
Pharmacy Essential Updates August 2021
82
Pharmacy Essential Updates August 2021 Rachel Maynard, PharmD Editor Vickie Danaher, PharmD Associate Editor Pharmacist’s Letter | Pharmacy Technician’s Letter Copyright © Therapeutic Research Center. All rights reserved.
Transcript of Pharmacy Essential Updates August 2021
Pharmacy Essential Updates August 2021
Rachel Maynard, PharmDEditorVickie Danaher, PharmDAssociate Editor Pharmacist’s Letter | Pharmacy Technician’s Letter
Copyright © Therapeutic Research Center. All rights reserved.
▪ Pharmacist's Letter / TRC Healthcare is accredited by the
Accreditation Council for Pharmacy Education (ACPE) as
a provider of continuing pharmacy education.
▪ Pharmacy Essential Updates editors disclose:
» No financial interests related to the content
» No commercial support and no advertising
» Supported entirely by subscriptions
CE Information
Copyright © Therapeutic Research Center. All rights reserved.
▪ Identify emerging trends in drug therapy and their place
in patient care practices.
▪ Discuss the use of injectable semaglutide for weight loss.
▪ Recommend appropriate treatment for rheumatoid
arthritis.
▪ State two considerations regarding rimegepant ODT for
migraine prevention.
▪ Describe four strategies to treat hypo- or hyperkalemia
in patients with heart failure.
Pharmacist Objectives
Copyright © Therapeutic Research Center. All rights reserved.
▪ Identify emerging trends in drug therapy and their place
in pharmacy practice and operations.
▪ Describe three key points about injectable semaglutide
for weight loss.
▪ Discuss treatment options for rheumatoid arthritis.
▪ Name two considerations regarding rimegepant ODT for
migraine prevention.
▪ Explain four strategies that may be used to treat low or
high potassium levels in patients with heart failure.
Pharmacy Technician Objectives
Copyright © Therapeutic Research Center. All rights reserved.

Injectable Product for Weight Loss
Copyright © Therapeutic Research Center. All rights reserved.

OBESITY & WEIGHT LOSS
Pharmacist's Letter. August 2021, No. 370802
Emphasize Lifestyle Changes for Obesity Before Wegovy
Copyright © Therapeutic Research Center. All rights reserved.
New Rx Wegovy for weight loss will hit your pharmacy shelves. It's injectable semaglutide...the same GLP-1 agonist as injectable Ozempic or oral Rybelsus for type 2 diabetes. Explain that Wegovy starts at the same 0.25 mg weekly dose as Ozempic...but titrates to 2.4 mg. Ozempic maxes out at 1 mg weekly. Using Wegovy 2.4 mg weekly for about a year leads to roughly 10% to 12% more weight loss than with placebo, or 20 lb for a 200 lb patient. This is about double the weight loss with daily Saxenda (liraglutide), the other GLP-1 agonist for obesity...and similar to Qsymia (phentermine/topiramate ER). Other Rx meds lead to less weight loss. Educate that GI side effects are common with Wegovy. But most patients can tolerate it if titrated appropriately...over 16 weeks. Balance this against downsides of other weight loss meds. For example, Qsymia has a REMS program due to the risk of birth defects. Point out that weight loss meds often aren't covered by payers. Wegovy or Saxenda costs about $1,400/month...versus $200/month for Qsymia. Continue to emphasize lifestyle changes BEFORE weight loss meds. Don't jump to discussing meds unless patients have a BMI of 30 or more...or 27 or more plus a weight-related condition (diabetes, etc). Lean toward Wegovy if a GLP-1 agonist is preferred for weight loss. But advise stopping the med if 2.4 mg/week isn't tolerated...or patients don't lose 5% of their body weight after 12 weeks at this dose. Expect long-term use for patients who are successful. Don't recommend combining Wegovy with other weight loss meds...due to lack of evidence. And avoid combining it with other GLP-1 agonists...or DPP-4 inhibitors (Januvia, etc), which work similarly. Compare options in our chart, Weight Loss Products. And get our toolbox, Weight Loss: Helping Your Overweight Patients, for advice on suggested diets, physical activity, and helping patients reach goals.
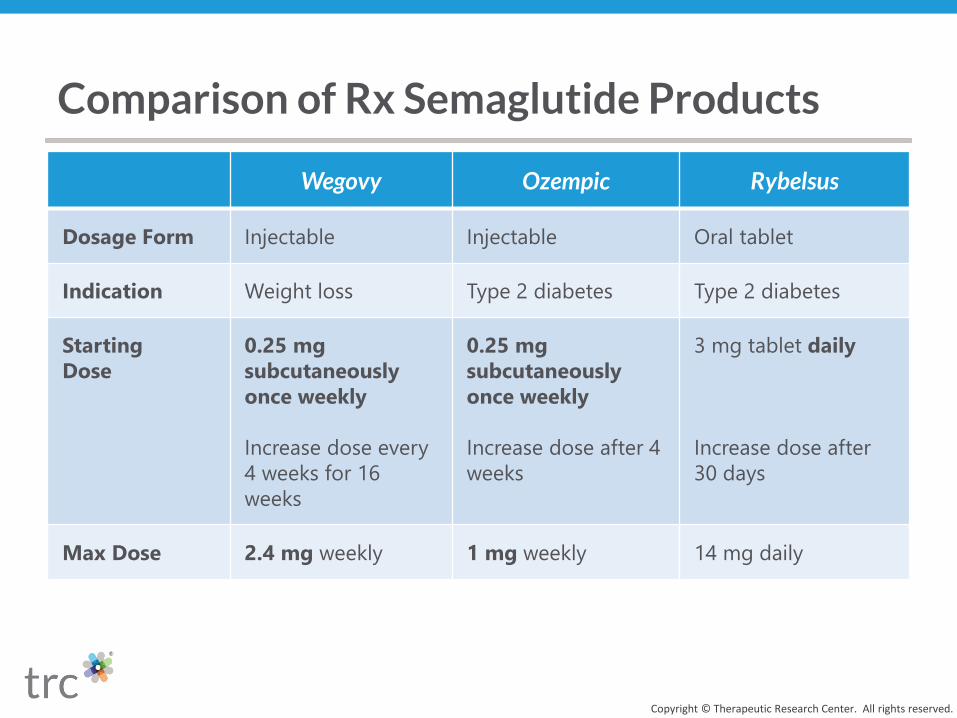
Wegovy Ozempic Rybelsus
Dosage Form Injectable Injectable Oral tablet
Indication Weight loss Type 2 diabetes Type 2 diabetes
Starting
Dose
0.25 mg
subcutaneously
once weekly
Increase dose every
4 weeks for 16
weeks
0.25 mg
subcutaneously
once weekly
Increase dose after 4
weeks
3 mg tablet daily
Increase dose after
30 days
Max Dose 2.4 mg weekly 1 mg weekly 14 mg daily
Comparison of Rx Semaglutide Products
Copyright © Therapeutic Research Center. All rights reserved.
Copyright © Therapeutic Research Center. All rights reserved.
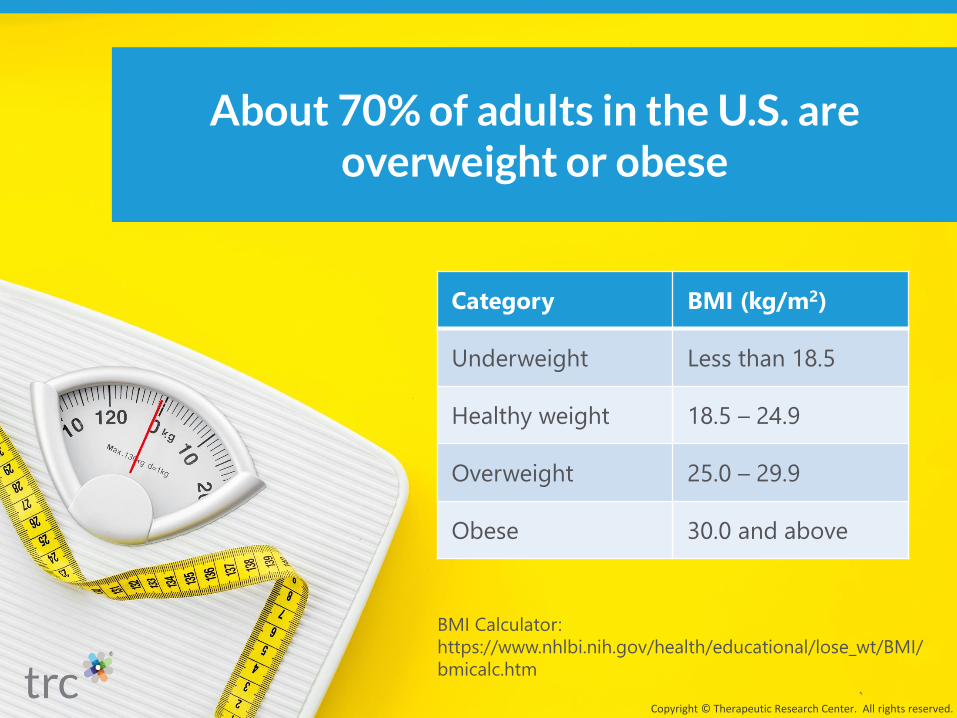
About 70% of adults in the U.S. are overweight or obese
Category BMI (kg/m2)
Underweight Less than 18.5
Healthy weight 18.5 – 24.9
Overweight 25.0 – 29.9
Obese 30.0 and above
BMI Calculator:
https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/
bmicalc.htm
▪ Being overweight or obese
increases the risk of:
» Heart disease, stroke, diabetes,
some cancers, etc
▪ A 5% to 10% drop in weight
may improve blood pressure,
cholesterol, and glucose
Impact of Weight
Copyright © Therapeutic Research Center. All rights reserved.

Case: Gloria
Copyright © Therapeutic Research Center. All rights reserved.
Current Medications
Drug Strength Sig
Metformin 500 mg Take 1 tablet by mouth twice
daily
Lisinopril 20 mg Take 1 tablet by mouth daily
Norethindrone/ethinyl
estradiol
1 mg/20
mcg
Take 1 tablet by mouth daily
for 28 days
Medical Conditions
Type 2 Diabetes
Hypertension
Patient Details
Name: Gloria Hernandez
DOB: 02/17/1975
Age: 46
Tobacco Use: N
BMI: 28
Allergies
Penicillin

▪ Leads to roughly 10% to
12% more weight loss than
with placebo after ~1 year
» About double the weight loss
than liraglutide (Saxenda)
» Similar to phentermine/
topiramate ER (Qsymia)
▪ Other Rx meds lead to less
weight loss
Wegovy Efficacy
Copyright © Therapeutic Research Center. All rights reserved.

Selected Weight Loss Products
Copyright © Therapeutic Research Center. All rights reserved.
Drug
(Brand)Usual Dosing
~Cost/
MonthComments
Injectable
semaglutide
(Wegovy)
2.4 mg once weekly
(0.25 mg once weekly, increase every four
weeks to 0.5 mg, 1 mg, 1.7 mg, and 2.4 mg)
$1,400 GI side effects
are common
Injectable
liraglutide
(Saxenda)
3 mg once daily
(0.6 mg once daily, increase weekly by
0.6 mg to 3 mg once daily)
$1,400 GI side effects
are common
Phentermine/
topiramate ER
(Qsymia)
7.5 mg/46 mg once daily
3.75 mg/23 mg PO once daily for 14 days,
then double the dose
$200 REMS program
(risk of birth
defects)
Medication pricing by Elsevier, accessed July 2021
Copyright © Therapeutic Research Center. All rights reserved.
Continue to emphasize lifestyle changes BEFORE
weight loss meds.

Reduced-Calorie Diet
▪ 1,200 to 1,500
kcal/day for women
▪ 1,500 to 1,800
kcal/day for men
Physical Activity
▪ 30 to 45 minutes,
3 to 5 days a week
Behavior Therapy
▪ Counseling,
education, or
support for at least
6 months
Lifestyle Changes for Weight Loss
Copyright © Therapeutic Research Center. All rights reserved.

Don’t jump to discussing meds unless patients have a BMI of 30 or more...or
27 or more plus a weight-related condition (diabetes, etc).
Copyright © Therapeutic Research Center. All rights reserved.
▪ Don’t recommend
combining with other
weight loss meds
▪ Avoid combining with
» Other GLP-1 agonists
▪ Exenatide, etc
» DPP-4 inhibitors
▪ Sitagliptin, etc
Wegovy Considerations
Copyright © Therapeutic Research Center. All rights reserved.
▪ Advise stopping if
» 2.4 mg/week isn’t tolerated
» Patients don’t lose 5% of body
weight after 12 weeks at this dose
▪ Expect long-term use for
patients who are successful
Wegovy Considerations
Copyright © Therapeutic Research Center. All rights reserved.

▪ Choose products carefully
» 0.25 mg/0.5 mL, 0.5 mg/0.5 mL, 1 mg/0.5 mL, 1.7 mg/0.75 mL,
2.4 mg/0.75 mL
▪ Enter a 28 days’ supply
» Four pens/box x 1 pen/7 days
▪ Don’t substitute Wegovy for Ozempic, or vice versa
Practice Pearls: Wegovy
Copyright © Therapeutic Research Center. All rights reserved.

▪ Tell patients to store Wegovy in the fridge
» If needed, a pen can be kept at room temp for up to 28 days
▪ Counsel on administration
» Injected subcutaneously in the abdomen, thigh, or upper arm
Practice Pearls: Wegovy
Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.
Copyright © Therapeutic Research Center. All rights reserved.
Rheumatoid Arthritis Meds
Copyright © Therapeutic Research Center. All rights reserved.

New guidelines will lead to questions about treating rheumatoid arthritis...especially with the plethora of med options.Which med is first-line? Recommend sticking with oral methotrexate 7.5 mg once weekly for most patients. Generally advise titrating to at least 15 mg/week within 4 to 6 weeks...and up to 25 mg/week if needed.But be aware that hydroxychloroquine or sulfasalazine can be enough for patients with low disease activity...and tend to be better tolerated.What are tips to optimize methotrexate? Educate all patients on methotrexate to take folic acid...usually 1 mg/day...to limit GI upset, liver damage, mouth sores, etc.Explain that it's okay to take folic acid and methotrexate on the same day...there's no proof this reduces methotrexate efficacy.Consider additional strategies if GI upset is an issue...or there's an inadequate response to higher doses of oral methotrexate.For example, suggest splitting once-weekly oral methotrexate into 2 doses given 12 hours apart on the same day. Or advise changing to subcutaneous methotrexate before adding or switching to other meds.What are considerations with oral steroids? Suggest limiting them to the lowest dose and shortest duration possible.And don't automatically recommend adding steroids when starting treatment. Risks often outweigh benefits...and patients may not want to taper off due to fear of having a disease flare.What if methotrexate isn't enough? Weigh pros and cons of adding another med after at least 3 months of optimized methotrexate.For instance, point out that biologics (Humira, etc) are injectable...but many have a longer track record than oral Janus kinase inhibitors (Xeljanz, etc), whose risks are piling up (thrombosis, etc).Find med dosing and monitoring advice in our charts, DMARDs for Rheumatoid Arthritis and Biologics for Rheumatoid Arthritis.
Pharmacist's Letter. August 2021, No. 370805
RHEUMATOID ARTHRITIS
Help Patients Stick With Methotrexate for Rheumatoid Arthritis
Copyright © Therapeutic Research Center. All rights reserved.

▪ Autoimmune disease that
causes the body to attack
the joints
» Joint pain, stiffness, damage
▪ Disease-modifying
antirheumatic drugs
(DMARDs) can help
» Gain control
» Slow further joint damage
Rheumatoid Arthritis
Copyright © Therapeutic Research Center. All rights reserved.

DMARDs for Rheumatoid Arthritis
Copyright © Therapeutic Research Center. All rights reserved.
Sulfasalazine
Hydroxychloroquine
Methotrexate
Biologics (Humira, etc)
JAK inhibitors (Xeljanz, etc)

Which med is first-line?
Copyright © Therapeutic Research Center. All rights reserved.

▪ Recommend oral
methotrexate 7.5 mg once
weekly for most patients
▪ Generally titrate to
» At least 15 mg/week within 4
to 6 weeks
» Up to 25 mg/week if needed
First-Line Meds
Copyright © Therapeutic Research Center. All rights reserved.
▪ Hydroxychloroquine or
sulfasalazine can be enough
» For patients with low disease
activity
» Tend to be better tolerated
First-Line Meds
Copyright © Therapeutic Research Center. All rights reserved.
What are tips to optimize methotrexate?
Copyright © Therapeutic Research Center. All rights reserved.
Educate all patients on methotrexate to take folic acid...usually 1 mg/day...to
limit GI upset, liver damage, mouth sores, etc.
Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.
Explain that it’s okay to take folic acid on the
same day as methotrexate.
Strategies to Improve Tolerability or Efficacy
Copyright © Therapeutic Research Center. All rights reserved.
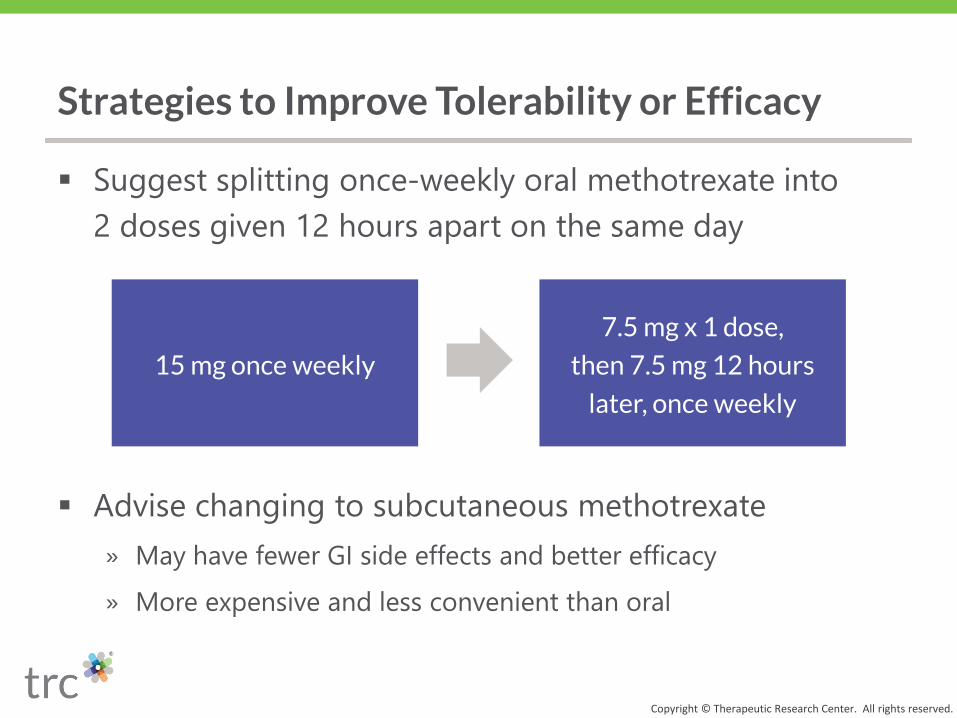
▪ Suggest splitting once-weekly oral methotrexate into
2 doses given 12 hours apart on the same day
▪ Advise changing to subcutaneous methotrexate
» May have fewer GI side effects and better efficacy
» More expensive and less convenient than oral
15 mg once weekly
7.5 mg x 1 dose,
then 7.5 mg 12 hours
later, once weekly

What if methotrexate isn’t enough?
Copyright © Therapeutic Research Center. All rights reserved.
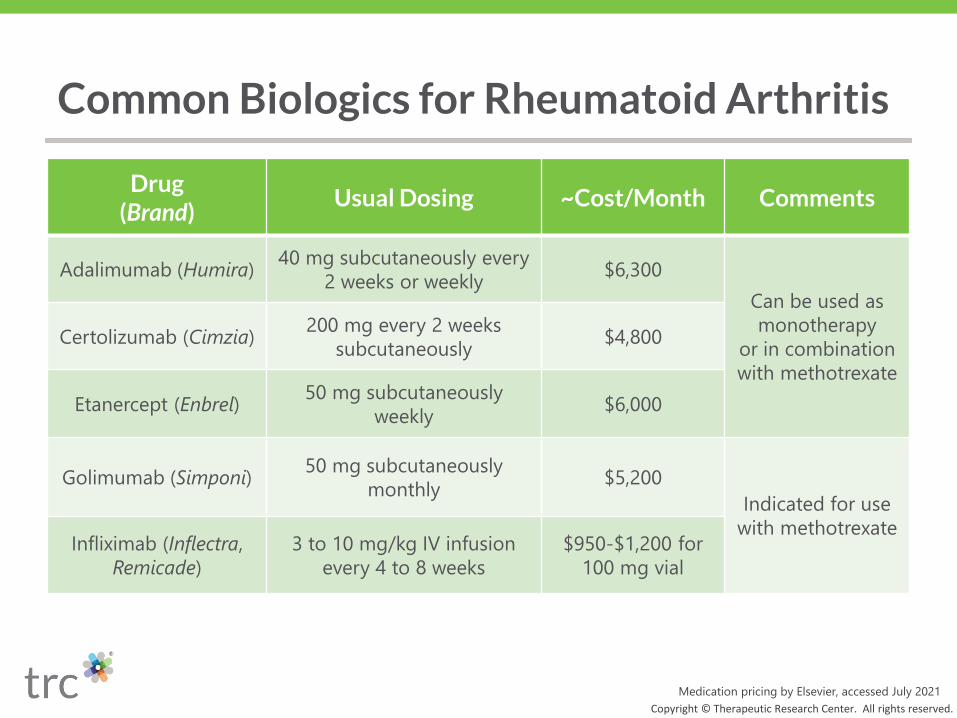
Common Biologics for Rheumatoid Arthritis
Copyright © Therapeutic Research Center. All rights reserved.
Drug (Brand)
Usual Dosing ~Cost/Month Comments
Adalimumab (Humira)40 mg subcutaneously every
2 weeks or weekly$6,300
Can be used as
monotherapy
or in combination
with methotrexate
Certolizumab (Cimzia)200 mg every 2 weeks
subcutaneously$4,800
Etanercept (Enbrel)50 mg subcutaneously
weekly$6,000
Golimumab (Simponi)50 mg subcutaneously
monthly$5,200
Indicated for use
with methotrexateInfliximab (Inflectra,
Remicade)
3 to 10 mg/kg IV infusion
every 4 to 8 weeks
$950-$1,200 for
100 mg vial
Medication pricing by Elsevier, accessed July 2021
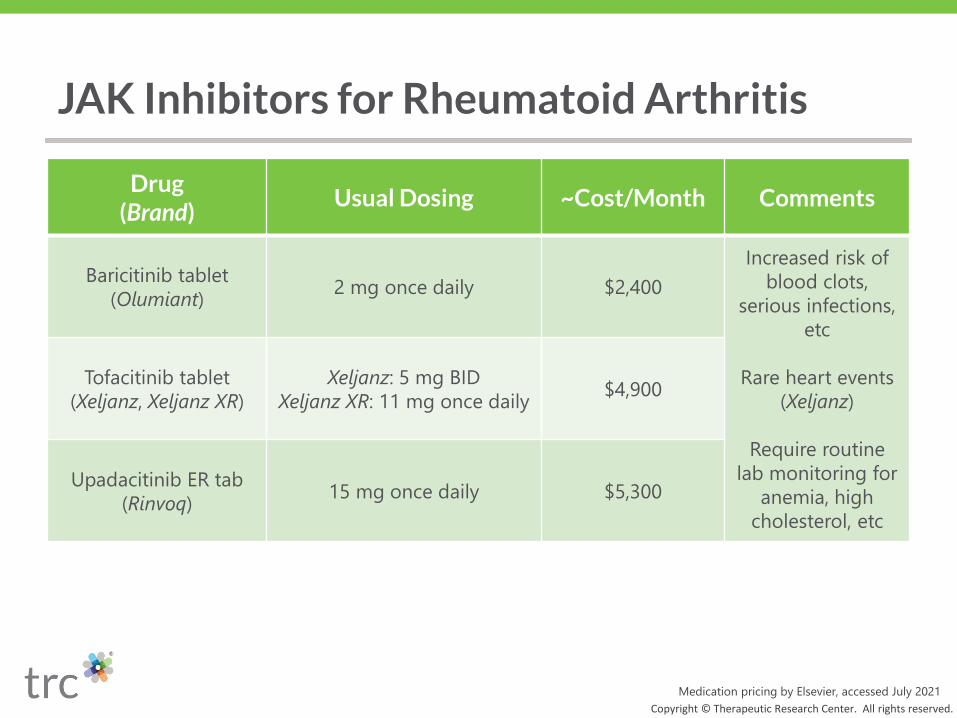
JAK Inhibitors for Rheumatoid Arthritis
Copyright © Therapeutic Research Center. All rights reserved.
Medication pricing by Elsevier, accessed July 2021
Drug (Brand)
Usual Dosing ~Cost/Month Comments
Baricitinib tablet
(Olumiant)2 mg once daily $2,400
Increased risk of
blood clots,
serious infections,
etc
Rare heart events
(Xeljanz)
Require routine
lab monitoring for
anemia, high
cholesterol, etc
Tofacitinib tablet
(Xeljanz, Xeljanz XR)
Xeljanz: 5 mg BID
Xeljanz XR: 11 mg once daily$4,900
Upadacitinib ER tab
(Rinvoq)15 mg once daily $5,300
▪ Triple-check methotrexate sigs
» Usually dosed once WEEKLY for rheumatoid arthritis...but DAILY
for some cancers
▪ Watch out for look-alike/sound-alike mix-ups
» Hydroxychloroquine with hydroCHLOROthiazide or hydrOXYzine
» SulfaSALAzine with sulfADIAZINE or sulfamethoxazole
Practice Pearls: Rheumatoid Arthritis Meds
Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.

Rimegepant ODT for Migraine Prevention
Copyright © Therapeutic Research Center. All rights reserved.
MIGRAINE
Pharmacist's Letter. August 2021, No. 370804
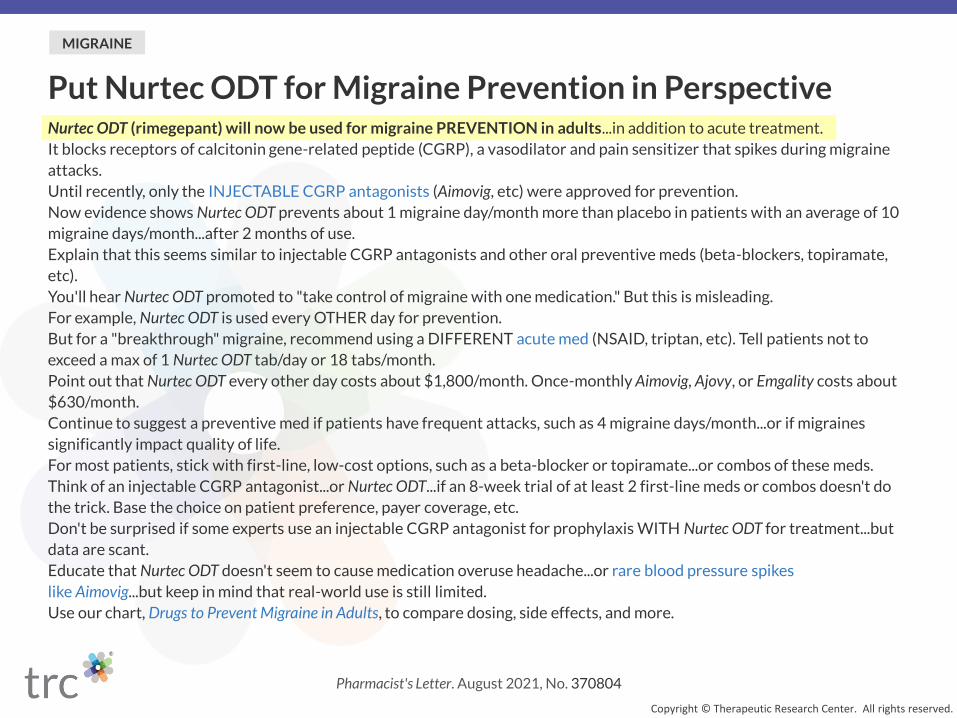
Put Nurtec ODT for Migraine Prevention in PerspectiveNurtec ODT (rimegepant) will now be used for migraine PREVENTION in adults...in addition to acute treatment.
It blocks receptors of calcitonin gene-related peptide (CGRP), a vasodilator and pain sensitizer that spikes during migraine
attacks.
Until recently, only the INJECTABLE CGRP antagonists (Aimovig, etc) were approved for prevention.
Now evidence shows Nurtec ODT prevents about 1 migraine day/month more than placebo in patients with an average of 10
migraine days/month...after 2 months of use.
Explain that this seems similar to injectable CGRP antagonists and other oral preventive meds (beta-blockers, topiramate,
etc).
You'll hear Nurtec ODT promoted to "take control of migraine with one medication." But this is misleading.
For example, Nurtec ODT is used every OTHER day for prevention.
But for a "breakthrough" migraine, recommend using a DIFFERENT acute med (NSAID, triptan, etc). Tell patients not to
exceed a max of 1 Nurtec ODT tab/day or 18 tabs/month.
Point out that Nurtec ODT every other day costs about $1,800/month. Once-monthly Aimovig, Ajovy, or Emgality costs about
$630/month.
Continue to suggest a preventive med if patients have frequent attacks, such as 4 migraine days/month...or if migraines
significantly impact quality of life.
For most patients, stick with first-line, low-cost options, such as a beta-blocker or topiramate...or combos of these meds.
Think of an injectable CGRP antagonist...or Nurtec ODT...if an 8-week trial of at least 2 first-line meds or combos doesn't do
the trick. Base the choice on patient preference, payer coverage, etc.
Don't be surprised if some experts use an injectable CGRP antagonist for prophylaxis WITH Nurtec ODT for treatment...but
data are scant.
Educate that Nurtec ODT doesn't seem to cause medication overuse headache...or rare blood pressure spikes
like Aimovig...but keep in mind that real-world use is still limited.
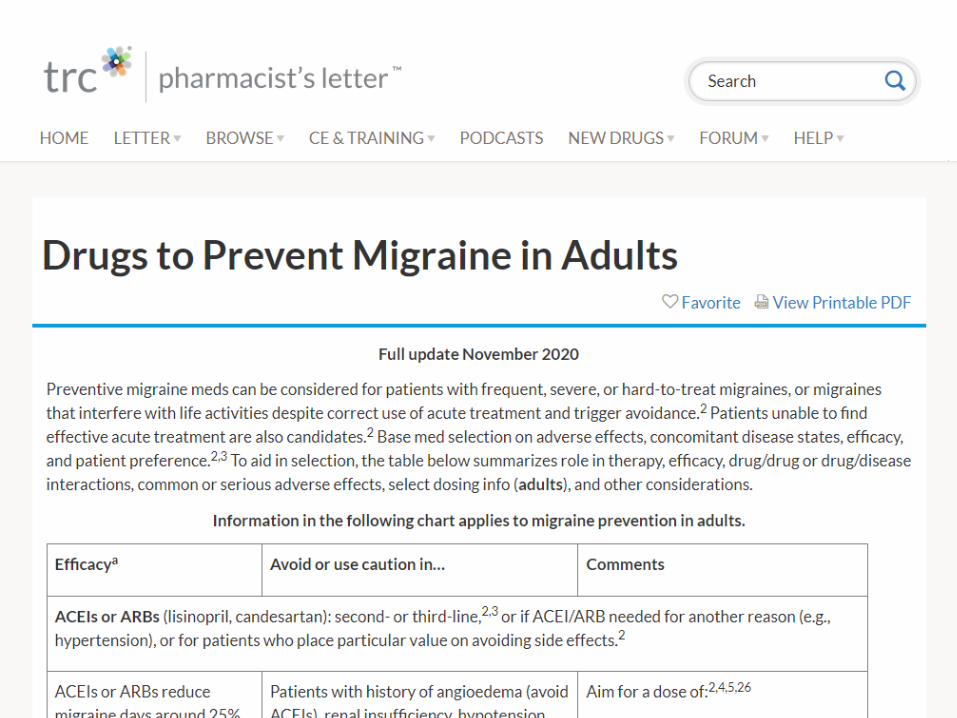
Use our chart, Drugs to Prevent Migraine in Adults, to compare dosing, side effects, and more.
Copyright © Therapeutic Research Center. All rights reserved.

Case
Rimegepant (Nurtec ODT) 75 mg
Take one tablet every other day
#16
Refills: 1 2 3 4 5 NRO Matt Welker
Smithfield Medical Group
234 Main Street
Somecity, ST 10001
Patient: Angeline Considine
DOB: 8/28/93

▪ Calcitonin gene-related peptide (CGRP) is a vasodilator
and pain sensitizer that spikes during migraine attacks
CGRP Antagonists
CGRP Antagonists
CGRP
CGRP Receptor

CGRP Antagonists
CGRP
CGRP Receptor
▪ CGRP antagonists either:
» Block CGRP receptors
» Bind CGRP so it can’t bind to receptors
CGRP Antagonists
Bound CGRP
Blocked CGRP
Receptor

▪ Erenumab (Aimovig)
▪ Fremanezumab (Ajovy)
▪ Galcanezumab
(Emgality)
▪ Eptinezumab (Vyepti)
▪ Rimegepant
(Nurtec ODT)
▪ Ubrogepant (Ubrelvy)
Injectable Oral
CGRP Antagonists
Copyright © Therapeutic Research Center. All rights reserved.
Rimegepant ODT for Migraine Prevention
Copyright © Therapeutic Research Center. All rights reserved.
Prevents about 1 migraine day/month more
than placebo in patients with ~10 migraine
days/month after 2 months of use
Seems similar to injectable CGRP antagonists
and other oral preventive meds

Copyright © Therapeutic Research Center. All rights reserved.
This is misleading.
“Take control of migraine with one
medication.”

Rimegepant ODT for Migraine: Dosing
Copyright © Therapeutic Research Center. All rights reserved.
75 mg every other day 75 mg/day as needed
Prevention Acute Treatment
1 tablet/day
18 tablets/month
Maximum
For a “breakthrough” migraine, recommend using a different acute med
(NSAID, triptan, etc).
Copyright © Therapeutic Research Center. All rights reserved.
▪ Rimegepant ODT
» Every other day
» ~$1,800/month
▪ Most injectable CGRP
antagonists
» Can be dosed once monthly
» ~$630/month
Meds for Migraine Prevention
Copyright © Therapeutic Research Center. All rights reserved.Medication pricing by Elsevier, accessed July 2021

▪ Continue to suggest migraine prophylaxis if:
Preventing Migraine in Adults
Copyright © Therapeutic Research Center. All rights reserved.
Migraines significantly
impact quality of life
Frequent attacks, such as
4 migraine days/month

For most patients, stick with first-line, low-cost options...
or combos of these meds.
Copyright © Therapeutic Research Center. All rights reserved.

First-Line Meds to Prevent Migraine
Copyright © Therapeutic Research Center. All rights reserved.
Beta-blockers (propranolol, etc)
Topiramate
ValproateTricyclic
antidepressants (amitriptyline, etc)

Copyright © Therapeutic Research Center. All rights reserved.
Think of an injectable CGRP antagonist...
or consider rimegepant ODT
If an 8-week trial of at least 2 first-line meds or
combos doesn’t do the trick
▪ Some experts may use it for
treatment + injectable CGRP
antagonist for prophylaxis
» Data are scant
▪ It doesn’t seem to:
» Cause medication overuse
headache
» Cause rare blood pressure
spikes like erenumab (Aimovig)
Considerations: Rimegepant ODT
Copyright © Therapeutic Research Center. All rights reserved.
Products
Copyright © Therapeutic Research Center. All rights reserved.
Managing Potassium Levels in Heart Failure
Copyright © Therapeutic Research Center. All rights reserved.
POTASSIUM
Pharmacist's Letter. August 2021, No. 370807
Be Armed With Tips to Get Potassium Levels Right
Copyright © Therapeutic Research Center. All rights reserved.
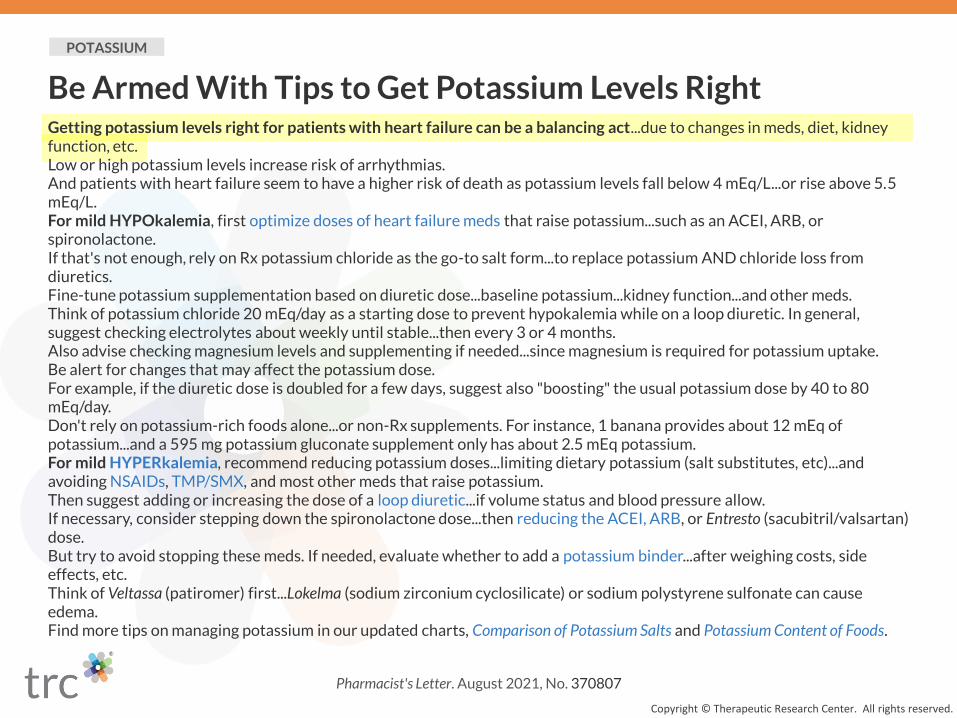
Getting potassium levels right for patients with heart failure can be a balancing act...due to changes in meds, diet, kidney function, etc.Low or high potassium levels increase risk of arrhythmias.And patients with heart failure seem to have a higher risk of death as potassium levels fall below 4 mEq/L...or rise above 5.5 mEq/L.For mild HYPOkalemia, first optimize doses of heart failure meds that raise potassium...such as an ACEI, ARB, or spironolactone.If that's not enough, rely on Rx potassium chloride as the go-to salt form...to replace potassium AND chloride loss from diuretics.Fine-tune potassium supplementation based on diuretic dose...baseline potassium...kidney function...and other meds.Think of potassium chloride 20 mEq/day as a starting dose to prevent hypokalemia while on a loop diuretic. In general, suggest checking electrolytes about weekly until stable...then every 3 or 4 months.Also advise checking magnesium levels and supplementing if needed...since magnesium is required for potassium uptake.Be alert for changes that may affect the potassium dose.For example, if the diuretic dose is doubled for a few days, suggest also "boosting" the usual potassium dose by 40 to 80 mEq/day.Don't rely on potassium-rich foods alone...or non-Rx supplements. For instance, 1 banana provides about 12 mEq of potassium...and a 595 mg potassium gluconate supplement only has about 2.5 mEq potassium.For mild HYPERkalemia, recommend reducing potassium doses...limiting dietary potassium (salt substitutes, etc)...and avoiding NSAIDs, TMP/SMX, and most other meds that raise potassium.Then suggest adding or increasing the dose of a loop diuretic...if volume status and blood pressure allow.If necessary, consider stepping down the spironolactone dose...then reducing the ACEI, ARB, or Entresto (sacubitril/valsartan) dose.But try to avoid stopping these meds. If needed, evaluate whether to add a potassium binder...after weighing costs, side effects, etc.Think of Veltassa (patiromer) first...Lokelma (sodium zirconium cyclosilicate) or sodium polystyrene sulfonate can cause edema.Find more tips on managing potassium in our updated charts, Comparison of Potassium Salts and Potassium Content of Foods.

▪ Low or high potassium levels increase risk of arrhythmias
▪ These patients seem to have a higher risk of death:
Potassium Levels in Patients With Heart Failure
As potassium levels fall below 4 mEq/L
As potassium levels rise above 5.5 mEq/L5.5 mEq/L
4 mEq/L
Mild Hypokalemia
Mild Hyperkalemia
Potassium Levels in Patients With Heart Failure
Copyright © Therapeutic Research Center. All rights reserved.
▪ Advise optimizing doses of
HF meds that raise potassium
» ACEI, ARB, spironolactone, etc
Managing Mild Hypokalemia
Copyright © Therapeutic Research Center. All rights reserved.
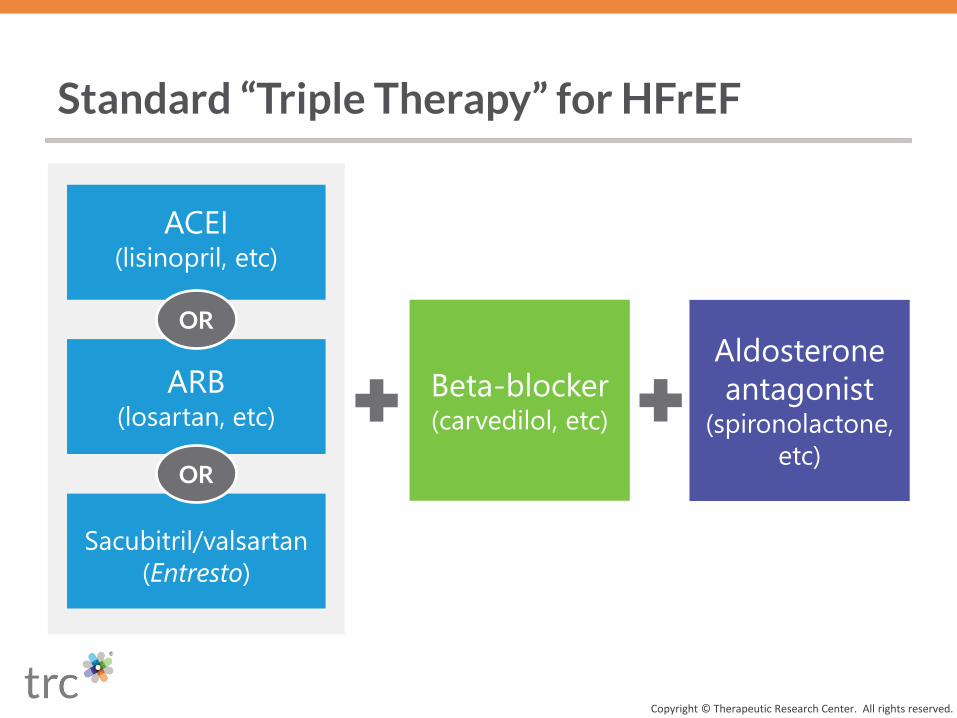
Standard “Triple Therapy” for HFrEF
Copyright © Therapeutic Research Center. All rights reserved.
ARB(losartan, etc)
ACEI (lisinopril, etc)
Beta-blocker (carvedilol, etc)
Aldosterone
antagonist (spironolactone,
etc)
Sacubitril/valsartan
(Entresto)
OR
OR
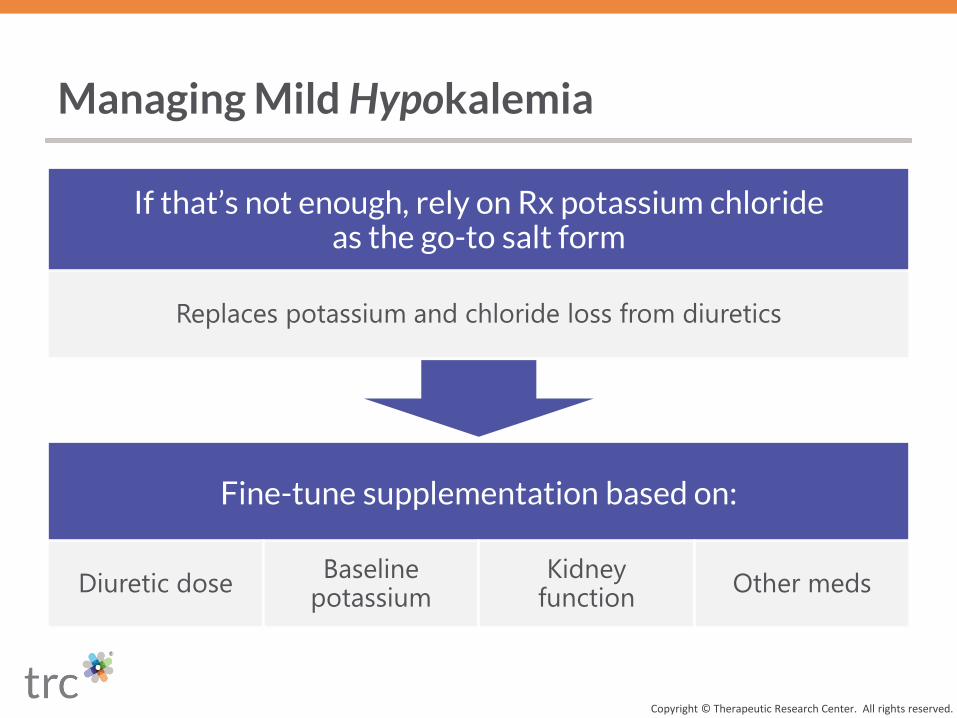
Fine-tune supplementation based on:
Diuretic doseBaseline
potassiumKidney
functionOther meds
If that’s not enough, rely on Rx potassium chloride as the go-to salt form
Replaces potassium and chloride loss from diuretics
Managing Mild Hypokalemia
Copyright © Therapeutic Research Center. All rights reserved.

Think of potassium chloride
20 mEq/day as a starting dose
In general, suggest checking electrolytes
weekly until stable, then every 3 or 4 months
Advise checking magnesium levels and
supplementing if needed
Managing Mild Hypokalemia
Copyright © Therapeutic Research Center. All rights reserved.
▪ Be alert for changes that may affect the potassium dose
» E.g., if the diuretic dose is doubled for a few days, suggest also
“boosting” the usual potassium dose by 40 to 80 mEq/day
Managing Mild Hypokalemia
Copyright © Therapeutic Research Center. All rights reserved.

▪ Don’t rely on these alone:
Managing Mild Hypokalemia
Copyright © Therapeutic Research Center. All rights reserved.
▪ 1 banana ≈
12 mEq potassium
▪ 595 mg potassium
gluconate supplement ≈
2.5 mEq potassium
Potassium-rich foods Non-Rx supplements
Potassium Levels in Patients With Heart Failure
Copyright © Therapeutic Research Center. All rights reserved.
Mild Hypokalemia
Mild Hyperkalemia
Managing Mild Hyperkalemia
Copyright © Therapeutic Research Center. All rights reserved.
Reducing potassium doses
Limiting dietary potassium
(salt substitutes, etc)
Avoiding NSAIDs, TMP/SMX, and most other meds that raise
potassium
Suggest adding or increasing the loop diuretic dose
If needed, consider stepping down the spironolactone dose
Then suggest reducing the ACEI, ARB, or sacubitril/valsartan dose
Managing Mild Hyperkalemia
Copyright © Therapeutic Research Center. All rights reserved.
But try to avoid stopping “triple therapy” meds.
Copyright © Therapeutic Research Center. All rights reserved.
▪ If needed, evaluate whether to add a potassium binder
» Weigh costs, side effects, interactions, etc
▪ If one is used, think of patiromer (Veltassa)
» Sodium zirconium cyclosilicate (Lokelma) or sodium polystyrene
sulfonate can cause edema
Managing Mild Hyperkalemia
Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.

Expanding Pharmacy Technician Roles
Copyright © Therapeutic Research Center. All rights reserved.
PHARMACY TECHNICIANS
Pharmacist’s Letter. August 2021, No. 370806
Empower Your Techs to Take on Advanced Roles
Copyright © Therapeutic Research Center. All rights reserved.
You'll be able to rely even more on your pharmacy technicians...as they take on new activities and expanded roles.COVID-19 was a catalyst that allowed pharmacy teams to clearly demonstrate their value...and changes will last beyond the pandemic.Techs still can't do tasks requiring your professional judgment.But there's a lot they CAN do to free up your time for patient care...so each of you can practice at the top of your ability.Immunizations. Many trained techs are already giving COVID-19 or childhood vaccines under supervision, based on emergency federal guidance.Now PERMANENT laws or regulations allowing qualified techs to administer routine vaccines are proposed or in place in at least 7 states.This may feel like a big change. But it lets you focus on tasks that require clinical judgment...such as evaluating which vaccines are needed, assessing contraindications and precautions, etc.Point-of-care testing. More patients are turning to pharmacies to identify certain infections (COVID-19, flu, etc)...or to screen for or monitor conditions (cholesterol, diabetes, etc).Consider leveraging techs beyond paperwork, scheduling, etc...to obtain samples (fingerstick, etc) and vital signs (BP, etc).Other patient services. Techs continue to be critical in supporting MTM and disease state management services (diabetes, etc).For instance, train techs to become experts at gathering med histories, monitoring adherence, or coordinating specialty meds.Operations. We know techs keep pharmacies running smoothly.Encourage techs to further improve efficiency and quality with specialized roles, such as leading internal audits...preventing diversion...or exploring tech product verification ("tech-check-tech").Look with "fresh eyes" at tasks you currently do that could be delegated...such as scheduling, training, or supervising other techs.If needed, recommend advanced training...so you and your techs feel comfortable as they take on new responsibilities.Our Pharmacy Technicians University's PTU Elite can help train your techs on Immunizations, Point-of-Care Testing, and Soft Skills.

Techs can’t do tasks requiring pharmacist professional judgment
But there’s a lot techs CAN do to free up pharmacist time for patient care
Allows each role to practice at the top of their ability
Expanding Technician Roles
Copyright © Therapeutic Research Center. All rights reserved.

Immunizations
Copyright © Therapeutic Research Center. All rights reserved.
Many trained techs are already giving certain vaccines (COVID-19, etc)
▪ Under emergency federal guidance
Permanent laws/regulations allowing qualified techs to administer routine vaccines are proposed or in place in at least 7 states

▪ Identifying infections
» COVID-19, flu, strep, etc
▪ Screening or monitoring
conditions
» Cholesterol, diabetes, etc
▪ Techs can go beyond
paperwork, scheduling, etc
» Obtaining samples, vital
signs, etc
Point-of-Care Testing
Copyright © Therapeutic Research Center. All rights reserved.
▪ Techs continue to be critical in
supporting activities such as:
» MTM
» Disease state management
services (diabetes, etc)
▪ Example tech roles:
» Gathering med histories
» Monitoring adherence
» Coordinating specialty meds
Other Patient Services
Copyright © Therapeutic Research Center. All rights reserved.

▪ Techs are the backbone that
keep pharmacies running
smoothly
▪ Consider specialized roles:
» Internal audits
» Controlled substance diversion
» Inventory management
» Tech product verification
(“tech-check-tech”)
Pharmacy Operations
Copyright © Therapeutic Research Center. All rights reserved.

▪ Look with “fresh eyes” at tasks
techs can do
» Scheduling, training, or
supervising other techs
» Resolving billing issues
Pharmacy Operations
Copyright © Therapeutic Research Center. All rights reserved.

▪ If needed, recommend
advanced training
» To improve knowledge,
proficiency, and comfort as techs
take on new responsibilities
Expanding Technician Roles
Copyright © Therapeutic Research Center. All rights reserved.

Copyright © Therapeutic Research Center. All rights reserved.


















