Pharyngitis n oral cavity
42
Oral cavity Foreign body in oropharynx Pharyngitis – Acute and chronic
-
Upload
kamal-ghimire -
Category
Health & Medicine
-
view
115 -
download
1
Transcript of Pharyngitis n oral cavity
Oral cavityForeign body in oropharynx
Pharyngitis – Acute and chronic

Presented by:
• Kamal Ghimire• Tsering dolma gurung• Gaurav jung karki

Oral cavityExtends from lip to the oropharyngeal isthmusCan be divided into 2 regions by upper and lower dental archs:a. Oral vestibule: between dental arches
and deep surfaces of cheeks and lipsb. oral cavity proper enclosed by dental
archades

Parts of oral cavity
Opening of Stensen's duct opposite second upper molar (arrow). Asterisk indicates retromolar trigone.
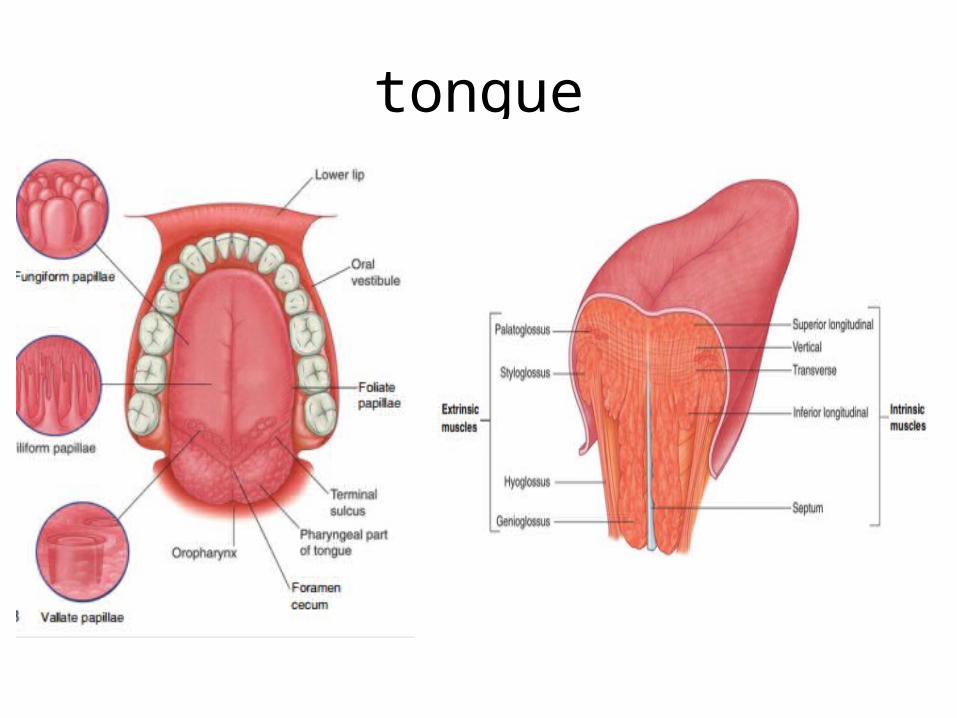
tongue
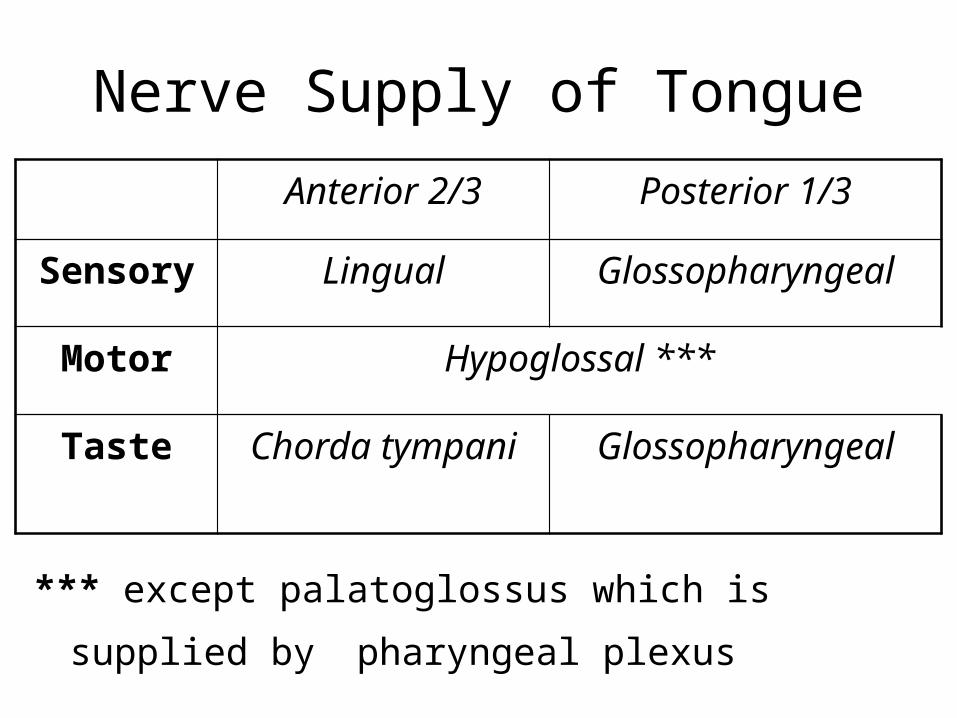
Nerve Supply of Tongue
*** except palatoglossus which is supplied by pharyngeal
plexus
Anterior 2/3 Posterior 1/3
Sensory Lingual Glossopharyngeal
Motor Hypoglossal ***
Taste Chorda tympani Glossopharyngeal
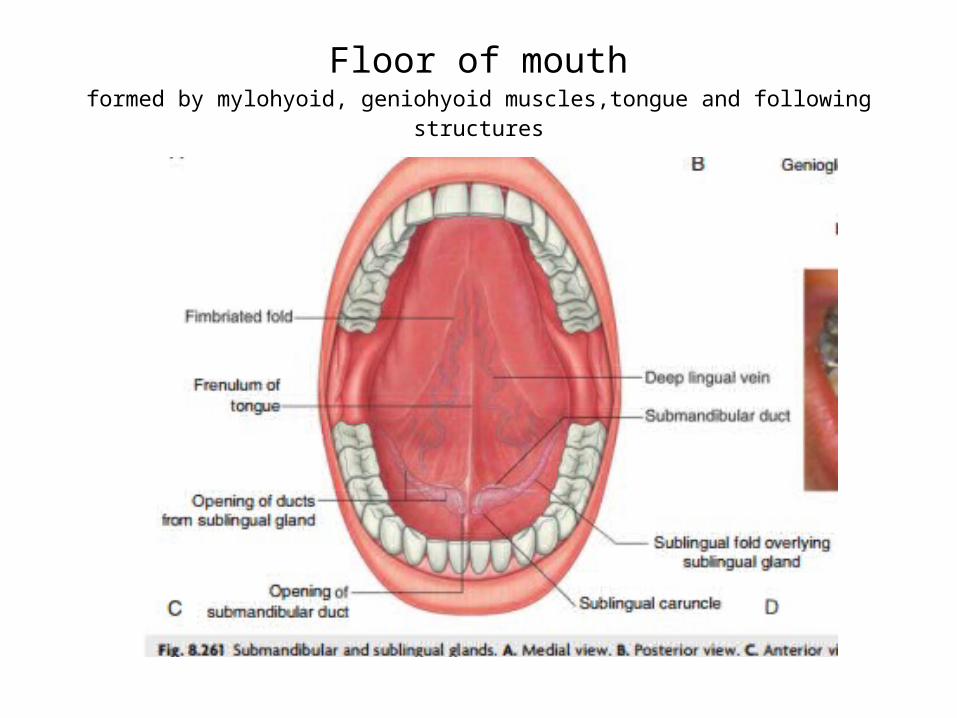
Floor of mouthformed by mylohyoid, geniohyoid muscles,tongue and following structures
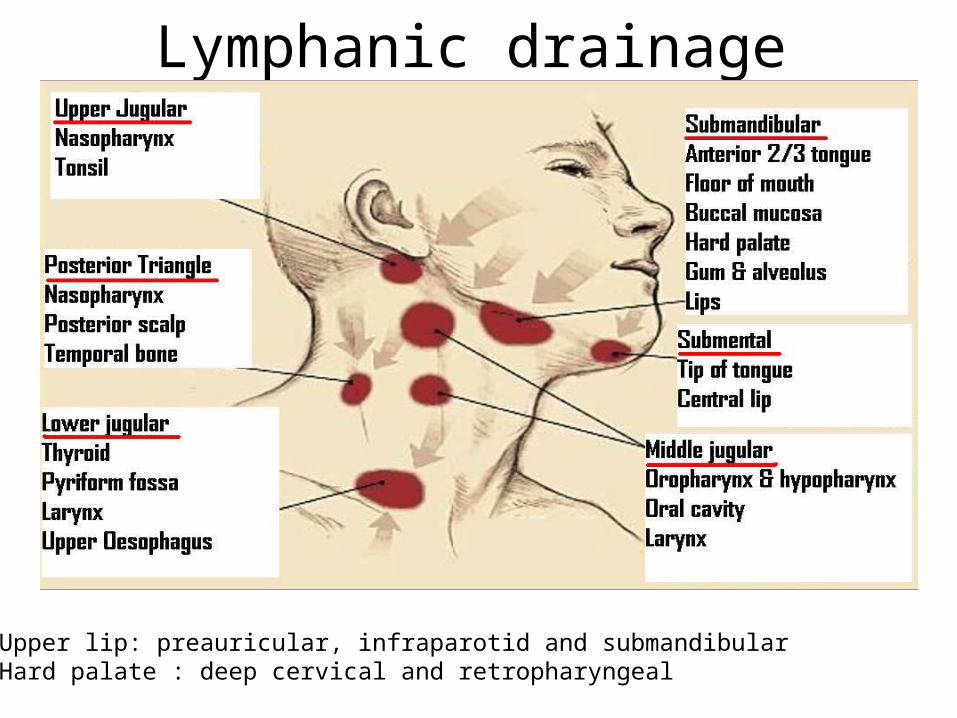
Lymphanic drainage
Upper lip: preauricular, infraparotid and submandibularHard palate : deep cervical and retropharyngeal

Oropharyngeal isthmus
It is the opening between oral cavity and oropharynx formed :• Laterally by palatoglosssus arches
• Superiorly by soft palate ( at the junction of soft palate and hard
palate
• Inferiorly by sulcus terminalis of tongue that divides oral surface of tongue( anterior 2/3rd ) from pharyngeal surface( posterior1/3rd )
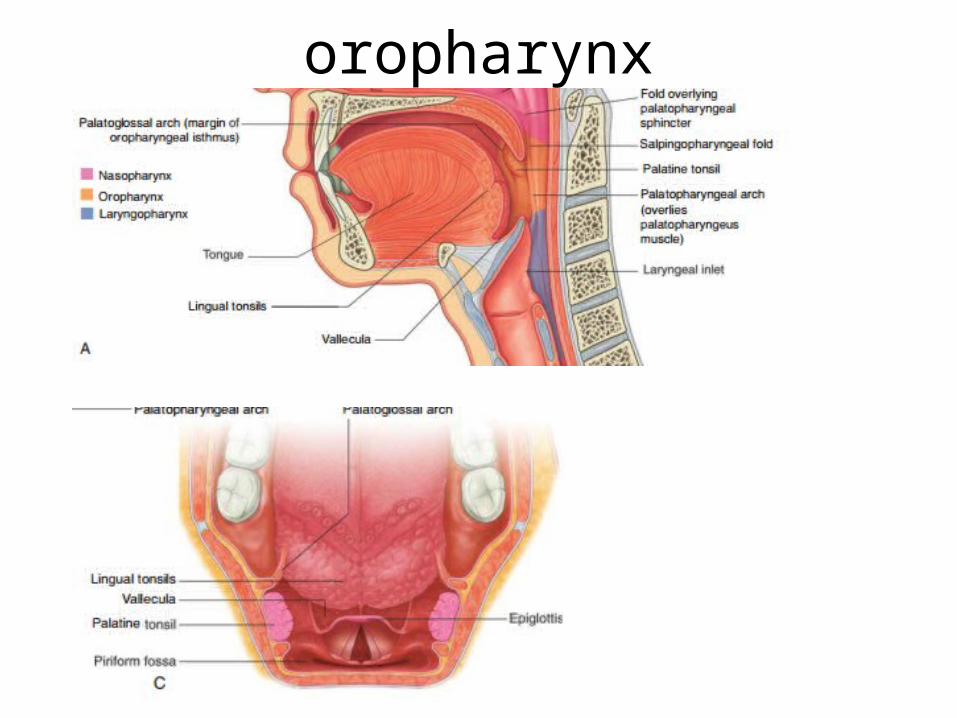
oropharynx
Foreign body in oropharynx

Etiology
• Age : children mostly below 5 years• Loss of protective mechansm :loss of
consciousness, seizures,deep sleep, alcohol• Carelessness• Psychotics
In the following structures of oropharynx foreign body can lodge1. The tonsil2. Base of tongue/ vallecula3. Posterior pharyngeal wall
Tonsil
• Usually it is a sharp fish bone or needle in one the tonsillar crepts.
• It can be easily observed by oropharyngeal examination and removed
• During swallowing, the soft palate is initially tensed to squeeze the bolus of food between the tongue and pharynx before elevation of the soft palate to block the nasal passages while the bolus is propelled into the pharynx. [
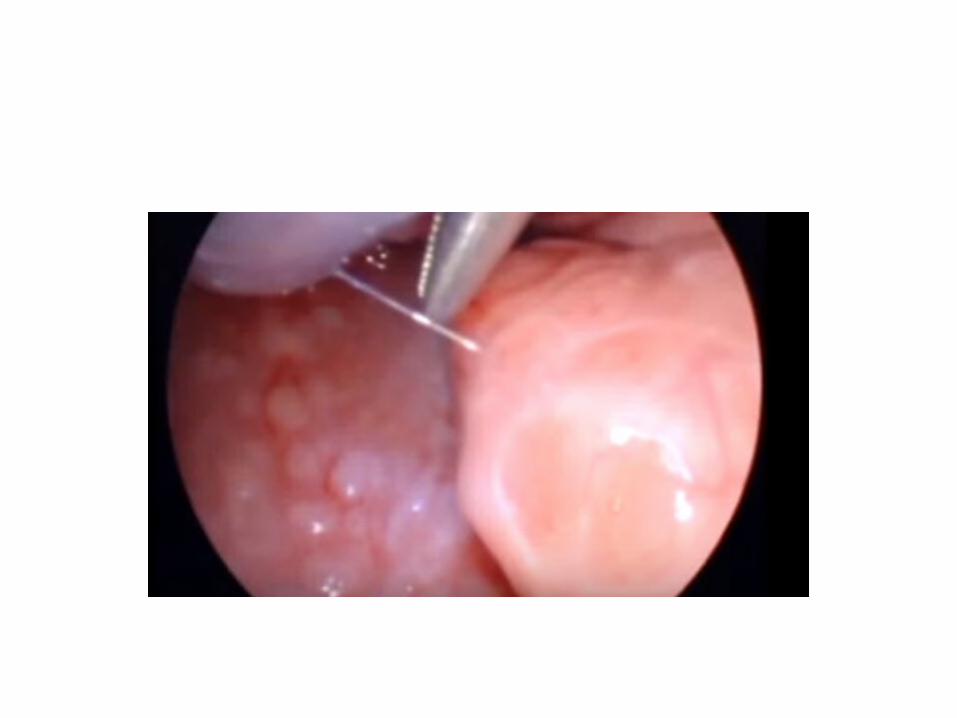

Base of tongue
• Usually fish bone or needle• Observed by indirect laryngoscopy. Removed
using curved forceps with the help of mirror or endoscopy.
• If foreign body get totally embedded in its substance, it can be diagnosed by radiology.

Posterior pharyngeal wall
• Usually wire, needle or staple can transfixed when taken with food accidently
• Can be observed by orophryngeal examination and removed with a curved forceps
Clinical features
• Discomfort or pain• DysphagiaOropharyngeal examination is mainstay of diagnosing.X rays may be required: Posteroanterior and lateral view can show radioopaque foreign bodies embedded in substance of pharynxTreatment : removal of foreign body by hypopharyngoscopy

Acute Pharyngitis
Causes of acute pharyngitis• VIRUS
Rhinoviruses InfluenzaParainfluenzaMeaslesChickenpoxCoxsackie virusHerpes simplexInfectious mononucleosisCytomegalovirus

• BACTERIA Streptococcus (Group A, Beta-hemolyticus) Diphtheria Gonococcus
• FUNGI Candida albicans
• MISCELLANEOUSChlamydia trachomatisToxoplasmosis (parasitic)
CLINICAL FEATURES
• Mild pharyngitisdiscomfort in throatlow grade fevermalaise Congested pharynxNo lymphadenopathy

• Moderate and severe pharyngitisPain in throatDysphagiaHigh fever with headache and malaisePharynx: Erythema, Exudate, Enlargement of
tonsils and lymphoid follicles on the posterior pharyngeal wall

• Very severe forms Edema of soft palate and uvulaEnlargement of cervical nodes

Diagnosis• Culture of throat swab helps in diagnosing
bacterial pharyngitis.• Failure to get any bacterial growth suggests
viral etiology.

Treatment
• General measuresBed restPlenty of fluidWarm saline gargles or pharyngeal irrigationsAnalgesicsIn severe cases, lignocaine viscous before meal
• Specific treatmentStreptococcal pharyngitis Penicillin G 200000-
250000 units orally 4 times a day for 10 days or Benzathine penicillin G once im -600000 units(60lb) or 1.2 million units (>60lb) or erythromycin
Diphtheria Diphtheria antitoxin , Penicillin or erythromycin
Gonococcal pharyngitis Penicillin or tetracycline

Viral infections causing pharyngitis• HERPANGINA
Group A coxsackie virusAffects childrenFever, sore throat, vesicles on soft palate and pillars
• ACUTE LYMPHONODULAR PHARYNGITISCoxsackie virusFever, malaise,sore throatWhite-yellow solid nodules on posterior pharyngeal wall
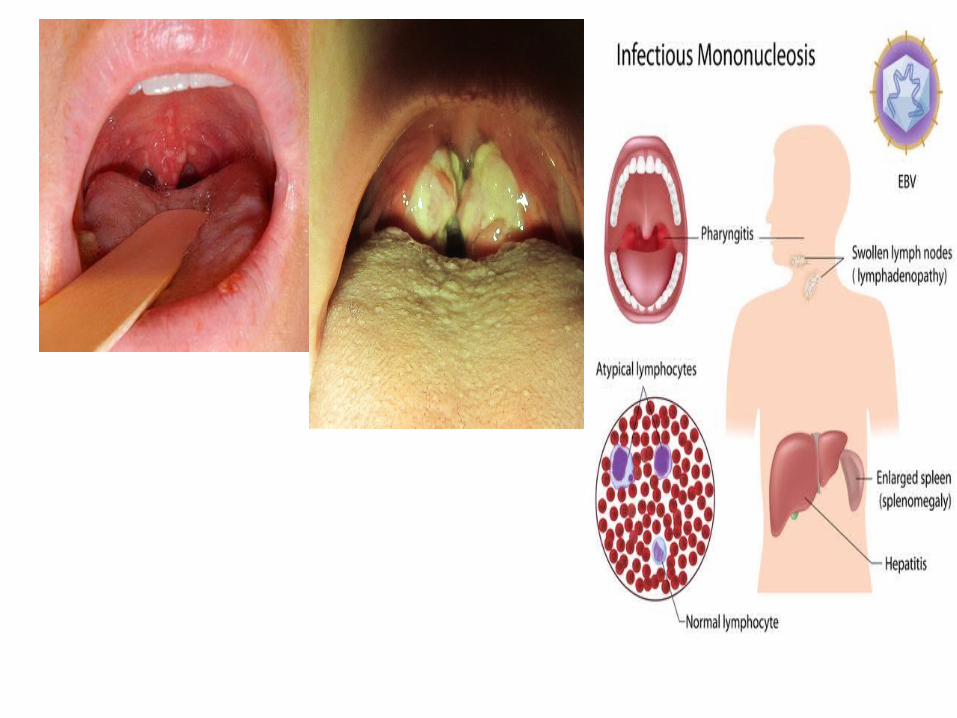
• INFECTIOUS MONONUCLEOSISEpstein-Barr virusAffects older children and young adultsFever, sore throat, exudative pharyngitis,
lymphadenopathy, splenomegaly, hepatitisPaul-Bunnell test

• CYTOMEGALOVIRUSAffects immunocompromised transplant patientsMimics infectious mononucleosis but heterophil
antibody test is negative
• PHARYGOCONJUNCTIVAL FEVERAdenovirusFever, sore throat, conjunctivitisMay mimic appendicitis
• MEASLES AND CHICKENPOXIn measles, Koplik’s spots on buccal mucosa opposite
molar teeth
FUNGAL PHARYNGITIS– Candida albicans– Extension of oral thrush– Seen in patients who are immunocompromised,
debilitated, taking high doses of antimicrobials– Pain in throat + Dysphagia– DOC: Nystatin

Chronic pharyngitis

• Chronic inflammatory condition of pharynx
• Hypertrophy of mucosa, seromucinous glands, subepithelial lymphoid follicles and the muscular coat of the pharynx
• Consist of two types - Chronic catarrhal pharyngitis - Chronic hypertrophic(Granular) pharyngitis

AETIOLOGY
• Persistent infection in the neighborhood: - purulent discharge in chronic rhinitis and sinusitis => constant source of infection causing hypertrophy of pharyngeal bands - also in chronic tonsillitis and dental sepsis • Mouth breathing: exposes the pharynx to
unfiltered unhumidified and unadjusted to body temp air
• Chronic irritation: smoking, chewing of tobacco and pan, heavy drinking and heavy spiced foods.
• Environmental pollution• Faulty voice production

SYMPTOMS
• Discomfort or pain in the throat • Foreign body sensation in throat :
swallowing,hawking• Tiredness of voice• Cough

SIGNS• Chronic catarrhal pharyngitis - congestion of post. pharyngeal wall with engorgement of vessels; faucial pillars may be thickened - increased mucus secretion,covering pharyngeal mucosa• Chronic hypertrophic pharyngitis - above features - reddish nodules in post pharyngeal wall(hypertrophied subepithelial lumphoid follicles) - hypertrophied pharyngeal bands and elongated and enlarged uvula


TREATMENT
• Aetiological factor should be sought and eradicated.
• Habits like hawking,clearing throat frequently should be stopped.
• Warm saline gargles are soothing and relieve discomfort
• Mandl's paint(compound Iodine paint) applied to pharyngeal mucosa
• Cautery of lymphoid granules is suggested.

Mandl’s paint

Thank you