Pharmacology (Corticosteroids Lecture)

If you can't read please download the document
-
Upload
ashfaq-ahmad -
Category
Health & Medicine
-
view
2.995 -
download
0
Transcript of Pharmacology (Corticosteroids Lecture)
Slide 1
ENDOCRINOLOGYDr. Ashfaq Ahmad
ADRENOCORTICAL HORMONE
ADRENOCORTICOSTEROIDS
CORTICOSTEROIDS
Dr. Ashfaq Ahmad
DERIVATIVES OF CHOLESTEROLCarbon atomsParent HydrocarbonBiologically imp. compoundC18OestraneOestrogenC19AndrostaneAndrogenC21PregnaneProgesteroneAdrenal hormones
Cyclo Pentano Perhydro Phenanthrine Ring
Steroid Nucleus
CholesterolPregnenoloneProgesterone17-hydroxy pregnenolone17-hydroxy progesteroneDeoxy CortocosteronDehydroEpiandrosterone11-DeoxycortisolCorticosteroneAndrostenedioneALDOSTERONECORTISOLETESTOSTERONE
CortisoneESTRADIOL
C21 SteroidsSELYS TERMINOLOGYGlucocorticoids ( Cortisole )Energy metabolismCarbohydrate, Protein,FatMineralocorticoids ( Aldosterone )ElectrolytesNa, K, Fluid balanceSyntheticPrednisoloneDexamethasone9-a-Flourocortisole
Adrenocortical HormonesZ. FasicuZ. GlomeruZ. ReticulataGlucocorticoidsAldosteroneAndrogen (Hydrocorisone)(Renin-Angiotensinsystem.) ( Salt Retaining )- DHEA, DHEAS, ( DEHYDROEPIANDROSTERONE )-AndrostenedioleSource of ESTROGEN- IN Or AFTER MenopauseNet effect- Defective/Absent OvaryAntagonism of Insulin
CVS FUNCTIONSGROWTHimmunity
Steroid PreparationsAn ideal Glucocorticoid should not have Mineralocorticoid Activity
By structural changes (many compounds)
With minimal Mineralocorticoid ActivityGreater PotencyLonger duration of actionStability Plasma Half lifeRate of Elimination
Injectable
Betamethasone, Dexamethasone MethylprednisolonePrednisolone, Hydrocortsone, TriamacinoloneOral
Betamethasone, Dexamethasone Methylprednisolone, Prednisolone,Prednisone. Fludricortisone
Topical
ClobetasolFlucinolonMometasoneBetamethasone
Inhalational
BeclomethasoneBudesonideFlunisolide
Mechanism of ActionSpecific ReceptorsGRsMRsTwo Genes Control the formation of these receptors
Alternative splicing of human GR Pre-mRNA generate two isoforms -- hGR alpha in human, Classic form of GRs ( transcriptionly active )--h GR beta - Not transcriptionaly active- Inhibit the effects of hormone-activated hGR alpha effects (Physiological Endogenous relevant inhibitor)Two hGR alternative transcripts have 8 translation initiation sites 16 GR alpha & GR beta Isoforms 256 homodiamers & heterodiamers
Glucocorticoid Receptor800 Aminoacids3 Functional DomainsGlucocorticoid binding domainAt carboxyl terminal of the moleculeDNA binding domainLocated in the middle, 9 cysteine Residues, Two finger structure Stabilized by Zinc ions connected with cysteine. Form two terahedronesTranscription activating domainAmino terminal ( Transactivation of receptor & Increase specificity)
Ligand binding conformational change (hsp90)DiamerizationEntry in nucleusIn the Responsive Gene promoter have receptor Element (GRE) attachment with GRE at specific site
Ligand bound receptor form complexes with other Transcription Factors (AP1, NF-KB) non GRE containing PromotersContribute to - Regulation of Transcription of responsive Genes- Regulation of Growth factors, proinflammotory cytokines, Antigrowth, Anti-inflammatory, Immunosuppressive effects of glucocortciods
Coregulators
Proteins (several families) are
Involved in
Interaction of ligand bound GR with GREs & other Transcription factors
Facilitate (co activators)Inhibit (co repressors)
Effects 0f GlucocorticoidsDirect EffectsGluconeogenesis (Net effect mimic Diabetes) Homeostatic ResponseIn Response ofInsulin, GlucagonPermissive Effects (Normal / Physiological)Sensitization to Catacholamine ActionsVascular SMsBronchial SMsFat CellsSensitization toACTH effectsGH effects
Fetal Lung Maturation
CVSSteroid receptors on SMs of vesselsDirect effects on VMSBy sensitazation to catecholaminesBy increasin circulating volumeDirect effects on Heart & Vessel toneB.P. Regulation
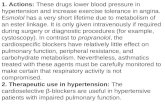
Therapeutic Effects/usesDiagnostic dexamethasone suppression TestTreatmentDefficiency( HRT ( Hormone Replacement Therapy )Anti-inflammatory (all steps of inflammation are blocked ( basis of use )Rh. Arthritis- HIV related disordersBr. Asthma- ShockHypersensitivity ReactionNephrotic Synd- LeukemiaSLE- Cronns DiseaseBells Palsy
Effects on Events of InflammationDramatically reduce inflammationsuppress cytokines, chemokines, Affect leukocytes (conc. Dist. Function)
Infiltration of leukocytesWhite cell adhesion moleculesIn the BloodNeutrophils Mono, Baso, EosinoLympho ( T, B )
ImmunosuppressionAntigen Presenting ( Grafted Cells )Delay VascularizationInterfere with sensitizationCytotoxic T-Lymphocytes ( Decrease )Antibody Forming Cells ( Decrease )
Dexamethasone Suppression TestFor Diagnosis of Cushing Syndrome& Depressive Psychatric IllnessFirst Screening test1mg at 11 PM . Plasma sample in morningIf more than 5mcg ( normal 3mcg)Then Suppression With Large Doses0.5 mg oral 6hrly for 2 days . Urine assay8mg at11PM . Plasma cortisol in the morning
Therapeutic Uses of Corticosteroids
COMPLICATIONSSide effects / ToxicityGITPeptic UlcerFatty LiverPancreatitisNausea, Vomiting OcularIncreased IOPPost. Sub. Cap. CataractSkinThinning, AchneHirsutismStriae PupuraCNSInsomniaDepressionPsychosisNervousnessFluid & ElectrolytesNa Retension, K lossHypertensionGeneralMetabolicHyperglycemiaMusculoskeletalMyopathy, Growth FailureOsteopenia
Mineralocorticoid
MinrelocorticoidsNatural
Aldosterone ( zona glomeruloza )Deoxycoticosterone ( DOC ) Not used
Synthetic
Fludrocortisone
Aldosterone
Zona glomeruloza
Relese is through ACTH .. 50% feed back controle on release as compared to cortisole
Angiotensin Maintain & regulate secretion
Physiological & PharmacologicalEffects of AldosteroneReabsorption Na from DCT, which is loosely coupled to excretion of K & H ions
Receptors in cytoplasm of target cellsDrug receptor complex MOA As GC This receptors has same affinity for GC Metebolism is same as GCDOC (Deoxy corticosterone ) is precursor as Aldosterone
Fludrocortisone Potent SteroidBoth Mineralocorticoid & Glucocorticoid activity
Oral 0.1mg, two to seven times weekly( potent salt retaining activity )Used in INSUFFICIENCY
Dose is too small to have anti inflamatory, or antigrowth activity
Adrenal AndrogensDHEA (Alternate source of Estrogen in menopausal age )AndrostendioneTestosterone
Do not stimulate or support major androgen puberty changes
Synthesis inhibitors & Glucocorticoid Antagonist
Aminoglutethemide ( Block conversion ofcholesterol to pregnenolone )Ketoconazole ( antifungal.. Also block synthesis)Metyrapone ( block cortisole & corticosterone synthesisTrilostane ( inhibit adrenal & Gonadal hormones)Abiraterone ( Synthesis Inhibitors )
Mifepristone ( RU486 )(GC receptor Blocker)
Mitotane ( Cytotoxic,DDT group, less toxic for human, ORAL, toxic effect may reduce dose, Withdrawn in USA, Available on compassionate
Mineralocorticoid AntagonistSpironolactone ( K sparing Diuretic )Eplerenone ( more selective than spironolactone, ( HTN 50-100mg/day)Drospirenone ( also progestin in OCP)
THANKS