PHO Infographic FoodborneIllness V7 copy€¦ · FDA National Retail Food Team. FDA trend analysis...
1
OCCURRENCE OF FOODBORNE ILLNESSES * WHAT WE DON’T KNOW CAN HARM US The burden of foodborne illness is esmated to be substanal. 3-5 Although self-limited in most instances, serious health effects or death may occur. 6 Determining the true impact foodborne illness has on Ontario is difficult as it is underreported. • Children are more likely to be diagnosed with foodborne illness • Adults aged 65 or older are most likely to be hospitalized or die as a result of infecon¹ The top four food sources for reported cases of domescally- acquired foodborne illness § in Ontario, 2007-2010, were: 7 SUSPECTED FOOD SOURCES Unsafe food pracces can lead to foodborne illness. To reduce risk of contaminaon and illness: 8,9 • Use proper hand hygiene • Obtain food from approved sources • Avoid cross-contamination • Follow safe cooking/preparation practices • Store food at appropriate temperatures Encourage reporng of suspected cases of foodborne illness. AN OUNCE OF PREVENTION REPORTED EXPOSURE SETTINGS Salmonellosis For more informaon, visit publichealthontario.ca FOODBORN E I L L N E S S 1. Centers for Disease Control and Prevention. Incidence and trends of infection with pathogens transmitted commonly through food - foodborne diseases active surveillance network, 10 U.S. sites, 1996 - 2012. Morb Mortal Wkly Rep Surveill Summ 2013;62(15):283-87. 2. Data Source: Ontario. Ministry of Health and Long-Term Care, Integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario, Date Extracted: 2013 Dec 6. 3. Thomas MK, Murray R, Flockhart L, Pintar K, Pollari F, Fazil A, et al. Estimates of the burden of foodborne illness in Canada for 30 specified pathogens and unspecified agents, circa 2006. Foodborne Pathog Dis. 2013;10(7):639-48. 4. Scallan E, Griffin PM, Angulo FJ, Tauxe RV, Hoekstra RM. Foodborne illness acquired in the United States - unspecified agents. Emerg Infect Dis. 2011;17(1):16-22. 5. Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, et al. Foodborne illness acquired in the United States - major pathogens. Emerg Infect Dis. 2011;17(2):7-15. 6. Batz MB, Henke E, Kowalcyk B. Long-term consequences of foodborne infections. Inf Dis Clin N Am. 2013;27:599-616. 7. Data Source: Ontario. Ministry of Health and Long-Term Care, Integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario, Date Extracted: 2011 Oct 3. 8. FDA National Retail Food Team. FDA trend analysis report on the occurrence of foodborne illness risk factors in selected institutional foodservice, restaurant, and retail food store facility types (1998 – 2008). Silver Spring, MD: U.S. Food and Drug Administration; 2008. Available from: http://www.fda.gov/downloads/Food/GuidanceRegulation/RetailFoodProtection/FoodborneIllnessRiskFactorReduction/UCM369245.pdf 9. Centers for Disease Control and Prevention [Internet]. Atlanta, GA: Centers for Disease Prevention and Control. Food Safety. Prevention and education; 2013 Sep 6. Available from: http://www.cdc.gov/foodsafety/prevention.html Average annual incidence of foodborne illness * by age group, Ontario, 2006-2012 2 AGE Chicken 29 % Undetermined 23 % Beef 7 % Egg 7 % Campylobacter enteritis Chicken 38 % Undetermined 27 % Beef 7 % Dairy products 7 % Verotoxin-producing E. coli infection Undetermined 39 % Beef 32 % Other meat 16 % Produce 4 % Place where reported foodborne illnesses *§ were contracted, Ontario, 2007-2010 7 Restaurants Other sengs Other retail food establishments Private homes Average annual number of foodborne illnesses * by month, Ontario, 2006-2012 2 Reported cases of foodborne illness increase in summer months. SEASON 600 500 400 300 200 100 0 Jan Jun Jul Feb Mar May Apr Aug Sep Oct Nov Dec Average number of reported cases Average annual incidence per 100,000 populaon 80 70 60 50 40 30 20 10 0 <1 1-4 5-9 10-19 20-44 45-64 65+ Age group (years) 13 % 37 % 42 % *Refers to domestically-acquired, laboratory-confirmed cases in iPHIS 2 of Campylobacter enteritis, listeriosis, salmonellosis, verotoxin-producing E. coli infection, and yersiniosis. These are believed to be the top five reportable foodborne illnesses in Ontario. † Laboratory-confirmed domestic cases in iPHIS 2 of the top five reportable enteric illnesses*, adjusted for foodborne transmission, under-reporting and under-diagnosis. 3 ‡ Laboratory-confirmed cases of the top five reportable enteric illnesses* in iPHIS 2 believed to be attributed to food, adjusted for foodborne transmission and domestic acquisition. 3 § Based on domestically-acquired cases for which most likely exposure data were available. While reportable, not all cases of foodborne illness are captured. Reasons cases may not be captured include: • Symptomatic individuals do not seek medical attention • Symptomatic individuals seek medical attention but a lab test is not ordered • A lab test is ordered but the individual does not submit a specimen • A specimen is submitted but does not contain the organism resulting in a negative test • The organism causing the illness may be present but cannot be identified by the lab • A positive test result may not be reported to the health unit and entered in the tracking system • Cases may be entered in the tracking system but a link to food as the source of the illness may not be made 100,000 Estimated true † number of cases of foodborne illnesses * in Ontario each year 2 8 % ? ? ? Approximately 4 % of the estimated true number of cases of foodborne illness * are reported: Estimated known ‡ cases of foodborne illnesses * in Ontario each year 2 3,700 April 24, 2014
Transcript of PHO Infographic FoodborneIllness V7 copy€¦ · FDA National Retail Food Team. FDA trend analysis...

OCCURRENCE OF FOODBORNE ILLNESSES*
WHAT WE DON’T KNOW CAN HARM USThe burden of foodborne illness is estimated to be substantial.3-5
Although self-limited in most instances, serious health effects or death may occur.6 Determining the true impact foodborne illness
has on Ontario is difficult as it is underreported.
• Children are more likely to be diagnosed with foodborne illness• Adults aged 65 or older are most likely to be hospitalized or die as a result of infection¹
The top four food sources for reported cases of domestically-acquired foodborne illness§ in Ontario, 2007-2010, were:7
SUSPECTED FOOD SOURCES
Unsafe food practices can lead to foodborne illness. To reduce risk of contamination and illness:8,9
• Use proper hand hygiene • Obtain food from approved sources• Avoid cross-contamination • Follow safe cooking/preparation practices• Store food at appropriate temperatures
Encourage reporting of suspected cases of foodborne illness.
AN OUNCE OF PREVENTION
REPORTED EXPOSURE SETTINGS
Salmonellosis
For more information, visitpublichealthontario.ca
FOODBORNE ILLNESS
1. Centers for Disease Control and Prevention. Incidence and trends of infection with pathogens transmitted commonly through food - foodborne diseases active surveillance network, 10 U.S. sites, 1996 - 2012. Morb Mortal Wkly Rep Surveill Summ 2013;62(15):283-87. 2. Data Source: Ontario. Ministry of Health and Long-Term Care, Integrated Public Health Information System (iPHIS) database, extracted by
Public Health Ontario, Date Extracted: 2013 Dec 6. 3. Thomas MK, Murray R, Flockhart L, Pintar K, Pollari F, Fazil A, et al. Estimates of the burden of foodborne illness in Canada for 30 specified pathogens and unspecified agents, circa 2006. Foodborne Pathog Dis. 2013;10(7):639-48. 4. Scallan E, Griffin PM, Angulo FJ, Tauxe RV, Hoekstra RM. Foodborne illness acquired in the United States - unspecified agents.
Emerg Infect Dis. 2011;17(1):16-22. 5. Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, et al. Foodborne illness acquired in the United States - major pathogens. Emerg Infect Dis. 2011;17(2):7-15. 6. Batz MB, Henke E, Kowalcyk B. Long-term consequences of foodborne infections. Inf Dis Clin N Am. 2013;27:599-616. 7. Data Source: Ontario. Ministry of Health and Long-Term Care,
Integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario, Date Extracted: 2011 Oct 3. 8. FDA National Retail Food Team. FDA trend analysis report on the occurrence of foodborne illness risk factors in selected institutional foodservice, restaurant, and retail food store facility types (1998 – 2008). Silver Spring, MD: U.S. Food and Drug Administration; 2008. Available from:
http://www.fda.gov/downloads/Food/GuidanceRegulation/RetailFoodProtection/FoodborneIllnessRiskFactorReduction/UCM369245.pdf 9. Centers for Disease Control and Prevention [Internet]. Atlanta, GA: Centers for Disease Prevention and Control. Food Safety. Prevention and education; 2013 Sep 6. Available from: http://www.cdc.gov/foodsafety/prevention.html
Average annual incidence of foodborne illness* by age group, Ontario, 2006-20122
AGE
Chicken
29%Undetermined
23%Beef
7%Egg
7%
Campylobacter enteritis
Chicken
38%
Undetermined
27%
Beef
7%
Dairy products
7%
Verotoxin-producing E. coli infection
Undetermined39%
Beef
32%Other meat
16%Produce
4%
Place where reported foodborne illnesses*§
were contracted, Ontario, 2007-20107
Restaurants
Other settings
Other retail foodestablishments
Private homes
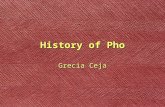
Average annual number of foodborne illnesses* by month, Ontario, 2006-20122
Reported cases of foodborne illness increase in summer months.
SEASON
600
500
400
300
200
100
0Jan Jun JulFeb Mar MayApr Aug Sep Oct Nov Dec
Aver
age
num
ber
of re
port
ed c
ases
Aver
age
annu
al in
cide
nce
per 1
00,0
00 p
opul
ation
80
70
60
50
40
30
20
10
0<1 1-4 5-9 10-19 20-44 45-64 65+
Age group (years)
13%
37%
42%
*Refers to domestically-acquired, laboratory-confirmed cases in iPHIS2 of Campylobacter enteritis, listeriosis, salmonellosis, verotoxin-producing E. coli infection, and yersiniosis. These are believed to be the top five reportable foodborne illnesses in Ontario. †Laboratory-confirmed domestic cases in iPHIS2 of the top five reportable enteric illnesses*, adjusted for foodborne transmission, under-reporting and under-diagnosis.3
‡Laboratory-confirmed cases of the top five reportable enteric illnesses* in iPHIS2 believed to be attributed to food, adjusted for foodborne transmission and domestic acquisition.3 §Based on domestically-acquired cases for which most likely exposure data were available.
While reportable, not all cases of foodborne illness are captured. Reasons cases may not be captured include: • Symptomatic individuals do not seek medical attention • Symptomatic individuals seek medical attention but a lab test is not ordered • A lab test is ordered but the individual does not submit a specimen • A specimen is submitted but does not contain the organism resulting in a negative test • The organism causing the illness may be present but cannot be identified by the lab • A positive test result may not be reported to the health unit and entered in the tracking system • Cases may be entered in the tracking system but a link to food as the source of the illness may not be made
100,000Estimated true† number of cases of foodborne illnesses* in Ontario each year2
8%
?
?
?Approximately 4% of the estimated true number of cases of foodborne illness* are reported:
Estimated known‡ cases of foodborne illnesses* in Ontario each year23,700
April 24, 2014