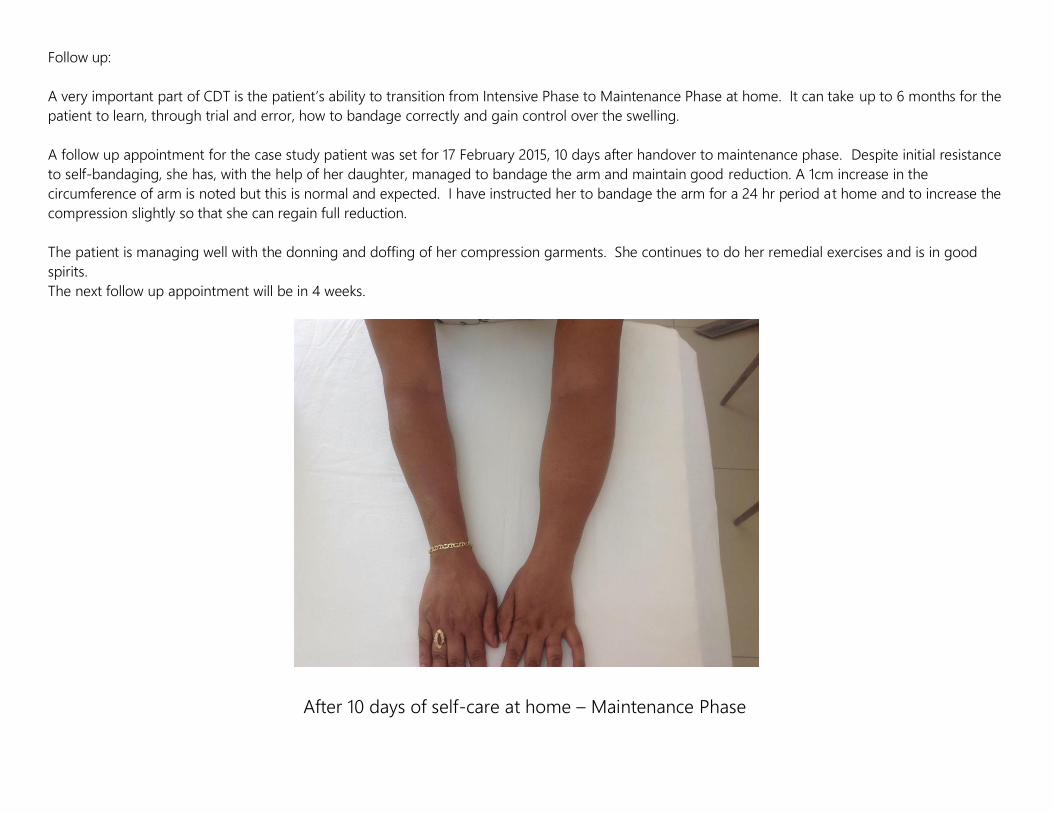
Follow up:
A very important part of CDT is the patient’s ability to transition from Intensive Phase to Maintenance Phase at home. It can take up to 6 months for the
patient to learn, through trial and error, how to bandage correctly and gain control over the swelling.
A follow up appointment for the case study patient was set for 17 February 2015, 10 days after handover to maintenance phase. Despite initial resistance
to self-bandaging, she has, with the help of her daughter, managed to bandage the arm and maintain good reduction. A 1cm increase in the
circumference of arm is noted but this is normal and expected. I have instructed her to bandage the arm for a 24 hr period at home and to increase the
compression slightly so that she can regain full reduction.
The patient is managing well with the donning and doffing of her compression garments. She continues to do her remedial exercises and is in good
spirits.
The next follow up appointment will be in 4 weeks.
After 10 days of self-care at home – Maintenance Phase

Acknowledgements and permission:
1. Some factual information contained in this case study is obtained from the website of The Norton School of Lymphatic Therapy, the school
though which N.Pearce received her training. For more information on lymphedema and training see www.nortonschool.com
2. Permission for the use of photographs is provided by the patient. I would hereby like to express my thanks to the patient for this privilege.