PIIS1542356512007975.pdf
2
Electronic Image of the Month Regression of Hepatocellular Carcinoma With Right Atrial Extension After Sorafenib and Transarterial Chemoembolization MADHU SUBRAMANIAN,* AMIT G. SINGAL, ‡ and ADAM C. YOPP* *Department of Surgery, Division of Surgical Oncology, and ‡ Department of Medicine, Division of Gastroenterology, University of Texas Southwestern Medical Center, Dallas, Texas A 57-year-old man with a past medical history of hepatitis B infection presented for evaluation of a liver mass found on surveillance abdominal ultrasound. On history and physical examination, he was a healthy-looking man with no pertinent signs or symptoms of abdominal pain, ascites, hepatic enceph- alopathy, or lower-extremity swelling. Laboratory results in- cluded the following: alanine aminotransferase level, 60 U/L; total bilirubin level, 1.2 mg/dL; serum albumin level, 4.5 g/dL; prothrombin time, 11.1 s; and international normalized ratio, 1.1. His -fetoprotein level was 5 ng/mL. Magnetic resonance imaging of the abdomen with gadolinium contrast showed a 7.3-cm hypervascular mass with washout consistent with hep- atocellular carcinoma occupying segments 7 and 8 of the right lobe of the liver with tumor thrombus invasion (Figure A, arrow) into the right hepatic vein, inferior vena cava, and right atrium. The patient underwent selective transarterial chemoemboliza- tion consisting of Lipiodol (Guerbet LLC, Bloomington, IN), cis- platin (100 mg), doxorubicin (50 mg), and mitomycin (10 mg), with particle embolization (300 –500 m embospheres) of the arterial supply (Figure B, arrowhead) of the tumor (Figure B, long arrow) and the tumor thrombus (Figure B, short arrow). Post- procedure noncontrast computed tomography of the abdomen showed uptake of Lipiodol within the parenchymal tumor (Figure C, long arrow) and tumor thrombus extending from the inferior vena cava into the right atrium (Figure C, short arrow). Periprocedurally, the patient was started on sorafenib therapy (400 mg orally twice a day) because of the concern for potential systemic spread. At 1 year after a single transarterial chemoem- bolization treatment, magnetic resonance imaging of the abdo- men showed not only a decrease in size of the parenchymal Conflicts of interest The authors disclose the following: Yopp and Singal are on the speakers board for Bayer and Onyx pharmaceuticals. The remaining author discloses no conflicts. © 2012 by the AGA Institute 1542-3565/$36.00 http://dx.doi.org/10.1016/j.cgh.2012.06.031 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:e83– e84
description
Transcript of PIIS1542356512007975.pdf

Electronic Image of the Month
Regression of Hepatocellular Carcinoma With Right Atrial Extension AfterSorafenib and Transarterial Chemoembolization
MADHU SUBRAMANIAN,* AMIT G. SINGAL,‡ and ADAM C. YOPP*‡
*Department of Surgery, Division of Surgical Oncology, and Department of Medicine, Division of Gastroenterology, University of TexasSouthwestern Medical Center, Dallas, Texas
A 57-year-old man with a past medical history of hepatitis Binfection presented for evaluation of a liver mass found
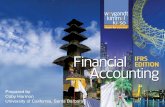
on surveillance abdominal ultrasound. On history and physicalexamination, he was a healthy-looking man with no pertinentsigns or symptoms of abdominal pain, ascites, hepatic enceph-alopathy, or lower-extremity swelling. Laboratory results in-cluded the following: alanine aminotransferase level, 60 U/L;total bilirubin level, 1.2 mg/dL; serum albumin level, 4.5 g/dL;prothrombin time, 11.1 s; and international normalized ratio,1.1. His �-fetoprotein level was 5 ng/mL. Magnetic resonanceimaging of the abdomen with gadolinium contrast showed a7.3-cm hypervascular mass with washout consistent with hep-atocellular carcinoma occupying segments 7 and 8 of the rightlobe of the liver with tumor thrombus invasion (Figure A,arrow) into the right hepatic vein, inferior vena cava, and rightatrium.
The patient underwent selective transarterial chemoemboliza-tion consisting of Lipiodol (Guerbet LLC, Bloomington, IN), cis-platin (100 mg), doxorubicin (50 mg), and mitomycin (10 mg),
with particle embolization (300 –500 �m embospheres) of theC
arterial supply (Figure B, arrowhead) of the tumor (Figure B, longarrow) and the tumor thrombus (Figure B, short arrow). Post-procedure noncontrast computed tomography of the abdomenshowed uptake of Lipiodol within the parenchymal tumor(Figure C, long arrow) and tumor thrombus extending from theinferior vena cava into the right atrium (Figure C, short arrow).Periprocedurally, the patient was started on sorafenib therapy(400 mg orally twice a day) because of the concern for potentialsystemic spread. At 1 year after a single transarterial chemoem-bolization treatment, magnetic resonance imaging of the abdo-men showed not only a decrease in size of the parenchymal
Conflicts of interestThe authors disclose the following: Yopp and Singal are on the
speakers board for Bayer and Onyx pharmaceuticals. The remainingauthor discloses no conflicts.
© 2012 by the AGA Institute1542-3565/$36.00
http://dx.doi.org/10.1016/j.cgh.2012.06.031
LINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:e83–e84

r
e84 IMAGE OF THE MONTH CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 10, No. 10
mass but also no evidence of hypervascularity either in theparenchymal mass (Figure D, arrow) or the inferior vena cava/ight atrial tumor thrombus (Figure E, arrow). The patient
remains asymptomatic at 1 year with no further evidence ofviable tumor, metastatic disease, propagation of tumor intopulmonary vasculature, or findings from chronic liver disease,and he remains on sorafenib.
Hepatocellular carcinoma, the fifth most common cancerworldwide, is the fastest growing cause of cancer-related deathsin the United States.1 Vascular invasion including malignanttumor thrombus in the portal vein or hepatic vein/inferior venacava occurs in 31% to 38% of patients at initial presentation.2
The prognosis for patients with vascular invasion is dismal,with the median overall survival generally less than 7 months.2
Traditionally seen as a harbinger for systemic spread, treatmentfor vascular invasion of the hepatic venous/inferior vena cava
system has relied on systemic chemotherapy with limited sur-vival benefit. With the efficacy of sorafenib and transarterialchemoembolization in systemic and locoregional disease con-trol, a combined treatment approach offers potential new mo-dalities in treating patients with a dismal prognosis.3,4
References1. El-Serag HB, Mason AC. Rising incidence of hepatocellular carci-
noma in the United States. N Engl J Med 1999;340:745–750.2. Marrero JA, Fontana RJ, Barrat A, et al. Prognosis of hepatocellular
carcinoma: comparison of 7 staging systems in an American cohort.Hepatology 2005;41:707–716.
3. Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or che-moembolisation versus symptomatic treatment in patients with un-resectable hepatocellular carcinoma: a randomised controlled trial.Lancet 2002;359:1734–1739.
4. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hep-
atocellular carcinoma. N Engl J Med 2008;359:378–390.