
PHONE 937-399-7100 1108 VESTER AVENUE … · OB/GYN, LTD PHONE 937-399-7100 1108 VESTER AVENUE...
8
OB/GYN, LTD PHONE 937-399-7100 www.springfie1dohioob2vn.com 1108 VESTER AVENUE SPRINGFIELD, OHIO 45503 FAX 937-399-7355 To: All Patients From: OB/GYN, LTD. Re: Office Policy This is to inform you of our present policies. We strive to serve you effectively and efficiently. If you have any suggestions on how we can serve you in a superior way, please let us know in written form. We are constantly evolving in an effort to serve your health care needs. 1. You must have current insurance information with you at each visit. If your insurance plan changes, please notify us so that we may update our information and avoid billing confusions. 2. If you are unable to keep your appointment, please notify us 24 hours in advance. A $15.00 fee will be assessed if notification is not received. 3. Any patient who is twenty minutes or more late will be rescheduled. 4. Please arrive approximately ten minutes prior to scheduled ultrasound appointments, as this will allow us to remain on a schedule. A $25.00 fee will be assessed for missed ultrasound appointments. 5. Patients unable to notify us as outlined above for three consecutive appointments will be referred elsewhere for care. We believe strongly that we are partners in your healthcare. We choose only to partner with those who have an interest in the maintenance of their health. Again, you play a vital role in the process. 6. NO FOOD, DRINK OR CELL PHONE USAGE IN THE OFFICE PLEASE. 7. NO CHILDREN UNDER THE AGE OF 14 ARE PERMITTED IN THE OFFICE. IF YOU ARE COMING FOR YOUR POST PARTUM EXAM, YOU MAY BRING YOUR NEWBORN WITH YOU. Finally, these policies are designed to facilitate delivering quality care to all of our patients. We look forward to partnering with you in your healthcare. Thank You. Revised 1/13
Transcript of PHONE 937-399-7100 1108 VESTER AVENUE … · OB/GYN, LTD PHONE 937-399-7100 1108 VESTER AVENUE...
OB/GYN, LTD PHONE 937-399-7100
www.springfie1dohioob2vn.com 1108 VESTER AVENUE
SPRINGFIELD, OHIO 45503 FAX 937-399-7355
To: All Patients From: OB/GYN, LTD. Re: Office Policy
This is to inform you of our present policies. We strive to serve you effectively and efficiently. If you have any suggestions on how we can serve you in a superior way, please let us know in written form. We are constantly evolving in an effort to serve your health care needs.
1. You must have current insurance information with you at each visit. If your insurance plan changes, please notify us so that we may update our information and avoid billing confusions.
2. If you are unable to keep your appointment, please notify us 24 hours in advance. A $15.00 fee will be assessed if notification is not received.
3. Any patient who is twenty minutes or more late will be rescheduled. 4. Please arrive approximately ten minutes prior to scheduled ultrasound
appointments, as this will allow us to remain on a schedule. A $25.00 fee will be assessed for missed ultrasound appointments.
5. Patients unable to notify us as outlined above for three consecutive appointments will be referred elsewhere for care. We believe strongly that we are partners in your healthcare. We choose only to partner with those who have an interest in the maintenance of their health. Again, you play a vital role in the process.
6. NO FOOD, DRINK OR CELL PHONE USAGE IN THE OFFICE PLEASE. 7. NO CHILDREN UNDER THE AGE OF 14 ARE PERMITTED IN THE
OFFICE. IF YOU ARE COMING FOR YOUR POST PARTUM EXAM, YOU MAY BRING YOUR NEWBORN WITH YOU.
Finally, these policies are designed to facilitate delivering quality care to all of our patients. We look forward to partnering with you in your healthcare.
Thank You.
Revised 1/13
OBIGYN, LTD.
PATIENT QUESTIONNAIRE
Please list the family members or other persons, if any, whom we may inform about your general medical condition and your diagnosis (including treatment, payment, and health care operations):
II. Please list the family members or significant others, if any, whom we may inform about your medical condition ONLY IN AN EMERGENCY:
Name
Phone Number Name
Phone Number
III. Please print the address of where you would like your billing statements and/or correspondence from our office to be sent if other than your home.
IV. Please indicate if you want all correspondence from our office sent in a sealed envelope marked "CONFIDENTIAL":
YES NO__________
V. Please print the telephone number where you want to receive calls about your appointments, lab and x-ray results, or other health care information if other than your home phone number:
*1 am fully aware that a ce//phone is not a secure and private line.
VI. Can confidential messages (i.e., appointment reminders) be left on your telephone answering machine or voicemail?
YES NO__________
PATIENT NAME
(guardian if under 18 yrs.)
PATIENT/GUARDIAN SIGNATURE
DATE
2/03
Receipt of Notice of Privacy Practices
Written Acknowledgement Form
I, , have received/been offered a copy of
OB/GYN's Notice of Privacy Practices.
Signature of Patient/Guardian
Date of Signature
OB/GYN, LTD. 937-399-7100
1108 Vester Avenue Springfield, Ohio 45503
Fax 937-399-7355 www.snrinfieIdobioobgvn.com
Payment Policy
Payment in Full: Full payment is required at the time of service from all patients that have not met their deductible or do not have insurance coverage. We offer several payment options that include MasterCard, Visa, Discover, and a 12-month interest-free payment progrm.
Patient Responsibility: The patient is required to pay all co-pay and co-insurance amounts at the time of service.
Your insurance policy is a contract between you and your insurance company. You are ultimately responsible for any unpaid balances. If your insurance company is contracted with your physician, we will bill them for you and make every effort to ensure that claims are promptly and correctly processed.
Occasionally, because of factors beyond our control, some insurance companies may not reimburse your physician within 60 days. Your physician will then request the payment in full from you. Payment received from your insurance company after you have paid, will promptly be refunded to you.
Past Due Balances: A past due balance is any amount due from a prior visit where insurance is not pending, the account has been sent to collections, or an insurance payment has not been received by your physician within 60 days. If you have a previous collection agency balance and wish to receive service, you will be required to pay the past due collection balance and any new charges at the time of service. If your account balance is sent to our collection agency you may be dismissed from our practice. Balances on accounts with payment plans where payments conform to the plan are not considered past due balances. Exceptions to this will be made if covered service's are contracted with your carrier.
Returned Checks: Checks returned for insufficient funds will be subject to a $35.00 service fee.
Disclosure: Dr. Osterholt and Dr. McNeely are investors in Ohio Valley Medical Center in Springfield, Ohio. At times, they may refer patients to OVMC in connection with their care and treatment.
I have read and agree to the terms of the above statements. After signing, I may request a copy of this payment policy for my own records.
Patient Signature Date
Today's Date
Patient Name:
E;oe, COmp"' /14
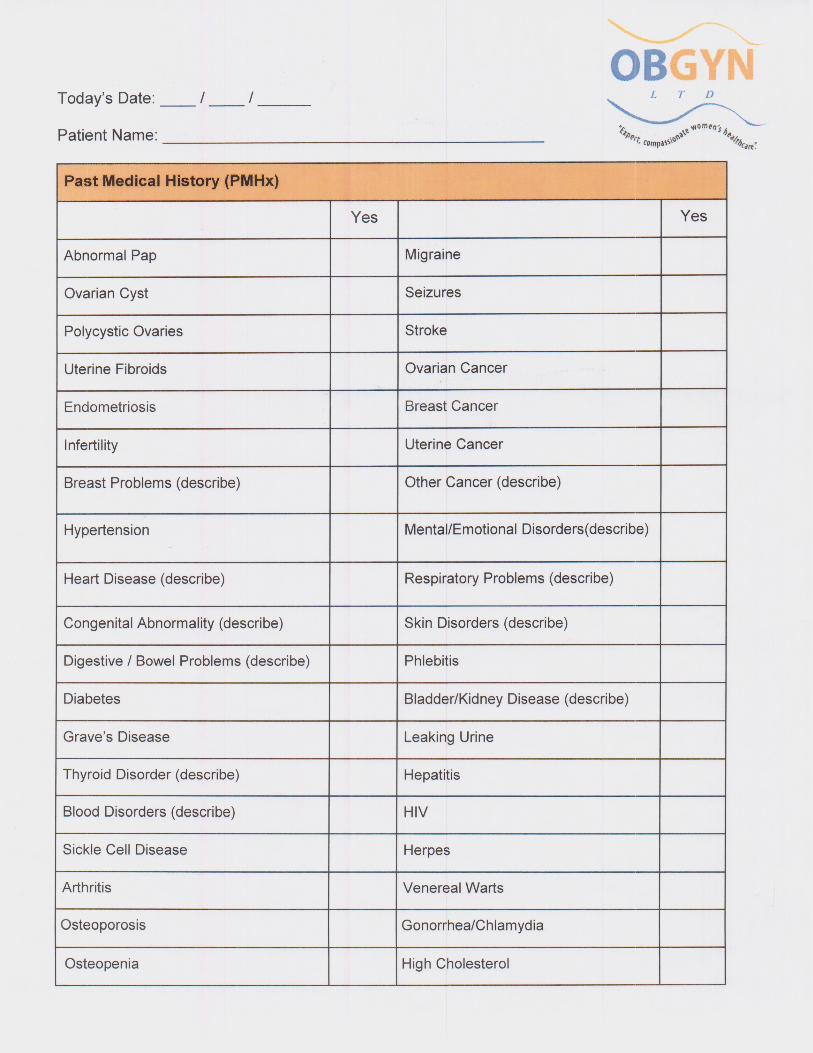
Past Medical History (PMHx)
Yes Yes
Abnormal Pap Migraine
Ovarian Cyst Seizures
Polycystic Ovaries Stroke
Uterine Fibroids Ovarian Cancer
Endometriosis Breast Cancer
Infertility Uterine Cancer
Breast Problems (describe) Other Cancer (describe)
Hypertension Mental/Emotional Disorders(describe)
Heart Disease (describe) Respiratory Problems (describe)
Congenital Abnormality (describe) Skin Disorders (describe)
Digestive I Bowel Problems (describe) Phlebitis
Diabetes Bladder/Kidney Disease (describe)
Grave's Disease Leaking Urine
Thyroid Disorder (describe) Hepatitis
Blood Disorders (describe) HIV
Sickle Cell Disease Herpes
Arthritis Venereal Warts
Osteoporosis GonorrhealChlamydia
Osteopenia High Cholesterol
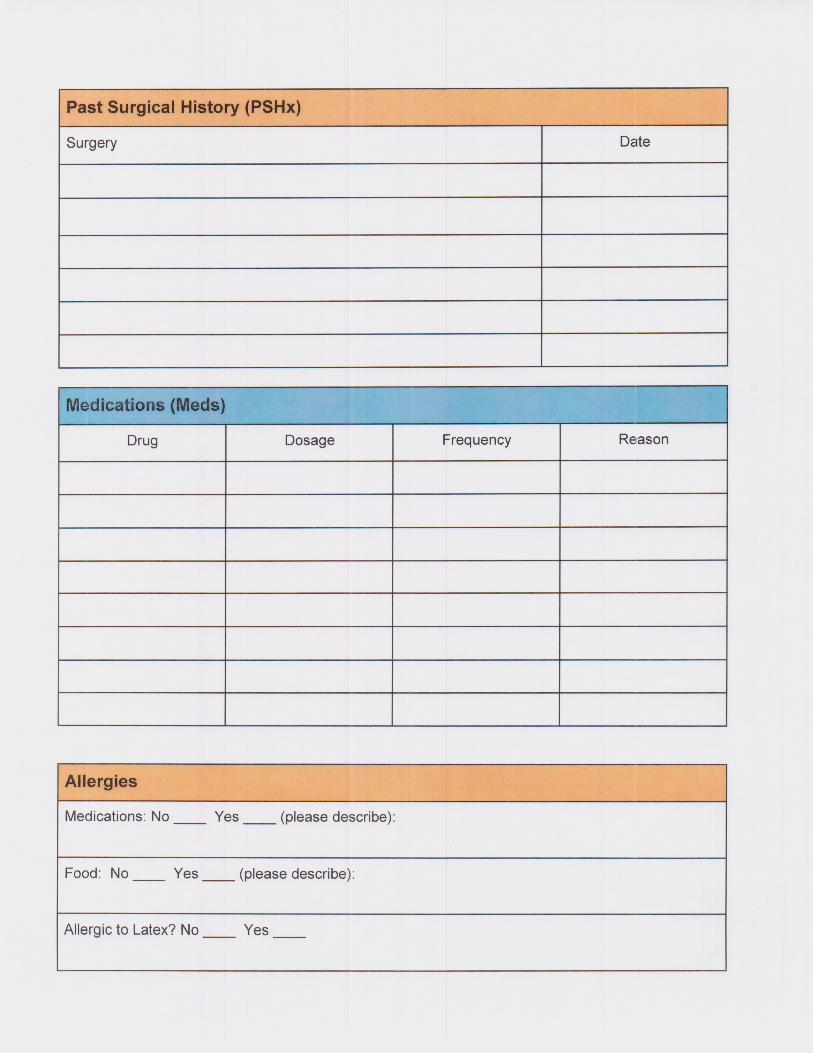
Past Surgical History (PSHx)
Surgery Date
Medications (Meds)
Drug Dosage Frequency Reason
Allergies
Medications: No ____ Yes ____ (please describe):
Food: No Yes ____ (please describe):
Allergic to Latex? No ____ Yes ____
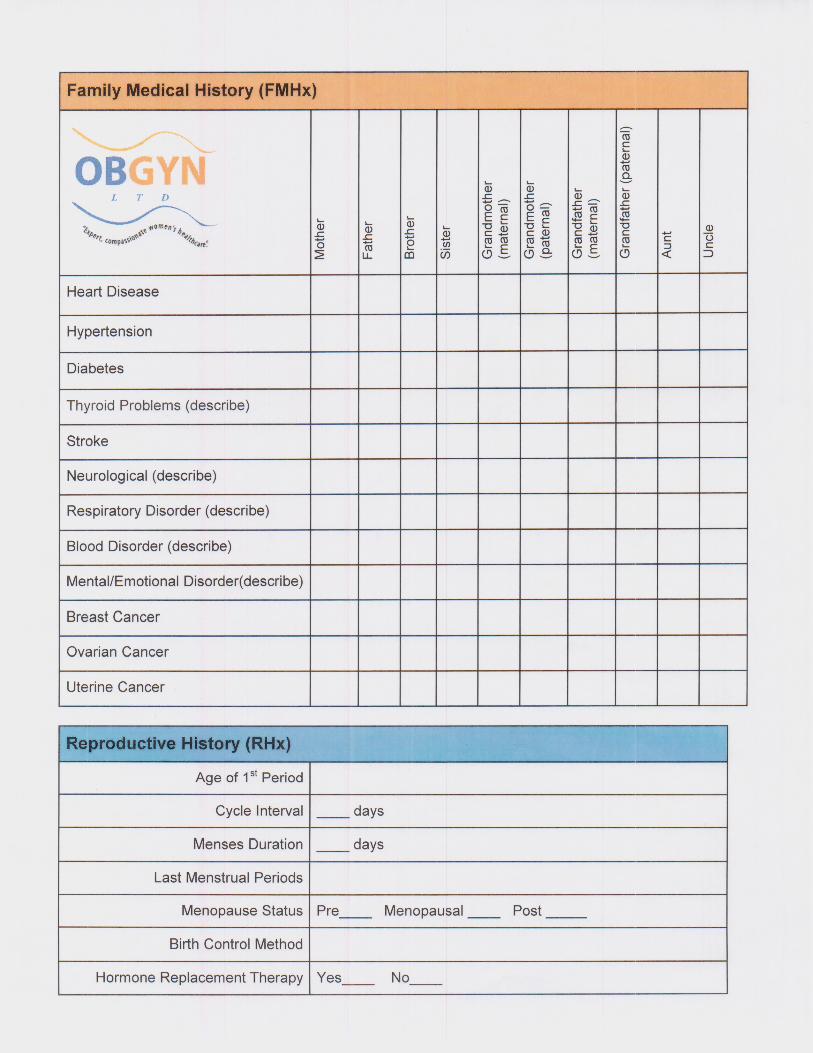
Family Medical History (FMHx)
OBGYN LTD Dhft
' COmp .3 CU .3
J (I) 0
Heart Disease
Hypertension
Diabetes
Thyroid Problems (describe)
Stroke
Neurological (describe)
Respiratory Disorder (describe)
Blood Disorder (describe)
Mental/Emotional Disorder(describe)
Breast Cancer
Ovarian Cancer
Uterine Cancer
Reproductive History (RHx)
Age of 1st Period
Cycle Interval days
Menses Duration days
Last Menstrual Periods
Menopause Status Pre Post
Birth Control Method
Hormone Replacement Therapy Yes
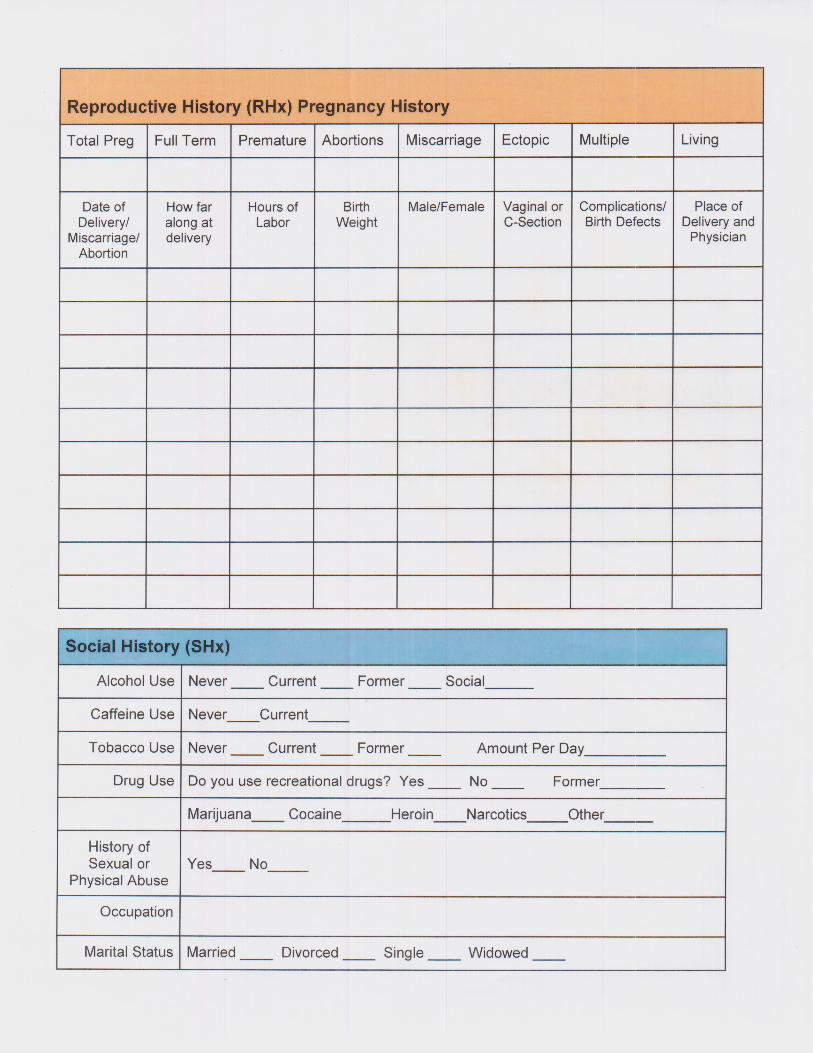
Reproductive History (RHx) Pregnancy History
Total Preg Full Term Premature Abortions Miscarriage Ectopic Multiple Living
Date of Delivery/
Miscarriage/ Abortion
How far along at delivery
Hours of Labor
Birth Weight
Male/Female Vaginal or C-Section
Complications! Birth Defects
Place of Delivery and
Physician
Social History (SHx)
Alcohol Use Never Current Former Social______
Caffeine Use Never Current _____
Tobacco Use Never Current Former Amount Per Day_______
Drug Use Do you use recreational drugs? Yes ____ No Former_____
Marijuana Heroin Narcotics Other_
History of Sexual or
Physical Abuse Yes
Occupation
Marital Status Married ____ Divorced ____ Single ____ Widowed ____


















