Pharmacol ogical Sci ences 2015; 19: 2983-2996 … · 2015. 9. 1. · on 6 th December 2013, when a...
14
Abstract. – OBJECTIVE: The deadly Ebola virus has been first known to mankind since 1976. In the past decades, Ebola outbreaks has often been ignored/neglected as erupted in the rural re- mote/isolated areas of Africa. The recent 2013-2014 epidemic is the most wide-spread with high inci- dence rates, morbidity and, mortality in the Ebola history. Eventually, the World Health Organization (WHO) has declared it as a ‘Public Health Concern of the International Community’. This scrutiny was conducted to initiate a serious debate on various aspects of Ebola, particularly blood transfusion as an empirical therapeutic modality. METHODS: A search has been performed us- ing the premier scientific databases, WHO docu- ments, and English language search engines. Of 278 potential articles that were identified using a fixed set of criteria, a convenience sample of eighty-two appropriate articles was chosen for this review. RESULTS: The current EBO outbreak is pre- dominantly driven by various confounding risk- factors like: (1) frail health care system, (2) unique cultural and religious customs, (3) huge- shortage of skilled professionals, (4) no licensed therapeutic agents, (5) ill-prepared monitoring and early warning systems, and (6) strained bud- gets; all these have bolstered this epidemic. As lack of neither specific treatments nor reliable interventions to quickly quell this epidemic, WHO has indorsed ‘blood transfusion as an em- pirical therapeutic modality’. Currently, several clinical trials are underway, particularly the two Ebola candidate vaccines and several antiviral drugs and it has been observed that the initial results are quite promising. However, there are several daunting ethical and practical chal- lenges ahead to stem off this outbreak. CONCLUSIONS: The Ebola-hit poverty strick- en West-African countries struggle to contain the outbreak, due to lack of potent therapeutics. Consequently, blood-transfusion could serve as an ideal therapeutic modality to save millions of lives. Therefore, industrialized nations and inter- national agencies must aid them to combat with this catastrophe. Besides, it must warrant further European Review for Medical and Pharmacological Sciences Ebola and blood transfusion: existing challenges and emerging opportunities S. ABDULLAH 1 , K. KARUNAMOORTHI 2 1 Laboratory Medicine Department, Faculty of Applied medical Sciences, Jazan University, Kingdom of Saudi Arabia 2 Unit of Tropical Diseases, Division of Medical Entomology and Vector Control, Department of Environmental Health, Faculty of Public Health and Tropical Medicine, Jazan University, Kingdom of Saudi Arabia Corresponding Author: Kaliyaperumal Karunamoorthi, MD; e-mail: [email protected] 2983 multi-layered interventions and interagency poli- cies, in order to build an Ebola-free safe world in the near future. Key Words: Ebola, Blood transfusion, Ebola virus, West African Countries, Therapuetic agents. Introduction Ebola is a deadly infectious disease of humans and other primates and is often fatal. Ebola virus- es (EBOV) cause a rash, reddened eyes, hiccups, substantial intravascular volume depletion and marked electrolyte abnormalities attributable to both internal and external bleeding 1 . It first emerged in a small remote village of the Democ- ratic Republic of Congo (DRC) near the Ebola River, subsequently it’s named as an ‘Ebola hem- orrhagic fever’ 2 . Though EBOV was first identi- fied in southern Sudan in 1976 3 , but most likely occurred as early as 1972 in Tandala, DRC (for- merly known as Zaire) 4 . The recent outbreak erupted in Guinea in De- cember 2013 but soon spurted into neighboring Liberia and Sierra Leone with a reported seventy percent of the case fatality rate 5 . It is unprecedent- ed in terms of number of cases, mortality rate and deleterious socio-economic impact. Thereupon World Health Organization (WHO) declared Ebo- la as a ‘Public Health Emergency of International Concern’ on 8 th August 2014 2 . To date there is no specific preventive and curative therapeutic agent in existence, henceforth, EBOV remains to pose a serious public health threat to both civilian and military populations as bio-weapons 6 . Though, ever since the mid of 1970s there are several sporadic outbreaks reported, 2014 epidem- ic has broken down the entire civic society by killing thousands of people, destroying families 2015; 19: 2983-2996
Transcript of Pharmacol ogical Sci ences 2015; 19: 2983-2996 … · 2015. 9. 1. · on 6 th December 2013, when a...
-
Abstract. – OBJECTIVE: The deadly Ebolavirus has been first known to mankind since 1976.In the past decades, Ebola outbreaks has oftenbeen ignored/neglected as erupted in the rural re-mote/isolated areas of Africa.The recent 2013-2014epidemic is the most wide-spread with high inci-dence rates, morbidity and, mortality in the Ebolahistory. Eventually, the World Health Organization(WHO) has declared it as a ‘Public Health Concernof the International Community’. This scrutiny wasconducted to initiate a serious debate on variousaspects of Ebola, particularly blood transfusion asan empirical therapeutic modality.
METHODS: A search has been performed us-ing the premier scientific databases, WHO docu-ments, and English language search engines. Of278 potential articles that were identified using afixed set of criteria, a convenience sample ofeighty-two appropriate articles was chosen forthis review.
RESULTS: The current EBO outbreak is pre-dominantly driven by various confounding risk-factors like: (1) frail health care system, (2)unique cultural and religious customs, (3) huge-shortage of skilled professionals, (4) no licensedtherapeutic agents, (5) ill-prepared monitoringand early warning systems, and (6) strained bud-gets; all these have bolstered this epidemic. Aslack of neither specific treatments nor reliableinterventions to quickly quell this epidemic,WHO has indorsed ‘blood transfusion as an em-pirical therapeutic modality’. Currently, severalclinical trials are underway, particularly the twoEbola candidate vaccines and several antiviraldrugs and it has been observed that the initialresults are quite promising. However, there areseveral daunting ethical and practical chal-lenges ahead to stem off this outbreak.
CONCLUSIONS: The Ebola-hit poverty strick-en West-African countries struggle to containthe outbreak, due to lack of potent therapeutics.Consequently, blood-transfusion could serve asan ideal therapeutic modality to save millions oflives. Therefore, industrialized nations and inter-national agencies must aid them to combat withthis catastrophe. Besides, it must warrant further
European Review for Medical and Pharmacological Sciences
Ebola and blood transfusion: existingchallenges and emerging opportunities
S. ABDULLAH1, K. KARUNAMOORTHI2
1Laboratory Medicine Department, Faculty of Applied medical Sciences, Jazan University, Kingdomof Saudi Arabia2Unit of Tropical Diseases, Division of Medical Entomology and Vector Control, Department ofEnvironmental Health, Faculty of Public Health and Tropical Medicine, Jazan University, Kingdomof Saudi Arabia
Corresponding Author: Kaliyaperumal Karunamoorthi, MD; e-mail: [email protected] 2983
multi-layered interventions and interagency poli-cies, in order to build an Ebola-free safe world inthe near future.
Key Words:Ebola, Blood transfusion, Ebola virus, West African
Countries, Therapuetic agents.
Introduction
Ebola is a deadly infectious disease of humansand other primates and is often fatal. Ebola virus-es (EBOV) cause a rash, reddened eyes, hiccups,substantial intravascular volume depletion andmarked electrolyte abnormalities attributable toboth internal and external bleeding1. It firstemerged in a small remote village of the Democ-ratic Republic of Congo (DRC) near the EbolaRiver, subsequently it’s named as an ‘Ebola hem-orrhagic fever’2. Though EBOV was first identi-fied in southern Sudan in 19763, but most likelyoccurred as early as 1972 in Tandala, DRC (for-merly known as Zaire)4.
The recent outbreak erupted in Guinea in De-cember 2013 but soon spurted into neighboringLiberia and Sierra Leone with a reported seventypercent of the case fatality rate5. It is unprecedent-ed in terms of number of cases, mortality rate anddeleterious socio-economic impact. ThereuponWorld Health Organization (WHO) declared Ebo-la as a ‘Public Health Emergency of InternationalConcern’ on 8th August 20142. To date there is nospecific preventive and curative therapeutic agentin existence, henceforth, EBOV remains to pose aserious public health threat to both civilian andmilitary populations as bio-weapons6.
Though, ever since the mid of 1970s there areseveral sporadic outbreaks reported, 2014 epidem-ic has broken down the entire civic society bykilling thousands of people, destroying families
2015; 19: 2983-2996
-
S. Abdullah, K. Karunamoorthi
Results
The study selection process is given in Figure1 as a flow diagram. Of 228 potentially relevant,unique citations from all literature searches, six-ty-one studies met the inclusion criteria. Twenty-seven studies were empirical research studies;three were booked chapters, two of them is fromconference and three involved systematic reviewsand meta-analyses, with the rest twenty-six in-volving case reports or press releases. The major-ity of studies was carried out in the WHO definedAfrican region (n=48), and the remaining studies(n=13), covers the rest of the world; the majorityof them have been published later than 2012.Meta-analysis was not performed as the includedstudies were heterogeneous in important aspects,including: populations (different ages and set-tings), and study designs (cross-sectional, case-control, cohort).
FilovirusesFiloviruses are lager, negative stranded, non-
segmented RNA viruses with a characteristic ofthread like structure, henceforth the family nameis Filoviridae (Latin filum = thread). Over thepast decades, several natural outbreaks have beenreported in the DRC, Sudan, Uganda, Angola,and Gabon6. Both Marburg and Ebola species aremorphologically identical, but vary in length7.They are imposing potential threats to humans aswell as non-human primates8. Filovirus illness ischaracterized by fever, myalgia, headache, andgastrointestinal symptoms, and patients may alsodevelop a maculopapular rash. Death has oftenbeen correlated with increased viremia, convul-sions, and disseminated intravascularcoagulation9.
Ebola Virus: An Old Enemy andRecent Killer
It is an ancient one, having split off from otherviruses dating back thousands of years with a rel-atively constant mutation rate10. Filoviridae in-cludes three genera viz., Cuevavirus, Mar-burgvirus, and Ebola virus. EBOV is a filoviruswith a 19-kb, non-segmented, negative-strandRNA genome that encodes seven viral proteins11.Till date, five genetically distinct subspecies havebeen identified, namely Zaire, Bundibugyo, Su-dan, Reston and Taï Forest. However, threespecies [(Bundibugyo Ebola virus (CôteD’Ivoire); Zaire Ebola virus (Democratic Repub-lic of the Congo, formerly Zaire); and Sudan
and threatening the world. It is a matter of graveconcern that urges us to find a countermeasurequickly to fight against the ‘common enemy’ ofmankind. In these perspectives, the present com-munication becomes more significant and pertain.
This review is an attempt to initiate serious de-bates on various Ebola related issues like modeof transmission, high risk-groups, symptoms, ex-isting therapeutic modalities, particularly bloodtransfusions. Furthermore, it is an effort to shedsome limelight on the existing practical chal-lenges and emerging opportunities to minimizethe Ebola related illness and deaths by adoptingblood transfusion as one of the empirical thera-peutic modalities. We strongly believe that theoutcome of this scrutiny could serve as a baselinedata for public health care providers and policy-makers to combat with Ebola outbreaks or epi-demics effectively in the near future.
Methods
Data Mining: Evidence AcquisitionIdentification of studies
The search strategy and terms were developedcollaboratively with the assistance from the in-formation specialists. An appropriate search wasperformed in PubMed, Google Scholar, Web ofScience, EMBASE, Scopus, World Health Orga-nization’s WHOLIS, Research gate, and Acade-mic Premier databases in English, using theterms: “Ebola virus disease /Recent outbreak”OR “Ebola and blood transfusion”, “Ebola andPublic Health”, “Ebola transmission”, “Ebolaand Human Health” ‘ Ebola and West Africa’ and“Ebola vaccine” to include articles publishedwithout time limitations i.e., from earliest tomost recent (December 2014).
Potentially relevant articles (in all languages)and websites were accessed in order to reviewthe full-text. Besides, references cited by eachrelevant paper, review, and book chapters werealso scrutinized to identify additional potentialpapers. Furthermore, the reference lists of all ar-ticles were hand-searched, and the full text ofthose references that appeared relevant to Ebolaand blood transfusion were retrieved. The exclu-sion and inclusion criteria for choosing the ap-propriate research articles, notes and reviewswere shown in Figure 1 for this narrative review,and their bibliographic details (authors, title, fullsource, document type and addresses) have beendownloaded and maintained in a file.
2984
-
Figure 1. The exclusion and inclusion criteria, for choosing the appropriate research articles, notes and reviews for this narra-tive review.
Ebola virus (Sudan)] have been associated withlarger outbreaks in Africa. The recent 2014 WestAfrican outbreak was caused by the Zaire Ebolavirus (ZEBOV)2, with a ninety percent of mortal-ity rate12 and it cannot further mutate and becomemore contagious10.
Existing Ebola Virus StrainsIn 1976, the first outbreak of Ebola (Ebola-Su-
dan) was reported in southern Sudan and a fewmonths later, the second Ebola virus emergedfrom Yambuku, Zaire, Ebola-Zaire (EBOZ). Thethird strain of Ebola, Ebola Reston (EBOR), wasfirst identified in 1989 when infected monkeyswere imported from the Philippines to Reston,Virginia, United States of America. The last
known strain of Ebola, Ebola Cote d’Ivoire(EBO-CI) was discovered in 1994 when a femaleethologist was performing a necropsy on a deadchimpanzee from the Tai Forest, Cote D’Ivoire,got accidentally infected herself during thenecropsy13.
The Deadly History of Ebola OutbreaksIt is not a new disease of mankind and typical-
ly occurs as deadly outbreak in the resource-con-strained tropical Sub-Saharan Africa. Since midof 1970s to until December 2013, 1,716 con-firmed cases have ever been reported2,10. To date,the ongoing 2014 West African Ebola outbreak isthe largest, which affects many African countriesviz., Guinea, Sierra Leone, Liberia, Mali, and
2985
Ebola and blood transfusion: existing challenges and emerging opportunities
-
2986
Nigeria. As of 7th January 2015, 20 747 suspect-ed cases and 8235 deaths had been reported14.Past Ebola outbreaks have been elaborately illus-trated in terms of number of cases and deaths inFigure 22.
High Risk GroupWhoever in close contact with Ebola patients
are at the highest risk of infection, notablyhealthcare providers, close family members, andfriends as they have higher probabilities to be in-fected by blood or body fluids of patients10. For-tunately, Ebola survivors cannot serve as a sourceof infection. It spreads rapidly during outbreakswithin healthcare settings and could be easilyevaded by wearing appropriate personal protec-tive equipment10. As of 23 October 2014, nearly450 health care workers (HCWs) [eighty-in-Guinea; 228 in Liberia; eleven in Nigeria; 127 inSierra Leone; one in Spain; and three in the US]are known to have been infected and a total of244 HCWs have died during 2014 outbreakalone15,16. Quite a considerable number of peoplehave acquired infection by means of attendingthe burial ceremonies of Ebola victims17.
Ebola Recent outbreak: a Public HealthEmergency of International ConcernGround Zero in Guinea: the outbreakSmoulders
Currently, West Africa is experiencing theworld’s largest Ebola outbreak18. It has eruptedon 6th December 2013, when a two-year-old malechild Emile (the first known case of 2014 Ebolaepidemic) in Meliandou village, Guéckédou Pre-fecture, in the Nzérékoré Region of southernGuinea got infected19-21. It is one of the most dif-ficult villages to reach by road and it is a two-daydrive from the national capital of Conakry, fol-lowed by a long walk through the dense rain-for-est22. This outbreak’s ‘hot zone’ (Meliandou) islocated in a triangle-shaped forested area, wherethe borders of Guinea, Liberia and Sierra Leoneshared. As a result of decades of civil wars andunrest, these countries has deeply been impover-ished and the health infrastructures have severelybeen damaged19.
Death Toll and MorbidityAs of 7th January 2015, a total of 20 747 cases
(confirmed, probable, and suspected cases ofEbola) and 8 235 deaths have been reported infive Ebola-hit countries viz., Guinea, Liberia,Mali, Sierra Leone, and the USA and in three
S. Abdullah, K. Karunamoorthi
Figure2.T
hepr
evio
usEbo
lavi
rusdi
seas
eou
tbre
aks.
-
previously affected countries viz., Nigeria, Sene-gal and Spain14. Reported case incidence isslightly increasing in Guinea, declining inLiberia, and may still be increasing in SierraLeone. The case fatality rate across the threemost-affected countries in all reported cases witha recorded definitive outcome is seventy-six per-cent; in hospitalized patients the case fatality rateis sixty-one percent23. WHO has estimated that itmay take nearly six-to-nine months to contain theongoing outbreak and during this period of timeit may likely to claim another 20,000 lives. Re-cent WHO (2014)24 report indicates that cases inLiberia are under-reported. It may be due toasymptomatic infections, which have also beenobserved in earlier outbreaks too25. Ebola impos-es an urgent public health threat not only toAfrica but also to the rest of the world.
Driving Forces of Recent OutbreakPast outbreaks have flared up in the remote
and isolated forested communities and these out-breaks die out, like the flare-up in the centralAfrican countries like DRC in the past fewmonths26. However, the recent 2013-2014 out-break is the largest and most complex in terms ofduration, number of people affected, and geo-graphic extent27. Currently, Ebola has been con-sidered as not only as a public health emergency,but also as a ‘poverty’, ‘infrastructure’, as well asa ‘educational’ crisis26. This epidemic (2014-2015) driven by various sociological, ecological,and environmental determinants, has both direct-ly and indirectly influenced the emergence ofEbola in the poverty pervasive West Africancountries.
High-risk of confounding factors (Alexanderet al, 2014)27:
• Free people movement – rural-to-urban mi-gration as well as extensive movement of peo-ple within and across borders.
• Decades of civil war/unrest – have severelyweakened the basic and health care sector in-frastructures.
• Behavioral and cultural practices – tradi-tional customs/practices like burial ceremonytraditions and rites.
• Bush meat consumption – principal mecha-nism of EBOV spillover from wildlife reser-voirs to humans.
• Traditional medicine and cures – it delaysthe Ebola patient to access life-saving qualityhealthcare.
Natural Host and Mode of TransmissionFruit Bats (Family: Pteropodidae) are serving
as a natural host. EBOV introduced into the hu-man through close contact through body fluidsand other secretions of infected wild-animalsviz., chimpanzees, gorillas, fruit bats, monkeys,antelope and porcupines found ill or dead5. Onceinfection is established, it can be transmittedthrough human-to-human via direct contact withthe blood, secretions, organs or other bodily flu-ids (including but not limited to urine, saliva,sweat, feces, vomit, breast milk, and semen) ofinfected human28, and animals [fruit bats or pri-mates (apes and monkeys)]. Human handling andconsumption of contaminated bushmeat (Ebolainfected animals) has been cited as a majorsource of transmission to human5.
A study found that the case mortality rateshighly correlate with the mode of transmission.Overall, hundred and eighty percent mortality wasobserved among those exposed via contaminatedneedles, and close-contact with infected people,respectively29. Aerosol transmission has also beenreported but only in the laboratory settings30 and israre or absent in natural outbreaks31. The contami-nated surfaces, materials (bedding, clothing), andobjects (needles and syringes) could also transmitinfection. Therefore, healthcare professional areat the highest risk of infection, when the transmis-sion control protocols (TCP) are not strictly prac-ticed5. People remain infectious as long as theirblood and body fluids (including semen and breastmilk), contain the Ebola virus5. There is no evi-dence that mosquitoes or other insects can trans-mit EBOV10.
Mode of Disease Causing Mechanismand Pathophysiology
Ebola virus kills cells, making some of them toexplode. Subsequently, it wrecks the immune sys-tem, causes heavy internal hemorrhage and elec-trolytes abnormalities. It virtually damages everyorgan32, often leading to death31,33. Distinguishingthe symptoms of Ebola from other infectious dis-eases is quite a challenging task. However, it canbe diagnosed by performing standard serologicaldiagnostic tests like antibody-capture enzyme-linked immunosorbent assay (ELISA), antigen-capture detection, serum neutralization, reversetranscriptase polymerase chain reaction (RT-PCR)assay, electron microscopy and virus isolation bycell culture5. Since, samples are potential biohazardrisks, diagnosis should be performed under high-est-level of biosafety containment conditions.
2987
Ebola and blood transfusion: existing challenges and emerging opportunities
-
2988
Ebola virus Infection Treatment andManagement
As there are currently no licensed vaccines ortherapeutics to prevent or treat any filovirus in-fection, particularly Ebola30, it has emerged as apotential global public health threat34. Prior EVDoutbreaks have been controlled by implementa-tion of integrated strategies like identification ofcases, contact tracing, quarantine, early diagno-sis, supportive care, infection control, and safeburial practices. Fortunately, the negative impactof current 2014 epidemic illustrate the impor-tance of effective novel preventive and curativearsenal35 to fight against the Ebola. Though todate no approved therapeutic agents exist to treator prevent Ebola, the following therapeutic op-tions have been administered to curb Ebola-asso-ciated illness and death (Table I).
Importance of Blood Transfusion toTreat EVD cases
Due to the absence of effective vaccine and re-liable drugs to neutralize the Ebola virus, thetreatment or management of Ebola patients have
been mainly focused on symptomatic treatmentswith available antiviral agents and blood transfu-sion17. Besides, early supportive care with rehy-dration and electrolyte correction, monitoring ba-sic physiological functions, protein deficiencies,has often been administered to improve the sur-vival of Ebola patients5.
In 1995, eight Ebola patients were transfusedwith convalescent whole blood (CWB) and plas-ma (CP) of EVD survivors to treat illness in theDRC. Donated blood contained only IgG EBO an-tibodies and no antigen. However, antigens weredetected in all the recipients just prior to the trans-fusion and this empirical study found that amongthe eight only one patient (12.5%) died. The per-cent of the mortality rate is significantly lowerthan other EBO epidemic in Congo and rest of theworld45. The reason for the lower- mortality rateremains to be scientifically authenticated and war-ranted by further clinical studies to evaluate andelucidate the passive immune therapy.
In addition, currently several blood transfusionstudies are underway by enrolling patients of2014 epidemic and the preliminary results are
S. Abdullah, K. Karunamoorthi
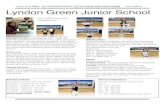
Figure 3. Ebola virus transmission cycle (Source: CDC 2014)10.
-
2989
Ebola and blood transfusion: existing challenges and emerging opportunities
Nam
eofthe
S.No.
therapeuticagent
Nature
Modeofaction
Rem
arks
Reference
(s)
1.AV
I60
02(A
VI-75
37)
Dru
gB
lock
ing
vira
lpro
tein
Ithe
lpsm
onke
ysto
surv
ive
from
Ebo
laA
xtel
leet
al.2
0123
6
forso
me
sixt
y-to
-eig
hty
perc
ent.
Itha
ssh
own
hum
anto
lera
bilit
yin
early
stud
ies.
2.H
yper
imm
une
glob
ulin
Prep
ared
bypu
rify
ing
and
Neu
tral
izin
gan
tibod
yPr
otec
tive
inm
onke
ys,b
utar
eno
tcur
rent
lyK
udoy
arov
a-co
ncen
trat
ing
plas
ma
ofag
ains
tEbo
lavi
rus
avai
labl
ean
dw
ould
notb
eex
pect
edbe
fore
Zub
avic
hene
etal
.im
mun
ized
anim
alsor
prev
ious
lym
idof
2015
1999
17;M
aron
infe
cted
hum
answ
ithhi
ghtit
ers.
2014
37
3.K
Z52
Ane
utra
lizin
ghu
man
Itpr
otec
tsgu
inea
pigs
KZ52
isa
prom
isin
gca
ndid
ate
for
Parren
etal
.200
238
mon
oclo
nala
ntib
ody
from
leth
alEbo
laZai
reim
mun
opro
phyl
axis
ofEbo
lavi
rusin
fect
ion
viru
sch
alle
nge
4.Fa
vipi
vavi
rA
ntiv
iral
drug
appr
oved
Blo
cksth
ere
plic
atio
nof
Nee
dto
beus
edat
muc
hhi
gher
dose
s.Tho
ugh
Furu
taet
al.2
0093
9 ,(T
-705
orAvi
gan)
forin
flue
nza
inJa
pan
man
yR
NA
viru
ses,
the
effici
ency
ofth
isdr
ugag
ains
thum
anEbo
la20
1340
partic
ular
lyit
inhi
bits
the
infe
ctio
nre
mai
nsun
clea
r,so
me
positiv
eR
NA
-dep
ende
ntR
NA
resu
ltsar
eem
ergi
ngin
anim
alex
perim
ents
poly
mer
ase
(RdR
P)of
influe
nza
5.In
terfer
ons
Targ
etin
gan
ddi
sabl
ing
Tho
ugh
they
did
noti
ncre
ase
over
alls
urvi
val,
Bas
leran
dth
eV
P24
prot
ein
butd
elay
the
deat
h.N
ever
thel
ess,
itre
mai
nsA
mar
asin
ghe
2009
41
uncl
earw
hich
inte
rfer
onto
use,
whe
nan
dat
wha
tdos
age
regi
men
toob
tain
optim
alre
sults
.6.
Bio
Cry
stD
rug
Itne
edsm
ore
anim
altrea
tmen
tdat
abe
fore
itco
uld
beco
nsid
ered
.7.
ZM
app
(am
ixtu
reof
Und
erde
velo
pmen
tas
Lik
ein
trav
enou
sIt
was
firs
tuse
dex
perim
enta
llyto
trea
tsom
eQ
iuet
al.2
0134
2 ;th
ree
antib
odie
s)a
trea
tmen
tfor
Ebo
laim
mun
oglo
bulin
ther
apy,
peop
lew
ithEbo
lavi
rusdi
seas
edu
ring
the
WH
O20
14g,
h43,
44
viru
sdi
seas
eZM
app
cont
ains
2014
Wes
tAfric
anEbo
laou
tbre
ak,b
utas
neut
raliz
ing
antib
odie
sof
Aug
ust2
014
itha
dno
tyet
been
tested
inth
atpr
ovid
epa
ssiv
ea
clin
ical
tria
lto
supp
ortw
ides
prea
dus
age
imm
unity
toth
evi
rusby
inhu
man
s;it
isno
tkno
wn
whe
ther
itis
dire
ctly
and
spec
ific
ally
effe
ctiv
eto
trea
tthe
dise
ase,
norif
itis
safe
reac
ting
with
itin
a"l
ock
and
key"
fash
ion.
TableII.E
xist
ing
ther
apeu
ticop
tions
totrea
tEbo
lavi
rusdi
seas
e.
-
2990
quite promising and encouraging too46-48. The un-precedented attack of Ebola on world communityhas created a high demand of blood transfusionthan ever before2. It remains to be considered asthe best option to treat Ebola virus disease in theabsence of effective therapeutic agents.
Accordingly, during the ongoing 2014 EVDoutbreak, whole blood and plasma obtained fromEbola recovered patients have been prioritizedfor reconnaissance, as one of the empirical treat-ment modalities49 for the patients with early EVDclinical symptoms and manifestations. As conva-lescent plasma has been successfully adminis-tered to treat various infectious diseases, thismodality is biologically plausible50 and could beefficacious too. In addition, by reviewing all theexisting experimental potential therapies and vac-cines, the WHO experts indicate that treatingEbola patients with blood transfusions from sur-vivors of EVD is the top most priority17 to savehundreds of thousands of lives.
Ebola and Blood TransfusionsMode of Mechanism
Since the survivors of Ebola infection typicallyproduce effective antibodies against the virus, thetransfusions of their blood into a newly Ebola in-fected individual could save life17. As none of theexisting/considered Ebola regimes have been ade-quately tested in humans, the convalescent whole-blood (CWB) and serum could serve as therapeu-tic agents against Ebola virus. Indeed, it has to betransfused safely with careful screening17, or elsemismatched blood type and infected blood couldcause a few severe reactions that may be life-threatening too. Therefore, both WHO and publichealth experts debated on the pros and cons oftreating Ebola patients with transfusions of wholeblood and plasma of EBVD survivors51.
In the past, CWB modality has been adoptedempirically among a small group of patients,with promising results45. However, the use ofCWB is technically more complex and demandsmore facilities and skills. Consequently the even-tual use of CP in Guinea, Sierra Leone and theDemocratic Republic of Congo will depend onthe availability of technical expertise51. Finally,WHO (2014)49 has issued an interim guidance tonational health authorities and blood transfusionservices to outline the steps required to collectCWB or CP from EVD recovered patients fortransfusion to patients with early EVD, as an em-pirical treatment modality. It includes the follow-ing phases:
Key phases for the BloodTransfusion Identification
The EVD recovered patients (those have beendischarged from the recognized Ebola treatmentcenters or units) could serve as potential donors(after 28 days of discharge) for CWB/CP. It is im-portant to note that the Ebola neutralizing antibod-ies are expected to be most effective whenCWB/CP is sourced from the epidemic/endemicareas of active Ebola virus (EBOV) transmission.However, in circumstances where the demand ishigh and the system is challenged by an over-whelming number of active EVD patients, andCWB/CP could also be sourced from the placeslinked to the current EVD outbreak in West Africawhere the outbreak has come under control49.
Screening/Pre-Donation Tests(WH O 2014)49• Estimation of donors hemoglobin concentration• ABO (A, B, AB and O) grouping and RhD
type screening tests for blood borne infectiousdiseases like human immunodeficiencyvirus (HIV), hepatitis B virus (HBV), hepatitisC virus (HCV), syphilis co-infections andother locally transmitted infections like malar-ia, as applicable
• Titration of total Ebola neutralizing antibodiesto identify the potential donor, particularly ifthe donor is willing to continue serving asCWB/CP source.
Review of Pre-Donation TestsIt is one of the critical phases in empirical
blood transfusion treatment. Results of the pre-donation tests must be carefully reviewed.Donors, those are shown negative for all TTItests and fulfilling the remaining all other criteriashould be chosen for CWD/CP donations. If theduration between predonation test and donationexceeds forty-eight h, then the routine TTI testsmust be repeated49. A minimum period of twelveand sixteen weeks for males and females, respec-tively is needed for further blood donation.
Selection of EVD Patients and BloodSample Collection
Only EVD confirmed patients in the earlystages should be selected for CWB/CP transfu-sion49. Two venous blood samples (5 mL) eachmust be drawned from the patient prior to trans-fusion; (a) one in EDTA for a plasma, while (b)another one in a plain tube (without anticoagu-lant) for a serum sample for the (a) ABO and
S. Abdullah, K. Karunamoorthi
-
RhD blood grouping, and cross-matching and,(b) baseline viral load assay. Plain sample is usedto measure the viral-load and other tests. Further-more, prior to discharge of recovered patients,two additional five mL plain samples have to becollected to analyze the viral-load in the succes-sive days. Residual serum of the blood samplesshould be stored in aliquots for retrospective an-tibody or any other future examinations49.
Selection of Convalescent Whole Bloodor Plasma Units
ABO and RhD matched blood or plasma unitsneed to be chosen for transfusion. RhD-ve unitsshould be transfused to RhD-ve women of child-bearing age (if possible). However, If the RhDgroup of the patient is not known or in case ofnon-availability of RhD specific group, bloodmatched only for ABO group may be used fortreatment49:
• In order to minimize the risk associated withhandling of infectious blood samples, crossmatching of patients’ serum and donors’ redcells, can be omitted if ABO group compatibleCWB/CP is selected.
• If it is not possible to test the patient’s ABOgroup or if ABO matched CWB/CP is notavailable then: (1) for whole blood transfusion- group O convalescent whole blood, ideallyfrom donors with low titer anti-A and anti-B,can be transfused; while (2) for plasma trans-fusion - group AB convalescent plasma sepa-rated by centrifugation should be used.
• Non ABO-matched CP could also be consid-ered if group AB plasma is not available, butshould preferably be group A or B.
• Transfusion needs to be done within twenty-four hours of CP preparation in order to obtainhigher RBC concentration.
Transfusion of Convalescent WholeBlood or Plasma
CWB/CP units should be transfused to theEVD patients by following the clinical transfu-sion protocols. One unit of CWB [equals is 450mL (just under a pint)] have to be transfused foradult patients. In the absence of evidence, 400-500 mL of CP in two doses of 200-250 mL each,separated from two different WB donations,should be considered for adult patients, andwhereas, in the case of pediatric CWB/CP trans-fusion, a dose of 10 mL/kg could be ideal basedon the considerations of blood volume49.
Patient MonitoringTransfused EVD patients must be closely
monitored in order to assess the patient improve-ment in terms of clinical conditions and the con-comitant decline of virus load detected inplasma18, as well as to evaluate the effectivenessof the treatment. In addition to clinical monitor-ing, Ebola antibody levels and other tests are alsoextremely important. Besides, standard case re-porting forms must also be maintained to moni-tor all potential interventions for EVD49, 52.
However, a few public health experts haveraised their concern regarding adopting bloodtransfusion as a therapeutic modality for the Ebo-la treatment: (1) the emergence of a black markettrading of blood of EVD survivors2, (2) risk ofescalating transmission of several infectious dis-eases, particularly killer diseases like human im-munodeficiency virus (HIV), malaria and viralhepatitis infection and, (3) other infectious dis-eases46, 53. Nevertheless, blood transfusion is oneof the easily adoptable empirical therapeuticmodalities with the potential to be implementedimmediately on a large scale to address the cur-rent epidemic54. If healthcare providers strictlyadopt the WHO standard protocol called ‘Interimguidance to national health authorities and bloodtransfusion services,’ it shall be one of the safestas well as suitable therapeutic modalities to savelives.
Though there is as yet no licensed treatmentproven to neutralize the virus but a wide-range ofblood, immunological and drug therapies are un-der development. At the moment, two potentialEbola candidate vaccines are undergoing for clin-ical and immunological evaluation55. One experi-mental drug viz., ZMapp was administered tosome of the patients (including two US aid work-ers) and a few of them died. Therefore, there isno substantial evidence to prove that the ZMapphas saved the lives of Ebola patients or had no ef-fect17.
Existing Major Challenges and EmergingOpportunities
The potentialities of Ebola fighting antibodiesare not identical and it may trigger a few adverseside-effects and negative sequelae17. The edict,from some two-hundred public health expertsand WHO scientists, was a follow-up to an earli-er Ebola ethics review on October 2014 and con-cluded that blood transfusion would be ethical totransfuse patients experimental therapies whenand if they are easily obtainable17: (1) possible to
2991
Ebola and blood transfusion: existing challenges and emerging opportunities
-
2992
recruit large number of potential donors, (2) col-lection and, (3) screening of any infectious dis-eases to potentially save Ebola patients.
Necessity of Adequate HealthcareProfessionals and Facilities
A strong health system immensely minimize acountry’s vulnerability to potential health risks interms of disease outbreaks and catastrophes witha high-level of preparedness to mitigate any pub-lic health crises. Subsequently, it ensures qualityhealthcare for their citizens56. However, if healthsystems are ill-equipped to deal with outbreaksand natural disasters, the populations can be verymuch vulnerable to several infections ultimatelydeath57. The Ebola hit West African countries likeGuinea, Sierra Leone and Liberia have very frag-ile health systems, lacking human and infrastruc-tural resources to deal with the outbreaks sincethey have recently emerged from decades of civilwar and insurgencies2. The 2014 Ebola outbreakhighlights how an epidemic can proliferate rapid-ly and pose huge problems in the absence of astrong health system56.
When the recent Ebola outbreak erupted, thecapacity of health systems in Guinea, Liberia andSierra Leone was limited56. Essential health-sys-tem functions were not performing well and thishampered the development of timely response tothe outbreak. Besides, there were inadequatequalified health professionals58 as well as infra-structure, logistics, health information, surveil-lance, governance and also, the drug supplychains were feeble56.
Sharing Knowledge and Resources:a Key to Saving Lives
In the Ebola-hit countries, all the febrile in-dividuals need to be screened for Ebola andeven if they are found to be negative, they stillneed to be treated for Ebola. Besides, normalroutine services like paediatric, antenatal, safedelivery and postnatal services should be as-sured while dealing with the direct and indirecteffects of epidemic. Otherwise breakdown ofgeneral health services may slay more peoplethan the epidemic56. In the remote rural areasthe health system is virtually nonexistent or if itdoes, it often runs down a clinic with shortageof essential life-saving medicines and thesecountries must improve with their nationalhealthcare sectors immediately.
Since these third world countries lack re-sources and funds to implement effective inter-
vention strategies, appropriate long-lastingworkable strategy has to be framed by bringingall potential stakeholders. It is extremely im-portant to fight against the ‘common enemy’,the so called ‘Ebola’. It must include variousnon-governmental organizations, civil societyand international organizations to incentivizethe national health systems, both to mitigate thedirect consequences of the outbreak and ensureall essential health services being delivered56. Itcould pave the way to combat with the Ebolarelated illness, deaths as well as to minimizethe avoidable deaths due to various other infec-tious diseases56. Besides, international donors,and agencies must assist them to bolster theirhealth system to develop stronger disaster pre-paredness for the future outbreaks.
Maximum Use of Supportive Therapy(MUST)
The purpose of the MUST is to save the lives.It includes intravenous (IV) drips to substitutethe excessive fluid loss due to diarrhea and vom-iting. Balancing of electrolytes such as calciumor potassium could prevent kidney and heart fail-ure. Furthermore, nasogastric tubes for feedingand as well as diagnosis and treatment of sec-ondary infections like malaria could be useful tominimize the Ebola related illness and deaths. Inaddition, MUST might reveal side-effects of newdrugs that would otherwise be masked by Ebolasymptoms, and it could reduce the rate of com-plications that might be incorrectly blamed on adrug59.
Integrative ApproachesIndeed interagency policies for outbreak de-
tection and rapid response is extremely impor-tant. Besides, understanding the cultural and tra-ditional risk factors within and between nationscould be useful to develop appropriate communi-cation strategies to generate awareness amongpeople. In addition, the regional coordination andcollaboration, particularly with governments andhealth ministries throughout Africa27 could pavethe way to minimize Ebola related illness anddeaths. Pandey et al60 urged the effective integra-tive approaches like case isolation, contact-trac-ing with quarantine, and sanitary funeral prac-tices must be strictly implemented in order tocontain the Ebola outbreak. It has been reportedthat the actual number of Ebola infection under-reported as much as seventy-five percent are dueto several factors and it has torn the society in the
S. Abdullah, K. Karunamoorthi
-
poverty stricken countries. This has to be ad-dressed immediately unless otherwise a single in-fected individual is enough to create Ebola out-break.
Formulation of Effective ChemotherapyThough currently we have a few anti-viral
drugs to treat several viral illnesses, there is noapproved specific therapeutics to treat filovirusinfections. It is a matter of deep and grave con-cern and pressing need to develop both preven-tive and curative antiviral agents against filovirusinfection6. The experimental Ebola drug called‘ZMapp’ has been administered to a limited num-ber of Ebola victims and the results are quitepromising. Notably the drug (ZMapp) has provedas a potent antiviral agent in monkeys. However,further clinical trials are yet to be conducted todemonstrate its safety and efficacy in human27.The WHO expert panel has considered the out-look for another seven potential Ebola drugs, butnone of them has been proved of effectivenessagainst Ebola in humans.
Ebola Vaccine Development andClinical Trials
The unprecedented 2014 EVD epidemic hasprompted an international response to acceleratethe availability of a preventive vaccine. Two vac-cine candidates viz., chimpanzee adenovirusserotype 3 (ChAD3-ZEBOV) and recombinantvesicular stomatitis virus (rVSV-ZEBOV) arecurrently being tested in humans. Both vaccineshave shown to be safe and efficacious in animals.Further Phase 1 results are expected to emergeduring December 2014 to January 201555.
• Phase I clinical trials of the cAd3-ZEBOVvaccine in healthy adults are nearing comple-tion in the United Kingdom, United States,Mali and Switzerland, whereas, the rVSV-ZE-BOV vaccine, trials are well advanced or nearcompletion in Canada, the United States,Gabon, Germany, and Switzerland. Trials inKenya are begin September 2014.
• Phase II clinical trials of the cdA3-ZEBOVwill test the safety and potential to induce animmune response in larger numbers and inbroader populations, particularly among chil-dren. These trials are expected to begin inCameroon, Ghana, Mali, Nigeria and Senegalin early 2015.
• Phase III clinical trials are planned to start inthe first quarter of 2015 in Guinea, Liberia and
Sierra Leone to assess the extent to which thevaccines protect against EVD and to gauge thefeasibility of full deployment.
Besides, two other vaccines – one developedby Johnson and Johnson and the other by No-vavax – are in due to enter clinical trials in thevery near future55.
Cost-free Ebola VaccinationWHO Director-General (Dr Margaret Chan)
has indicated that developing Ebola vaccine isnot a profit-driven industry, as the victims arepoorest people to procure vaccine. At least in thehumanity ground the international stake holdersand concerned authorities must initiate to devel-op low-cost potential vaccine and all people mustbe vaccinated at least in the Ebola-prone Africancountries. However, with the available existingresources we can substantially contain the Ebolaoutbreaks by generating awareness and creatingsupportive community.
Conclusions
Indeed, EVD remains one of the most dreadfulinfectious diseases and the recent 2014 outbreakis the most devastating in terms of fatality rate inrecorded Ebola history. At the moment, there isno effective curative agents to fight against ourcommon enemy. WHO scientists and a group ofkey public health experts endorse the bloodtransfusion as an empirical modality by consider-ing various existing therapeutic options to con-tain this deadliest outbreak. Nevertheless, it isone of the challenging tasks to implement in theresource-limited settings of tropical sub-SaharanAfrica. Therefore, the following interventionsmust be adopted to address the existing majorchallenges effectively and immediately: (1) pin-pointing the virus’s source, (2) early case detec-tion, (3) quarantine the infected people, (4) track-ing and treating the Ebola patients, (5) providingsupportive care, (6) free supply of personal pro-tective equipment (PPE) in Ebola epicenters, (7)development and application of simple diagnos-tic tools and potent therapeutic interventions, (8)identifying and understanding the emerging viralstrains through gene sequencing, (9) building astrong global health infrastructure/network, (10)generating the awareness through print and E-media (11) patients who died of Ebola should becremated or buried promptly in a hermetically
2993
Ebola and blood transfusion: existing challenges and emerging opportunities
-
2994
sealed casket and, (12) community engagementsthrough social mobilization.
Besides, presently several clinical trials are un-derway to assess the potentialities of various an-ti-viral agents and vaccines against EBOV andthe preliminary results are quite encouraging.Until acquiring reliable therapeutic agents, wecan adopt blood transfusion as therapeuticmodality by strictly following the WHO standardprotocol in order to avoid any undesirable ef-fects. Furthermore, strong regional, national andinternational multilayered collaborations bybringing all the stakeholders is extremely impor-tant to address the existing challenges to build aEbola-free healthiest society in the near future.
––––––––––––––––––––AcknowledgementsThe authors would like to acknowledge Ms. L. Melita forher sincere assistance in editing the manuscript. Our last butnot least heartfelt thanks go to our colleagues from the De-partment of Environmental Health, Faculty of Public Healthand Tropical Medicine, Jazan University, Kingdom of SaudiArabia, for their kind support and cooperation.
–––––––––––––––––-––––Conflict of InterestThe Authors declare that there are no conflicts of interest.
References
1) RUZEK B. EDITED BY SUNIT K. Singh, Daniel. Viral he-morrhagic fevers. Boca Raton: CRC Press, Taylor& Francis Group, 2014; p. 444.
2) WHO. Ebola virus disease. Fact sheet N°103. Up-dated September 2014. Available at:http://www.who.int/mediacentre/factsheets/fs103/en/ [accessed on 30th November 2014].
3) TEAM ROAWIS. Ebola haemorrhagic fever in Su-dan, 1976. Bull World Health Organ 1978; 56:247.
4) HEYMANN D, WEISFELD J, WEBB P, JOHNSON K, CAIRNS T,BERQUIST H. Ebola hemorrhagic fever: Tandala, Zaire,1977-1978. J Infect Dis 1980; 142: 372-376.
5) WHO. Ebola response roadmap situation re-port-17 December 2014. World Health organiza-t ion. 17 December 2014b. Avai lable at:http://apps.who.int/iris/bitstream/10665/136020/1/roadmapsitrep_8Oct2014_eng.pdf?ua=1. [ac-cessed October 29, 2014].
6) JOHANSEN LM, BRANNAN JM, DELOS SE, SHOEMAKERCJ, STOSSEL A, LEAR C, HOFFSTROM BG, DEWALD LE,SCHORNBERG KL, SCULLY C, LEHÁR J, HENSLEY LE,WHITE JM, OLINGER GG. FDA-approved selectiveestrogen receptor modulators inhibit Ebola virusinfection. Sci Transl Med 2013; 5: 190ra79.
7) BRAY M. Viral Hemorrhagic Fever (Crimean-Con-go, Ebola, Lassa, Marburg, Rift Valley, and YellowFever). 2014. Available at: http://www.antimi-crobe.org/v39.asp (accessed on 15th December2014).
8) MAHANTY S, BRAY M. Pathogenesis of filoviralhaemorrhagic fevers. Lancet Infect Dis 2004; 4:487-498.
9) GEISBERT WT, HENSLEY LE. Ebola virus: New insightsinto disease aetiopathology and possible thera-peutic interventions. Expert Rev Mol Med 2004; 6:1-24.
10) CDC (Centers for Disease Control and Preven-tion): Ebola Transmission. November 2014. Avail-able at: http://www.cdc.gov/vhf/ebola/transmis-sion/ (accessed on 2nd December 2014).
11) ZAMPIERI CA, SULLIVAN NJ, NABEL GJ. Immunopathol-ogy of highly virulent pathogens: insights fromEbola virus. Nat Immunol 2007; 8: 1159-1164.
12) WILSON JA, BOSIO CM, HART MK. Ebola virus: Thesearch for vaccines and treatments. Cell Mol LifeSci 2001; 58: 1826–1841.
13) WATERMAN T. Brief General History of Ebola. 1999.Available at:https://web.stanford.edu/group/virus/filo/history.html (accessed on 15th December 2014).
14) WHO. Ebola Situation Report. 7th January 2015.Available at: http://www.who.int/csr/disease/ebo-la/situation-reports/en/ (accessed on 14th Janu-ary 2015).
15) TEAM WHOER: Ebola Virus Disease in West Africa- The First 9 Months of the Epidemic and ForwardProjections. N Engl J Med 2014; 371: 1481-1495
16) WHO. Ebola Response Roadmap SituationRepor t 25 October 2014. Ava i lable athttp://apps.who.int/iris/bitstream/10665/137185/1/roadmapupdate25Oct14_eng.pdf [accessed on30th November 2014].
17) MARON DF. Patient Zero Believed to Be Sole Sourceof Ebola Outbreak. August 28, 2014. Available at:|http://www.scientificamerican.com/article/patient-ze-ro-believed-to-be-sole-source-of-ebola-outbreak/(accessed on 11th December 2014).
18) LYON GM, MEHTA AK, VARKEY JB, BRANTLY K, PLYLERL, MCELROY AK, KRAFT CS, TOWNER JS, SPIROPOULOUC, STRÖHER U, UYEKI TM, RIBNER BS. Emory Seri-ous Communicable Diseases Unit: Clinical careof two patients with Ebola virus disease in theUnited States. N Engl J Med 2014; 371: 2402-2409.
19) WHO. Ground zero in Guinea: the outbreaksmoulders – undetected – for more than 3months. Available at: http://www.who.int/csr/dis-ease/ebola/ebola-6-months/guinea/en/ (Retrievedon 27th December 2014).
20) BAIZE S, PANNETIER D, OESTEREICH L, RIEGER T,KOIVOGUI L, MAGASSOUBA N, SOROPOGUI B, SOW MS,KEÏTA S, DE CLERCK H, TIFFANY A, DOMINGUEZ G, LOUAM, TRAORÉ A, KOLIÉ M, MALANO ER, HELEZE E, BOC-QUIN A, MÉLY S, RAOUL H, CARO V, CADAR D, GABRIELM, PAHLMANN M, TAPPE D, SCHMIDT-CHANASIT J, IM-
S. Abdullah, K. Karunamoorthi
-
POUMA B, DIALLO AK, FORMENTY P, VAN HERP M, GÜN-THER S. Emergence of Zaire Ebola virus disease inGuinea-preliminary report. N Engl J Med 2014;371: 1418-1425.
21) DIXON MG, SCHAFER IJ. Ebola Viral Disease Out-break-West Africa 2014. MMWR Morb Mortal Wk-ly Rep 2014; 63: 548-551.
22) UNICEF. Ebola and its devastating impact on chil-dren. 2014. Available at: http://blogs.unicef.org/2014/10/01/ebola-and-its-devastating-impact-on-children/ (Retrieved on 27th December 2014).
23) WHO. WHO Ebola R&D Effort - Vaccines, Thera-pies, Diagnostics. 18 December 2014. Availableat: http://www.who.int/medicines/ebola-treat-ment/ebola_r_d_effort/en/ (accessed on 23rd De-cember 2014).
24) WORLD HEALTH ORGANIZATION. Why the Ebola out-break has been underestimated. World Health Or-ganization, Geneva, Switzerland. 2014. Availableat www.who.int/mediacentre/news/ebola/22-au-gust-2014/en.
25) LEROY EM, BAIZE S, VOLCHKOV VE, FISHER-HOCH SP,GEORGES -COURBOT MC, LANSOUD-SOUKATE J ,CAPRON M, DEBRÉ P, MCCORMICK JB, GEORGES AJ.Human asymptomatic Ebola infect ion andstrong inflammatory response. Lancet 2000;355: 2210-2215.
26) BIELLO D. Ebola Exacerbates West Africa’s Pover-ty Crisis. October 30, 2014. Available at:http://www.scientificamerican.com/article/ebola-exacerbates-west-africa-s-poverty-crisis/ (ac-cessed on 23rd December 2014).
27) ALEXANDER KA, SANDERSON CE, MARATHE M, LEWIS BL,RIVERS CM, SHAMAN JM, DRAKE JM, LOFGREN E, DATOVM, EISENBERG MC, EUBANK S. What Factors MightHave Led to the Emergence of Ebola in WestAfrica? PLOS Neglected Tropical Diseases.Available at: http://blogs.plos.org/speakingofmedi-cine/files/2014/11/Alexanderetal.pdf (accessed on25th February 2015).
28) BAUSCH DG, TOWNER JS, DOWELL SF, KADUCU F, LUK-WIYA M, SANCHEZ A, NICHOL ST, KSIAZEK TG, ROLLINPE. Assessment of the risk of Ebola virus trans-mission from bodily fluids and fomites. J Infect Dis2007; 196: S142-S147.
29) GEISBERT TW, HENSLEY LE, JAHRLING PB, LARSEN T,GEISBERT JB, PARAGAS J, YOUNG HA, FREDEKING TM,ROTE WE, VLASUK GP. Treatment of Ebola virus in-fection with a recombinant inhibitor of factorVIIa/tissue factor: a study in rhesus monkeys.Lancet 2003; 362: 1953-1958.
30) WEINGARTL HM, EMBURY-HYATT C, NFON C, LEUNG A,SMITH G, KOBINGER G. Transmission of Ebola virusfrom pigs to non-human primates. Sci Rep 2012;2: 811.
31) FELDMANN H, GEISBERT TW. Ebola hemorrhagicfever. The Lancet 2011; 377: 849-862.
32) WEBMD: Visual Guide to Ebola. 06th October2014. Available at: http://www.webmd.com/a-to-z-guides/ss/slideshow-visual-guide-to-ebola (ac-cessed on 2nd December 2014).
33) FELDMANN HS, JONES H, KLENK D, SCHNITTLER HJ.Ebola virus: From discovery to vaccine. Nat RevImmunol 2003; 3: 677-685.
34) MACNEIL A, ROLLIN PE. Ebola and Marburg hemor-rhagic fevers: Neglected tropical diseases? PLoSNegl Trop Dis 2012; 6: e1546.
35) LEDGERWOOD JE, DEZURE AD, STANLEY DA, NOVIK L,ENAMA ME, BERKOWITZ NM, HU Z, JOSHI G, PLOQUIN A,SITAR S, GORDON IJ, PLUMMER SA, HOLMAN LA, HENDELCS, YAMSHCHIKOV G, ROMAN F, NICOSIA A, COLLOCA S,CORTESE R, BAILER RT, SCHWARTZ RM, ROEDERER M, MAS-COLA JR, KOUP RA, SULLIVAN NJ, GRAHAM BS; THE VRC207 STUDY TEAM. Chimpanzee Adenovirus VectorEbola Vaccine - Preliminary Report. Available at:http://www.nejm.org/doi/pdf/10.1056/NEJMoa1410863 (accessed on 25th February 2015).
36) AXTELLE HA, THIMMARAYAPPA TJ, SMITH W. A phase 1,single ascending-dose study of AVI-6002, a com-bination of two PMOplusTM compounds with ac-tivity against ebolavirus. Clin Microbiol Infect2012; 18: 3221.
37) KUDOYAROVA-ZUBAVICHENE NM, SERGEYEV NN, CHEP-URNOV AA, NETESOV SV. Preparation and use of hy-perimmune serum for prophylaxis and therapy ofEbola virus infections. J Infect Dis 1999; 179:S218-223.
38) PARREN PW, GEISBERT TW, MARUYAMA T, JAHRLING PB,BURTON DR. Pre- and postexposure prophylaxis ofEbola virus infection in an animal model by pas-sive transfer of a neutralizing human antibody. JVirol 2002; 76: 6408-6412.
39) FURUTA Y, GOWEN BB, TAKAHASHI K, SHIRAKI K, SMEEDF, BARNARD DL. Favipiravir (T-705), a novel viralRNA polymerase inhibitor. Antiviral Res 2013;100: 446-454.
40) FURUTA Y, TAKAHASHI K, SHIRAKI K, SAKAMOTO K, SMEEDF, BARNARD DL, GOWEN BB, JULANDER JG, MORREYJD. T-705 (favipiravir) and related compounds:Novel broad-spectrum inhibitors of RNA viral in-fections. Antiviral Res 2009; 82: 95-102.
41) BASLER CF, AMARASINGHE GK. Evasion of interferonresponses by Ebola and Marburg viruses. J Inter-feron Cytokine Res 2009; 29: 511-520.
42) QIU XG, WONG L, FERNANDO J, AUDET A, BELLO J,STRONG JB, ALIMONTI GP. Kobinger, mAbs and ad-vectored IFN-a therapy rescue Ebola-infectednonhuman primates when administered after thedetection of viremia and symptoms. Sci TranslMed 2013; 5: 207ra143.
43) WEBMD. WHO Experts Give Nod to Using Untest-ed Ebola Drugs. Available at:http://www.webmd.com/news/20140812/who-ex-perts-give-nod-to-using-untested-ebola-drugs Au-gust 12, 2014. (Accessed on 25th December2014).
44) WHO.WHO Ethical considerations for use of unreg-istered interventions for Ebola virus disease. WorldHealth Organization. Retrieved 8 October 2014.
45) MUPAPA K, MASSAMBA M, KIBADI K, KUVULA K, BWAKAA, KIPASA M, COLEBUNDERS R, MUYEMBE-TAMFUM JJ.Treatment of Ebola hemorrhagic fever with blood
2995
Ebola and blood transfusion: existing challenges and emerging opportunities
-
2996
transfusions from convalescent patients. Interna-tional Scientific and Technical Committee. J InfectDis 1999; 179: S18-23.
46) MORIN M. WHO to issue guidelines on treatingEbola with blood, plasma therapy. Available at:http://www.latimes.com/science/sciencenow/la-sci-sn-ebola-blood-20140926-story.html[cited 27September 2014].
47) News24nigeria. Doctor gives blood for Ebola-in fec ted Dal las nurse. Ava i lable from:http://www.news24.com.ng/World/News/Doctor-gives-blood-for-Ebola-infected-Dallas-nurse-20141014-2[cited 14 October 2014].
48) ROBERTS M. Ebola serum for Africa patients with-in weeks says WHO. Avai lable from:http://www.bbc.com/news/health-29707393[cited21 September 2014].
49) WHO. Use of Convalescent Whole Blood orPlasma Collected from Patients Recovered fromEbola Virus Disease for Transfusion, as an Em-pirical Treatment during Outbreaks. InterimGuidance for National Health Authorities andBlood Transfusion Services. Version 1.0 Sep-tember 2014, World Health Organization, Gene-va, Switzerland.
50) LUKE TC, CASADEVALL A, WATOWICH SJ, HOFFMAN SL,BEIGEL JH, BURGESS TH. Hark back: Passive im-munotherapy for influenza and other serious in-fections. Crit Care Med 2010; 38: e66-73.
51) WHO. Global Alert and Response (GAR): What this– the largest Ebola outbreak in history – tells theworld. 2014. Available at: http://www.who.int/csr/dis-ease/ebola/ebola-6-months/lessons/en/ (accessedon 24th December 2014).
52) WORLD HEALTH ORGANIZATION. Ebola virus disease:Cuban medical team heading for Sierra Leone.2014. Available at: http://www.who.int/csr/dis-ease/ebola/en/. (Accessed on 15th January 2015).
53) WORLD HEALTH ORGANIZATION. Experimental thera-pies: growing interest in the use of whole bloodor plasma from recovered Ebola patients (con-valescent therapies). 2014. Avai lable at:http://www.who.int/mediacentre/news/ebola/26-september-2014/en/[cited 26 September 2014].
54) BUTLER D. Blood transfusion named as prioritytreatment for Ebola. Available from: http://www.na-ture.com/news/bloodtransfusion-named-as-priority-treatment-for-ebola-1.15854 [cited 5 Sep-tember 2014].
55) WHO. Meeting summary of the WHO consultationon potential Ebola therapies and vaccines. WHO,Geneva, Switzerland. 4–5 September 2014. Avail-able at:http://apps.who.int/iris/bitstream/10665/136103/1/WHO_EVD_Meet_EMP_14.1_eng.pdf (accessedon 1st January 2015).
56) KIENY M, EVANS DB, SCHMETS G, KADANDALE S.Health-system resilience: reflections on the Ebolacrisis in western Africa. Bull World Health Organ2014; 92: 850.
57) WHO. Strengthening health-system emergencypreparedness: toolkit for assessing health-systemcapacity for crisis management. Copenhagen:World Health Organization; 2012. Available at:http://www.euro.who.int/__data/assets/pdf_file/0008/157886/e96187.pdf [cited 2014 Nov 3].
58) GLOBAL HEALTH OBSERVATORY. World Health Organi-zation; Geneva: 2014. Available from:http://www.who.int/gho/en/ [cited 2014 Nov 3].
59) COHEN J, KUPFERSCHMIDT K. A dose of reality. Sci-ence 2014; 346: 908-911.
60) PANDEY A, KATHERINE EA, JAN M, NATASHA W, JEFFREYPT, JAMES EC, TOLBERT GN, MARTIAL LN, ALISON PG.Ebola epidemiology Strategies for containingEbola in West Africa. Science 2014; 346: 991-996.
S. Abdullah, K. Karunamoorthi