PHARMACOKINETICS OF RECOMBINANT HUMAN ERYTHROPOIETIN IN PATIENTS ON CONTINUOUS AMBULATORY PERITONEAL...
3
425 RESULTS 33 of the 36 patients completed the course of treatment and follow-up. For the 3 patients who defaulted, information from general practitioners indicated that their symptoms had improved (no further consultations or therapy requested for irritable bowel symptoms), but they were excluded from the analysis. 20 patients reported an improvement in their symptoms, and 13 found no benefit. Of those who felt better, 11 were virtually symptom-free by the end of the study. Factors which might have affected the response rate are shown in the table. There was no significant difference in the response rate between men and women, hypnotherapists, or patients treated in groups or individually. Patients with a GHQ score of 5 or more (suggesting psychological illness) were less likely to improve with hypnotherapy. Patients who became symptom-free tended to have had less severe symptoms but, for an individual patient, the severity of symptoms at the start of treatment was a poor indicator of outcome. There was little tendency for symptoms to recur between the end of formal treatment at 7 weeks, and the follow-up visit 3 months later (see figure); the patients who did best improved without further formal treatment, although they continued with the autohypnosis. DISCUSSION The mechanisms by which hypnotherapy improves symptoms of the irritable bowel syndrome remain unclear. A placebo effect alone is unlikely, because few patients who improved on hypnotherapy suffered a relapse after formal treatment ended at 7 weeks; many patients continued to improve after the end of formal treatment. There was no disproportionate improvement in the feeling of wellbeing of patients who improved, and most of the patients who became nearly symptom-free had no initial tension or anxiety, as judged by GHQ scores. This suggests that the treatment is not just producing a psychological effect. The effects of hypnotherapy in this group of patients with irritable bowel syndrome were less striking than those reported by Whorwell and colleagues.6’ Nevertheless, the results were encouraging because all 33 had been refractory to conventional medical treatment. Patients treated by group hypnotherapy showed as great an improvement in symptoms as those treated individually. One therapist can treat up to 8 patients in a single session, therefore group hypnotherapy should be cost-effective. Correspondence should be addressed to R. F. H., Gastroenterology Unit, Frenchay Hospital, Bristol BS16 1LE. REFERENCES 1. Thompson WG, Heaton KW Functional bowel disorders in apparently healthy people Gastroenterology 1980; 79: 283-88. 2. Drossman DA, Sandler RS, McKee DC, Lovitz AJ. Bowel dysfunction among subjects not seeking health care. Gastroenterology 1982; 83: 529-34. 3. Switz DM. What the gastroenterologist does all day. Gastroenterology 1976; 70: 1048-50. 4 Harvey RF, Salih SY, Read AE. Organic and functional disorders in 2000 gastroenterology outpatients. Lancet 1983; i: 632-34 5. Harvey RF, Mauad EC, Brown AM. Prognosis in the irritable bowel syndrome. a 5-year prospective study. Lancet 1987; i 963-65. 6 Whorwell PJ, Prior A, Faragher EB Controlled trial of hypnotherapy in the treatment of severe refractory irritable-bowel syndrome Lancet 1984; ii: 1232-34. 7. Whorwell PJ, Prior A, Colgan SM. Hypnotherapy in severe irritable bowel syndrome: further experience. Gut 1987, 28: 423-25 8. Manning AP, Thompson WG, Heaton KW, Morris AF. Towards positive diagnosis of the irritable bowel. Br Med J 1978; ii: 653-54. 9 Goldberg DP. The detection of psychiatric illness by questionnaire. Maudsley Monograph, no 21. London. Oxford University Press, 1972 Therapeutics PHARMACOKINETICS OF RECOMBINANT HUMAN ERYTHROPOIETIN IN PATIENTS ON CONTINUOUS AMBULATORY PERITONEAL DIALYSIS IAIN C. MACDOUGALL1 PETER NEUBERT3 GERALD A. COLES1 DAVID E. ROBERTS2 A. DOUGLAS DHARMASENA1 JOHN D. WILLIAMS1 KR UF Institute of Renal Disease, Royal Infirmary, Cardiff CF2 1SZ;1 Department of Pharmacy, University Hospital of Wales, Cardiff;2 College of Medicine, and Boehringer Mannheim GmbH, Mannheim, West Germany3 Summary To determine the optimum regimen for giving recombinant human erythropoietin (EPO) to patients on continuous ambulatory peritoneal dialysis (CAPD), the pharmacokinetics of single-dose EPO administered intravenously (120 U/kg), intraperitoneally (50 000 U), and subcutaneously (120 U/kg) was investigated. After intravenous administration serum EPO levels decayed exponentially from a peak of 3959 mU/ml, with a half-life of 8·2 h. 2·3% of the total intravenous dose was lost in the dialysate during the first 24 h. Peak serum EPO levels of 375 mU/ml at 12 h and 176 mU/ml at 18 h were attained following intraperitoneal and subcutaneous administration, respectively. The bioavailability of subcutaneous EPO (21·5%) was seven times greater than that of intraperitoneal EPO (2·9%). These results suggest that subcutaneous EPO represents the most satisfactory route of administration for CAPD patients. INTRODUCTION RECOMBINANT human erythropoietin (EPO) is now established as an effective therapeutic agent for anaemia in patients undergoing chronic haemodialysis,l but there is a lack of reports on its efficacy in CAPD patients, and the optimum dose and route of administration of EPO have yet to be determined.2 Chronic intravenous administration is impractical since ready vascular access is not available in CAPD patients. In rabbits EPO is well absorbed from the peritoneal cavity. To assess whether intraperitoneal administration might be suitable for patients on CAPD, we have studied the single-dose pharmacokinetics of EPO given intravenously (IV), intraperitoneally (IP), and subcutaneously (SC) to a group of stable CAPD patients. PATIENTS AND METHODS The subjects were 8 patients on CAPD-4 males, 4 females- whose mean age was 62 (SD 10) years, whose mean weight was 67 (SD 13) kg, and whose median duration on CAPD was 17 (range 7-70) months. All were well at the time of the study and none had had any episodes of peritonitis within the previous 6 months. Baseline serum levels of EPO ranged from 18-46 mU/ml, except in 1 patient with polycystic kidney disease who had a concentration of 236 mU/ml. Each patient received EPO (Boehringer Mannheim GmbH) on three occasions separated by at least 4 weeks. The doses received were: IV 120 U/kg (mean dose per patient = 8043 U), IP 50 000 U, and SC 120 U/kg. Blood samples for measurement of serum EPO were taken at regular intervals over the first 24 h following IV and IP administration, and up to 96 h following SC administration.
Transcript of PHARMACOKINETICS OF RECOMBINANT HUMAN ERYTHROPOIETIN IN PATIENTS ON CONTINUOUS AMBULATORY PERITONEAL...

425
RESULTS
33 of the 36 patients completed the course of treatmentand follow-up. For the 3 patients who defaulted,information from general practitioners indicated that theirsymptoms had improved (no further consultations or
therapy requested for irritable bowel symptoms), but theywere excluded from the analysis.
20 patients reported an improvement in their symptoms,and 13 found no benefit. Of those who felt better, 11 werevirtually symptom-free by the end of the study. Factorswhich might have affected the response rate are shown in thetable. There was no significant difference in the responserate between men and women, hypnotherapists, or patientstreated in groups or individually. Patients with a GHQ scoreof 5 or more (suggesting psychological illness) were lesslikely to improve with hypnotherapy. Patients who becamesymptom-free tended to have had less severe symptoms but,for an individual patient, the severity of symptoms at thestart of treatment was a poor indicator of outcome.There was little tendency for symptoms to recur between
the end of formal treatment at 7 weeks, and the follow-upvisit 3 months later (see figure); the patients who did bestimproved without further formal treatment, although theycontinued with the autohypnosis.
DISCUSSION
The mechanisms by which hypnotherapy improvessymptoms of the irritable bowel syndrome remain unclear.A placebo effect alone is unlikely, because few patients whoimproved on hypnotherapy suffered a relapse after formaltreatment ended at 7 weeks; many patients continued toimprove after the end of formal treatment. There was nodisproportionate improvement in the feeling of wellbeing ofpatients who improved, and most of the patients whobecame nearly symptom-free had no initial tension or
anxiety, as judged by GHQ scores. This suggests that thetreatment is not just producing a psychological effect.The effects of hypnotherapy in this group of patients with
irritable bowel syndrome were less striking than thosereported by Whorwell and colleagues.6’ Nevertheless, theresults were encouraging because all 33 had been refractoryto conventional medical treatment. Patients treated bygroup hypnotherapy showed as great an improvement insymptoms as those treated individually. One therapist cantreat up to 8 patients in a single session, therefore grouphypnotherapy should be cost-effective.
Correspondence should be addressed to R. F. H., Gastroenterology Unit,Frenchay Hospital, Bristol BS16 1LE.
REFERENCES
1. Thompson WG, Heaton KW Functional bowel disorders in apparently healthypeople Gastroenterology 1980; 79: 283-88.
2. Drossman DA, Sandler RS, McKee DC, Lovitz AJ. Bowel dysfunction amongsubjects not seeking health care. Gastroenterology 1982; 83: 529-34.
3. Switz DM. What the gastroenterologist does all day. Gastroenterology 1976; 70:1048-50.
4 Harvey RF, Salih SY, Read AE. Organic and functional disorders in 2000
gastroenterology outpatients. Lancet 1983; i: 632-345. Harvey RF, Mauad EC, Brown AM. Prognosis in the irritable bowel syndrome. a
5-year prospective study. Lancet 1987; i 963-65.6 Whorwell PJ, Prior A, Faragher EB Controlled trial of hypnotherapy in the treatment
of severe refractory irritable-bowel syndrome Lancet 1984; ii: 1232-34.7. Whorwell PJ, Prior A, Colgan SM. Hypnotherapy in severe irritable bowel syndrome:
further experience. Gut 1987, 28: 423-258. Manning AP, Thompson WG, Heaton KW, Morris AF. Towards positive diagnosis
of the irritable bowel. Br Med J 1978; ii: 653-54.9 Goldberg DP. The detection of psychiatric illness by questionnaire. Maudsley
Monograph, no 21. London. Oxford University Press, 1972
Therapeutics
PHARMACOKINETICS OF RECOMBINANTHUMAN ERYTHROPOIETIN IN PATIENTS ONCONTINUOUS AMBULATORY PERITONEAL
DIALYSIS
IAIN C. MACDOUGALL1PETER NEUBERT3GERALD A. COLES1
DAVID E. ROBERTS2A. DOUGLAS DHARMASENA1
JOHN D. WILLIAMS1
KR UF Institute of Renal Disease, Royal Infirmary,Cardiff CF2 1SZ;1 Department of Pharmacy, University Hospitalof Wales, Cardiff;2 College of Medicine, and Boehringer Mannheim
GmbH, Mannheim, West Germany3
Summary To determine the optimum regimen forgiving recombinant human erythropoietin
(EPO) to patients on continuous ambulatory peritonealdialysis (CAPD), the pharmacokinetics of single-dose EPOadministered intravenously (120 U/kg), intraperitoneally(50 000 U), and subcutaneously (120 U/kg) was
investigated. After intravenous administration serum EPOlevels decayed exponentially from a peak of 3959 mU/ml,with a half-life of 8·2 h. 2·3% of the total intravenous dosewas lost in the dialysate during the first 24 h. Peak serumEPO levels of 375 mU/ml at 12 h and 176 mU/ml at 18 hwere attained following intraperitoneal and subcutaneousadministration, respectively. The bioavailability ofsubcutaneous EPO (21·5%) was seven times greater thanthat of intraperitoneal EPO (2·9%). These results suggestthat subcutaneous EPO represents the most satisfactoryroute of administration for CAPD patients.
INTRODUCTION
RECOMBINANT human erythropoietin (EPO) is nowestablished as an effective therapeutic agent for anaemia inpatients undergoing chronic haemodialysis,l but there is alack of reports on its efficacy in CAPD patients, and theoptimum dose and route of administration of EPO have yetto be determined.2 Chronic intravenous administration is
impractical since ready vascular access is not available inCAPD patients. In rabbits EPO is well absorbed from theperitoneal cavity. To assess whether intraperitonealadministration might be suitable for patients on CAPD, wehave studied the single-dose pharmacokinetics of EPOgiven intravenously (IV), intraperitoneally (IP), and
subcutaneously (SC) to a group of stable CAPD patients.
PATIENTS AND METHODS
The subjects were 8 patients on CAPD-4 males, 4 females-whose mean age was 62 (SD 10) years, whose mean weight was 67(SD 13) kg, and whose median duration on CAPD was 17 (range7-70) months. All were well at the time of the study and none hadhad any episodes of peritonitis within the previous 6 months.
Baseline serum levels of EPO ranged from 18-46 mU/ml, exceptin 1 patient with polycystic kidney disease who had a concentrationof 236 mU/ml.Each patient received EPO (Boehringer Mannheim GmbH) on
three occasions separated by at least 4 weeks. The doses receivedwere: IV 120 U/kg (mean dose per patient = 8043 U), IP 50 000 U,and SC 120 U/kg. Blood samples for measurement of serum EPOwere taken at regular intervals over the first 24 h following IV andIP administration, and up to 96 h following SC administration.
426
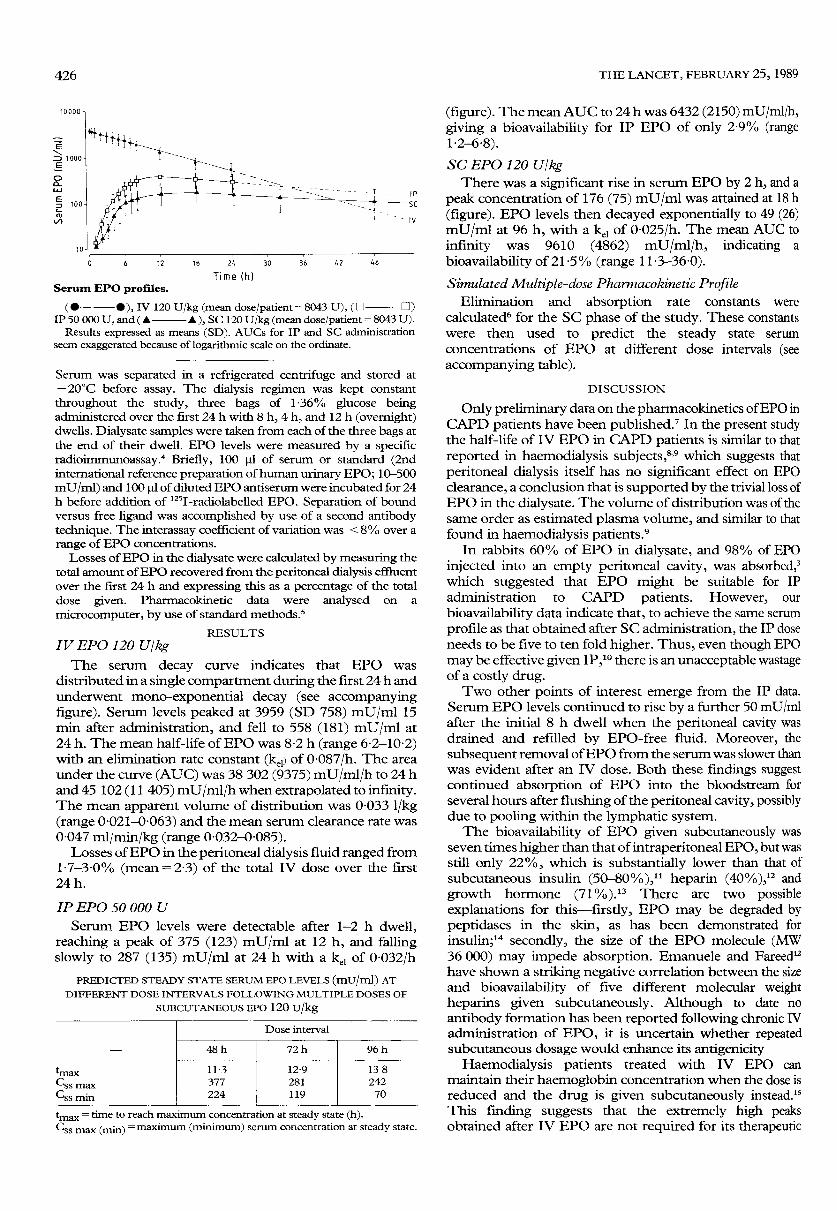
Serum EPO profiles.
(W————W), IV 120 U/kg (mean dose/patient = 8043 U), ( 0 0 )IP 50 000 U, and ( . . ), SC 120 U/kg (mean dose/patient = 8043 U).
Results expressed as means (SD). AUCs for IP and SC administrationseem exaggerated because of logarithmic scale on the ordinate.
Serum was separated in a refrigerated centrifuge and stored at- 20°C before assay. The dialysis regimen was kept constantthroughout the study, three bags of 1 36% glucose beingadministered over the first 24 h with 8 h, 4 h, and 12 h (overnight)dwells. Dialysate samples were taken from each of the three bags atthe end of their dwell. EPO levels were measured by a specificradioir=unoassay.1 Briefly, 100 )il of serum or standard (2ndinternational reference preparation of human urinary EPO; 10-500mU/ml) and 100 ul of diluted EPO antiserum were incubated for 24h before addition of 1251-radiolabelled EPO. Separation of boundversus free ligand was accomplished by use of a second antibodytechnique. The interassay coefficient of variation was < 8% over a
range of EPO concentrations.Losses of EPO in the dialysate were calculated by measuring the
total amount of EPO recovered from the peritoneal dialysis effluentover the first 24 h and expressing this as a percentage of the totaldose given. Pharmacokinetic data were analysed on a
microcomputer, by use of standard methods.5
RESULTSIV EPO 120 UjkgThe serum decay curve indicates that EPO was
distributed in a single compartment during the first 24 h andunderwent mono-exponential decay (see accompanyingfigure). Serum levels peaked at 3959 (SD 758) mU/ml 15min after administration, and fell to 558 (181) mU/ml at24 h. The mean half-life of EPO was 8-2 h (range 6-2-10-2)with an elimination rate constant (kel) of 0-087/h. The areaunder the curve (AUC) was 38 302 (9375) mU/ml/h to 24 hand 45 102 (11 405) mU/ml/h when extrapolated to infinity.The mean apparent volume of distribution was 0-033 1/kg(range 0-021-0-063) and the mean serum clearance rate was0-047 ml/min/kg (range 0-032-0-085).
Losses of EPO in the peritoneal dialysis fluid ranged from1-7-3-0% (mean=23) of the total IV dose over the first24 h.
IP EPO 50 000 U
Serum EPO levels were detectable after 1-2 h dwell,reaching a peak of 375 (123) mU/ml at 12 h, and fallingslowly to 287 (135) mU/ml at 24 h with a kel of 0-032/h
PREDICTED STEADY STATE SERUM EPO LEVELS (mU/ml) ATDIFFERENT DOSE INTERVALS FOLLOWING MULTIPLE DOSES OF
SUBCUTANEOUS EPO 120 U/kg
tmax = time to reach maximum concentration at steady state (h).Css max (min) = maximum (minimum) serum concentration at steady state.
(figure). The mean AUC to 24 h was 6432 (2150) mU/ml/h,giving a bioavailability for IP EPO of only 2-9% (range1-2-6-8).
SC EPO 120 U/kgThere was a significant rise in serum EPO by 2 h, and a
peak concentration of 176 (75) mU/ml was attained at 18 h(figure). EPO levels then decayed exponentially to 49 (26)mU/ml at 96 h, with a ke1 of 0-025/h. The mean AUC toinfinity was 9610 (4862) mU/ml/h, indicating a
bioavailability of 21-5% (range 11 -3-36-0).Simulated Multiple-dose Pharmacokinetic Profile
Elimination and absorption rate constants were
calculated6 for the SC phase of the study. These constantswere then used to predict the steady state serum
concentrations of EPO at different dose intervals (seeaccompanying table).
DISCUSSION
Only preliminary data on the pharmacokinetics of EPO inCAPD patients have been published? In the present studythe half-life of IV EPO in CAPD patients is similar to thatreported in haemodialysis subjects,8,9 which suggests thatperitoneal dialysis itself has no significant effect on EPOclearance, a conclusion that is supported by the trivial loss ofEPO in the dialysate. The volume of distribution was of thesame order as estimated plasma volume, and similar to thatfound in haemodialysis patients.9
In rabbits 60% of EPO in dialysate, and 98% of EPOinjected into an empty peritoneal cavity, was absorbed,3which suggested that EPO might be suitable for IPadministration to CAPD patients. However, our
bioavailability data indicate that, to achieve the same serumprofile as that obtained after SC administration, the IP doseneeds to be five to ten fold higher. Thus, even though EPOmay be effective given IP,10 there is an unacceptable wastageof a costly drug.Two other points of interest emerge from the IP data.
Serum EPO levels continued to rise by a further 50 mU/mlafter the initial 8 h dwell when the peritoneal cavity wasdrained and refilled by EPO-free fluid. Moreover, thesubsequent removal of EPO from the serum was slower thanwas evident after an IV dose. Both these fmdings suggestcontinued absorption of EPO into the bloodstream forseveral hours after flushing of the peritoneal cavity, possiblydue to pooling within the lymphatic system.The bioavailability of EPO given subcutaneously was
seven times higher than that of intraperitoneal EPO, but wasstill only 22%, which is substantially lower than that ofsubcutaneous insulin (50-80%),1’ heparin (40%),12 andgrowth hormone (71%).13 There are two possibleexplanations for this-firstly, EPO may be degraded bypeptidases in the skin, as has been demonstrated for
insulin;14 secondly, the size of the EPO molecule (MW36 000) may impede absorption. Emanuele and Fareed12have shown a striking negative correlation between the sizeand bioavailability of five different molecular weightheparins given subcutaneously. Although to date no
antibody formation has been reported following chronic IVadministration of EPO, it is uncertain whether repeatedsubcutaneous dosage would enhance its antigenicity
Haemodialysis patients treated with IV EPO can
maintain their haemoglobin concentration when the dose isreduced and the drug is given subcutaneously instead.’sThis finding suggests that the extremely high peaksobtained after IV EPO are not required for its therapeutic
427
efficacy. For this reason, and because EPO levels after SCadministration persist longer (3-4 days) than after IV
injection, it would seem reasonable to recommend the
subcutaneous route for treating CAPD and haemodialysispatients with EPO. Whether there would be a shortening ofhalf-life with repeated administration as described for
haemodialysis patients8 remains uncertain.Whilst the simulated multiple-dose pharmacokinetic
profile has its limitations, the data it yields suggest that asensible starting dose might be 60-120 U/kg subcutaneouslytwice a week. Subsequent doses would depend on thehaemoglobin response. The bioavailability of SC EPO,however, is still less than ideal, a feature likely to be related toits molecular size. If the active moiety of the EPO moleculeis assumed to be a fraction of its entire structure, perhaps asmaller molecule of similar efficacy but greaterbioavailability, could be synthesised.Correspondence should be addressed to 1. C. M.
We thank Dr Philip Routledge for advice and use of his computerprogramme, Mrs Susan Murphy for assistance with collection of samples,Miss Cheryl Patterson for secretarial help, and MCP Pharmaceuticals forfinancial support and supply of EPO.
REFERENCES
1 Winearls CG, Oliver DO, Pippard MJ, Reid C, Downing MR, Cotes PM Effect ofhuman erythropoietin derived from recombinant DNA on the anaemia of patientsmaintained by chronic haemodialysis. Lancet 1986; ii: 1175-78.
2. Boughton KJ, Abels RI, Rudnick SA. Subcutaneous erythropoietin Lancet 1988; ii:684.
3. Bargman J M, Breborowicz A, Rodela H, Abraham G, Oreopoulos DG. Absorption ofrecombinant human erythropoietin (EPO) from the peritoneal cavity in rabbits.Kidney Int 1988, 33: 243 (abstr).
4. Eckardt K-U, Kurtz A, Hirth P, Scigalla P, Wieczorek L, Bauer C Evaluation of thestability of human erythropoietin in samples for radioimmimoassay. KlinWochenschr 1988; 66: 241-45.
5. Ritschel WA, ed In: Handbook of basic pharmacokinetics, 3rd ed. Hamilton, Illinois:Drug Intelligence Publications Inc, 1986: 282-301, 462-94.
6. Ritschel WA, ed. Multiple dose pharmacokinetics. In: Handbook of basic
pharmacokinetics 3rd ed. Hamilton, Illinois: Drug Intelligence Publications Inc,1986 302-31
7. Boelaert J, Schurgers M, Matthys E, Daneels R, DeCre M, Bogaert M. Recombinanthuman erythropoietin pharmacokinetics in CAPD patients comparison of theintravenous, subcutaneous, and intraperitoneal routes. Nephrol Dial Transpl 1988;3: 493 (abstr).
8. Egrie JC, Eschbach JW, McGuire T, Adamson JW. Pharmacokinetics of recombinanthuman erythropoietin (rHuEPO) administered to hemodialysis (HD) patients.Kidney Int 1988; 33: 262 (abstr).
9. Wikstrom B, Salmonson T, Grahnen A, Danielson BG. Pharmacokinetics ofrecombinant human erythropoietin in haemodialysis patients. Nephrol DialTranspl 1988; 3: 503 (abstr).
10. Frenken LAM, Coppens PJW, Tiggeler RGWL, Koene RAP. Intraperitonealerythropoietin Lancet 1988; ii: 1495.
11. Galloway JA, Spradlin CT, Nelson RL, Wentworth SM, Davidson JA, Swarner JL.Factors influencing thr absorption, serum insulin concentration, and blood glucoseresponses after injections of regular insulin and various insulin mixtures. DiabetesCare 1981; 4: 366-76
12. Emanuele RM, Fareed J. The effect of molecular weight on the bioavailability ofheparin Thromb Res 1987, 48: 591-96.
13. Wilton P, Widlund L, Guilbaud O. Bioequivalence of Genotropin and Somatonorm.Acta Paediatr Scand 1987; 337 (suppl): 118-21.
14. Paulsen EP, Courtney JW, Duckworth WC. Insulin resistance caused by massivedegradation of subcutaneous insulin. Diabetes 1979; 28: 640-45.
15. Bommer J, Ritz E, Weinreich T, Bommer G, Ziegler T. Subcutaneous erythropoietin.Lancet 1988; ii: 406.
Environmental Health
INDOOR AIR POLLUTION IN DEVELOPINGCOUNTRIES AND ACUTE RESPIRATORY
INFECTION IN CHILDREN
M. R. PANDEY1K. R. SMITH3
J. S. M. BOLEIJ2E. M. WAFULA4
Tribhuvan University, Kathmandu, Nepal;1 AgriculturalUniversity, Wageningen, The Netherlands;2 East-West Centre,Honolulu, Hawaii, USA;3 and University of Nairobi, Kenya4
RESPIRATORY diseases are the main cause of morbidityand mortality in children in developing countries. Amongthese diseases, acute respiratory infections (ARI) are
responsible for nearly a third of all childhood deaths under 5years of age.1 Although immunisation and case-
management are partly effective in ARI, it seems clear thatlong-term solutions will depend on the control of riskfactors. Such control, for example, led to striking decreasesof moderate and severe ARI in the developed countries longbefore effective case-management became available.
Widespread case-management would be expensive and notan answer in the longterm since mild ARI can progressthrough moderate and severe phases to death, often in only2-3 days. In areas without carefully implemented case-management programmes, antibiotics, even if available, arelikely to be given too early, leading to drug resistance, or toolate.There are several important risk factors for ARI,
including poor nutrition, overcrowding, low birthweight,and personal hygiene. In developed countries, air pollutionhas also been identified as a factor, particularlyenvironmental tobacco smoke (ETS), for ARI in youngchildren.2,3 In many developing countries, in addition to anincreasing amount of tobacco smoke, many homes containhigh levels of smoke from the combusion of biofuels such aswood, crop residues, and animal dung for cooking or
heating. In about half the world’s households such fuels areused for cooking daily, usually without a flue or chimney andwith poor ventilation.4
INVESTIGATIONS
Results of investigations in six developing countries haveshown the range of indoor pollution in such circumstances(table). Although thousands of chemicals are found intobacco and biofuel smoke, the best single indicator forcomparison of toxic non-carcinogenic effects is probablyrespirable particulates, similar to tar reported for cigaretteemissions. Results of studies in animals suggest anydifference in respiratory-system toxicity according to massis not likely to be large.21As shown in the table, indoor particulate concentrations
in rural areas of developing countries, where ARI morbidityand mortality are highest, range from a few hundred to morethan 10 000 J.1g/m3, although different techniques andaveraging times were used in the studies reported. In someof the studies other pollutants were also measured, includingcarbon monoxide and benzo-apyrene (sometimes found inconcentrations well above those in public settings in
developed countries) as well as nitrogen, sulfur oxides, andformaldehyde (found in concentrations at roughly the upperlevels of those measured indoors in developing countries).By comparison, ETS levels are about 1 J.1g/m3 for eachcigarette smoked per day in households in developedcountries22-ie, about 40 J.1g/m3 in a household where twopacks are smoked per day. Peak indoor concentrationsduring the day are about three times higher than this value,and even higher levels may be reached for short periods inthe immediate vicinity of smokers. Thus, on the sparseevidence, peak and daily exposures to indoor particulatelevels in villages in developing countries would seem to besome twenty times greater than in developed countries.The results of a semi-quantitative epidemiological study
in Nepal showed a direct relation between reported hoursper day spent near the stove by infants and children aged