Physiology of blood - u-szeged.hu · Physiology of blood Gyöngyi KarcsúnéDr. Kis Evening seminar...
26
2019.11.08. 1 Physiology of blood Gyöngyi Karcsúné Dr. Kis Evening seminar LOs 8-13., highlighted, bold red color #8 Identify the protein fractions of blood plasma, explain the method (electrophoresis) used for their measurement. Give 1-1 example from each fraction. #9 Describe the mechanism of blood sedimentation, the method of its measurement, significance and normal value. #10 Provide the definition of reticulocyte, its staining and the significance of reticulocyte count. Erythropoietin: production (kidney), trigger, function. #11 Provide the definition of direct and indirect bilirubin. Urobilinogen (UBG), and the significance of its detection in the urine. #12 Describe the role and structure of immunoglobulins and their subtypes and functions. #13 Describe the antigens and the circulating antibodies (Landsteiner-rules). #14 Explain the adhesion, aggregation and activation of thrombocytes. #15 Describe the extrinsic pathway. Describe the intrinsic pathway and the contact phase. #16 Expound the activation and regulation of the plasmin system.
Transcript of Physiology of blood - u-szeged.hu · Physiology of blood Gyöngyi KarcsúnéDr. Kis Evening seminar...

2019.11.08.
1
Physiology of bloodGyöngyi Karcsúné Dr. Kis
Evening seminar
LOs 8-13., highlighted, bold red color
#8 Identify the protein fractions of blood plasma, explain the method (electrophoresis) used for their measurement. Give 1-1 example from each fraction.
#9 Describe the mechanism of blood sedimentation, the method of its measurement, significance and normal value.
#10 Provide the definition of reticulocyte, its staining and the significance of reticulocyte count. Erythropoietin: production (kidney), trigger, function.
#11 Provide the definition of direct and indirect bilirubin. Urobilinogen (UBG), and the significance of its detection in the urine.
#12 Describe the role and structure of immunoglobulins and their subtypes and functions.
#13 Describe the antigens and the circulating antibodies (Landsteiner-rules).
#14 Explain the adhesion, aggregation and activation of thrombocytes.
#15 Describe the extrinsic pathway. Describe the intrinsic pathway and the contact phase.
#16 Expound the activation and regulation of the plasmin system.

2019.11.08.
2
##PlasmaPlasma proteinsproteins� 60-80 g/l
� > 70 kDa
� Non-diffusible
� Mainly glycoproteins (polysaccharide chain, hexose, frucose), [except albumin]!
� Functions:� Colloid-osmotic pressure (albumin)
� Transport
� Buffer (pH regulation)
� Proteolytic enzymes (e.g. blood clotting, complement system)
� Anti-proteolytic proteins and protease inhibitors
� Enzymes
� Immunoglobulins
� Modulators and acute phase proteins
� Tumour markers
Plasma/serum proteins - quantitative measurement� Routine: biuret test
� Normal: 60-80 g/l, plasma fibrinogen +2-6 g/l
� Hyperproteinaemia: dehydration - renal fluid loss; multiple myeloma
� Hypoproteinaemia: protein loss - haemorrhage, burn; malnutrition; malabsorption; hepatic diseases – decreased protein production; infection – increased protein catabolism
� Dysproteinaemia: abnormality of the protein content (ratio)
� Disease � protein content/alteration can be characteristic

2019.11.08.
3
Plasma protein - electrophoresis
Background:
� Alkaline environment: negative (pH=8.6)
� Traveling towards anode (electromotive force)
� Speed: depends on charges, molecular weight
� AAs (glutamic acid, aspartic acid)
� Various mediums: paper, agarose (gel), polyacrylamide (gel) –separation
Plasma protein - PAGE
Workflow
SDS-PAGE
(www.bio-rad.com)
• Molecular filter (gel) (separates 20
fractions)
• Staining:
• Silver (small quantities)
• Oil-Red, Sudan-black
(lipoprotein)
• Periodic acid-Schiff
(glikoprotein)
• Specific substrates and enzymes
• Measurement: densitometry

2019.11.08.
4
##ExamplesExamples
Albumin
� 35-50 g/l
� Albumin/globulin diagnostic importance (1,5-2,5); decrease: hepatic dysfunction, diarrhea, malnutrition
Antitrypsin
� α1- globulin
� 2-4 g/l
� Inhibition of proteolysis in inflammatory processes
� Absence: liver damage
Haptoglobin
� α2- globulin
� Binding free haemoglobin
� 0,5-2,2 g/l
� Acute phase protein
Transferrin
� Β-globulin
� Transport of iron ions
� 2-4 g/l
� Increased level in iron deficiency
Other methods 1.Radial immunodiffusion (Mancini):
Ag-At binding, specificity, quantitative
Agarose plate
standard protein solutions �
calibration
Precipitation rings, diameter and area
proportional to the Ag concentration
Immunoelectrophoresis:
Agarose
Specificity
Semiquantitative
Rocket elektrophoresis:
Quantitative
2019.11.08.
5
Other methods 2.
� RIA
� ELISA
� Immunoturbidimetry, nephelometry
� Measurement of biological activity
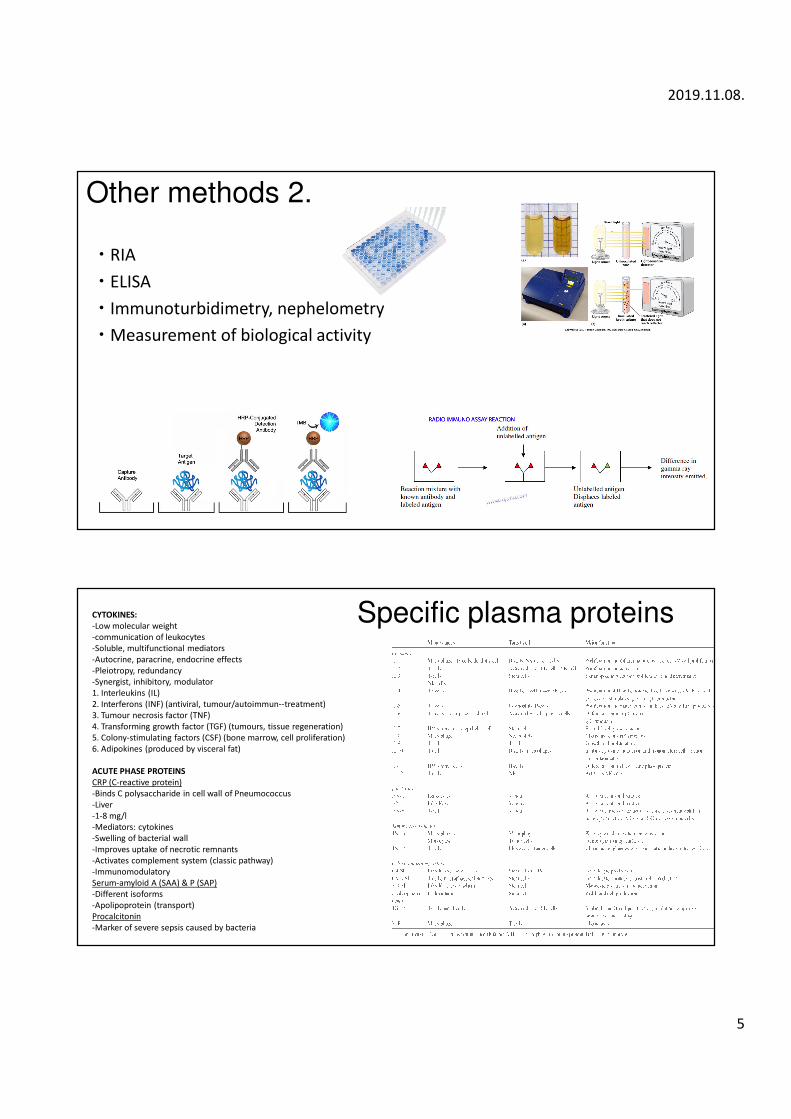
Specific plasma proteinsCYTOKINES:
-Low molecular weight
-communication of leukocytes
-Soluble, multifunctional mediators
-Autocrine, paracrine, endocrine effects
-Pleiotropy, redundancy
-Synergist, inhibitory, modulator
1. Interleukins (IL)
2. Interferons (INF) (antiviral, tumour/autoimmun--treatment)
3. Tumour necrosis factor (TNF)
4. Transforming growth factor (TGF) (tumours, tissue regeneration)
5. Colony-stimulating factors (CSF) (bone marrow, cell proliferation)
6. Adipokines (produced by visceral fat)
ACUTE PHASE PROTEINS
CRP (C-reactive protein)
-Binds C polysaccharide in cell wall of Pneumococcus
-Liver
-1-8 mg/l
-Mediators: cytokines
-Swelling of bacterial wall
-Improves uptake of necrotic remnants
-Activates complement system (classic pathway)
-Immunomodulatory
Serum-amyloid A (SAA) & P (SAP)
-Different isoforms
-Apolipoprotein (transport)
Procalcitonin
-Marker of severe sepsis caused by bacteria

2019.11.08.
6
#Erythrocyte sedimentation#Erythrocyte sedimentation
� inhibited coagulation (e.g. citrate, EDTA), gravitation
� 3 phases:
� Aggregation: slow, proteins have important role � aggregate (rouleauxformation)
� Precipitation: aggregates precipitate in the plasma, faster
� Clustering: aggregates sink, slow
� Normal values:
� Male: 2-6 mm/h
� Female: 8-10 mm/h
� Non specific!!!
Erythrocyte sedimentation rate (ERS)
� Westergren
� Na-citrate, EDTA
Faster sedimentation (>normal value)
Age, anaemia, pregnancy, macrocytosis, inflammation, tumour
Slower sedimentation (<normal value)
Haematocrit (male!), microcytosis, hypogammaglobinaemia, spherocytosis
2019.11.08.
7
##ReticulocyteReticulocyte
� RBC precursor
� Contains: RNA, haemoglobin (34 %), network of granules or filaments (residual RNA and organelles)
� Bone marrow (<1 % RBCs) (diapedesis)
� Immature � 1-2 days � mature erythrocyte
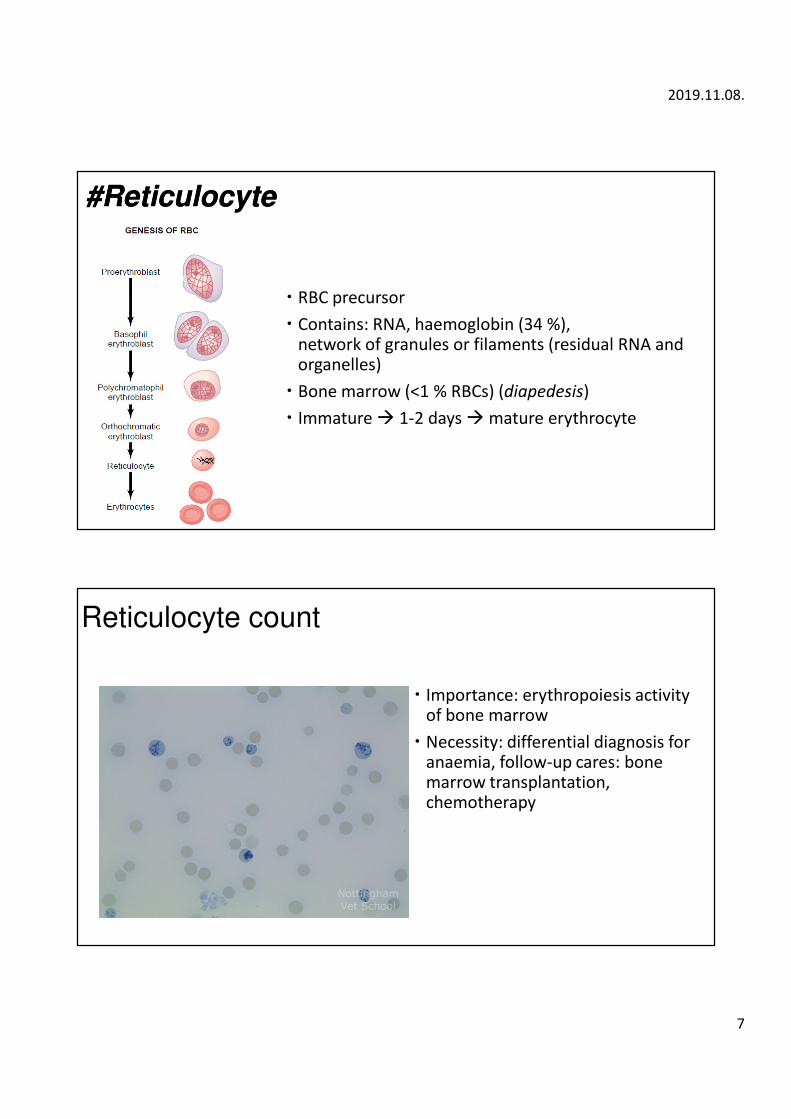
Reticulocyte count
� Importance: erythropoiesis activity of bone marrow
� Necessity: differential diagnosis for anaemia, follow-up cares: bone marrow transplantation, chemotherapy

2019.11.08.
8
Reticulocyte count methods
1. Brilliant cresyl blue or methylene blue staining � light microscope(see lab practice!) (Hb, RNA precipitate)
(time-consuming, inaccurate)
2. Automatic methods:� Larger number of counted cells� Faster� Reproducible results� Less possible error1. Electric resistance -- Coulter- counter
As each particle enters the aperture, it has essentially displaced a volume ofelectrically-conductive fluid equal to its own volume, and the baseimpedance is therefore modulated by an amount proportional to thevolume of the particle. This results in an electrical pulse of short durationbeing created by each particle; the height of the pulse being essentiallyproportional to the volume of the particle. The pulse may be measuredas a change in resistance, current or voltage across the electrodes.(ThermopediaTM)
2. Flow cytometer� Optical� cells are forced one at a time through a focused light beam� Labelling with fluorescent dye, e.g. auramin-O, thiazole orange (TO), 488 nm
Changes in reticulocyte count
� > : increased RBC production (due to blood loss, anaemia)
� < : decreased RBC production (anaemia (pernicious, aplastic, iron deficiency), radiation, infection, bone marrow deficiency)
� Result might interfere with:
� drugs for Parkinson’s disease, rheumatoid arthritis, fever, malaria, chemotherapy
� Radiation
� Antibiotics
� Pregnancy
� Blood transfusion
2019.11.08.
9
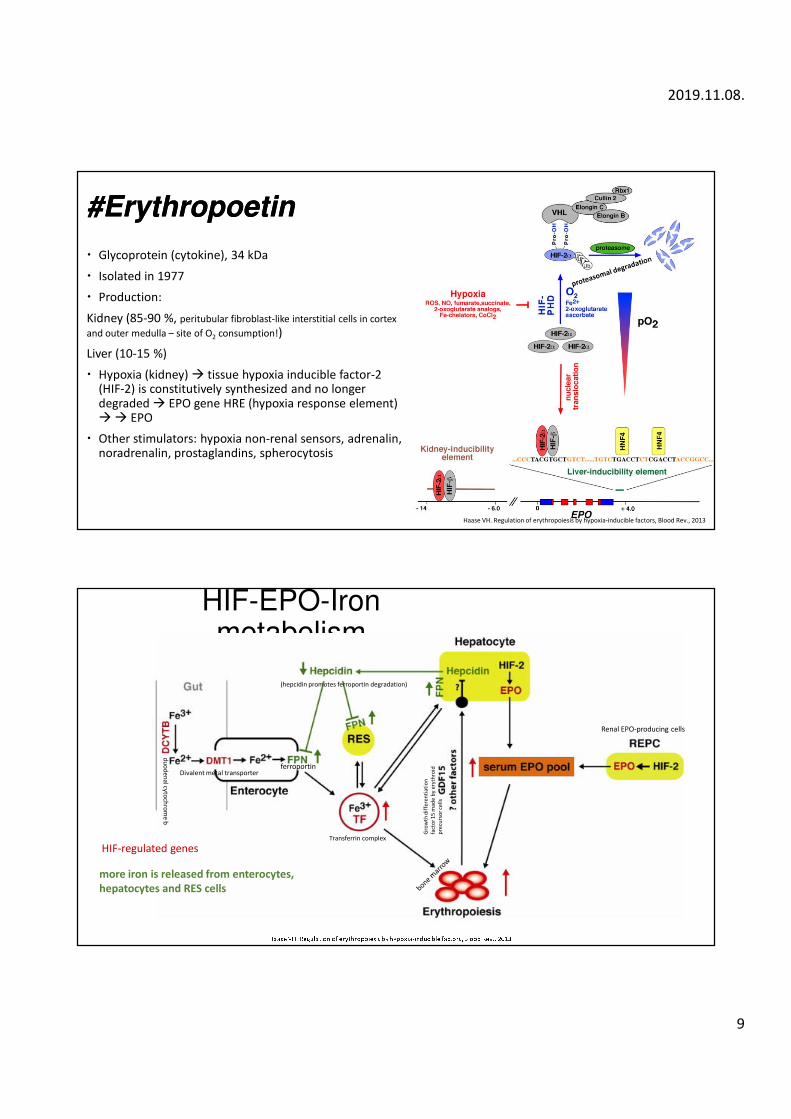
##ErythropoetinErythropoetin
� Glycoprotein (cytokine), 34 kDa
� Isolated in 1977
� Production:
Kidney (85-90 %, peritubular fibroblast-like interstitial cells in cortex
and outer medulla – site of O2 consumption!)
Liver (10-15 %)
� Hypoxia (kidney) � tissue hypoxia inducible factor-2 (HIF-2) is constitutively synthesized and no longer degraded � EPO gene HRE (hypoxia response element) �� EPO
� Other stimulators: hypoxia non-renal sensors, adrenalin, noradrenalin, prostaglandins, spherocytosis
Haase VH. Regulation of erythropoiesis by hypoxia-inducible factors, Blood Rev., 2013
HIF-EPO-Ironmetabolism
Renal EPO-producing cells
Divalent metal transporter
du
od
en
alcy
toch
rom
eb
ferroportin
Transferrin complex
(hepcidin promotes ferroportin degradation)
more iron is released from enterocytes,
hepatocytes and RES cells
HIF-regulated genes
Gro
wth
dif
fere
nti
ati
on
fact
or
15
ma
de
by
ery
thro
id
pre
curs
or
cell
s
2019.11.08.
10
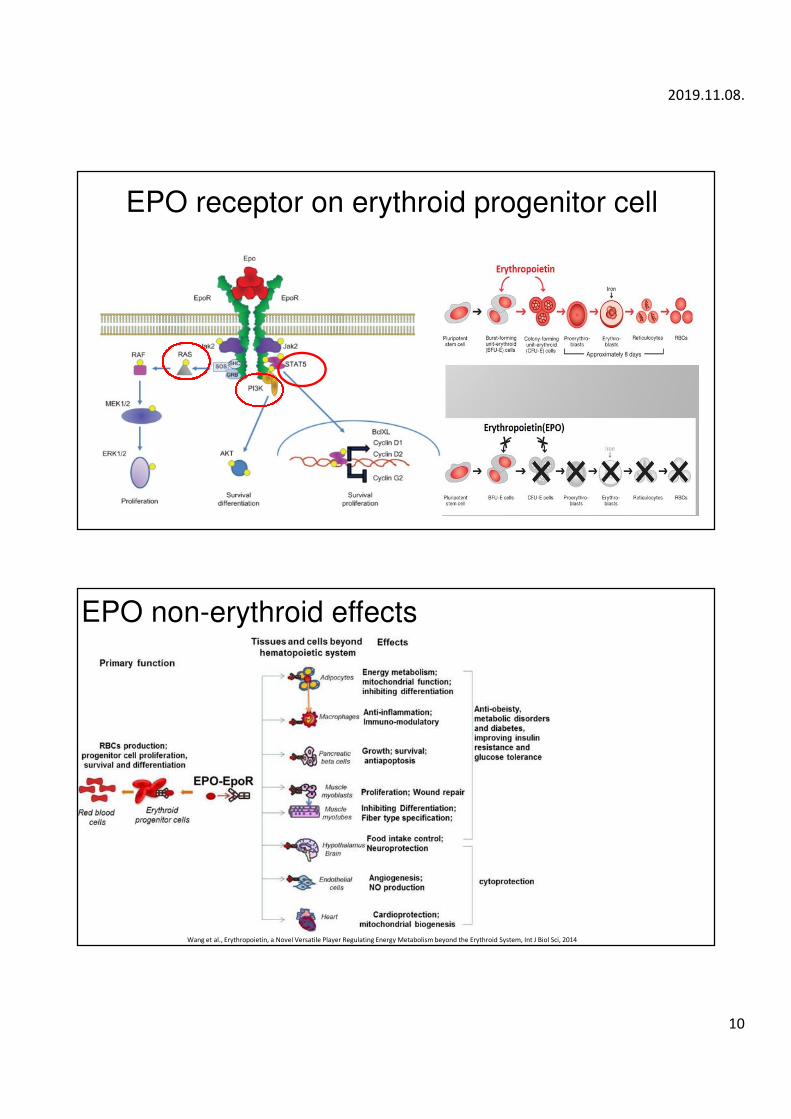
EPO receptor on erythroid progenitor cell
EPO non-erythroid effects
Wang et al., Erythropoietin, a Novel Versatile Player Regulating Energy Metabolism beyond the Erythroid System, Int J Biol Sci, 2014

2019.11.08.
11
EPO as a PED
� most widely used PED (performance-enhancing drug)
� Stroke, thrombus, heart attack
#Bilirubin#Bilirubin

2019.11.08.
12
Bilirubin: Hemoglobin (80%) + tissue hemproteins)
1. Worn RBC�issue macrophage (liver, spleen)
2. Hemoglobin binds temporarily to haptoglobin in the blood (hem-binding protein in the blood:
hemopexin)
3. Fe2 + dissociates and utilized or stored, and proteolysis of β-globin also occurs
4. Porphyrin backbone splits: CO + biliverdin, then bilirubin
5. Circulation: albumin bound indirect (unconjugated) bilirubin (5-17µmol / l)
6. Bilirubin is taken up by hepatocytes (bilirubin-Na + co-transporter)
7. It binds to ligandin inside the liver cell
8. Conjugation with glucuronic acid (hydrophobic hydrophilic) by glucuronyl transferase produces direct
(conjugated) bilirubin
9. Bilirubin-glucuronides enter ABC transporters into the lumen of the epecanaliculus (yellow bile), not
towards the sinusoids!
10.Bile excreted in the intestine (500 µmol / day)
11. Intestinal bacteria � bilirubin degradation products: eg. urobilinogen, stericobilinogen (spontaneous
oxidation - faeces)
12.Urobilinogen reuptake:
In the liver, hepatocytes are converted to bilirubin and re-enter the intestine via the bile (enterohepatic
circulation)
It is excreted through the kidneys (urine color)
13.Daily selection of bile dye: 1-2 mg
Bile pigment
� Haemoglobin (80 %), tissue haemoproteins (myoglobin, cytochromes, enzymes)
� Antioxidants effects
� Non-conjugated bilirubin: van den Bergh-reagent + alcohol discoloration �indirect reaction � indirect bilirubin
� Not filtrated in kidney, no presence in urine (albumin)
� Increased RBC degradation, haemolysis, haematoma � glucuronide production ↓�
Hyperbilirubinemia: > 40 µmol/l (sclera, skin yellowish, icterus, Kernicterus – blood-brain barrier!)
� Blood contains indirect bilirubin (5-17 µmol/l)
� Conjugated bilirubin: direct bilirubin
� hepatocyte dysfunction (direct bilirubin returns into sinusoidal blood) � water soluble, hyperbilirubinemia � filtrated in kidneys � presence in urine
2019.11.08.
13
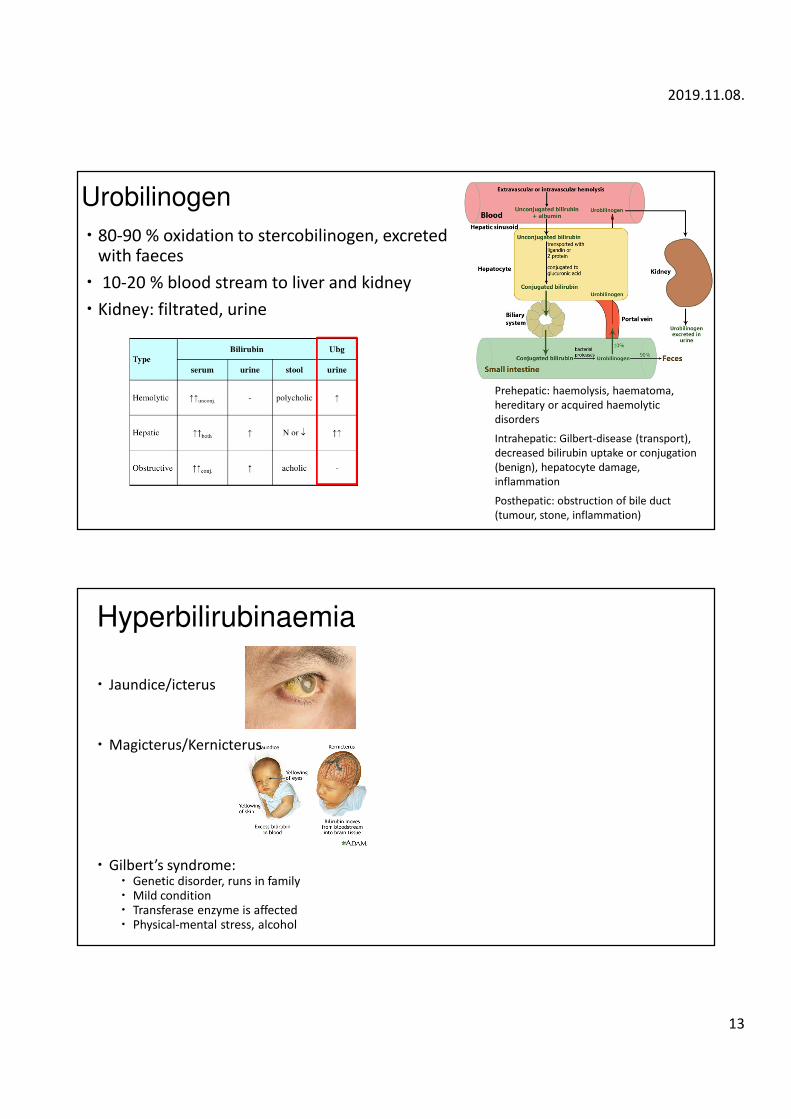
Urobilinogen
� 80-90 % oxidation to stercobilinogen, excreted with faeces
� 10-20 % blood stream to liver and kidney
� Kidney: filtrated, urine
Prehepatic: haemolysis, haematoma,
hereditary or acquired haemolytic
disorders
Intrahepatic: Gilbert-disease (transport),
decreased bilirubin uptake or conjugation
(benign), hepatocyte damage,
inflammation
Posthepatic: obstruction of bile duct
(tumour, stone, inflammation)
Hyperbilirubinaemia
� Jaundice/icterus
� Magicterus/Kernicterus
� Gilbert’s syndrome: � Genetic disorder, runs in family� Mild condition� Transferase enzyme is affected� Physical-mental stress, alcohol

2019.11.08.
14
White blood cells (leukocytes)
May-Grünwald-Giemsa staining
Flow-cytometry (marker of cell
surface)
� Number: 5-8 000 cells/µl
� Haematopoietic stem cell, HSC
� Bone marrow, blood stream, lymphatic system, organs
� Quantitative blood test:
� leukocytosis(↑), leukopenia(↓)
� Qualitative blood: percentage of the leukocyte types
Types of leukocytes
� NEUTROPHIL - 50-70%
� diameter: 10-12 μm
� nucleus: segmented (multiple lobes)
� granules: small, poorly stained
� lifespan: hours (spleen-tissue: days)
� targets: bacteria, fungi
� Phagocytosis
� EOSINOPHIL - 2-4%
� diameter: 10-12 μm
� nucleus: two lobes
� granules: large, haematoxylin-eosin staining
� lifespan: 1-2 weeks (hours in circulation)
� Targets: parasites, allergic reactions

2019.11.08.
15
� BASOPHIL - < 1%
� diameter: 12-15 μm
� nucleus: 2 or 3 lobes
� granules: strong basophil staining (blue)
� lifespan: several hours-days
� Histamine release (inflammation and allergy) – anaphylaxis
� LYMPHOCYTE - 20-40%
� diameter: 7-8 μm
� nucleus: non-central, round
� Life-span: weeks-years
� B-cells: antibody production (plasma cell) – humoral immunity
� T-cells: destroying cells infected by viruses (and tumour cells) – cellular immunity
� NK (Natural Killer) cell: large lymphocyte, non-specific cellular immunity
� MONOCYTE - 4-8%
� diameter: 15-20 μm
� nucleus: bean shape
� phagosome in the cytoplasm
� lifespan: hours-days in circulation, in tissue: macrophage (without activation months-years), activated by cytokines, chemoattractant
� phagocytosis (microbes, tissue debris), antigen presentation
� Tissue macrophages (Histiocytes) (reticuloendothelial system/monocyte-macrophage cell system):� Dendritic cells (skin, mucous epithelium)
� Kupffer cells (liver)
� Microglia (brain)
� Osteoclast (bone)
� Langerhans cell (skin, mucosa)
� Alveolar macrophages (lung)

2019.11.08.
16
Phagocytosis� Phago=devour, cyto=cell, sis=process
� Engulfing and destruction of particulate matter
� Neutrophil granulocyte, monocyteAutophagy:
Nobel Prize in Physiology or Medicine (Ohsumi, 2016)
- new type of vesicle (autophagosome) transporting cellular cargo to the
lysosome for degradation
- controls important physiological functions where cellular components
need to be degraded and recycled
- Fuels the renewal of cellular components
- essential for the cellular response to starvation and other types of stress
- eliminate invading intracellular bacteria and viruses
- embryo development, cell differentiation, eliminates damaged proteins
and organelles, quality control mechanisms
- Disrupted autophagy has been linked to Parkinson’s disease, type 2
diabetes and other disorders that appear in the elderly
Oxidative burst
Reactive Oxygen Intermediates
Reactive Nitrogen Intermediates
Enzymes
Immune responses
1. Natural (innate) immunity
• First contact with the infectious agents
• No memory
• mechanism: phagocytosis, complement proteins (stimulation of phagocytosis [opsonisation], chemotaxis, cytolysis)
2. Adaptive (acquired) immunity
• Based on the recognition of the antigen
• Cell-based (cytolysis) and humoral immunity (production of antibodies)
• memory (vaccination)
Communication and regulation of leukocytes: CYTOKINES
Inflammation response: Arachidonic-acid derivate
2019.11.08.
17
Natural immunity
� Pathogen-associated molecular pattern (PAMP)(e.g. polysaccharide of bacteria, viral RNA): indicating groups of microorganisms, but not specific ones
� Pattern recognition receptors (PRR): PAMP detection: � Toll-like receptors
� NOD-receptor (intracellular, viruses)
� Mannose-binding lectin
� Cells:� MACROPHAGES
� DENDRITIC CELL
� GRANULOCYTES
� NK CELLS (virus)
� Attachment to the endothelial wall � „rolling”, stepping out to the tissue �migration
Humoral part of innate immune system – complement system
Cascade of proteolytic enzymes
Produced in liver (precursor forms)
3 pathways:
ClassicalLectin
Alternative
Function: � Cytolysis (pore formation in membrane – C5-9)
� Chemotaxis (C5a fragment)
� Opsonisation (C3b, C4b)
� Changing the molecular structure of viruses

2019.11.08.
18
Membrane attack complex
(MAC)
Adaptive immunity
� Antigen presentation in the membrane:
MHC (major histocompatibility complex) � A protein joined to the antigen for cell surface display (HLA- human leukocyte antigen)
� MHC-I � Found in every cell that has nucleus
� High degree of variety, individual differences („marker of my cells”)
� cytotoxic T-cells can recognise (virus infected cells, tumour cells)
� MHC- II � Immune cells (antigen presenting cells)
� Join to antigen fragments digested in lysosomes (e.g. bacteria)
� Helper T cells can recognise
2019.11.08.
19
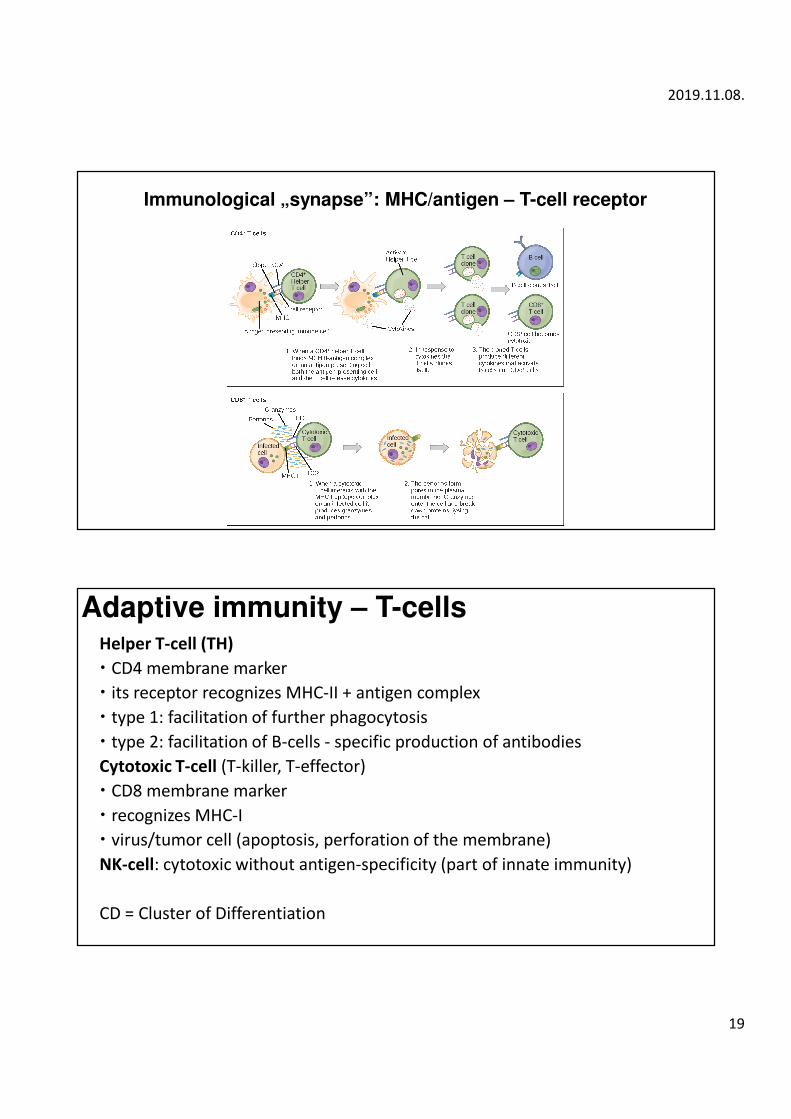
Immunological „synapse”: MHC/antigen – T-cell receptor
Adaptive immunity – T-cellsHelper T-cell (TH)
� CD4 membrane marker
� its receptor recognizes MHC-II + antigen complex
� type 1: facilitation of further phagocytosis
� type 2: facilitation of B-cells - specific production of antibodies
Cytotoxic T-cell (T-killer, T-effector)
� CD8 membrane marker
� recognizes MHC-I
� virus/tumor cell (apoptosis, perforation of the membrane)
NK-cell: cytotoxic without antigen-specificity (part of innate immunity)
CD = Cluster of Differentiation

2019.11.08.
20
Memory cell
� CD8+/CD4+ or B-cell
� stores the memory of antigens for years
� fast activation and division in the case of new exposition
Regulatory T-cell (suppressor T-cell)
� immunotolerance: active inhibition of response in the case of the antigens of self-tissue and tolerated (non-harmful) others
� central: selection of autoreactive cells in the thymus
� peripheral: demarcation (e.g. brain, eye, joints), inhibitory cytokines (TGF), negative co-stimulation (CD molecules)
γδ T-cell
� receptor consists of γδ subunits instead of the common αβ
� intraepithelial lymphocyte in the mucosa
� recognizing whole proteins without MHC
Adaptive immunity – B-cells
� Plasma cell: antibody production
� Antigen presenting cells

2019.11.08.
21
##ImmunoglobulinsImmunoglobulins
IgG: most common, binds phagocytes (opsonisation),
passes placenta
IgM: ancient, initial synthesis
IgA: in mucosa-secreted fluid
IgE: cytophil antibody, binds to basophils and mast cells
IgD: B-cell receptor before antigen exposition
Mediators of immune response
ARACHIDONIC ACID derivates:
ACUTE PHASE PROTEINS
CYTOKINES
(see slide #10)
2019.11.08.
22
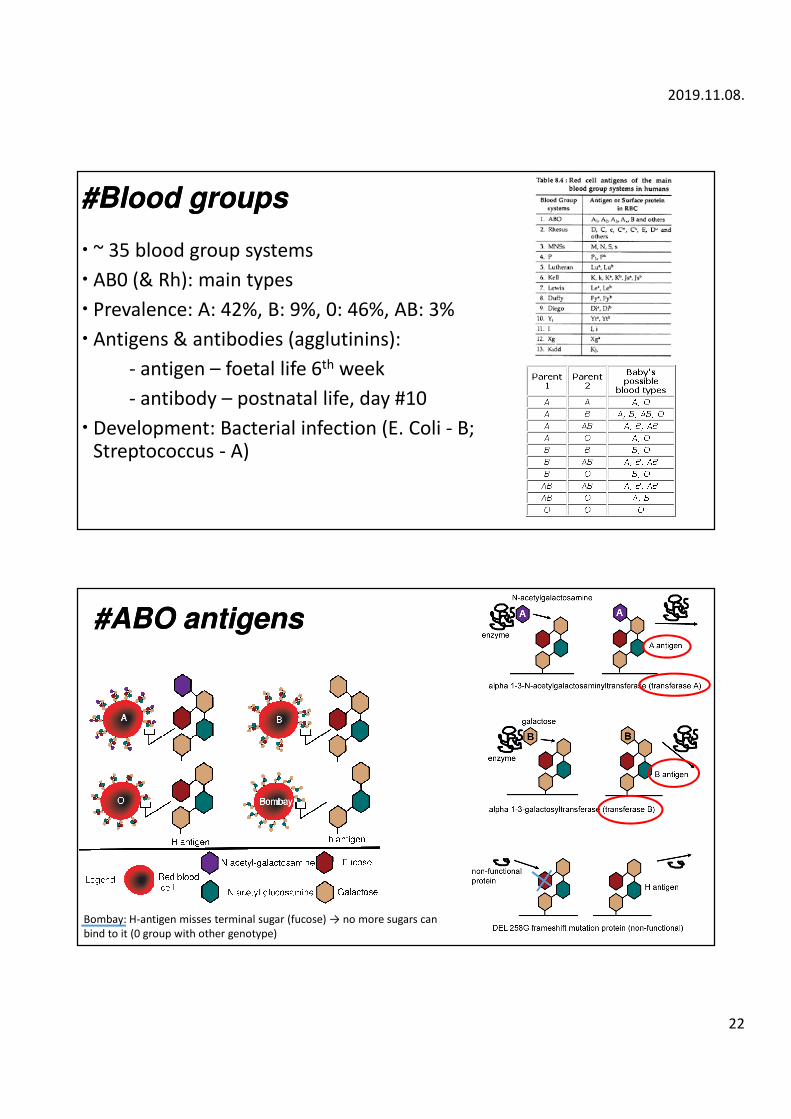
##BloodBlood groupsgroups
� ~ 35 blood group systems
� AB0 (& Rh): main types
� Prevalence: A: 42%, B: 9%, 0: 46%, AB: 3%
� Antigens & antibodies (agglutinins):
- antigen – foetal life 6th week
- antibody – postnatal life, day #10
� Development: Bacterial infection (E. Coli - B; Streptococcus - A)
#ABO #ABO antigensantigens
Bombay: H-antigen misses terminal sugar (fucose) → no more sugars can
bind to it (0 group with other genotype)

2019.11.08.
23
Testing for blood group determination
� Not for paternity testing, only excludes!
� Cross reaction:
� Major test
� Minor test
� Non-compatible blood transfusion:
� Antibody-antigen reaction � haemolysis of donor cells � haemoglobin release, kidney failure
agglutination
#Landsteiner #Landsteiner principleprinciple
(Karl Landsteiner, 1900)

2019.11.08.
24
Rh (Rhesus) blood group� Protein antigens, 3 allelic pairs: c/C, d/D, e/E
� D is the only strong antigen – Rh+ blood group
� there is no spontaneous immunization (antibodies)only if:
a. Rh-receives Rh+blood
b. Rh-mother has Rh+ baby (Rh prophylaxis by giving incomplete Rh-antibodies that suppress production, unless possibility of erythroblastosis fetalis)
Blood clotting

2019.11.08.
25
#14 Explain the adhesion, aggregation and activation of thrombocytes.
Serotonin
TXA2
ADR
collagen
Primary
adhesion
before
activation
Aggregation
of the
activated
platelets
#15 Describe the extrinsic pathway. Describe the intrinsic pathway and the contact phase.
Glass

2019.11.08.
26
# 16 Expound the activation and regulation of the plasmin system.