Pharmacogenetics of chronic pain management · 2016. 12. 3. · Chronic pain Pain management...
19
Review Pharmacogenetics of chronic pain management Bhushan M. Kapur a,b,c, ⁎, Prateek K. Lala b , Julie L.V. Shaw c a Department of Clinical Pathology, Sunnybrook Health Sciences Center, Toronto, Canada b Division of Clinical Pharmacology and Toxicology, The Hospital for Sick Children University of Toronto, Canada c Department of Laboratory Medicine and Pathobiology, Faculty of Medicine, University of Toronto, Canada abstract article info Article history: Received 8 March 2014 Received in revised form 25 May 2014 Accepted 27 May 2014 Available online 7 June 2014 Keywords: Chronic pain Pain management Pharmacokinetics Pharmacogenetics Opioids NSAIDs Triptans Objective: The experience of chronic pain is one of the commonest reasons individuals seek medical atten- tion, making the management of chronic pain a major issue in clinical practice. Drug metabolism and responses are affected by many factors, with genetic variations offering only a partial explanation of an individual’s response. There is a paucity of evidence for the benefits of pharmacogenetic testing in the context of pain management. Design and methods: We reviewed the literature between 2000 and 2013, and references cited therein, using various keywords related to pain management, pharmacology and pharmacogenetics. Results: Opioids continue to be the mainstay of chronic pain management. Several non-opioid based therapies, such as treatment with cannabinoids, gene therapy and epigenetic-based approaches are now available for these patients. Adjuvant therapies with antidepressants, benzodiazepines or anticonvulsants can also be useful in man- aging pain. Currently, laboratory monitoring of pain management patients, if performed, is largely through urine drug measurements. Conclusions: Drug half-life calculations can be used as functional markers of the cumulative effect of pharma- cogenetics and drug–drug interactions. Assessment of half-life and therapeutic effects may be more useful than ge- netic testing in preventing adverse drug reactions to pain medications, while ensuring effective analgesia. Definitive, mass spectrometry-based methods, capable of measuring parent drug and metabolite levels, are the most useful assays for this purpose. Urine drug measurements do not necessarily correlate with serum drug concentrations or therapeutic effects. Therefore, they are limited in their use in monitoring efficacy and toxicity. © 2014 The Authors. The Canadian Society of Clinical Chemists. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/). Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170 Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170 Chronic pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171 Pharmacogenetics and pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171 Cytochrome P450 enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171 P-glycoprotein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172 Cyclooxygenases 1 and 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172 Opioid receptor μ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172 Catechol-O-methyltransferase (COMT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173 Clinical use of pharmacogenetics in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173 Genetics and pain susceptibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173 Chronic pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174 Drugs used in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174 NSAIDs and acetaminophen in pain management (Table 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174 Opioids and pain management (Table 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174 Issues with opioids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175 Specific opioids used in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175 Clinical Biochemistry 47 (2014) 1169–1187 ⁎ Corresponding author at: Department of Clinical Pathology, Sunnybrook Health Science Centre, 2075 Bayview Ave, Toronto, Ontario, M4N 3M5, Canada. Fax: +1 905 849 4389. E-mail address: [email protected] (B.M. Kapur). http://dx.doi.org/10.1016/j.clinbiochem.2014.05.065 0009-9120/© 2014 The Authors. The Canadian Society of Clinical Chemists. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/). Contents lists available at ScienceDirect Clinical Biochemistry journal homepage: www.elsevier.com/locate/clinbiochem
Transcript of Pharmacogenetics of chronic pain management · 2016. 12. 3. · Chronic pain Pain management...

Clinical Biochemistry 47 (2014) 1169–1187
Contents lists available at ScienceDirect
Clinical Biochemistry
j ourna l homepage: www.e lsev ie r .com/ locate /c l inb iochem
Review
Pharmacogenetics of chronic pain management
Bhushan M. Kapur a,b,c,⁎, Prateek K. Lala b, Julie L.V. Shaw c
a Department of Clinical Pathology, Sunnybrook Health Sciences Center, Toronto, Canadab Division of Clinical Pharmacology and Toxicology, The Hospital for Sick Children University of Toronto, Canadac Department of Laboratory Medicine and Pathobiology, Faculty of Medicine, University of Toronto, Canada
⁎ Corresponding author at: Department of Clinical PathE-mail address: [email protected] (B.M. Kapur).
http://dx.doi.org/10.1016/j.clinbiochem.2014.05.0650009-9120/© 2014 The Authors. The Canadian Socie(http://creativecommons.org/licenses/by-nc-nd/3.0/).
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 8 March 2014Received in revised form 25 May 2014Accepted 27 May 2014Available online 7 June 2014Keywords:Chronic painPain managementPharmacokineticsPharmacogeneticsOpioidsNSAIDsTriptans
Objective: The experience of chronic pain is one of the commonest reasons individuals seek medical atten-tion, making the management of chronic pain a major issue in clinical practice. Drug metabolism and responsesare affectedbymany factors,with genetic variations offering only a partial explanation of an individual’s response.There is a paucity of evidence for the benefits of pharmacogenetic testing in the context of pain management.
Design andmethods:We reviewed the literature between2000 and 2013, and references cited therein, usingvarious keywords related to pain management, pharmacology and pharmacogenetics.
Results:Opioids continue to be themainstay of chronic painmanagement. Several non-opioid based therapies,such as treatment with cannabinoids, gene therapy and epigenetic-based approaches are now available for thesepatients. Adjuvant therapies with antidepressants, benzodiazepines or anticonvulsants can also be useful in man-aging pain. Currently, laboratory monitoring of pain management patients, if performed, is largely through urinedrug measurements.
Conclusions:Drug half-life calculations can be used as functional markers of the cumulative effect of pharma-cogenetics and drug–drug interactions. Assessment of half-life and therapeutic effectsmay bemore useful than ge-
netic testing in preventing adverse drug reactions to pain medications, while ensuring effective analgesia.Definitive, mass spectrometry-based methods, capable of measuring parent drug and metabolite levels, are themost useful assays for this purpose. Urine drug measurements do not necessarily correlate with serum drugconcentrations or therapeutic effects. Therefore, they are limited in their use in monitoring efficacy and toxicity.© 2014 The Authors. The Canadian Society of Clinical Chemists. Published by Elsevier Inc. This is an open accessarticle under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1170Chronic pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171Pharmacogenetics and pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171
Cytochrome P450 enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1171P-glycoprotein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172Cyclooxygenases 1 and 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172Opioid receptor μ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1172Catechol-O-methyltransferase (COMT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173Clinical use of pharmacogenetics in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173
Genetics and pain susceptibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1173Chronic pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174
Drugs used in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174NSAIDs and acetaminophen in pain management (Table 1) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174Opioids and pain management (Table 2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1174Issues with opioids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175Specific opioids used in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175
ology, Sunnybrook Health Science Centre, 2075 Bayview Ave, Toronto, Ontario, M4N 3M5, Canada. Fax: +1 905 849 4389.
ty of Clinical Chemists. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license

1170 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
Weak opioids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175Codeine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1175Hydrocodone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Tramadol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178
Strong opioids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Morphine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Hydromorphone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Fentanyl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Remifentanil . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Methadone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Buprenorphine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178Oxycodone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1179Oxymorphone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1179Meperidine (pethidine) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1180Levorphanol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1180
Other medications in the treatment of chronic pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1180Antidepressants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1180Anticonvulsants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1180Triptans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1181Benzodiazepines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182Cannabinoids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182Ziconotide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182
Novel therapies in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182Targeting epigenetic modifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1182Gene therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1183
Therapeutic drug monitoring in pain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1183Summary and conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1184References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1184
Introduction
According to the International Association for the Study of Pain(IASP), pain is defined as an “unpleasant sensory and emotional experi-ence associated with actual or potential tissue damage, or described interms of such damage”. Several different subtypes of pain can be de-scribed, based on their neuropsychological basis and duration, includingneuropathic, nociceptive, psychogenic, referred, phantom, acute andchronic [1]. Chronic pain is very common, with one in three Americansand one in five Canadians reported to suffer from this problem [2,3]. Itis one of the most frequent reasons for individuals to seek medicalcare. If untreated, chronic pain can lead to physical and social dysfunctionand diminished quality of life.
Successful pain management provides adequate analgesia withoutexcessive adverse effects. Current pain management strategies largelyemploy the use of the World Health Organization (WHO) pain ladder,beginning with non-opioid medications, such as NSAIDs, progressingto weak opioids, and culminating with strong opioids, particularly incancer pain [4]. The WHO also recommends adjuvant therapy with an-tidepressant medications to aid in reducing anxiety often associatedwith chronic pain [4].
Management of pain can be complicated by lack of adherence, thepotential for abuse or dependence on themedications used and adversedrug side effects. Many factors can influence drug disposition, includinggenetic variation, which can further complicate management of thesepatients.
Genetic studies have identified several loci in which polymorphicchanges can influence the pharmacodynamics and kinetics of analgesicdrugs. Current patientmonitoring in painmanagement (if performed atall) is largely based on urine drugmeasurements. However, therapeuticdrug monitoring (TDM) via plasma drug levels and half-life may provemore useful in monitoring patients prescribed pain medications toensure efficacy while minimizing adverse drug reactions. TDM canalso be very useful for the identification of drug-related side effectsand patient-reported lack of effect (e.g., tolerance).
Finally, non-opioid analgesics are often tried as options for manage-ment of pain, particularly in individuals where opioids are not a suitable
choice. In addition, novel therapies, including targeting of epigeneticchanges and gene therapy-based approaches are further broadeningfuture options for the treatment of chronic pain.
Methods
We conducted an online systematic search for papers and relatedabstracts published between 2000 and 2013 using the National Libraryof Medicine database, PubMed. Using the following headings: “painmanagement medications”, “pain management drugs”, “chronic painmanagement”, “pharmacogenetics and pain management”, and “drugmonitoring and pain management”, we identified 6670 papers. The ab-stracts of all papers were reviewed and those that appeared to be rele-vant to the subject were selected for further study. References citedtherein, including original publications, were also selected for furtherreview.
Pain
Pain is the most common presenting physical symptom in primarycare, accounting for an enormous burden of patient suffering, qualityof life, work and social disability, and health care and societal costs [5].Pain is defined as an unpleasant sensory and emotional experienceassociated with actual or potential tissue damage [1]. However, the ex-perience of pain is highly subjective and idiosyncratic, and individualsdevelop pain thresholds through experiences of injury or pathology inearly life [1].
Neuropathic pain results from actual damage to nerve fibers them-selves in the central or peripheral nervous system [6]. This damage canlead to nerve dysfunction, causing numbness, weakness and/or loss ofreflexes. Common descriptions accompanying neuropathic pain include“burning”, “shooting” or “shock-like” sensations [7]. The most commoncauses of chronic neuropathic pain include diabetic neuropathy, post-herpetic neuralgia, fibromyalgia, lower back pain (radiculopathy dueto disc herniation) and osteoarthritis [8].
Nociceptive pain is caused by stimulation of specialized sensoryneurons, called nociceptors, by noxious stimuli including extremes of

1171B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
temperature, or mechanical or chemical excitation. It is often catego-rized as somatic (derived from skin and deep tissue) or visceral(originating from internal organs). Due to high concentrations ofnociceptors in somatic tissues, chronic somatic pain is typically local-ized, and often results from degenerative or inflammatory processes.Nociceptive pain is frequently described as stabbing, pricking, burning,throbbing or cramping [9].
Psychogenic pain refers to painful sensations caused or amplified bymental or emotional factors with no evident physical tissue damage[10]. Referred pain is perceived at a site adjacent to or distant from thesite of painful stimulus; the mechanism for this process is not yet wellunderstood [11]. Phantom pain, a sub-type of referred pain, is the feelingof painful sensations from a part of the body which has been lost, andfrom which the brain no longer receives signals. Individuals who haveundergone limb amputation often experience phantom pain [12].
Acute and chronic are terms commonly used to describe the durationof painful sensations, but are difficult to categorically define. In general,acute pain resolves within weeks of the initial causative insult, whereaschronic pain is continuous, long-term pain which can last months oryears [13].
Chronic pain
The IASP defines chronic pain as that pain which persists past thenormal time of healing following an injury. However, since determiningthe end of the healing phase is problematic,most clinical definitions usea fixed time of persistent pain after initial onset. This demarcation be-tween acute and chronic pain is somewhat arbitrary, and typicallyranges from three months (e.g., for post-herpetic neuralgia) to sixmonths (e.g., for chronic lowbackpain) [14,15]. The treatment of chron-ic pain can be difficult because it is a complex condition influenced bygenetic makeup as well as physiological and psychological factors.
Chronic pain is a problem inmany societies,with prevalence rangingfrom 2% to 40% in the adult population, resulting in social and economicimpacts [16–18]. Chronic pain can interfere with an individual’s activi-ties of daily living, leading to work or school absenteeism, inability toparticipate in leisure activities, sleep disturbances and problems eating.In the United States, one in three Americans experiences chronic painand chronic pain is the most common reason for people to visit theirfamily doctor [3]; one in five Canadians is reported to suffer fromchronic pain [2]. It is therefore important that chronic pain be diagnosedaccurately and treated effectively. Recently, an increased focus on painmanagement has led to a six-fold increase in the sales of prescriptionopioids in the U.S. between1997 and 2006 [19]. Use of analgesics has in-creased from 7.2% of the U.S. population in 1988–1994 to 10.2% duringthe period 2007–2010 [20].
Pharmacogenetics and pain management
Pharmacogenetics refers to the way in which genetic differencesbetween individuals influence patient drug responses and drug disposi-tion [21]. Empirically, it is well understood that large inter-individualvariations exist with respect to the response to analgesics [22].Withconventional drug dosing, some patients will experience toxicitywhereas other patients will not receive adequate analgesia from thesame dose. Variations in drug efficacy can vary as much as 2- to 10-fold or even 100-fold among members of the same family [23–25].These differences can be due to pharmacodynamics factors, based onvariations in drug target receptors and downstream signal transduction,and pharmacokinetic factors, which affect drug metabolism and/orelimination, altering the relationship between drug dose and steadystate serum drug concentrations. Development of tolerance, whichmay occur through both dynamic and kinetic mechanisms, can alsoplay a significant role in this response variation.
Genetic variability is one factor playing a role in the way in whichdrugs affect physiology. Generally, genes affecting outcome of treatment
can be divided into two broad categories: those genes affecting pharma-cokinetics, and those affecting pharmacodynamics [22]. In the case ofpain management drugs, genes associated with altered pharmacokinet-ics include thosewhich encodemembers of the cytochrome P450 familyof enzymes, enzymes responsible for glucuronidation and drug trans-porter proteins [21,22]. Genes encoding cyclooxygenase enzymes, theopioid receptors and the enzyme catecholamine methyltransferase(COMT) can affect drug pharmacodynamics [21,22]. Světlík and col-leagues provide an up-to-date review of results from pharmacogeneticstudies of candidate genes in both the kinetic anddynamic domains [26].
Cytochrome P450 enzymes
The cytochrome P450 (CYP) enzymes comprise a category ofproteins whose biosynthesis is controlled by a large super-family ofgenes. Members of the CYP family play important roles in drug metab-olism and therefore influence the concentration of a drug present incirculation. The primary catalytic function of CYP enzymes is identifiedas the transfer of one oxygen atom frommolecular oxygen into varioussubstrates. Additionally, some CYP enzymes act as isomerases, reduc-tases, dehydrases, or nitric oxide (NO) synthases, and some can catalyseoxidative cleavage of esters [27].
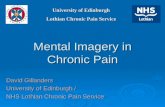
CYPs are responsible for approximately 80% of all phase I metabo-lism reactions (Fig. 1) [27,28]. Genetic changes in CYP genes can resultin alterations in enzyme activities. One CYP isoformwhich has been ex-tensively studied with respect to genetic variation is CYP2D6. This en-zyme accounts for a very small percentage (b2%) (Fig. 1b) of all CYPsexpressed in the human body, but is responsible for the metabolism ofalmost 20% of all drugs (Fig. 1a), includingmany drugs used inmanage-ment of pain [29]. Most of these enzymes are polymorphic [30]; morethan 80 CYP2D6 variants have been identified which, functionally, areassociated with four general phenotypes: extensive metabolizer (EM),intermediate metabolizer (IM), poor metabolizer (PM) and ultra-rapidmetabolizer (UM) [31]. The prevalence of these phenotypes varies byethnicity [22] and there are several examples in which phenotypic dif-ferences in individuals have led to adverse drug reactions.
In 2004, a case reported by Gasche and colleagues described a 62-year-old male, with a history of chronic lymphocytic leukemia, whopresented with fatigue, dyspnea, fever and cough with a bronchoalveo-lar lavage culture revealing yeast [33]. Hewas treated with codeine as acough suppressant. However on day4 of treatment, hedeteriorated rap-idly and became unresponsive. Hewas given naloxone, an opioid recep-tor antagonist, which resulted in rapid improvement in his condition.Several factorswere at play in this case, leading to the patient’s rapid de-terioration. Genetic studies revealed that he had CYP2D6 duplications,causing him to be an ultra-rapid metabolizer of the pro-drug (codeine)to the active metabolite (morphine). Furthermore, CYP3A4 is also in-volved in codeine metabolism, specifically in the conversion of codeineto (relatively inactive) norcodeine. In this case, co-treatment withclarithromycin and voriconazole, both CYP3A4 inhibitors, resulted indecreased conversion of codeine to norcodeine, shunting more codeineinto the CYP2D6 morphine pathway. The patient also developed acuterenal failure which resulted in the accumulation of glucuronide metab-olites with opioid activity (morphine-6-glucuronide) [33].
Opioids, including codeine, are among the pain medications metab-olized by CYP2D6. In 2006, Koren and colleagues reported a case of abreast-fed infant who died at 13 days of age [34]. The infant’s motherhad been prescribed codeine for episiotomy pain. Stored breastmilk was found to contain higher than expected levels of morphine(87 ng/mL; expected 1.9–20.5 ng/mL). CYP2D6 genotyping revealedthat the infant’s mother was heterozygous for a CYP2D6 duplication,making her an UM of codeine to morphine. The infant died from CNSdepression and this, along with the genetic results, were consistentwith opioid toxicity resulting from increased conversion of codeine tomorphine. This case prompted the FDA in the USA as well as Health

b) a)
Fig. 1. Cytochrome p450: Abundance and proportions. a) Proportions of drugs metabolized by CYP 450 enzymes. Adapted from: Rendic S and Di Carlo FJ [27]. b) CYP Abundance inhuman liver. Adapted from Yeo et al. [32].
1172 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
Canada to advise physicians against the prescription of codeine tonursing mothers [35,36].
Studies have also shown that CYP polymorphisms have an influenceon the metabolism of non-steroidal anti-inflammatory drugs (NSAIDs)and have the potential to cause adverse drug reactions, most notablygastrointestinal (GI) bleeding, a frequent reaction resulting insignificant patient morbidity and mortality. The risk of GI bleeding isparticularly high with higher doses of NSAIDs [37]. Many NSAIDs aremetabolized by CYP2C9, which has been shown to have two allelic var-iants, referred to as CYP2C9*2 and CYP2C9*3 [37]. The CYP2C9 enzymesencoded by the *2 and *3 alleles are reported to have 50% and 15% of theactivity of the wild-type enzyme, respectively, resulting in poor metab-olism, and thus prolonged action, of NSAIDs in individuals with either ofthese two alleles [38,39].
Due to their platelet-inhibiting action, NSAIDs are also responsiblefor an increased risk of bleeding, particularly in patients taking the anti-coagulant warfarin [38], since CYP2C9 is also important for warfarinmetabolism. Patients with the CYP2C9 *2 or *3 genotypes taking bothan NSAID and warfarin have been shown to have a significantly higherrisk for an elevated prothrombin time, compared to patients with thewild-type 2C9 genotype [38].
Celecoxib is a selective COX-2 inhibitor which is metabolized byCYP2C9. In a study of patients prescribed celecoxib for rheumatoid orosteoarthritis, patients with the *2 or *3 genotypes showed an increasedelimination half-life compared to patients with the wild-type genotype[40]. In a similar study, the investigators looked at patients prescribedone of several different NSAIDs, including celecoxib, ibuprofen andnaproxen. They grouped the patients into those who experienced GIbleeding and thosewho did not, and performed CYP 2C9 genotype anal-ysis on all patients. Within the group of patients with GI bleeding, ahigher number of individuals had the *2 or *3 genotype compared tothe group not experiencing gastrointestinal bleeding [41]. The increasedrisk of bleedingwas believed to result from reduced CYP2C9 enzyme ac-tivity in patients with the *2 or *3 alleles, leading to increased NSAIDconcentrations [41].
P-glycoprotein
The ABCB1/MDR1 gene encodes P-glycoprotein, an efflux transporterthat influences drug transport in several tissues, particularly theintestine, kidney and brain [42,43]. P-glycoprotein is highly expressedin endothelial cells of the brain vasculature, and is believed to effectthe efflux of drugs across the blood brain barrier [43]. ABCB1/MDR1 isa highly polymorphic gene, with 38 single nucleotide polymorphisms(SNPs) identified in the coding region [44]. The activity of P-glycoprotein is thought to be affected by genetic variability, with certainSNPs leading to decreased P-glycoprotein expression and activity.
One study, which examined individuals prescribed oxycodone,found that people homozygous or heterozygous for variant ABCB1/MDR1 alleles reported larger decreases in pain, but also a higherfrequency of adverse drug reactions to oxycodone, presumably due todecreased efflux and therefore higher plasma concentrations of thedrug [42]. Genetic variability of ABCB1/MDR1 has also been found tobe associated with inter-individual differences in pain relief achievedby morphine [43]. In a study of Korean patients receiving intravenousfentanyl, certain ABCB1/MDR1 genotypes were associated withprolonged fentanyl-induced suppression of respiration rate [45].
Cyclooxygenases 1 and 2
Cyclooxygenase 1 and 2 are encoded by two separate genes, PTGS1(COX1) and PTGS2 (COX2). Genetic variation in either of these enzymeswould be expected to cause altered pharmacodynamic responses toNSAIDs. In a study which investigated post-surgical expression ofPTGS1 and PTGS2, in relation to SNPs in each gene, certain SNPs wereshown to be associated with altered expression of the PTGS2 transcript[46]. The authors also reported differences in patient response to twoNSAIDs, rofecoxib, a selective COX-2 inhibitor and ibuprofen, a non-selective COX inhibitor. In particular, the G → C polymorphism at−765, in the promoter region of PTGS2, was found to be associatedwith lower PTGS2 expression in individuals heterozygous (G/C) or ho-mozygous (C/C) for the minor allele, compared to those homozygousfor the major allele (G/G) [46]. Subjects with G/G genotype alsoreported lower pain intensity with rofecoxib treatment for 48 h follow-ing surgery, compared to G/C or C/C subjects. This difference was notdemonstrated for patients treated with ibuprofen. However, subjectswith G/C and C/C genotypes reported decreased pain intensity with ibu-profen treatment at 48 h following surgery, compared to G/G patients.This difference was not seen in subjects treated with rofecoxib [46].These data suggest that patients with increased PTGS2 expression(G/G genotype) benefittedmore from treatmentwith rofecoxib, where-as patients with decreased PTGS2 expression (G/C or C/C genotypes)benefited more from treatment with ibuprofen [46]. These findingsare likely explained by the selectivity of rofecoxib for COX-2, encodedby PTGS2.
Opioid receptor μ
Opioid receptor μ is the primary site of action for many endogenousopioids, as well as those used for analgesia. A number of SNPs have beendescribed in OPRM1, the gene encoding this receptor. The most wellcharacterized SNP in OPRM1 is A118G. A study by Janicki et al. [47]found the minor allele (G) present at lower frequency in subjects withchronic pain treatedwith opioids, compared to a control group of opioid

1173B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
naïve patients, suggesting that the G allele may confer protectionagainst pain.
Epidural opioids are commonly used to provide analgesia to womenduring labor. Women heterozygous or homozygous for the OPRM1A118G allele have been demonstrated to have higher pressure painthresholds than women homozygous for the more common A allele[48]. The A → G nucleotide substitution leads to an amino acid changefrom asparagine to aspartic acid, and is thought to result in higher bind-ing affinity of β-endorphin to the opioid-μ receptor. In another study ofwomen in labor, themedian effective dose (ED50) of intrathecal fentanylrequired to achieve effective analgesia was significantly higher inwomen homozygous for the A allele (26.8 μg) compared to womenheterozygous or homozygous for the G allele (17.7 μg) [49].
Catechol-O-methyltransferase (COMT)
The COMT enzyme is responsible for the inactivation of catechol-amines such as dopamine, norepinephrine and epinephrine. Severalpolymorphisms have been identified in the COMT gene; however, themost widely studied variant is a G to A nucleotide substitution resultingin an amino acid change from valine to methionine at codon 158(Val158Met). This amino acid change is reported to decrease thethermal stability of the COMT protein, resulting in reduced enzymaticactivity. In studies of cancer patients experiencing chronic pain, patientshomozygous for the more common Val 158 were found to requirehigher doses of morphine to achieve analgesia, compared to patientsheterozygous or homozygous for Met 158 [50,51]. These findingssuggest that variable COMT activity may influence the effects of opioids.Animal studies have demonstrated reduced neuronal enkephalin con-tent in the brain with chronic activation of dopaminergic transmission.The reduced enkephalin content has been shown to be followed by anupregulation of the opioid-μ receptor [52,53]. The lower doses of mor-phine required by individuals with the Met158 variant may be ex-plained by reduced COMT activity which is associated with increaseddopaminergic stimulation, resulting in upregulation of opioid-μreceptor expression in the brain, making morphine more effective.Another study demonstrated differences in morphine side effects,such as drowsiness, confusion and hallucinations, associated withcertain COMT variants, which influenced how well patients toleratedmorphine [54].
Fig. 2. Genetic and non-genetic factors effecting dru
Clinical use of pharmacogenetics in pain management
Ideally, pharmacogenetic studies aim to aid in the selection anddosing of an optimal drug therapy for a specific patient. Choosing theoptimal therapy should lead to maximized therapeutic benefit,improved patient adherence and a reduction in adverse drug reac-tions [55]. The cases of opioid overdose discussed above illustrate in-stances where knowledge of patient genotypes may have been usefulto improve patient outcomes. However, most pharmacogenetic studiesto date have examined variability in single candidate genes, such asCYP2D6, and associated outcomes [22]. There are limitations to this ap-proach, as very few drugs aremetabolized by a single enzyme. Genome-wide association studies (GWAS) may possibly improve upon this limi-tation. Furthermore, in addition to genetics, many other factors affectdrug responses, such as patient age, disease co-morbidities and, inparticular, co-medication [22,56] (Fig. 2). Genetics can only partiallyexplain the variability in patient responses to analgesic drugs. Patientsare very commonly prescribed several medications for multipleco-morbidities. Some medications induce CYP enzyme activity [57], asillustrated in the case above [33], while others inhibit activity [57],which can lead to altered metabolism unrelated to the patient’s CYPphenotype. In general, pharmacogenetic studies thus far in pain man-agement have failed to yield evidence of improved clinical outcomes as-sociated with knowledge of patient genotypes when prescribing painmedications. As GWAS studies continue, and panels of gene testing be-come more widely accessible, pharmacogenetics of pain managementmay yet become more clinically useful [58].
Genetics and pain susceptibility
An individual’s genetic susceptibility to chronic pain is thought to becomplex, involving multiple genes, similar to the genetics of otherchronic diseases, such as diabetes [21]. As discussed above, several can-didate genes have been identified, with specific mutations shown toalter pain perception profiles between individuals. Examples include:OPRM1, the gene encoding the μ-opioid receptor; COMT, encodingcatechol-O-methyltransferase, involved in the metabolism of catechol-amines; GCH1, encoding an enzyme involved in phenylalaninemetabo-lismand the production of dopamine; themelanocortin-1 receptorwithmutations showing sex-specific differences in pain perception; and
g metabolism. Adapted from Stamer et al. [22].

1174 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
members of the cytochrome P450 enzyme family, important for thebiotransformation of many drugs. Genome-wide association studiesand other types of genetic investigations will likely identify manymore genes involved in pain perception.
Chronic pain management
Successful pain management can be viewed as providing adequateanalgesia without excessive adverse effects [59]. In 1982, Rane and col-leagues [60] proposed a pharmacological approach to treat cancer painwith morphine. They proposed a step-wise approach that was lateradopted by the World Health Organization (WHO) in 1986 [61,62]. Al-though this WHO stepladder approach was originally aimed at thetreatment of chronic cancer pain (Fig. 3) [61,62], it is also widely usedin the treatment of chronic non-cancer pain [63]. The WHO analgesicladder recommends initial treatment of pain with non-opioids, such asNSAIDs and acetaminophen. If pain persists, treatmentwith aweak opi-oid, such as codeine or tramadol is recommended, followed by a strongopioid, such as morphine, until the patient is free of pain. At each stageof the treatment ladder, adjuvant medications, such as antidepressantsor anticonvulsants, may also be given to aid in alleviating patient anxi-ety; some of these adjuvant drugs may also act directly to counterpain [4,61]. Evident from this scheme is the fact that opioids remainthemainstay of chronic painmanagement andwill be discussed furtherbelow.
Drugs used in pain management
NSAIDs and acetaminophen in pain management (Table 1)NSAIDs such as aspirin and ibuprofen, as well as acetaminophen, act
by inhibiting the enzymes cyclooxygenase-1 and -2, which catalyze thesynthesis of prostaglandins. The inhibition of prostaglandin synthesisresults in the analgesic, anti-pyretic and anti-inflammatory propertiesof these drugs, with the exception of acetaminophen, which does notshow anti-inflammatory affects. Due to the widespread use of NSAIDs,they are the drugs most commonly associated with adverse effects,the most common of which are those involving the GI tract. Reducedprostaglandin levels in the gastrointestinal mucosa decrease mucusand bicarbonate secretions, thereby reducing their protective effectsagainst the acidic gastric environment. In addition, NSAIDs can be di-rectly toxic to the gastric mucosa, leading to ulceration, and potentiallyfatal bleeding in the most extreme cases. Furthermore, reduced prosta-glandin synthesis in the kidney has been shown to cause renal impair-ment. Chronic or acutely toxic acetaminophen exposure can lead toliver toxicity through hepatocellular necrosis [64,65]. Additionally, aspi-rin (acetylsalicylic acid) is associated with Reye’s syndrome, primarilyaffecting children [66,67], and high doses of salicylates can cause
Fig. 3. TheWHO three-stepanalgesic ladder.Adapted from [60,61]. Legend: The pain lad-der shows a progressive rationale for stronger opioids. Before a new medication isintroduced, it is important to wait until the previously administered drug has reached a“steady state” or full effect is achieved. *Adjuvants: antidepressants, anticonvulsants,steroids.
metabolic acidosis and respiratory depression. More recently, cardio-vascular risks associated with the use of NSAIDs have gained attention.NSAIDs, particularly COX-2 selective agents, such as celecoxib, havebeen reported to increase the risk for thrombotic events, myocardial in-farction and stroke in patients with coronary artery disease and athero-sclerosis [68,69]. These findings have prompted the American HeartAssociation to recommend use of acetaminophen or non-acetylated sa-licylates for the treatment of chronic pain in patients with coronary ar-tery disease [70]. Although classified with nonsteroidal anti-inflammatory agents, acetaminophen has minimal peripheral anti-inflammatory activity.
IV acetaminophen has become a part of the multimodal analgesiaapproach for pain. Intravenous acetaminophen was made availableover 10 years ago in Europe, but in the United States only very recently.Three randomized placebo controlled trials provided the bases of its ap-proval. Clinical studies show that for management of pain, intravenousacetaminophen injection was at least as effective as morphine injectionin renal colic and oral ibuprofen after cesarean delivery. In children asingle-dose acetaminophen injection was similar to meperidineintramuscular (IM) for pain after tonsillectomy [71]. Effects begin 5 to10 min after IV administration, and peak effects occur in about 1 hwith an effective duration of 4 to 6 h. Table 1 provides pharmacokineticdetails of specific NSAIDs and acetaminophen, as used in painmanagement.
Opioids and pain management (Table 2)Opioids remain the most potent analgesics available and are the
mainstay of chronic pain management in both cancer patients and pa-tients with non-malignant pain [2,72]. To manage chronic cancer pain,oral morphine is commonly administered at regular intervals. Chronicdosing can lead to pharmacological tolerance, but not to therapeuticfailure. In simple pharmacological terms, opioid-induced tolerance canbe described as a “shift to the right” in the dose–response curve; thatis, a higher dose is required over time to maintain the same level of an-algesia. Differentmechanisms have been proposed for the developmentof tolerance. Säwe and colleagues [73] investigated themetabolic corre-late to the development of tolerance to therapeutic effects bymeasuringmorphine, morphine-3- and morphine-6-glucuronide in plasma andurine samples. They showed that the conjugation ofmorphinewith glu-curonic acid is proportional to the dose during long-term treatmentwith escalating doses, suggesting that this metabolic pathway is subjectto neither auto-induction nor saturation. Both in vitro and in vivo studieshave shown that, on the cellular level, chronic opioid treatment leads toa rapid reduction of agonist response, accompanied by internalizationof opioid receptors [74]. These early adaptive processes as well aslong-term adaptations, such as receptor downregulation, or counter-regulatory processes such as adenylate cyclase superactivation, havebeen suggested to be crucial to the development of opioid tolerance[75–77].
In recent years, there has been an increased focus on pain manage-ment which has resulted in a societal escalation in opioid use, with opi-oids being currently among themost commonly prescribedmedicationsin developed nations [78]. Despite this, the suitability of opioids forchronic non-cancer pain treatment is under debate. The efficacy ofopioids in this clinical situation has only been reported in short-termtrials, and evidence for their overall benefit in long-term therapy islacking [79].
The analgesic properties of opioids beginwith their binding to opioidreceptors in the central nervous system (CNS). There are three opioidreceptor subtypes, mu (μ), kappa (κ) and delta (δ), which differ intheir function and specificity for the drugs they bind. Opioids them-selves can be classified, based on their interactionswith these receptors,as agonists, mixed agonists–antagonists and antagonists. The binding ofopioids to their G-protein coupled receptors produces signals causinghyperpolarization of neuronal cell membranes and the suppression ofneurotransmitter release, resulting in analgesia [78,80,81].

Table 1Properties of NSAIDs and acetaminophen used in the management of chronic pain⁎.
Drug# Common route ofadministration
Protein binding Bioavailability# Route of elimination Vd
L/kgt½(h)
Acetylsalicylic acid(aspirin ®) [164]
Oral 99% 80%–100% Renal 0.1–0.2 2–3(low doses)
Ibuprofen [165] Oral 99% 49%–73% Renal 0.14 0.9–2.5
Indomethacin [166] Oral 98% ~100 %(oral),80% to 90% (rectal)
RenalFecal
0.4–1.2 5–10
Acetaminophen [167] Oral 20% ~100% Renal 0.25 1–4
Celecoxib [168] Oral 97% unknown Renal 5.7–7.0 11–16
# All chemical formulas and bioavailability are from their respective pages in Wikipedia.⁎ [169].
1175B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
Issues with opioidsThe increased use of opioids for pain management has led to an ex-
pansion in opioidmisuse, resulting in an increased number of emergen-cy room visits related to drug-seeking behavior aswell as in the numberof opioid-related overdose deaths [82,83]. Although opioids are amongthe most commonly used analgesics, their clinical use is limited by thedevelopment of tolerance and physical dependence. Another growingconcern relates to the diversion of opioids from patients to otherindividuals not under medical supervision.
Opioids have several well-known side effects, including nausea, seda-tion and bowel dysfunction [84]. Themost serious potential adverse effectis respiratory depression and failure, which is the most common cause ofdeath related to opioid use [80]. Prolonged use leads to tolerance,resulting in higher dose requirements, which can lead to physical depen-dence, demonstrated by withdrawal symptoms in patients experiencingchills, muscle aches, vomiting, diarrhea, hyperthermia, anxiety and hostil-ity [80]. Additionally, opioid use can result in feelings of euphoria whichcan promote compulsive use leading to psychological dependence.
A detailedmedical assessment is recommended prior to prescriptionof opioids. This should include a detailed medical history, review ofmedical records, urine toxicology screen and psychological evaluation,including questionnaires aimed at determining an individual’s risk forabuse [84,85]. This is of particular importance in those populations athigher risk for opioid misuse. Chronic pain frequently occurs in individ-uals with psychological conditions, including anxiety and depression; itis estimated that 30%–60% of individuals with depression also experi-ence chronic pain [86]. Psychological conditions are often comorbid inindividuals with substance-abuse disorders, resulting in a high riskfor opioid abuse in many chronic pain patients including those withsubstance abuse issues and mental health disorders [85].
Newer opioid formulations have been designed in efforts to preventabuse. These include Embeda™, an extended-release morphine co-formulated with the opioid antagonist naltrexone, produced by Pfizer;and an extended-release form of oxycodone, called OxyNeo™, byPurdue Pharma [84]. OxyNeo™ contains polyethylene oxide, whichforms a viscous gel when in contact with water, rendering it unsuitablefor injection or snorting, and also more difficult to chew or crush [87].Buprenorphine, a semi-synthetic opioid was approved by the FDAin 2002. Sublingual preparations, used in addiction medicine, areco-formulated with the antagonist naloxone to prevent abuse.
Specific opioids used in pain managementOpioids can be classified as either weak or strong, depending on their
“analgesic ceiling”. This term is defined as the dose above which a drughas no further effect on pain [88].Weakopioids include tramadol, codeineand hydrocodone; strong opioids include morphine, methadone,buprenorphine, fentanyl, oxycodone, hydromorphone, oxymorphone,meperidine and levorphanol. Detailed pharmacokinetic information foreach of these drugs can be found in Table 2.
Weak opioids
Codeine
Codeine is considered a weak opioid, and is used for its analgesic,anti-tussive and anti-diarrheal properties. It is a pro-drug which re-quires biotransformation via hepatic CYP2D6 to the active metabolitemorphine [89]. Approximately 5%–10% of codeine is converted to mor-phine in the liver, while the remainder is either conjugated, forming

Table 2Properties of opioid medications commonly used in the management of chronic pain.
Drug# Common route ofadministration⁎
Protein binding Bioavailability# Route of elimination Vd⁎⁎
L/kgt½⁎⁎
(h)CYP
Buprenorphine [170,171] TD, B, IV 96% 31%(sublingual)
Renalbiliary
2–3 (IV)⁎
19 (B)26 (TD)
2–4 (parental)18–49 (sublingual)
3A4
Codeine [89] Oral b1% ~90%(oral)
Renal 2.5–3.5 1.2–3.9 3A4, 2D6
Fentanyl [89,172] TD, oral 79% 92% (transdermal)89% (intranasal)50% (buccal)33% (ingestion)
Renal 3–8 3–12 3A4
Hydro Hydrocodone codone [89,90] Oral 20%–50% ??????? Renal 3.3–4.7 3.4–8.8 2D6, 3A4
Hydromorphone [89,173] Oral, IV 19% 30%–35%, (Oral)52%–58%(intranasal)
Renal 2–4 3–9 glucuronidation
Levorphanol [89,120] IV, oral 40% 70% (oral); 100% (IV) Renal 10–13 11–16 glucuronidation
Methadone [108,109] Oral 87% 41%–99%(oral)
Renal 4–7 15–55 3A4 N 2B6 N 2D6
1176B.M
.Kapuretal./ClinicalBiochem
istry47
(2014)1169
–1187

Morphine [89,98] IV, IM, oral 35% 20%–40%(oral),36%–71% (rectally), 100%(IV/IM)
Renal (90%)Biliary (10%)
2–5 1.3–6.7 Glucuronidation (major)2D6 (minor)
Meperidine (Pethidine) [174,175] Oral, IV, IM 45%–64% 50%–60% (Oral),80%–90%(Oral, in cases of hepatic impairment)
hepatic 3.7–4.2 2–5 2B6, 3A4 & 2C19(minor)
Oxycodone [114] Oral 45% 60%–87% Renal 1.8–3.7 3–6 2D6
Oxymorphone [115] Oral 10–12% 10%(oral),40% (Intranasal), 100%(IV, IM)
Renalfecal
2.4 4–12 glucuronidation
Remifentanyl i.v 70% (bound to plasma proteins) Not applicableGiven iv
- - 1–20 min Nonspecific esterases
Tramadol [89,95] Oral 15–20% 70%–75%(oral),77%(rectal),100% (IM)
Renal 2.6–2.9 4.3–6.7 2D6 N 2B6, 3A4
# All chemical formulas and bioavailability are from their respective pages in Wikipedia.⁎ depends on formulation; 2–3 h for immediate release, 5 h for continuous release; TD transdermal; B buccal; IV intra venous.⁎⁎ [169].
1177B.M
.Kapuretal./ClinicalBiochem
istry47
(2014)1169
–1187

1178 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
codeine-6-glucuronide (active), or methylated via CYP3A4, producingnorcodeine (inactive) [89].
Hydrocodone
This is a semi-synthetic drug, similar to codeine in structure and tomorphine in its effects [89]. Hydrocodone is metabolized by CYP2D6to active hydromorphone, which binds to the μ-opioid receptor, andby CYP3A4 to the inactive metabolite norhydrocodone [90].
Tramadol
Tramadol is a synthetic codeine analog that binds to the μ-opioidreceptor and inhibits the reuptake of serotonin and norepinephrine[89]. Tramadol has a lower risk of addiction than other opioids; howev-er, it is associated with two significant adverse drug reactions: seizureand serotonin syndrome [91]. Tramadol seizures usually occur in pa-tients already taking anticonvulsant medications. Serotonin syndromeis characterized by neuromuscular and autonomic hyperactivity aswell as altered mental status, due to excess serotonin activity in theCNS. Higher risk of this syndrome is associated with tramadol overdoseor co-administration of antidepressant medications, such as tricyclicantidepressants and selective serotonin reuptake inhibitors (SSRIs),which, in addition to tramadol, inhibit serotonin reuptake, leading tohigh serotonin levels in the synaptic space[92,93].
Tramadol is metabolized by CYP2D6 in the liver to its main metabo-lite, O-desmethyl-tramadol which shows a higher affinity for opioid re-ceptors than the parent drug [94]. Metabolism to the minor metabolite,N-desmethyl-tramadol occurs via CYP2B6 and CYP3A4 [95].
Strong opioids
Morphine
Morphine increases the threshold for pain perception by bindingstrongly to the μ-opioid receptor; it also has activity towards κ- andδ-opioid receptors. Morphine administered orally undergoes a largefirst-pass effect, resulting in oral bioavailability of 38% on average [96].The major morphine metabolites result from glucuronidation bythe hepatic isoenzyme UGT2B7 to inactive morphine-3-glucuronide(approximately 60%) and active morphine-6-glucuronide (up to 10%)[97]. CYP2D6 plays a minor role in morphine metabolism. Side effectsof morphine include sedation, nausea, a feeling of warmth, urinaryretention, euphoria, reduced ability to concentrate and constipation.The most serious side effect of morphine is potentially fatal respiratorydepression with morphine toxicity [89,98].
Hydromorphone
Hydromorphone, a hydrogenated ketone of morphine, is a syntheticopioid with effects similar to morphine [89]. When given orally,hydromorphone is rapidly absorbed by the GI tract and undergoesextensive first-pass metabolism in the liver. Like morphine, it isglucuronidated in the liver to hydromorphone-3-glucuronide andhydromorphone-6-glucuronide; hydromorphone-3-glucuronide hasno analgesic properties, but has been shown to exhibit neuroexcitatoryeffects [99]. Hydromorphone suppresses the cough reflex, similar toother opioids. Side effects of hydromorphone are dose-related and caninclude mood changes, euphoria, nausea, vomiting, and hypotension,as well as respiratory depression in large doses [89].
Fentanyl
Fentanyl is a highly lipophilic, synthetic opioid which is 100 timesmore potent than morphine. Its potency is due to its efficiency in cross-ing the blood brain barrier, rapidly gaining access to the central nervous
system [89,100,101]. Given intravenously, fentanyl has a very rapidonset but short duration of action, and is thus administered as a contin-uous infusion. In managing pain, fentanyl is most often providedthrough transdermal patches or buccal tablets [89]. This allows thedrug to distribute throughout fatty tissues, leading to slower releaseand prolonged effects. Fentanyl undergoes extensive pulmonaryfirst-pass metabolism as well as hepatic metabolism to the inactivemetabolite norfentanyl via CYP3A4 [89].
Remifentanil
Remifentanil is a μ-opioid receptor agonistwith an analgesic potencysimilar to that of fentanyl. It was studied for analgesic efficacy correlat-ing with expression of the serotonin transporter (5-HTT), as serotonincan influence the antinociceptive effects of opioids at the spinal cord.Remifentanil has a significantly better analgesic effect in individualswith a genotype coding for low 5-HTT expression (SA/SA and SA/LG)compared to those with high expression (LA/LA) [102]. It is predomi-nantly metabolized by non-specific esterases [103], and because of itsrapid systemic elimination and ultra-short half-file, it has a pharmacoki-netic advantage in clinical situations requiring predictable terminationof effect such as analgesia during labor [104]. In a systematic review,Leong and colleagues compared remifentanil with meperidine forlabor analgesia. They found remifentanil to be superior in reducingmean visual analog scale pain scores for labor pain after 1 h [105].Remifentanil crosses the placenta, but is rapidly metabolized andredistributed. Although maternal sedation and respiratory changes dooccur, they are without adverse neonatal or maternal effects [106].
Methadone
Methadone is a synthetic opioidwithmorphine-like effects. It is com-monly used in the treatment of opioid addiction, but also in the treat-ment of chronic pain [89,107,108]. Given orally, methadone has amuch higher bioavailability compared with oral morphine (70%–90%,compared to 38%, respectively). Due to its relatively slow metabolismand high lipid solubility, methadone also has a long half-life (between8 and 60 h), leading to longer term analgesia than with morphine [107,108]. Methadone is extensively metabolized by CYP3A4, and to a lesserextent by CYP1A2, -2D6, -2D8, -2C9/2C8, -2C19, and -2B6, to its inactivemetabolite, 2-ethylidene-1,5-dimethyl-3,3-diphenylpyrrolidine (EDDP)[107–110]. Caution must be exercised when co-prescribing methadonewith QT-prolonging cardiac drugs due to methadone’s ability to interactwith voltage-gated potassium channels in the myocardium, also leadingto QT prolongation [111] and ventricular arrhythmias such as Torsadesde Pointes. Significant drug–drug interactions have been reported formethadone, when combined, for example, with fluoxetine, quetiapine,or promethazine [110].
Buprenorphine
As an alternative to methadone, buprenorphine can be used for thetreatment of opioid addiction [89]. It has also been approved forthe treatment of moderate to severe pain [112]. Similarly to morphine,buprenorphine must be used with caution in the setting of co-administration of other QT-prolonging medications or in individualswith hyperkalemia [112]. Buprenorphine has a ceiling effect withrespect to respiratory depression, thereby reducing the likelihood ofthis potentially fatal consequence, making it an attractive choice for an-algesia [113]. Given orally, buprenorphine undergoes extensive first-pass metabolism and is therefore usually administered by transdermalor buccal routes to improve bioavailability [112]. Prolonged analgesiacan be achieved with buprenorphine due to its lipophilic propertiesand its slow dissociation from opioid receptors. Buprenorphine ismetabolized by CYP3A4 in the liver primarily to nor-buprenorphine.

1179B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
Oxycodone
Oxycodone is a synthetic opioid, similar in structure to codeine andprescribed for moderate to severe pain [89]. This drug is commonlycompounded with other drugs, such as acetaminophen or ibuprofen[89]. Side effects of oxycodone treatment include euphoria, sedation,constipation, cough suppression and respiratory depression. The eupho-ria caused by oxycodone is quite pronounced and can therefore lead toabuse of and dependence on the drug. Oxycodone is metabolized, via
Table 3Antidepressants commonly used in pain management.
Drug# Common route ofadministration
Protein binding Bioavailability#
Amitriptyline [176] Oral N 90% 30%–60%due to first pas
Bupropion [177] Oral 85% ??????
Citalopram [178] Oral 50% 80%
Desipramine [179] Oral 70%–90% 73%–92%
Duloxetine [180] Oral N90% 32% to 80%
Fluoxetine [181] Oral 94% 72%
Venlafaxine [182] Oral 27% 42% ± 15%
# All chemical formulas and bioavailability data are from their respective pages in Wikipedi⁎ [169].
CYP2D6, to the potent metabolite oxymorphone (see below) as wellas noroxycodone, a weakly active metabolite [114].
Oxymorphone
Oxymorphone offers excellent analgesia, comparable to that ofmorphine, but with less sedative effects [115]. This results from thelipophilic nature of oxymorphone, allowing ease of access to the cen-tral nervous system. Oxymorphone undergoes extensive hepatic
Route of elimination Vd⁎
L/kgt½⁎
(h)CYP
s metabolismRenal 6–10 8–51 2D6
RenalFecal
40 4–24 2B6
Renal 12–16 25–40 2C19, 3A4, 2D6
Renal 22–59 12–54 2D6
RenalFecal
17–26 8–17 1A2,2D6
RenalFecal
20–42 1–3 days 2D6
renal 4–12 3–7 2D6, 3A4
a.

1180 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
first-pass metabolism, and its major route of metabolism is viaglucuronidation [89,115].
Meperidine (pethidine)
Meperidine (Demerol™), also known as pethidine, is a syntheticμ-opioid receptor agonist that is structurally similar to atropine.Pharmacologically, it represents both morphine and atropine. Thisunique property of an analgesic with spasmolytic and sedative actionaccounts for its wide range of clinical applications [116]. Althoughmeperidine efficacy has been questioned [117], a survey of intrapartumanalgesia practice in United Kingdom and Norway reported that thisopioid is still commonly used during labor [118,119].
Levorphanol
Levorphanol is a synthetic opioid, similar in structure to morphine,but more potent in its analgesic effects [89,120] and also has anticholin-ergic effects [120]. This drug is usually given orally or intravenously andis eliminated through glucuronidation in the liver [120].
Other medications in the treatment of chronic pain
Antidepressants
Tricyclic antidepressants (TCAs) and selective serotonin re-uptakeinhibitors (SSRIs) are commonly used as adjuvant therapy in thetreatment of chronic pain. Themechanisms bywhich thesemedicationsalleviate pain are not fully understood, but are believed to be mediatedthrough their inhibition of neurotransmitter reuptake in the synapticcleft. These mechanisms are related to pain signaling in descendingspinal pain pathways [121]. In addition to their analgesic role, antide-pressants are commonly used in pain management because depression
Table 4Anticonvulsant drugs used in pain management.
Drug# Common route ofadministration
Protein binding Bioavailability#
Carbamazepine [183,184] Oral 75% ??????
Gabapentin [185] Oral b 3% 27%–60% (inversely
Lamotrigine [186] Oral 55% 98%
Phenytoin [187,188] Oral, IV 87%–93% 70%–100%oral,24.4%(rectal, IV)
# All chemical formulas and bioavailability data are from their respective pages in Wikipedi⁎ [169].
is often a co-morbidity of chronic pain. Patients experiencing chronicpain have been shown to have 2–5 times the risk of developing depres-sion than the general population [122].
Common TCAs used in pain management include amitriptyline andimipramine (Table 3), administered at much lower doses for painmanagement than for psychiatric indications [22]. These two drugsare metabolized to the active metabolites nortriptyline and desipra-mine, respectively, by hepatic CYP2D6 [22]. Side effects of TCAs thatcan limit their use includeweight gain, anticholinergic effects, hypoten-sion and cardiovascular effects [22,121]. TCAs have been better charac-terized for their role in painmanagement than SSRIs [121].SSRIs used inpainmanagement include fluoxetine and citalopram(Table 3). SSRIs areoften better tolerated than TCAs, due to their milder side effects; how-ever, data regarding their efficacy in the treatment of chronic painhave been inconsistent [121].
More recently, antidepressants able to target several neurotransmit-ters, such as venlafaxine (serotonin, norepinephrine, and dopamine),duloxetine (serotonin and norepinephrine) and bupropion (serotoninand dopamine) have been more widely used in pain management(Table 3). Venlafaxine has been shown to be particularly efficaciouswhen prescribed in combination with gabapentin, a GABA analogueoften used to treat neuropathic pain [123].
Anticonvulsants
Anticonvulsants (Table 4) have been used in painmanagement sincethe 1960’s when these drugs were originally introduced for the treat-ment of epileptic seizures [124]. These medications work by a varietyof mechanisms to suppress the rapid firing of neurons. Phenytoin, oneof the first anticonvulsants introduced, reduces neuronal excitabilityby blocking sodium channels. It has been used in the treatment ofchronic neuropathic pain, but today its use for this indication is limiteddue to side effects, namely, sedation and motor disturbances [125].
Route of elimination Vd⁎
L/kgt½⁎
(h)CYP
Renal 0.8–1.8 18–65 3A4
proportional to dose) Renal 0.8–1.3 5–9 Not metabolized
Renal 0.9–1.3 12–62 glucuronidation
Biliary 0.5–0.8 8–60 2C19
a.

1181B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
Carbamazepine has largely replaced phenytoin in chronic painmanagement and has been shown to be effective in the treatment ofneuropathic pain, in particular trigeminal neuralgia [124,126] (a disor-der characterized by episodes of intense facial pain, originating fromthe trigeminal nerve) [126]. Side effects of carbamazepine includedrowsiness, blurred vision, nausea and vomiting. There is a dose–effectrelationship and it can be difficult to achieve a therapeutic effect in pa-tients who are sensitive to these side effects [125]. This is of particularrelevance in elderly patients, where conditions such as cardiac diseaseand hypernatremia can further complicate adverse effects [127]; thus,close monitoring of these patients is required [124,125].
Newer anticonvulsants, such as lamotrigine and gabapentin, areshowing promise in chronic pain management; gabapentin, in particu-lar, has been shown to be well tolerated with few side effects [128].Gabapentin binds to voltage-gated calciumchannels, leading to a reduc-tion in the release of the neurotransmitters glutamate and substance P.It has demonstrated effectiveness in the treatment of diabetic neuropa-thy, post-herpetic neuralgia, trigeminal neuralgia, multiple sclerosis,migraine as well as in chronic pain caused by malignancy [128].Lamotrigine has been shown to be useful in the treatment of trigeminal
Table 5Triptans used in migraine therapy [130,132].
Drug# Common route ofadministration
Protein binding Bioav
Almotriptan[131] Oral 35% 70%
Eletriptan[131] Oral 85% 50%
Frovatriptan[131] Oral 15% 20%–
Naratriptan[131] Oral 20%–30% 74%
Rizatriptan[131] Oral 14% 45%
Sumatriptan[131] Oral 14%–21% 15%(oral)96%(s.c)
Zolmitriptan[131] Oral, nasal 25% 40% (
# All chemical formulas and bioavailability data are from their respective pages in Wikipedi⁎ MAO: monoamine oxidase.⁎⁎ [169].
neuralgia and diabetic neuropathy [124]. However, careful titration oflamotrigine dose is required because of the risk of Stevens–Johnsonsyndrome, a life-threatening dermatological condition leading to cellnecrosis, causing the epidermis to separate from the dermis [129].
Triptans
Triptans are serotonin agonists with high affinity for the 5HT1B and5HT1D receptors [130,131]. The serotonergic system is known to play arole in the pathophysiology of migraines, leading to the developmentand prescription of triptans for this condition. Binding of these drugsto 5HT receptors in the brainstem and thalamus leads to the blockadeof vasoactive peptide release from perivascular trigeminal neurons,and thus reduced cerebral vasodilation [131]. Currently, there areseven triptanmolecules available, eachwith its unique pharmacokineticand pharmacodynamic profile. The fourmost commonly prescribed andwell characterized triptans are sumatriptan, naratriptan, zolmitriptanand rizatriptan (Table 5) [132]. Triptans are not recommended for mi-graine treatment in individuals with poorly controlled hypertension,
ailability# Route of elimination Vd⁎⁎
L/kgt½⁎⁎
(h)CYP
RenalFecal
2.5–4 3–4 3A4, MAO⁎, 2D6
Renal 2.1–3.3 3–7 3A4
30% Renal 3–4.2 20–30 1A2, 2D6
Renal 2–3 5–6 Unknown CYP
Renal 1.3–2.2 1.6–3.2 MAO, 1A2
Renal 1.3–4.6 1–4 MOA
oral) RenalFecal
7.0 1.6–3.8 1A2, MAO, 3A4
a.

1182 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
hepatic or renal impairment or coronary artery disease, as serotonergicblockade may exacerbate these conditions [131].
Benzodiazepines
Benzodiazepines play a role in the treatment of insomnia, muscletension, and, in particular, anxiety related to chronic pain [133]. Chronicpain patients experience increased anxiety compared to the generalpopulation, and this can often worsen the subjective experience ofpain. Evidence suggests that benzodiazepines are only effective intreating acute anxiety related to chronic pain, but are not effective inthe setting of chronic anxiety [133] (for which antidepressants havebeen found to be more effective). The caveats to benzodiazepine treat-ment for chronic pain are the potential for abuse as well as side effects,including paradoxical reactions (increased hostility, psychosis andbehavioral disturbances) [133].
Cannabinoids
Cannabis is an annual plant that grows wild in regions of mild ortropical weather, and has been used to treat pain for centuries. It is byfar the most widely cultivated, trafficked and abused illicit drug; halfof all drug seizures worldwide are of cannabis. The geographical spreadof those seizures is also global, covering practically every country of theworld. Delta-9-tetrahydrocannabinol (THC) is the active componentin cannabis, responsible for its analgesic and psychoactive effects.Ingestion of THC results in feelings of euphoria, relaxation and a generalsense of well-being. However, heavy cannabis use can result in halluci-nations, anxiety and depression [134,135].
Endogenous cannabinoids, referred to as endocannabinoids, havebeen identified, as well as two endocannabinoid receptors, the G-protein coupled receptors CB1 and CB2. High levels of CB1 are expressedin the brain and spinal cord, particularly in areas known to be involvedin nociception. CB2 is not as well characterized, but has been shown tohave lower expression levels in the brain than CB1. Endocannabinoidsare bioactive lipids which regulate neural activity by binding to CB1and CB2, causing inhibition of neurotransmitter release. Endogenousand exogenous cannabinoid activity results in anti-nociceptive effectsas well as short-term memory impairment, stimulation of appetiteand antiemetic effects [134–136].
THC acts synergistically with other analgesic agents, such asmorphine and some NSAIDs, though the mechanism for the synergisticaction between morphine and THC is unknown [134]. In the case ofNSAIDs, cannabinoids and prostaglandin share a similar structurewhich is believed to result in a convergence of signals. Activity of CB1 re-ceptors is increased by NSAIDs including ibuprofen and indomethacin.Furthermore, CB1 receptor antagonists block the analgesic effects ofibuprofen [134].
Evidence for the use of cannabinoids in pain management is lackingdue to the small number of clinical trials in this area. The best evidencefor cannabinoid use in chronic pain comes fromHIVandmultiple sclerosisstudies inwhich cannabinoidswere used to treat the chronic neuropathicpain associated with these conditions [136]. Smoking cannabis 3–5 timesper week was shown to be effective in alleviating neuropathic painassociated with HIV as well as AIDS-related anorexia [137,138]. Severalstudies demonstrated benefit of oral treatment with synthetic THC forcentral pain and spasticity associated with multiple sclerosis [139–142].
There are several issues associated with the use of cannabinoids inpainmanagement. Firstly, themethod of drug delivery poses a problem.Smoking of cannabis is the easiest delivery route and allows for ade-quate control of dose [135,136]. However, the adverse effects ofsmoking are well known, with THC contents varying depending onwhere and how the cannabis plants are grown. Canada, which allowsprescription of cannabis for chronic pain therapy, requires that patientsobtain their medicinal cannabis from a centralized source so that theTHC content may be monitored over time [136]. Similar strategies are
now under consideration in different parts of the world including theUnited States. Synthetic cannabinoids, such as dronabinol and nabilone,are available in the U.S. and Canada for use as antiemetics during cancerchemotherapy, and as adjunct therapies for neuropathic and chronicpain. They are not yet widely used, and are under further study to delin-eate their efficacy and pharmacological parameters in various clinicalcontexts [143]. Side effects include increased heart rate, blood pressurechanges, anxiety, psychomotor retardation, impaired memory and psy-chosis. Cannabinoids are contraindicated in pregnancy, uncontrolledhypertension, active ischemic heart disease, arrhythmias and schizo-phrenia. Clark and co-workers suggest guidelines for the use of thesecannabinoid compounds [144].
Cannabis and cannabinoids have a potential for dependence, whichcan lead to preoccupation and compulsion. Prescription of cannabinoidsfor chronic pain management requires clinician to appropriately selectpatient and adequately monitor to avoid the development of depen-dence [134,136]. Recently, Donoghue and colleagues report the interac-tion effect of cannabis use on gender and age of onset of schizophreniaand schizoaffective disorder. They show that use of cannabis is associat-ed with an earlier age of onset of schizophrenia. There is a significantinteraction between gender and cannabis use whereby the genderdifference in age of onset is diminished in cannabis users [145].
Ziconotide
Ziconotide is a synthetic conopeptide that selectively inhibits N-typevoltage-gated calcium channels, reducing the release of pain-modulating neurotransmitters. Conopeptides are derived from thevenom of predatory cone snails, and ziconotide is specifically derivedfrom the venom of a Pacific fish-hunting snail, Conus magus [146].
Ziconotide has been approved for intrathecal administration bycontinuous infusion for the treatment of severe chronic pain in situa-tions where patients are not responding to conventional therapies[147]. Evidence indicates that this drug is useful in the treatment ofboth neuropathic and non-neuropathic pain. Intrathecal administrationis required because, given intravenously, ziconotide demonstrates poorpenetration of the blood brain barrier and results in sympatholyticeffects leading to orthostatic hypotension [147]; oral preparations arenot available. Ziconotide is highly hydrophilic and is thought to moveslowly through the CSF to its target receptor, leading to a lag time toanalgesia upon administration. The efficacy of ziconotide shows awide inter-individual variation [147,148].
The most common side effects of ziconotide include dizziness,confusion, ataxia, memory impairment and hallucinations. However,there is also large inter-individual variation in the experience of side ef-fects [147]. Toxicity appears to be related to the rate of infusion and isreversible after discontinuation, but, because of low tissue diffusion,the effects can persist for several weeks [147,148]. Data regardingziconotidemetabolism are sparse. The drug is not believed to bemetab-olized in the CSF but rather cleared by transport into the systemiccirculation where it is degraded by serum proteases [147].
Novel therapies in pain management
Targeting epigenetic modifications
Epigenetics refers to functionally relevant genomic changes not in-volving alterations in nucleotide sequence, in response to developmen-tal or environmental cues. Epigenetic mechanisms are manifestedthrough dynamic, reversible chemical modifications in the genomeand are involved in differential gene expression throughout life[149]. The most well characterized epigenetic modifications are DNAmethylation and histone acetylation.
DNAmethylation is regulated by DNAmethyltransferases,while his-tone modifications are largely regulated by histone deacetylases(HDAC) [149]. Abnormal DNA methylation [150] and histone

1183B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
acetylation [151,152] have been demonstrated to occur in pain states. Ithas also been proposed that primary injuriesmay result in lasting epige-netic marks leading to an increased risk of chronic pain [149], whichmay even persist trans-generationally. Drugs aimed at targeting the en-zymes responsible for epigenetic modifications are under developmentand in some cases have been approved by the FDA. While these drugshave been developed largely for the purpose of cancer treatment, theyare also believed to have potential in painmanagement. In animal injurymodels, rat hind-paw injection of Freund’s complete adjuvant (CFA)followed by intrathecal injection of zebularine, a DNA methyltransfer-ase inhibitor, was shown to reduce pain sensitivity [153]. In a similarrat model, pre-injection treatment with HDAC inhibitors was reportedto delay CFA-induced thermal hyperalgesia whereas post-injectiontreatment was shown to reduce the intensity of CFA-induced thermalhyperalgesia [154]. In human patients with type 2 diabetes, treatmentwith valproic acid, which is a known to act as a strong the HDAC inhib-itor, conferred improved pain sensitivity scores after treatmentcompared to before treatment [155].
Gene therapy
Gene therapy involves the use of viral vectors where the viral ge-nome is replaced with nucleic acid sequences encoding a promoter todrive gene expression as well as a transgene of interest [156]. For painmanagement therapies, the transgene encodes for an analgesic agent.Gene therapy based approaches have several advantages in painmanagement. In contrast to pharmacotherapies, gene therapy allowsfor persistent expression of a protein-based analgesic agent at the siteof action. These methods avoid the first-pass effect and can improvebioavailability [156]. Gene therapy can also reduce side effects associat-ed with systemic drug use. There are limitations to these approaches,including inadequate transgene expression and the evocation ofimmune responses against the viral vectors [156]. Nevertheless, newparadigms using non-viral insertion of therapeutic transgenes areunder way to bypass some of these limitations.
In a recent study, terminal cancer patients were given different genedoses of human PENK, encoding preproenkephalin, the protein precur-sor that is processed to 6-met-enkephalin and 1-leu-enkaphalin, endog-enous opioid peptide ligands for the delta opioid receptor [157].Patients in the two highest virus dose groups reported decreases in nu-meric rating scale (NRS) pain scores of up to 50% from before treatment.Patients in the higher dose groups reported substantial reductions inpain compared to patients in the lowest dose group. This study demon-strates proof-of-concept for gene therapy in pain management.
0500100015002000250030003500400045005000
EDD
P n
g/m
L
date of
Pt X
EDDP
UEW
Fig. 4. EDDP urine excretion window at steady state. Legend: *UEW urinary excretion win(EDDP) excretion window.
Therapeutic drug monitoring in pain management
In pain management, the rationale for drug monitoring has largelyfocused on monitoring patient adherence, detecting diversion, anddetecting the presence of illicit, non-prescription drugs. Traditionally,drug monitoring in pain management patients has been in the form ofurine drug testing.
Urine drug testing has been demonstrated to reduce illicit druguse and has been widely used in monitoring patients in treatmentfor drug addiction [158,159]. However, most urine methodologieshave been adapted from occupational deterrent-based testing forillicit drug use and have not been optimized for use in the painmanagement setting [160]. Given the chronicity of treatment drugadministration, and the wide range of drug half-lives (Tables 1–5)a “positive” urine result is to be expected if a patient is adherent intaking his/her medication. A “negative” urine results suggests non-compliance with the treatment protocol or urine sample tampering.To be used effectively in monitoring pain management patients,urine drug testing requires understanding of the principles of drugpharmacokinetics and pharmacodynamics, and an understandingof the type of information urine drug testing can provide alongwith an appreciation of the limitations of such testing [161].
Urine drug concentrations are often calculated relative to urinecreatinine concentrations in order to correct for in vivo dilution, whichcan vary through time, depending on an individual’s fluid intake.However, these calculations assume stable renal function and creatinineproduction, an assumption which can lead to errors if unjustified. Painmedications are usually prescribed to be taken in a chronic manner sothat steady state plasma concentrations and therapeutic pharmacody-namic effects can be achieved. Steady state drug concentrations inserum imply that the urine excretion window (UEW) of the drug/me-tabolite is also at “steady state” in patients with stable renal function.Fig. 4 shows the concentration of methadone metabolite 2-ethylidene-1,5-dimethyl-3,3-diphenylpyrrolidine (EDDP) in a patient receivingmethadone chronically. This figure clearly shows that urine creatininecorrection does not add value to the EDDP adherence monitoring.Here, patient non-adherence can be detected when the urine EDDPconcentration falls outside the UEW [162]. Extremely low creatinineconcentrations are indicative of potential adulteration and can be usefulin detecting specimens that have been tampered with [161]. Unfortu-nately, urine drug testing is not effective in estimating serum drugconcentrations or assessing drug efficacy.
In light of the limitations associated with urine drug testing, moni-toring of pain management patients through serum or plasma drugmeasurements has been advocated. Therapeutic drug monitoring
0.00
10.00
20.00
30.00
40.00
50.00
60.00
pHan
dU
Cr
analysis
Y
Creatinine PH
problem samples
dow. The green lines represent the 2-ethylidene-1,5-dimethyl-3,3-diphenylpyrrolidine

1184 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
(TDM) involves the measurement of serum or plasma drug levels attimed intervals to determine whether steady state drug concentrationsare within the therapeutic or expected range given the drug dosage[163]. TDM can be used by clinicians to explain drug toxicity or lack ofefficacy, and can aid in adjusting drug doses or in choosing specificmedications [163]. A major advantage of plasma drug measurement isthat it integrates many factors affecting drug metabolism, as outlined inFig. 2. Half-lifemeasurement can be a functionalmarker of the cumulativeeffect of pathophysiological and drug–drug interactions and provide anoverall picture of the specific drug disposition and pharmacodynamicsin the individual patient. However, TDM requires the collection of serialblood samples from patients, which can be difficult and inconvenient[160,163]. Timing of sample collection also becomes an important consid-eration, depending on whether peak or trough measurements (or both)are to be monitored. The time window within which a particular drugor its metabolite can be detected in serum is an important considerationfor sample collection. To assist in appropriate clinical interpretation,knowledge of tolerance and pharmacokinetics of particular drug(s)under investigation is essential.
Summary and conclusions
The experience of chronic pain is one of the commonest reasons in-dividuals seek medical attention, making the management of chronicpain a major issue in clinical practice. Left untreated, chronic pain canlead to diminished quality of life and socioeconomic difficulties.
Opioids continue to be the mainstay of chronic pain management.However, opioid use can lead to abuse, diversion and physical depen-dence, meaning that opioidsmay not be suitable for all patients. An indi-vidual’s risk for abuse should be considered, by way of a detailed history,before opioids are prescribed. Several non-opioid based therapies arenowpotentially available for these patients, such as triptans, ziconotides,as well as novel therapies, such as treatment with cannabinoids and, inthe not-so-distant future, gene therapy or epigenetic-based approaches.Adjuvant therapies with antidepressants, benzodiazepines or anticon-vulsants can also be useful in managing pain, particularly in the treat-ment of anxiety and depression, which are commonly associated withchronic pain.
Genetic variability can have profound effects on drug metabolismand contribute to the inter-individual diversity in responses to painmedications. However, there is a paucity of evidence for the benefitsof pharmacogenetic testing in the context of pain management. Drugmetabolism and responses are affected by many factors, includingpharmacogenetics, with genetics offering only a partial explanation ofan individual’s response.
At this point in time, therapeutic drug monitoring, through plasmadrug measurements, may be more useful than pharmacogenetics inpreventing adverse drug reactions to pain medications, while ensuringeffective analgesia. Definitive, mass spectrometry based methods,capable of measuring parent drug and metabolite levels, are the mostuseful assays for this purpose. Drug half-life can be a functional markerof the cumulative effect of drug–drug interactions as well as pathophys-iological interactions that may affect the treatment drug’s disposition.Currently, monitoring of pain management patients, if performed atall, is largely through urine drug measurements, which do not correlatewith serum drug concentrations therefore limiting their use inmonitor-ing efficacy and toxicity. Direct determination of serum or plasma druglevels may provide a more clinically useful, if logistically more difficult,avenue for optimization of drug therapy, particularly in the context ofchronic pain management.
References
[1] Bonica JJ. The need of a taxonomy. Pain 1979;6:247–8.[2] Furlan AD, Reardon R, Weppler C, Group NOUG. Opioids for chronic noncancer
pain: a new Canadian practice guideline. Can Med Assoc J 2010;182:923–30.
[3] Hardt J, Jacobsen C, Goldberg J, Nickel R, Buchwald D. Prevalence of chronic pain ina representative sample in the united states. Pain Med 2008;9:803–12.
[4] Organization W.H. Cancer pain relief with a guide to opioid availability; 1996.[5] Kroenke K, Krebs E,Wu J, Bair MJ, Damush T, Chumbler N, et al. Stepped care to op-
timize pain care effectiveness (scope) trial study design and sample characteristics.Contemp Clin Trials 2013;34:270–81.
[6] Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al.Neuropathic pain: redefinition and a grading system for clinical and researchpurposes. Neurology 2008;70:1630–5.
[7] Gilron I, Watson CP, Cahill CM, Moulin DE. Neuropathic pain: a practical guide forthe clinician. Can Med Assoc J 2006;175:265–75.
[8] Kroenke K, Krebs EE, Bair MJ. Pharmacotherapy of chronic pain: a synthesis of rec-ommendations from systematic reviews. Gen Hosp Psychiatry 2009;31:206–19.
[9] Dubin AE, Patapoutian A. Nociceptors: the sensors of the pain pathway. J Clin Invest2010;120:3760–72.
[10] Tyrer S. Psychosomatic pain. Br J Psychiatry 2006;188:91–3.[11] Arendt-Nielsen L, Svensson P. Referred muscle pain: basic and clinical findings. Clin
J Pain 2001;17:11–9.[12] Kooijman CM, Dijkstra PU, Geertzen JH, Elzinga A, van der Schans CP. Phantompain
and phantom sensations in upper limb amputees: an epidemiological study. Pain2000;87:33–41.
[13] Carr DB, Goudas LC. Acute pain. Lancet 1999;353:2051–8.[14] Schopflocher D, Taenzer P, Jovey R. The prevalence of chronic pain in canada. Pain
Res Manag 2011;16:445–50.[15] Pergolizzi J, Ahlbeck K, Aldington D, Alon E, Coluzzi F, Dahan A, et al. The develop-
ment of chronic pain: physiological change necessitates a multidisciplinaryapproach to treatment. Curr Med Res Opin 2013;29:1127–35.
[16] Ricci JA, StewartWF, Chee E, Leotta C, Foley K, HochbergMC. Back pain exacerbationsand lost productive time costs in united states workers. Spine 2006;31:3052–60.
[17] Eriksen J, Ekholm O, Sjogren P, Rasmussen NK. Development of and recovery fromlong-term pain. A 6-year follow-up study of a cross-section of the adult danishpopulation. Pain 2004;108:154–62.
[18] Elliott AM, Smith BH, Penny KI, Smith WC, Chambers WA. The epidemiology ofchronic pain in the community. Lancet 1999;354:1248–52.
[19] Kuehn BM. Opioid prescriptions soar: increase in legitimate use as well as abuse.JAMA 2007;297:249–51.
[20] National Center for Health Statistics. Health, United States, 2012: with Special Fea-ture on Emergency Care. Selected prescription drug classes used in the past 30days, by sex and age: United States, selected years 1988–1994 through 2007–2010, Table 92; 2012. http://www.cdc.gov/nchs/hus/contents2012.htm#092.
[21] Stamer UM, Stuber F. Genetic factors in pain and its treatment. Curr OpinAnaesthesiol 2007;20:478–84.
[22] Stamer UM, Zhang L, Stuber F. Personalized therapy in pain management: wheredo we stand? Pharmacogenomics 2010;11:843–64.
[23] Klepstad P, Rakvag TT, Kaasa S, Holthe M, Dale O, Borchgrevink PC, et al. The 118A N G polymorphism in the human mu-opioid receptor gene may increasemorphine requirements in patients with pain caused by malignant disease. ActaAnaesthesiol Scand 2004;48:1232–9.
[24] Lalovic B, Kharasch E, Hoffer C, Risler L, Liu-Chen LY, Shen DD. Pharmacokineticsand pharmacodynamics of oral oxycodone in healthy human subjects: role ofcirculating active metabolites. Clin Pharmacol Ther 2006;79:461–79.
[25] Kirchheiner J, Schmidt H, Tzvetkov M, Keulen JT, Lotsch J, Roots I, et al. Pharmaco-kinetics of codeine and its metabolite morphine in ultra-rapid metabolizers due tocyp2d6 duplication. Pharmacogenomics J 2007;7:257–65.
[26] Světlík S, Hronova K, Bakhouche H, Matouskova O, Slanar O. Pharmacogenetics ofchronic pain and its treatment. Mediators Inflamm 2013;2013:864319.
[27] Rendic S, Di Carlo FJ. Human cytochrome p450 enzymes: a status report summarizingtheir reactions, substrates, inducers, and inhibitors.DrugMetabRev1997;29:413–580.
[28] EichelbaumM, Ingelman-Sundberg M, Evans WE. Pharmacogenomics and individ-ualized drug therapy. Annu Rev Med 2006;57:119–37.
[29] Wang B, Yang LP, Zhang XZ, Huang SQ, Bartlam M, Zhou SF. New insights into thestructural characteristics and functional relevance of the human cytochrome P4502D6 enzyme. Drug Metab Rev 2009;41:573–643.
[30] Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome p450 enzymesand its clinical impact. Drug Metab Rev 2009;41:89–295.
[31] Johansson I, Lundqvist E, Bertilsson L, Dahl ML, Sjoqvist F, Ingelman-Sundberg M.Inherited amplification of an active gene in the cytochrome p450 cyp2d locus asa cause of ultrarapid metabolism of debrisoquine. Proc Natl Acad Sci U S A1993;90:11825–9.
[32] Yeo RK, Rostami-Hodjegan A, Tucker GT. Abundance of cytochromes P450 inhuman liver: a meta-analysis. Br J Clin Pharmacol 2004;57(5):687–8.
[33] Gasche Y, Daali Y, Fathi M, Chiappe A, Cottini S, Dayer P, et al. Codeine intoxicationassociated with ultrarapid CYP2D6 metabolism. N Engl J Med 2004;351:2827–31.
[34] Koren G, Cairns J, Chitayat D, Gaedigk A, Leeder SJ. Pharmacogenetics of morphinepoisoning in a breastfed neonate of a codeine-prescribed mother. Lancet2006;368:704.
[35] Health Canada. Important safety information on tylenol with codeine in nursingmothers and ultra-rapid metabolizers of codeine - for health professionals; 2008.
[36] FDA warning on codeine use by nursing mothers. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108968.htm; 2007 [Accessed 21 January2014].
[37] Pilotto A, Franceschi M, Vitale DF, Zaninelli A, Masotti G, Rengo F, et al. Upper gas-trointestinal symptoms and therapies in elderly out-patients, users of non-selectivensaids or coxibs. Aliment Pharmacol Ther 2005;22:147–55.
[38] Visser LE, van Schaik RH, van VM, Trienekens PH, De Smet PA, Vulto AG, et al. Allelicvariants of cytochrome P450 2C9 modify the interaction between nonsteroidal

1185B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
anti-inflammatory drugs and coumarin anticoagulants. Clin Pharmacol Ther2005;77:479–85.
[39] Wadelius M, Chen LY, Lindh JD, Eriksson N, Ghori MJ, Bumpstead S, et al. Thelargest prospective warfarin-treated cohort supports genetic forecasting.[erratumappears in blood. 2014 feb 13;123(7):1113]. Blood 2009;113:784–92.
[40] Kirchheiner J, Stormer E, Meisel C, Steinbach N, Roots I, Brockmoller J. Influence ofCYP2C9 genetic polymorphisms on pharmacokinetics of celecoxib and its metabo-lites. Pharmacogenetics 2003;13:473–80.
[41] Pilotto A, Seripa D, Franceschi M, Scarcelli C, Colaizzo D, Grandone E, et al. Geneticsusceptibility to nonsteroidal anti-inflammatory drug-related gastroduodenalbleeding: role of cytochrome P450 2C9 polymorphisms. Gastroenterology2007;133:465–71.
[42] Zwisler ST, Enggaard TP, Noehr-Jensen L, Mikkelsen S, Verstuyft C, Becquemont L,et al. The antinociceptive effect and adverse drug reactions of oxycodone inhuman experimental pain in relation to genetic variations in the oprm1 andabcb1 genes. Fundam Clin Pharmacol 2010;24:517–24.
[43] Campa D, Gioia A, Tomei A, Poli P, Barale R. Association of abcb1/mdr1 andoprm1 gene polymorphisms with morphine pain relief. Clin Pharmacol Ther2008;83:559–66.
[44] Levran O, O'Hara K, Peles E, Li D, Barral S, Ray B, et al. ABCB1 (MDR1) geneticvariants are associated with methadone doses required for effective treatment ofheroin dependence. Hum Mol Genet 2008;17:2219–27.
[45] Park HJ, Shinn HK, Ryu SH, Lee HS, Park CS, Kang JH. Genetic polymorphisms inthe ABCB1 gene and the effects of fentanyl in Koreans. Clin Pharmacol Ther2007;81:539–46.
[46] Lee YS, Kim H, Wu TX, Wang XM, Dionne RA. Genetically mediated interindividualvariation in analgesic responses to cyclooxygenase inhibitory drugs. ClinPharmacol Ther 2006;79:407–18.
[47] Janicki PK, Schuler G, Francis D, Bohr A, Gordin V, Jarzembowski T, et al. A geneticassociation study of the functional A118G polymorphism of the human mu-opioidreceptor gene in patients with acute and chronic pain. Anesth Analg2006;103:1011–7.
[48] Fillingim RB, Kaplan L, Staud R, Ness TJ, Glover TL, Campbell CM, et al. The a118gsingle nucleotide polymorphism of the mu-opioid receptor gene (OPRM1) isassociated with pressure pain sensitivity in humans. J Pain 2005;6:159–67.
[49] Landau R, Kern C, Columb MO, Smiley RM, Blouin JL. Genetic variability of the mu-opioid receptor influences intrathecal fentanyl analgesia requirements in laboringwomen. Pain 2008;139:5–14.
[50] Rakvag TT, Klepstad P, Baar C, Kvam TM, Dale O, Kaasa S, et al. The val158met poly-morphism of the human catechol-O-methyltransferase (COMT) gene may influ-ence morphine requirements in cancer pain patients. Pain 2005;116:73–8.
[51] Reyes-Gibby CC, Shete S, Rakvag T, Bhat SV, Skorpen F, Bruera E, et al. Exploringjoint effects of genes and the clinical efficacy of morphine for cancer pain:OPRM1 and COMT gene. Pain 2007;130:25–30.
[52] Chen JF, Aloyo VJ, Weiss B. Continuous treatment with the d2 dopamine receptoragonist quinpirole decreases D2 dopamine receptors, D2 dopamine receptor mes-senger RNA and proenkephalin messenger RNA, and increases mu opioid receptorsin mouse striatum. Neuroscience 1993;54:669–80.
[53] Steiner H, Gerfen CR. Role of dynorphin and enkephalin in the regulation of striataloutput pathways and behavior. Exp Brain Res 1998;123:60–76.
[54] Ross JR, Riley J, Taegetmeyer AB, Sato H, Gretton S, du Bois RM, et al. Genetic vari-ation and response to morphine in cancer patients: catechol-O-methyltransferaseand multidrug resistance-1 gene polymorphisms are associated with central sideeffects. Cancer 2008;112:1390–403.
[55] Kadiev E, Patel V, Rad P, Thankachan L, Tram A, Weinlein M, et al. Role of pharma-cogenetics in variable response to drugs: focus on opioids. Expert Opin DrugMetabToxicol 2008;4:77–91.
[56] Fishbain DA, Fishbain D, Lewis J, Cutler RB, Cole B, Rosomoff HL, et al. Genetic test-ing for enzymes of drug metabolism: does it have clinical utility for pain medicineat the present time? A structured review. Pain Med 2004;5:81–93.
[57] Flockhart DA. Drug interactions: cytochrome p450 drug interaction. http://medi-cine.iupui.edu/clinpharm/ddis/clinical-table/; 2014 . [Accessed 28 January 2014].
[58] Ablin JN, Buskila D. Personalized treatment of pain. Curr Rheumatol Rep2013;15:298.
[59] Cherny N, Ripamonti C, Pereira J, Davis C, Fallon M, McQuay H, et al. Strategies tomanage the adverse effects of oral morphine: an evidence-based report. J ClinOncol 2001;19:2542–54.
[60] Rane A, Sawe J, Dahlstrom B, Paalzow L, Kager L. Pharmacological treatment of can-cer pain with special reference to the oral use of morphine. Acta AnaesthesiolScand 1982:74–103 [Supplementum].
[61] World Health Organization Cancer pain relief. http://www.whocancerpain.wisc.edu/?q=node/169; 1986 . [Accessed 21 January 2014].
[62] Vargas-Schaffer G. Is the who analgesic ladder still valid? Twenty-four years ofexperience. Can Fam Physician 2010;56:514–7.
[63] Varrassi G. Severe chronic pain–the reality of treatment in europe. Curr Med ResOpin 2011;27:2063–4.
[64] Rollins DE, von BC, Glaumann H, Moldeus P, Rane A. Acetaminophen: potentiallytoxic metabolite formed by human fetal and adult liver microsomes and isolatedfetal liver cells. Science 1979;205:1414–6.
[65] Mitchell JR, Jollow DJ, Potter WZ, Davis DC, Gillette JR, Brodie BB. Acetaminophen-induced hepatic necrosis. I. Role of drug metabolism. J Pharmacol Exp Ther1973;187:185–94.
[66] You K. Salicylate and mitochondrial injury in Reye's syndrome. Science1983;221:163–5.
[67] Reye RDK, Morgan G, Baral J. Encephalopathy and fatty degeneration of the visceraa disease entity on childhood. Lancet 1963;2(7311):749–52.
[68] Grosser T, Fries S, FitzGerald GA. Biological basis for the cardiovascular conse-quences of cox-2 inhibition: therapeutic challenges and opportunities. J Clin Invest2006;116:4–15.
[69] Mukherjee D. Does a coxib-associated thrombotic risk limit the clinical use of thecompounds as analgesic anti-inflammatory drugs? Arguments in favor. ThrombHaemost 2006;96:407–12.
[70] Antman EM, Bennett JS, Daugherty A, Furberg C, Roberts H, Taubert KA, et al. Use ofnonsteroidal antiinflammatory drugs: an update for clinicians: a scientific state-ment from the American Heart Association. Circulation 2007;115:1634–42.
[71] Jones VM. Acetaminophen injection: a review of clinical information. J Pain PalliatCare Pharmacother 2011;25:340–9.
[72] Portenoy RK. Treatment of cancer pain. Lancet 2011;377:2236–47.[73] Sawe J, Svensson JO, Rane A.Morphinemetabolism in cancer patients on increasing
oral doses–no evidence for autoinduction or dose-dependence. Br J Clin Pharmacol1983;16:85–93.
[74] Koch T, Hollt V. Role of receptor internalization in opioid tolerance and depen-dence. Pharmacol Ther 2008;117:199–206.
[75] Ferguson SS. Evolving concepts in g protein-coupled receptor endocytosis: the rolein receptor desensitization and signaling. Pharmacol Rev 2001;53:1–24.
[76] von Zastrow, Svingos A, Haberstock-Debic H, Evans C. Regulated endocytosis ofopioid receptors: cellular mechanisms and proposed roles in physiological adapta-tion to opiate drugs. Curr Opin Neurobiol 2003;13:348–53.
[77] Bailey CP, Connor M. Opioids: cellular mechanisms of tolerance and physical de-pendence. Curr Opin Pharmacol 2005;5:60–8.
[78] Mercadante S. Prospects and challenges in opioid analgesia for pain management.Curr Med Res Opin 2011;27:1741–3.
[79] Manchikanti L, Ailinani H, Koyyalagunta D, Datta S, Singh V, Eriator I, et al. A sys-tematic review of randomized trials of long-term opioid management for chronicnon-cancer pain. Pain Physician 2011;14:91–121.
[80] Al-Sayed AA, Al-Numay AM. Update and review on the basics of painmanagement.Neurosciences 2011;16:203–12.
[81] Martin WR. Pharmacology of opioids. Pharmacol Rev 1983;35:283–323.[82] Bohnert AS, Valenstein M, Bair MJ, Ganoczy D, McCarthy JF, Ilgen MA, et al. Associ-
ation between opioid prescribing patterns and opioid overdose-related deaths.JAMA 2011;305:1315–21.
[83] Chang G, Chen L, Mao J. Opioid tolerance and hyperalgesia. Med Clin North Am2007;91:199–211.
[84] Jamison RN, Serraillier J, Michna E. Assessment and treatment of abuse risk in opi-oid prescribing for chronic pain. Pain Res Treat 2011;2011:941808.
[85] Savage SR. Management of opioid medications in patients with chronic pain andrisk of substance misuse. Curr Psychiatry Rep 2009;11:377–84.
[86] Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a lit-erature review. Arch Intern Med 2003;163:2433–45.
[87] Cupp M. New oxycodone formulation: Oxyneo. Pharmaacist's Letter/Prescriber'sLetter; 2012.
[88] Houde RW. Analgesic effectiveness of the narcotic agonist-antagonists. Br J ClinPharmacol 1979;7:297S–308S.
[89] Vallejo R, Barkin RL, Wang VC. Pharmacology of opioids in the treatment of chronicpain syndromes. Pain Physician 2011;14:E343–60.
[90] Hutchinson MR, Menelaou A, Foster DJ, Coller JK, Somogyi AA. Cyp2d6 and cyp3a4involvement in the primary oxidative metabolism of hydrocodone by human livermicrosomes. Br J Clin Pharmacol 2004;57:287–97.
[91] Sansone RA, Sansone LA. Tramadol: seizures, serotonin syndrome, andcoadministered antidepressants. Psychiatry (Edgmont) 2009;6:17–21.
[92] Stahl SM. Mechanism of action of serotonin selective reuptake inhibitors. Serotoninreceptors and pathways mediate therapeutic effects and side effects. J Affect Disord1998;51:215–35.
[93] Nelson EM, Philbrick AM. Avoiding serotonin syndrome: the nature of the interac-tion between tramadol and selective serotonin reuptake inhibitors. AnnPharmacother 2012;46:1712–6.
[94] Dayer P, Desmeules J, Collart L. Pharmacologie du tramadol. Drugs 1997;53(Suppl.-24).
[95] Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet2004;43:879–923.
[96] Sawe J, Dahlstrom B, Paalzow L, Rane A. Morphine kinetics in cancer patients. AnnPharmacother 1981;30:629–35.
[97] Cregg R, Russo G, Gubbay A, Branford R, Sato H. Pharmacogenetics of analgesicdrugs. Br Pain 2013;7:189–206.
[98] Berkenstadt H, Segal E, Mayan H, Almog S, RotenbergM, Perel A, et al. The pharma-cokinetics of morphine and lidocaine in critically ill patients. Intensive Care Med1999;25:110–2.
[99] SmithMT. Neuroexcitatory effects of morphine and hydromorphone: evidence impli-cating the 3-glucuronide metabolites. Clin Exp Pharmacol Physiol 2000;27:524–8.
[100] Mather LE. Clinical pharmacokinetics of fentanyl and its newer derivatives. ClinPharmacokinet 1983;8:422–46.
[101] Reynolds L, Rauck R, Webster L, DuPen S, Heinze E, Portenoy R, et al. Relativeanalgesic potency of fentanyl and sufentanil during intermediate-term infusions inpatients after long-term opioid treatment for chronic pain. Pain 2004;110:182–8.
[102] Kosek E, Jensen KB, Lonsdorf TB, Schalling M, Ingvar M. Genetic variationin the serotonin transporter gene (5-HTTLPR, RS25531) influences the analge-sic response to the short acting opioid remifentanil in humans. Mol Pain2009;5:37.
[103] Burkle H, Dunbar S, Van AH. Remifentanil: a novel, short-acting, mu-opioid. AnesthAnalg 1996;83:646–51.
[104] Anderson D. A review of systemic opioids commonly used for labor pain relief. JMidwifery Womens Health 2011;56:222–39.

1186 B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
[105] Leong WL, Sng BL, Sia AT. A comparison between remifentanil and meperidine forlabor analgesia: A systematic review. Anesth Analg 2011;113:818–25.
[106] Kan RE, Hughes SC, Rosen MA, Kessin C, Preston PG, Lobo EP. Intravenousremifentanil: placental transfer, maternal and neonatal effects. Anesthesiology1998;88:1467–74.
[107] FredheimOM, Borchgrevink PC, Klepstad P, Kaasa S, Dale O. Long termmethadone forchronic pain: a pilot study of pharmacokinetic aspects. Eur J Pain 2007;11:599–604.
[108] Lugo RA, Satterfield KL, Kern SE. Pharmacokinetics of methadone. J Pain Palliat CarePharmacother 2005;19:13–24.
[109] Eap CB, Buclin T, Baumann P. Interindividual variability of the clinical pharmacoki-netics of methadone: implications for the treatment of opioid dependence. ClinPharmacokinet 2002;41:1153–93.
[110] Kapur BM, Hutson JR, Chibber T, Luk A, Selby P. Methadone: a review of drug–drugand pathophysiological interactions. Crit Rev Clin Lab Sci 2011;48:171–95.
[111] Perrin-Terrin A, Pathak A, Lapeyre-Mestre M. Qt interval prolongation: prevalence,risk factors and pharmacovigilance data among methadone-treated patients infrance. Fundam Clin Pharmacol 2011;25:503–10.
[112] Johnson RE, Fudala PJ, Payne R. Buprenorphine: considerations for pain manage-ment. J Pain Symptom Manage 2005;29:297–326.
[113] Pergolizzi J, Aloisi AM,DahanA, Filitz J, Langford R, Likar R, et al. Current knowledge ofbuprenorphine and its unique pharmacological profile. Pain Pract 2010;10:428–50.
[114] Leow KP, Cramond T, Smith MT. Pharmacokinetics and pharmacodynamics of oxy-codone when given intravenously and rectally to adult patients with cancer pain.Anesth Analg 1995;80:296–302.
[115] Sloan P. Review of oral oxymorphone in the management of pain. Ther Clin RiskManage 2008;4:777–87.
[116] Batterman RC. Clinical effectiveness and safety of a new synthetic analgesic drug,demerol. Arch Intern Med 1943;71:345–56.
[117] Latta KS, Ginsberg B, Barkin RL. Meperidine: a critical review. Am J Ther2002;9:53–68.
[118] Saravanakumar K, Garstang JS, Hasan K. Intravenous patient-controlled analgesiafor labour: a survey of UK practice. Int J Obstet Anesth 2007;16:221–5.
[119] Tveit TO, Halvorsen A, Rosland JH. Analgesia for labour: a survey of Norwegianpractice — with a focus on parenteral opioids. Acta Anaesthesiol Scand2009;53:794–9.
[120] Prommer E. Levorphanol: the forgotten opioid. Support Care Cancer 2007;15:259–64.[121] Sansone RA, Sansone LA. Pain, pain, go away: antidepressants and pain manage-
ment. Psychiatry (Edgmont) 2008;5:16–9.[122] Gureje O, Von KM, Simon GE, Gater R. Persistent pain and well-being: a World
Health Organization study in primary care. JAMA 1998;280:147–51.[123] Eardley W, Toth C. An open-label, non-randomized comparison of venlafaxine and
gabapentin as monotherapy or adjuvant therapy in themanagement of neuropath-ic pain in patients with peripheral neuropathy. J Pain Res 2010;1:33–49.
[124] Moulin DE, Clark AJ, Gilron I, Ware MA,Watson CP, Sessle BJ, et al. Pharmacologicalmanagement of chronic neuropathic pain - consensus statement and guidelinesfrom the canadian pain society. Pain Res Manag 2007;12:13–21.
[125] Jensen TS. Anticonvulsants in neuropathic pain: rationale and clinical evidence. EurJ Pain 2002;6:A61–8.
[126] Bagheri SC, Farhidvash F, Perciaccante VJ. Diagnosis and treatment of patients withtrigeminal neuralgia. J Am Dent Assoc 2004;135:1713–37.
[127] Dolder CR, Nealy KL. The efficacy and safety of newer anticonvulsants in patientswith dementia. Drugs Aging 2012;29:627–37.
[128] Rose MA, Kam PC. Gabapentin: pharmacology and its use in pain management.Anaesthesia 2002;57:451–62.
[129] Ward KE, Archambault R, Mersfelder TL. Severe adverse skin reactions to nonste-roidal antiinflammatory drugs: a review of the literature. Am J Health Syst Pharm2010;67:206–13.
[130] Gentile G, Borro M, Simmaco M, Missori S, Lala N, Martelletti P. Gene polymor-phisms involved in triptans pharmacokinetics and pharmacodynamics in migrainetherapy. Expert Opin Drug Metab Toxicol 2011;7:39–47.
[131] Loder E. Triptan therapy in migraine. N Engl J Med 2010;363:63–70.[132] Gawel MJ, Worthington I, Maggisano A. A systematic review of the use of triptans
in acute migraine. Can J Neurol Sci 2001;28:30–41.[133] Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain manage-
ment? Pain 1994;57:137–52.[134] Manzanares J, Julian M, Carrascosa A. Role of the cannabinoid system in pain con-
trol and therapeutic implications for the management of acute and chronic painepisodes. Curr Neuropharmacol 2006;4:239–57.
[135] Walker JM, Huang SM. Cannabinoid analgesia. Pharmacol Ther 2002;95:127–35.[136] Leung L. Cannabis and its derivatives: review of medical use. J Am Board Fam Med
2011;24:452–62.[137] Abrams DI, Jay CA, Shade SB, Vizoso H, Reda H, Press S, et al. Cannabis in painful
hiv-associated sensory neuropathy: a randomized placebo-controlled trial. Neurol-ogy 2007;68:515–21.
[138] Ellis RJ, Toperoff W, Vaida F, van den BG, Gonzales J, Gouaux B, et al. Smoked me-dicinal cannabis for neuropathic pain in HIV: a randomized, crossover clinical trial.Neuropsychopharmacology 2009;34:672–80.
[139] Rog DJ, Nurmikko TJ, Friede T, Young CA. Randomized, controlled trial of cannabis-based medicine in central pain in multiple sclerosis. Neurology 2005;65:812–9.
[140] Vaney C, Heinzel-Gutenbrunner M, Jobin P, Tschopp F, Gattlen B, Hagen U, et al.Efficacy, safety and tolerability of an orally administered cannabis extract in thetreatment of spasticity in patients with multiple sclerosis: a randomized, double-blind, placebo-controlled, crossover study. Mult Scler 2004;10:417–24.
[141] Zajicek JP, Sanders HP, Wright DE, Vickery PJ, Ingram WM, Reilly SM, et al. Canna-binoids in multiple sclerosis (cams) study: safety and efficacy data for 12 monthsfollow up. J Neurol Neurosurg Psychiatry 2005;76:1664–9.
[142] Ware M, Beaulieu P. Cannabinoids for the treatment of pain: an update on recentclinical trials. Pain Res Manag 2005;10:27A–30A.
[143] de Vries M, van Rijckevorsel DC, Wilser-Smith OH, van Goor H. Dronabinoland chronic pain: importance of mechanistic considerations. Expert OpinPharmacother 2014;12:1–10.
[144] Clark AJ, Lynch ME, Ware M, Beaulieu P, McGilveray IJ, Gourlay D. Guidelines forthe use of cannabinoid compounds in chronic pain. Pain Res Manag2005;10:44A–6A.
[145] Donoghue K, Doody GA, Murray RM, Jones PB, Morgan C, Dazzan P, et al. Cannabisuse, gender and age of onset of schizophrenia: data from the ÆSOP Study. Psychi-atry Res 2014;215:528–32.
[146] Olivera BM. Conus peptides: biodiversity-based discovery and exogenomics. J BiolChem 2006;281:31173–7.
[147] Schmidtko A, Lotsch J, Freynhagen R, Geisslinger G. Ziconotide for treatment ofsevere chronic pain. Lancet 2010;375:1569–77.
[148] Wermeling D, Drass M, Ellis D, Mayo M, McGuire D, O'Connell D, et al. Pharmaco-kinetics and pharmacodynamics of intrathecal ziconotide in chronic pain patients.J Clin Pharmacol 2003;43:624–36.
[149] Geranton SM. Targeting epigenetic mechanisms for pain relief. Curr OpinPharmacol 2012;12:35–41.
[150] Tajerian M, Alvarado S, Millecamps M, Dashwood T, Anderson KM, Haglund L, et al.DNA methylation of sparc and chronic low back pain. Mol Pain 2011;7:65.
[151] Uchida H, Sasaki K, Ma L, Ueda H. Neuron-restrictive silencer factor causes epige-netic silencing of Kv4.3 gene after peripheral nerve injury. Neuroscience2010;166:1–4.
[152] Uchida H, Ma L, Ueda H. Epigenetic gene silencing underlies c-fiber dysfunctions inneuropathic pain. J Neurosci 2010;30:4806–14.
[153] Robak T. New nucleoside analogs for patients with hematological malignancies.Expert Opin Investig Drugs 2011;20:343–59.
[154] Bai G, Wei D, Zou S, Ren K, Dubner R. Inhibition of class ii histone deacetylases inthe spinal cord attenuates inflammatory hyperalgesia. Mol Pain 2010;6:51.
[155] Agrawal RP, Goswami J, Jain S, Kochar DK. Management of diabetic neuropathy bysodium valproate and glyceryl trinitrate spray: a prospective double-blindrandomized placebo-controlled study. Diabetes Res Clin Pract 2009;83:371–8.
[156] Handy CR, Krudy C, Boulis N. Gene therapy: a potential approach for cancer pain.Pain Res Treat 2011:987597.
[157] Fink DJ, Wechuck J, Mata M, Glorioso JC, Goss J, Krisky D, et al. Gene therapy forpain: results of a phase i clinical trial. Ann Neurol 2011;70:207–12.
[158] Manchikanti L, Damron KS, McManus CD, Barnhill RC. Patterns of illicit drug useand opioid abuse in patients with chronic pain at initial evaluation: a prospective,observational study. Pain Physician 2004;7:431–7.
[159] Manchikanti L, Manchukonda R, Pampati V, Damron KS, Brandon DE, Cash KA, et al.Does random urine drug testing reduce illicit drug use in chronic pain patientsreceiving opioids? Pain Physician 2006;9:123–9.
[160] Manchikanti L, Atluri S, Trescot AM,Giordano J.Monitoring opioid adherence in chron-ic pain patients: tools, techniques, and utility. Pain Physician 2008;11(Suppl.-80).
[161] Nafziger AN, Bertino Jr JS. Utility and application of urine drug testing in chronicpain management with opioids. Clin J Pain 2009;25:73–9.
[162] Kapur BM, Verjee Z, AndersonM, Geisbrecht E. Urinary eddp (methadonemetabolite)as amarker of compliance anddiversion ofmethadone. TherDrugMonit 1995;17:388.
[163] Jannetto PJ, Bratanow NC. Pain management in the 21st century: utilization ofpharmacogenomics and therapeutic drug monitoring. Expert Opin Drug MetabToxicol 2011;7:745–52.
[164] Levy G, Tsuchiya T. Salicylate accumulation kinetics in man. N Engl J Med1972;287:430–2.
[165] Adams SS, McCullough KF, Nicholson JS. The pharmacological properties of ibupro-fen, an anti-inflammatory, analgesic and antipyretic agent. Arch Int PharmacodynTher 1969;178:115–29.
[166] Alvan G, Orme M, Bertilsson L, Ekstrand R, Palmer L. Pharmacokinetics of indo-methacin. Clin Pharmacol Ther 1975;18:364–73.
[167] Morris ME, Levy G. Renal clearance and serum protein binding of acetaminophenand its major conjugates in humans. J Pharm Sci 1984;73:1038–41.
[168] Davies NM, McLachlan AJ, Day RO, Williams KM. Clinical pharmacokinetics andpharmacodynamics of celecoxib: a selective cyclo-oxygenase-2 inhibitor. ClinPharmacokinet 2000;38:225–42.
[169] Baselt R. Disposition of toxic drugs and chemicals in man. Ninth Edition ed. SealBeach, California: Biomedical Publications; 2011.
[170] Blaine JD. Buprenorphine: an alternative treatment for opioid dependence. In: JackD, Blaine P, editors. 5600 Fishers Lane, Rockville, MD 20857, USA: National Instituteon Drug Abuse; 1992.
[171] Bullingham RE, McQuay HJ, Moore A, Bennett MR. Buprenorphine kinetics. ClinPharmacol Ther 1980;28:667–72.
[172] Han T, Harmatz JS, Greenblatt DJ, Martyn JA. Fentanyl clearance and volume ofdistribution are increased in patients with major burns. J Clin Pharmacol2007;47:674–80.
[173] Parab PV, Ritschel WA, Coyle DE, Gregg RV, Denson DD. Pharmacokinetics ofhydromorphone after intravenous, peroral and rectal administration to humansubjects. Biopharm Drug Dispos 1988;9:187–99.
[174] Ramirez J, Innocenti F, Schuetz EG, Flockhart DA, Relling MV, Santucci R, et al.CYP2B6, CYP3A4, and CYP2C19 are responsible for the in vitro n-demethylationof meperidine in human liver microsomes. Drug Metab Dispos 2004;32:930–6.
[175] Pond SM, Tong T, Benowitz NL, Jacob P, Rigod J. Presystemic metabolism of meper-idine to normeperidine in normal and cirrhotic subjects. Clin Pharmacol Ther1981;30:183–8.
[176] Schulz P, Turner-Tamiyasu K, Smith G, Giacomini KM, Blaschke TF. Amitriptylinedisposition in young and elderly normal men. Clin Pharmacol Ther 1983;33:360–6.

1187B.M. Kapur et al. / Clinical Biochemistry 47 (2014) 1169–1187
[177] Stewart JJ, Berkel HJ, Parish RC, Simar MR, Syed A, Bocchini Jr JA, et al. Single-dosepharmacokinetics of bupropion in adolescents: effects of smoking status andgender. J Clin Pharmacol 2001;41:770–8.
[178] Rampono J, Kristensen JH, Hackett LP, Paech M, Kohan R, Ilett KF. Citalopram anddemethylcitalopram in human milk; distribution, excretion and effects in breastfed infants. Br J Clin Pharmacol 2000;50:263–8.
[179] Rudorfer MV, Lane EA, Chang WH, Zhang MD, Potter WZ. Desipramine pharmaco-kinetics in chinese and caucasian volunteers. Br J Clin Pharmacol 1984;17:433–40.
[180] Deepak P, Kumar TN. Duloxetine - pharmacological aspects. Int J Biol Med Res2011;2:589–92.
[181] Altamura AC, Moro AR, Percudani M. Clinical pharmacokinetics of fluoxetine. ClinPharmacokinet 1994;26:201–14.
[182] Ellingrod VL, Perry PJ. Venlafaxine: a heterocyclic antidepressant. Am J Hosp Pharm1994;51:3033–46.
[183] Mesdjian E, Seree E, Charvet B, Mirrione A, Bourgarel-Rey V, Desobry A, et al.Metabolism of carbamazepine by CYP3A6: a model for in vitro drug interactionsstudies. Life Sci 1999;64:827–35.
[184] Rawlins MD, Collste P, Bertilsson L, Palmer L. Distribution and elimination kineticsof carbamazepine in man. Eur J Clin Pharmacol 1975;8:91–6.
[185] McLean MJ. Clinical pharmacokinetics of gabapentin. Neurology 1994;44(Suppl.-22).[186] Chan V, Morris RG, Ilett KF, Tett SE. Population pharmacokinetics of lamotrigine.
Ther Drug Monit 2001;23:630–5.[187] Bergen DC. Pharmacokinetics of phenytoin: reminders and discoveries. Epilepsy
Curr 2009;9:102–4.[188] Cuttle L, Munns AJ, Hogg NA, Scott JR, Hooper WD, Dickinson RG, et al. Phenytoin
metabolism by human cytochrome P450: involvement of P450 3A and 2C formsin secondary metabolism and drug-protein adduct formation. Drug Metab Dispos2000;28:945–50.