PHARMACOLOGY II - جامعة نزوى€¦ · PHARMACOLOGY II Dr A.SHYAM SUNDAR.,M.Pharm.,Ph.D...
169
PHARMACOLOGY II Dr A.SHYAM SUNDAR.,M.Pharm.,Ph.D Assistant professor in Pharmacology, University of Nizwa, Sultanate of Oman
Transcript of PHARMACOLOGY II - جامعة نزوى€¦ · PHARMACOLOGY II Dr A.SHYAM SUNDAR.,M.Pharm.,Ph.D...

PHARMACOLOGY II
Dr A.SHYAM SUNDAR.,M.Pharm.,Ph.D
Assistant professor in Pharmacology,
University of Nizwa,
Sultanate of Oman

What is Pharmacology?
• Pharmacology is the science that deals with
drugs.
• It explains what drugs do,and how they do
it.
• A knowledge of Pharmacology is essential
for using drugs effectively in treatment.

Drugs...
• Drug is a substance used to cure,diagnose or prevent the
disease.
• WHO defines drug as product that is used or intended to be
used to modify or explore physiological systems or
pathological states for the benefit of recipient.
• Drugs are intended to have a selective action,but this ideal
is seldom achieved
• There is always a risk of adverse effects as well as a
benefit connected with using any drug.

Pharmacokinetics...
• ‗Kinesis‘ means ‗movement‘,hence
pharmacokinetics means ―how drugs move
inside the body‖.
• It deals with Absorption, distribution and
metabolism and excretion of drugs.
• Simply it gives details regarding ―what the
body does to the drug.

Pharmacodynamics...
• ‗Dynamics‘ means ‗power‘,hence
Pharmacodynamics detail about the power
the drug.
• Pharmacodynamics is the study of drug
effects.
• Simply it deals with what the drug does to
the body.

Drug names...
• Chemical name explains the drug‘s chemical
composition and molecular structure. ex.( +/- ) – 2
– ( p-isobutylphenyl ) proponic acid.
• Generic Name ( Nonproprietary name ) name
given by the United States Adopted Name
Council.Universally accepted. ex.ibuprofen.
• Trade Name ( Brand name/ Proprietary name)
the drug has a registered trademark ; use of the
name restricted by the drug‘s owner ex. Motrin

Receptors
• Receptors are proteins in nature.
• They may be located inside the cell or on
the cell‘s surface.
• Most of the drugs and endogenous
substance binds with receptors and then
produce Biological actions.

Agonists and Antagonists...
• Agonists are the drugs that bind to receptors and stimulate/
enhance a response ex. Insulin, isoproterenol – stimulate
beta 1 receptor.
• Antagonists are the drugs that bind to receptors and block a
response ex. cimetidine – blocks H2 receptor.
• Agonists and Antagonists can preferably defined with the
terms Affinity and Intrinsic activity.
• Affinity is the tendency of the drug to bind with the receptor.
• Intrinsic activity is the capacity of the drug to produce
biological action after binding with the receptor.

Sources of drugs...
From plants (eg, morphine).
From animals (eg, insulin).
From minerals (eg, iron).
From synthetic chemical compounds manufactured in laboratories.
(Eg, adding, deleting, or altering a side-chain).
From micro organisms (eg, many antibiotics).
From biotechnology origin: this process involves manipulating
Deoxyribonucleic acid (dna) and ribonucleic acid (rna)

Types of drugs...
• Prescription drugs.
• Non-Prescription drugs.
• Controlled drugs

Prescription Drugs • Prescription drugs are drugs that the
government has designated to be
potentially harmful unless their use
is supervised by a licensed health
care provider.
• Although these drugs have been tested
for safety and therapeutic effect,
prescription drugs may cause different
reactions in some individuals.
• Prescription drugs, also called legend
drugs, are the largest category of drugs.
Prescription drugs are prescribed by a
licensed health care provider.
• The prescription (see Fig) contains the
name of the drug, the dosage, the method
and times of administration, and the
signature of the licensed health care
provider prescribing the drug.

Non-Prescription drugs
• Declared by the FDA to be safe (if
taken as directed) and obtained
without a prescription.
• These drugs are also referred to as
over-the-counter (OTC) drugs and
may be purchased in a variety of
settings, such as a pharmacy,
drugstore, or in the local
supermarket.
• OTC drugs include those given for
symptoms of the common cold,
headaches, constipation, diarrhea,
and upset stomach.
• These drugs are not without risk
and may produce adverse reactions.
For example, acetylsalicylic acid,
commonly known as aspirin, is
potentially harmful and can cause
gastrointestinal bleeding and
salicylism .
• Labeling requirements give the
consumer important information
regarding the drug, dosage,
contraindications,precautions, and
adverse reactions.
• Consumers are urged to read the
directions carefully before taking
OTC drugs.

Controlled Substances...
• Controlled substances are the
most carefully monitored of all
drugs.
• These drugs have a high
potential for abuse and may
cause physical or
psychological dependence.
• Prescriptions for controlled
substances must be written in ink
and include the name and address
of the patient and the Drug
Enforcement Agency number of
the primary health care provider.

Drug use in Pregnancy...
• Drugs administered to pregnant
women, particularly during the first
trimester (3 months), may cause
teratogenic effects.
• A teratogen is any substance that
causes abnormal development of
the fetus leading to a severely
deformed fetus. Drugs are one type
of teratogen.
• In an effort to prevent teratogenic
effects, the FDA has established
five categories suggesting the
potential of a drug for causing birth
defects.

PHARMACIST...

PHARMACIST...

CARDIOVASCULAR
PHARMACOLOGY


4 BASIC POINTS & 4 MAIN DISEASES
Heart Failure is a condition in which the heart is unable to meet the
metabolic demands of the body.
Hypertension is a condition in which the pressure at which heart ejects its
blood into the arteries persistently increases abnormally.
Cardiac Arrhythmias, a group of disorders in which there will be abnormality
either in the impulse generation or impulse conduction.
Angina is the hearts way of signaling that it doesn't receive sufficient blood supply
and Myocardial Infarction occurs when oxygen deprived myocardial cells start
dying.

ANS AND CVS When sympathetic nervous
system is stimulated...
When parasympathetic nervous
system is stimulated...
β1 receptors activated and causes
Increase in heart rate,
Increase in conduction velocity and
Increase in force of contraction
M2 receptors activated and causes
Decrease in heart rate,
Decrease in conduction velocity and
Decrease in force of contraction
α1 receptors activated and causes
vasoconstriction
Secretion of Catacholamines
and α1and β1 actions occur.

UNIT 1:
CONGESTIVE HEART FAILURE
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Differentiate the types of heart failure
• Explain compensatory mechanisms of heart failure
• Understand the physiology of cardiac contraction and
ionic movement during cardiac contraction
• List the classes of drugs used to treat cardiac failure and
their mechanism of action
• Recall vital information about the drugs used in CHF.
• Apply pharmacological knowledge gained in the clinical
scenario.

Types of heart failure...
• Low-output heart failure vs High-output heart failure.
• In LOHF,the metabolic demands of the body is normal and
heart will not be able to supply the normal demand.
• In HOHF,the metabolic demands may be very high (due to
anemia or hyperthyroidism),and the heart will not be able
to supply blood to meet this increase in demand.
• Left sided heart failure vs Right sided heart failure.
• LSHF leads to pulmonary edema and RSHF leads to
systemic edema

COMPENSATORY MECHANISMS OF HEART
FAILURE
• Increased sympathetic activity.
• Retention of sodium and water.
• Myocardial hypertrophy.

Increased force of contraction
and heart rate
Workload of the heart increases
Further decline in heart’s pumping
capacity
Myocardial
hypertrophy

Physiology of cardiac contraction
• Actin and myosin
• Tropomyosin
• Troponin complex
• Ca++ Ions


Classification of drugs

MOA OF CARDIAC GLYCOSIDES

MOA OF BETA ADRENERGIC AGONISTS
AND PHOSPHODIESTERASE INHIBITORS

DOPAMINE


PHOSPHODIESTERASE INHIBITORS

Direct acting Vasodilators
Nitrates
Hydralazine
• Vasodilators reduces both
preload and afterload.
• Venodilation reduces preload
and Arterial dilation reduces
afterload.
• Minoxidil is used to treat male
pattern bladness.

MOA OF ACE INHIBITORS
CONTRAINDICATED IN PREGNANCY

• β-blockers decrease sympathetic activity
by blocking the β-receptors on the
excitable cells in the myocardium and
blood vessels.
• A blockade of these receptors results in
decreased cardiac contractile activity
and heart rate, decreased blood pressure,
and decreased peripheral circulation.
• All these effects reduce the oxygen
demand of myocytes.
β-blockers such as bisoprolol,
carvedilol, metoprolol are used in
treatment of heart failure in addition to
the treatment of diuretics and ACE-
inhibitors
BETA-BLOCKERS IN CHF

• Diuretics increase excretion of Na+ ions
from the kidney.
• As a result water is excreted as well, which
lowers plasma volume, extra cellular fluid,
cardiac output and ultimately relieve edema
and dyspnea.
Two classes of diuretics are applied in the
treatment of the symptoms of heart failure.
• Loop diuretics act in the ascending loop of
Henle.
Example: Furosemide.
• Thiazide diuretics act in the distal tubule.
Example: Hydrochlorothiazide.
• Spiranolactone is also used in
maintenance of severe heart failure since it
slows down the remodeling of the heart by
antagonising the aldosterone receptors of
the heart.
DIURETICS IN CHF

CONGESTIVE HEART FAILURE - Summary
Therapeutic goals: 1)Reduce workload of the heart
2)Improve myocardial contractility

ANTIHYPERTENSIVE DRUGS

UNIT 2:
ANTIHYPERTENSIVE DRUGS
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Differentiate the types of hypertension
• Explain short and long term control of blood pressure
• List the classes of drugs used to treat hypertension and
their mechanism of action
• Recall vital information about the drugs used in
hypertension.
• Apply pharmacological knowledge gained in the clinical
scenario.

Filling Pressure: A measure of the average (arterial and venous) pressure necessary to cause
filling of the circulation with blood; it varies with blood volume and is directly proportional to
the rate of venous return and thus to cardiac output.



ANTI-HYPERTENSIVES

ACE INHIBITORS
CONTRAINDICATED IN PREGNANCY

Angiotensin antagonists
Losartan and Valsartan are examples
CONTRAINDICATED IN PREGNANCY

BETA ADRENERGIC BLOCKERS
• Beta-1 blockade in cardio myocyte
blocks tachycardia,hypertension and
force of contraction of heart.
• Beta-2 blockade in lungs causes
bronchoconstriction,poor peripheral
circulation.
• Selective beta-1 blockers are preferred
in patients with respiratory troubles as
the non selective blockers alters both
heart and lungs.
• Example for selective beta-1 blockers
and non selective blockers are
atenelol,metaprolol and propranolol
respectively.

MOA and ADR of beta blockers

CALCIUM CHANNEL BLOCKERS
Contraindicated in patients with CHF


Apart from Thiazide diuretics,Loop diuretics and
Spiranolactone also employed in treatment of hypertension.
All diuretics reduce BP by lowering blood volume
which eventually decrease cardiac output.
DIURETICS

ALPHA ADRENERGIC ANTAGONISTS

Both drugs are used to treat mild to moderate
hypertension.
Guanafacine has same ADR and MOA as that of
clonidine
Positive coomb’s test and rebound hypertension
are the respective ADR of methyl dopa and
clonidine respectively.
CENTRALLY ACTING ANTIHYPERTENSIVES

HYPERTENSION -Summary Therapeutic goals:
1)Reduce volume overload
2)Reduce sympathetic outflow
3)Block adrenergic receptors of the heart
4)Dilate blood vessels

HYPERTENSIVE EMERGENCY
Sodiumnitroprusside,Diazoxide and Labetalol are used in hypertensive
emergency.
Sodiumnitroprusside is the doc but cyanide toxicity is prodoced during its
metabolism which is treated with an enzyme called Rhodanase
Diazoxide is used in patients with coronary insufficiency.
Labetelol is also used to treat hypertensive emergency but carries the ADR of
nonselective beta blocker.
Hypertensive emergency is a rare, but life-threatening situation in which
the diastolic blood pressure is either over 150 mm Hg (with systolic
blood pressure greater than 210 mm Hg) in an otherwise healthy per-
son, or 130 mm Hg in an individual with preexisting complications, such
as encephalopathy, cerebral hemorrhage, left ventricular failure, or aor-
tic stenosis.


HYPERTENSION- Summary Therapeutic goals:
1)Reduce volume overload
2)Reduce sympathetic outflow
3)Block adrenergic receptors of the heart
4)Dilate blood vessels

ANTI-ARRHYTHMIC
AGENTS

UNIT 3:
ANTI-ARRHYTHMIC AGENTS
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Explain the processes of cardiac impulse generation and
conduction
• List arrhythmias arising from Atrium, AV node and
Ventricles.
• List the classes of drugs used to treat arrhythmias
• Recall vital information about the drugs used in
arrhythmias.
• Apply pharmacological knowledge gained in the clinical
scenario.

Classification of anti-arrhythmic agents



Cardiac Arrhythmia- Summarys
Therapeutic goals:
Restore normal rhythm of the heart

UNIT 4:
ANTI-ANGINAL AGENTS
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Classify types of angina
• Understand the concept of oxygen demand versus oxygen
supply.
• List the classes of drugs used to treat angina.
• Recall vital information about the drugs used in angina.
• Apply pharmacological knowledge gained in the clinical
scenario.

Anti anginal drugs
In angina, oxygen demand is more than
oxygen supply the treatment strategy
is to
1. Increase oxygen supply and
2.Decrease oxygen demand of heart.


Mechanism of action of Nitrates

• Beta blockers block the beta-1
receptors of the heart and reduces
heart rate,force of contraction and
blood pressure.So,the workload of
heart decreases.
• As the workload of the heart
decreases, the oxygen demand also
decreases and thus beta blockers are
indicated.
• Calcium channel blockers dilates
arteries and veins.
• Dilation of arteries reduce
afterload and dilation of veins
reduce preload of the heart.
• As the preload and afterload
decreases, the workload of the heart
also decreases and thus calcium
channel blockers are inicated in
angina.
Anti-anginal mechanisms of Beta blockers
and
Calcium channel blockers

ANGINAL TREATMENT IN THE PRESENCE OF OTHER DISEASES

ANGINA- Summary
Therapeutic goals:
Reduce work of heart and improve cardiac blood flow
Stable angina Unstable angina

DIURETICS
Dr A.Shyam Sundar,
Assistant professor in Pharmacology,
University of Nizwa,
Sultanate of Oman

UNIT 5:
DIURETICS
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Explain the processes of sodium and water reabsorption
at nephron.
• Classify diuretic drugs
• Recall vital information about the diuretics.
• Apply pharmacological knowledge gained in the clinical
scenario.

Diuretics are drugs that increase renal excretion of
water, sodium, and other electrolytes, thereby
increasing urine formation and output.
They are important therapeutic agents widely used in
the management of both edematous (e.g., heart failure,
renal and hepatic disease) and non edematous (e.g.,
hypertension, ophthalmic surgery) conditions.
Diuretics are also useful in preventing renal failure by
their ability to sustain urine flow.



ACETAZOLAMIDE
Therapeutic uses
Adverse reactions
Therapeutic uses
Adverse reactions
LOOP DIURETICS

THIAZIDE DIURETICS OSMATIC DIURETICS
Therapeutic uses Therapeutic uses
Adverse reactions
Adverse reactions

Potassium sparing Diuretics
Clinical uses Adverse reactions

Drugs used in anemia and other
blood cell deficiencies
Dr A.Shyam Sundar,
Assistant Professor in Pharmacology and Toxicology,
College of Pharmacy and Nursing,
University of Nizwa,
Sultanate of Oman

UNIT 6:
Drugs used in anemia and other blood cell
deficiencies UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• List different types of anemia
• List drugs used in the treatment of anemia and other
blood cell deficiencies
• Recall vital information about the drugs used in anemia
and other blood cell deficiencies.
• Apply pharmacological knowledge gained in the clinical
scenario.

Common Anemias 1. Microcytic Hypochromic Anemia:
Caused by iron deficiency. Hence called as iron deficiency anemia
Most common
2. Megaloblastic Anemia:
Caused by deficiency of Vit B12 / Folic acid ( Co-Factors required for maturation of RBC).
3. Perinicious Anemia:
Common type of Vit B 12 Deficiency anemia.
Caused by defect in the synthesis of IF, a protein required for absorption of dietary vit B12.
4. Hemolytic Anemia:
Due to destruction of RBC.
Iron stores are elevated, not decreased.

Other blood cell deficiencies
• By the manifestation of diseases or as a side
effect of radiation or cancer chemotherapy,
there may be deficiency in either erythrocytes
or neutrophils and platelets.

Drugs used in anemias and other blood
cell deficiencies Oral Iron Supplements:
Ferrous Sulfate, Ferrous Gluconate and Ferrous Fumarate.
Parenteral Iron:
Iron dextran.
Vitamin B12:
Cyanocobalamine.
Hydroxocobalamine.
Red Cell Factor:
Erythropoietin (Epoitin-alfa)
Myeloid Growth Factors:
Filgrastim (G-CSF).
Sargramostim (GM-CSF).
Megakaryocyte Factors:
Oprelvekin
Thrombopoietin

Iron
Essential metallic component of heme.
Present in Hb, transferrin, Ferritin
Deficiency of iron occurs in all woman, malnourished, inadequete and
Iron intake.
Children and pregnant woman need excess requirement of iron.
Used in microcytic anemia.
Ferrous ion supplementation ( Dietary) and in special cases parenteral iron
administration.
Should not be given in hemolytic anemia, because iron stores are elevated
not depressed in hemolytic anemia.
Parenteral defurroxime, is used to treat acute iron intoxication.

Vitamin-B12
• Vit-B12 deficiency and Folic acid deficiency first manifest
as anemia. Vit-B12 also cause neurologic damage/defect.
• Available as hydrocobalamine and Cyanocobalamine.
• Used in pernicious anemia.
• Vit-B12 deficiency anemia is mostly due to inadequate
absorption, therapy should be through parenteral
administration of Vit-B12.

Folic Acid
• Required for normal DNA synthesis.
• Deficiency may lead to either Megaloblastic
anemia or Neural tube defects in fetus.
• Rapidly dividing cells are highly sensitive to folic
acid deficiency. For this reason anti folate drugs
are useful in the treatment of various infections.
• Folic acid supplements will also correct the
anemia but not the neurologic defects of Vit-B12.

Hematopoietic Growth Factors
• Almost a dozen glycoprotein hormones regulate the differentiation and maturation of stem cells within the bone marrow have been discovered.
• Four r-DNA products are approved by US-FDA for the treatment of patient with blood cell deficiencies, such as
1. Erythropoietin.
2. Myeloid Growth Factors. [granulocytes ( basophil, neutrophil and Eosinophil), monocyte and platelets]
3. Megakaryocyte Growth Factors. (A giant cell in the bone marrow that is ancestor of blood platelets)
4. Other Hematopoietic Growth Factors.

Erythropoietin:
Used for anemias associated
with renal failure, bone marrow
disorders, anemias due to cancer
chemotherapy, Zidovudin therapy,
bone marrow transplantation,
AIDS and Cancer.
Myeloid Growth Factors:
Filgrastim(G-CSF) and
Sargramostin(GM-CSF).
stimulate the production of
neutrophils.
Accelerate the recovery of
neutrophils after
Chemotherapy,aplastic anemia
and congenital neutropenia.
Sargramostim causes fever,
arthralgia and capillary damage
with edema.

Megakaryocyte
Growth Factors:
Oprelvekin and
Thrombopoietin are used in
thrombocytopenia and
reduces the need for platelet
transfusion.
Both drugs cause fatigue,
headache and fluid
retention.
Other Hematopoietic
Growth Factors
M-CSF, stem cell
factors, IL-3,6,9 are other
HG factors.
SCF and IL-3 have the
broadest progenetor cell
line effect, producing red
cell, granulocyte,
monocyte, macrophage,
megakaryocyte, eosinophil
and basophil and basophil
cell lines.

Next lecture We will start Respiratory
Pharmacology…
So, revisit the physiology of
respiratory system in advance.

Drugs for Hyperlipidemias
Dr.A.Shyam Sundar. M.Pharm.,Ph.D,
Assistant Professor in Pharmacology And Toxicology
University Of Nizwa
Sultanate of Oman Source: Henry Hitner and Barbara Nagle

UNIT 7:
Drugs used in the treatment of Dyslipedemia
UNIT INSTRUCTIONAL OUTCOMES:
At the end of this unit, the student should be able to,
• Differentiate good and bad lipids
• List drugs used in the treatment of dyslipidemia
• Recall vital information about the drugs used in
dyslipidemia
• Apply pharmacological knowledge gained in the clinical
scenario.

Atherosclerosis
• Atherosclerosis is a
progressive condition
that leads to CAD and
PAD.
• Fat buildup inside the
arteries—plaque
• CAD—coronary
artery disease
• PAD—peripheral
artery disease


Hepatic Cholesterol Synthesis
Cholesterol and
Atherosaclerosis, Grundy)
Rate Limiting
Only pathway
for cholesterol
degradation
Energetically expensive;
prefer to conserve what is
already made/acquired – LDL
receptor pathway

Dyslipidemia The normal range of plasma total CHO concentration < 6.5 mmol/L.
There are smooth gradations of increased risk with
elevated LDL CHO conc, and with reduced HDL CHO conc.
Dyslipidemia can be primary or secondary.
The primary forms are genetically determined
Secondary forms are a consequence of other conditions
such as diabetes mellitus, alcoholism, nephrotic
syndrome,chronic renal failure, administration of
drugs

Lipoproteins
• There are several different lipoproteins:
– Low-density lipoprotein (LDL)
– Very-low-density lipoprotein (VLDL)
– High-density lipoprotein (HDL)

Triglycerides
• Main form of fat from diet
• Provide body with energy
• Chylomicrons:
– Very large lipoproteins that deliver
triglycerides to muscle and fat tissue

Monitoring the Disease • Risk factors for
atherosclerosis
– Age
– History of smoking
– Hypertension
– Premature menopause
– Obesity
– Diabetes mellitus
– Hyperthyroidism

Monitoring the Disease
• The goals of treatment are:
– Lowering LDL cholesterol
– Reducing total serum cholesterol and
triglycerides
– Increasing HDL cholesterol

Lipid-lowering drugs
• Several drugs are used to decrease plasma LDL-CHO
• Drug therapy to lower plasma lipids is only one approach to treatment
• and is used in addition to dietary management
and correction of other modifiable cardiovascular risk factors

Hypolipidemic Drugs
• There are five
groups of drugs
used in the
management of
hyperlipidemia:
– HMG-CoA reductase
inhibitors
– Cholesterol absorption
inhibitors
– Bile acid sequestrants
– Fibric acid derivatives
– Nicotinic acid

Hypolipidemic Drugs

HMG-CoA Reductase Inhibitors
• Also referred to as statins
• MOA—inhibit enzyme that causes
cholesterol synthesis
• IND—adjunct to dietary treatment to
decrease total serum and LDL cholesterol:
– Reduce LDL level up to 30%
– Raise HDL level up to 20%

HMG-CoA Reductase Inhibitors
• Adverse effects:
– Headache, dizziness, alteration of taste,
insomnia, abdominal cramping and
photosensitivity
• May cause myalgias, leg ache, and
muscle weakness
• Contraindicated during pregancy

Cholesterol Absorption Inhibitors
• Ezetimibe:
– MOA—blocks absorption of cholesterol
in the intestines
• Decreases VLDL
• Decreases circulating LDL cholesterol
– IND—treatment of hyperlipidemia in
conjunction with diet alteration

Cholesterol Absorption Inhibitors
• Ezetimibe:
– Modestly reduces total cholesterol, LDL,
and triglyceride blood levels
– Ideal to combine with other hypolipidemic
drugs
– Adverse effects—abdominal pain, fatigue,
coughing, diarrhea, back pain, and arthralgia

Bile Acid Sequestrants
• MOA—bind bile salts and cholesterol in the GI tract, preventing absorption of both
• IND—hyperlipidemia: – Increased elimination of bile salts, cholesterol, and
other fats in the feces.
– Adverse effects include GI disturbances, severe constipation, and fecal impaction.
– Most serious adverse effect is intestinal obstruction.

Nicotinic Acid
• MOA—affects cholesterol synthesis through a G proteinScoupled receptor: – Inhibits triglyceride lipase
– Stimulates lipoprotein lipase
– Decreases free fatty acid release and removes triglycerides
• IND—hyperlipidemia
• Adverse effects—flushing, nausea, vomiting, and diarrhea

Fibric Acid Derivatives
• Gemfibrozil:
– MOA—inhibits breakdown of fat into
triglycerides, and limits liver production
of triglycerides
– IND—to decrease triglycerides
– Adverse effects—nausea, vomiting,
diarrhea, and flatulence

Preferred Therapy
• All hypolipidemic drugs are indicated as
adjunctive therapy to reduce elevated
cholesterol levels.
• HMG-CoA reductase inhibitors are the most
prescribed.
• Cholestyramine can also be used in the
treatment of partial biliary obstruction.

Contraindications
• Systemic hypolipidemic drugs should not be
used in patients with liver dysfunction.
• Bile acid sequestrants should not be used in
patients with biliary obstruction.
• Statins should not be used in pregnant
women.

Drug Interactions


DRUGS AFFECTING
THE
RESPIRATORY SYSTEM
Dr A.Shyam Sundar,
Assistant Professor in Pharmacology,
University of Nizwa,
Sultanate of Oman

OVERVIEW
Asthma is a reversible obstructive disease of the lower airway.
With asthma, there is increasing airway obstruction caused by bronchoconstriction,
inflammation and edema of the lining of the bronchioles, and the production of thick mucus
that can plug the airway.
Chronic obstructive pulmonary disease (COPD) is the name given collectively to
emphysema and chronic bronchitis because the obstruction to the airflow is present most of
the time.
Emphysema is a lung disorder in which the terminal bronchioles or alveoli become enlarged
and plugged with mucus.
Chronic bronchitis is the chronic inflammation and possible infection of the bronchi.
Rhinitis is an inflammation of the mucous membranes of the nose, and is characterized by
sneezing, nasal itching, watery rhinorrhea and congestion.
Coughing is the forceful expulsion of air from the lungs.
A cough may be productive or nonproductive.
With a productive cough, secretions from the lower respiratory tract are expelled.
A nonproductive cough is a dry, hacking one that produces no secretions.

DRUGS USED IN RESPIRATORY DISORDERS

ASTHMA
There are three types of Asthma
1. Extrinsic Asthma (also referred to as
allergic asthma and caused in response to
an allergen such as pollen, dust, and animal
dander).
2. Intrinsic asthma (also called non-allergic
asthma and caused by chronic or recurrent
respiratory infections, emotional upset, and
exercise).
3. Mixed asthma (caused by both intrinsic
and extrinsic factors).
In asthma,there will be
Contraction of bronchial smooth muscle,
Inflammation of the bronchial wall,
Increased mucous secretion.

Drugs addressing bronchoconstriction and inflammatory issues





Leukotriene inhibitors




An antitussive is a drug used to relieve coughing.
A mucolytic is a drug that loosens respiratory secretions.
An expectorant is a drug that aids in raising thick, tenacious mucus from the respiratory
passages.
The mucolytic acetylcysteine may be used as part of the treatment of bronchopulmonary
diseases such as emphysema,as adjunctive therapy in chronic bronchopulmonary diseases,
such as chronic emphysema, emphysema with bronchitis, chronic asthma, tuberculosis,
and bronchiectasis, pneumonia and tracheobronchitis,cystic fibrosis,in acetaminophen
overdosage.
Expectorants are used to help raise respiratory secretions.
An expectorant may also be included along with one or more additional drugs, such as an
antihistamine, decongestant, or antitussive, in some prescription and nonprescription
cough medicines.
Antitussives,Mucolytics and Expectorants





AUTOCOIDS
Dr A. Shyam Sundar,
Assistant Professor in Pharmacology,
University of Nizwa,
Sultanate of Oman

Overview Autocoids are local hormones which are produced locally, exert their
actions locally and degraded locally.
They can be derivatives of
1. Amines (Histamine and Serotonin).
2. Peptides (Bradykinin,Angiotensin).
3. Lipids (Prostaglandins, Leukotrienes and Platelet activating factor)
Histamine , Serotonin will be discussed in detail in this lecture.
We have already discussed the actions of Angiotensin in the chapter
anti-hypertensive drugs and Leukotrienes were discussed during
anti asthmatic lectures.

HISTAMINE- RECEPTORS LOCATION AND
ACTIONS

HISTAMINE RECEPTOR BLOCKERS AND THEIR
CLINICAL USES
H1 receptor blockers:
First generation:
Azelastine
Chlorpheniramine
cyproheptadine
Diphenhydramine
Hydroxyzine
Phenindamine
Promethazine
Tripelenamine
Second generation :
Cetirizine
Desoratadine
Fexofenadine
Loratadine
Clinical uses of H1 receptor blockers
Urticaria
Hypersensitivity reactions

ADRs of
H1 antagonists

HISTAMINE RECEPTOR BLOCKERS AND THEIR
CLINICAL USES
Clinical uses:
Peptic Ulcer
Zollinger-Ellison Syndrome
Acute Stress ulcers
Gastroesophagal reflex disease

SEROTONIN
Serotonin is an indole ethylamine found in both plant and animal tissues.
90% of serotonin is present in GI tract and 10% present in CNS.
Serotonin exert its action through seven major 5-HT cell membrane receptor
subtypes.
Physiological actions of Serotonin:


PROSTAGLANDINS
Impotence
Therapeutic Uses of Prostaglandins:
Several of the naturally occurring prostaglandins, such
as dinoprost , dinoprostone , and carboprost , find use as
abortifacients . Misoprostol in combination with methotrexate is
particularly effective in terminating pregancy in the first trimester.
Misoprostol is a synthetic prostaglandin E1 analog used to inhibit
the secretion of hydrochloric acid in the stomach. It produces
inhibition of gastric acid and pepsin secretion and enhances
mucosal resistance to injury. Misoprostol is particularly useful in
patients with gastric ulcer who are chronically taking nonsteroidal
anti-inflammatory agents
Alprostadil injected into the corpus cavernosum of
the penis provides effective treatment of some forms
of male impotence.

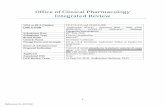
ANTI ULCER DRUGS

ANTIULCER DRUGS DR A SHYAM SUNDAR., A peptic ulcer is an open sore or raw area on the lining of the stomach
(gastric ulcers), or on the duodenum (duodenal ulcers). Define ulcer and compare and contrast Gastric &duodenal Ulcer Identify the classification of drugs Used to treat PUD Describe treatment goals for PUD Know prototype drugs in each classification &their details Use Pharmaceutical process for the welfare of the clients receiving
drug therapy for PUD

Proglumide ACh
PGE2
Histamine Gastrin
Adenyl
cyclase
_ +
ATP cAMP
Protein Kinase (Activated)
Ca++
+
Ca++
Proton pump
K K+ H+
Gastric acid
Parietal cell
Lumen of stomach
Antacid Omeprazole
Ranitidine
H2 M3
Misoprostol
_
_
_
_
+
PGE receptor
+
+
Gastrin
receptor +
+
+
See Animation

Can you identify these people ?
Nobel prize
Medicine –
2005
Barry J Marshall J. Robin Warren
Discovery of
H.pylori &
its role in
ulcer

Antacids
• Weak bases that neutralise acid
• Also inhibit formation of pepsin
(As pepsinogen converted to pepsin at acidic pH)
• Present day antacids :
Aluminium Hydroxide
Magnesium Hydroxide
• OTC drug for symptomatic relief of dyspepsia
Duration of action :
30 min when taken in empty stomach
2 hrs when taken after a meal
Side effects :
Al3+ antacids – constipation (As they relax gastric smooth muscle & delay gastric emptying)
Mg2+ antacids – Osmotic diarrhoea .
In renal failure Al3+ antacid – Aluminium toxicity & Encephalopathy

Antacids – Common additives & Interactions
Adsorb drugs and form
insoluble complexes that
are not absorbed .
Clinical importance :
Interactions can be
avoided by taking antacids
2 hrs before or after
ingestion of other drugs .
Simethicone – Decrease
surface tension ,thereby
reduce bubble formation
Added to prevent reflux .
Alginates- Form a layer of
foam on top of gastric
contents & reduce reflux
Oxethazaine – Surface
anaesthetic

Histamine H2 Receptor Antagonist
• Reversible competitive inhibitors of H2 receptor
• Highly selective, No action on H1 or H3 receptors
• Very effective in inhibiting nocturnal acid secretion (as it depends largely on Histamine )
• Modest impact on meal stimulated acid secretion (As it depends on gastrin, acetyl choline and histamine)
H2 Blockers–Side effects &
Interactions
Extremely safe drugs
• Cimetidine causes gynecomastia, galactorrhea
(as it is antiandrogenic & increases prolactin level)
• Cimetidine inhibits CYP450 & increases conc. of Warfarin, Theophylline, Phenytoin, Ethanol.

Proton Pump Inhibitors
Most effective drugs in antiulcer therapy
Irreversible inhibitor of H+ K+ ATPase
Prodrugs requiring activation in acid environment
Weakly basic drugs & so accumulate in canaliculi
of parietal cell
Activated in canaliculi & binds covalently to
extracellular domain of H+ K+ ATPase
Acid secretion resumes only after synthesis of new
molecules
Half life is about 1.5 hrs

Proton Pump Inhibitors
Omeprazole 20 mg o.d.
Esomeprazole 20 - 40 mg o.d.
Lansoprazole 30 mg o.d.
Pantoprazole 40 mg o.d.
Rabeprazole 20 mg o.d.

Poton Pump Inhibitors – Kinetics
Given as enteric coated granules in capsule or
enteric coated tablets
Pantoprazole also given intravenously
Half life – 1.5 hrs
Since it requires acid for activation - given 1 hr
before meals
Other acid suppressing agents not coadministered

P.P.I. – Side effects & Interactions
Extremely safe drugs
Causes hypergastrinemia which leads to carcinod
tumor in rats
But no evidence of such tumors in man
Inhibit CYP 450 & hence metabolsim of warfarin,
phenytoin, etc
Pantoprazole & Rabeprazole have no significant
interactions

Mucosal Protective Agents
• Sucralfate
• Misoprostol
• Colloidal Bismuth compounds
Sucralfate • Salt of sucrose complexed to
sulfated aluminium hydroxide
• In acidic pH polymerises to viscous gel that adheres to ulcer crater
• Taken on empty stomach 1 hr. before meals
• Concurrent antacids, H2 antagonist avoided
( as it needs acid for activation )

Colloidal Bismuth Compounds
• Coats ulcer, stimulates mucus & bicarbonate secretion
• Direct antimicrobial activity against H.pylori
• May cause blackening of stools & tongue
• Not used for long periods – bismuth toxicity
Misoprostol • PGE1 analogue
• Modest acid inhibition
• Stimulate mucus & bicarbonate secretion
• Enhance mucusal blood flow
• Approved for prevention of NSAID induced ulcer
• Diarrhoea & cramping abd. pain – 20 %
• Not so popular as P.P.I are more effective & better tolerated

Triple Therapy
The BEST among all the Triple therapy regimen is
Omeprazole / Lansoprazole - 20 / 30 mg bd
Clarithromycin - 500 mg bd
Amoxycillin / Metronidazole - 1gm / 500 mg bd
Given for 14 days followed by P.P.I for 4 – 6 weeks
Short regimens for 7 – 10 days not very effective

Triple Therapy – cont …
Bismuth subsalicylate – 2 tab qid
Metronidazole - 250 mg qid
Tetracycline - 500 mg qid
Some other Triple Therapy Regimens are
Ranitidine Bismuth citrate - 400 mg bd
Tetracycline - 500 mg bd
Clarithromycin / Metronidazole - 500 mg bd

Quadruple Therapy
Given when Triple Therapy fails
Omeprazole / Lansoprazole - 20 / 30 mg bd
Bismuth subsalycilate - 2 tabs qid
Metronidazole - 250 mg qid
Tetracycline - 500 mg qid

Now you have learnt about drugs used for treating
peptic ulcer ? Are there any drugs that can cause peptic
ulcer ?
Drugs causing peptic ulcer
Non Steroidal Anti Inflammatory Drugs
(NSAIDs)
Glucocorticoids
Cytotoxic agents

Antiemetics

Vomiting
Centre
(medulla)
Cerebral cortex
Anticipatory
emesis
Smell
Sight
Thought
Vestibular
nuclei Motion
sickness
Pharynx &
GIT
Chemo & radio
therapy
Gastroenteritis
Chemoreceptor
Trigger Zone
(CTZ)
(Outside BBB)
Cancer chemotherapy
Opioids
Muscarinic, 5 HT3
& Histaminic H1
5 HT3
receptors
Dopamine D2
5 HT3,,Opioid Receptors
Muscarinic
Histaminic
H1
Pathophysiology of Emesis

Now answer this question
Which group of drugs can be used as
antiemetics ?
Serotonin 5 HT3 Antagonists
Dopamine D2 Antagonist
Anticholinergics
H1 Antihistaminics
Cannabinoids

Serotonin 5 HT3 Antagonist
Potent antiemetics
Even though 5 HT3 receptors are present in
vomiting centre & CTZ, the antiemetic action is
restricted to emesis caused by vagal
stimulation.
High first pass metabolism
Excreted by liver & kidney
No dose reduction in renal insufficiency but
needed in hepatic insufficiency
Given once or twice daily – orally or
intravenously.

Drugs Available
Ondansetron 32 mg / day
Granisetron 10 mg / kg / day
Dolasetron 1.8 mg / kg / day Indications Chemotherapy induced nausea & vomiting – given 30
min. before chemotherapy.
Postoperative & postradiation nausea & vomiting
Adverse Effects
Excellent safety profile
Headache & constipation
All three drugs cause prolongation of QT interval, but
more pronounced with dolasetron.

Dopamine D2 Antagonist
Antagonise D2 receptors in CTZ.
Drugs available
Metoclopramide 2.5 mg b.d
Domperidone 10 mg b.d
Both drugs are also prokinetic agents due to
their 5 HT4 agonist activity.
Domperidone – oral ; Metoclopramide – oral &
i.v
Metoclopramide crosses BBB but domperidone
cannot.

Phenothiazines & Butyrophenones
Phenothiazines
Prochlorperazine
Promethazine
Phenothiazines are antipsychotic with
potent antiemetic property due to D2
antagonism.
Butyrophenone
Droperidol
Droperidol used for postop. nausea &
vomiting, but cause QT prolongation.

H1 Antihistaminics
Most effective drugs for motion sickness
Drugs available
Meclizine
Cyclizine
Dimenhydrinate
Diphenydramine
Promethazine – Used in pregnancy, used by
NASA for space motion
sickness

Anticholinergics
Scopolamine (hyoscine) – used as
transdermal patch for motion sickness
Cannabinoids
Dronabinol – used as adjuvant in
chemotherapy induced vomiting.It is a
psychoactive substance
Nabilone

Summary

What’s Latest?
Aprepitant…(nk-1 receptor Blocker)
Rational Thinking:
a. Atropine
b. Scopolamine (TDP)



















