Pharmacotherapy for opioid addiction - Home | California … · 2008-11-03 · Pharmacotherapy for...
49
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
Transcript of Pharmacotherapy for opioid addiction - Home | California … · 2008-11-03 · Pharmacotherapy for...

Pharmacotherapy for opioid addiction
Judith Martin, MDMedical Director
BAART Turk Street ClinicSan Francisco

Disclosure slide
No commercial conflicts to disclose.

810,000 to 1,000,000 chronic users of heroin
250,000± patients receiving opioid maintenance treatment (OMT), mostly methadone. (SAMHSA, TEDS)
Gaps in current treatment of opioid dependence

Number of new non-medical users of therapeutics
(NSDUH, 2002)

Diacetylmorphine (Heroin)Hydromorphone (Dilaudid)Oxycodone (OxyContin, Percodan, Percocet, Tylox)Meperidine (Demerol)Hydrocodone (Lortab, Vicodin)
Commonly Abused Opioids

Morphine (MS Contin, Oramorph)Fentanyl (Sublimaze)Propoxyphene (Darvon)Methadone (Dolophine)CodeineOpium
Commonly Abused Opioids (continued)
Outline:
Opioid maintenance treatment (OMT)RationalePhases of maintenanceMedications for maintenance
Other pharmacotherapyTapers and detoxificationSymptomatic treatment of withdrawalAntagonists

Four questions patients ask about OMT:
How is methadone (buprenorphine) better for me than heroin?What is the right dose of methadone (buprenorphine) for me?How long should I stay on OMT?What are the side effects of methadone (buprenorphine)?

THE DOSING WINDOW

Counseling staff

Four questions patients ask about OMT:
How is methadone (buprenorphine) better for me than heroin?What is the right dose of methadone (buprenorphine) for me?How long should I stay on OMT?What are the side effects of methadone (buprenorphine)?

How is methadone better than heroin?
LegalAvoids needlesKnown amount ingested

Dos
e R
espo
nse
Time
“Loaded”“High”
Normal Range“Comfort Zone”
“Sick”
Methadone Simulated 24 Hr. Dose/ResponseAt steady-state in tolerant patient
0 hrs.
24 hrs.
“Abnormal Normality”
Subjective w/d
Objective w/d
Opioid Agonist Treatment of Addiction - Payte - 1998

How is methadone better than heroin?
• Legal• Avoids needles• Known amount ingested• Slow onset: no “rush” • Long acting: can maintain “comfort” or
normal brain function• Stabilized physiology, hormones, tolerance
Four questions patients ask:
• How is methadone better for me than heroin?
• What is the right dose of methadone for me?
• How long should I stay on methadone?• What are the side effects of methadone?
What is the right dose?
Eliminate physical withdrawalEliminate ‘craving’Comfort/function: High tolerance trough is 400-600 ng/ml, peak no more than twice the trough.Not over-sedatedBlocking dose

Dos
e R
espo
nse
Time
“Loaded”“High”
Normal Range“Comfort Zone”
“Sick”
Methadone Simulated 24 Hr. Dose/ResponseAt steady-state in tolerant patient
0 hrs.
24 hrs.
“Abnormal Normality”
Subjective w/d
Objective w/d
Opioid Agonist Treatment of Addiction - Payte - 1998
trough

Recent Heroin Use by Current Methadone Dose
020406080
100
0 10 20 30 40 50 60 70 80 90 100
Methadone Dose, in mg.
% H
eroi
n U
se
Ref: J. C. Ball, November 18, 1988Slide adapted from Tom Payte

“How Much????
Enough!!!”Tom Payte, MD

Average dose range for MMT in the US:
80 to 120 mg per day

Phases of Methadone Maintenance treatment:Induction: 3-7 days
Achieve tissue stores without overdose.
Stabilization: 2-8 weeks, dose titrationMaintenance: steady dose

Steady State: The point at which during each interdose interval the rise and fall of drug concentration for the
interdose interval is identical for each dose
050
100150200250300350400450
1 2 3 4 5 6 7 8
ng/ml
Days/Half-Lives – Methadone half-life= 24-36 hoursDose constant at 30 mg daily. Interdose interval = 24 hrs (trough to
trough)Peak levels increase daily for 5-6 days with NO increase in dose!22Colonial Management Group, LP -- J. Thomas Payte, MD

Induction safety, MMT
Regulation limits first methadone dose to 30mg.First day total to 40mg.First 7-10 days of treatment is the overdose danger time (rare).“Start low and go slow”

Four questions patients ask:
• How is methadone better for me than heroin?
• What is the right dose of methadone for me?
• How long should I stay on methadone?
• What are the side effects of methadone?
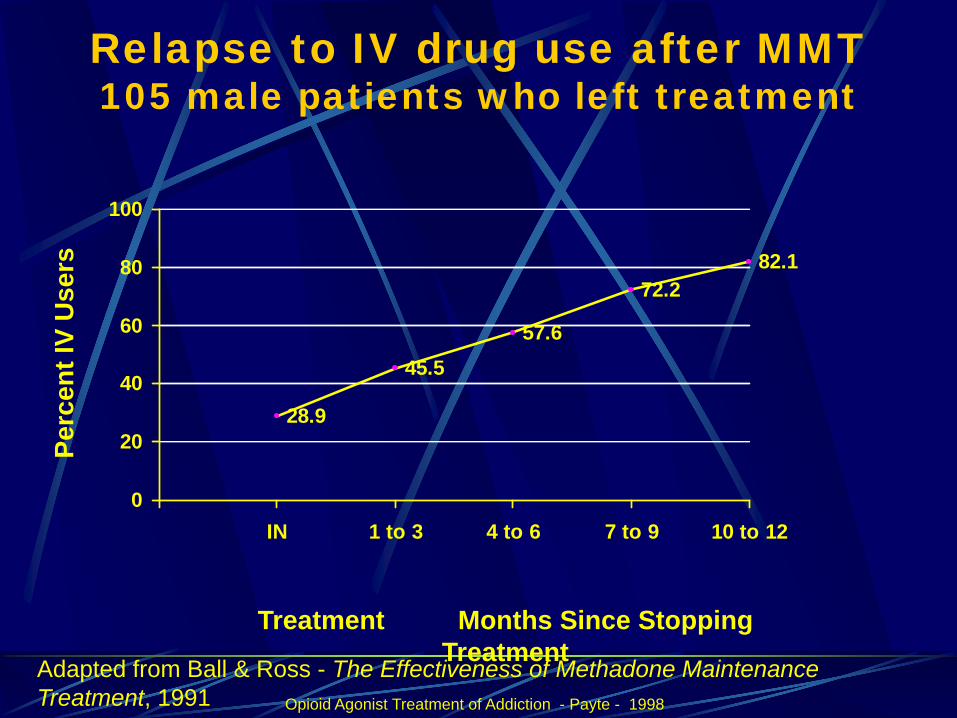
Relapse to IV drug use after MMT105 male patients who left treatment
28.9
45.557.6
72.282.1
0
20
40
60
80
100
IN 1 to 3 4 to 6 7 to 9 10 to 12
Perc
ent I
V U
sers
Treatment Months Since Stopping Treatment
Opioid Agonist Treatment of Addiction - Payte - 1998
Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991
“How Long???
Long Enough!!”Tom Payte, MD

Four questions patients ask:
• How is methadone better for me than heroin?
• What is the right dose of methadone for me?
• How long should I stay on methadone?• What are the side effects of
methadone?

Side effects of methadone:
General opiate effects: Sedation/stimulationMaintained phys. dependence (stable)hypogonadism (not as severe as with heroin, may be dose dependent)
ConstipationSlight QTc prolongation on ECG (Martell etal)SweatingMethadone treatment tied to regulated clinic

Treatment Outcome Data
4-5 fold reduction in death ratereduction of drug usereduction of criminal activityengagement in socially productive rolesreduced spread of HIVexcellent retention
(see: Joseph et al, 2000, Mt. Sinai J.Med., vol67, # 5, 6)

Heroin Addiction, Death rates MMT vs Untreated
01
23
4
56
7
8
MMT UNTREATED
OBSERVEDEXPECTED
Slide data courtesy of Frank Vocci, MD, NIDA - Reference: Grondblah, L. et al. ACTA PSCHIATR SCAND, P. 223-227, 1990
Opioid Agonist Treatment of Addiction - Payte - 1998
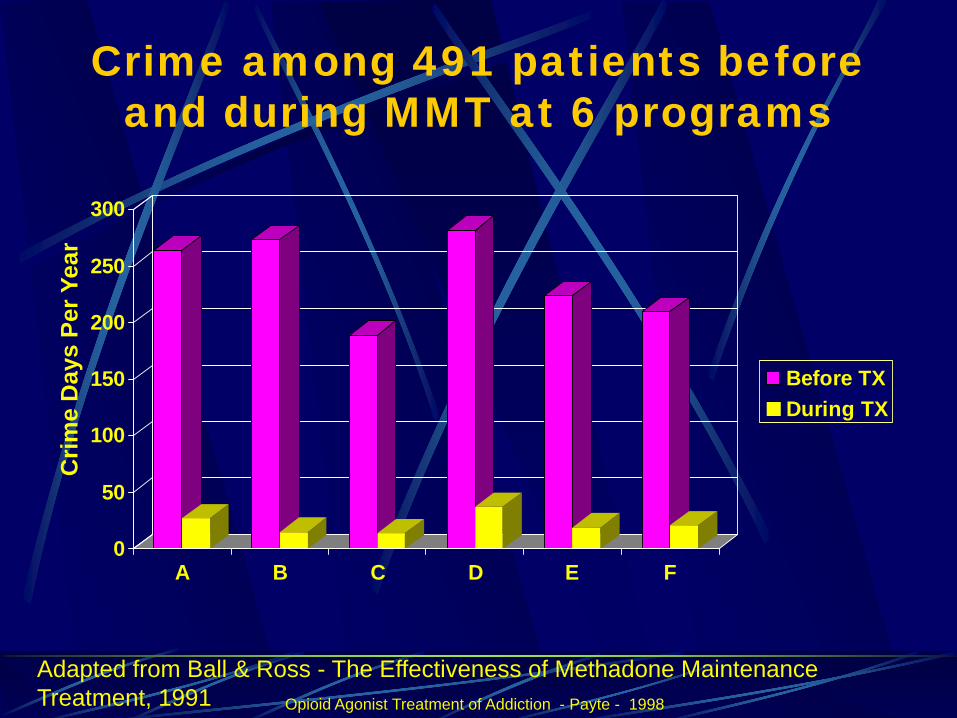
Crime among 491 patients before and during MMT at 6 programs
0
50
100
150
200
250
300
A B C D E F
Before TXDuring TX
Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991
Crim
e D
ays
Per Y
ear
Opioid Agonist Treatment of Addiction - Payte - 1998

HIV CONVERSION IN TREATMENT
0%
5%
10%
15%
20%
25%
30%
35%
Base line 6 Month 12 Month 18 Month
ITOT
HIV infection rates by baseline treatment status. In treatment (IT) n=138, not in treatment (OT) n=88Source: Metzger, D. et. al. J of AIDS 6:1993. p.1052
Opioid Maintenance Pharmacotherapy - A Course for Clinicians - 1997

Pregnancy
MMT treatment of choice for pregnant, opioid-abusing women. Efforts to avoid intra-uterine fetal withdrawal, including split dose. Neonatal withdrawal occurs within 72 hours, at least 45% need treatment.Breastfeeding recommended if not HIV positive.

Pain in patients on MMT
Methadone is prescribed for pain treatment in twice or three times daily doses. Up to 60% of MMT patients have chronic pain (Jamison 2000, Rosenblum 2003)Divided doses may be indicated.

Methadone detoxification
Defined in the regs: Short-term= under 30 daysLong-term= 30-180 days

Pattern of typical shortterm detoxification on
methadone
05
1015202530354045
Doses, mg
Days 1-21 of detoxification
Mg.
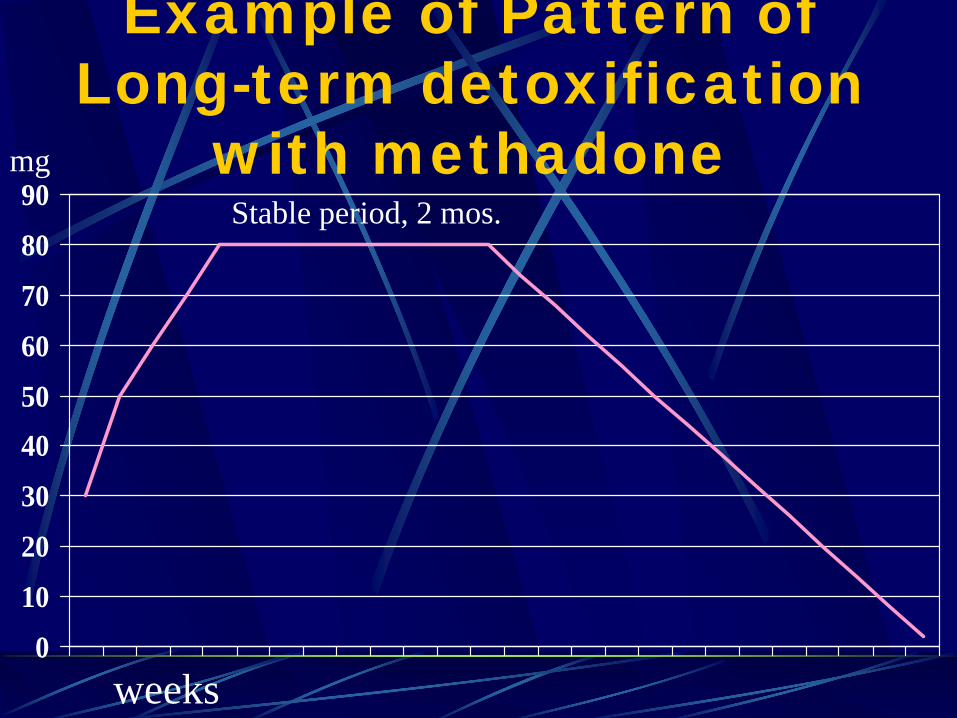
Example of Pattern of Long-term detoxification
with methadone
0
10
20
30
4050
60
70
80
90
weeks
Stable period, 2 mos.mg

Outcome of detoxifications:
Long-term no better than short after detox is over.Most patients relapse within six months.
Ref: Sees et al.

Sublingual buprenorphine :
Partial agonist, sublingual tablet formulated with naloxone. Schedule 3, available in office-based practice with certain restrictions. Induction – stabilization period only 3 days. Strong receptor attachment displaces other opioids.

Comparison of Activity Levels
0
10
20
30
40
50
60
70
80
90
100
% Mu Receptor
IntrinsicActivity
Full Agonist(e.g. methadone)
Partial Agonist(e.g. buprenorphine)
Antagonist (e.g. naloxone)
no drug high dose
DRUG DOSE
low dose
Slide: courtesy Reckitt Benkiser

One slide about LAAM
Stands for levo alpha acetyl methadol.Long acting, allows MWF dosing schedule.Listed as a maintenance medication in the regulationsNot available in US, nobody marketing it.QT lengthened

Buprenorphine, Methadone, LAAM: Treatment Retention
Per
cent
Ret
aine
d
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
20% Lo Meth
58% Bup
73% Hi Meth
53% LAAM
Study WeekJohnson et al, 2000

Buprenorphine, Methadone, LAAM:Opioid Urine Results
Mea
n %
Neg
ativ
e
Study Week
All Subjects
Lo Meth
BupHi Meth
LAAM
1 3 5 7 9 11 13 15 170
20
40
60
80
100
19%
40%
39%
49%

Retention in treatment
Treatment duration (days)
Rem
aini
ng in
trea
tmen
t (n
r)
0
5
10
15
20
0 50 100 150 200 250 300 350
Control, 6-day detoxBuprenorphine maintenance
Kakko et al, 2003,
Opioid pharmacotherapy,
summary:Methadone, buprenorphine and LAAM all approved by the FDA for treatment of opiate dependence. (LAAM not currently available from any drug company)Best evidence so far supports maintenance.Detoxification attempts should have maintenance as a back up in case of relapse.

Naltrexone
Used as a deterrent, blocks opioid receptor.Can be instituted after withdrawal from other opioids.Some success in patients who are professionals.Danger of overdose if discontinued.

Clonidine
Off-label use of antihypertensive, helps control opioid withdrawal symptomsPart of some supervised withdrawal protocols, pills or patches.Main side effect is low blood pressure.Buprenorphine taper may supersede.