PHOSPHATEMIA - Zoovet · Pathophysiology of renal secondary ... PHOSPHATEMIA MANAGEMENT IN THE ......
16
Sponsored by PHOSPHATEMIA MANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE A ROUNDTABLE DISSCUSSION
Transcript of PHOSPHATEMIA - Zoovet · Pathophysiology of renal secondary ... PHOSPHATEMIA MANAGEMENT IN THE ......

Sponsored by
PHOSPHATEMIAMANAGEMENT IN THE TREATMENTOF CHRONIC KIDNEY DISEASE A ROUNDTABLE D ISSCUSS ION

Dr. Jonathan Elliott: Today we willdiscuss an old-fashioned kidneyproblem: disorders of mineral bal-ance and phosphate. One of ourgoals is to build a consensus on theimportance of phosphate and para-thyroid hormone (PTH); we’ll debatewhether phosphate, PTH, or a com-bination of the two is important inkidney disease. A second objective isto provide treatment guidelines forhyperphosphatemia and hyperpara-thyroidism, indicating the quality ofthe evidence supporting the guide-lines. We will also identify areaswhere new research is warranted.____________________________
Pathophysiology of renal secondary
hyperparathyroidism____________________________
Elliott: Let’s begin by consideringthe pathophysiology of secondaryrenal hyperparathyroidism and therole of phosphate. Regulation of theconcentration of calcium and phos-phate in extracellular fluid involvesthe intestines, bones, kidneys, and
the movement of calcium and phos-phate between intracellular andextracellular fluid. The bones’ mas-sive store of bound calcium andphosphate is released or replenishedto protect the animal against a lackor excess of calcium and phosphatein extracellular fluid, includingblood. Hormones regulate this move-ment. When you study a patient’scomplex endocrine system by evalu-ating a blood sample, it’s difficult tounderstand what’s occurring in thisdynamic system—many differentfactors can influence each other(Figure 1, page 4). For example, adecreased ionized calcium concentra-tion and an increased phosphate con-centration in the extracellular fluidstimulate PTH secretion, and PTHincreases the release of calcium andphosphate from the bones. This stim-ulates the kidneys to produce morevitamin D, which increases calciumand phosphate absorption from theintestine. Phosphate and calcium arereleased from the bone to defendagainst hypocalcemia, and along
with PTH and vitamin D, they influ-ence the kidneys, such that calciumis retained and phosphate is excreted.Vitamin D feedback inhibits PTHsynthesis. It also ensures that somenutritional calcium replenishes thatwhich came out of the bone. So PTHand vitamin D together are neededfor calcium to be released from andreplenished into the bones.
Let’s look at the Kidney DiseaseOutcomes Quality Initiative (KDOQI)guidelines in human medicine.KDOQI is an educational initiativeof the National Kidney Foundationin the United States whose aim is toimprove the quality of care ofhuman patients with kidney diseasethrough the development of scientifi-cally rigorous guidelines based on acritical appraisal of the available evi-dence. These guidelines maintainthat phosphate retention occurs earlyin the course of chronic kidney dis-ease, probably during KDOQI stageI (glomerular filtration rate, or GFR,is normal or decreased; less than 90ml/min/1.73 m2) but certainly by
Gregory F. Grauer,DVM, MS, DACVIM
Department of Clinical Sciences
College of Veterinary Medicine
Kansas State UniversityManhattan, Kansas
Herve Lefebvre,DVM, PhD, DECVPT
Department of Clinical Sciences
National Veterinary School
Toulouse, France
Maria Josefa Fernandezdel Palacio, DVM, PhD,DECVIM-CA (cardiology)
Departamento de Medicina y Cirugía Animal
Facultad de VeterinariaUniversidad de MurciaMurcia, Spain
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
ModeratorJonathan Elliott, MA,
Vet MB, PhD, Cert SAC, DECVPT, MRCVS
Department of Veterinary Basic Sciences
Royal Veterinary CollegeUniversity of LondonLondon, England
ParticipantsScott A. Brown, VMD,
PhD, DACVIMDepartment of Small Animal
Medicine and SurgeryCollege of Veterinary MedicineUniversity of GeorgiaAthens, Georgia
Larry D. Cowgill, DVM, PhD, DACVIM
Department of Medicine and Epidemiology
School of Veterinary MedicineUniversity of California-DavisDavis, CaliforniaUniversity of CaliforniaVeterinary Medical CenterSan Diego, California
z2y

z3y
KDOQI stage II (GFR equals 60 to89 ml/min/1.73 m2). This does notmean that the serum phosphateconcentration is elevated at thattime; in fact, the serum phosphateconcentration may actually be low.This phosphate retention is not theonly contributor to hyperparathy-roidism; the PTH concentrationstarts to rise when the GFR is 50%of normal or below. Serum phos-phate concentrations might benormal or even reduced at KDOQIstages I to III (stage III equals GFRof 30 to 59 ml/min/1.73 m2).Whenever there is a reduction inGFR, whole-body phosphate reten-tion is occurring.
Phosphate is filtered and partiallyreabsorbed in the proximal tubule.The only way to excrete more is toreduce the amount that is reabsorbedin the proximal tubule. This is con-trolled by PTH, which reduces thetransport maximum of phosphate inthe proximal tubule and can causeup to 70% of the filtered load toappear in the urine. However, onceGFR becomes limited (less than50% of normal) and dietary phos-phate remains the same, phosphatewill be retained in the body as intakeexceeds the capacity of the kidneysto excrete phosphate. PTH secretionthen becomes maladaptive as itbrings more phosphate out of thebound stores in the bone. Becausethe kidneys cannot excrete thisphosphate, it accumulates in cellsand extracellular fluid. The logicalway we can address this problem
and restore the balance is by re-ducing phosphate intake.
Secondary renal hyperparathy-roidism is an extremely commonfinding in chronic kidney disease;it is evident early in the disease syn-drome. Phosphate retention plays animportant role in its genesis. Evi-dence from human medicine showsthat this phenomenon decreases thequality of life and increases the riskof mortality.
The questions I have are: Is PTHresponsible for this detrimental effect,or is the phosphate overload detri-mental? Perhaps PTH is just a goodindicator of phosphate overload.How important is this syndrome incausing progressive renal injury instages I to III of chronic kidney dis-ease, using the International Renal
Interest Society (IRIS) classification(Table 1, page 5)? And how does thissyndrome relate to other causes ofprogressive renal injury, such ashypertension and proteinuria?
Dr. Larry Cowgill: Is phosphate orPTH the bad guy? We have dealt withthe problem of secondary hyperpara-thyroidism from the human perspec-tive, in which metabolic bone diseaseis one of the major clinical problemsassociated with this syndrome.
In the majority of veterinary pa-tients, I think renal osteodystrophyisn’t clinically manifested enough towarrant therapeutic management. Wemay have to shift our perspective onhyperparathyroidism and hyperphos-phatemia from the human concept towhat is relevant in our patients.
Elliott: Renal osteodystrophydefinitely occurs. If you see theseanimals late enough in the diseaseprocess, you can see it radiographi-cally, which presumably means thatit has occurred for quite some time.
Cowgill: But it generally is not clin-ically manifested.
Dr. Astrid van Dongen: Eventhough practitioners don’t see thesigns, they shouldn’t just forgetabout the problem. We may not seebone-related disease that often inrenal patients, but when we findother evidence of calcium-phosphateimbalance, there is something terri-bly wrong.
A ROUNDTABLE DISCUSSION
Astrid van Dongen, DVM, RNVA (specialist CAinternal medicine)
Department of Internal Medicine
University of UtrechtUtrecht, The Netherlands
Bernhard Gerber, Dr. med. vet., DACVIM,DECVIM-CA
Clinic for Small Animal Internal Medicine
Vetsuisse FacilityUniversity of ZurichZurich, Switzerland
David Polzin, DVM,PhD, DACVIM
Department of Veterinary Clinical Sciences
College of Veterinary Medicine
University of MinnesotaSt. Paul, Minnesota
Secondary renalhyperparathyroidism
is an extremelycommon finding in chronic kidney
disease; it isevident early in thedisease syndrome.
—Dr. Jonathan Elliott

____________________________The role of phosphate
in chronic kidney disease ____________________________
Cowgill: Let’s discuss what clinicalproblems occur in animals with kid-ney disease relative to mineral bal-ance or mineral metabolism.
Elliott: The main issue is how pa-tients excrete enough phosphate tostay in balance when their GFR drops.
Cowgill: If we can’t identify any clin-ical significance to hyperparathyroid-ism in animals with chronic kidneydisease—other than developing bonedisease at a late stage—then maybe wedon’t need to be as concerned about it.
Elliott: The problem is that the twoare intrinsically linked. In my
experience, if you change phosphatelevels, you change PTH levels.
Dr. David Polzin: I suspect there isa big difference there. You can havephosphate levels that, while withinthe normal range, are at the high endof the range, with PTH valuesremaining quite elevated. I think itreally matters which one we focus onto influence the clinical outcome. Ifwe base therapy on PTH, we have toprove that there’s a link between theclinical outcome and PTH. We knowthe clinical outcome is linked tophosphate control.
Elliott: So the practical approach isto control phosphate. The difficultconcept to sell to practitioners is atwhat phosphate concentration they
will see benefits. Do we need moreclinical studies?
Dr. Scott Brown: Recent clinicalstudies from Minnesota have con-firmed the applicability of laboratorystudies of models to animals withspontaneous kidney disease.1,2
Further, we know that structural orfunctional progression in the remnantkidney model is directly related toserum phosphate concentration indogs and cats.3-4 It’s thus reasonableto argue that we should restrict phos-phate and/or provide an intestinalphosphate binder to control theserum phosphate concentration. Andthere is enough evidence in otherspecies to suggest that “under con-trol” means a serum phosphate con-centration well within the normalrange or even in the bottom half ofthe normal range.
Elliott: Our experience in cats hasbeen if we can control phosphate, wecan control PTH. To summarize,hyperphosphatemia related to chronickidney disease warrants treatment andcan lead to secondary renal hyperpara-thyroidism through PTH stimulation.
van Dongen: Practitioners shouldmeasure phosphate levels and adjusttheir therapy accordingly. But in anideal situation, PTH and vitamin Dlevels should also be checked inaddition to phosphate.
Dr. Maria Josefa Fernandez del Palacio: I agree with Dr. vanDongen that for practitioners, it wouldbe more practical to measure phos-phate levels first because this parame-ter is usually included in the biochem-ical panels. As a second step, PTHmeasurements would be desirable.
Dr. Greg Grauer: On the scale of1 to 10, the quality of evidence forcontrolling hyperphosphatemia in
z4y
MANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
1. This schematic diagram shows the sequence of events following a decrease in plas-ma ionized calcium. For simplicity, this schematic only considers calcium and doesnot make reference to phosphate.
1. A fall in extracellular fluid ionized calcium is sensed by calcium-sensing recep-tors at the level of the parathyroid gland.
2. PTH is secreted into the blood.3. PTH acts on the bone and kidney via active vitamin D3 (1,25 D3) on the intestine
to raise extracellular fluid ionized calcium.4. The increase in ionized calcium and 1,25 D3 concentrations act on the parathy-
roid gland to inhibit PTH secretion.5. Raised 1,25 D3, over a longer time scale, allows the calcium coming into the
body from the intestines to replenish the bone stores with calcium.
Figure 1: Regulation of the endocrine system
PHOSPHATEMIA
1
2
3
44
5

chronic kidney disease is close to 10.We don’t have nearly the same levelof evidence for controlling PTH.
Cowgill: Despite this, I have a con-cern about this broad range of earlykidney disease occurring with a nor-mal serum phosphate concentration.The only indication that phosphatemetabolism is disordered at that dis-ease stage is probably the PTH,which could identify the need forphosphate restriction at an earlierdisease stage than the serum phos-phate concentration. I am concernedthat we are not seeing elevations inthe serum phosphate concentrationuntil creatinine levels are 3.5 to 4mg/dl (310 to 360 µmol/l). Phosphatemanagement could be beneficial atan earlier stage, and practitionerswould miss this opportunity if theyjust focused on serum phosphate
concentration. Monitoring serumPTH levels at IRIS stage II andprobably early stage III would likelybe beneficial.
Elliott: My concern is that practi-tioners tend to think that if phos-phate isn’t elevated, they don’t needto restrict it. They might feed a renaldiet anyway just because the creati-nine is elevated. They may misun-derstand the reason why that bene-fits the individual animal—they maythink it helps because of decreasedprotein levels but the decreasedphosphate levels in the diet alsohelps. Another concern is that asphosphate starts to increase, theyshould target the lower end of thereference range. Practitioners needto recognize that a phosphate in thenormal range could still be abnormalin renal patients.
Cowgill: Given the lack of a strongcorrelation between hyperparathy-roidism and clinical signs relative toanimals with kidney disease, could wesay that—at a minimum—PTH servesas a surrogate marker for dysregulationof mineral balance in the face of a nor-mal serum phosphate concentration?
Dr. Herve Lefebvre: That’s a goodpoint. If the serum phosphate con-centration is normal in animals withchronic kidney disease, I’d recom-mend assessing the PTH to confirmhyperparathyroidism.
Grauer: Clinical experience suggeststhat PTH levels can be elevated inearly chronic kidney disease, prior tothe onset of hyperphosphatemia. Butdo we have data showing that treat-ment of hyperparathyroidism at thisstage affects patient outcome?
z5y
A ROUNDTABLE DISCUSSION
Stage Description GFR IRIS stage* Plasma creatinine (KDOQI) (ml/min/1.73 m2) (µmol/l)**
I Kidney damage >90 I Feline: <140with normal or Canine: <125increased GFR (<1.6 mg/dl)
II Kidney damage 60 to 89 I to early stage II Feline: 140 to 249with mild Canine: 125 to 179decreased (1.6 to 2.8 mg/dl)GFR
III Moderately 30 to 59 Later stage II and stage III Feline: 180 to 439decreased GFR Canine: 140 to 439
(2.9 to 5.0 mg/dl)
IV Severe reduction 15 to 29 Stage IV Feline and canine: >440in GFR (>5.0 mg/dl)
V Kidney failure <15 (or dialysis) Late stage IV Not defined but >440 for feline and canine(>5.0 mg/dl)
* The IRIS classification is based on plasma creatinine and the limitations of this are recognized, particularly in precise definition of kidney function in stages I to III.
** The creatinine concentration values stated above are a guide based on expert opinion.
Table 1: Classification of kidney disease in KDOQI vs IRIS stages
Cowgill: We have lots of caninedata showing that in the early stageof disease, treating the phosphateimbalance with dietary reductioncorrects the hyperparathyroidism.5,6
So hyperparathyroidism can serve asa sensitive marker that the mineralbalance is abnormal.
Brown: There is certainly correla-tive evidence that PTH may bedetrimental, but the confoundingproblem is that the PTH level is alsodirectly correlated to the degree ofphosphate imbalance. If we makeclinically relevant recommendations,the logical target is the serumphosphate concentration. To me, the first step is targeting the phos-phate level with appropriate dietary
maneuvers, rather than recommend-ing an ancillary test.
Polzin: I don’t think we have proofof a cause and effect relationshipbetween PTH levels and progressionof kidney disease, but we do betweenphosphate intake and progression.Another issue is that I’m not sure it’spossible to identify the phosphatelevel within stage II, for example,that reliably normalizes PTH levels.If we answer that question, it wouldbe easier to focus on the phosphatelevel. Then you get into the issue thatis confronting the IRIS—we are sug-gesting that phosphate should bebelow a number that is well withinthe normal range. We are essentiallychanging the normal range in the
renal patient, which practitioners canfind confusing.
Grauer: Well, we’ve recently changedwhat we think is normal and abnormalfor hypertension and proteinuria. May-be we need to do the same for creati-nine and phosphate concentrations.
Polzin: The implication might bethat if you treat a patient appropriate-ly over an extended period of timeyou could, in fact, just monitor theserum phosphate concentration.
Elliott: Yes, as long as you keep thephosphate in the optimal range.
Grauer: So should practitionersinitiate dietary phosphate restriction
z6y
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
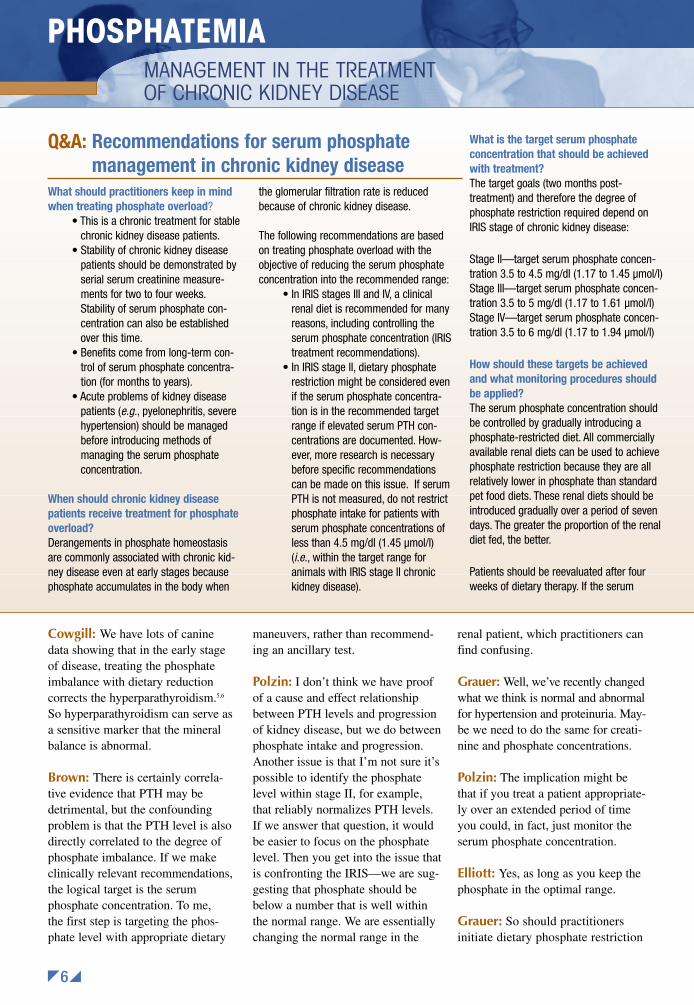
What should practitioners keep in mindwhen treating phosphate overload?
• This is a chronic treatment for stablechronic kidney disease patients.
• Stability of chronic kidney diseasepatients should be demonstrated byserial serum creatinine measure-ments for two to four weeks.Stability of serum phosphate con-centration can also be establishedover this time.
• Benefits come from long-term con-trol of serum phosphate concentra-tion (for months to years).
• Acute problems of kidney diseasepatients (e.g., pyelonephritis, severehypertension) should be managedbefore introducing methods ofmanaging the serum phosphateconcentration.
When should chronic kidney diseasepatients receive treatment for phosphateoverload?Derangements in phosphate homeostasisare commonly associated with chronic kid-ney disease even at early stages becausephosphate accumulates in the body when
the glomerular filtration rate is reducedbecause of chronic kidney disease.
The following recommendations are basedon treating phosphate overload with theobjective of reducing the serum phosphateconcentration into the recommended range:
• In IRIS stages III and IV, a clinicalrenal diet is recommended for manyreasons, including controlling theserum phosphate concentration (IRIStreatment recommendations).
• In IRIS stage II, dietary phosphaterestriction might be considered evenif the serum phosphate concentra-tion is in the recommended targetrange if elevated serum PTH con-centrations are documented. How-ever, more research is necessarybefore specific recommendationscan be made on this issue. If serumPTH is not measured, do not restrictphosphate intake for patients withserum phosphate concentrations ofless than 4.5 mg/dl (1.45 µmol/l)(i.e., within the target range foranimals with IRIS stage II chronickidney disease).
What is the target serum phosphateconcentration that should be achievedwith treatment?The target goals (two months post-treatment) and therefore the degree ofphosphate restriction required depend onIRIS stage of chronic kidney disease:
Stage II—target serum phosphate concen-tration 3.5 to 4.5 mg/dl (1.17 to 1.45 µmol/l)Stage III—target serum phosphate concen-tration 3.5 to 5 mg/dl (1.17 to 1.61 µmol/l)Stage IV—target serum phosphate concen-tration 3.5 to 6 mg/dl (1.17 to 1.94 µmol/l)
How should these targets be achievedand what monitoring procedures shouldbe applied?The serum phosphate concentration shouldbe controlled by gradually introducing aphosphate-restricted diet. All commerciallyavailable renal diets can be used to achievephosphate restriction because they are allrelatively lower in phosphate than standardpet food diets. These renal diets should beintroduced gradually over a period of sevendays. The greater the proportion of the renaldiet fed, the better.
Patients should be reevaluated after fourweeks of dietary therapy. If the serum
Q&A: Recommendations for serum phosphate management in chronic kidney disease

prior to the onset of hyperphos-phatemia?
Brown: There are data suggestingthat using a phosphate-restricted dietat IRIS stages II to III has a benefi-cial effect on clinical outcome.1,2
It’s important that we not becometrapped in the concept that evidence-based medicine means we only useevidence from prospective clinicaltrials or that we not extrapolateresults of a trial to animals or con-ditions to which they do not apply.Evidence-based medicine means wehighly value randomized, placebo-based, blinded prospective clinicaltrials—but as nephrologists andveterinarians, if we don’t have appli-cable prospective trials, we are
obligated to rely on the best availableevidence. This is really what evi-dence-based medicine means. Thus,if we have no clinical trials but thereare results available from goodmodel studies that are applicable, webase our decisions on those modelstudies. If we don’t have model stud-ies in our species of interest, then welook at studies in other species. Here,evidence in rodents and people clear-ly shows some benefit of phosphaterestriction in normophosphatemic,early-stage kidney disease.
Polzin: That is an important point.Evidence-based medicine meanslooking at the best available evi-dence. If the best evidence is frompeople, we should use that.
Elliott: So our consensus is that weshould monitor the serum phosphateconcentration in animals with chron-ic kidney disease. We may also lookat PTH in animals that are normo-phosphatemic to see whether weneed to restrict phosphate. Thismight be a reasonable marker forphosphate and mineral imbalance.
____________________________Evidence from experimental
animal models and clinical cases____________________________
Brown: The data from multiplelaboratory studies on the relation-ship of phosphate to kidney diseaseare quite clear: Dietary phosphaterestriction, at least in IRIS stages II
z7y
A ROUNDTABLE DISCUSSION
phosphate concentration is greater than 6mg/dl (1.94 µmol/l), introduce an intestinalphosphate binding agent, reevaluate afterfour weeks, and adjust the dose to achievethe target level for the stage of chronickidney disease.
If the serum phosphate concentration is lessthan or equal to 6 mg/dl (1.94 µmol/l) afterfour weeks, continue dietary therapy for fourmore weeks. If the target serum phosphateconcentration has not been achieved at thistime, introduce an intestinal phosphatebinder. Reassess after four weeks and adjustthe dose of phosphate binder to achieve thetarget phosphate concentration.
Once the target serum phosphate concen-tration has been achieved, monitor everytwo to four months to maintain the phos-phate level within the desired range. Aschronic kidney disease progresses, thedegree of phosphate restriction, dosage ofintestinal phosphate binding agent, or bothwill need to increase. This occurs despitethe fact that the target serum phosphateconcentration increases as chronic kidneydisease progresses from IRIS stages II to IV.
What intestinal phosphate-bindingagents are available?
The available binding agents are:• Aluminium carbonate• Aluminium hydroxide• Aluminium oxide• Calcium carbonate (+/- chitosan)• Calcium acetate• Calcium citrate• Lanthanum carbonate• Sevelamer hydrochloride
How should phosphate-binding agentsbe used?The following recommendations are fordosing:
• Starting dose should be 30 to 60mg/kg.
• Powdered and granular preparationsare recommended over liquids andgels, which might affect palatabilityof the diet.
• The binder must be mixed with thediet.
• Serum phosphate concentrationshould be reassessed every 4weeks.
• Increase dose to effect (doublingincrements to a maximum tolerabledose) and reassess.
• When using aluminium-containingbinders, drug-induced microcytosis,muscular weakness, and
encephalopathy are possible.• Higher doses of the binder will be
required if the animal is consuminglow amounts of a clinical renal diet(or a diet relatively higher in phos-phate) and as the stage of chronickidney disease increases.
• Constipation is a potential complica-tion of higher doses of any of theavailable intestinal phosphate-binding agents.
What are the recommendations for theserum calcium concentration?Phosphate and calcium homeostasis areintrinsically linked—both are affected bychronic kidney disease as a response to theaccumulation of phosphate in the body asGFR decreases. Thus:
• Serum calcium concentrationsshould be monitored together withphosphate.
• If the total calcium concentration iselevated, assess ionized calciumconcentration.
• In cases where ionized calciumconcentrations are elevated, replacecalcium-containing phosphatebinders with alternatives (aluminiumhydroxide, lanthanum carbonate, orsevelamer hydrochloride).

and III, is protective of renalstructure, function, and survival.3-4
Polzin: A number of studies havebeen performed on dogs and catswith naturally occurring chronickidney disease. In these studies, thephosphate-restricted diets in bothdogs and cats were associated withsignificant improvement in survival.In a study examining the effect ofdiet on survival in dogs with IRISstages III and IV chronic kidneydisease, dogs consuming a phos-phate-restricted diet survivedapproximately three times longerthan dogs fed a standard mainte-nance diet. Similar beneficialeffects have been observed in catswith stages II and III chronic kid-ney disease.1,2,7
Cowgill: So these data indicate asurvival advantage for dietary phos-phate restriction, but the advantagewas independent of any change inthe serum phosphate concentration.The serum phosphate concentrationwas not a marker or predictor.
Polzin: Nor was PTH. What do youthink this means in terms of usingphosphate or PTH as an endpoint fortherapy?
Grauer: Well, at one level, it con-founds things. But at the practical,everyday level, it creates a nicescenario. We don’t deal with renalfailure diets that are just sodium-reduced, omega-3 fatty acid-supplemented, alkalinized, protein-reduced, or phosphate-restricted. Weare looking at the whole package,and the whole package works.
Elliott: We need to remember that aphosphate in the top end of the refer-ence range is probably not appropri-ate for IRIS stage II and stage IIIkidney disease.
Cowgill: Just as creatinine at thetop of the normal range doesn’tmean that your patient is normal orthat there aren’t consequences. Thiswhole concept of important para-meters being within the normalrange is a problem throughout allstages of kidney disease. Practition-ers could fail to recognize diseasebecause the levels are within thenormal range, when in fact the ani-mal has progressive disease. It is not
until it extends out of the normalrange that you recognize it. If creati-nine and other blood values are nor-mal, you can recognize renal diseaseby identifying other parameters thatreflect alterations of renal structureor function.
____________________________Experience from human medicine____________________________
Elliott: Let’s now talk about guide-lines for human medicine. I think itwould be interesting to contrast thosewith the experiences and recommen-dations that practitioners make whenmanaging their patients.
To summarize the study findings,hyperphosphatemia is associatedwith morbidity and mortality inpeople with kidney disease. Theevidence supports an associationbetween the serum phosphate con-centration, both above and below thereference ranges, with poor out-
comes.8 So the maintenance of a nor-mal serum phosphate concentrationis critical for the prevention ofabnormalities in PTH metabolism.The KDOQI guidelines for the con-trol of phosphate and PTH are pre-sented in Table 2.
____________________________Effective treatment protocols____________________________
Grauer: Let’s look at how hyper-phosphatemia and hyperparathyroid-ism should be managed in chronickidney disease patients and how wecan monitor the effectiveness of treat-ment (see Q&A: Recommendationsfor serum phosphate management inchronic kidney disease, pages 6 to 7).We determined a serum phosphateconcentration of 3.5 to 4.5 mg/dl forstage II, 3.5 to 5 mg/dl for stage III,and 3.5 to 6 mg/dl for stage IV. Wediscussed monitoring PTH levels, butthis is probably not something practi-tioners will do until we can attributemore significance to the outcome. Ithink we agree that you start with arenal failure diet, monitor the re-sponse, add phosphate binders (ifneeded), again monitor the response,and then add calcitriol (at least indogs) if you can’t reach your serumphosphate concentration goals withthe initial treatments.
____________________________Renal diets____________________________
van Dongen: The renal diet is dif-ferent from the maintenance diet inmore than one way. So the first stepin managing patients with chronickidney disease is to change the dietas much as possible before even con-sidering a phosphate binder. We haveevidence indicating that a completerenal diet with all its differences hasa better clinical outcome.
Brown: In dogs and cats withchronic kidney disease, no one hascompared the efficacy of phosphate
z8y
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
The first step in managing patientswith chronic kidney
disease is tochange the diet.—Dr. Astrid van Dongen

control with a maintenance diet plusa phosphate binder to a phosphate-restricted prescription renal dietalone. While the results might besimilar, there are other nutritionalchanges in special diets, such aspotassium and alkali supplementa-tion, that make them preferable.
Because of the nature of theavailable data, we don’t know if it’sjust phosphate restriction that isbeneficial in the clinical trials. I thinkit is the phosphate restriction partial-ly, but it could be some combinationof dietary factors. To me a logicalfirst step—after the dog or cat iscompletely evaluated diagnosticallyand you establish that it has chronickidney disease—is to recommend arenal diet. Then you follow it forseveral weeks to determine what ishappening to the serum phosphateconcentrations before you add aphosphate binder.
Elliott: We know that about 40% ofthe cats put on a renal diet will eithernot eat enough or not eat at all.2 Arewe recommending that these cats befed a standard maintenance diet plusphosphate binders?
Brown: Yes, but only as a last resortafter attempting to feed a renal diet.There are many other benefits to arenal diet, depending on the stage ofkidney disease. There is no doubtthat if an IRIS stage III or higher
animal is given a high-protein diet,this substantially increases its risk ofhaving a uremic crisis. It is importantto recommend that it be introducedto a renal diet in a very controlledand gradual manner. Some expertsalso say there is a benefit to changesin fatty acid, sodium, and/or proteincomposition in the renal diets.
Cowgill: In your experience, are the40% of patients that won’t eat a renaldiet in a higher stage of chronic kid-ney disease?
Elliott: They tend to be cats thathave been fed a variety of foods. Ifthey’ve had prawns, then they justdon’t look at the renal diet.
Polzin: Cats that accept a renal dietgenerally do well on them. Most ofthese cats maintain body weight,and their hair coats and body condi-tions remain good. But problemsarise if they fail to consume an ade-quate number of calories. If youcombine lower protein intake withinadequate dietary intake, then youget into trouble.
Brown: Yes. Inadequate intake of aprotein-restricted diet may pose moreof a nutritional risk than inadequateintake of a nonrestricted diet. That isprobably true for many nutrients. Butwhen addressing phosphate balanceonly, there are alternatives to a renal
diet. In early chronic kidney disease,we have already suggested that prac-titioners can consider a diet mixturewith intermediate levels of proteinand phosphate plus a phosphatebinder if they are worried about haircoat or diet palatability.
Polzin: Studies in people havelooked at the effect of partial dietcompliance. They have documentedthat partial compliance is superior tononcompliance. In our trials in dogsand cats, we assumed that we’d getpartial compliance, so we toleratedup to 20% noncompliance. We keptdietary records, and most dogs andcats were 90% or greater compliant.One way to address the noncompli-ance issue would be to recommendthat clients use as much of a renal-type diet as possible, so at least someof the diet consumed is renal. Oursuccess rate is much higher thanyours, which in part reflects thatmore people in the United Statesfeed a commercial pet food than inGreat Britain. You could also formu-late a homemade renal diet if the petwould be more likely to eat it.
Grauer: How much difference isthere between the various renal diets?
Brown: I don’t see how you candistinguish them for a variety ofreasons. For one, depending on howthe phosphate level in the diet is
z9y
A ROUNDTABLE DISCUSSION
KDOQI stage Recommended serum Recommended target Strength of evidencephosphate level intact PTH
III 0.87 to 1.48 µmol/l 35 to 70 pg/ml Opinion(2.7 to 4.6 mg/dl)
IV 0.87 to 1.48 µmol/l 70 to 110 pg/ml Opinion(2.7 to 4.6 mg/dl)
V 1.13 to 1.78 µmol/l 150 to 300 pg/ml Evidence(3.5 to 5.5 mg/dl)
Table 2: Kidney Disease Outcomes Quality Initiative recommendations for phosphate and PTH levels

expressed and what the caloric con-tent of the diet is, it’s difficult to knowwhich diet really provides the lowestphosphate intake per kg of patient.The other variable is that phosphateavailability in these diets has neverbeen compared and dietary phytinlevels alter phosphate absorption con-siderably. Furthermore, we should becareful not to simply recommend aphosphate-restricted diet as the bestoption; we should clearly indicate thata diet formulated for chronic kidneydisease is our first preference.
Elliott: The renal diets are morethan phosphate-restricted; they haveother potential benefits and for thiscategory of patient, they are allappropriate. So the renal diet is fedfor four weeks and is introducedgradually over one to two weeks bymixing it with the original diet andincreasing the proportion over time.Then the animal is reevaluated afterfour weeks.
____________________________Phosphate binders____________________________
Cowgill: Let’s discuss the manage-ment of patients that require morethan a renal diet to manage hyper-phosphatemia—patients that needphosphate binders. I think the biggestfailure in the management of hyper-phosphatemia in uremic animals isnot necessarily what phosphatebinder is prescribed but how it isused. Veterinarians may not have agood understanding of how thesedrugs should be used; there is nostandard dose. You dose to the out-come that you want within reason.The dose is markedly dependent onthe diet’s basal phosphate content andthe timing of the medication with thediet—all potential causes of treatmentfailure. It is a dietary phosphatebinder, so the medication has to bephysically coupled with the diet.
Animals with kidney failure don’t
eat like young, healthy Labradors—they don’t eat all of their food in onegulp. If you administer a pill and theanimal eats throughout the day, thereis no timing of medication with thediet—and no likelihood that thismedication will work. It will workbest if mixed with food, but only tothe extent that it doesn’t adulteratethe food so the animal will not con-sume it. Practitioners should recom-mend medications that are not fla-vored. Practitioners may not embracephosphate management because theydon’t understand how to effectivelyprescribe it and, therefore, don’t seeclinical benefits.
van Dongen: Practitioners alsoneed to be sure that they are dealingwith a patient with stable chronickidney disease. Sometimes it is noteasy to be sure about the nature (e.g.,acute, extrarenal, a combination, orcomplicated by ascending infection)of kidney failure on initial consulta-tion. Rather, practitioners shouldpostpone phosphate managementuntil initial treatment, results, andfollow-up have confirmed that therenal patient is not deteriorating orimproving rapidly, is capable of
maintaining its fluid balance, and isingesting enough food. You cannotforget the basic steps.
Elliott: So our recommendation isthat phosphate binders are used forlong-term treatment; they aren’t aquick fix. This treatment involveslong-term phosphate control, which isimportant in managing patients withchronic kidney failure. And to ensurea good outcome, practitioners need tomonitor phosphate levels periodicallybecause these levels can increase evenif phosphate binders are administered.
Cowgill: I find it amazing how manyreferrals I get for acute kidney failure.These patients often have a phosphatelevel approaching or exceeding 25mg/dl and are being treated with in-testinal phosphate binders, despite thefact that the animal was not eating.
van Dongen: Or worse, sometimesan animal is referred for kidney dis-ease and a urinary tract infection isalso detected during the workup buturine was not checked before refer-ral. These initial steps are important.
Cowgill: Historically, the way wehave dosed phosphate binders isintrinsically wrong. They should bedosed based on the amount of phos-phate in the diet, but we make blan-ket recommendations of 30 to 60mg/kg. We need to understand howmuch phosphate is in the diet andhow much phosphate binder—basedon its binding capacity—would tieup that phosphate. We know the con-tent of most of the diets animals eatthese days, so it’s possible to esti-mate the phosphate intake.
Elliott: We also want to encouragemonitoring the serum phosphateconcentration as part of longitudinalmonitoring of animals with chronickidney disease, which help us adjust
z10y
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
The biggest failure inthe management ofhyperphosphatemiain uremic animalsis not necessarilywhat phosphate
binder is prescribedbut how it is used.
—Dr. Larry Cowgill

the dose to suit the individual patient.The other factor that influences doseis the stage of kidney disease.
Dr. Bernhard Gerber: What start-ing dose of phosphate binders shouldpractitioners recommend?
Grauer: Typically, aluminumhydroxide or calcium carbonate isrecommended, starting at 30 mg/kgand increasing to 90 mg/kg or aboveas needed.
Polzin: Two important factors playa role in dosing. First, the dietaryphosphate level, even with the sameGFR, can profoundly alter thestarting dose of phosphate binder.Then there is the concept of propor-tional reduction in phosphate accord-ing to the reduction of GFR, whichinvolves the stage of kidney disease.So with an animal at a certain stageof chronic kidney disease on a partic-ular diet, you can estimate the phos-phate intake, which may lead you toa very different starting dose than thestandard recommendation. Is there away to use those two factors togetherto determine a dosing recommenda-tion? Again, practitioners can be-come frustrated quickly because thephosphate binder isn’t working—they may be looking too soon or thedosing is not optimal. For example,if you use a phosphate binder with astandard diet in an animal that hasfairly advanced kidney failure andyou start with a 30 mg/kg dose, youmay see no response at all. So weshould probably do a better job oflinking starting dosage to the severityof the disease and providing veryexplicit follow-up recommendations.
Elliott: How stable is this animalbefore we start treatment? If you takeone pretreatment sample for theserum phosphate concentration and alater posttreatment sample shows that
the phosphate has increased ordecreased, you don’t actually knowhow stable that animal was initially.The recommendation is that you taketwo pretreatment samples to evaluatewhether this animal presented to youbecause it suddenly deteriorated andif its second pretreatment sampleshows a further deterioration. Quiteoften, it has improved since the firstsample. Then you take a third sampleto see whether it really stabilized,and that is what you base your treat-ment on.
Cowgill: There is no rationale foradding a phosphate binder until youhave exhausted the limits of dietaryphosphate reduction. As you transi-tion the animal to the diet, you havethe opportunity for two or threeserum phosphate measurements todetermine the stability and baselinevalue. So another thing that isn’tdone routinely in the first line ofhyperphosphatemia management ischanging the diet because it isn’t aseasy as just adding a phosphatebinder to an existing diet.
Polzin: I’d be surprised if waitingtwo or three weeks to modifyphosphate levels would make anydifference in the long-term. The firstthing practitioners focus on isdecreasing the phosphate level. Itdoesn’t have anything to do withsymptomatology, and I doubt start-ing phosphate binders a few weeksearlier will alter the disease out-come. It makes sense to establish theserum phosphate concentration base-line for the patient first and thendetermine what to do. Again, youdon’t want to make abrupt dietchanges as most dogs and cats won’taccept them. It may be a couple ofweeks to months before you candecide to add a phosphate binder.We don’t want to present this as anurgent thing.
Elliott: Are calcium-containing phos-phate binders and the risk of hyper-calcemia an issue in veterinary medi-cine as they are in human medicine?
Cowgill: First, I don’t think we havenecessarily excluded aluminum as aneffective phosphate binder in ani-mals. We don’t know if animals havethe same historical problems withaluminum as people. Do we knowthat aluminum affects the neurologicsystem? Do we know that we havealuminum bone disease or aluminumtoxicity? As you use higher doses ofaluminum-based phosphate bindersin animals with more advanced dis-ease, the likelihood of seeing alu-minum toxicity is real and needs tobe monitored. But at varying stagesof chronic kidney disease, you canalso see definite effects of hypercal-cemia from calcium-based binders.
Elliott: The problem I have is thataluminum-based binders have disap-peared from the pharmacy shelf.
Polzin: It is sometimes difficult forowners and practitioners to getaluminum-based phosphate bindersunless it is through a veterinary dis-tributor or university.
Cowgill: If you use an aluminumpowder, you can sprinkle it on thefood. I think gels are a disaster. Wehave ordered reagent-grade aluminumvery economically from suppliers,and you can provide that in a veryeasy form and mix it with canned orkibble foods. Aluminum hydroxidealso works very effectively.
Dosing has become a problemwith aluminum because of the diffi-culties of finding effective prepara-tions. But I think aluminum is still areasonable choice. People usingaluminum binders have years ofexposure with no effective means ofeliminating the aluminum. I’m not
z11y
A ROUNDTABLE DISCUSSION
sure we have those same concernsin dogs and cats.
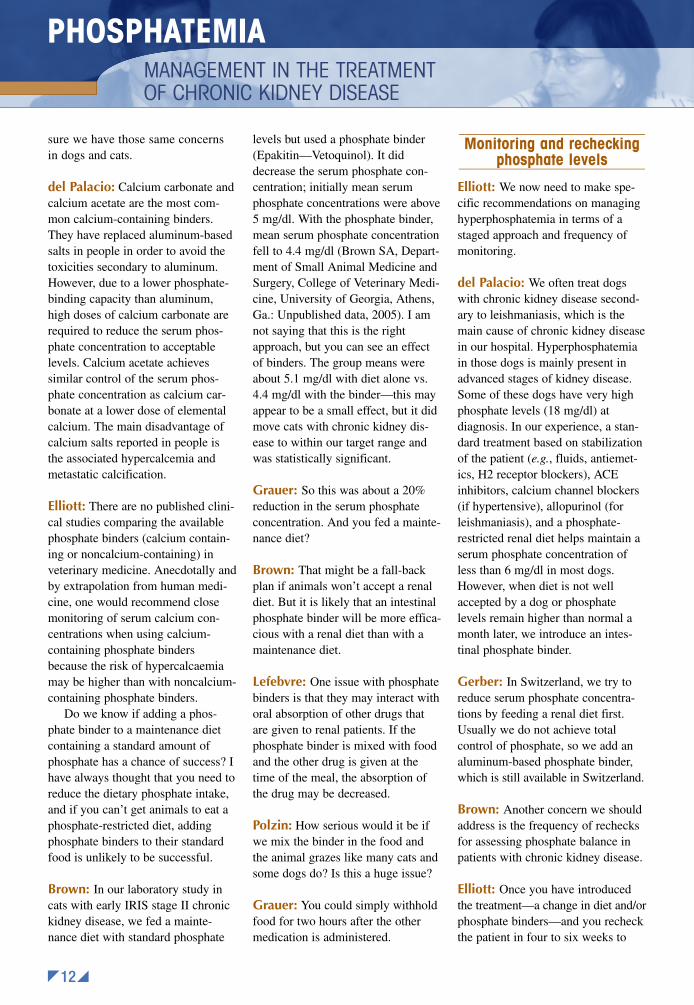
del Palacio: Calcium carbonate andcalcium acetate are the most com-mon calcium-containing binders.They have replaced aluminum-basedsalts in people in order to avoid thetoxicities secondary to aluminum.However, due to a lower phosphate-binding capacity than aluminum,high doses of calcium carbonate arerequired to reduce the serum phos-phate concentration to acceptablelevels. Calcium acetate achievessimilar control of the serum phos-phate concentration as calcium car-bonate at a lower dose of elementalcalcium. The main disadvantage ofcalcium salts reported in people isthe associated hypercalcemia andmetastatic calcification.
Elliott: There are no published clini-cal studies comparing the availablephosphate binders (calcium contain-ing or noncalcium-containing) inveterinary medicine. Anecdotally andby extrapolation from human medi-cine, one would recommend closemonitoring of serum calcium con-centrations when using calcium-containing phosphate bindersbecause the risk of hypercalcaemiamay be higher than with noncalcium-containing phosphate binders.
Do we know if adding a phos-phate binder to a maintenance dietcontaining a standard amount ofphosphate has a chance of success? Ihave always thought that you need toreduce the dietary phosphate intake,and if you can’t get animals to eat aphosphate-restricted diet, addingphosphate binders to their standardfood is unlikely to be successful.
Brown: In our laboratory study incats with early IRIS stage II chronickidney disease, we fed a mainte-nance diet with standard phosphate
levels but used a phosphate binder(Epakitin—Vetoquinol). It diddecrease the serum phosphate con-centration; initially mean serumphosphate concentrations were above5 mg/dl. With the phosphate binder,mean serum phosphate concentrationfell to 4.4 mg/dl (Brown SA, Depart-ment of Small Animal Medicine andSurgery, College of Veterinary Medi-cine, University of Georgia, Athens,Ga.: Unpublished data, 2005). I amnot saying that this is the rightapproach, but you can see an effectof binders. The group means wereabout 5.1 mg/dl with diet alone vs.4.4 mg/dl with the binder—this mayappear to be a small effect, but it didmove cats with chronic kidney dis-ease to within our target range andwas statistically significant.
Grauer: So this was about a 20%reduction in the serum phosphateconcentration. And you fed a mainte-nance diet?
Brown: That might be a fall-backplan if animals won’t accept a renaldiet. But it is likely that an intestinalphosphate binder will be more effica-cious with a renal diet than with amaintenance diet.
Lefebvre: One issue with phosphatebinders is that they may interact withoral absorption of other drugs thatare given to renal patients. If thephosphate binder is mixed with foodand the other drug is given at thetime of the meal, the absorption ofthe drug may be decreased.
Polzin: How serious would it be ifwe mix the binder in the food andthe animal grazes like many cats andsome dogs do? Is this a huge issue?
Grauer: You could simply withholdfood for two hours after the othermedication is administered.
____________________________Monitoring and rechecking
phosphate levels____________________________
Elliott: We now need to make spe-cific recommendations on managinghyperphosphatemia in terms of astaged approach and frequency ofmonitoring.
del Palacio: We often treat dogswith chronic kidney disease second-ary to leishmaniasis, which is themain cause of chronic kidney diseasein our hospital. Hyperphosphatemiain those dogs is mainly present inadvanced stages of kidney disease.Some of these dogs have very highphosphate levels (18 mg/dl) atdiagnosis. In our experience, a stan-dard treatment based on stabilizationof the patient (e.g., fluids, antiemet-ics, H2 receptor blockers), ACEinhibitors, calcium channel blockers(if hypertensive), allopurinol (forleishmaniasis), and a phosphate-restricted renal diet helps maintain aserum phosphate concentration ofless than 6 mg/dl in most dogs.However, when diet is not wellaccepted by a dog or phosphatelevels remain higher than normal amonth later, we introduce an intes-tinal phosphate binder.
Gerber: In Switzerland, we try toreduce serum phosphate concentra-tions by feeding a renal diet first.Usually we do not achieve totalcontrol of phosphate, so we add analuminum-based phosphate binder,which is still available in Switzerland.
Brown: Another concern we shouldaddress is the frequency of rechecksfor assessing phosphate balance inpatients with chronic kidney disease.
Elliott: Once you have introducedthe treatment—a change in diet and/orphosphate binders—and you recheckthe patient in four to six weeks to
z12y
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE

ensure compliance, then monitoringevery two to three months is frequentenough for IRIS stage II to III.
Brown: So ask them to return in onemonth and then check them everytwo months?
Polzin: Our philosophy is more fre-quent rechecks in the early stages.Then you can back off depending onhow the patient responds. For dogsand cats in stage III, you can recheckthem every three or four months. Andyou can recheck cats less often if theyare stable. Dogs and cats in stage IVmay require more frequent visits.
Grauer: We should not lose sight ofthe fact that checking early allows usto look at other parameters than justthe serum phosphate concentration. Itallows us to have a better handle onthe stability—or lack thereof—of thedisease process.
Polzin: If you wait too long betweenexaminations, compliance will fallprecipitously. I think three to fourmonths is the longest you can gowithout having to reintroduce anydrug in this situation—includingphosphate binders—to clients.
Grauer: It depends, too, on whetherthere are other medications onboard. If you have a hypertensive,proteinuric patient on ACE inhibi-tors, you’ll need to look sooner atresponse, and you may or may notinclude your serum phosphate evalu-ation at that time.
Polzin: Again, there is a chance youwon’t see much change in the phos-phate level if you evaluate it too soon.
van Dongen: You only start evalu-ating the phosphate level once otherparameters have stabilized, such asproteinuria.
Polzin: As mentioned earlier, itdoesn’t have to be solved in the firsttwo weeks of treatment.
van Dongen: You have a reasonfor regular checkups in the begin-ning. But don’t only monitorphosphate levels; also follow-up onclinical signs, the intake of fluidsand food (e.g., quantity, quality,amount of renal diet), parametersindicative of renal function itself
(e.g., plasma creatinine, proteinuria,improvement in urine sediment),and underlying or secondary ab-normalities, such as hypertension.Phosphate does become importantto reevaluate after the patient hasstabilized.
Brown: I used to recommend moni-toring at two-week intervals, but Inow realize that’s too frequent toreassess the full effects of either dietor a binder on serum phosphate con-centration. If you put an animal on adiet, recheck it in one or two weeks,add a binder, and then recheck it inanother week or two, soon you maybe overdosing the binder and inter-fering with food intake. So a pre-ferred plan would be to recheck oncea month for the first three months.With this approach, once your
patient is stable and eating a recom-mended diet, you then assess theserum phosphate concentration amonth later and make a decisionabout a binder. Then a month afterthat, decide about adjusting thebinder dose.
Grauer: So that begs this question:Should we have different initial start-ing dosages of binders given duringdifferent stages of chronic kidneydisease?
Polzin: If you start an IRIS stage IIanimal at the same dose that youstart a stage IV animal and your planis to recheck monthly for threemonths and then every three to fourmonths, the stage IV animal may notbe there by the third month.
Grauer: What would you recom-mend?
Polzin: We need to determinedifferent starting doses. There issome logic to reducing the serumphosphate concentration in parallelto the reduction in GFR. So deter-mine the serum phosphate concen-tration, figure out the bindingcapacity, get an idea of the dietaryphosphate intake, and calculate theappropriate dose to reduce theserum phosphate concentrationproportionately. It will vary, depend-ing on the diet and the severity ofthe GFR reduction.
Elliott: So the important point weneed to make is that phosphate bind-ing is a long-term treatment.
Polzin: And the dose is to effect.
Elliott: It’s also important to estab-lish the stability of the given diseasebefore starting the intervention. Be-cause it is a long-term treatment, thefollow-up and monitoring can be as
z13y
A ROUNDTABLE DISCUSSION
The important pointwe need to make is that phosphate
binding is a long-term treatment.
—Dr. Jonathan Elliott

infrequent as once monthly to beginwith and then every two months,depending on the stage of disease.
Grauer: Would we automaticallyadd a binder to the diet in an initialtreatment for an advanced IRIS stageIII or IV patient, or would youalways assess the effect of diet first?
Polzin: I don’t think hyperphos-phatemia is something you have tofix immediately, so I would start withdiet to see what that does. I’d followthe diet until it’s stable, which couldbe two months or more. At thatpoint, you could choose to intervene.
Elliott: In one feline study, research-ers rechecked the cats at four toseven weeks after a renal diet wasintroduced and then at four to fivemonths.9 There was very little changebetween the initial decrease in serumphosphate concentration after amonth or two on the diet. These werecats in IRIS stages II and III. Four-teen cats were fed the renal dietalone or renal diet and aluminiumhydroxide, and eight cats were fed astandard maintenance diet.
Brown: And this study was on dietalone?
Elliott: Primarily. Some of thesecats would have been reassessed atpoints in between, and two werethen given phosphate bindersbecause researchers were not happywith the degree of phosphate restric-tion. I think only two cats out of 14in the first four to five months need-ed phosphate binders. These catstended to be in more advancedstages of kidney disease, so the dietalone was insufficient to control theserum phosphate concentration andPTH. Thus, the degree of phosphaterestriction needs to be tailored tothe individual cat. A logical way to
do this is with regular reassessmentof the treatment response in relationto a defined post-treatment serumphosphate target concentration;practitioners should use stepwiseincrements of phosphate restrictioneach month until they achieveeffective control.
Cowgill: Particularly as you treatthese late stage III to stage IV ani-mals, it is problematic to throw allof the therapy at the patient at once.It is more tolerable for the animaland the client in steps, and they arenot dealing with four or five medica-tions at the beginning.
Grauer: I don’t disagree with that.But in my experience, in an ad-vanced stage III or stage IV patient,it’s unlikely that diet alone is goingto get you where you want to be. Soyou’re right; there are different waysto approach it. These cats or dogsare fragile, so you should change thediet gradually. If you have a phos-phate binder that doesn’t affectpalatability, this might not be a badtime to introduce it so you aren’tintroducing a subsequent changedown the road.
Polzin: Do you think step-wise ther-apy is a problem in terms of serumphosphate concentration adjustment?
Grauer: No.
Cowgill: What is a dog’s life expec-tancy in early or late stage III orearly stage IV? Six or eight months?
Polzin: We didn’t look at the data inthose terms, but that’s probably right.
Cowgill: So are you going to taketwo and a half months to get this ani-mal on a low-phosphate diet?
Elliott: Should we check dogs thatare in the late stages after four weeksand add the phosphate binder then?
Cowgill: You may want to be moreaggressive with your approach. Idon’t have evidence, but my feelingwould be that hyperphosphatemiamay accelerate their demise.
Elliott: Could we say that with acertain level of hyperphosphatemiayou should treat initially with dietand binders? So what if the serumphosphate concentration is higherthan 6 or 6.5 mg/dl (1.94 or 2.10µmol/l) after one month?
Cowgill: Then you have two op-tions. You could either try to get agreater proportion of dietary phos-phate reduction or add a binder.
Polzin: You could set two targets: 6mg/dl (1.94 µmol/l) at one month,and 4.5 mg/dl (1.45 µmol/l) at twomonths. If you are above 6 mg/dl(1.94 µmol/l) at one month, then youadd the binder If you are below 6mg/dl, then you keep going.
Brown: So you are proposing thatat one month, if the animal’s serumphosphate concentration is above 6
z14y
PHOSPHATEMIAMANAGEMENT IN THE TREATMENT OF CHRONIC KIDNEY DISEASE
In my experience,in an advanced
stage III or stage IVpatient, it’s unlikely
that diet alone is going to get you where you
want to be.—Dr. Gregory F. Grauer

mg/dl, you would add a binder, bringthat animal back in a month, andcontinue at monthly intervals untilyou reach stability in the serumphosphate concentration? Ultimatelydo we still have the same targets thatwe had before?
Polzin: Yes. The serum phosphateconcentration target stays the same.Ideally, you would reach it by twomonths. If you don’t, you might con-sider increasing the binder dose.
Brown: By all likelihood, the stageIV animal would be on a phosphatebinder at one month.
____________________________Calcium monitoring____________________________
Brown: Practitioners should alsomonitor calcium.
Elliott: What limits are we puttingon calcium? What should we do ifwe are outside of those limits?
Polzin: A lot of these dogs and catsare hypercalcemic, but the hypercal-cemia isn’t necessarily associatedwith ionized calcium elevations.Frankly, I am not 100% sure whatthat means physiologically or patho-logically to a patient. It might sug-gest a higher probability of tissuemineral deposition.
Grauer: You have made a criticalpoint. If you see hypercalcemia, youneed to analyze ionized calcium levels.
Polzin: But is it going to changewhat you do? Clearly it will if theionized calcium is elevated, but if it’snot, what do you do?
Brown: If the animal is hypercal-cemic, you should measure the ion-ized calcium. If the ionized calcium
is in the normal range, you make noadjustments; you just monitor thecalcium. But if the ionized calcium iselevated and the animal is taking acalcium-containing phosphate binder,I would switch to a noncalcium-containing binder.
van Dongen: If you use a calcium-based binder, it would be wise tomonitor the calcium and preferablyionized calcium levels.
____________________________Conclusion____________________________
Elliott: Our recommendations forserum phosphate concentrationmanagement are summarized onpages 6 to 7. This treatment is forstable chronic kidney disease pa-tients, and the benefit comes fromlong-term control of the serum phos-phate concentration. Manage yourkey problems first before consideringthe serum phosphate concentration;for example, address pyelonephritisand severe hypertension. Demon-strate stability in the patient withchronic kidney disease by perform-ing serial serum creatinine measure-ments every two to four weeks.Phosphate restriction can also beaddressed at this time.
Control of the serum phosphateconcentration should be achieved bygradually introducing a phosphate-restricted diet. All commerciallyavailable renal diets can be used toachieve phosphate restriction. Theseshould be introduced gradually overa period of seven days. The greaterthe proportion of the renal diet fed,the better.
Patients should be reevaluatedafter four weeks. If the serum phos-phate concentration is greater than 6mg/dl (1.94 µmol/l) at this time,introduce intestinal phosphate bind-ing agents, reevaluate after another
four weeks, and adjust the dose toachieve the target level for the stageof chronic kidney disease. If theserum phosphate concentration isless than or equal to 6 mg/dl (1.94µmol/l) after four weeks, continuedietary therapy for an additional fourweeks. If the target serum phosphateconcentration has not been achievedat this time, introduce intestinalphosphate binders.
____________________________References____________________________
1. Jacob F, Polzin DJ, Osborne CA, et al.Clinical evaluation of dietary modification fortreatment of spontaneous chronic renal failurein dogs. J Am Vet Med Assoc 2002;220:1163-1170.
2. Elliott J, Rawlings JM, Markwell PJ, etal. Survival of cats with naturally occurringchronic renal failure: effect of dietary manage-ment. J Small Anim Pract 2000;41:235-242.
3. Ross LA, Finco DR, Crowell, WA. Effect ofdietary phosphate restriction on the kidneys ofcats with reduced renal mass. Am J Vet Res1982;43:1023-1026.
4. Brown SA, Crowell WA, Barsanti JA, etal. Beneficial effects of dietary mineral restric-tion in dogs with marked reduction of func-tional renal mass. J Am Soc Nephrol 1991;1:1169-1179.
5. Slatopolsky E, Bricker NS. The role ofphosphorus restriction in the prevention ofsecondary hyperparathyroidism in chronic renaldisease. Kidney Int 1973;4:141-145.
6. Slatopolsky E, Caglar S, Gradowska L,et al. On the prevention of secondary hyper-parathyroidism in experimental chronic renaldisease using “proportional reduction” ofdietary phosphorus intake. Kidney Int 1972;2:147-151.
7. Ross S, Polzin D, Osborne C, et al.Clinical evaluation of dietary modification forthe treatment of spontaneous chronic renalfailure in cats, in Proceedings. ACVIM Forum,June 2005.
8. KDOQI clinical practice guidelines forbone metabolism and disease in chronic kidneydisease. Am J Kidney Dis 2003;42(suppl 3):S1-S201.
9. Barber PJ, Rawlings JM, Markwell PJ,et al. Effect of dietary phosphate restriction onrenal secondary hyperparathyroidism in thecat. J Small Anim Pract 1999;40:62-70.
z15y
A ROUNDTABLE DISCUSSION
© 2006 Vétoquinol. All rights reserved. Cover art by Sandy Ostroff.





![Index [pharmrev.aspetjournals.org]pharmrev.aspetjournals.org/content/pharmrev/43/4/local/back-matter.pdf · primary structure, kidney (fig.), 497 ... pathophysiology, ... schematic](https://static.fdocuments.us/doc/165x107/5b82cde67f8b9a315b8bcf1a/index-primary-structure-kidney-fig-497-pathophysiology-schematic.jpg)