Physiological Barriers to Delivery of Monoclonal Antibodies and … · Rakesh K. Jain Department of...
7
(CANCER RESEARCH (SUPPL.) 50. 814s-819s. February 1, 1990] Physiological Barriers to Delivery of Monoclonal Antibodies and Other Macromolecules in Tumors1 Rakesh K. Jain Department of Chemical Engineering, Carnegie Mellon University, Pittsburgh, Pennsylvania 15213-3890 Abstract The efficacy in cancer treatment of monoclonal antibodies or other macromolecules bound to radionuclides, chemotherapeutic agents, toxins, enzymes, growth factors, or effector antibodies has been limited by their inability to reach their target in vivo in adequate quantities. Heterogeneity of tumor-associated antigen expression alone has failed to explain the nonuniform uptake of antibodies. As a result, only in recent years have the peculiarities of tumor physiology been recognized as determinants of antibody distribution. Three physiological barriers responsible for the poor localization of macromolecules in tumors have been identified: (a) heterogeneous blood supply; (/>) elevated interstitial pressure; and (<•) large transport distances in the interstitium. The first barrier limits the delivery of blood-borne molecules to well-perfused regions of a tumor; the second barrier reduces extravasation of fluid and macromolecules in the high interstitial pressure regions and also leads to an experimentally verifiable, radially outward convection in the tumor periphery which opposes the inward diffusion; and the third barrier increases the time required for slowly moving macromolecules to reach distal regions of a tumor. Binding of antibody to an antigen further lowers the effective diffusion rate of the antibody by reducing the amount of mobile antibody. Due to micro- and macroscopic heterogeneities in tumors, the relative magnitude of each of these barriers would vary from one location to another and from one day to the next in the same tumor and from one tumor to another. If the genetically engineered macromolecules, e.g., lymphokines, and other new modalities, e.g., killer lymphocytes, as well as low molecular weight cytotoxic agents, are to fulfill their clinical promise, methods must be developed to overcome these physiological barriers. Some of these methods are discussed, and situations wherein these barriers may not be a problem are pointed out. Introduction The advent of hybridoma technology and genetic engineering has led to the design and large-scale production of monoclonal antibodies and other biological macromolecules potentially use ful for cancer detection and treatment. These molecules can be conjugated to radionuclides, chemotherapeutic agents, toxins, growth factors, enzymes, effector antibodies, or liposomes. Moreover, a number of macromolecular cytolytic molecules (e.g., tumor necrosis factor, lymphokines) and killer cells are under active investigation as potential therapeutic agents. While the concept of using antibodies with a high degree of specificity for tumor-associated antigens remains attractive for cancer therapy, clinical results have not, to date, lived up to the earlier promises of their perceived potential (for review, see Refs. 1 and 2). A key problem with antibodies and other macromole cules is their inability to reach all regions of a tumor in adequate quantities. Heterogeneity of tumor associated antigen alone cannot account for the poor penetration of antibodies in tumors. What mechanisms then are responsible for this maldistribution of monoclonal antibodies and other macromolecules in tumors? A blood-borne molecule that enters the tumor circulation reaches cancer cells via: (a) distribution through the vascular 1Presented at the "Second Conference on Radioimmunodetection and Ra- dioimmunotherapy of Cancer." September 8-10, 1988, Princeton. NJ. This article is based on research supported by grants from the National Cancer Institute, The National Science Foundation, the American Cancer Society, and the R. K. Mellon Foundation; by an NIH Research Cancer Development Award; and by a Guggen heim Fellowship. space; (b) transport across the microvascular wall; and (c) transport through the interstitial space. Each of these transport processes may involve convection (i.e., solute movement asso ciated with bulk solvent movement) and diffusion (i.e., solute movement resulting from solute concentration gradients). In addition, during this journey the molecule may bind nonspecif- ically to proteins or other tissue components, bind specifically to the target(s), and/or be metabolized (for review, see Refs. 3 and 4). In this article, I will critically review these physiological barriers to macromolecular transport in tumors and discuss some strategies to overcome them for therapeutic benefit. Distribution through Vascular Space The tumor vasculature consists of (a) vessels recruited from the preexisting network of the host vasculature and (b) vessels resulting from the angiogenic response of host vessels to cancer cells (5, 6). Movement of molecules through the vasculature is governed by the vascular morphology (i.e., the number, length, diameter, and geometrical arrangement of various blood ves sels) and the blood flow rate. Vascular Morphology. Although the tumor vasculature orig inates from the host vasculature, its organization may be com pletely different depending upon the tumor type, its growth rate, and its location. The architecture is different not only among various tumor types but also between a spontaneous tumor and its transplants (for review, see Ref. 7). Macroscopically, the tumor vasculature can be studied in terms of two idealized categories: peripheral and central. In tumors with peripheral vascularization, the centers are usually poorly perfused (Fig. 1). In those with central vascularization, one would expect the opposite. Hence, the penetration of blood borne substances should follow the same pattern. In reality, a tumor may consist of many territories, each exhibiting one or the other of these two types of idealized vascular patterns. Microscopically, the tumor vasculature is highly heteroge neous and does not conform to the standard normal vascular organization (i.e., artery to arteriole to capillaries to postcapil- lary venule to venule to vein). Based on their ultrastructure, the tumor vessels can be classified into nine categories: (a) arteries and arterioles; (b) nonfenestrated capillaries; (c) fenestrated capillaries; (d) discontinuous capillaries (sinusoids); (e) blood channels without endothelial lining; (/) capillary sprouts; (g) postcapillary venules (giant capillaries); (h) venules and veins; and (/) arteriovenous anastomoses (shunts) (7). Note that except for vessels of classes e and /, the remaining vessel types are structurally similar to those found in a normal tissue. The vessels of classes e and / are found in healing (granulation) tissue. A key difference between normal and tumor vessels is that the latter are dilated, saccular, and tortuous and may contain tumor cells within the endothelial lining of the vessel wall (7). In addition, unlike a normal tissue with a fixed route between arterial and venous sides, a tumor may have blood flowing from one venule to another via vessels of classes b through g, or directly via an arteriovenous shunt. Furthermore, due to the peculiar nature of the vasculature, the organization 814s Research. on November 1, 2020. © 1990 American Association for Cancer cancerres.aacrjournals.org Downloaded from
Transcript of Physiological Barriers to Delivery of Monoclonal Antibodies and … · Rakesh K. Jain Department of...

(CANCER RESEARCH (SUPPL.) 50. 814s-819s. February 1, 1990]
Physiological Barriers to Delivery of Monoclonal Antibodies and OtherMacromolecules in Tumors1
Rakesh K. JainDepartment of Chemical Engineering, Carnegie Mellon University, Pittsburgh, Pennsylvania 15213-3890
Abstract
The efficacy in cancer treatment of monoclonal antibodies or othermacromolecules bound to radionuclides, chemotherapeutic agents, toxins,enzymes, growth factors, or effector antibodies has been limited by theirinability to reach their target in vivo in adequate quantities. Heterogeneityof tumor-associated antigen expression alone has failed to explain the
nonuniform uptake of antibodies. As a result, only in recent years havethe peculiarities of tumor physiology been recognized as determinants ofantibody distribution. Three physiological barriers responsible for thepoor localization of macromolecules in tumors have been identified: (a)heterogeneous blood supply; (/>) elevated interstitial pressure; and (<•)
large transport distances in the interstitium. The first barrier limits thedelivery of blood-borne molecules to well-perfused regions of a tumor;
the second barrier reduces extravasation of fluid and macromolecules inthe high interstitial pressure regions and also leads to an experimentallyverifiable, radially outward convection in the tumor periphery whichopposes the inward diffusion; and the third barrier increases the timerequired for slowly moving macromolecules to reach distal regions of atumor. Binding of antibody to an antigen further lowers the effectivediffusion rate of the antibody by reducing the amount of mobile antibody.Due to micro- and macroscopic heterogeneities in tumors, the relative
magnitude of each of these barriers would vary from one location toanother and from one day to the next in the same tumor and from onetumor to another. If the genetically engineered macromolecules, e.g.,lymphokines, and other new modalities, e.g., killer lymphocytes, as wellas low molecular weight cytotoxic agents, are to fulfill their clinicalpromise, methods must be developed to overcome these physiologicalbarriers. Some of these methods are discussed, and situations whereinthese barriers may not be a problem are pointed out.
Introduction
The advent of hybridoma technology and genetic engineeringhas led to the design and large-scale production of monoclonalantibodies and other biological macromolecules potentially useful for cancer detection and treatment. These molecules can beconjugated to radionuclides, chemotherapeutic agents, toxins,growth factors, enzymes, effector antibodies, or liposomes.Moreover, a number of macromolecular cytolytic molecules(e.g., tumor necrosis factor, lymphokines) and killer cells areunder active investigation as potential therapeutic agents. Whilethe concept of using antibodies with a high degree of specificityfor tumor-associated antigens remains attractive for cancertherapy, clinical results have not, to date, lived up to the earlierpromises of their perceived potential (for review, see Refs. 1and 2). A key problem with antibodies and other macromolecules is their inability to reach all regions of a tumor in adequatequantities. Heterogeneity of tumor associated antigen alonecannot account for the poor penetration of antibodies in tumors.What mechanisms then are responsible for this maldistributionof monoclonal antibodies and other macromolecules in tumors?
A blood-borne molecule that enters the tumor circulationreaches cancer cells via: (a) distribution through the vascular
1Presented at the "Second Conference on Radioimmunodetection and Ra-dioimmunotherapy of Cancer." September 8-10, 1988, Princeton. NJ. This article
is based on research supported by grants from the National Cancer Institute, TheNational Science Foundation, the American Cancer Society, and the R. K. MellonFoundation; by an NIH Research Cancer Development Award; and by a Guggenheim Fellowship.
space; (b) transport across the microvascular wall; and (c)transport through the interstitial space. Each of these transportprocesses may involve convection (i.e., solute movement associated with bulk solvent movement) and diffusion (i.e., solutemovement resulting from solute concentration gradients). Inaddition, during this journey the molecule may bind nonspecif-ically to proteins or other tissue components, bind specificallyto the target(s), and/or be metabolized (for review, see Refs. 3and 4). In this article, I will critically review these physiologicalbarriers to macromolecular transport in tumors and discusssome strategies to overcome them for therapeutic benefit.
Distribution through Vascular Space
The tumor vasculature consists of (a) vessels recruited fromthe preexisting network of the host vasculature and (b) vesselsresulting from the angiogenic response of host vessels to cancercells (5, 6). Movement of molecules through the vasculature isgoverned by the vascular morphology (i.e., the number, length,diameter, and geometrical arrangement of various blood vessels) and the blood flow rate.
Vascular Morphology. Although the tumor vasculature originates from the host vasculature, its organization may be completely different depending upon the tumor type, its growthrate, and its location. The architecture is different not onlyamong various tumor types but also between a spontaneoustumor and its transplants (for review, see Ref. 7).
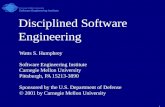
Macroscopically, the tumor vasculature can be studied interms of two idealized categories: peripheral and central. Intumors with peripheral vascularization, the centers are usuallypoorly perfused (Fig. 1). In those with central vascularization,one would expect the opposite. Hence, the penetration of bloodborne substances should follow the same pattern. In reality, atumor may consist of many territories, each exhibiting one orthe other of these two types of idealized vascular patterns.
Microscopically, the tumor vasculature is highly heterogeneous and does not conform to the standard normal vascularorganization (i.e., artery to arteriole to capillaries to postcapil-lary venule to venule to vein). Based on their ultrastructure, thetumor vessels can be classified into nine categories: (a) arteriesand arterioles; (b) nonfenestrated capillaries; (c) fenestratedcapillaries; (d) discontinuous capillaries (sinusoids); (e) bloodchannels without endothelial lining; (/) capillary sprouts; (g)postcapillary venules (giant capillaries); (h) venules and veins;and (/) arteriovenous anastomoses (shunts) (7). Note that exceptfor vessels of classes e and /, the remaining vessel types arestructurally similar to those found in a normal tissue. Thevessels of classes e and / are found in healing (granulation)tissue. A key difference between normal and tumor vessels isthat the latter are dilated, saccular, and tortuous and maycontain tumor cells within the endothelial lining of the vesselwall (7). In addition, unlike a normal tissue with a fixed routebetween arterial and venous sides, a tumor may have bloodflowing from one venule to another via vessels of classes bthrough g, or directly via an arteriovenous shunt. Furthermore,due to the peculiar nature of the vasculature, the organization
814s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

TUMOR PHYSIOLOGY AND ANTIBODY DELIVERY
Diffusion
t INecrotic Semi-Region Necrotic
Region
Convection
Well VoscularizedRegion
Fig. 1. Schematic of a tumor showing well vascularized periphery; semine-crotic, intermediate zone; and an avascular. necrotic central region. Low interstitial pressure in the periphery permits adequate extravasation of fluid and macro-molecules. These macromolecules move towards the center by the slow processof diffusion, which is further retarded by extravascular binding. In addition,interstitial fluid oozing out from tumor carries macromolecules with it by convection into the normal tissue.
of vessels may be different from one location to another andfrom one time to the next. As a result, one would expectdifferent routes for blood flow in the well perfused advancingzone, seminecrotic zone, and necrotic zone (Fig. 1).
Following the pioneering studies of Algire and Chalkley (8),several investigators have measured morphometric parametersof vessels in thin, two-dimensional tumors grown in transparentwindows. The pioneering work of Cullino and Grantham (9)led to similar studies in three-dimensional experimental andhuman tumors (for review, see Ref. 7). The vascular space intumors varies from 1 to 20% depending upon the tumor type,weight, and method of measurement. Studies in two-dimensional tumors show that vascular volume, length, and surfacearea increase during the early stages of growth and then decrease; this behavior correlates with the onset of necrosis. Thefrequency of large diameter vessels increases in the later stagesof growth. Most quantitative studies in three-dimensional tumors miss the early growth period of increase in vascularvolume, length, and surface area. While studies of later stagesof growth show an increase in the intercapillary distance and adecrease in vessel length and surface area, the results on vascularvolume are inconclusive. Some studies show that the fractionalvascular volume of tumors remains fairly constant duringgrowth (suggesting an increase in the number of blood vesselswith sluggish flow), while others show that the fractional vascular volume decreases as a tumor grows (in agreement withthe observation that tumor perfusion rate decreases as a tumorgrows) (for a review, see Ref. 7). Possible reasons for thisdiscrepancy include errors associated with different measurement techniques as well as presence of arteriovenous shuntsand blood vessels with stagnant blood in them. Whether thevascular volume decreases or not, a reduction in vascular surfacearea would lead to a reduction in the transvascular exchange ofmolecules. In addition, an increase in the intercapillary distancewould require the molecules to traverse longer distances in theinterstitium to reach all regions of a tumor.
Blood Flow Rate. Most investigators have measured localblood flow rate of tumors based on uptake or clearance of a
tracer from a single or a limited number of regions of the tumor.Due to noticeable spatial and temporal heterogeneity in tumorblood supply, these values may not be representative of thewhole tumor. A limited number of studies, in which the bloodflow rate of the whole tumor has been measured, shows thatthe average perfusion rate of carcinomas is less than that of thehost tissue or the tissue of origin. Sarcomas and lymphomashave higher perfusion rates than carcinomas (for a review, seeRef. 10). In general, as tumors grow larger, they may developnecrotic foci, and as a result, the average perfusion rate decreases with tumor size (10). Note that even in these largenecrotic tumors, antibody would be delivered in the well perfused regions.
Since the seminal work of Ide et al.(\\ ), several investigatorshave examined the microscopic flow heterogeneities of tumorsgrown in transparent windows. Blood flow in tumor vessels hasbeen found to be intermittent. There are random periods offlow reduction and stasis followed by resumption of flow,sometimes in the opposite direction (12,13). These fluctuationsmay result from (a) vasomotor activity of the host arterioles;(b) respiratory or cardiac cycle; (c) passage of RBC, WBC, orcancer cells in a vessel; (d) low perfusion pressures in tumorvessels, and/or (e) elevated interstitial pressure in tumors (forreview, see Ref. 7).
Quantitative studies on the macroscopic spatial heterogeneities in the tumor perfusion rate as a function of tumor growth(size) are limited. Based on perfusion rates four regions can berecognized in a tumor: (a) an avascular, necrotic region; (b) aseminecrotic region; (c) a stabilized microcirculation region;and (d) an advancing front. In a rhabdomyosarcoma grown inthe transparent chamber in a rat, the widths of the stabilizedregion and the advancing front were found to remain constant,while the widths of the necrotic and the seminecrotic zonesincreased with tumor growth. In addition, the perfusion rate inthe tumor periphery (i.e., the stabilized and advancing zones)was found to be higher than that in the surrounding normaltissue (12). Intratumor blood flow distributions in spontaneousanimal and human tumors are now being investigated usingnuclear magnetic resonance and positron emission tomography.While limited, these results are in concert with the transplantedtumor studies: blood flow rates in necrotic/seminecrotic regionsof tumors are low, while those in nonnecrotic regions arevariable and substantially higher than in surrounding/contra-lateral host normal tissues (14, 15). As a result of these spatialand temporal heterogeneities in blood supply coupled withvariations in the vascular morphology at both macroscopic andmicroscopic levels, it is not surprising that the spatial distribution of macromolecules in tumors is heterogeneous and theaverage uptake decreases with an increase in tumor weight.
Transport across Microvascular Wall
Once a blood-borne molecule has reached an exchange vessel,its extravasation, Js (g/s), occurs by diffusion and convectionand, to some extent, by transcytosis. Diffusion is proportionalto the surface area, 5 (cm2), of the exchange vessel and the
difference between the plasma and interstitial concentrations(Cp —¿�C¡;g/ml). Convection is proportional to the rate of fluid
leakage, JF (ml/s), from the vessel. Jf, in turn, is proportionalto S and the difference between the vascular and interstitialhydrostatis pressures (p,, —¿�p¡,mm Hg) minus the differencebetween the vascular and interstitial osmotic pressures (w,.—¿�TT¡,mm Hg). The proportionality constant which relates transluminal diffusive flux to concentration gradients (C, —¿�C,) is
815s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

TUMOR PHYSIOLOGY AND ANTIBODY DELIVERY
Pxicrcm/sec
PxlO"
cm/sec
140120100
80
604020
0
140120100
80
6040
20
0
Normol Tissue
n=IO n>8
Tumor Tissue
II I
n=IO n=9 n=9 n=ll n=8 n=ll n=8
Control Saline '—Glucose—' LGaiactose^ '•Hyper02 20 02 20 43°
g/kg g/kg
50*
Fig. 2. Effective microvascular permeability coefficient (P) of M, 150,000dextran in normal (mature granulation) and neoplastic (VX2 carcinoma) tissuesunder various conditions: control; following saline (1 ml/kg body weight) injection: following glucose injections; following galactose injections; and followinghyperthermia for l h (37) (mean ±SD; n = number of measurements). (FromRef. 8; reproduced with permission.)
referred to as the vascular permeability, P (cm/s), and theconstant which relates fluid leakage to pressure gradients isreferred to as the hydraulic conductivity, Lp (cm/mm Hg-s).The effectiveness of the transluminal osmotic pressure difference in producing fluid movement across a vessel wall is characterized by the osmotic reflection coefficient, a; a is close to 1for a macromolecule and close to zero for a small molecule(16). Thus, transport of a molecule across normal or tumorvessels is governed by three transport parameters, P, Lp, and <r;the surface area for exchange, 5; and the transvascular concentration and pressure gradients.
Transvascular Transport Parameters. For a macromoleculeof specified size, charge, configuration, and binding constants,the transport parameters depend upon the physiological properties of the vessel wall (e.g., wall structure, charge). Ultrastructural studies of animal and human tumors have shown thattumor vessels have wide interendothelial junctions, a largenumber of fenestrae and transendothelial channels formed byvesicles, and discontinuous or absent basement membrane (16).These characteristics of tumor vessels suggest that they shouldhave relatively high P and Lp. As a matter of fact, various tissueuptake studies have found vascular permeability of tumors tobe significantly higher than that of skin or muscle (Fig. 2; for areview, see Ref. 16). If tumor vessels are indeed "leakier" to
fluid and macromolecules compared to several normal tissues,what leads to their poor extravasation? As discussed below,tumors contain regions of high interstitial pressure, whichlowers the fluid extravasation. Since the transvascular transportof macromolecules under normal conditions occurs primarilyby convection (16), a decrease in fluid extravasation would leadto a decrease in extravasation of macromolecules (17, 18).2
Furthermore, the average vascular surface area decreases withtumor growth; hence one would expect reduced transvascular
Large Tumor
CentralRegion(Tumor)
MiddleRegion(Tumor)
OuterRegion(Tumor)
SurroundingTissue
(Normal)
Fig. 3. Interstitial pressure gradients in a small versus a large tumor (22).3Note that the tumor pressure increases with growth while the pressure in thesurrounding normal tissue remains constant. Elevated pressure in the centralregion retards the extravasation of fluid and macromolecules. In addition thepressure drop from the center to the periphery leads to an experimentallyverifiable, radially outward fluid flow.
exchange in large tumors compared to smaller tumors (17).2
Transvascular Pressure Gradients. Decreased p,. and/or increased/»,in tumors has been indirectly demonstrated by severalinvestigators working with tumors grown in transparent chambers. By raising venous pressure in the chamber or by looseningthe chamber, blood flow can be restored in ischemic/necrotictumor areas. Direct measurements in sandwich tumors or inthe superficial layer of three-dimensional tumors have shownthat on the arterial side vascular pressure does not differ significantly between nontumor and tumor vessels, whereas venouspressures may be lower in tumor vessels compared to those innormal vessels (for a review, see Ref. 7).
Since the initial work of Young et al. (19), several investigators have shown that p¡in tumors is significantly higher thanin normal tissues (for a review, see Ref. 20). Further, as thetumor grows, p¡rises up to 30 mm Hg, presumably due to theproliferation of tumor cells in a confined space and the absenceof functioning lymphatic vessels (5, 20). This increase in/»,alsocorrelates with a reduction in tumor blood flow and the development of necrosis in a growing tumor (20). Investigations ofintratumor pressure gradients show that the interstitial pressureis higher in the center of a tumor and it approaches normalphysiological pressure towards the periphery [Fig. 3 (20-22)3].
In normal tissues TT,.and TT,are approximately 20-25 and 5-15 mm Hg, respectively (17, 18). Although there are no directmeasurements of ir¡in tumors, based on high vascular permeability and high interstitial diffusion coefficient in tumors, onewould expect higher concentration of endogenous plasma proteins in the tumor interstitium than in normal interstitium.This hypothesis is supported by the data in the literature (23).As a result, ir, in tumors may be higher than that in normaltissues, and may lead to reduced osmotic flow.
As shown in Fig. 3, p, in tumors is close to zero in theperiphery, therefore the filtration of fluid from vessels, JF,would be close to normal. However, as one moves towards thecenter of the tumor, the increase in p¡would reduce the extravasation of fluid, Jr. As stated earlier, convective transport of amacromolecule is proportional to Jr\ therefore, the rate ofextravasation of a blood-borne macromolecule would be negligible in the center of a tumor (17, 18). Since transvascular
2 L. T. Baxter and R. K. Jain. Transport of fluid and macromolecules in * M. Misiewicz and R. K. Jain. Interstitial pressure gradients in VX2 carci-
tumors. II. Role of heterogeneous perfusion, manuscript in preparation. noma, manuscript in preparation.
816s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

TL'MOR PHYSIOLOGY AND ANTIBODY DELIVERY
transport by diffusion is negligible for a macromolecule to beginwith, macromolecular extravasation would be very small in thehigh interstitial pressure regions of a tumor. Since high pressureregions usually coincide with regions of poor perfusion rate andlower vessel surface area, leakage of blood borne macromole-cules from vessels would be further restricted.2
Transport through Interstitial Space
Once a macromolecule has extravasated, its movement occursby diffusion and convection through the interstitial space. Diffusion is proportional to the concentration gradient in theinterstitium, and convection is proportional to the interstitialfluid velocity, u¡(cm/s). The latter, in turn, is proportional tothe pressure gradient in the interstitium. The proportionalityconstant which relates diffusive flux to the concentration gradient is referred to as the interstitial diffusion coefficient, D(cm2/s), and the constant which relates u¡to the pressure
gradient is referred to as the interstitial hydraulic conductivity,A"(cm2/mm Hg-s) (for a review, see Ref. 20). Values of transport
coefficients D and K are determined by the structure and composition of the interstitial compartment as well as the physico-chemical properties of the solute molecule. Larger values ofthese parameters lead to less hindered movement of fluid andmacromolecules through the interstitium. Similarly, large values of interstitial pressure and concentration gradients lead tolarge convective and diffusive fluxes.
Interstitial Transport Coefficients. The interstitial space intumors, in general, is very large compared to that in host normaltissues (for a review, see Ref. 20). Similar to normal tissues, theinterstitial space of tumors is composed predominantly of acollagen and elastic fiber network. Interdispersed within thiscross-linked structure are the interstitial fluid and macromolecular constituents (polysaccharides) which form a hydrophilicgel. While collagen and elastin impart structural integrity to atissue, the polysaccharides (glycosaminoglycan and proteogly-cans) are presumably responsible for the resistance to fluid andmacromolecular motion in the interstitium. In several tumorsstudied to date, collagen content of tumors is higher than thatof the host normal tissue. On the other hand, hyaluronate andproteoglycans are, in general, present in lower concentrationsin tumors than in the host normal tissue (for a review, see Ref.20). The lower concentration of these polysaccharide moleculesis presumably due to increased activity of lytic enzymes, e.g.,hyaluronidase, in the tumor interstitial fluid (for a review, seeRef. 5).
The large interstitial space and low concentrations of polysaccharides suggest that values of ATand D should be relativelyhigh in tumors. As a matter of fact, the data on hydraulicconductivity of hepatoma 5123 (24) and the data on effectivediffusion coefficients of various macromolecules in VX2 carcinoma (Fig. 4) (25, 26)4 support this hypothesis. An order of
magnitude higher values of D and K in tumors comparedcompared to several normal tissues should favor movement ofmacromolecules in the tumor interstitium. Then, why do theexogenously injected macromolecules not distribute uniformlyin tumors? As discussed below, there are two reasons for thisapparent paradox.
Large Distances in the Interstitium. The time constant, TI>,for a molecule, with diffusion coefficient D, to move by diffusionacross distance Cis approximately C2/4D. For diffusion of IgG
in tumors (using D from Fig. 4), TDis of the order of l h for
100
10
ox Ol
0.01
O.C
W T Na a m Dextran
o e •¿�Albumin
O * » Ig G
i
10,000 100,000 200,000
Molecular Weight
Fig. 4. Molecular weight dependence of effective diffusion coefficients, Ö,ofdextrans (25, 26), albumin (25). and IgG4 in water (HO. tumor (7"), and anontumor tissue (A'). Note that transport is hindered in both tissues compared to
water. Despite higher values of I) in tumors compared to in nontumor tissues.macromolecules do not reach uniform concentration in a large tumor for a longtime due to large diffusion distances.
100 ¡imdistance, ~2 days for 1 mm distance, and ~7-8 monthsfor 1 cm distance (17). These numbers are consistent with thedata on the penetration of MAbs in spheroids. Now consider ahypothetical tumor which is uniformly perfused, has nearly zeroPi, and has exchange vessels ~200 pm apart. In such a tumor,IgG would reach uniform concentration in ~1 h postinjectionprovided the plasma concentration remains constant. In a normal tissue with the value of D lower by an order of magnitude(Fig. 4), it will take —¿�10h to reach uniform concentration.
Now consider a more realistic situation, where the tumorvessels are ~200 ^m apart and uniformly perfused, but p¡hasincreased in the center so that fluid extravasation, and, hence,convective transport of macromolecules across vessels hasstopped. In such a case the only way macromolecules extravasate in the center is by the slow process of diffusion acrossvessel walls. Also they can reach the center from the periphery(where p, is near zero) by interstitial diffusion. As stated earlier,if the distance between the center and periphery is ~1 mm, itwould take days for them to get there and if it is ~1 cm, itwould take months (17). If due to elevated p, and cellularproliferation, the central vessels have collapsed completely,then there is no delivery of macromolecules by blood flow tothe necrotic center (7). In such a case, there are no moleculesavailable for extravasation by diffusion across the vessel wall,and consequently the central concentration would be evenlower!2
Thus far the interstitial movement of molecules which do notbind to any extravascular sites or undergo metabolism has beendiscussed. It is well known that the binding reaction lowers theapparent diffusion rate of molecules (for a review, see Ref. 27).Therefore, although higher affinity of antibody to antigen significantly increases the concentration of the antibody proximalto the vessel, it retards their movement to distal locations inthe interstitium (28, 29). 5 The metabolism of antibodies in
normal and tumor tissues is poorly understood. However, theproducts of metabolism are usually smaller in molecular weightand hence may be cleared relatively rapidly.5
4 M. A. Clauss and R. K. Jain. Interstitial diffusion coefficients of IgG in *L. T. Baxter and R. K. Jain. Transport of fluid and macromolecules in
normal and neoplastic tissues, submitted for publication. tumors. III. Role of binding and metabolism, manuscript in preparation.
817s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

TUMOR PHYSIOLOGY AND ANTIBODY DELIVERY
Interstitial Fluid Loss from Periphery of the Tumor. It is awell known law of physics that fluid flows from a high to a lowpressure region. As discussed earlier, p¡is high in the center oftumors and low in the periphery. Therefore one would expectinterstitial fluid motion from the center of a tumor towards itsperiphery from where it will ooze out into the surroundingnormal tissue. Using a tissue isolated tumor preparation. Butleret al. (30) measured this fluid loss to be 0.14-0.22 ml/h/g tissue
in four different rat mammary carcinomas. This fluid leakageleads to a radially outward interstitial fluid velocity of 0.1-0.2pm/s at the periphery of a 1-cm "tissue isolated" tumor (16).
[The radially outward velocity is an order of magnitude lowerin a tumor grown in the s.c. tissue or muscle (17).] A macro-molecule at the tumor periphery must overcome this outwardconvection to penetrate into the tumor by diffusion. The relativecontribution of this mechanism of heterogeneous distributionof antibodies in tumors is, however, smaller than the contribution of heterogeneous extravasation due to elevated pressureand necrosis (17, 18).2
Conclusions, Implications, and Future Perspective
Antibodies linked to radionuclides, drugs, toxins, enzymes,growth factors, and effector antibodies offer a promising approach to the treatment of solid tumors. Their strengths includetheir high degree of specificity for tumor associated antigensand the fact that exchange vessels and interstitium of tumorsare more "leaky" to macromolecules than those of several
normal tissues. Their clinical limitation, however, results fromtheir inadequate uptake and non-optimal distribution in tumors.The physiological factors which contribute to the poor deliveryin tumors include heterogeneous blood supply, interstitial hypertension, and relatively long transport distances in the interstitium (Table 1). How can these physiological barriers beovercome?
Several physical (e.g., radiation, heat) and chemical (e.g.,vasoactive drugs) agents may lead to an increase in tumor bloodflow (7, 10, 31). A key problem with this approach is that theincrease in blood flow is short-lived and usually confined towell vascularized regions. Increased delivery of macromoleculesto well perfused regions would not solve the maldistributionproblem.
The second approach may be based on lowering the tumorinterstitial pressure. The interstitial hypertension results presumably from interstitial fluid accumulation which, in turn,results from the lack of functioning lymphatics in tumors (5,17, 20). Since A:is a key determinant of interstitial fluid motion,any method which increases K may lower pressure. Use of lyticenzymes (e.g., hyaluronidase) to increase K is one possibility(24). An alternate strategy would be to lower the tumor celldensity without destroying the vasculature. Whether fraction-
Table1 Physiologicaladvantagesandproblemsin thedeliveryofmacromoleculesto tumors
AdvantagesRelatively high degree of specificity of antibodies for tumor associated anti
gensRelatively large vascular permeability, interstitial diffusion coefficient, and
hydraulic conductivity
ProblemsHeterogeneous blood supplyElevated interstitial pressureFluid loss from peripheryLarge distances in the interstitiumLarge affinity and heterogeneous bindingMetabolism
ated radiation lowers /?, in tumors via this mechanism remainsa plausible hypothesis to be tested (16, 17). The use of anosmotic agent (e.g, mannitol) may increase TT,.and hence increase antibody penetration (32). However, this increase maybe too short-lived to yield practical results.
The third approach may be based on increasing the interstitialtransport rate of molecules. Use of cocktails of antibodies wouldnot overcome this problem because each antibody must crossthe same physiological barriers. One method of accomplishingthis goal would be to use lower molecular weight agents, e.g.,antibody fragments F(ab')2 and Fab. While the fragments have
higher values of P and D compared to the intact antibody andhence penetrate deeper into tumors, there are two physiologicalproblems associated with their use; they are eliminated morerapidly from blood, and their uptake into normal tissues is alsoincreased. The elimination problem can be overcome by repeated or continuous injections of high doses of nonimmuno-genic fragments of chimeric or human antibodies. However, asthe molecular weight is lowered further, the normal tissuetoxicity problem may become more pronounced similar to thatencountered with conventional anticancer agents (M, < 2,000)(33, 34). Some of the problems with the systemic toxicity maybe overcome by local injection (e.g., intraarterial, interstitial) atthe cost of not being able to reach the distant métastases.If thetoxicity to normal tissues could be overcome, combination oflocal and systemic injections would be more effective. Similarly,delivering low molecular weight agents (e.g., drug, toxin, enzyme, hormone) linked to monoclonal antibodies and releasingthem once they have extravasated or entered cells seems reasonable. However, once a small molecule is uncoupled from theantibody it may diffuse back into a nearby blood vessel and maybe rapidly eliminated. To what extent bifunctional antibodiesretard the clearance of small molecules (e.g., individually infused chelated isotopes) from both normal and tumor tissuesremains to be tested. Finally, increasing the number of antigenicsites using biological response modifiers such as interferon (35)would increase the concentration of antibody near the bloodvessels but would not increase the depth of penetration. Oneway of overcoming some of these problems is to use radioiso-topes with large tumor dose deposition and large depths ofpenetration; however, toxicity to normal tissues may become alimiting factor. Protecting bone marrow using growth factors(e.g., interleukin 1, colony stimulating factors) or bone marrowtransplant may alleviate the normal tissue toxicity problem.Another method is to combine antibody treatment with othermodalities (e.g., radiation sensitizers, low molecular weightcytotoxic drugs to synchronize cell cycle) depending upon thetumor type.
In contrast, the physiological barriers discussed in this articlemay not be a problem for: (a) radioimmunodetection; (b) treatment of leukemia, lymphomas, and small tumors (e.g., micro-metastases) in which the interstitial pressure is low and diffusion distances are small; (c) treatment of adequately perfused,low pressure regions of large tumors (36); and (d) treatmentwith antibodies directed against the tumor endothelial cells ormicroenvironment of the subendothelial matrix. These barriersmay also not pose any problems for treatment with a moleculewhich has nearly 100% specificity for cancer cells. Until suchmolecules are developed, methods are urgently needed to overcome these physiological barriers in tumors. It is likely that animproved understanding of tumor physiology will help in developing these strategies. It is also likely that such physiologicalinsight would be a prerequisite to the optimal development ofalternative therapeutic strategies for control of established ma-
818s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

TUMOR PHYSIOLOGY AND ANTIBODY DELIVERY
lignancies including the development of anti-angiogenic modalities as well as the delivery of killer lymphocytes (e.g.,lymphokine activated killer cells, tumor infiltrating lymphocytes) to the tumor microenvironment.
Acknowledgments
I thank my former and current students for their collaboration; D.Dlugokecki for typing this manuscript; and the Journal of the NationalCancer Institute for permission to reproduce the material from theoriginal, slightly different, article published in April 1989.
References
1. Dykes, P. W., Bradwell, A. R., Chapman, C. E., and Vaughan, A. T. M.Radioimmunotherapy of cancer: clinical studies and limiting factors. CancerTreat. Rev., 14: 87-106, 1987.
2. Sands, H., and Jones, P. K. Physiology of monoclonal antibody accretion bytumors. In: D. M. Goldenberg (ed.). Cancer Imaging with RadioactiveAntibodies. Boston: Martinus Nijhoff, in press, 1990.
3. Jain, R. K., Weissbrod, J., and Wei, J. Mass transfer in tumors: characterization and applications in chemotherapy. Adv. Cancer Res.. 33: 251-310,1980.
4. Gerlowski, L. E., and Jain, R. K. Physiologically-based pharmacokinetics:Principles and applications. J. Pharm. Sci., 72: 1103-1127, 1983.
5. Cullino, P. M. Extracellular compartments of solid tumors. In: F. F. Becker(ed.), Cancer, pp. 327-354. New York: Plenum Publishing Corporation,1975.
6. Folkman, J. Tumor angiogenesis. Adv. Cancer Res., 43: 175-201, 1985.7. Jain, R. K. Determinants of tumor blood flow: a review. Cancer Res., 48:
2641-2658, 1988.8. Algire, G. H., and Chalkley, H. W. Vascular reactions of normal and
malignant tissues in vivo. I. Vascular reactions of mice to wounds and tonormal and neoplastic transplants. J. Nati. Cancer Inst., 6: 73-85, 1945.
9. Cullino, P. M., and Grantham, F. H. The vascular space of growing tumors.Cancer Res., 24: 1727-1732, 1964.
10. Jain, R. K., and Ward-Hartley, K. Tumor blood flow—characterization,modifications, and role in hyperthermia. IEEE Tr. Sonics Ultrasonics, SU-31: 504-526, 1984.
11. Ide, A. G., Baker, N. H., and Warren, S. L. Vascularization of the Brown-Pearce rabbit epithelioma transplant as seen in the transparent ear chamber.Am. J. Roentgenol., 41: 891-899, 1939.
12. Endrich, B., Reinhold, H. A., Gross, J. F., and Intaglietta, M. Tissueperfusion inhomogeneity during early tumor growth in rats. J. Nati. CancerInst., 62: 387-395, 1979.
13. Dudar, T. E., and Jain, R. K. Differential responses of normal and tumormicrocirculation to hyperthermia. Cancer Res., 44: 605-612, 1984.
14. Straw, J., Hart, M., Klubes, P., Zaharko, D., and Dedrick. R. L. Distributionof anticancer agents in spontaneous animal tumors. I. Regional blood flowand methotrexate distribution in canine lymphosarcoma. J. Nati. CancerInst., 52: 1327-1331, 1974.
15. Beaney, R. P., Lammertsma, A. A., Jones, T., McKenzie, C. G., and Hainan,K. E. In vivo measurements of regional blood flow, oxygen utilization andblood volume in patients with carcinoma of the breast using positron tomography. Lancet, /: 131-133, 1984.
16. Jain. R. K. Transport of molecules across tumor vasculature. Cancer Metastasis Rev., 6: 559-594, 1987.
17. Jain. R. K., and Baxter, L. T. Mechanisms of heterogeneous distribution ofmonoclonal antibodies and other macromolecules in tumors: significance ofelevated interstitial pressure. Cancer Res.. 48: 7022-7032. 1988.
18. Baxter, L. T., and Jain. R. K. Transport of fluid and macromolecules intumors. I. Role of interstitial pressure and convection. Microvasc. Res., 37:77-104, 1989.
19. Young, J. S., Lumsden, C. E.. and Stalker, A. L. The significance of the"tissue pressure" of normal testicular and of neoplastic (Brown-Pearce carcinoma) tissue in the rabbit. J. Pathol. Bacteriol., 62: 313-333, 1950.
20. Jain, R. K. Transport of molecules in the tumor interstitium: a review. CancerRes., 47:3039-3051, 1987.
21. Wiig, H., Tveit, E. Hultborn. R.. Reed, R. K.. and Weiss, L. Interstitial fluidpressure in DMBA-induced rat mammary tumors. Scand. J. Clin. Lab.Invest., 42: 159-164, 1982.
22. Misiewicz, M. Microvascular and interstitial pressures in normal and neoplastic tissues. M. S. Thesis, Carnegie Mellon University. 1986.
23. Sylven. B., and Bois, I. Protein content and enzymatic assays of interstitialfluid from some normal tissues and transplanted mouse tumors. Cancer Res..20:831-835, 1960.
24. Swabb, E. A., Wei, J., and Cullino, P. M. Diffusion and convection in normaland neoplastic tissues. Cancer Res., 34: 2814-2822, 1974.
25. Nugent, L. J., and Jain, R. K. Extravascular diffusion in normal and neoplastic tissues. Cancer Res., 44: 238-244, 1984.
26. Gerlowski, L. E., and Jain, R. K. Microvascular permeability of normal andneoplastic tissues. Microvasc. Res., 31: 288-305. 1986.
27. Astarita, G. Mass Transfer with Chemical Reactions. Amsterdam: Elsevier,1967.
28. Weinstein, J. N., Eger, R. R., Covell, D. G., Black, C. D. V.. Mulshine, J.,Carrasquillo, J. A., Larson, S. M., and Keenan, A. M. The pharmacology ofmonoclonal antibodies. Ann. NY Acad. Sci., 507: 199-210, 1987.
29. Dedrick, R. L., and Flessner. M. F. Pharmacokinetic considerations ofmonoclonal antibodies. In: M. Mitchell (ed.). Immunity to Cancer II, pp429-438, 1989.
30. Butler, T. P., Grantham. F. H., and Cullino, P. M. Bulk transfer of fluid inthe interstitial compartment of mammary tumors. Cancer Res., 35: 3084-3088, 1975.
31. Jain, R. K. Tumor blood flow response to heat and pharmacological agents.In: E. M. Fielden. J. F. Fowler. J. H. Hendry. and D. Scott (eds.). RadiationResearch (Proceedings of the Eighth Intl. Congress of Radiation Research).Vol. 2, pp. 813-818. London: Taylor and Francis, 1987.
32. Neuwelt, E. A., Sprecht. H. D., Barnett, R. A., Dahlborg, S. A., Miley, A.,Larson, S. M.. Brown. P.. McKerman. K. F.. Hellström. K. E., and Hellström,I. Increased delivery of tumor specific monoclonal antibodies to brainafter osmotic blood-brain barrier modification in patients with melanomametastatic to central nervous system. Neurosurgery, 20: 885-895, 1987.
33. Jain, R. K.. and Wei, J. Dynamics of drug transport in solid tumors:distributed parameter model. J. Bioeng.. /: 313-330, 1977.
34. Jain, R. K., Wei, J., and Cullino, P. M. Pharmacokinetics of methotrexatein solid tumors. J. Pharmacokinet. Biopharm., 7: 181-194. 1979.
35. Greiner, J. W., Guadagni, F., Noguchi, P., Pestka, S., Colcher, D., Fisher,P. B., and Schlom, J. Recombinant ¡nterferonenhances monoclonal antibody-targeting of carcinoma lesions in vivo. Science (Wash. DC), 235: 895-898, 1987.
36. Sitzman, J. V., Order, S. E., Klein, J. L., Leichner, P. K., Fishman. E. K.,and Smith. G. W. Conversion by new treatment modalities of nonresectableto resectable hepatocellular cancer. J. Clin. Oncol., 5: 1566-1573, 1987.
37. Gerlowski, L. E., and Jain. R. K. Effect of hyperthermia on microvascularpermeability of normal and neoplastic tissues. Int. J. Microcirc. Clin. Exp.,4:336-372, 1985.
38. Jain. R. K. Transport of macromolecules in tumor microcirculation. Biotech.Prog., /: 81-94, 1985.
819s
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

1990;50:814s-819s. Cancer Res Rakesh K. Jain Other Macromolecules in TumorsPhysiological Barriers to Delivery of Monoclonal Antibodies and
Updated version
http://cancerres.aacrjournals.org/content/50/3_Supplement/814s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/50/3_Supplement/814sTo request permission to re-use all or part of this article, use this link
Research. on November 1, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from