
Pharmacotherapy of smoking cessation
1
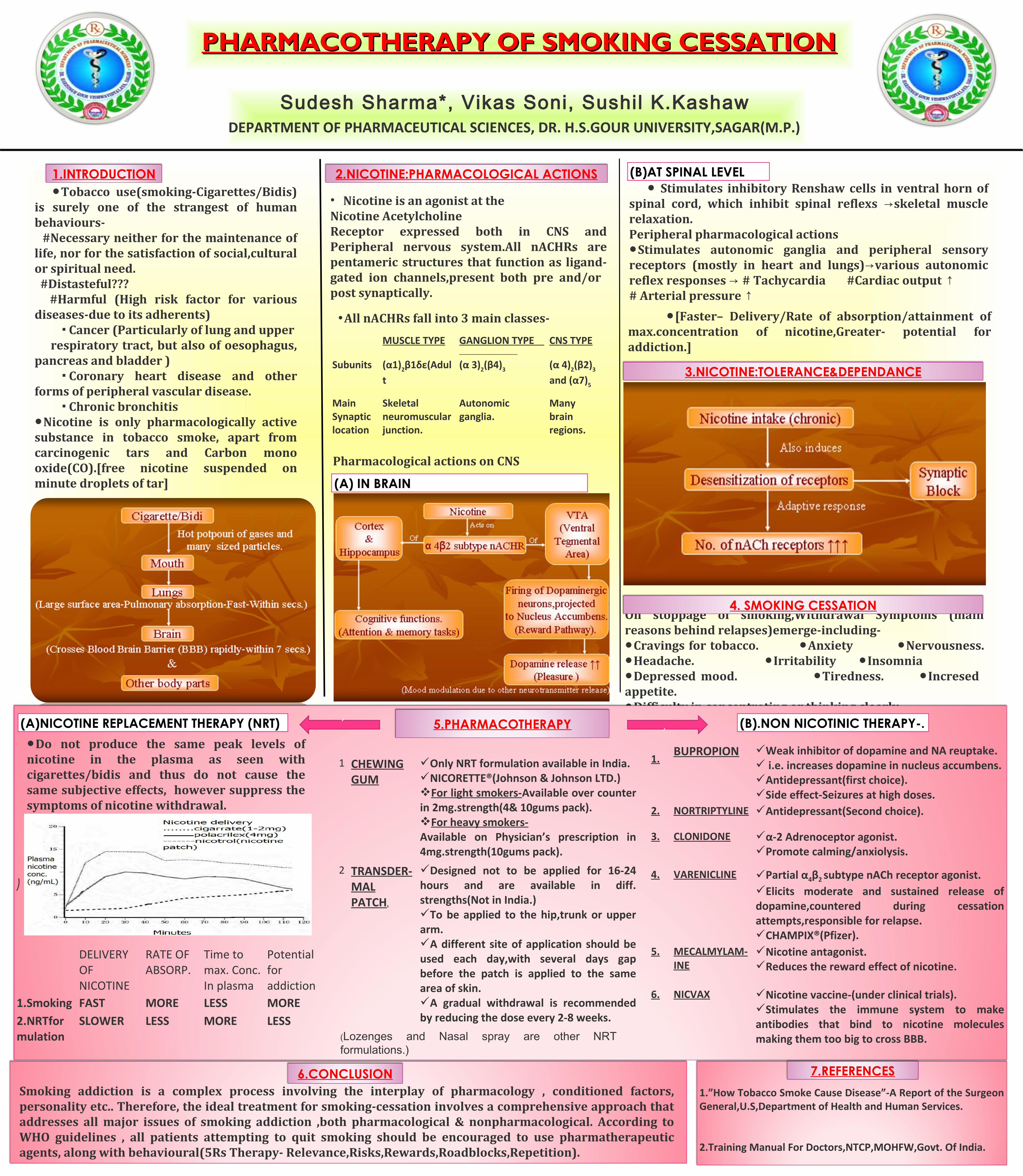
PHARMACOTHERAPY OF SMOKING CESSATION PHARMACOTHERAPY OF SMOKING CESSATION DEPARTMENT OF PHARMACEUTICAL SCIENCES, DR. H.S.GOUR UNIVERSITY,SAGAR(M.P.) Sudesh Sharma*, Vikas Soni, Sushil K.Kashaw ● Tobacco use(smoking-Cigarettes/Bidis) is surely one of the strangest of human behaviours- #Necessary neither for the maintenance of life, nor for the satisfaction of social,cultural or spiritual need. #Distasteful??? #Harmful (High risk factor for various diseases-due to its adherents) ▪ Cancer (Particularly of lung and upper respiratory tract, but also of oesophagus, pancreas and bladder ) ▪ Coronary heart disease and other forms of peripheral vascular disease. ▪ Chronic bronchitis ● Nicotine is only pharmacologically active substance in tobacco smoke, apart from carcinogenic tars and Carbon mono oxide(CO).[free nicotine suspended on minute droplets of tar] • Nicotine is an agonist at the Nicotine Acetylcholine Receptor expressed both in CNS and Peripheral nervous system.All nACHRs are pentameric structures that function as ligand- gated ion channels,present both pre and/or post synaptically. • All nACHRs fall into 3 main classes- MUSCLE TYPE GANGLION TYPE CNS TYPE Subunits (α1) 2 β1δε(Adul t (α 3) 2 (β4) 3 (α 4) 2 (β2) 3 and (α7) 5 Main Synaptic location Skeletal neuromuscular junction. Autonomic ganglia. Many brain regions. •Pharmacological actions on CNS- -In BRAIN Pharmacological actions on CNS ● Stimulates inhibitory Renshaw cells in ventral horn of spinal cord, which inhibit spinal reflexs skeletal muscle → relaxation. Peripheral pharmacological actions ● Stimulates autonomic ganglia and peripheral sensory receptors (mostly in heart and lungs) various autonomic → reflex responses # Tachycardia #Cardiac output → ↑ # Arterial pressure ↑ ● [Faster– Delivery/Rate of absorption/attainment of max.concentration of nicotine,Greater- potential for addiction.] On stoppage of smoking,Withdrawal Symptoms (main reasons behind relapses)emerge-including- ● Cravings for tobacco. ● Anxiety ● Nervousness. ● Headache. ● Irritability ● Insomnia ● Depressed mood. ● Tiredness. ● Incresed appetite. ● Difficulty in concentrating or thinking clearly. ) ● Do not produce the same peak levels of nicotine in the plasma as seen with cigarettes/bidis and thus do not cause the same subjective effects, however suppress the symptoms of nicotine withdrawal. DELIVERY OF NICOTINE RATE OF ABSORP. Time to max. Conc. In plasma Potential for addiction 1.Smoking FAST MORE LESS MORE 2.NRTfor mulation SLOWER LESS MORE LESS 1 CHEWING GUM Only NRT formulation available in India. NICORETTE®(Johnson & Johnson LTD.) For light smokers- Available over counter in 2mg.strength(4& 10gums pack). For heavy smokers- Available on Physician’s prescription in 4mg.strength(10gums pack). 2 TRANSDER- MAL PATCH . Designed not to be applied for 16-24 hours and are available in diff. strengths(Not in India.) To be applied to the hip,trunk or upper arm. A different site of application should be used each day,with several days gap before the patch is applied to the same area of skin. A gradual withdrawal is recommended by reducing the dose every 2-8 weeks. 1. BUPROPION Weak inhibitor of dopamine and NA reuptake. i.e. increases dopamine in nucleus accumbens. Antidepressant(first choice). Side effect-Seizures at high doses. 2. NORTRIPTYLINE Antidepressant(Second choice). 3. CLONIDONE α-2 Adrenoceptor agonist. Promote calming/anxiolysis. 4. VARENICLINE Partial α 4 β 2 subtype nACh receptor agonist. Elicits moderate and sustained release of dopamine,countered during cessation attempts,responsible for relapse. CHAMPIX®(Pfizer). 5. MECALMYLAM- INE Nicotine antagonist. Reduces the reward effect of nicotine. 6. NICVAX Nicotine vaccine-(under clinical trials). Stimulates the immune system to make antibodies that bind to nicotine molecules making them too big to cross BBB. (Lozenges and Nasal spray are other NRT formulations.) (B).NON NICOTINIC THERAPY-. 6.CONCLUSION 7.REFERENCES 1.”How Tobacco Smoke Cause Disease”-A Report of the Surgeon General,U.S,Department of Health and Human Services. 2.Training Manual For Doctors,NTCP,MOHFW,Govt. Of India. Smoking addiction is a complex process involving the interplay of pharmacology , conditioned factors, personality etc.. Therefore, the ideal treatment for smoking-cessation involves a comprehensive approach that addresses all major issues of smoking addiction ,both pharmacological & nonpharmacological. According to WHO guidelines , all patients attempting to quit smoking should be encouraged to use pharmatherapeutic agents, along with behavioural(5Rs Therapy- Relevance,Risks,Rewards,Roadblocks,Repetition). 5.PHARMACOTHERAPY 4. SMOKING CESSATION 1.INTRODUCTION 3.NICOTINE:TOLERANCE&DEPENDANCE 2.NICOTINE:PHARMACOLOGICAL ACTIONS (A)NICOTINE REPLACEMENT THERAPY (NRT) , , (B)AT SPINAL LEVEL (A) IN BRAIN
-
Upload
vikas-soni -
Category
Health & Medicine
-
view
63 -
download
6
Transcript of Pharmacotherapy of smoking cessation
PHARMACOTHERAPY OF SMOKING CESSATIONPHARMACOTHERAPY OF SMOKING CESSATION
DEPARTMENT OF PHARMACEUTICAL SCIENCES, DR. H.S.GOUR UNIVERSITY,SAGAR(M.P.)
Sudesh Sharma*, Vikas Soni, Sushil K.Kashaw
●Tobacco use(smoking-Cigarettes/Bidis) is surely one of the strangest of human behaviours- #Necessary neither for the maintenance of life, nor for the satisfaction of social,cultural or spiritual need. #Distasteful??? #Harmful (High risk factor for various diseases-due to its adherents)
▪Cancer (Particularly of lung and upper respiratory tract, but also of oesophagus, pancreas and bladder )
▪Coronary heart disease and other forms of peripheral vascular disease.
▪Chronic bronchitis●Nicotine is only pharmacologically active substance in tobacco smoke, apart from carcinogenic tars and Carbon mono oxide(CO).[free nicotine suspended on minute droplets of tar]
• Nicotine is an agonist at theNicotine Acetylcholine Receptor expressed both in CNS and Peripheral nervous system.All nACHRs are pentameric structures that function as ligand-gated ion channels,present both pre and/or post synaptically.
•All nACHRs fall into 3 main classes-
MUSCLE TYPE GANGLION TYPE
CNS TYPE
Subunits (α1)2β1δε(Adult
(α 3)2(β4)3 (α 4)2(β2)3
and (α7)5
Main Synaptic location
Skeletal neuromuscular junction.
Autonomic ganglia.
Many brain regions.
•Pharmacological actions on CNS-
-In BRAIN
Pharmacological actions on CNS
● Stimulates inhibitory Renshaw cells in ventral horn of spinal cord, which inhibit spinal reflexs skeletal muscle →relaxation.Peripheral pharmacological actions●Stimulates autonomic ganglia and peripheral sensory receptors (mostly in heart and lungs) various autonomic →reflex responses # Tachycardia #Cardiac output → ↑# Arterial pressure ↑ ●[Faster– Delivery/Rate of absorption/attainment of max.concentration of nicotine,Greater- potential for addiction.]
On stoppage of smoking,Withdrawal Symptoms (main reasons behind relapses)emerge-including-●Cravings for tobacco. ●Anxiety ●Nervousness. ●Headache. ●Irritability ●Insomnia●Depressed mood. ●Tiredness. ●Incresed appetite. ●Difficulty in concentrating or thinking clearly.
)
●Do not produce the same peak levels of nicotine in the plasma as seen with cigarettes/bidis and thus do not cause the same subjective effects, however suppress the symptoms of nicotine withdrawal.
DELIVERY OF NICOTINE
RATE OF ABSORP.
Time to max. Conc. In plasma
Potential for addiction
1.Smoking FAST MORE LESS MORE2.NRTformulation
SLOWER LESS MORE LESS
1 CHEWING GUM
Only NRT formulation available in India.NICORETTE®(Johnson & Johnson LTD.)For light smokers-Available over counter in 2mg.strength(4& 10gums pack).For heavy smokers-Available on Physician’s prescription in 4mg.strength(10gums pack).
2 TRANSDER-MAL PATCH.
Designed not to be applied for 16-24 hours and are available in diff. strengths(Not in India.)To be applied to the hip,trunk or upper arm.A different site of application should be used each day,with several days gap before the patch is applied to the same area of skin.A gradual withdrawal is recommended by reducing the dose every 2-8 weeks.
1.BUPROPION Weak inhibitor of dopamine and NA reuptake.
i.e. increases dopamine in nucleus accumbens.Antidepressant(first choice).Side effect-Seizures at high doses.
2. NORTRIPTYLINE Antidepressant(Second choice).
3. CLONIDONE α-2 Adrenoceptor agonist.Promote calming/anxiolysis.
4. VARENICLINE Partial α4β2 subtype nACh receptor agonist.Elicits moderate and sustained release of dopamine,countered during cessation attempts,responsible for relapse.CHAMPIX®(Pfizer).
5. MECALMYLAM-INE
Nicotine antagonist.Reduces the reward effect of nicotine.
6. NICVAX Nicotine vaccine-(under clinical trials).Stimulates the immune system to make antibodies that bind to nicotine molecules making them too big to cross BBB.(Lozenges and Nasal spray are other NRT
formulations.)
(B).NON NICOTINIC THERAPY-.
6.CONCLUSION 7.REFERENCES
1.”How Tobacco Smoke Cause Disease”-A Report of the Surgeon General,U.S,Department of Health and Human Services.
2.Training Manual For Doctors,NTCP,MOHFW,Govt. Of India.
Smoking addiction is a complex process involving the interplay of pharmacology , conditioned factors, personality etc.. Therefore, the ideal treatment for smoking-cessation involves a comprehensive approach that addresses all major issues of smoking addiction ,both pharmacological & nonpharmacological. According to WHO guidelines , all patients attempting to quit smoking should be encouraged to use pharmatherapeutic agents, along with behavioural(5Rs Therapy- Relevance,Risks,Rewards,Roadblocks,Repetition).
5.PHARMACOTHERAPY
4. SMOKING CESSATION
1.INTRODUCTION
3.NICOTINE:TOLERANCE&DEPENDANCE
2.NICOTINE:PHARMACOLOGICAL ACTIONS
(A)NICOTINE REPLACEMENT THERAPY (NRT)
,
,
(B)AT SPINAL LEVEL
(A) IN BRAIN


















